 YongSheng Cao1
YongSheng Cao1 Ying Liu
Ying Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 19 July 2024
Sec. Renal Endocrinology
Volume 15 - 2024 | https://doi.org/10.3389/fendo.2024.1387993
This article is part of the Research TopicNovel Pathophysiologic Mechanisms and Reno-protective Pharmacotherapies in Diabetic Kidney DiseaseView all 9 articles
Objective: This study aimed to evaluate the efficacy and safety of polyethylene glycol loxenatide (PEG-Loxe) compared to those of dapagliflozin in patients with mild-to-moderate diabetic kidney disease (DKD), a prevalent microvascular complication of type 2 diabetes mellitus (T2DM). The study is set against the backdrop of increasing global diabetes incidence and the need for effective DKD management.
Methods: This study constituted a single-center, randomized, open-label, clinical trial. The trial included patients with mild-to-moderate DKD and suboptimal glycemic control. Eligible participants were randomly allocated to one of the two groups for treatment with either PEG-Loxe or dapagliflozin. The primary endpoint was the change in UACR from baseline at 24 weeks.
Results: Overall, 106 patients were randomized and 80 patients completed the study. Following 24 weeks of treatment, the PEG-Loxe group exhibited a mean percent change in baseline UACR of −29.3% (95% confidence interval [CI]: −34.8, −23.7), compared to that of −31.8% in the dapagliflozin group (95% CI: −34.8, −23.7). Both PEG-Loxe and dapagliflozin showed similar efficacy in reducing UACR, with no significant difference between the groups (p = 0.336). The HbA1c levels decreased by −1.30% (95% CI: −1.43, −1.18) in the PEG-Loxe group and by −1.29% (95% CI: −1.42, −1.17) in the dapagliflozin group (p = 0.905). The TG levels decreased by −0.56 mmol/L (95% CI: −0.71, −0.42) in the PEG-Loxe group and −0.33 mmol/L (95% CI: −0.48, −0.19) in the dapagliflozin group (p = 0.023). Differences in TC, HDL-C, LDL-C, SBP, and DBP levels between the groups were not statistically significant (all p > 0.05). Safety profiles were consistent with previous findings, with gastrointestinal adverse events being more common in the PEG-Loxe group.
Conclusions: PEG-Loxe is as effective as dapagliflozin in improving urine protein levels in patients with mild-to-moderate DKD and offers superior benefits in improving lipid profiles. These findings support the use of PEG-Loxe in DKD management, contributing to evidence-based treatment options.
Clinical Trial Registration: www.chictr.org.cn, identifier ChiCTR2300070919.
In recent years, the incidence of diabetes has steadily risen, affecting 540 million adults globally, with more than 90% diagnosed with type 2 diabetes mellitus (T2DM) (1). Diabetes mellitus results in a range of macrovascular and microvascular complications, posing significant health risks (2). Diabetic kidney disease (DKD) represents one such microvascular complication of diabetes mellitus (3). Approximately 20%–40% of individuals with diabetes develop DKD (4).
DKD constitutes a chronic kidney disease characterized by a complex pathogenesis (5). Clinically, it is marked by persistent albuminuria and/or a gradual decline in the glomerular filtration rate (GFR), eventually leading to end-stage renal disease (ESRD) (6). Besides being a primary cause of ESRD, DKD significantly elevates the risk of cardiovascular events and all-cause mortality in individuals with T2DM (7).
Recently, advancements in drug therapy for DKD have emerged from research into the pathogenic mechanisms of diabetes mellitus, its complications, and the introduction of new drug classes. One notable drug is GLP-1RA, which induces hypoglycemic effects by boosting insulin secretion and suppressing glucagon secretion (8, 9), while also ameliorating lipid and blood pressure levels (10, 11). Research indicates that this drug class markedly lowers the risk of kidney-related composite endpoints, such as progression to macroalbuminuria, doubling of serum creatinine, ESRD, and kidney disease-related mortality, compared to those by placebo (12, 13).
Polyethylene glycol loxenatide (PEG-Loxe), approved in 2019, is a once-weekly GLP-1RA formulation derived from amino acid and polyethylene glycol (PEG) modifications of exendin-4 (14). A prior phase 3 study reported that PEG-Loxe therapy, either alone or combined with metformin for 24 weeks in T2DM patients, showed promising efficacy and safety, evidenced by reductions of 1.14%–1.34% in hemoglobin A1c (HbA1c) levels and 10.3%–25.0% in gastrointestinal adverse event (AE) rates (15, 16). Additionally, a randomized-controlled trial demonstrated that 16 weeks of PEG-Loxe treatment led to an average weight loss of 7.52 kg in T2DM patients that were also overweight or obese (17). However, the efficacy and safety of PEG-Loxe in DKD patients remain unreported and unknown. Thus, this study aimed to assess the efficacy and safety of PEG-Loxe in patients with mild-to-moderate DKD.
This study constituted a single-center, randomized, open-label, clinical trial. Approval for the study was granted by the Institutional Review Board of Sunshine Union Hospital (IRB no.: YGRHLLKY-0005). Prior to inclusion in the study, all patients provided informed consent. Conducted in alignment with the Declaration of Helsinki and Good Clinical Practice, the study was registered with the Chinese Clinical Trial Registry (ChiCTR) (no.: ChiCTR2300070919).
The inclusion criteria included the following:
a. Written informed consent.
b. Age ≥ 18 years with a clinical diagnosis of T2DM.
c. HbA1c between 7.0% and 10.0%.
d. estimated glomerular filtration rate (eGFR) ranging from 30 to 90 mL/min/1.73 m2.
e. Urinary albumin-to-creatinine ratio (UACR) >30 mg/g and ≤5,000 mg/g.
f. Agreement by women to use contraception during the intervention.
The exclusion criteria included the following:
a. History of diabetic ketoacidosis or type 1 diabetes mellitus.
b. Severe cardiovascular, cerebrovascular, or hepatic disease.
c. Renal transplant recipients or patients on dialysis therapy.
d. Allergy or intolerance to GLP-1RA.
e. Use of GLP-1RA or SGLT2 inhibitors within 12 weeks before study enrollment.
f. Severe gastrointestinal disorders.
g. History of pancreatitis.
Eligible participants were randomly allocated to one of the two groups for treatment with either PEG-Loxe or dapagliflozin. The randomization was conducted by a statistician using a computer-generated random number sequence, assigning patients to the groups in a 1:1 ratio. During data analysis, statisticians were blinded to the group assignments of the participants.
Each patient’s existing treatment regimen was supplemented with either PEG-Loxe or dapagliflozin. PEG-Loxe was administered subcutaneously once weekly. The treatment adhered to a fixed-dose escalation schedule, starting with an initial dose of 0.1 mg for 4 weeks, followed by a maintenance dose of 0.2 mg until study completion. Likewise, dapagliflozin was initiated at 5 mg for 2 weeks, followed by a maintenance dose of 10 mg until the study’s conclusion.
Patients were subjected to follow-up examinations at 12 and 24 weeks, encompassing physical examinations and data collection. Demographic data, vital signs, and laboratory results were systematically recorded. Systolic and diastolic blood pressure (SBP and DBP, respectively) measurements were taken using a sphygmomanometer (HBP-1300, OMRON, Dalian, China). Morning fasting blood samples were collected and analyzed in the Laboratory Department of Sunshine Union Hospital. Laboratory examination encompassed UACR, 24-h urine protein, eGFR, HbA1c, fasting plasma glucose (FPG), and a blood lipid panel. Furthermore, all AEs were recorded.
The primary endpoint focused on the change in UACR from baseline till after 24 weeks of treatment. Secondary endpoints encompassed 24-h urine protein, eGFR, HbA1c, FPG, body weight, total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), SBP, and DBP after 24 weeks of treatment.
The primary outcome assessed was the non-inferiority of PEG-Loxe compared that of to dapagliflozin in terms of UACR change from baseline. A sample size of 64 offered an 80% power to affirm the non-inferiority of UACR change (35% margin), presuming a geometric mean coefficient of variation of 66% (18) and a bilateral α level of 0.05. The withdrawal rate was established at 20%, resulting in a total sample size of 80.
To evaluate the primary endpoint, a mixed model for repeated measures (MMRM) was employed to compare changes in log-transformed UACR (log UACR) between the two groups. In this model, treatment group, time, and their interaction were considered fixed effects, with baseline log UACR as a covariate. MMRM analysis was also applied to 24-h urine protein, eGFR, HbA1c, FPG, TC, TG, LDL-C, HDL-C, SBP, and DBP. Patients lacking UACR data at 6 months were excluded from the analysis due to the inability to calculate change values. Differences yielding a p-value < 0.05 were deemed statistically significant. Statistical analyses were conducted using SAS v. 9.4 software.
Between April 2023 and July 2023, 106 participants were evaluated for eligibility, with 88 ultimately being included in the study. Throughout the study, three participants withdrew consent, two exited due to AEs, and three were lost to follow-up, culminating in 80 participants completing the study (Figure 1). Table 1 displays the baseline characteristics of both groups. Except for those in LDL-C, there were no statistically significant differences in any parameters between the groups.
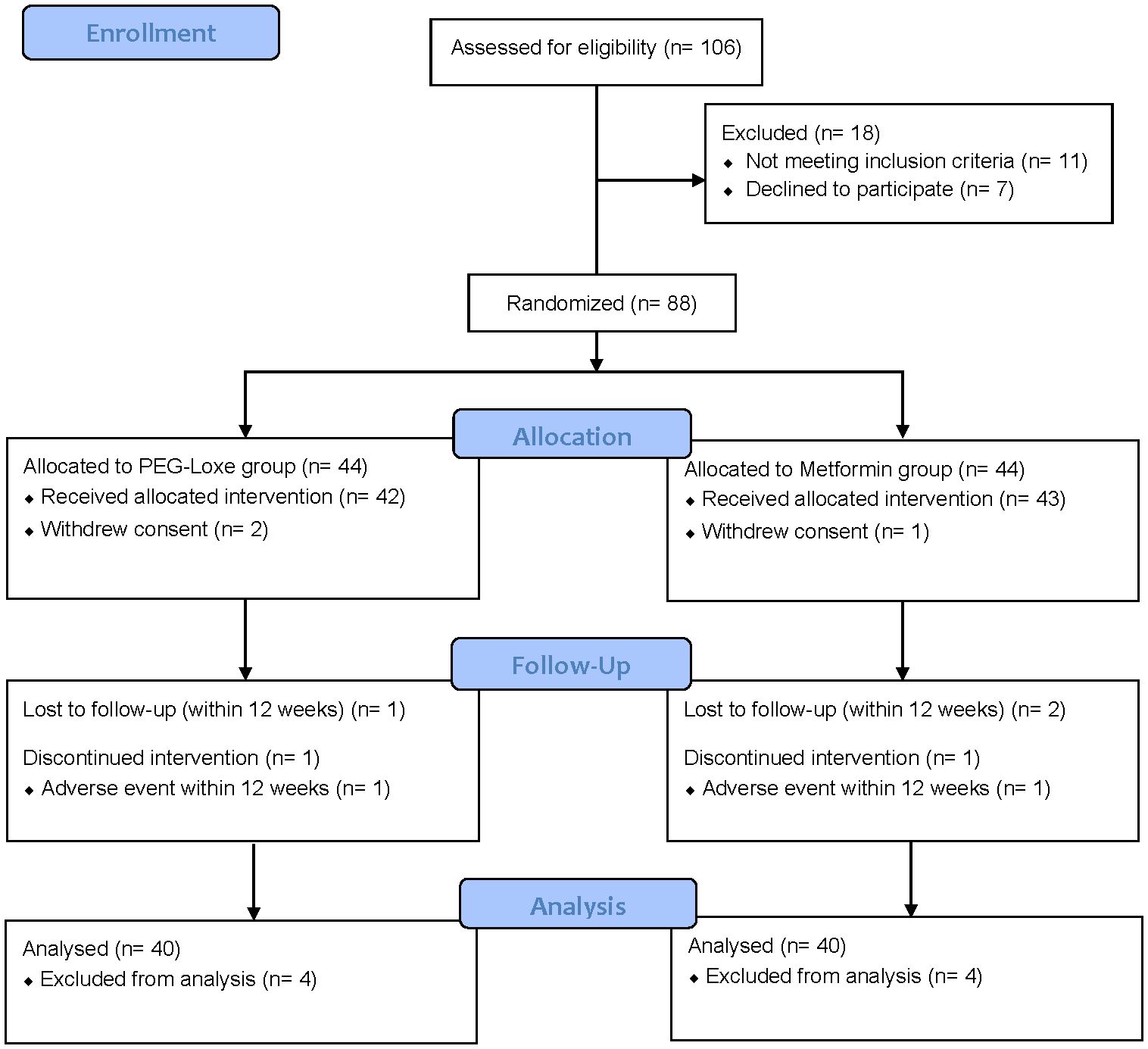
Figure 1 Consort flow diagram.
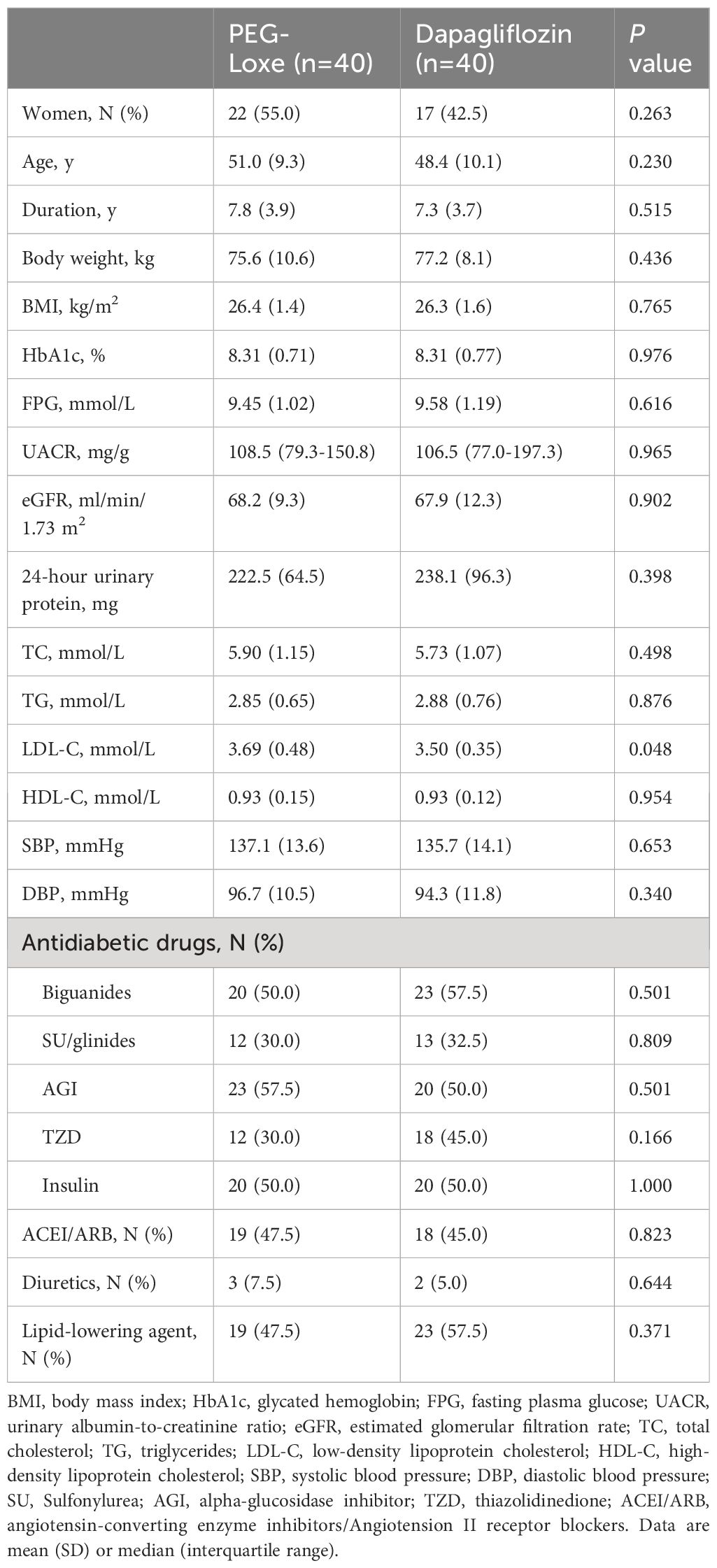
Table 1 Baseline characteristics.
Initially, the median UACR stood at 108.5 mg/g in the PEG-Loxe group (interquartile range [IQR]: 79.3–150.8) and 106.5 mg/g in the dapagliflozin group (IQR: 77.0–197.3). Following 24 weeks of treatment, the PEG-Loxe group exhibited a mean percent change in baseline UACR of −29.3% (95% confidence interval [CI]: −34.8, −23.7), compared to that of −31.8% in the dapagliflozin group (95% CI: −34.8, −23.7). The intergroup difference was 2.6% (95% CI: −5.3, −10.4), a non-statistically significant variation (p = 0.336). After 24 weeks of treatment, the change in eGFR was 6.3 mL/min/1.73 m2 (4.4, 8.2) in the PEG-Loxe group and 7.2 mL/min/1.73 m2 (5.3, 9.1) in the dapagliflozin group. The difference between the groups was −0.9 mL/min/1.73 m2 (−3.6, 1.8), which was not statistically significant (p = 0.504). The intergroup difference in 24-h urine protein was −0.6 mg (−19.2, 18.1; p = 0.953) (Table 2).
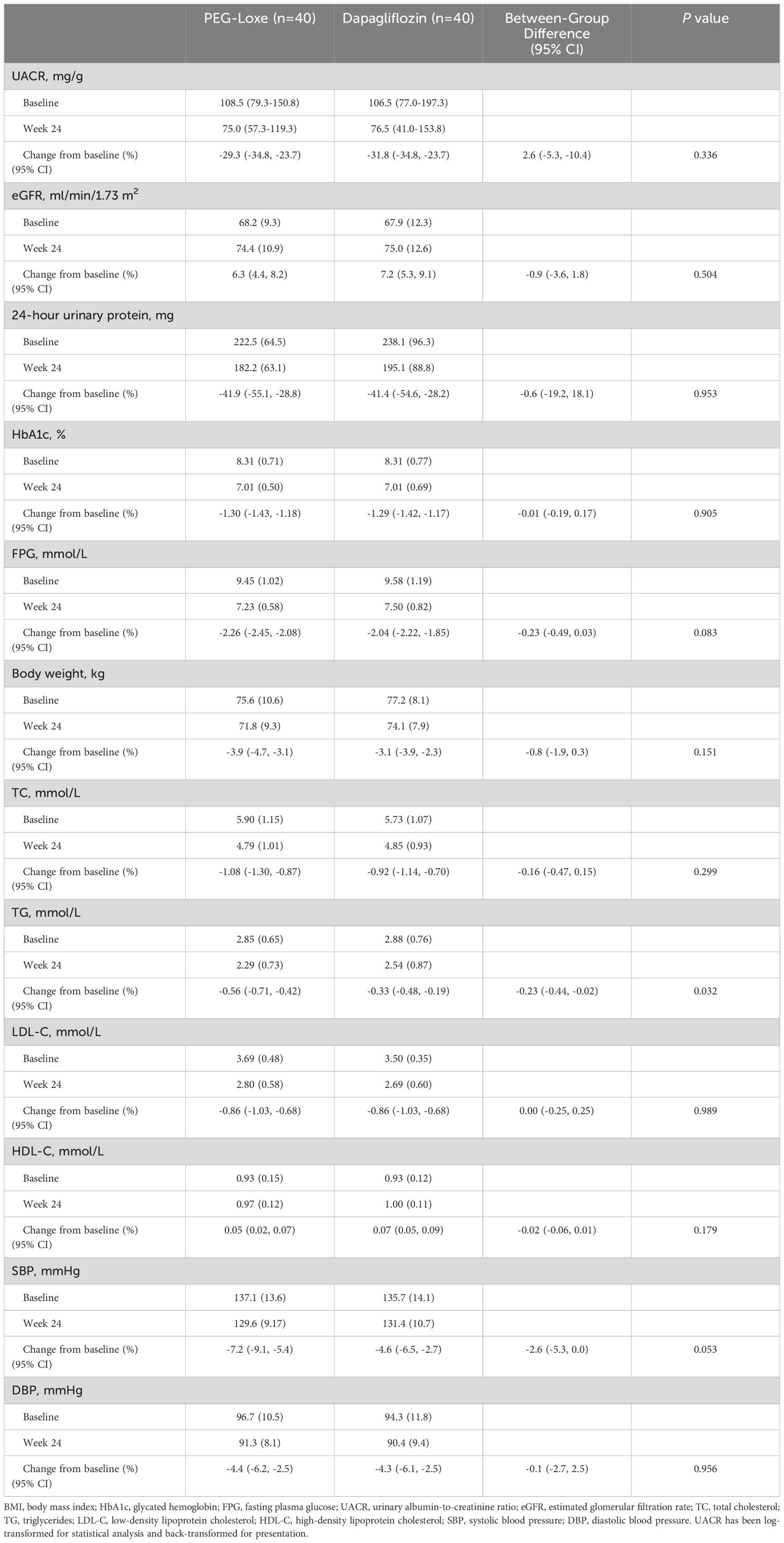
Table 2 Primary and secondary endpoints at week 24.
Following 24 weeks of treatment, HbA1c levels decreased by −1.30% (−1.43, −1.18) in the PEG-Loxe group and by −1.29% (−1.42, −1.17) in the dapagliflozin group (p = 0.905), while FPG levels decreased by −2.26 mmol/L (−2.45, −2.08) in the PEG-Loxe group and −2.04 mmol/L (−2.22, −1.85) in the dapagliflozin group (p = 0.083). The weight change difference between the PEG-Loxe and dapagliflozin groups was −0.8 kg (−1.9, 0.3), lacking statistical significance (p = 0.151) (Table 2).
Regarding blood lipids and blood pressure, TG levels decreased by −0.56 mmol/L (−0.71, −0.42) in the PEG-Loxe group and −0.33 mmol/L (−0.48, −0.19) in the dapagliflozin group. The intergroup difference was −0.23 mmol/L (−0.44, −0.02) (p = 0.023). Differences in TC, HDL-C, LDL-C, SBP, and DBP levels between the groups were not statistically significant (all p > 0.05) (Table 2).Table 3 presents efficacy indicators at 12 weeks of treatment, mirroring those observed at 24 weeks. In terms of safety, the drug was generally well-tolerated, with AEs aligning with expectations. Gastrointestinal AEs occurred more frequently with PEG-Loxe, while urinary tract infections were more prevalent with dapagliflozin (Table 4).
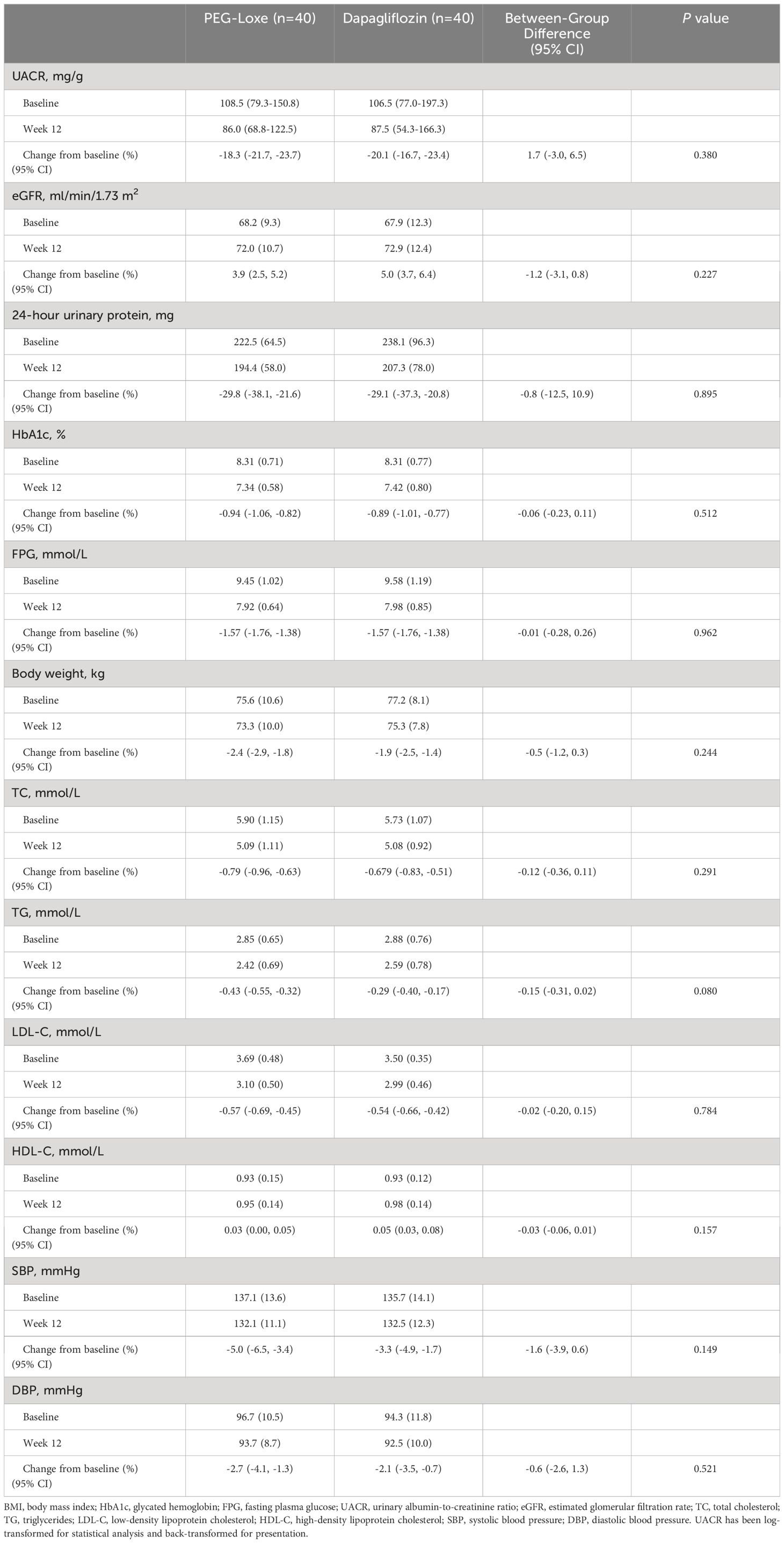
Table 3 Efficacy endpoints at week 12.
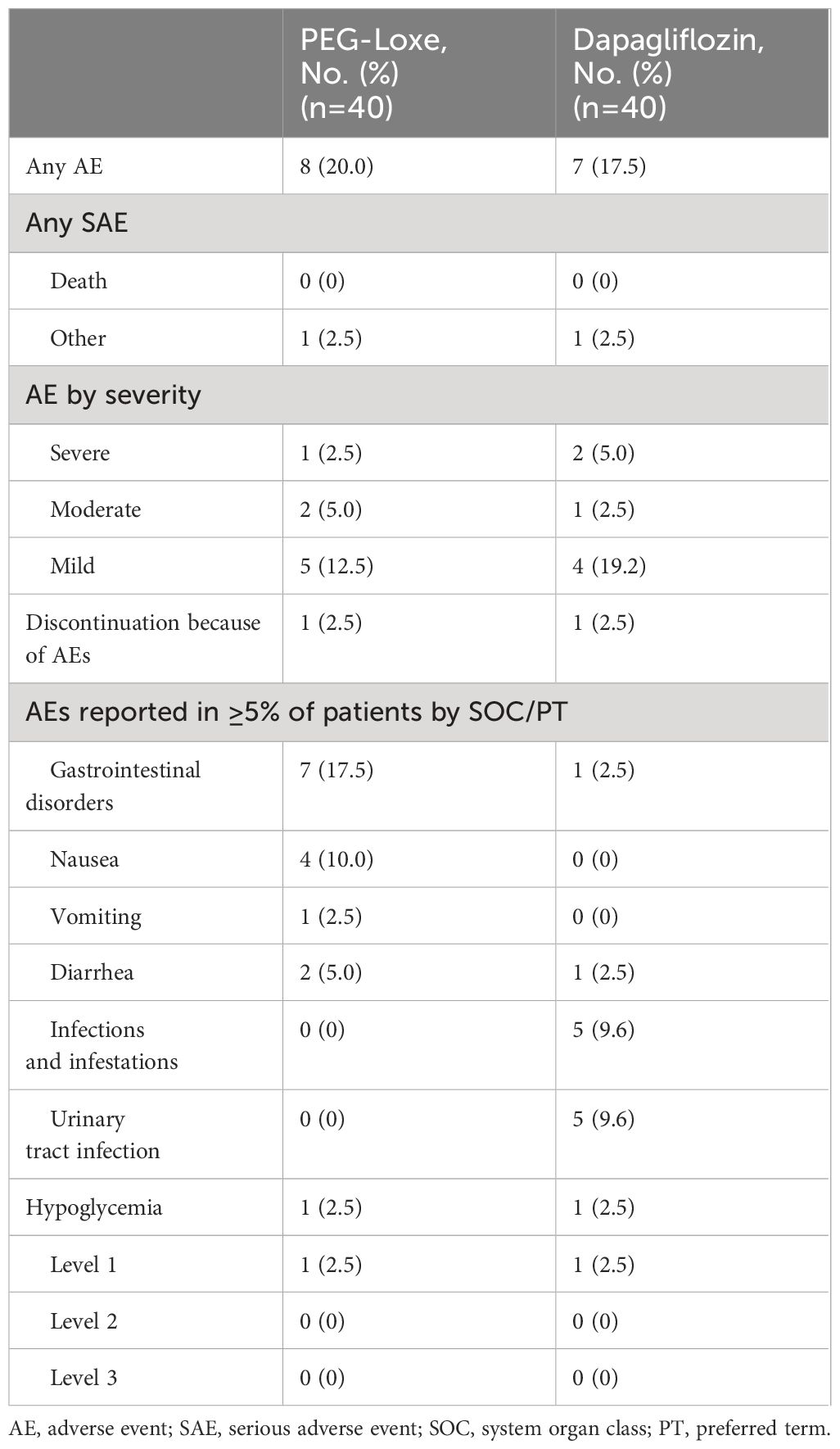
Table 4 Summary of safety.
To the best of our knowledge, this study presents the first direct comparison of PEG-Loxe and dapagliflozin in patients with mild-to-moderate DKD. This single-center, randomized, open-label clinical trial demonstrated that PEG-Loxe’s efficacy in reducing proteinuria was comparable to that of dapagliflozin in patients with mild-to-moderate DKD. Furthermore, PEG-Loxe also offered the advantage of enhancing blood lipid levels.
GLP-1 RA, a novel class of glucose-lowering agents, has demonstrated cardiorenal protection in T2DM patients in trials focusing on cardiovascular outcomes (19–21). Clinical guidelines endorse GLP-1 RA as the primary glucose-lowering agents for treating T2DM patients with concurrent atherosclerotic cardiovascular disease and as a secondary option for DKD treatment (1, 22). A previous study reported that 24 weeks of liraglutide treatment led to a 13.2% reduction in UACR in T2DM patients with a baseline UACR of 24.8 mg/g (23). For T2DM patients with concurrent moderate-to-severe chronic kidney disease, 26 weeks of dulaglutide treatment resulted in a 27.7% decrease in UACR (24). In T2DM patients with a baseline UACR of 135 mg/g, a 26-week semaglutide treatment regimen led to a 14% reduction in UACR (25). In this study, the baseline UACR in the PEG-Loxe group was 108.5 mg/g, and it decreased by 29.3% after 6 months of treatment, indicating renoprotective effects of PEG-Loxe akin to other GLP-1 RAs.
SGLT2 inhibitors (SGLT2i), such as dapagliflozin, are universally recommended as first-line therapeutic agents in DKD treatment, supported by large-scale studies demonstrating cardiac and renal benefits (26–29). A meta-analysis encompassing 16 clinical studies with T2DM patients having a baseline eGFR of 30–90 mL/min/1.73 m2 revealed that over 2 years, SGLT2i reduced UACR by 17%–33%, while GLP-1 RA achieved a 19%–22% reduction. Overall, the effect of SGLT2i in reducing urine protein levels was comparable to or marginally more potent than that of GLP-1 RA (30). This study also involved patients with a baseline eGFR of 30–90 mL/min/1.73 m2, where 6 months of treatment with dapagliflozin and PEG-Loxe led to UACR reductions of 31.8% and 29.3%, respectively, aligning with previous findings that PEG-Loxe and dapagliflozin have comparable efficacy in improving urine protein levels. This study suggests that PEG-Loxe may be considered for patients with mild-to-moderate DKD if SGLT2i is insufficient to meet glycemic targets or not tolerated.
Regarding glycemic control, a meta-analysis of 315 trials (involving 35,022 patients) revealed no significant disparity in the efficacy of GLP-1 RA and SGLT2i in reducing HbA1c levels; however, GLP-1 RA was more effective in lowering fasting glucose levels than SGLT2i (31). GLP-1 RA regulates blood glucose levels via various mechanisms, such as by enhancing insulin secretion and inhibiting glucagon secretion in a glucose concentration-dependent manner, alongside delaying gastric emptying and diminishing food intake through central appetite suppression (32, 33). This multifaceted approach might account for GLP-1 RA’s superior glycemic control compared to that by SGLT2i’s singular glucose-lowering mechanism SGLT2i. While the reduction in FPG levels in the PEG-Loxe group was not significantly different from that in the SGLT2i group in this study, PEG-Loxe seemed to marginally outperform dapagliflozin in lowering FPG.
Both GLP-1 RA and SGLT2i are effective in improving lipid levels (34, 35). A meta-analysis comprising 25 studies with 1,595 non-alcoholic fatty liver disease patients showed that GLP-1RA reduced TG levels more effectively than SGLT2i; however, the effect on TC, HDL-C, and LDL-C levels was similar for both (36). The current study yielded similar findings in patients with mild-to-moderate DKD. Compared to that by dapagliflozin, PEG-Loxe exhibited a more pronounced reduction in TG, with no significant differences in TC, HDL-C, and LDL-C levels between the groups. This finding indicates that PEG-Loxe surpasses dapagliflozin in improving lipid levels in patients with mild-to-moderate DKD.
Prior to this study, the safety of PEG-Loxe in treating patients with mild-to-moderate DKD was not reported. In this study, the AEs in the PEG-Loxe group were mainly gastrointestinal, with no unexpected AEs being noted. This observation aligns with previous safety outcomes observed in T2DM patients and those with T2DM that are also overweight or obese (16, 17), suggesting that PEG-Loxe can be safely used to treat patients with mild-to-moderate DKD.
The study has the following limitations. First, this study assessed only the short-term efficacy results over 24 weeks, without assessing long-term efficacy. Second, the sample size was small, which necessitates validation of the findings with larger cohorts in future studies. Third, the single-center, open-label design of the study could have potentially introduced reporting bias.
In conclusion, the findings of this randomized clinical trial demonstrated that the efficacy of PEG-Loxe in reducing urine protein in mild-to-moderate DKD patients was akin to that of dapagliflozin, with the added benefit of improving lipid levels. These findings offer significant evidence-based research for the use of PEG-Loxe in DKD patients.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Institutional Review Board of Sunshine Union Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
YC: Writing – original draft, Writing – review & editing. SC: Data curation, Writing – original draft, Writing – review & editing. JGZ: Data curation, Writing – original draft, Writing – review & editing. JQZ: Data curation, Writing – original draft, Writing – review & editing. YZ: Data curation, Writing – original draft, Writing – review & editing. YL: Methodology, Project administration, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors declare that this study received funding from Jiangsu Hansoh Pharmaceutical Group Co., Ltd. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
The authors thank Yale Duan for assistance with statistical analyses.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. (2022) 183:109119. doi: 10.1016/j.diabres.2021.109119
2. Zakir M, Ahuja N, Surksha MA, Sachdev R, Kalariya Y, Nasir M, et al. Cardiovascular complications of diabetes: from microvascular to macrovascular pathways. Cureus. (2023) 15:e45835. doi: 10.7759/cureus.45835
3. Mishriky BM, Cummings DM, Powell JR. Diabetes-related microvascular complications - A practical approach. Prim Care. (2022) 49:239–54. doi: 10.1016/j.pop.2021.11.008
4. Society CD. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Diabetes Mellitus. (2021) 13:315–409.
5. Jung CY, Yoo TH. Pathophysiologic mechanisms and potential biomarkers in diabetic kidney disease. Diabetes Metab J. (2022) 46:181–97. doi: 10.4093/dmj.2021.0329
6. Ruiz-Ortega M, Rodrigues-Diez RR, Lavoz C, Rayego-Mateos S. Special issue "Diabetic nephropathy: diagnosis, prevention and treatment". J Clin Med. (2020) 9:813. doi: 10.3390/jcm9030813
7. Chen S, Chen L, Jiang H. Prognosis and risk factors of chronic kidney disease progression in patients with diabetic kidney disease and non-diabetic kidney disease: a prospective cohort CKD-ROUTE study. Ren Fail. (2022) 44:1309–18. doi: 10.1080/0886022X.2022.2106872
8. Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. (2021) 46:101102. doi: 10.1016/j.molmet.2020.101102
9. Andreasen CR, Andersen A, Knop FK, Vilsboll T. Understanding the place for GLP-1RA therapy: Translating guidelines for treatment of type 2 diabetes into everyday clinical practice and patient selection. Diabetes Obes Metab. (2021) 23:40–52. doi: 10.1111/dom.14500
10. Zhao X, Wang M, Wen Z, Lu Z, Cui L, Fu C, et al. GLP-1 receptor agonists: beyond their pancreatic effects. Front Endocrinol (Lausanne). (2021) 12:721135. doi: 10.3389/fendo.2021.721135
11. Heuvelman VD, Van Raalte DH, Smits MM. Cardiovascular effects of glucagon-like peptide 1 receptor agonists: from mechanistic studies in humans to clinical outcomes. Cardiovasc Res. (2020) 116:916–30. doi: 10.1093/cvr/cvz323
12. Kristensen SL, Rorth R, Jhund PS, Docherty KF, Sattar N, Preiss D, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. (2019) 7:776–85. doi: 10.1016/S2213-8587(19)30249-9
13. Gorriz JL, Soler MJ, Navarro-Gonzalez JF, Garcia-Carro C, PuChades MJ, D'Marco L, et al. GLP-1 receptor agonists and diabetic kidney disease: A call of attention to nephrologists. J Clin Med. (2020) 9:947. doi: 10.3390/jcm9040947
14. Wang J, Huang J, Li W, Tang S, Sun J, Zhang X, et al. Polyethylene glycol loxenatide (PEX168) in subjects with renal impairment: A pharmacokinetic study. Br J Clin Pharmacol. (2019) 85:2714–20. doi: 10.1111/bcp.14091
15. Shuai Y, Yang G, Zhang Q, Li W, Luo Y, Ma J, et al. Efficacy and safety of polyethylene glycol loxenatide monotherapy in type 2 diabetes patients: A multicentre, randomized, double-blind, placebo-controlled phase 3a clinical trial. Diabetes Obes Metab. (2021) 23:116–24. doi: 10.1111/dom.14198
16. Gao F, Lv X, Mo Z, Ma J, Zhang Q, Yang G, et al. Efficacy and safety of polyethylene glycol loxenatide as add-on to metformin in patients with type 2 diabetes: A multicentre, randomized, double-blind, placebo-controlled, phase 3b trial. Diabetes Obes Metab. (2020) 22:2375–83. doi: 10.1111/dom.14163
17. Cai H, Chen Q, Duan Y, Zhao Y, Zhang X. Short-term effect of polyethylene glycol loxenatide on weight loss in overweight or obese patients with type 2 diabetes: An open-label, parallel-arm, randomized, metformin-controlled trial. Front Endocrinol (Lausanne). (2023) 14:1106868. doi: 10.3389/fendo.2023.1106868
18. van Ruiten CC, van der Aart-van der Beek AB, IJzerman RG, Nieuwdorp M, Hoogenberg K, van Raalte DH, et al. Effect of exenatide twice daily and dapagliflozin, alone and in combination, on markers of kidney function in obese patients with type 2 diabetes: A prespecified secondary analysis of a randomized controlled clinical trial. Diabetes Obes Metab. (2021) 23:1851–8. doi: 10.1111/dom.14410
19. Parab P, Chaudhary P, Mukhtar S, Moradi A, Kodali A, Okoye C, et al. Role of glucagon-like peptide-1 (GLP-1) receptor agonists in cardiovascular risk management in patients with type 2 diabetes mellitus: A systematic review. Cureus. (2023) 15:e45487. doi: 10.7759/cureus.45487
20. Pedrosa MR, Franco DR, Gieremek HW, Vidal CM, Bronzeri F, de Cassia Rocha A, et al. GLP-1 agonist to treat obesity and prevent cardiovascular disease: what have we achieved so far? Curr Atheroscler Rep. (2022) 24:867–84. doi: 10.1007/s11883-022-01062-2
21. Kutz A, Kim DH, Wexler DJ, Liu J, Schneeweiss S, Glynn RJ, et al. Comparative cardiovascular effectiveness and safety of SGLT-2 inhibitors, GLP-1 receptor agonists, and DPP-4 inhibitors according to frailty in type 2 diabetes. Diabetes Care. (2023) 46:2004–14. doi: 10.2337/dc23-0671
22. ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 9. Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2023. Diabetes Care. (2023) 46:S140–S57. doi: 10.2337/dc23-S009
23. Tye SC, de Vries ST, Mann JFE, Schechter M, Mosenzon O, Denig P, et al. Prediction of the effects of liraglutide on kidney and cardiovascular outcomes based on short-term changes in multiple risk markers. Front Pharmacol. (2022) 13:786767. doi: 10.3389/fphar.2022.786767
24. Tuttle KR, Lakshmanan MC, Rayner B, Busch RS, Zimmermann AG, Woodward DB, et al. Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7): a multicentre, open-label, randomised trial. Lancet Diabetes Endocrinol. (2018) 6:605–17. doi: 10.1016/S2213-8587(18)30104-9
25. Sivalingam S, Wasehuus VS, Rotbain Curovic V, Blond MB, Hansen TW, Persson F, et al. Albuminuria-lowering effect of adding semaglutide on top of empagliflozin in individuals with type 2 diabetes: A randomized and placebo-controlled study. Diabetes Obes Metab. (2024) 26:54–64. doi: 10.1111/dom.15287
26. Xu B, Li S, Kang B, Zhou J. The current role of sodium-glucose cotransporter 2 inhibitors in type 2 diabetes mellitus management. Cardiovasc Diabetol. (2022) 21:83. doi: 10.1186/s12933-022-01512-w
27. Wu J, Chen Y, Yang H, Gu L, Ni Z, Mou S, et al. Sodium glucose co-transporter 2 (SGLT2) inhibition via dapagliflozin improves diabetic kidney disease (DKD) over time associatied with increasing effect on the gut microbiota in db/db mice. Front Endocrinol (Lausanne). (2023) 14:1026040. doi: 10.3389/fendo.2023.1026040
28. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. (2019) 380:347–57. doi: 10.1056/NEJMoa1812389
29. Wheeler DC, Stefansson BV, Jongs N, Chertow GM, Greene T, Hou FF, et al. Effects of dapagliflozin on major adverse kidney and cardiovascular events in patients with diabetic and non-diabetic chronic kidney disease: a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. (2021) 9:22–31. doi: 10.1016/S2213-8587(20)30369-7
30. Liu G, Zhong X, Zheng J, Zhang J, Kong W, Hu X, et al. Comparative efficacy of novel antidiabetic drugs on albuminuria outcomes in type 2 diabetes: A systematic review. Diabetes Ther. (2023) 14:789–822. doi: 10.1007/s13300-023-01391-8
31. Gu S, Hu X, Zhen X, Shi L, Shao H, Sun X, et al. Comparison of glucose-lowering drugs as second-line treatment for type 2 diabetes: A systematic review and meta-analysis. J Clin Med. (2022) 11:5435. doi: 10.3390/jcm11185435
32. Lu JM. The role of glucagon-like peptide-1 receptor agonists in type 2 diabetes in asia. Adv Ther. (2019) 36:798–805. doi: 10.1007/s12325-019-00914-9
33. Bain EK, Bain SC. Recent developments in GLP-1RA therapy: A review of the latest evidence of efficacy and safety and differences within the class. Diabetes Obes Metab. (2021) 23:30–9. doi: 10.1111/dom.14487
34. Fan G, Guo DL, Zuo H. The impact of sodium-glucose Cotransporter-2 inhibitors on lipid profile: A meta-analysis of 28 randomized controlled trials. Eur J Pharmacol. (2023) 959:176087. doi: 10.1016/j.ejphar.2023.176087
35. Rezaei S, Tabrizi R, Nowrouzi-Sohrabi P, Jalali M, Atkin SL, Al-Rasadi K, et al. GLP-1 receptor agonist effects on lipid and liver profiles in patients with nonalcoholic fatty liver disease: systematic review and meta-analysis. Can J Gastroenterol Hepatol. (2021) 2021:8936865. doi: 10.1155/2021/8936865
Keywords: dapagliflozin, diabetic kidney disease, glomerular filtration rate, lipid profiles, polyethylene glycol loxenatide, type 2 diabetes mellitus, urinary albumin-to-creatinine ratio
Citation: Cao Y, Cao S, Zhao J, Zhao J, Zhao Y and Liu Y (2024) Efficacy and safety of polyethylene glycol loxenatide in treating mild-to-moderate diabetic kidney disease in type 2 diabetes patients: a randomized, open-label, clinical trial. Front. Endocrinol. 15:1387993. doi: 10.3389/fendo.2024.1387993
Received: 19 February 2024; Accepted: 08 July 2024;
Published: 19 July 2024.
Edited by:
Gopalakrishnan Natarajan, Madras Medical College, IndiaReviewed by:
Cristian Sandoval, Santo Tomás University, ChileCopyright © 2024 Cao, Cao, Zhao, Zhao, Zhao and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ying Liu, MTc1MTk4OTg5QHFxLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.