 Qiujiang Li
Qiujiang Li Xingxia Long2†
Xingxia Long2† Yueming Song
Yueming Song
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 19 June 2024
Sec. Bone Research
Volume 15 - 2024 | https://doi.org/10.3389/fendo.2024.1391970
This article is part of the Research TopicOrgan System Crosstalk in Degenerative Musculoskeletal DiseasesView all 11 articles
Objective: To investigate the relationship between degeneration of cervical intervertebral disc and degeneration of paravertebral muscles[multifidus (MF), cervical semispinalis (SCer), semispinalis capitis (SCap) and splenius capitis (SPL)].
Methods: 82 patients with chronic neck pain were randomly selected, including 43 males and 39 females, with 50.73 0.7.51 years old. All patients were scanned by 3.0T MRI Philips Ingenia performed conventional MRI sequence scanning and fat measurement sequence mDIXON-Quant scanning of cervical. Fat infiltration (FI) and cross-sectional area (CSA) of cervical paravertebral muscle (MF, SCer, SCap and SPL) at central level of C5–6 disc were measured by Philips 3.0T MRI image post-processing workstation. According to Pfirrmann grading system, there was no grade I in the included cases. The number of grade IIr IV cases were n=16, 40, 19 and 7 respectively. CSA and FI of cervical paravertebral muscles were compared with t test or one-way ANOVA, Spearman correlation analysis was used to evaluate the correlation between age, disc degeneration, and CSA, FI of cervical paravertebral muscles, and multiple linear regression analysis was used to analyze the independent influencing factors of CSA and FI.
Results: CSA of cervical paravertebral muscles in male patients was significantly higher than that in female patients (all P<0.001), but there was no significant difference in FI (all P>0.05). Age was weakly correlated with CSA of MF+SCer, moderately correlated with CSA of SCap and SPL (r=-0.256, -0.355 and -0.361, P<0.05), weakly correlated with FI of SCap and SPL (r= 0.182 and 0.264, P<0.001), moderately correlated with FI of MF+SCer (r=0.408, P<0.001). There were significant differences in FI with disc degeneration (P<0.001, P=0.028 and P=0.005). Further correlation analysis showed that disc degeneration was strongly correlated with FI of MF+SCer (r=0.629, P<0.001), and moderately correlated with FI of SCap and SPL (r=0.363, P=0.001; r=0.345, P=0.002). Multiple linear regression analysis showed that sex and age were the influencing factors of CSA of SCap and SPL, sex was the independent influencing factor of CSA of MF+SCer, and disc degeneration was the independent influencing factor of FI.
Conclusions: Age is negatively correlated with CSA and positively correlated with FI. Disc degeneration was correlated with FI of paravertebral muscles, especially with FI of MF and SCer. Sex and age were the influencing factors of CSA, while disc degeneration was the independent influencing factor of FI.
Chronic neck pain and low back pain are common symptoms in the general population, mostly in middle-aged and elderly people, and increase with age (1). The degeneration of paravertebral muscles may be one of the important causes of chronic neck pain and low back pain (2). One study has reported reduced muscle CSA in patients with low back pain compared to asymptomatic controls (3). Similarly, related studies have found that paraspinal muscle atrophy is more pronounced in patients with low back pain than in those without low back pain, and that paraspinal muscle atrophy is more pronounced on the symptomatic side than on the asymptomatic side (4–6). Therefore, many studies have confirmed that lumbar paravertebral muscle degeneration is closely related to the occurrence, development, clinical efficacy and prognosis of lumbar degenerative diseases. Paracervical musculature plays an important role in maintaining the level and neutrality of the cervical spine and in distributing head loads through flexion, extension, and translation movements (7, 8). It is estimated that neck muscles provide about 80% of total stability, while bony ligament structures contribute the remaining 20%. Degeneration of the deep neck extensors, which support neck movement and provide neck stability, has been associated with neck pain.
Spinal degeneration begins at the intervertebral disc. The early imaging signs of cervical disc degeneration show changes in disc signal, but few scholars have evaluated the FI of paravertebral muscles and cervical disc degeneration. Therefore, the correlation between disc signal and paravertebral muscle degeneration can better reflect the role of paravertebral muscle in the occurrence and development of cervical degenerative diseases. However, there are no relevant research reports. Meanwhile, most of the studies are subjective evaluation or semi-quantitative analysis of paravertebral muscle degeneration, and there are observation data bias and lack of reliability of experimental data to some extent (9, 10). The mDIXON-Quant technology is a new magnetic resonance scanning technology for quantitative fat measurement based on the principle of water-fat separation technology based on chemical shift introduced in recent years (11–13). At present, it is mainly applied to quantitative measurement of liver fat, but there is no report on FI evaluation of paravertebral muscle (11). Therefore, this study intends to use mDIXON-Quant technique to quantitatively measure FI of paravertebral muscles and evaluate the correlation between FI of paravertebral muscles and cervical disc degeneration.
82 patients with chronic neck pain were randomly selected from outpatient or inpatient department. In order to exclude the influence of different MRI machines on the results, we uniformly selected the cases scanned by Philips Ingenia 3.0T MRI scanner in our hospital. Inclusion criteria were as follows: (1) Patients with chronic neck pain; (2) mDIXON-Quant sequence for 3.0T MRI and fat measurement; (3) aged from 30 to 75 years old; (4) Body Mass Index (BMI) between 18.5 and 23.9; (5) No physical therapy, acupuncture and other treatment measures affecting paravertebral muscles. Exclusion criteria were as follows: (1) Patients with a history of cervical spine surgery or cervical spine trauma; (2) Patients with concomitant diseases of important organs or serious systemic diseases; (3) MRI images were poor, and the range and boundary of muscles could not be distinguished and recognized well;④ Patients with MRI contraindications exist.
Conventional MRI sequences (T1WI, T2WI, T2WI-mDIXON) and fat-measuring sequences (mDIXON-Quant) of cervical spine were performed with Philips Ingenia in supine position. mDIXON-Quant parameters: flip angle, 3°; TR, 5.8 ms; TE, 1.02 ms; voxel, 2.5 mm×2.5 mm×6mm; slice thickness, 6mm; field of view, 400mm×350mm×210mm; matrix, 160×40×70; and number of excitations, 1. The relevant scanning parameters are shown in Table 1.
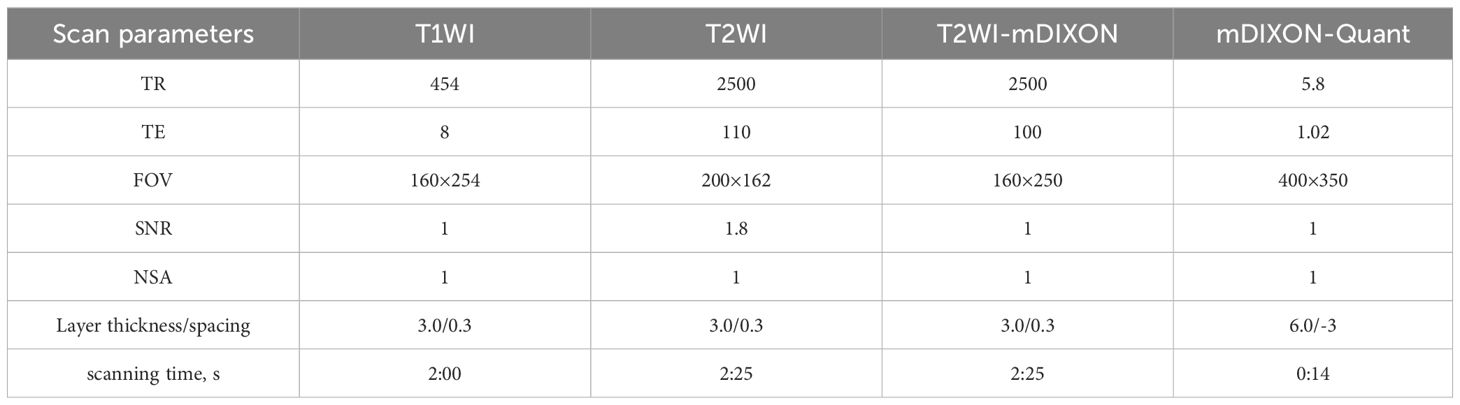
Table 1 List of scanning parameters of MRI sequences.
We graded the degree of cervical disc degeneration by using the internationally common Pfirrmann classification system on the median sagittal position of 3.0T MRI with the help of Picture Archiving and Communications Systems (PACS) (14). Pfirrmann classification system divides disc degeneration into 5 grades. Pfirrmann grade I is mainly found in children, so only Pfirrmann grade II~IV disc degeneration is studied in this study. C5–6 is the most common segment for cervical disc degenerative disease, so this study will analyze this segment. The cervical disc grading results were assessed independently by 3 spine surgeons, and the results with different opinions were discussed and decided together. Finally, all the results were summarized and collected.
The axial scan images of mDIXON-Quant sequence were transmitted to Philips 3.0T MRI image post-processing workstation. Two doctors with more than 5 years of experience in skeletal muscle imaging delineated the region of interest (ROI) of all C5–6 disc center layers on fat fraction images respectively. The ROI of cervical paravertebral muscles was set at multifidus (MF), cervical semispinalis (SCer), semispinalis capitis (SCap) and splenius capitis (SPL) on both sides respectively. Along the muscle contour, the system automatically generates ROI fat fraction (FF), i.e. FI and CSA, as shown in Figure 1. The left and right sides of each paravertebral muscle were measured three times and the average value was taken. The CSA representative value of the muscle at the same level was taken as the average value of CSA of the muscle at the same level. Similarly, the average FI value of the left and right muscles at the same level was taken as the FI representative value of the muscle at that level. In previous studies, MF and SCer muscles were not clearly demarcated on MRI in some cases, and both muscles belonged to deep neck extensors. Therefore, MF and SCer muscles were analyzed as a whole in this study.
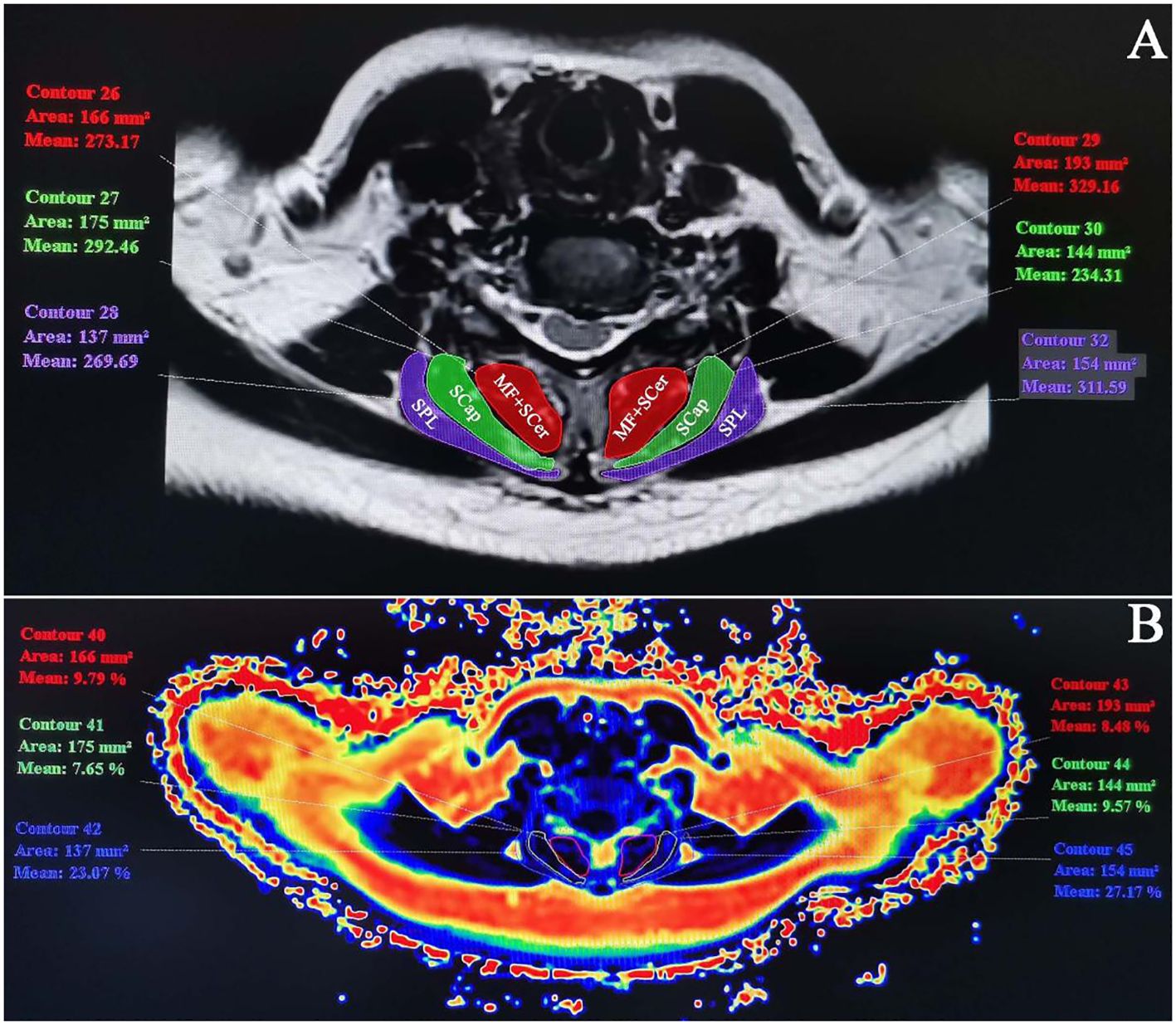
Figure 1 CSA and FI measurements of cervical paravertebral muscles at C5–6. (A) C5–6 T2WI axial sequence. CSA was measured along the outline of the muscles: MF+SCer, SCap and SPL. (B) Fat pseudo-color map. Measure ROI muscle FI in FF image.).
Twenty patients were randomly selected for repeated measurement. CSA and FI of paracervical muscles were measured independently and without interference by two observers. Inter-observer consistency of measurements was evaluated using intra-class correlation coefficients (ICC) between two observers measuring one week apart; in addition, intra-observer consistency of measurements was evaluated using ICC when one of the observers repeated measurements one week later. ICC>0.75 is considered to have good measurement consistency.
Data were analyzed statistically using SPSS 26.0 software (SPSS Inc., Chicago, IL, USA) and presented as mean ± standard deviation. For quantitative data conforming to normal distribution, t test was used for comparison between two groups, variance analysis was used for comparison between multiple groups, and rank sum test was used for non-normal distribution. Spearman correlation analysis was used to analyze the correlation between variables, and multiple linear regression analysis was used to analyze the independent influencing factors of paravertebral muscle degeneration. Correlation coefficient r≥0.7 was considered significant correlation; r=0.5~0.7 was strong correlation; r=0.3~0.5 was moderate correlation; r ≤ 0.3 was weak correlation. P<0.05 was statistically significant.
The ICC of CSA and FI of cervical paraspinal muscles was greater than 0.75 within and between observers, indicating good consistency (Table 2). A total of 82 patients were included in this study, 43 males and 39 females, with an average age of 50.73 0.7.51 years, of which 40 - 50 years and 50 - 60 years were the main population, accounting for 30.49% (25/82) and 35.37% (29/82) respectively. In this study, C5–6 was selected as the most common cervical segment degeneration. 16 cases (19.51%), 40 cases (48.78%), 19 cases (23.17%) and 7 cases (8.54%) of C5–6 were grade II, III, IV and V, respectively (Table 3).
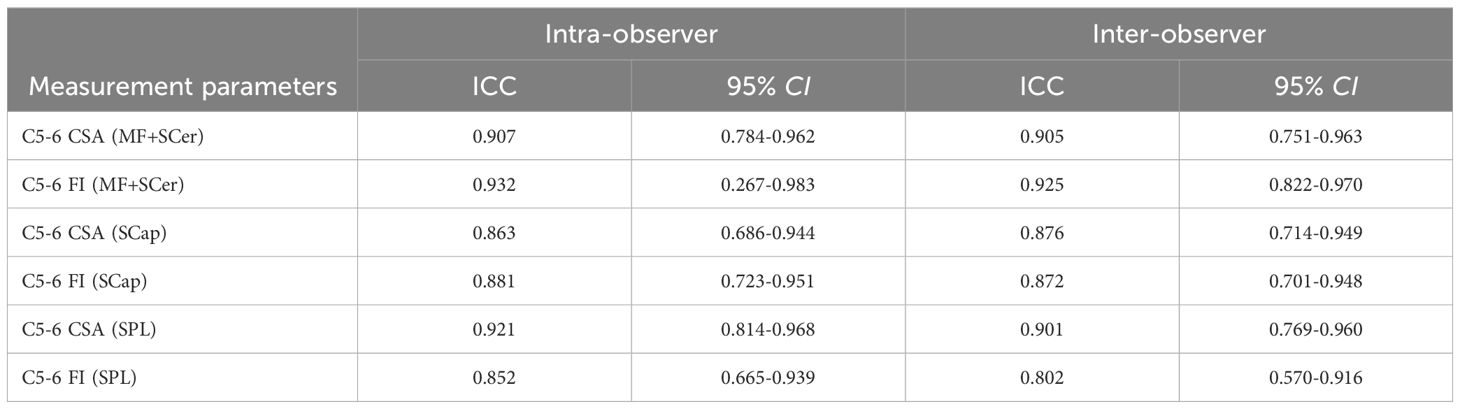
Table 2 Intra-and inter-observer consistency of CSA and FI measurements of cervical paravertebral muscles.
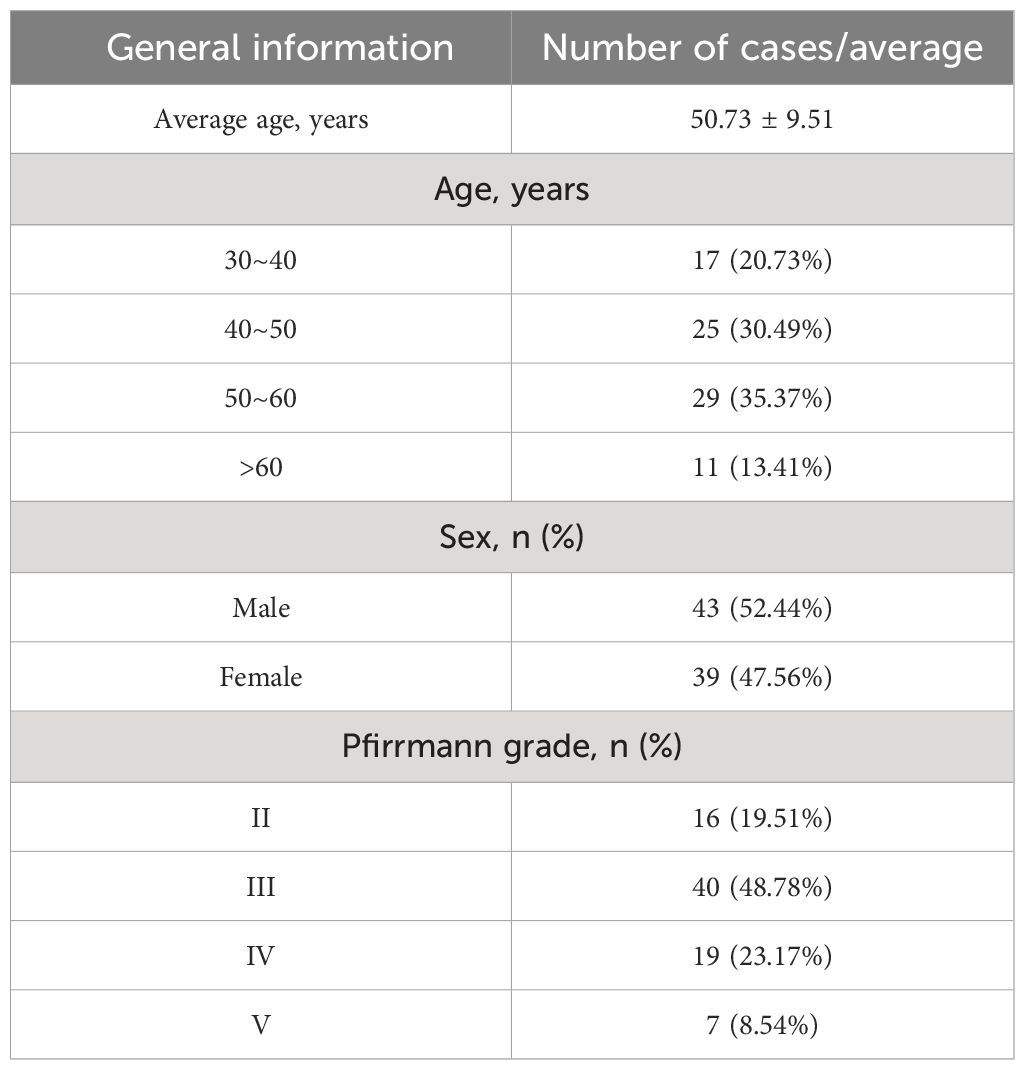
Table 3 General information of patients with cervical degenerative diseases.
CSA in MF+SCer, SCap, and SPL were significantly higher in males than in females (all P<0.001), but not in FI (all P>0.05) (Table 4). In CSA of cervical paravertebral muscles, there were statistically significant differences in SCap and SPL between age (P=0.007 and P=0.005); in FI of cervical paravertebral muscles, there were statistically significant differences in MF+SCer and SPL between age (P=0.015 and P=0.019) (Table 5). Further Spearman correlation analysis showed that age was positively correlated with CSA of MF+SCer, SCap and SPL, and weakly correlated with CSA of MF+SCer, and moderately correlated with CSA of SCap and SPL (r =-0.256,-0.355 and-0.361, respectively, P<0.05); age was positively correlated with FI of MF+SCer, SCap and SPL, and weakly correlated with FI of SCap and SPL (r = 0.182 and 0.264, respectively), and moderately correlated with FI of MF+SCer (r=0.408, P<0.001) (Figure 2).
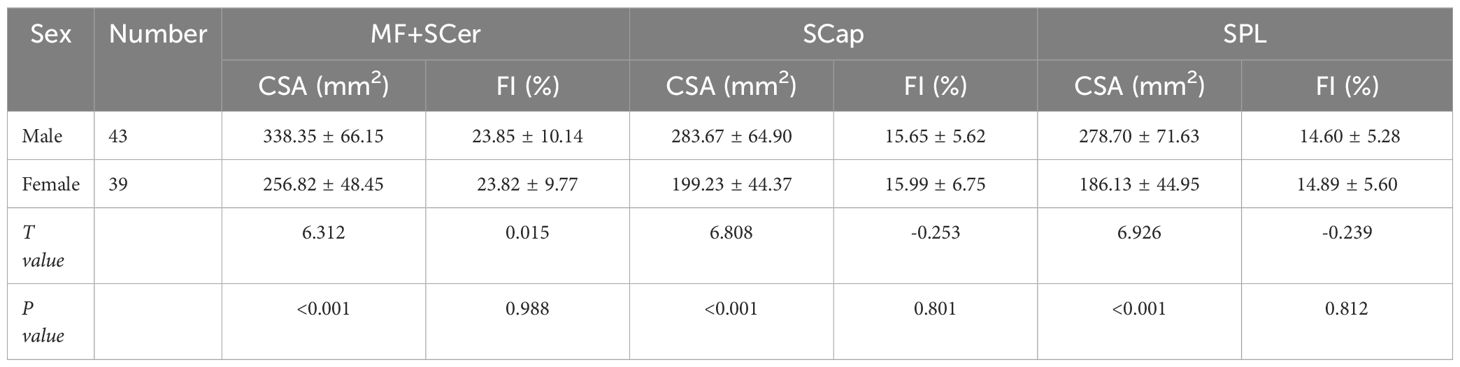
Table 4 Comparison of CSA and FI of Paracervical muscle between sex( ± s).
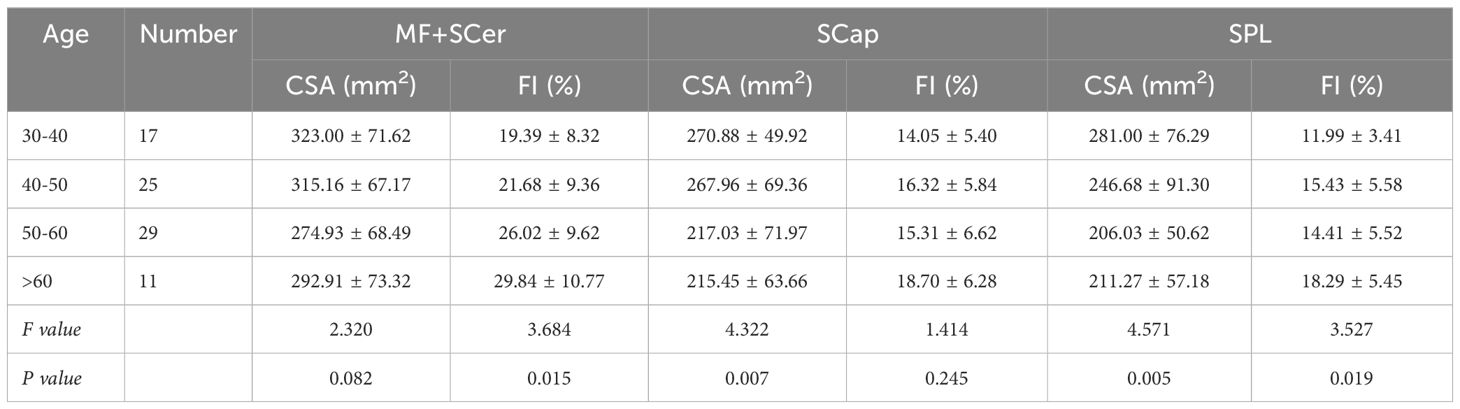
Table 5 Comparison of CSA and FI of cervical paravertebral muscles between age ( ± s).
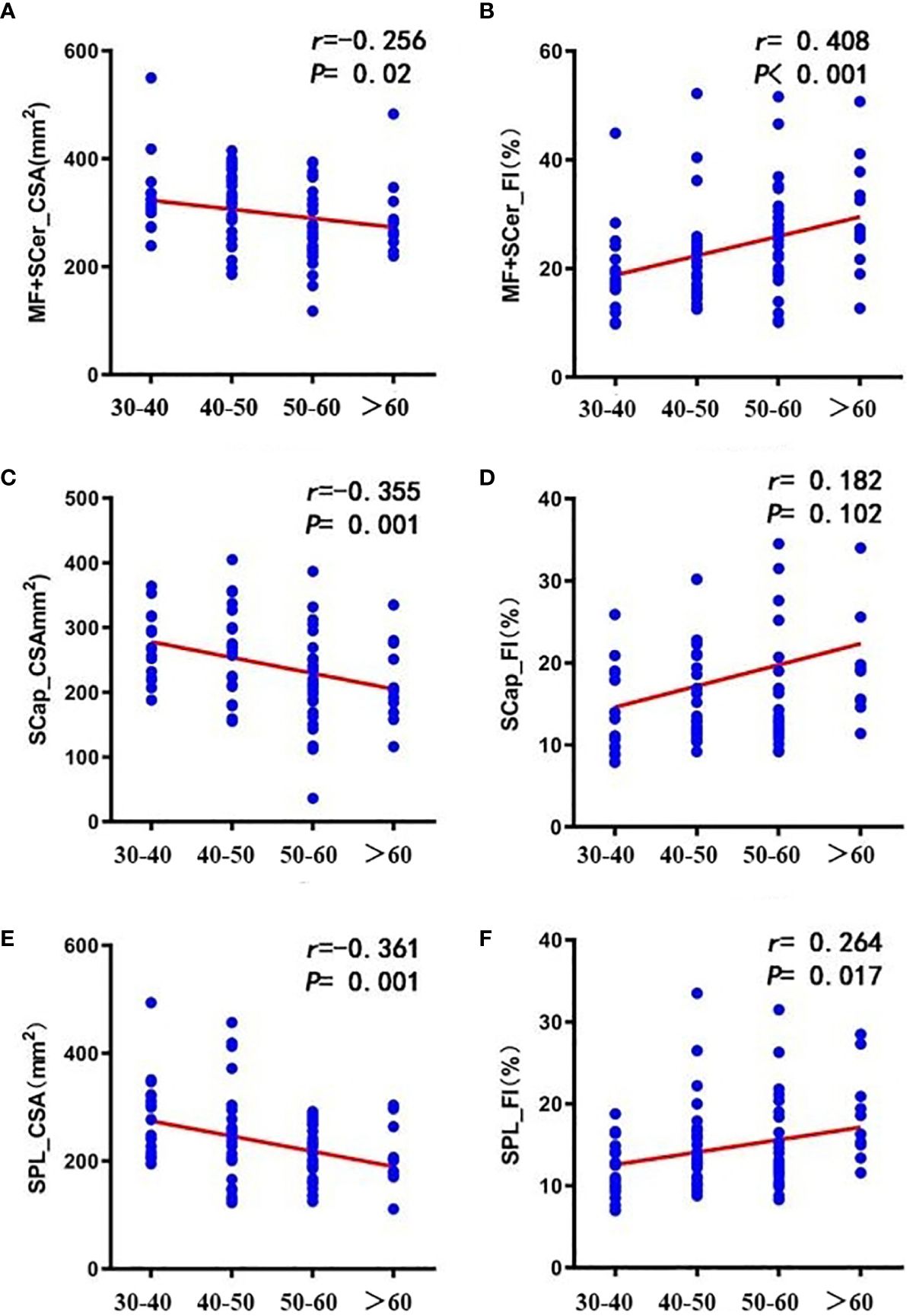
Figure 2 Correlation between age and CSA (A, C, E) and FI (B, D, F) of cervical paravertebral muscles. [(A, B) MF+SCer; (C, D) SCap; (E, F) SPL].
FI of cervical paravertebral muscles was significantly different in patients with different degree of disc degeneration (P<0.001, P=0.028 and P=0.005) (Table 6). Spearman correlation analysis showed that the degree of disc degeneration was strongly correlated with FI of MF+SCer (r=0.629, P<0.001), and moderately correlated with FI of SCap and SPL (r=0.363, P=0.001;r=0.345, P=0.002) (Figure 3).
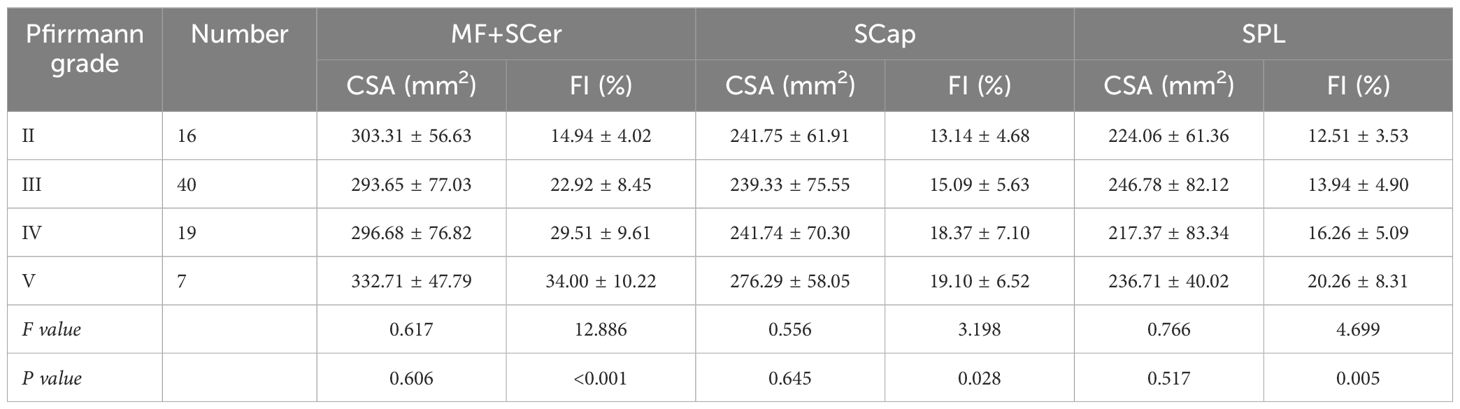
Table 6 Differences in CSA and FI of cervical paravertebral muscles in patients with different degrees of cervical disc degeneration ( ± s).
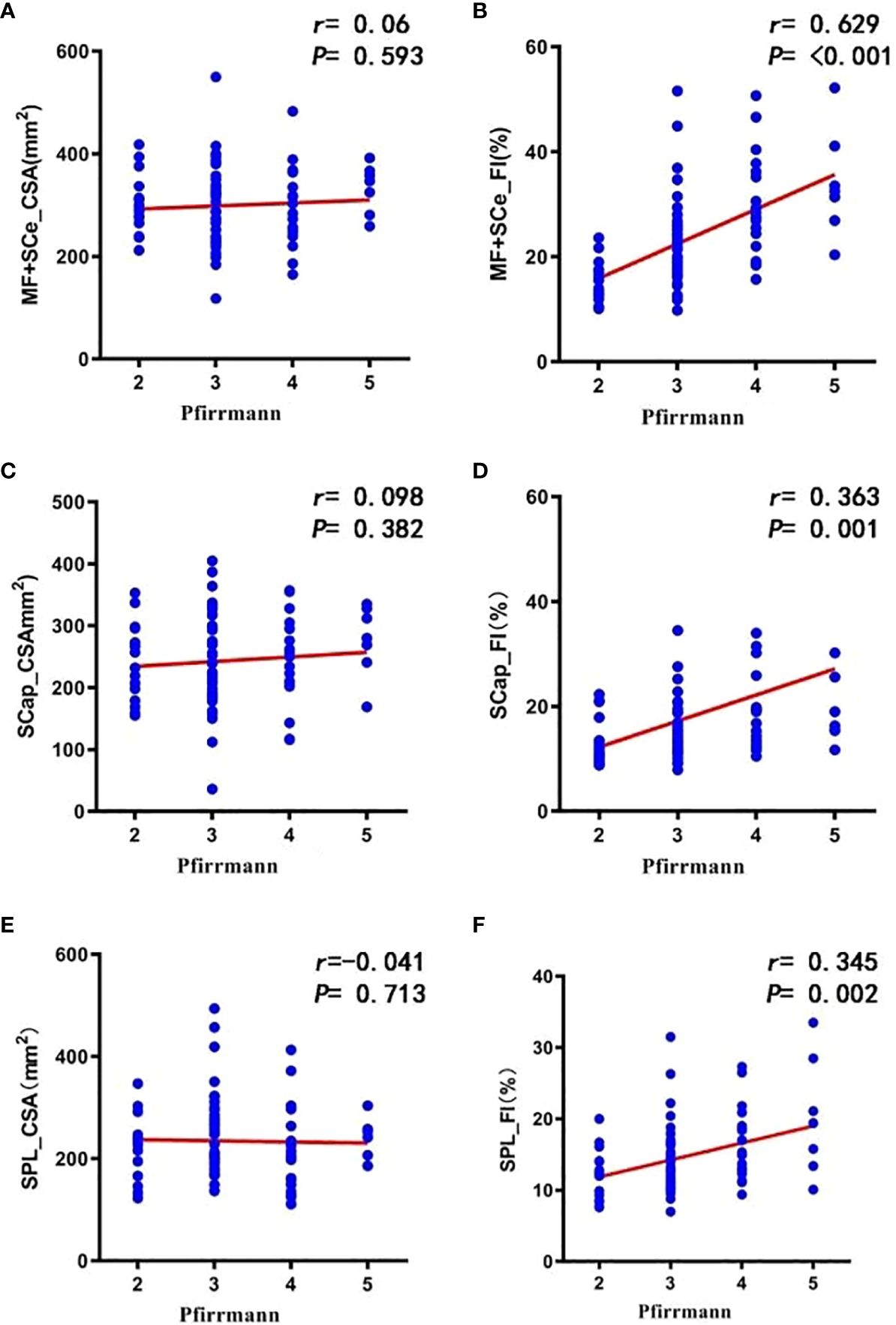
Figure 3 Correlation between the degree of disc degeneration and total CSA (A, C, E) and total FI (B, D, F) of cervical paravertebral muscles.
Multivariate linear regression analysis was used to evaluate whether sex, age and disc degeneration grade were independent factors of CSA and FI. The results showed that sex and age were independent factors of CSA and SPL of paravertebral muscles; sex was independent factor of MF+SCer CSA; disc degeneration grade was independent factor of FI of paravertebral muscles (P<0.001, P<0.001, P=0.01, P=0.006) (Tables 7–9).
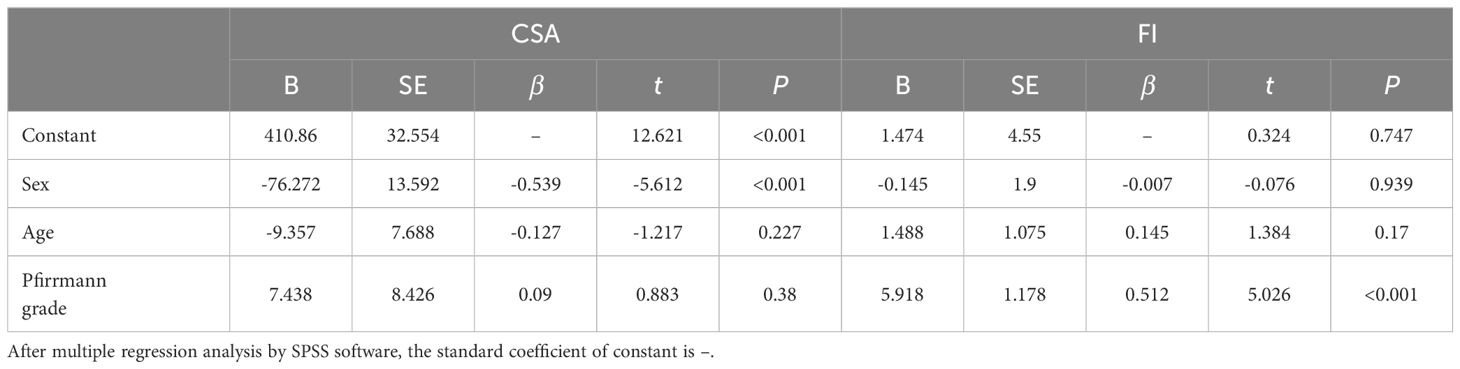
Table 7 Multiple linear regression analysis of independent influencing factors of MF+SCer CSA and FI in cervical paravertebral muscles.
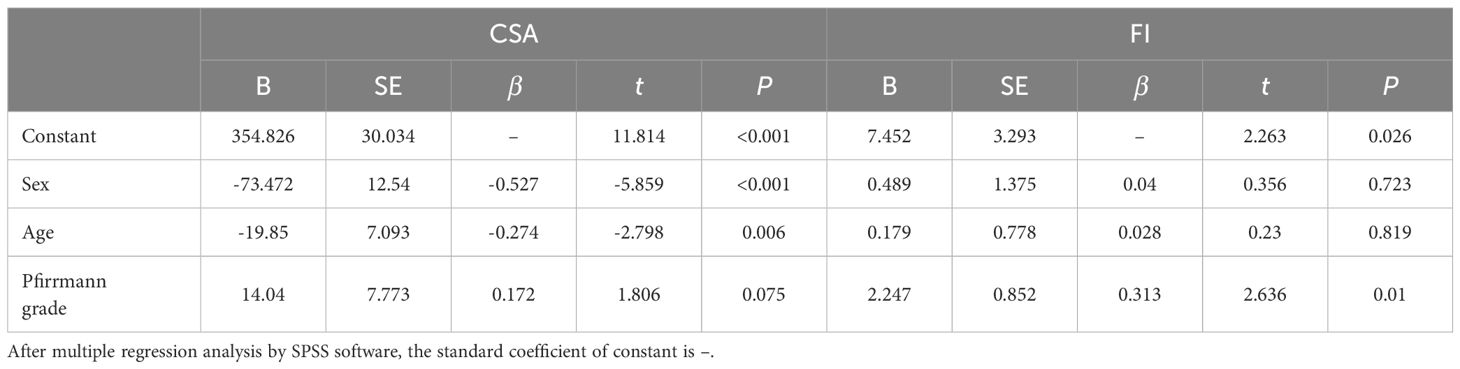
Table 8 Multiple linear regression analysis of independent influencing factors of CSA and FI in cervical paravertebral muscles.
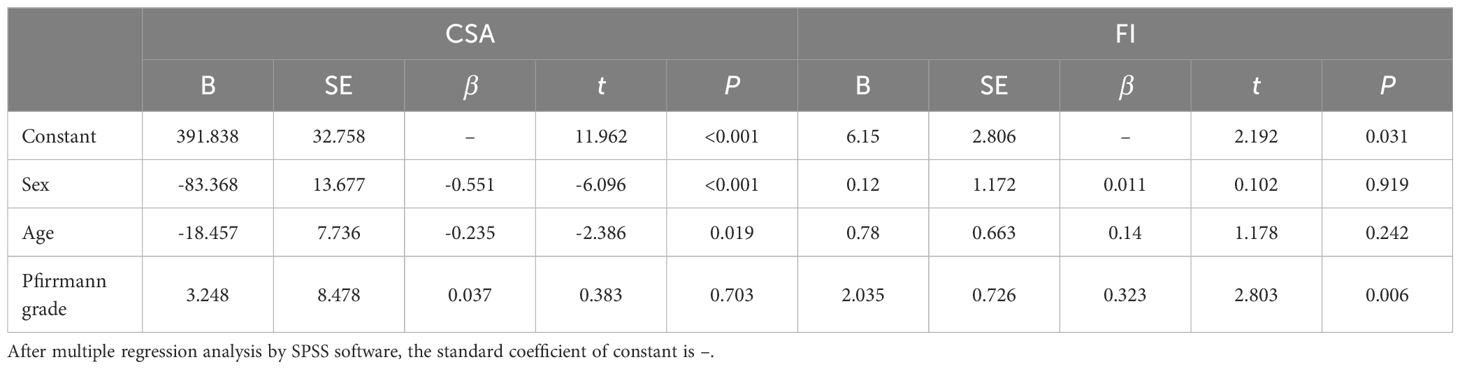
Table 9 Multivariate linear regression analysis of independent influencing factors of SPL CSA and FI in cervical paravertebral muscles.
Cervical hypermobility and overload is an important factor causing cervical spine degeneration (15–17). Teraguchi et al. (18) surveyed 975 participants aged 21 - 97 years and found that the highest prevalence of disc degeneration was at the C5–6 level, 51.5% in males and 46% in females. Therefore, in this study, C5–6 segment with the most obvious and representative cervical degeneration was selected for the study of intervertebral disc degeneration. At present, a large number of studies have confirmed that the number of muscle fibers in muscle decreases gradually with the increase of age, and muscle fiber degeneration occurs gradually, resulting in muscle atrophy and mass decline (19). A 10-year MRI study of cervical posterior extensor CSA in asymptomatic subjects showed a gradual increase in muscle CSA in subjects aged 10 to 30 years and a gradual decrease in muscle CSA in subjects aged 40 years and older (11). Therefore, the study controlled the age of the population to be included before the reduction of muscle CSA, i.e., 30 years. Valera-Calero et al. (20) analyzed cervical extensor CSA in healthy subjects using panoramic ultrasound and found that males had greater cervical extensor CSA than females. Sasaki et al. (21) reported that CSA in men was greater than that in women, while FI in paravertebral muscles in women was higher than that in men. The results of our study showed that at C5–6 level, CSA of paracervical muscles in male patients was significantly greater than that in female patients. This result is consistent with the study described above.
At present, the evaluation of paravertebral muscle degeneration is divided into quantitative evaluation and visual semi-quantitative evaluation (9, 10). The most widely used semi-quantitative assessment is the Goutallier grading system (22, 23). However, visual semi-quantitative assessment methods are affected by inter-observer differences, which will affect the results of analysis to some extent. The mDIXON-Quant sequence is a 3-dimensional Fast Field Echo (3D-FFE) sequence that uses multiple acquired echoes to generate water, fat, in-phase, and inverted images synthesized from water-fat images (24–26). Because there is almost no limit on echo time, mDIXON-Quant has the advantage of being more efficient and accurate than other MR fat quantification techniques. However, only a few studies have reported quantitative measurements of paravertebral muscle fat based on the mDIXON-Quant sequence. Zhang et al. (27) evaluated the reliability of measuring fat content in lumbar bone marrow and paravertebral muscle using mDIXON-Quant sequence, and found that mDIXON-Quant imaging has high reliability in measuring fat content in lumbar bone marrow and paravertebral muscle, which is suitable for clinical use. However, quantitative measurements of fat content in paravertebral muscles using the mDIXON-Quant sequence have not been reported. In addition, in order to ensure the reliability of the results, we used ICC to evaluate the consistency of the measurements within and between observers. The correlation coefficients were all>0.75, indicating that the measurement results were consistent and reproducible.
The relationship between muscle atrophy and fatty infiltration due to degeneration of the cervical paracervical muscles and the degree of cervical disc degeneration is unclear. There was no statistical difference between the degree of disc degeneration and CSA (P>0.05), or between the degree of disc degeneration and CSA (P>0.05). The possible reason is that muscle morphology and CSA are affected by many factors, and when CSA does not change, FI of neck muscle has increased, and CSA of paravertebral muscle is not correlated with FI (28). FI was more pronounced in MF and erector spinae in patients with severe disc degeneration (29). Cloney et al. (30) found that FI of cervical MF was associated with decreased sensation and function in CSM patients. Meanwhile, extensive FI was observed in the cervical extensors of patients with chronic neck pain-related diseases, but the maximum FI was observed in the deep neck extensors such as MF and SCer compared with the superficial tissues (such as SCap, SPL) (31). Our study found that there was a difference in FI of paracervical muscles among patients with disc degeneration degree, and multiple regression analysis showed that disc degeneration degree was an independent factor affecting FI of paracervical muscles, indicating that it was not affected by other factors. Further Spearman correlation analysis showed that the degree of disc degeneration was moderately or strongly correlated with FI, and the degree of disc degeneration at C5–6 was most closely correlated with FI of deep cervical extensor (MF+SCer), showing a strong correlation. Among the cervical paravertebral muscles, the deep cervical extensor group, dominated by MF and SCer, attaches directly to the cervical spine and is considered to play a key role in maintaining stability and biomechanics, and these muscles may be sensitive to changes in neck function and pain (31). It may be related to the distribution, morphology and density of muscle spindles of different muscles in the neck, which is one of the factors for proprioceptive regulation of skeletal muscles (32). It has been found that the relative CSA of the most superficial extensors of the neck (SCap, SPL) is not reduced compared to the rectus capitis posterior minor, because muscles with high muscle spindle density (e.g., rectus capitis posterior minor and rectus capitis posterior major) may be more sensitive than those with low spindle density (SCap, SPL) (33). Our results show that the more severe the disc degeneration, the more likely the fat infiltration of the deep neck extensors (MF+SCer) is, similar to the results previously reported in patients with low back pain, and muscle degeneration is more common in lumbar MF.
There are a few limitations of the present study. Our study only selected C5–6, the most common cervical disc degeneration, and did not include more segments (such as C4–5 and C6–7) for comparative study. The Pfirrmann classification system for evaluating disc degeneration in this study is not perfect, and other signs of disc degeneration such as spinal cord compression, disc herniation, intervertebral foraminal stenosis, Schmermer’s node, etc. cannot be considered. It is impossible to accurately identify and isolate individual muscles in the deep neck extensors due to MRI images. In the future, it is hoped that higher resolution images and more advanced MRI sequences will better identify and differentiate individual muscles in the cervical paravertebral muscle group.
There is a correlation between disc degeneration and paravertebral muscle degeneration, especially in deep neck extensors (MF and SCer). Therefore, patients with cervical disc degeneration should exercise paraspinal muscles more actively in the early stage, which is helpful to restore paraspinal muscle degeneration function and delay degeneration process.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by ethics committee of the People’s Hospital of Ningxia Hui Autonomous Region. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
QL: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. XL: Data curation, Writing – original draft, Writing – review & editing. RW: Conceptualization, Data curation, Software, Writing – review & editing. PN: Conceptualization, Methodology, Software, Writing – review & editing. LC: Conceptualization, Methodology, Software, Supervision, Writing – review & editing. LW: Conceptualization, Funding acquisition, Methodology, Supervision, Visualization, Writing – review & editing. YS: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by Science and Technology Project of the Health Planning Committee of Sichuan (2022NSFSC1528); the 1-3-5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYGD21001); Sichuan Provincial Science and Technology Department Key Projects (No. 2022YFS0016 and 2022YFS0260); the National Natural Science Foundation of China (82072386 and 82102521).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gudavalli MR, Salsbury SA, Vining RD, Long CR, Corber L, Patwardhan AG, et al. Development of an attention-touch control for manual cervical distraction: a pilot randomized clinical trial for patients with neck pain. Trials. (2015) 16:259. doi: 10.1186/s13063-015-0770-6
2. Gabel CP, Mokhtarinia HR, Melloh M. The politics of chronic LBP: can we rely on a proxy-vote? Linking multifidus intra-myo-cellular lipid (IMCL) fatty infiltration with arthrogenic muscle inhibition (AMI)-induced chronic nonspecific low back pain. Spine (Phila Pa 1976). (2021) 46:129–30. doi: 10.1097/BRS.0000000000003758
3. Hides J, Gilmore C, Stanton W, Bohlscheid E. Multifidus size and symmetry among chronic LBP and healthy asymptomatic subjects. Man Ther. (2008) 13:43–9. doi: 10.1016/j.math.2006.07.017
4. Fortin M, Gibbons LE, Videman T, Battie MC. Do variations in paraspinal muscle morphology and composition predict low back pain in men? Scand J Med Sci Sports. (2015) 25:880–7. doi: 10.1111/sms.12301
5. Wan Q, Lin C, Li X, Zeng W, Ma C. MRI assessment of paraspinal muscles in patients with acute and chronic unilateral low back pain. Br J Radiol. (2015) 88:20140546. doi: 10.1259/bjr.20140546
6. Ekin EE, Kurtul YH, Mutlu H. Age and sex-based distribution of lumbar multifidus muscle atrophy and coexistence of disc hernia: an MRI study of 2028 patients. Diagn Interv Radiol. (2016) 22:273–6. doi: 10.5152/dir
7. Tan LA, Riew KD, Traynelis VC. Cervical spine deformity-part 1: biomechanics, radiographic parameters, and classification. Neurosurgery. (2017) 81:197–203. doi: 10.1093/neuros/nyx249
8. Etame AB, Wang AC, Than KD, La Marca F, Park P. Outcomes after surgery for cervical spine deformity: review of the literature. Neurosurg Focus. (2010) 28:E14. doi: 10.3171/2010.1.FOCUS09278
9. Pinter ZW, Wagner SC, Fredericks DJ, Xiong A, Freedman BA, Elder BD, et al. Higher paraspinal muscle density effect on outcomes after anterior cervical discectomy and fusion. Global Spine J. (2021) 11:931–5. doi: 10.1177/2192568220935108
10. Pinter ZW, Wagner S, Fredericks DJ, Xiong A, Helgeson M, Currier B, et al. Cervical paraspinal muscle fatty degeneration is not associated with muscle cross-sectional area: qualitative assessment is preferable for cervical sarcopenia. Clin Orthop Relat Res. (2021) 479:726–32. doi: 10.1097/CORR.0000000000001621
11. Okada E, Matsumoto M, Ichihara D, Chiba K, Toyama Y, Fujiwara H, et al. Cross-sectional area of posterior extensor muscles of the cervical spine in asymptomatic subjects: a 10-year longitudinal magnetic resonance imaging study. Eur Spine J. (2011) 20:1567–73. doi: 10.1007/s00586-011-1774-x
12. Tang R, Tang G, Hua T, Tu Y, Ji R, Zhu J. mDIXON-Quant technique diagnostic accuracy for assessing bone mineral density in male adult population. BMC Musculoskelet Disord. (2023) 24:125. doi: 10.1186/s12891-023-06225-z
13. Wang Y, Ju Y, An Q, Lin L, Liu AL. mDIXON-Quant for differentiation of renal damage degree in patients with chronic kidney disease. Front Endocrinol (Lausanne). (2023) 14:1187042. doi: 10.3389/fendo.2023.1267914
14. Oh CH, Kim DY, Ji GY, Kim YJ, Yoon SH, Hyun D, et al. Cervical arthroplasty for moderate to severe disc degeneration: clinical and radiological assessments after a minimum follow-up of 18 months–Pfirrmann grade and cervical arthroplasty. Yonsei Med J. (2014) 55:1072–9. doi: 10.3349/ymj.2014.55.4.1072
15. Li XH, She LJ, Zhang W, Cheng XD, Fan JP. Biomechanics of extreme lateral interbody fusion with different internal fixation methods: a finite element analysis. BMC Musculoskelet Disord. (2022) 23:134. doi: 10.1186/s12891-022-05049-7
16. Satin AM, Rogers-LaVanne MP, Derman PB. Cervical disk arthroplasty and range of motion at 7 years: impact on adjacent level degeneration. Clin Spine Surg. (2023) 36:83–9. doi: 10.1097/BSD.0000000000001446
17. Godlewski B, Bebenek A, Dominiak M, Bochniak M, Cieslik P, Pawelczyk T. Adjacent segment mobility after ACDF considering fusion status at the implant insertion site. Eur Spine J. (2023) 32:1616–23. doi: 10.1007/s00586-023-07634-3
18. Teraguchi M, Yoshimura N, Hashizume H, Muraki S, Yamada H, Minamide A, et al. Prevalence and distribution of intervertebral disc degeneration over the entire spine in a population-based cohort: the Wakayama Spine Study. Osteoarthritis Cartilage. (2014) 22:104–10. doi: 10.1016/j.joca.2013.10.019
19. Snodgrass SJ, Croker C, Yerrapothu M, Shepherd S, Stanwell P, Holder C, et al. Cervical muscle volume in individuals with idiopathic neck pain compared to asymptomatic controls: A cross-sectional magnetic resonance imaging study. Musculoskelet Sci Pract. (2019) 44:102050. doi: 10.1016/j.msksp.2019.102050
20. Valera-Calero JA, Gallego-Sendarrubias G, Fernandez-de-Las-Penas C, Cleland JA, Ortega-Santiago R, Arias-Buría JL. Cross-sectional area of the cervical extensors assessed with panoramic ultrasound imaging: Preliminary data in healthy people. Musculoskelet Sci Pract. (2020) 50:102257. doi: 10.1016/j.msksp.2020.102257
21. Sasaki T, Yoshimura N, Hashizume H, Yamada H, Oka H, Matsudaira K, et al. MRI-defined paraspinal muscle morphology in Japanese population: The Wakayama Spine Study. PloS One. (2017) 12:e187765. doi: 10.1371/journal.pone.0187765
22. Mandelli F, Nuesch C, Zhang Y, Halbeisen F, Schären S, Mündermann A, et al. Assessing fatty infiltration of paraspinal muscles in patients with lumbar spinal stenosis: goutallier classification and quantitative MRI measurements. Front Neurol. (2021) 12:656487. doi: 10.3389/fneur.2021.656487
23. Duan PG, Mummaneni PV, Guinn J, Rivera J, Berven SH, Chou D. Is the Goutallier grade of multifidus fat infiltration associated with adjacent-segment degeneration after lumbar spinal fusion? J Neurosurg Spine. (2020) 34:190–5. doi: 10.3171/2020.6.SPINE20238
24. Zhu S, Tian A, Guo L, Xu H, Li X, Wang Z, et al. Investigation of diagnostic biomarkers for osteoporosis based on differentially expressed gene profile with QCT and mDixon-quant techniques. Orthop Surg. (2021) 13:2137–44. doi: 10.1111/os.13094
25. Chu C, Feng Q, Zhang H, Zhao S, Chen W, He J, et al. Evaluation of salivary gland fat fraction values in patients with primary Sjogren's syndrome by mDIXON quant imaging: Initial findings. Eur J Radiol. (2020) 123:108776. doi: 10.1016/j.ejrad.2019.108776
26. Meng X, Tian S, Ma C, Lin L, Zhang X, Wang J, et al. APTw combined with mDixon-Quant imaging to distinguish the differentiation degree of cervical squamous carcinoma. Front Oncol. (2023) 13:1105867. doi: 10.3389/fonc.2023.1105867
27. Zhang Y, Zhou Z, Wang C, Cheng X, Wang L, Duanmu Y, et al. Reliability of measuring the fat content of the lumbar vertebral marrow and paraspinal muscles using MRI mDIXON-Quant sequence. Diagn Interv Radiol. (2018) 24:302–7. doi: 10.5152/dir
28. Fortin M, Wilk N, Dobrescu O, Martel P, Santaguida C, Weber MH. Relationship between cervical muscle morphology evaluated by MRI, cervical muscle strength and functional outcomes in patients with degenerative cervical myelopathy. Musculoskelet Sci Pract. (2018) 38:1–7. doi: 10.1016/j.msksp.2018.07.003
29. Ozcan-Eksi EE, Eksi MS, Akcal MA. Severe Lumbar Intervertebral Disc Degeneration Is Associated with Modic Changes and Fatty Infiltration in the Paraspinal Muscles at all Lumbar Levels, Except for L1-L2: A Cross-Sectional Analysis of 50 Symptomatic Women and 50 Age-Matched Symptomatic Men. World Neurosurg. (2019) 122:e1069–77. doi: 10.1016/j.wneu.2018.10.229
30. Cloney M, Smith AC, Coffey T, Paliwal M, Dhaher Y, Parrish T, et al. Fatty infiltration of the cervical multifidus musculature and their clinical correlates in spondylotic myelopathy. J Clin Neurosci. (2018) 57:208–13. doi: 10.1016/j.jocn.2018.03.028
31. Abbott R, Pedler A, Sterling M, Hides J, Murphey T, Hoggarth M, et al. The geography of fatty infiltrates within the cervical multifidus and semispinalis cervicis in individuals with chronic whiplash-associated disorders. J Orthop Sports Phys Ther. (2015) 45:281–8. doi: 10.2519/jospt.2015.5719
32. Boyd-Clark LC, Briggs CA, Galea MP. Muscle spindle distribution, morphology, and density in longus colli and multifidus muscles of the cervical spine. Spine (Phila Pa 1976). (2002) 27:694–701. doi: 10.1097/00007632-200204010-00005
Keywords: paraspinal muscle degeneration, intervertebral disc degeneration, mDIXON-Quant, fat infiltration, cervical
Citation: Li Q, Long X, Wang R, Niu P, Cai L, Wang L and Song Y (2024) Correlation between degeneration of cervical intervertebral disc and degeneration of paravertebral muscle. Front. Endocrinol. 15:1391970. doi: 10.3389/fendo.2024.1391970
Received: 26 February 2024; Accepted: 31 May 2024;
Published: 19 June 2024.
Edited by:
Jiajia Xu, Southern Medical University, ChinaReviewed by:
Fulvio Tartara, University Hospital of Parma, ItalyCopyright © 2024 Li, Long, Wang, Niu, Cai, Wang and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lijun Cai, bGlqdW4tY2FpMTgwMUAxNjMuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.