 Qing Su
Qing Su Zhuo Pan
Zhuo Pan Rong Yin1
Rong Yin1- 1Chongqing University Central Hospital, Chongqing Emergency Medical Center, Chongqing, China
- 2Center for Reproductive Medicine, Chongqing Key Laboratory of Human Embryo Engineering, Chongqing Reproduction Genetics Institute, Chongqing Health Center for Women and Children, Women and Children's Hospital of Chongqing Medical University, Chongqing, China
Objective: Despite the developments of in vitro fertilization (IVF) protocols, implantation failure remains a challenging problem, owing to the unbalance between the embryo, endometrium, and immune system interactions. Effective treatments are urgently required to improve successful implantation. Recently, many researchers have focused on granulocyte colony-stimulating factor (G-CSF) to regulate immune response and embryo-endometrium cross-talk. However, previous studies have reported inconsistent findings on the efficacy of G-CSF therapy on implantation failure. The objective of this review was to further explore the effects of G-CSF according to administration dosage and timing among women who experienced at least one implantation failure.
Methods: We systematically searched MEDLINE, Embase, the Cochrane Central Register of Controlled Trials, Scopus, and Web of Science for randomized controlled trials of G-CSF on implantation failure up to July 21, 2023. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated and the heterogeneity of the studies with the I2 index was analyzed.
Results: We identified a total of 2031 studies and finally included 10 studies in the systematic review and meta-analysis. G-CSF administration improved the clinical pregnancy rate (CPR), implantation rate (IR), biochemical pregnancy rate (BPR), and live birth rate (LBR) in women with at least one implantation failure. Subgroup analyses showed that G-CSF treatment could exert good advantages in improving CPR [OR=2.49, 95%CI (1.56, 3.98), I2 = 0%], IR [OR=2.82, 95%CI (1.29, 6.15)], BPR [OR=3.30, 95%CI (1.42, 7.67)] and LBR [OR=3.16, 95%CI (1.61, 6.22), I2 = 0%] compared with the blank control group. However, compared with placebo controls, G-CSF showed beneficial effects on CPR [OR=1.71, 95%CI (1.04, 2.84), I2 = 38%] and IR [OR=2.01, 95%CI (1.29, 3.15), I2 = 24%], but not on LBR. In addition, >150μg of G-CSF treatment increased CPR [OR=2.22, 95%CI (1.47, 3.35), I2 = 0%], IR [OR=2.67, 95%CI (1.47, 4.82), I2 = 0%] and BPR [OR=2.02, 95%CI (1.17, 3.47), I2 = 22%], while ≤150μg of G-CSF treatment improved miscarriage rate (MR) [OR=0.14, 95%CI (0.05, 0.38), I2 = 0%] and LBR [OR=2.65, 95%CI (1.56, 4.51), I2 = 0%]. Moreover, G-CSF administration on the day of embryo transfer (ET) could increase CPR [OR=2.81, 95%CI (1.37, 5.75), I2 = 0%], but not on the day of ovum pick-up (OPU) or human chorionic gonadotropin (HCG) injection.
Conclusion: G-CSF has a beneficial effect on pregnancy outcomes to some extent among women who experienced at least one implantation failure, and the administration dosage and timing influence the effect size.
Systematic review registration
https://www.crd.york.ac.uk/prospero/, identifier CRD42023447046.
Highlights
● Question/Objective: What are the effects of different administration dosages and timing of granulocyte colony-stimulating factor (G-CSF) for women experienced at least one implantation failure?
● Findings: Ten RCTs evaluating the effect of different administration dosages and timing of G-CSF for women with at least one implantation failure were included. The present study demonstrated that G-CSF improved pregnancy outcomes. More specifically, >150μg of G-CSF treatment increased clinical pregnancy rate (CPR), implantation rate (IR), and biochemical pregnancy rate (BPR), while ≤150μg of G-CSF treatment improved miscarriage rate (MR) and live birth rate (LBR). In addition, G-CSF administration on the day of embryo transfer (ET) could increase CPR, but not on the day of ovum pick-up (OPU) or human chorionic gonadotropin (HCG) injection.
● Meaning: Based on the meta-analysis, G-CSF could improve pregnancy outcomes, and the administration dosage and timing influence the effect size.
Introduction
Embryo implantation is a key process in reproduction, most of the pregnancy failures happen during the embryo implantation period (1). The incidence of implantation failures varies from 8 to 33% in the general population (2). Despite the developments of in vitro fertilization (IVF) protocols, the embryo implantation rate is only 20-30%, and only 40% even if the blastocyst is transferred. Around 10-15% of patients undergoing assisted reproductive technology (ART) procedures experience unexplained recurrent implantation failures (3–5). Given the challenges encountered with the incidence of implantation failure, additional efforts are urgently required to increase successful fertilization and implantation.
Embryo implantation is regulated by several factors, the balance between the embryo, endometrium, and immune system interactions are essential for successful implantation (2, 6). It is estimated that embryos account for one-third of implantation failures, while suboptimal endometrial receptivity and altered embryo-endometrial cross-talk are responsible for the remaining two-thirds (7–9). However, there are some other influential factors, such as anatomic structure, autoimmune factors, thrombophilic conditions and lifestyle (10), which means that a multidisciplinary approach is required for the management of implantation failure. Various interventions have been developed to improve implantation, especially for those with repeated implantation failure. These approaches include endometrial scratch injury (11), improving endometrial thickness in women with thin endometrium (12), intrauterine human chorionic gonadotrophin (13), intravenous Atosiban (14), preimplantation genetic screening (15), and the use of immunomodulators (16). Despite these therapeutic alternatives, implantation failure remains a challenging problem.
Granulocyte colony-stimulating factor (G-CSF) is a hematopoietic-specific cytokine synthesized by bone marrow cells, stromal cells, fibroblasts, and macrophages (17), and has been proven to originate from some reproductive tissue cells (18). Particularly, some pieces of evidence have shown that G-CSF and its receptor are located in luteinized granulose cells, trophoblastic cells and oocytes (19–21), indicating the importance of this cytokine in implantation. Moldenhauer LM et al. found that G-CSF temporarily suppresses the immune response and plays an essential part in embryo-endometrium cross-talk through its effects on type two T helper cells and endometrial angiogenesis (22). In 2009, G-CSF was first successfully used in patients with recurrent abortions (23), and later several clinical trials suggested that G-CSF administration may improve the success of IVF in thin endometrium (24, 25). The therapeutic effect of G-CSF in patients with recurrent implantation failure (RIF) has been investigated as early as 2000, and the results show that systematic administration of G-CSF can enhance the implantation rate dramatically (26). Since then, bulks of studies with controversial results have evaluated the effect of G-CSF on implantation failures due to poor endometrial thickness or other reasons. In the study of Aleyasin and coworkers, administration of single-dose subcutaneous G-CSF before implantation significantly increases implantation and pregnancy rates in infertile women with repeated IVF failure (27). However, Kalem and colleagues showed that the administration of G-CSF into the uterine cavity in RIF patients with normal endometrium did not alter the endometrial thickness, clinical pregnancy rate, or live birth rate (28).
Synthesized evidence is needed to help clinicians choose an appropriate treatment for infertility women with implantation failure. However, the current meta-analysis shows many shortcomings. For example, Kamath MS et al. showed that the pregnancy rate of RIF in the G-CSF group was significantly higher than that in the placebo group (29). Nevertheless, only two articles were included, which contributed to bias in the outcome. Recently, Hou, et al. indicated that G-CSF improved the clinical pregnancy rate (CPR) in patients with unexplained RIF for both the fresh and frozen embryo transfer cycles, and for both subcutaneous injection and intrauterine infusion (30). However, it failed to compare the effects of different dosages of G-CSF on pregnancy outcomes. Furthermore, the best administration timing for G-CSF remains uncertain. In this systematic review and meta-analysis, in addition to the CPR, biochemical pregnancy rate (BPR), implantation rate (IR), miscarriage rate (MR) and live birth rate (LBR), subgroup analysis was conducted according to administration dosage of G-CSF and timing of intervention to obtain further information on the influence of G-CSF on implantation failure patients.
Methods
This systematic review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and was registered with the International Prospective Register of Systematic Reviews (PROSPERO), number CRD42023447046.
Search strategy and eligibility criteria
We selected relevant studies from the following databases: MEDLINE, Embase, the Cochrane Central Register of Controlled Trials, Scopus and Web of Science. We developed a search strategy from text and MeSH terms related to “granulocyte colony-stimulating factor,” “G-CSF,” “implantation failure,” “endometrium,” “in vitro fertilization,” “IVF,” and “intracytoplasmic sperm injection” up to July 21, 2023. Additionally, references and citations of the relevant literature retrieved were carefully searched to find more additional eligible literature.
We included studies that compared G-CSF to no intervention, placebo, or any other treatments. We identified eligible studies according to the following criteria: participants had to be subfertile women who experienced one or more implantation failures and have no uterine adhesions; the outcomes were medically confirmed pregnancy outcomes including CPR, IR, BPR, LBR, and MR; study design must be double-blind RCTs. Exclusion criteria were as follows: observation studies, animal studies, case reports, self-pro-post studies, conference abstracts and review articles; studies not published in English. For the overlapped sample sources, we included the report with more information and larger sample sizes.
Two independent investigators reviewed study titles and abstracts, and studies that satisfied the inclusion criteria were retrieved for full-text assessment. The agreement of both investigators determined final eligibility. Disagreements were referred to a third reviewer to reach consensus.
Data extraction and assessment of risk bias
Two reviewers independently extracted the following data from each included study using a specifically designed form: study design, sample sizes, participant characteristics, the number of previous implantation failures, intervention details, and outcome parameters. Extracted data were abstracted directly onto previously designed standardized electronic form.
Two independent reviewers assessed the included studies for methodological quality using the Cochrane risk of bias tool, containing seven specific domains. We resolved any disagreements by consensus or by discussion with a third author. Each domain was assigned a judgment relating to the risk of bias for that study classified as low, high, or unclear risk. Disagreements were referred to a third reviewer to reach a consensus.
Statistical analysis
The odd ratio(OR) and the corresponding 95% CI were calculated for all dichotomous data. The pooled ORs were calculated through a Mantel-Hansel fixed-effects model if there was no heterogeneity; otherwise, a random-effects model was adopted. We assessed statistical heterogeneity using the I2 statistic, with values greater than 50% regarded as moderate-to-high heterogeneity. We performed prespecified subgroup analyses according to the following parameters: dosage of administration of G-CSF and intervention timing. We did Egger tests to assess funnel plot asymmetry and defined significant publication bias with a p-value lowing 0.1. We conducted the statistical analyses with Review Manager(Revman5.3.3, Cochrane Collaboration, Copenhagen, Denmark, 2014) and Stata software (version 14.0, Stata Corp LP, Texas, USA, 1985-2015).
Results
Search results
In total, we identified 2031 studies, and 1049 studies remained after we removed duplicates. Subsequently, we excluded 999 studies after reviewing the titles and abstracts. Of the remaining 50 articles assessed for eligibility, 40 studies were further excluded after reading the full text for the following reasons: 9 were abstracts; 15 studies were not part of the literature about implantation failures; 12 studies were not RCTs, 4 of them were self-pro-post control studies. Finally, ten studies reported sufficient data (27, 28, 31–38), while nine studies were included in the quantitative synthesis (27, 28, 31–37). A flow diagram depicting the search and selection process is shown in Figure 1.
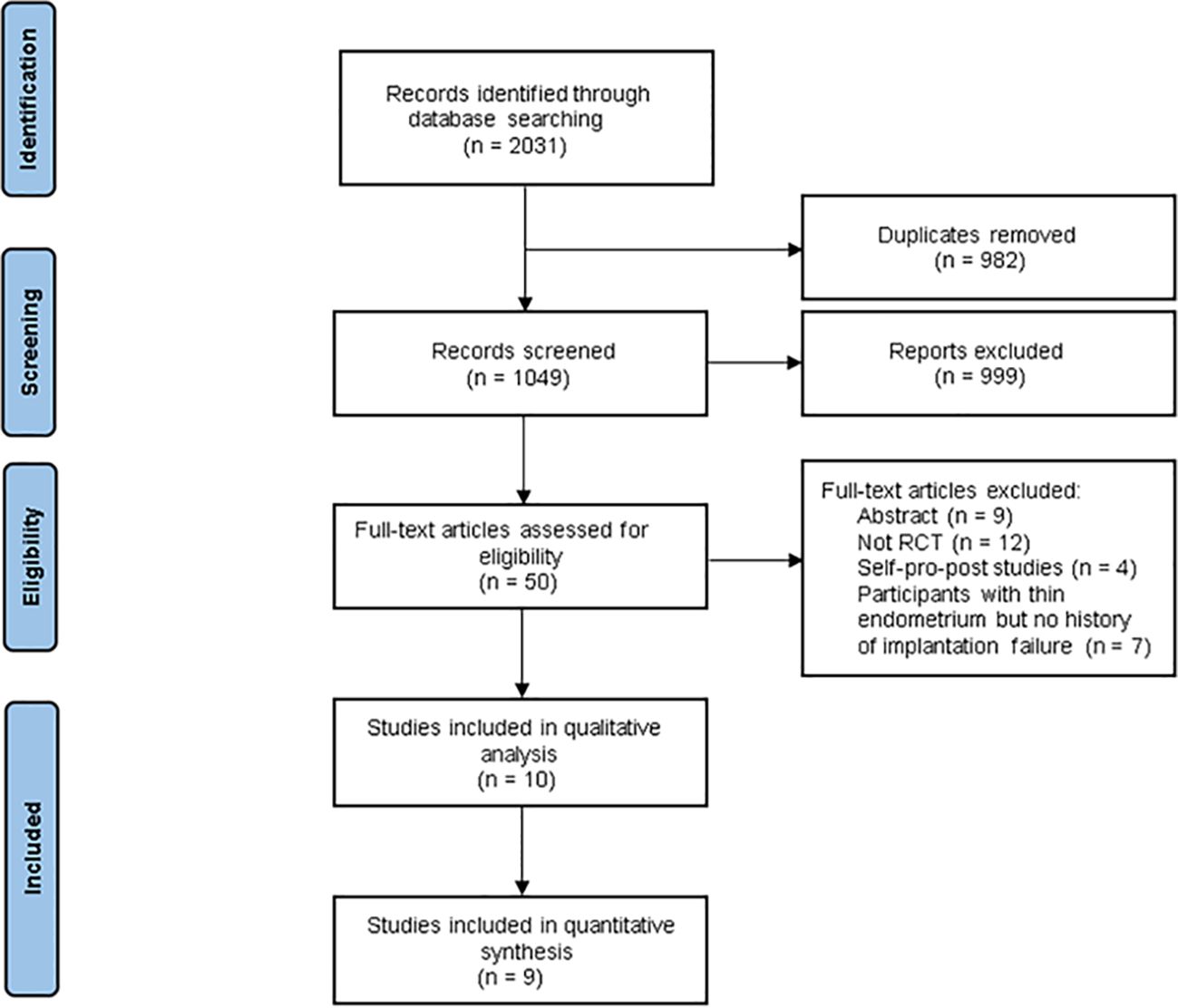
Figure 1 Flow diagram for study selection process.
Description of included studies
The meta-analysis contained 942 participants: 454 women in the intervention group,99 of whom were in the HCG group, and 389 were in the control group. Mean age ranged from 31.75 ± 5.16 to 35.5 ± 4.32 years old. Seven studies compared the G-CSF group with the control group (no intervention or placebo) (27, 28, 31, 33–36), one compared the G-CSF group with the HCG group (32), and one study included three arms: G-CSF group, placebo group and HCG group (37). In two studies, G-CSF was administered by subcutaneous injection (27, 31), while in all the other studies included, G-CSF was used by intrauterine perfusion. Seven studies analyzed fresh cycles (27, 28, 31, 32, 34, 36, 37), one compared frozen cycles (35), and one included both fresh and frozen cycles (33). Participants in all of these studies had endometrial thicknesses greater than 7mm (Table 1).
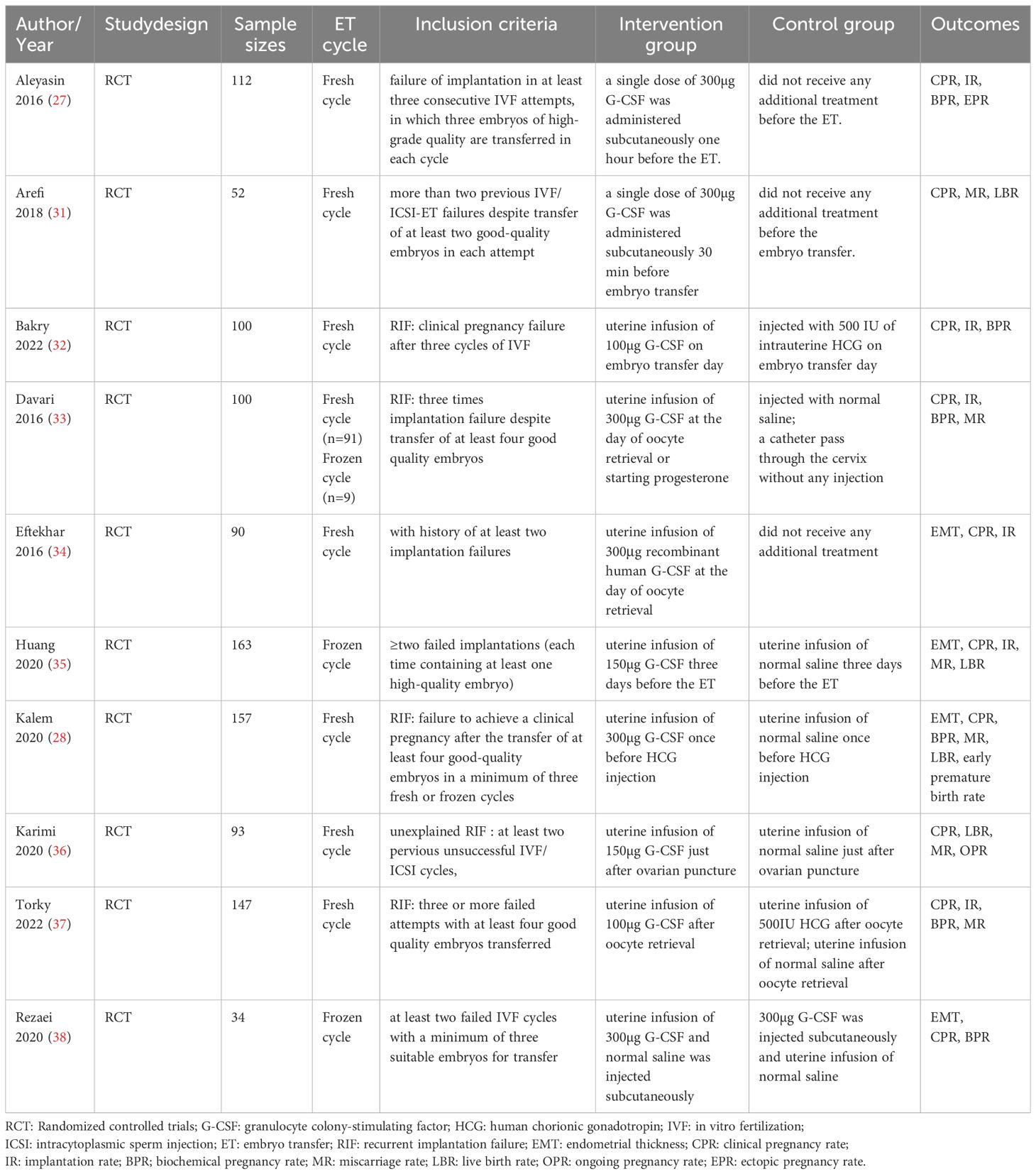
Table 1 Characteristics of included trials.
One RCT could not be included in the quantitative analysis due to the absence of outcomes in the placebo group. Rezaei Z. et al. observed the beneficial effects of CPR in both the intrauterine group and the subcutaneous group, with no significant difference between the two groups. Besides, they also reported significantly lower drug side effects in the intrauterine group (38).
Risk of bias in included studies
We assessed the risk of bias in all included studies, as demonstrated in Figure 2. All of the included studies reported adequate methods for random sequence generation. Five studies did not specify whether data collectors and outcome assessors were masked to treatment allocation (28, 31, 33–35). Two studies were rated at low risk of bias (32, 36), and two were judged to be at high risk because of open-label or incomplete outcome data (27, 31).
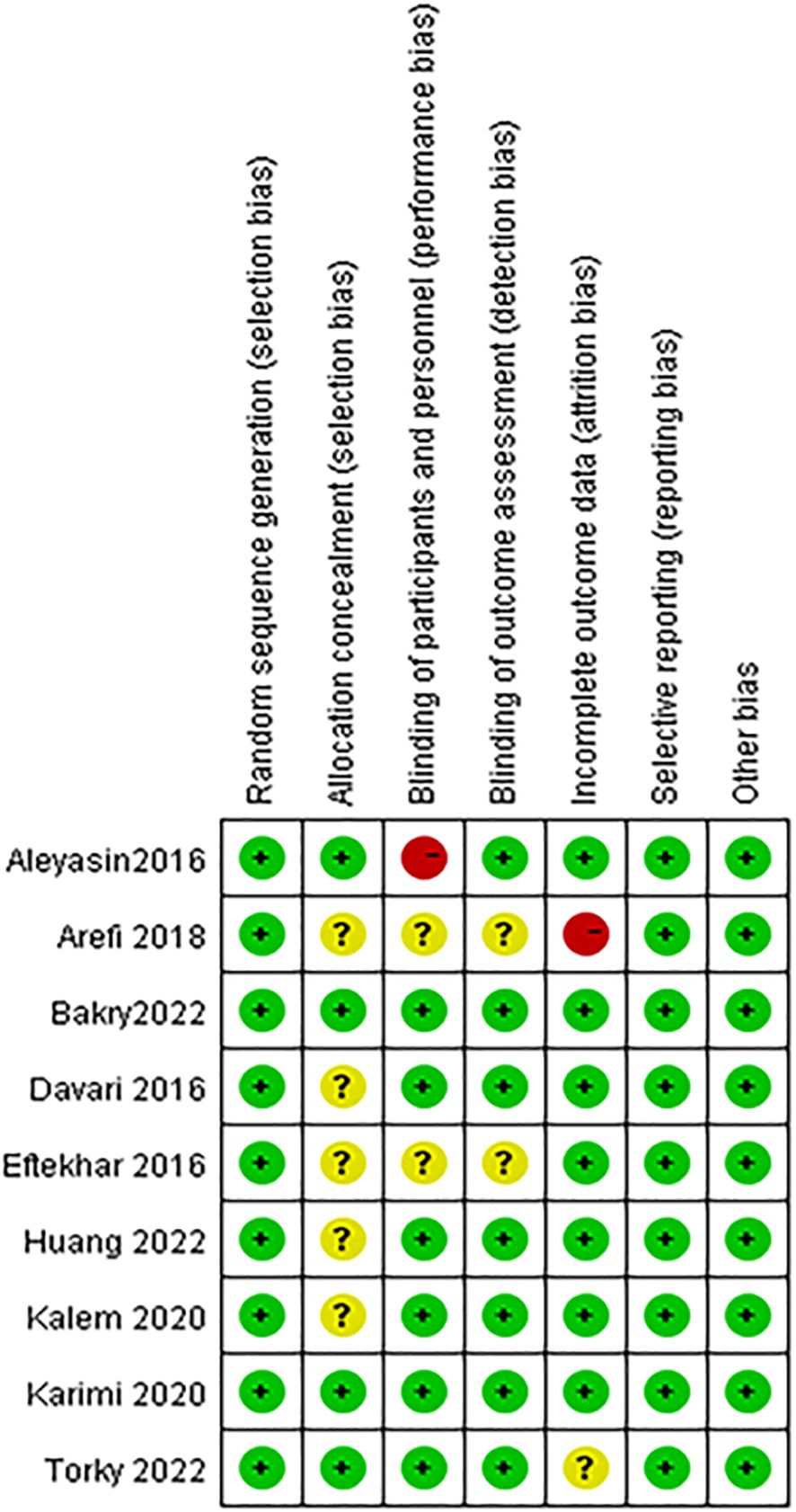
Figure 2 Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
G-CSF versus no intervention
CPR
All of the studies, comparing the G-CSF group with the control group, described CPR. Considering the low heterogeneity (I2 = 15%), a fixed-effects model was utilized for the meta-analysis, and the result showed that G-CSF could better improve the CPR [OR=1.98, 95%CI (1.48, 2.65)], as shown in Figure 3A.
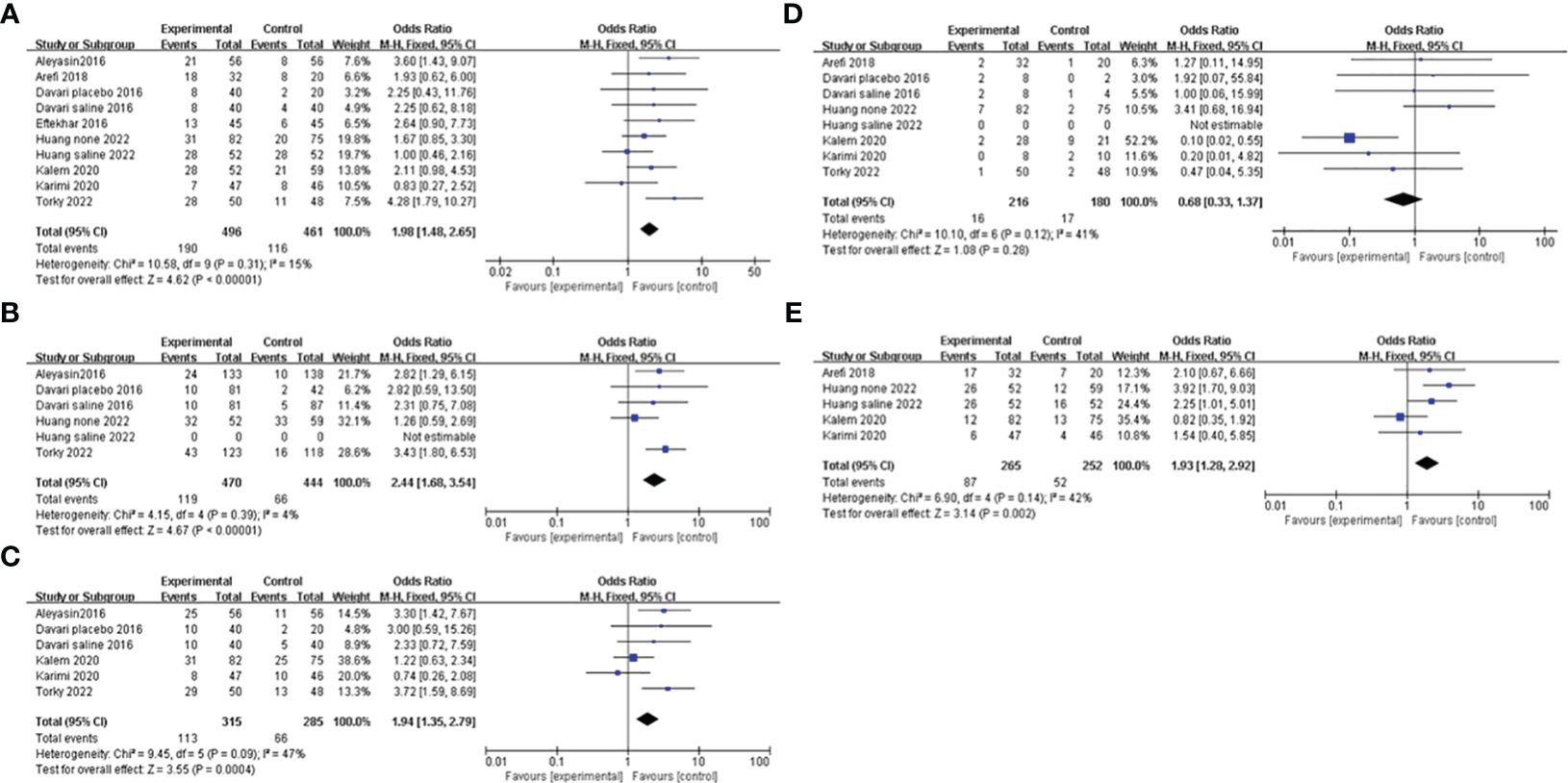
Figure 3 Forest plot showing individual and combined effect size estimates and 95% confidence intervals (CIs) in studies that evaluated the effect of G-CSF on pregnancy outcomes in women who experienced at least one implantation failure. (A) clinical pregnancy rate. (B) implantation rate. (C) biochemical pregnancy rate. (D) miscarriage rate. (E) live birth rate.
IR
Four studies reported the IR and included 914 patients, 470 of whom were in the study group and 444 of whom were in the control group. A fixed-effects model was used for data synthesis, and the results indicated that G-CSF treatment improved the IR in patients with a history of implantation failure [OR=2.44, 95%CI (1.68, 3.54), I2 = 4%]; see Figure 3B for details.
BPR
Five studies compared BPR after different interventions in two groups. A fixed-effects model was adopted for data analysis, and the results showed that BPR was increased by G-CSF administration [OR=1.94, 95%CI (1.35, 2.79), I2 = 47%]; see Figure 3C for details.
MR
A total of six studies were reported and included 386 patients. A fixed-effects model was used for meta-analysis, and the results revealed that there was no significant difference in MR in the two groups with or without G-CSF [OR=0.68, 95%CI (0.33, 1.37), I2 = 41%]; see Figure 3D for details.
LBR
Four studies investigated the LBR after different treatments in the two groups, and the fixed-effects model was utilized for comparison. The results revealed that LBR was increased by G-CSF administration[OR=1.93, 95%CI (1.28,2.92), I2 = 42%]; see Figure 3E for details.
Subgroup analysis
We conducted a subgroup analysis based on different controls. Four studies were blank controls and five were placebo controls (saline or empty catheter entry into the uterine cavity). The results indicated that G-CSF treatment could exert good advantages in improving CPR [OR=2.49, 95%CI (1.56, 3.98), I2 = 0%], IR [OR=2.82, 95%CI (1.29, 6.15)], BPR[OR=3.30, 95%CI (1.42, 7.67)] and LBR [OR=3.16, 95%CI (1.61, 6.22), I2 = 0%] compared with the blank control group. However, compared with placebo controls, G-CSF showed beneficial effects on CPR [OR=1.71, 95%CI (1.04, 2.84), I2 = 38%] and IR [OR=2.01, 95%CI (1.29, 3.15), I2 = 24%], but not on LBR; see Figure 4 for details.
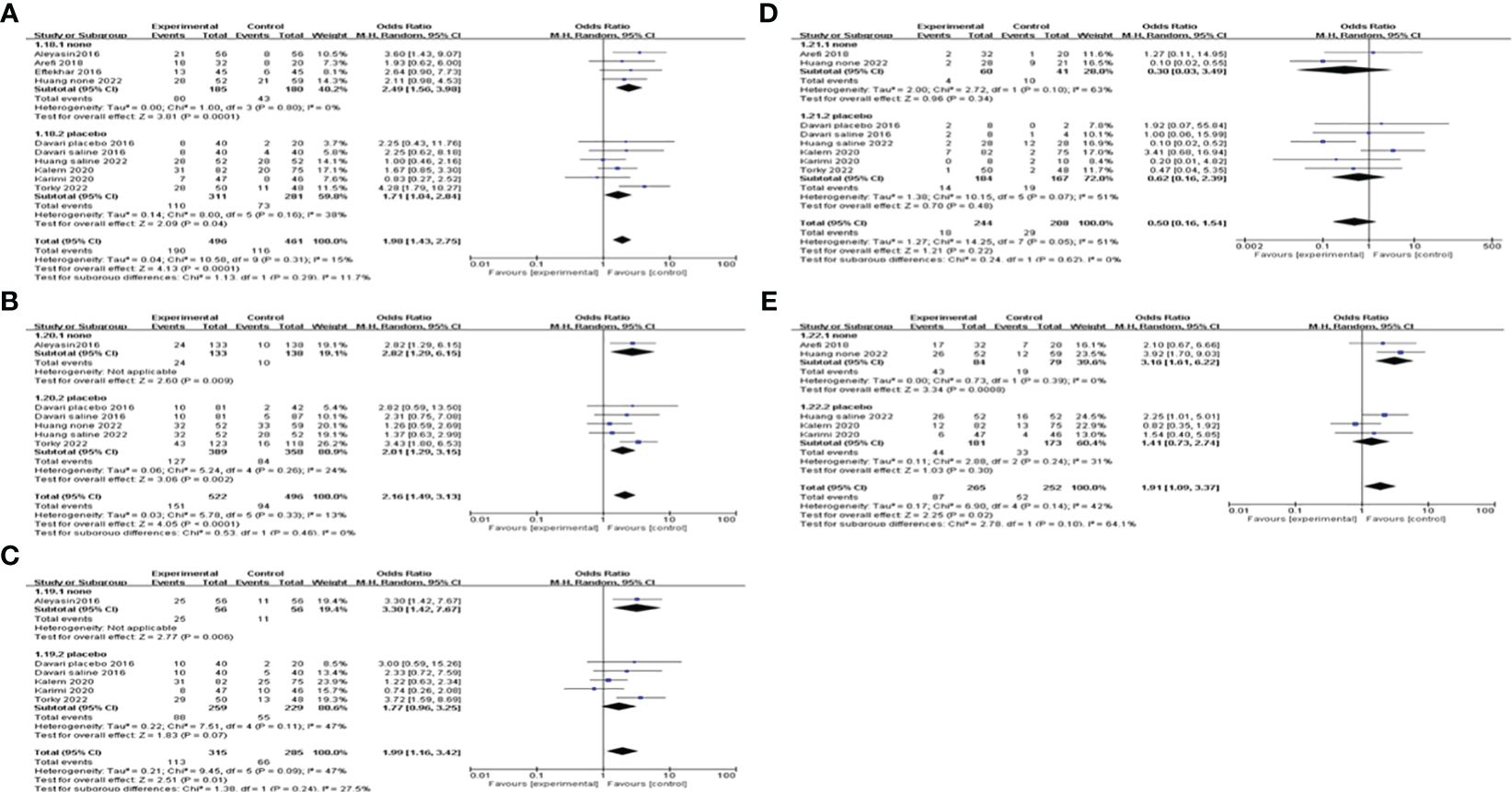
Figure 4 Subgroup analysis comparing the effect of G-CSF on pregnancy outcomes based on different controls. (A) clinical pregnancy rate. (B) implantation rate. (C) biochemical pregnancy rate. (D) miscarriage rate. (E) live birth rate.
We also did subgroup analysis by administering a dosage of G-CSF on all of the pregnancy outcomes. The pooling results indicated that >150μg of G-CSF treatment could exert good advantages in improving CPR [OR=2.22, 95%CI (1.47, 3.35), I2 = 0%], but ≤150μg could not. Furthermore, both IR and BPR were higher in the >150μg subgroup[IR: OR=2.67, 95%CI (1.47, 4.82), I2 = 0%; BPR: OR=2.02, 95%CI (1.17, 3.47), I2 = 22%], but not in the ≤150μg subgroup. However, in the ≤150μg subgroup, MR was lower [OR=0.14, 95%CI (0.05, 0.38), I2 = 0%], and LBR was improved [OR=2.65, 95%CI (1.56, 4.51), I2 = 0%], but neither of them showed a significant difference in the >150μg subgroup; see Figure 5 for details.
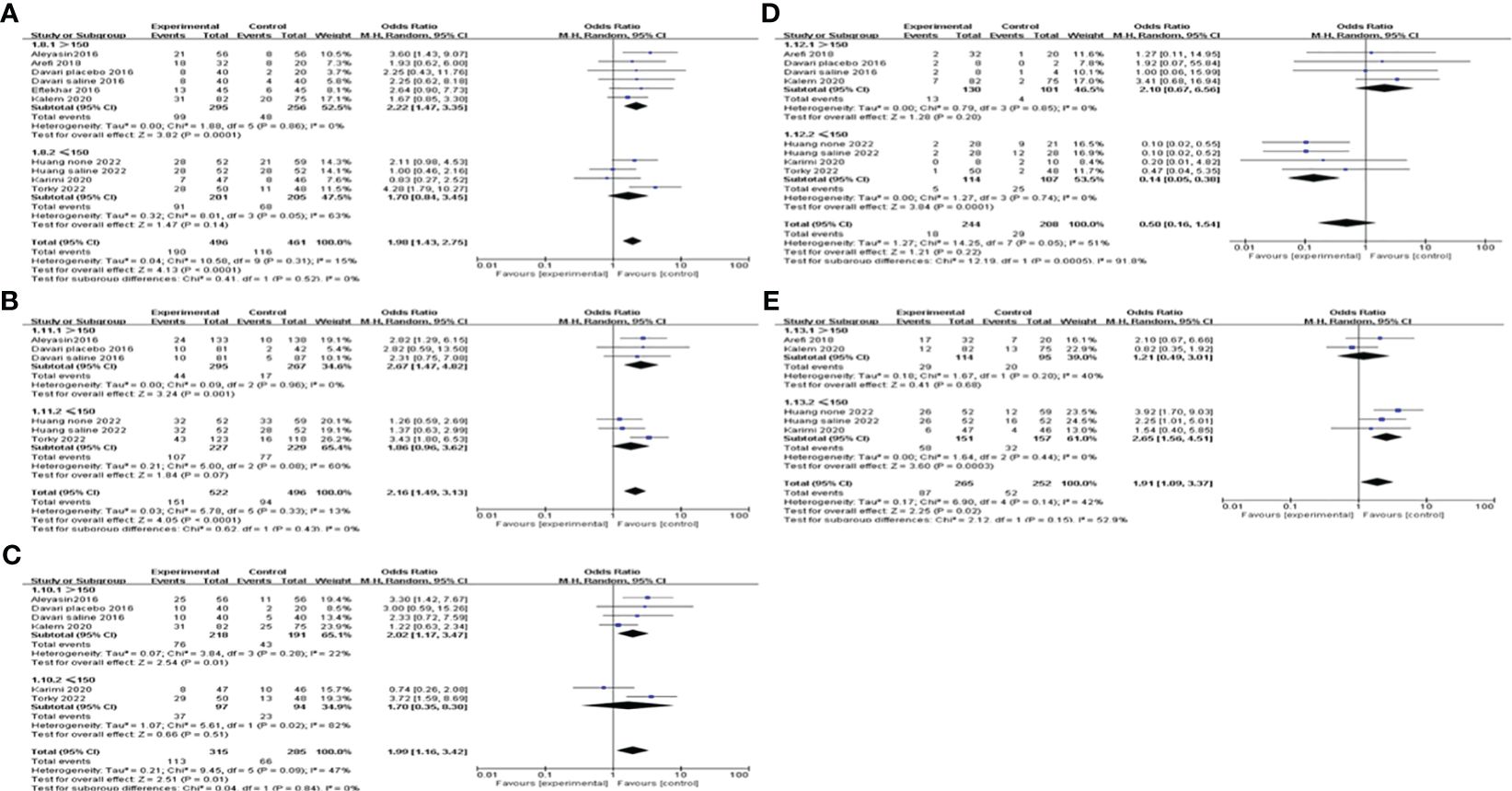
Figure 5 Subgroup analysis comparing the effect of G-CSF on pregnancy outcomes based on different administration dosages. (A) clinical pregnancy rate. (B) implantation rate. (C) biochemical pregnancy rate. (D) miscarriage rate. (E) live birth rate.
When subgroup analysis was carried out according to different intervention timing, the results showed that G-CSF administration on the day of ET could increase CPR [OR=2.81, 95%CI (1.37, 5.75), I2 = 0%], IR[OR=2.82, 95%CI (1.29, 6.15)]and BPR[OR=3.30, 95%CI (1.42, 7.67)], while not on the day of ovum pick-up (OPU) or HCG injection. MR and LBR of different administration timing subgroups did not differ significantly; see Figure 6 for details.
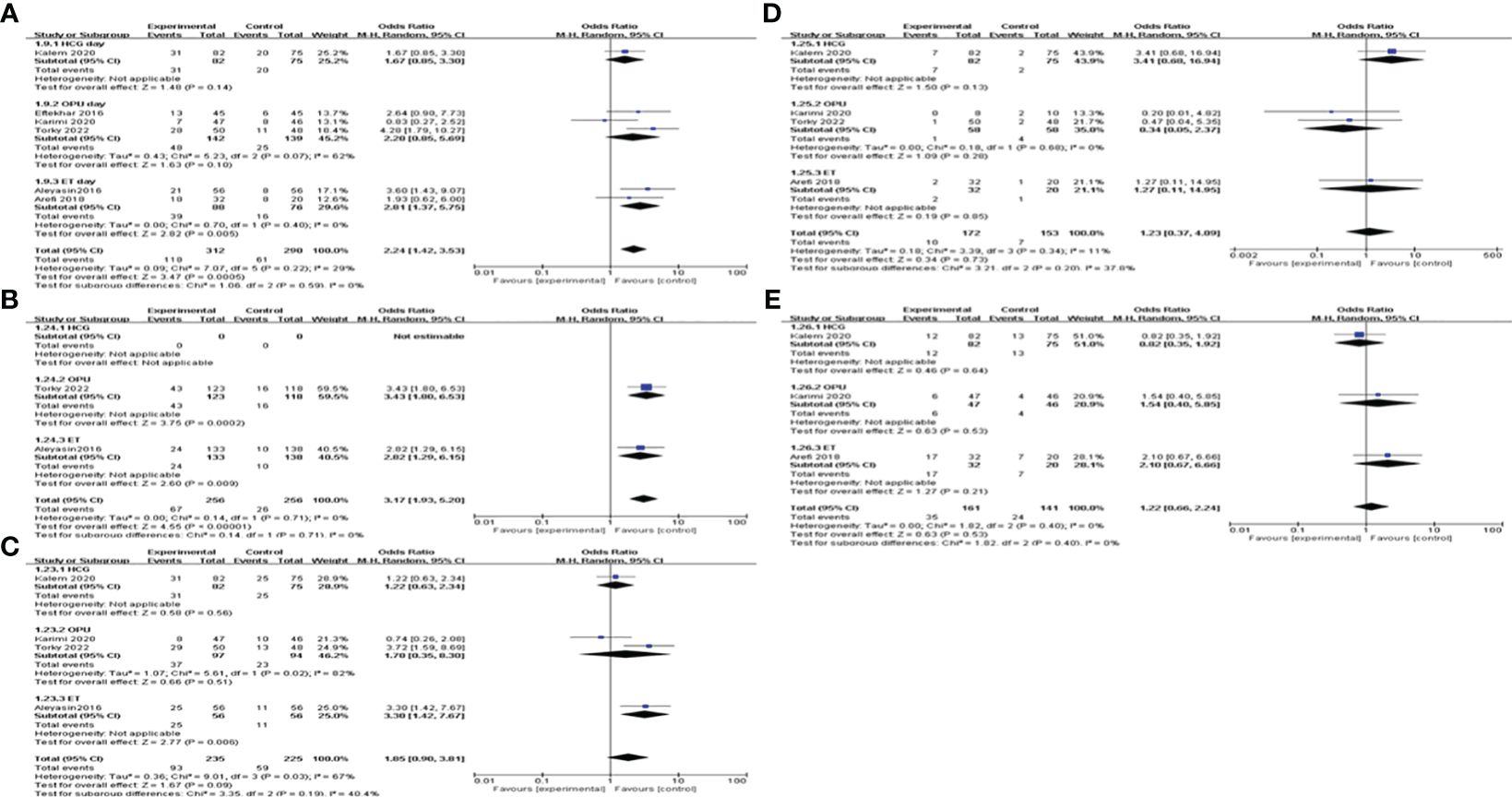
Figure 6 Subgroup analysis comparing the effect of G-CSF on pregnancy outcomes based on different intervention timing. (A) clinical pregnancy rate. (B) implantation rate. (C) biochemical pregnancy rate. (D) miscarriage rate. (E) live birth rate.
We conducted a subgroup analysis based on the route of G-CSF administration. The pooling results indicated that both subcutaneous injection and intrauterine infusion of G-CSF improve CPR [subcutaneous OR=2.83, 95%CI (1.39, 5.75), I2 = 0%; intrauterine OR=1.84, 95%CI (1.34, 2.53), I2 = 20%]; and IR [subcutaneous OR=2.82, 95%CI (1.29, 6.15); intrauterine OR=2.01, 95%CI (1.29, 3.15), I2 = 24%]; see Figure 7 for details.
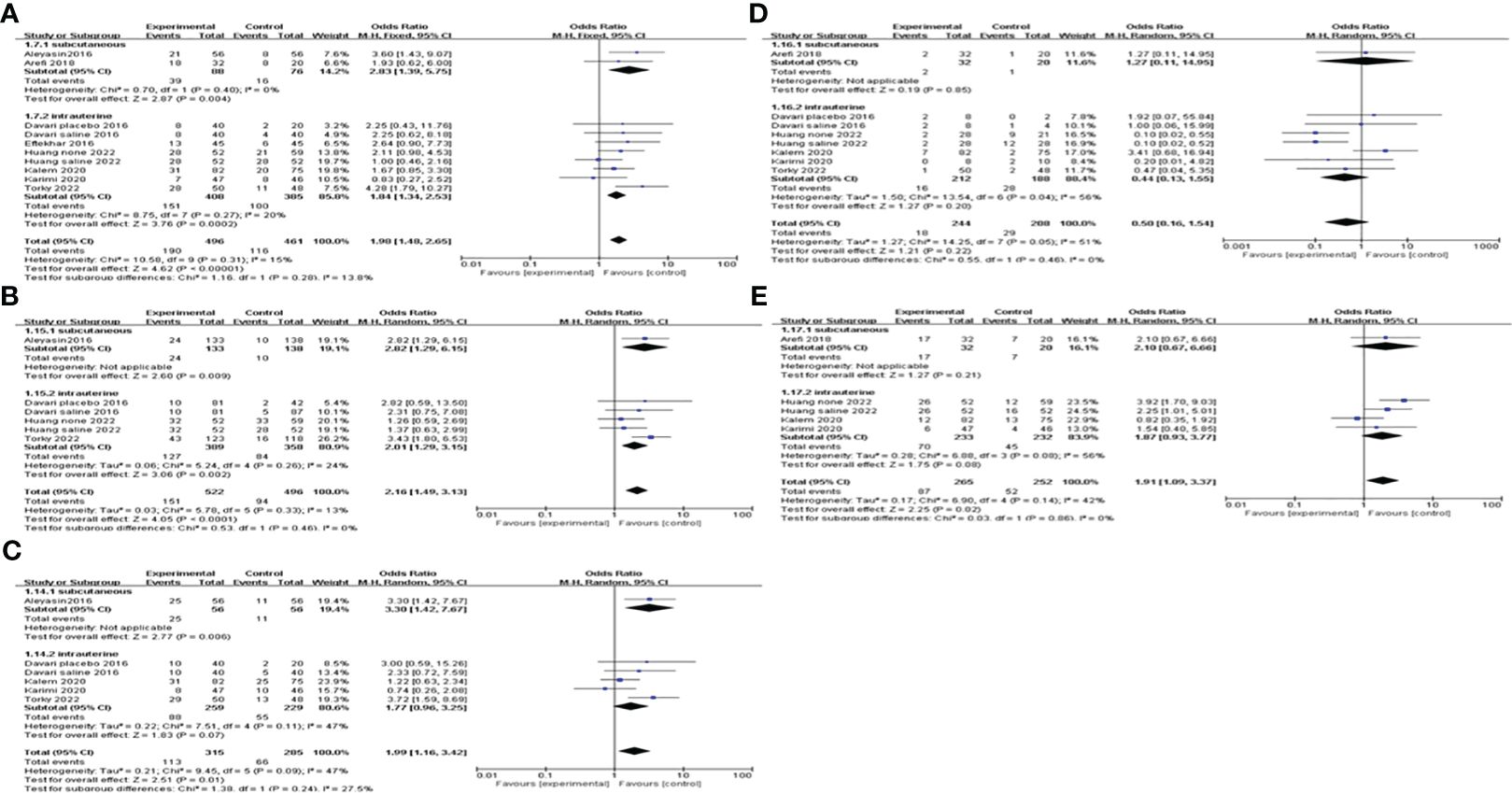
Figure 7 Subgroup analysis comparing the effect of G-CSF on pregnancy outcomes based on the route of G-CSF administration. (A) clinical pregnancy rate. (B) implantation rate. (C) biochemical pregnancy rate. (D) miscarriage rate. (E) live birth rate.
G-CSF versus HCG
Two articles compared the values of G-CSF with HCG on pregnancy outcomes in patients with a history of implantation failure. Pooled analysis indicated that the CPR, IR and BPR in the G-CSF group were higher than those in the HCG group, but the difference was not statistically significant; see Figure 8 for details.
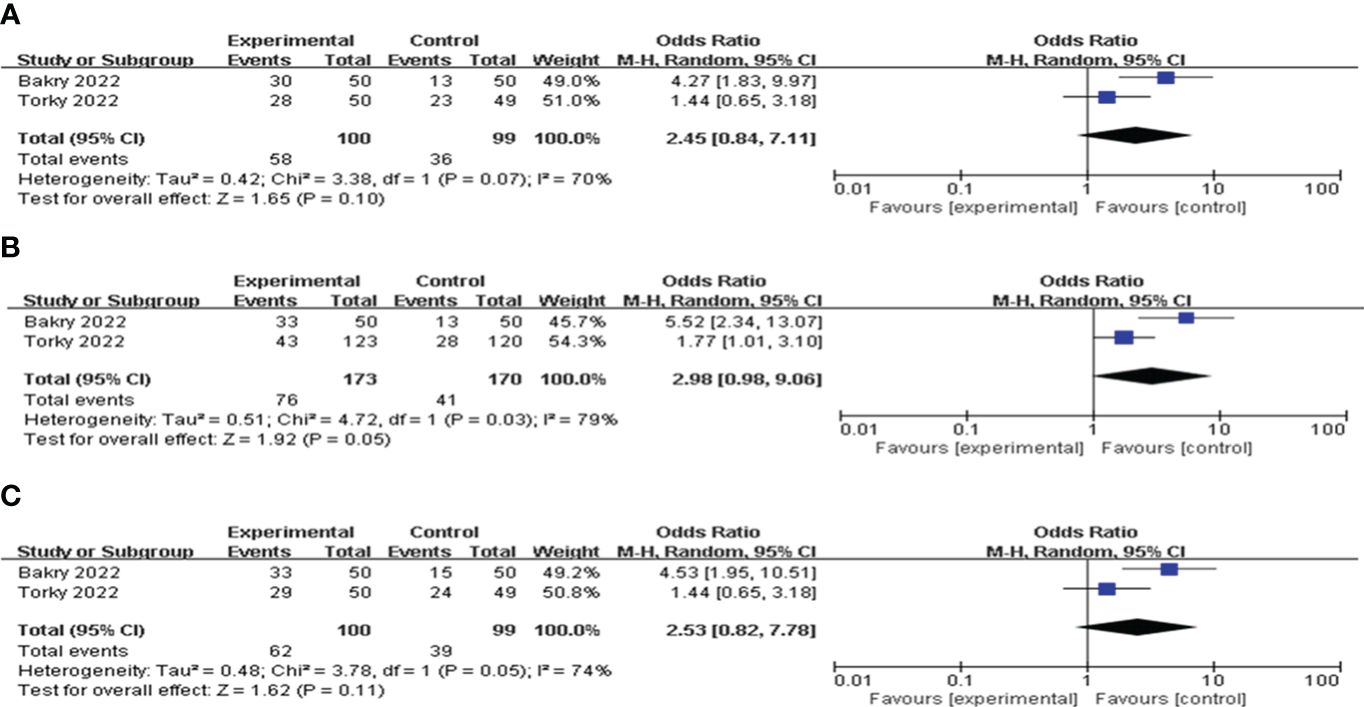
Figure 8 Forest plot comparing the effect of G-CSF on pregnancy outcomes versus HCG. (A) clinical pregnancy rate. (B) implantation rate. (C) biochemical pregnancy rate.
Publication bias analysis
For publication bias, the funnel plot and regression analyses of Egger’s test indicated a relatively low likelihood of publication bias. The result is presented in Supplementary Figure 1.
Discussion
We performed a systematic review and meta-analysis to summarize the efficacy of G-CSF in women who experienced at least one implantation failure. Nine RCTs reported sufficient quantitative data which allowed for statistical pooling. The meta-analysis outcome showed that patients with a history of implantation failure could benefit from the use of G-CSF. When compared to the control group, the use of G-CSF was related to a statistically significant increase in the rates of clinical pregnancy, implantation, chemical pregnancy and live birth. However, G-CSF did not show significant advantages in improving MR. We estimated that such results may be attributed to the single injection of G-CSF, with the decrease in the sustaining effects of G-CSF, some patients with poor endometrial receptivity are unable to maintain pregnancy, leading to the occurrence of miscarriage.
Some studies found that an endometrial thickness of <7 mm and a high reproductive age may negatively impact the pregnancy results (39–42). A meta-analysis to explore the efficiency of G-CSF on infertile women with thin endometrium reported that intrauterine perfusion of G-CSF could significantly improve endometrial thickness and CPR (43). In this review, all of the women included were below 40 years old and had endometrial thicknesses greater than 7mm, so we excluded the influence of endometrium thickness and childbearing age.
Over the last two decades, endometrial injury has been studied to improve implantation rates and decrease the incidence of implantation failure in IVF cycles. A previous meta-analysis has proved that endometrial injury could exert good advantages in improving implantation success, CPR and LBR in patients with at least one failed IVF cycle (44). During the intrauterine infusion G-CSF, the insertion and removal of tubes are needed to finish the treatments. If the controls only took measures of no treatment, it was unable to assess the effect of the mechanical manipulation of the uterine cavity on the pregnancy outcomes. Since some included studies in this meta-analysis were blank controls and some were placebo controls, we conducted a subgroup analysis based on different controls. The results indicated that G-CSF treatment could exert good advantages in improving CPR, IR, and LBR compared with the blank control group. However, compared with placebo controls (saline or empty catheter entry into the uterine cavity), G-CSF showed beneficial effects on CPR and IR, but not on LBR. This suggested that G-CSF therapy had a beneficial influence on CPR and IR, rather than due to mechanical manipulation.
The reasons for this improvement may include induction of local immune regulation of the endometrium, embryo adhesion and implantation, proliferation of trophoblasts and endometrial vascular remodeling by G-CSF. Some studies have reported that the receptor for G-CSF can be found in trophoblastic cells, endometrial glandular cells, follicular cells and oocytes (19–21). Moreover, as an important medium of intercellular communication, G-CSF could recruit dendritic cells, activate Tregs and promote the secretion of Th2 cytokine, which influence the gene expression regulating cellular adhesion pathways, vascular remodeling and immune modulation in the endometrium (45). Recently, Ding JL et al. demonstrated that G-CSF derived from M2 macrophage could promote trophoblasts invasion and migration through activating PI3K/AKT/Erk1/2 pathway, thereby involving in normal pregnancy program (46).
We performed a subgroup analysis by the route of G-CSF administration, and our results showed that both subcutaneous injection and intrauterine infusion of G-CSF improve CPR in women with implantation failure. Consistent with this study, a previous meta-analysis by Hou, et al. reported that the administration of G-CSF via either subcutaneous injection or intrauterine infusion for RIF patients can improve CPR (30). However, it failed to explore the optimal administration dosage of G-CSF. We conducted subgroup analysis by administration dosage of G-CSF, the results suggested that >150μg of G-CSF therapy could exert good advantages in improving CPR, IR, and BPR, but not abortion and LBR. It is interesting that in the ≤150μg subgroup, both MR and LBR were improved, while CPR, IR, and BPR were not significantly different. This is the only study to investigate the relationship between G-CSF dose and pregnancy outcome so far. However, due to the small sample size and indirect evidence, no accurate conclusions can be drawn, and further studies with rigorously designed RCT are needed.
In addition, we noted that the timing of G-CSF administration was inconsistent across the included studies, so we conducted a subgroup analysis according to different intervention timing. The results suggested that G-CSF administration on the day of ET could increase CPR, while not on the day of OPU or HCG injection. This meta-analysis may provide a favorable time point to initiate G-CSF.
On the other hand, when compared to HCG, G-CSF increased the CPR, IR and BPR in patients with implantation failure, but did not achieve a statistical difference. Considerable heterogeneity was observed in the synthesis, which might have been caused by the small number of included studies and small sample size.
Limitations
There are several limitations of this systematic review and meta-analysis. First, in most of the included studies, the cause of implantation failure was not mentioned, so we were not able to perform a sub-group analysis regarding the cause of implantation failure, and still more studies are needed for a definitive conclusion. Second, not all of the included studies gave the research outcomes that we needed, more well-designed clinical studies are needed to investigate the optimal dosage and timing of G-CSF therapy to improve LBRs. Third, most of the studies we included analyzed fresh cycles, while one compared frozen cycles, and another one included both fresh and frozen cycles. However, we could not extract them from the statistics to conduct a subgroup analysis and draw a conclusion as to which embryo transfer protocol benefits more from G-CSF. At the same time, our included studies did not report whether euploid tests were carried out or not. We suggest that the following studies list more detailed data if they include more than one embryo transfer method. Despite this, our study provides a comprehensive review of the current literature guided by a prospectively registered protocol. Overall, the conclusions drawn from this review represent a current collation of evidence.
Conclusions
In conclusion, G-CSF has a beneficial effect on CPR to some extent, and the administration dosage and timing influence the effect size. Our findings from indirect evidence support the use of >150μg G-CSF administration on the day of ET in women who experienced at least one implantation failure. Further, head-to-head RCTs with high quality and larger sample sizes are needed to evaluate the effects of different dosages and timing of G-CSF administration on pregnancy outcomes to provide direct evidence.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
QS: Writing – review & editing, Writing – original draft, Supervision. ZP: Writing – original draft, Writing – review & editing. RY: Writing – original draft. XL: Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2024.1370114/full#supplementary-material
References
1. Teklenburg G, Salker M, Heijnen C, Macklon NS, Brosens JJ. The molecular basis of recurrent pregnancy loss: impaired natural embryo selection. Mol Hum Reproduction. (2010) 16:886–95. doi: 10.1093/molehr/gaq079
2. Salamonsen LA, Evans J, Nguyen HP, Edgell TA. The microenvironment of human implantation: determinant of reproductive success. Am J Reprod Immunol (New York NY 1989). (2016) 75:218–25. doi: 10.1111/aji.12450
3. Calhaz-Jorge C, De Geyter C, Kupka MS, Mouzon J, Erb K, Mocanu E, et al. Assisted reproductive technology in Europe, 2013: results generated from European registers by ESHRE. Hum Reprod (Oxford England). (2017) 32:1957–73. doi: 10.1093/humrep/dex264
4. Madkour A, Bouamoud N, Louanjli N, Kaarouch I, Copin H, Benkhalifa M, et al. Intrauterine insemination of cultured peripheral blood mononuclear cells prior to embryo transfer improves clinical outcome for patients with repeated implantation failures. Zygote (Cambridge England). (2016) 24:58–69. doi: 10.1017/S0967199414000719
5. Coughlan C, Ledger W, Wang Q, Liu F, Demirol A, Gurgan T, et al. Recurrent implantation failure: definition and management. Reprod Biomed online. (2014) 28:14–38. doi: 10.1016/j.rbmo.2013.08.011
6. Fox C, Morin S, Jeong JW, Scott RT Jr, Lessey B. Local and systemic factors and implantation: what is the evidence? Fertil Steril. (2016) 105:873–84. doi: 10.1016/j.fertnstert.2016.02.018
7. Edwards RG. Implantation, interception and contraception. Hum Reprod (Oxford England). (1994) 9:985–95. doi: 10.1093/oxfordjournals.humrep.a138673
8. Simón C, Moreno C, Remohí J, Pellicer A. Cytokines and embryo implantation. J Reprod Immunol. (1998) 39:117–31. doi: 10.1016/S0165-0378(98)00017-5
9. Franasiak JM, Forman EJ, Hong KH, Werner MD, Upham KM, Treff NR, et al. The nature of aneuploidy with increasing age of the female partner: a review of 15,169 consecutive trophectoderm biopsies evaluated with comprehensive chromosomal screening. Fertil Steril. (2014) 101:656–63.e1. doi: 10.1016/j.fertnstert.2013.11.004
10. Macklon N. Recurrent implantation failure is a pathology with a specific transcriptomic signature. Fertil Steril. (2017) 108:9–14. doi: 10.1016/j.fertnstert.2017.05.028
11. Maged AM, Rashwan H, AbdelAziz S, Ramadan W, Mostafa WA, Metwally AA, et al. Randomized controlled trial of the effect of endometrial injury on implantation and clinical pregnancy rates during the first ICSI cycle. Int J Gynaecol Obstetrics. (2018) 140:211–6. doi: 10.1002/ijgo.12355
12. Glujovsky D, Farquhar C, Quinteiro Retamar AM, Alvarez Sedo CR, Blake D. Cleavage stage versus blastocyst stage embryo transfer in assisted reproductive technology. Cochrane Database Sys Rev. (2016) 6):Cd002118. doi: 10.1002/14651858.CD002118.pub5
13. Bienert M, Habib P, Buck V, Classen-Linke I, Skoblo R, Rösing B, et al. Intrauterine hCG application increases expression of endothelial cell-cell adhesion molecules in human. Arch Gynecol Obstetrics. (2021) 304:1587–97. doi: 10.1007/s00404-021-06031-9
14. Tang CL, Li QY, Chen FL, Cai CT, Dong YY, Wu YY, et al. A randomized double blind comparison of atosiban in patients with recurrent implantation failure undergoing IVF treatment. Reprod Biol Endocrinol RB&E. (2022) 20:124. doi: 10.1186/s12958-022-00999-y
15. Caglar GS, Asimakopoulos B, Nikolettos N, Diedrich K, Al-Hasani S. Preimplantation genetic diagnosis for aneuploidy screening in repeated implantation failure. Reprod Biomed online. (2005) 10:381–8. doi: 10.1016/S1472-6483(10)61800-7
16. Mekinian A, Cohen J, Alijotas-Reig J, Carbillon L, Nicaise-Roland P, Kayem G, et al. Unexplained recurrent miscarriage and recurrent implantation failure: is there a place for immunomodulation? Am J Reprod Immunol (New York NY 1989). (2016) 76:8–28. doi: 10.1111/aji.12493
17. Bussolino F, Wang JM, Defilippi P, Turrini F, Sanavio F, Edgell CJ, et al. Granulocyte- and granulocyte-macrophage-colony stimulating factors induce human endothelial cells to migrate and proliferate. Nature. (1989) 337:471–3. doi: 10.1038/337471a0
18. Zhao Y, Rong H, Chegini N. Expression and selective cellular localization of granulocyte-macrophage colony-stimulating factor (GM-CSF) and GM-CSF alpha and beta receptor messenger ribonucleic acid and protein in human ovarian tissue. Biol Reproduction. (1995) 53:923–30. doi: 10.1095/biolreprod53.4.923
19. Salmassi A, Schmutzler AG, Huang L, Hedderich J, Jonat W, Mettler L. Detection of granulocyte colony-stimulating factor and its receptor in human follicular luteinized granulosa cells. Fertil Steril. (2004) 81 Suppl 1:786–91. doi: 10.1016/j.fertnstert.2003.09.039
20. Uzumaki H, Okabe T, Sasaki N, Hagiwara K, Takaku F, Tobita M, et al. Identification and characterization of receptors for granulocyte colony-stimulating factor on human placenta and trophoblastic cells. Proc Natl Acad Sci United States America. (1989) 86:9323–6. doi: 10.1073/pnas.86.23.9323
21. Cai L, Jeon Y, Yoon JD, Hwang SU, Kim E, Park KM, et al. The effects of human recombinant granulocyte-colony stimulating factor treatment during in vitro maturation of porcine oocyte on subsequent embryonic development. Theriogenol. (2015) 84:1075–87. doi: 10.1016/j.theriogenology.2015.06.008
22. Moldenhauer LM, Keenihan SN, Hayball JD, Robertson SA. GM-CSF is an essential regulator of T cell activation competence in uterine dendritic cells during early pregnancy in mice. J Immunol (Baltimore Md 1950). (2010) 185:7085–96. doi: 10.4049/jimmunol.1001374
23. Scarpellini F, Sbracia M. Use of granulocyte colony-stimulating factor for the treatment of unexplained recurrent miscarriage: a randomised controlled trial. Hum Reprod (Oxford England). (2009) 24:2703–8. doi: 10.1093/humrep/dep240
24. Gleicher N, Vidali A, Barad DH. Successful treatment of unresponsive thin endometrium. Fertil Steril. (2011) 95:2123.e13–7. doi: 10.1016/j.fertnstert.2011.01.143
25. Gleicher N, Kim A, Michaeli T, Lee HJ, Shohat-Tal A, Lazzaroni E, et al. A pilot cohort study of granulocyte colony-stimulating factor in the treatment of unresponsive thin endometrium resistant to standard therapies. Hum Reprod (Oxford England). (2013) 28:172–7. doi: 10.1093/humrep/des370
27. Aleyasin A, Abediasl Z, Nazari A, Sheikh M. Granulocyte colony-stimulating factor in repeated IVF failure, a randomized trial. Reprod (Cambridge England). (2016) 151:637–42. doi: 10.1530/REP-16-0046
28. Kalem Z, Namli Kalem M, Bakirarar B, Kent E, Makrigiannakis A, Gurgan T. Intrauterine G-CSF administration in recurrent implantation failure (RIF): an rct. Sci Rep. (2020) 10:5139. doi: 10.1038/s41598-020-61955-7
29. Kamath MS, Chittawar PB, Kirubakaran R, Mascarenhas M. Use of granulocyte-colony stimulating factor in assisted reproductive technology: A systematic review and meta-analysis. Eur J Obstetrics Gynecol Reprod Biol. (2017) 214:16–24. doi: 10.1016/j.ejogrb.2017.04.022
30. Hou Z, Jiang F, Yang J, Liu Y, Zha H, Yang X, et al. What is the impact of granulocyte colony-stimulating factor (G-CSF) in subcutaneous injection or intrauterine infusion and during both the fresh and frozen embryo transfer cycles on recurrent implantation failure: a systematic review and meta-analysis? Reprod Biol Endocrinol RB&E. (2021) 19:125. doi: 10.1186/s12958-021-00810-4
31. Arefi S, Fazeli E, Esfahani M, Borhani N, Yamini N, Hosseini A, et al. Granulocyte-colony stimulating factor may improve pregnancy outcome in patients with history of unexplained recurrent implantation failure: An RCT. Int J Reprod Biomed. (2018) 16:299–304. doi: 10.29252/ijrm.16.5.299
32. Bakry MS, Eldesouky E, Alghazaly MM, Farag E, Sultan EEK, Elazzazy H, et al. Granulocyte colony stimulating factor versus human chorionic gonadotropin for recurrent implantation failure in intra cytoplasmic sperm injection: a randomized clinical trial. BMC Pregnancy Childbirth. (2022) 22:881. doi: 10.1186/s12884-022-05098-9
33. Davari-Tanha F, Shahrokh Tehraninejad E, Ghazi M, Shahraki Z. The role of G-CSF in recurrent implantation failure: A randomized double blind placebo control trial. Int J Reprod Biomed. (2016) 14:737–42.
34. Eftekhar M, Miraj S, Farid Mojtahedi M, Neghab N. Efficacy of Intrauterine infusion of granulocyte colony stimulating factor on patients with history of implantation failure: A randomized control trial. Int J Reprod Biomed. (2016) 14:687–90. doi: 10.29252/ijrm.14.11.687
35. Huang P, Yao C, Wei L, Lin Z. The intrauterine perfusion of granulocyte-colony stimulating factor (G-CSF) before frozen-thawed embryo transfer in patients with two or more implantation failures. Hum Fertil (Cambridge England). (2020) 31:1–5. doi: 10.1080/14647273.2020.1811904
36. Karimi A, Mokhtar S, Sadeghi MR, Zafardoust S, Ataei M, Ghoodjani A, et al. May intrauterine granulocyte colony stimulating factor improve clinical & ongoing pregnancy & live birth rates in unexplained repeated implantation failure patients? A Randomized Clinical Trial. Eur J Mol Clin Med. (2020) 7:82–7.
37. Torky H, El-Desouky ES, El-Baz A, Aly R, El-Taher Q, Shata A, et al. Effect of intra uterine granulocyte colony stimulating factor vs. human chorionic gonadotropin at ovum pick up day on pregnancy rate in IVF/ICSI cases with recurrent implantation failure. JBRA Assisted Reproduction. (2022) 26(2):274–9. doi: 10.5935/1518-0557.20210056
38. Rezaei Z, Adabi K, Sadjadi A. A comparison of endometrial thickness and pregnancy outcomes in two methods of intrauterine injection and subcutaneous injection of gcsf in infertile women candidates for ivf. J Obstetrics Gynecol Cancer Res. (2020) 5:39–43. doi: 10.30699/jogcr.5.2.39
39. Liu KE, Hartman M, Hartman A, Luo ZC, Mahutte N. The impact of a thin endometrial lining on fresh and frozen-thaw IVF outcomes: an analysis of over 40 000 embryo transfers. Hum Reprod (Oxford England). (2018) 33:1883–8. doi: 10.1093/humrep/dey281
40. von Wolff M, Fäh M, Roumet M, Mitter V, Stute P, Griesinger G, et al. Thin endometrium is also associated with lower clinical pregnancy rate in unstimulated menstrual cycles: A study based on natural cycle IVF. Front Endocrinol. (2018) 9:776. doi: 10.3389/fendo.2018.00776
41. Correa-de-Araujo R, Yoon SSS. Clinical outcomes in high-risk pregnancies due to advanced maternal age. J Women's Health (2002). (2021) 30:160–7. doi: 10.1089/jwh.2020.8860
42. Attali E, Yogev Y. The impact of advanced maternal age on pregnancy outcome. Best Pract Res Clin Obstetrics Gynaecol. (2021) 70:2–9. doi: 10.1016/j.bpobgyn.2020.06.006
43. Xie Y, Zhang T, Tian Z, Zhang J, Wang W, Zhang H, et al. Efficacy of intrauterine perfusion of granulocyte colony-stimulating factor (G-CSF) for Infertile women with thin endometrium: A systematic review and meta-analysis. Am J Reprod Immunol (New York NY 1989). (2017) 78. doi: 10.1111/aji.12701
44. Sar-Shalom Nahshon C, Sagi-Dain L, Wiener-Megnazi Z, Dirnfeld M. The impact of intentional endometrial injury on reproductive outcomes: a systematic review and meta-analysis. Hum Reprod Update. (2019) 25:95–113. doi: 10.1093/humupd/dmy034
45. Mona R, Marie P, Sylvie D, Bensussan A, Chaouat G, Ledee N. Granulocyte-colony stimulating factor related pathways tested on an endometrial ex-vivo model. PloS One. (2014) 9(9):e102286. doi: 10.1371/journal.pone.0102286
Keywords: granulocyte colony-stimulating factor, implantation failure, in vitro fertilization, intracytoplasmic sperm injection, pregnancy outcome
Citation: Su Q, Pan Z, Yin R and Li X (2024) The value of G-CSF in women experienced at least one implantation failure: a systematic review and meta-analysis. Front. Endocrinol. 15:1370114. doi: 10.3389/fendo.2024.1370114
Received: 13 January 2024; Accepted: 22 March 2024;
Published: 16 April 2024.
Edited by:
Diego Raimondo, University of Bologna, ItalyCopyright © 2024 Su, Pan, Yin and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhuo Pan, cGFuOTl6aHVvQDE2My5jb20=