 Diliyaer Dilixiati1†
Diliyaer Dilixiati1† Alapati Waili2†
Alapati Waili2† Aizihaier Tuerxunmaimaiti3
Aizihaier Tuerxunmaimaiti3 Liwen Tao2
Liwen Tao2 Abudureheman Zebibula1*Mulati Rexiati1*
Abudureheman Zebibula1*Mulati Rexiati1*- 1Department of Urology, First Affiliated Hospital of Xinjiang Medical University, Urumqi, China
- 2Department of Pancreatic Surgery, First Affiliated Hospital of Xinjiang Medical University, Urumqi, China
- 3Department of Cardiac Surgery, First Affiliated Hospital of Xinjiang Medical University, Urumqi, China
Background: Previous studies have established that diabetes mellitus (DM) markedly raises the risk of developing erectile dysfunction (ED). Despite extensive investigations, the risk factors associated with ED in diabetic men have yet to be unequivocally determined, owing to incongruent and inconclusive results reported in various studies.
Objective: The objective of this systematic review and meta-analysis was to assess the risk factors for ED in men with DM.
Methods: A comprehensive systematic review was conducted, encompassing studies published in the PubMed, Scopus and Embase databases up to August 24th, 2023. All studies examining the risk factors of ED in patients with DM were included in the analysis. To identify significant variations among the risk factors, odds ratios (ORs) and their corresponding 95% confidence intervals (CIs) were employed. The risk of bias was evaluated using the Newcastle-Ottawa Scale(NOS) for longitudinal studies and the Agency for Healthcare Research and Quality Scale(AHRQ) for cross-sectional studies.
Results: A total of 58 studies, including a substantial participant pool of 66,925 individuals diagnosed with DM, both with or without ED, were included in the meta-analysis. Mean age (OR: 1.31, 95% CI=1.24-1.37), smoking status (OR: 1.32, 95% CI=1.18-1.47), HbA1C (OR: 1.44, 95% CI=1.28-1.62), duration of DM (OR: 1.39, 95% CI=1.29-1.50), diabetic neuropathy (OR: 3.47, 95% CI=2.16-5.56), diabetic retinopathy (OR: 3.01, 95% CI=2.02-4.48), diabetic foot (OR: 3.96, 95% CI=2.87-5.47), cardiovascular disease (OR: 1.92, 95% CI=1.71-2.16), hypertension (OR: 1.74, 95% CI=1.52-2.00), microvascular disease (OR: 2.14, 95% CI=1.61-2.85), vascular disease (OR: 2.75, 95% CI=2.35-3.21), nephropathy (OR: 2.67, 95% CI=2.06-3.46), depression (OR: 1.82, 95% CI=1.04-3.20), metabolic syndrome (OR: 2.22, 95% CI=1.98-2.49), and diuretic treatment (OR: 2.42, 95% CI=1.38-4.22) were associated with increased risk factors of ED in men with DM.
Conclusion: Our study indicates that in men with DM, several risk factors for ED have been identified, including mean age, HbA1C, duration of DM, diabetic neuropathy, diabetic retinopathy, diabetic foot, cardiovascular disease, hypertension, microvascular disease, vascular disease, nephropathy, depression, metabolic syndrome, and diuretic treatment. By clarifying the connection between these risk factors and ED, clinicians and scientific experts can intervene and address these risk factors, ultimately reducing the occurrence of ED and improving patient management.
Introduction
Diabetes mellitus stands as a prevalent and formidable non-communicable disease that profoundly impacts the health and well-being of individuals, their families, and broader societies. DM represents a substantial global burden, exerting a significant impact on morbidity and mortality rates, and stands as the ninth leading cause of death worldwide (1). Epidemiological investigations have revealed a remarkable upsurge in the prevalence and mortality associated with DM from 2007 to 2017 (2). Projections suggest that by 2030, an estimated 10.2% of the global population will be affected by this chronic condition (3).
ED refers to the repetitive or persistent inability to attain and/or sustain an adequate level of erectile function required for satisfactory sexual intercourse (4). In individuals with DM, this condition typically emerges from the intricate interplay of neurogenic, vasogenic, and psychological factors, which are closely interlinked with the chronic complications related to DM (5). The prevalence of DM has rapidly increased due to higher consumption of high-sugar diets and decreased physical activity as a result of social development. The prevalence of ED among diabetic patients exhibits significant variation, spanning from 35% to 90% (6). Furthermore, in the United States, the total direct cost of evaluating ED treatment is estimated to be $400 million, with approximately a quarter of this amount linked to DM and obesity (7).
A recent study examined the association between DM and ED, treatment options, and diabetes-related ED, incorporating 106 relevant studies in the review (8). This extensive inclusion of studies highlights the widespread interest and significance of the association between DM and ED as a current and highly pertinent topic. Men with DM often contend with several comorbidities that serve as independent risk factors for ED, including advancing age, obesity, smoking, cardiovascular disease(CVD), hypertension, metabolic syndrome, and dyslipidemia (9, 10). In addition, the presence of diabetic complications such as diabetic retinopathy and diabetic foot can further precipitate the development of ED (5). The effects of ED reach far beyond physical symptoms, encompassing significant psychosocial and clinical implications. These implications are linked to men’s social interactions, emotional and psychological well-being, as well as their relationships with their partners. Nevertheless, it is important to highlight that ED stands as one of the most treatable complications of DM, with a success rate exceeding 95% in treatment outcomes (11).
ED is a prevalent complication of DM and high-quality meta-analyses and ED guidelines (12) have recognized DM as a significant risk factor. However, there remains a notable gap in the literature regarding a comprehensive analysis and synthesis of the various risk factors associated with ED in men affected by DM. Thus, we conducted a comprehensive exploration of the risk factors for ED in the diabetic population, aiming to furnish clinicians and preventive physicians with valuable insights for averting the onset of ED.
Materials and methods
This meta-analysis adheres to the 2020 guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (13). The study protocol has been registered with the international prospective register of systematic reviews (PROSPERO) under the registration number CRD42023495323.
Search strategy
A comprehensive systematic review was conducted, encompassing studies published in the PubMed, Scopus and Embase databases up to August 24th, 2023. Relevant studies derived from the references of the studies included in the initial search, along with significant reviews and systematic reviews pertinent to this field, were also comprehensively assessed to ensure comprehensive coverage of the literature. By utilizing a combination of medical subject heading (MeSH) terms and text words, we devised a preliminary search strategy that incorporated the following terms: “Diabet”; “insulin”; “resistance glucose”; “Intolerant”; “diabetes mellitus”; “T1DM”; “T2DM”; “Erectile Dysfunction”; “Impotence”. The comprehensive search strategy employed for all databases can be found in Supplementary Material 1.
Study selection criteria
Three researchers (AW, AT, and L-WT) independently assessed all articles for eligibility and cross-validated their findings. Any discrepancies were resolved through discussion or consultation with the senior authors (DD).The inclusion criteria for the selected articles were as follows: (1) diagnosis of DM was conducted by either a specialist clinician, a qualified health manager, or through analysis of database data adhering to internationally recognized diagnostic criteria. (2) studies investigating risk factors for ED in men with DM. (3) studies involving male participants aged 18 years or older, and publications in English, irrespective of study design(longitudinal or cross-sectional). And (4) any studies that provided OR, relative risks (RR), hazard ratios (HR) with 95% CIs, or sufficient data to facilitate the calculation of these values. The following exclusion criteria were applied: (1) no control group was established in the study; (2) reviews, letters, conference abstracts, case reports, case series, or editorials; (3) duplicates, animal studies, non-English articles, or articles for which full-text access could not be obtained were excluded. When multiple articles from a single study reported on the same endpoint, only the data representing the longest follow-up period were extracted. Furthermore, in studies that reported multivariate adjusted effects, we extracted results from models that controlled for the most significant potential confounders. In cases where studies did not report an effect result or where data could only be extracted from baseline, we computed the effect result using a fourfold table and defined the result as unadjusted.
Data extraction and quality assessment
Data extraction from each article was performed by three independent observers (AW, AT, and L-WT). Any discrepancies were resolved either by a third observer (DD) or through consensus among the observers. The extracted data included the first author’s name, year of publication, country of origin, study design, sample size, number of participants, mean age, ascertainment of DM and ED, type of DM, pharmaceutical treatments, outcomes, and other relevant factors.
The quality and methodological robustness of the included longitudinal studies were assessed by three researchers (AW, AT, and L-WT) using the Newcastle-Ottawa Scale (NOS) (14). As for the cross-sectional studies, these three researchers utilized the guidelines provided by the Agency for Healthcare Research and Quality (AHRQ) to evaluate their methodological rigor (15).
Statistical analyses
Data analysis was performed using STATA software version 12.0 (STATA Corporation, Texas, USA). The primary outcome of this study examines the risk factors for ED in diabetic patients, while the secondary outcome focuses on conducting subgroup analyses to stratify risk factors based on the type of DM, age, and other relevant factors. Given the substantial representation of cross-sectional studies, ORs were used as effect sizes, and findings from a combination of longitudinal and cross-sectional studies were integrated to enhance the generalizability of our study, drawing upon insights from previous research endeavors (16, 17). Additionally, we conducted separate subgroup analyses to rigorously examine the results of studies, thereby enhancing the robustness of our findings. Heterogeneity in the study was evaluated through Cochrane’s Q test and I2 statistics. The fixed-effect model was adopted when P ≥ 0.1 and I2 ≤ 50%, while the random-effect model was utilized for cases when P < 0.1 and I2 > 50%. Further subgroup analyses were conducted using a comprehensive dataset including more than 10 studies to investigate potential causes of heterogeneity. We conducted sensitivity analyses by excluding individual studies and assessing their impact on the overall pooled results. Furthermore, we performed funnel plot analysis and evaluated publication bias using the Egger tests. Statistical significance was defined as a p-value less than 0.05 for all two-sided statistical tests.
Results
The initial search involved a systematic review of a vast array of 7,885 studies, including 2,694 from PubMed, 2,496 from Scopus, and 2,666 from Embase. Furthermore, an additional 29 studies were identified through alternative sources. After the removal of 1,417 duplicated studies and the exclusion of an additional 4,504 based on the evaluation of their title and abstract content, a rigorous assessment was conducted on 1,964 studies for full-text evaluation. Finally, 58 articles met the criteria for inclusion in the meta-analysis and literature review. The process employed to identify eligible articles is depicted in Figure 1.
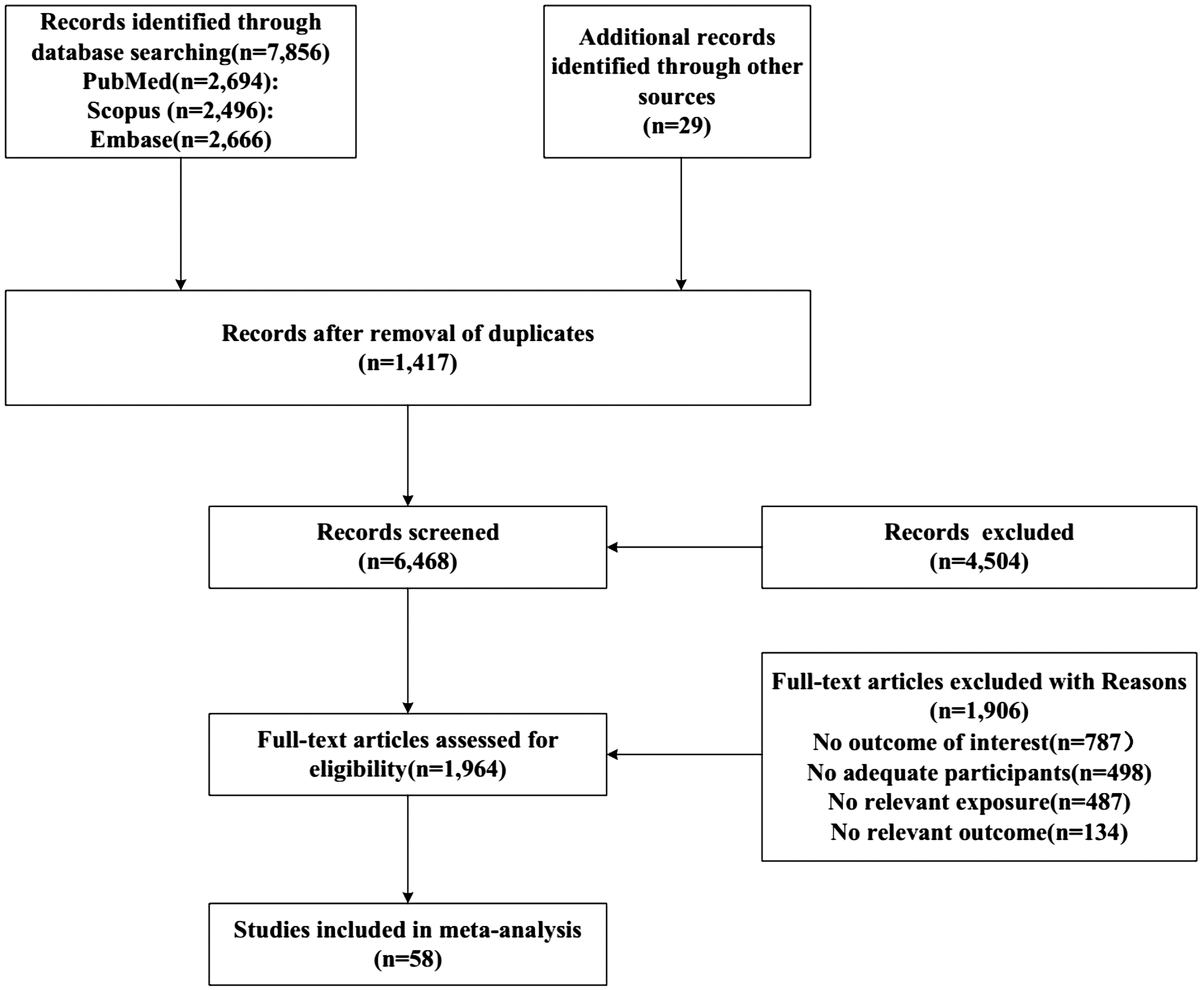
Figure 1 Flow chart of study selection.
Of the 58 studies ultimately included, a comprehensive analysis revealed a total of 37 identified risk factors, encompassing the following categories: demographic and lifestyle characteristics (mean age, BMI, weight, waist-to-hip ratio, alcohol consumption, smoking status, lower income, physical activity, sitting time); laboratory analyses (systolic blood pressure, low HDL cholesterol, estimated glomerular filtration rate, testosterone levels, Hemoglobin, microalbuminuria); diabetes-related complications (HbA1c levels, inadequate glycemic control, duration of DM, diabetic neuropathy, diabetic retinopathy, Diabetic foot); and medical history and symptomatology (CVD, hypertension, microvascular disease, vascular disease, nephropathy, depression, premature ejaculation, atherogenic dyslipidemia, reduced libido, metabolic syndrome, hyperuricemia, nocturia, cardiorespiratory fitness diuretics, ACE inhibitors, injectable insulin).
Study characteristics
During the conclusive analysis, 22 of the 37 identified risk factors were subjected to meta-analysis, indicating that they were each supported by a minimum of two included studies. As there was an insufficient number of eligible studies, a meta-analysis could not be conducted on the 15 risk factors. Therefore, Table 1 presents the raw data extracted from the individual articles that were included in this study. All included articles, spanning from 1996 to 2023, encompassed a total cohort of 66,925 participants. Among the studies, 9 were conducted in Europe, 26 in Asia, 10 in North America, 1 in South America, 2 in Oceania, and 10 in Africa. The mean age of subjects ranged from 18.0 to 78.8 years. Table 2 shows the characteristics of the included articles and the quality of each. Table 1 presents the results of a meta-analysis or original outcome analysis that evaluates the influence of 37 identified risk factors on the occurrence of ED in men with DM.
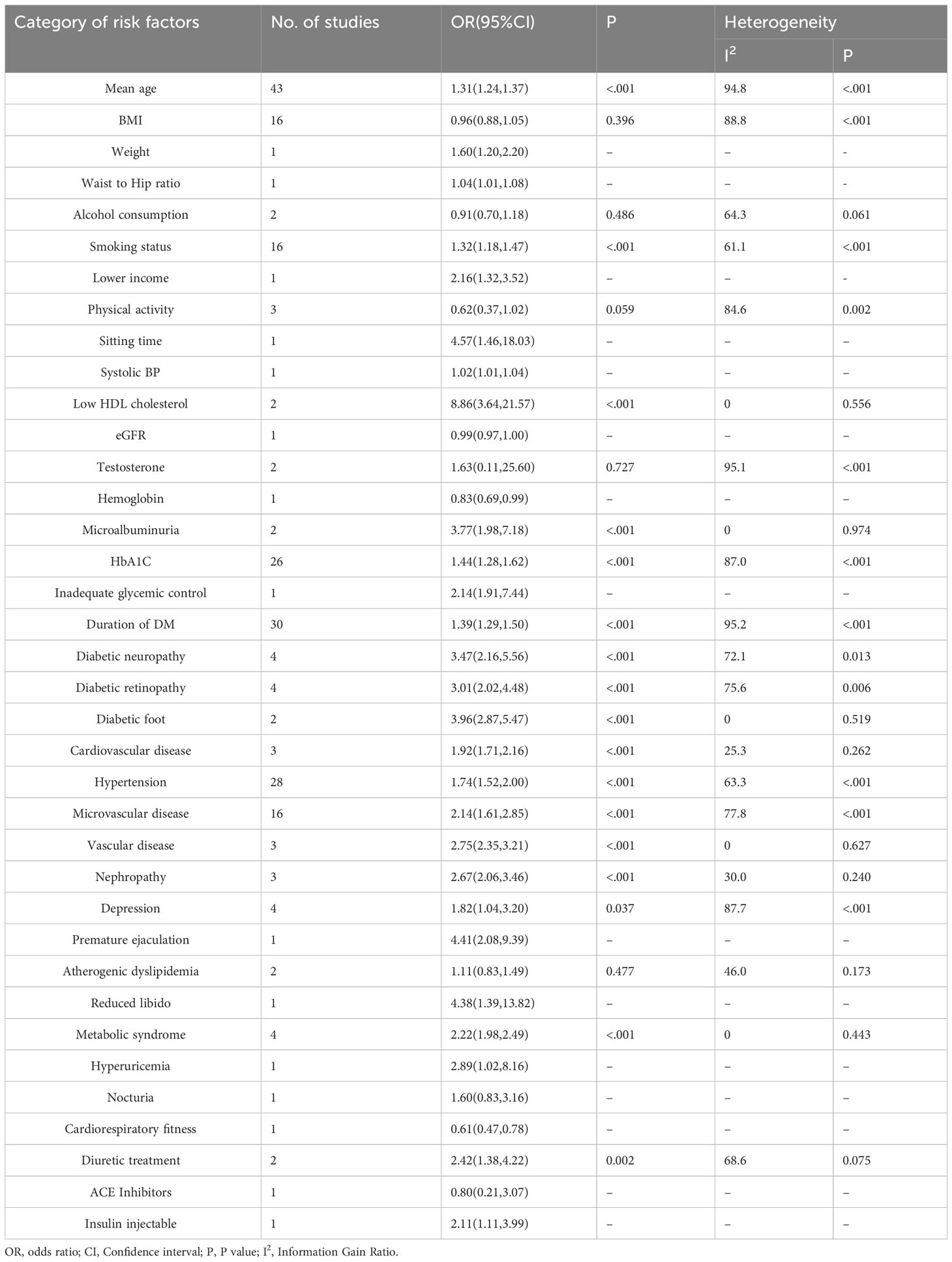
Table 1 Categorical analysis on the correlation between risk factors for erectile dysfunction and diabetes mellitus.
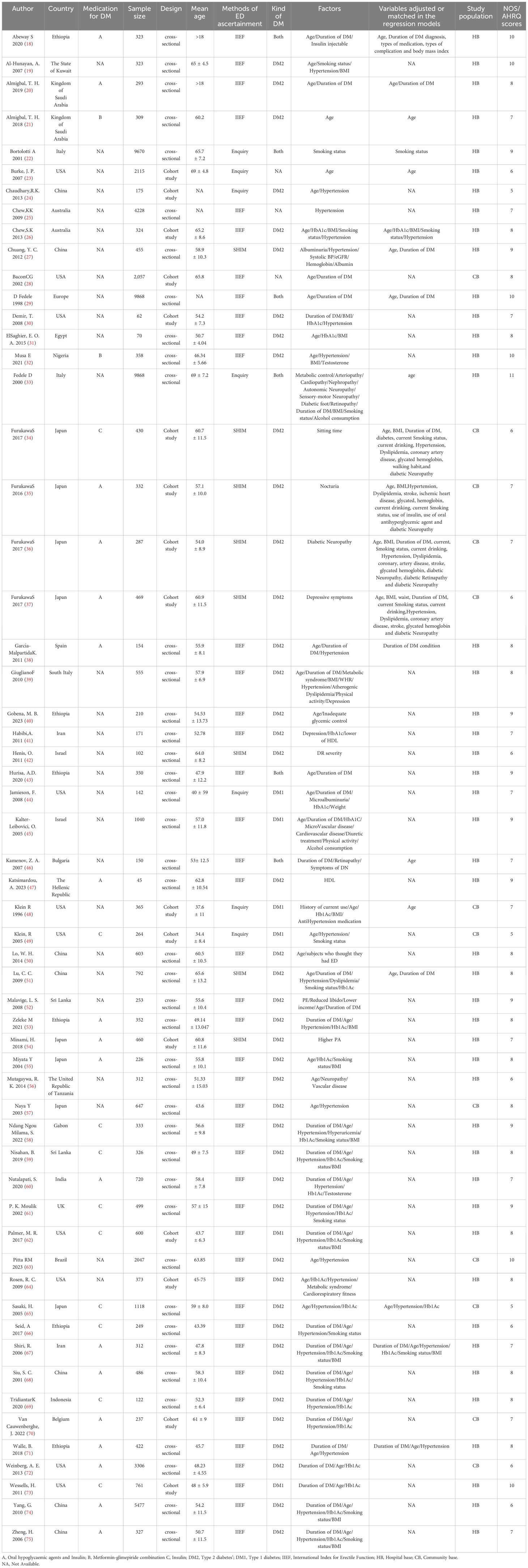
Table 2 Characteristics of studies included in the meta-analysis.
Demographic and lifestyle characteristics
The meta-analysis encompassed 43, 16, 2, 16, and 3 studies investigating the mean age, BMI, alcohol consumption, smoking status, and physical activity factors, respectively. Among these, mean age (OR: 1.31, 95% CI=1.24-1.37) and smoking status (OR: 1.32, 95% CI=1.18-1.47) were identified as significant risk factors, while BMI, alcohol consumption, and physical activity did not show significance(P ≥.05). Significant heterogeneity is present in both the mean age factor and smoking status factor(I2 = 94.8% and 64.1%, respectively). Furthermore, we observed a significant publication bias in relation to the mean age factor (Egger’s test: P <.001). However, when employing the trim and filling method, the results remained stable after applying the necessary adjustments. Additionally, the smoking status factor displayed no significant bias (Egger’s test: P = .631).The results of all meta-analyses involving demographic and lifestyle characteristics factors are presented in Supplementary Figures 1-12.
Laboratory analyses
low HDL cholesterol, testosterone, and microalbuminuria factors were analyzed in two separate articles for meta-analysis. The results revealed no significant heterogeneity between low HDL cholesterol and microalbuminuria factors(I2 = 0% and 0%, respectively), prompting the utilization of the fixed-effect model. This model yielded significant results, indicating that both low HDL cholesterol(OR: 8.86, 95% CI=3.64-21.57) and microalbuminuria(OR: 3.77, 95% CI=1.98-7.18) were substantial risk factors. However, no discernible association was found between testosterone and the occurrence of ED(P = .727). The results of all meta-analyses involving Laboratory analyses factors are presented in Supplementary Figures 13-15.
Diabetes-related complications
Meta-analyses were conducted on the factors of HbA1C(OR: 1.44, 95% CI=1.28-1.62), Duration of DM(OR: 1.39, 95% CI=1.29-1.50), Diabetic neuropathy(OR: 3.47, 95% CI=2.16-5.56), Diabetic retinopathy(OR: 3.01, 95% CI=2.02-4.48), and Diabetic foot(OR: 3.96, 95% CI=2.87-5.47), with a total of 26, 30, 4, 4, and 2 studies included, respectively. The findings demonstrated that these factors were substantiated as risk factors associated with an increased occurrence of ED in diabetic men. Significant heterogeneity was detected among the factors of HbA1C, Duration of DM, Diabetic neuropathy, and Diabetic retinopathy(I2 = 87.0%, 95.2%,72.1% and 75.6%, respectively), while no significant heterogeneity was observed for the Diabetic foot factor(I2 = 0%). Evidence of publication bias was identified in the studies examining the HbA1C and Duration of DM factors, as indicated by the results of the Egger’s test (P = 0.024, <.001, respectively). However, when employing the trim and filling method, the results remained stable after applying the necessary adjustments. The results of all meta-analyses involving Diabetes-related complications factors are presented in Supplementary Figures 16-26.
Medical history and symptomatology
The meta-analysis conducted on CVD(OR: 1.92, 95% CI=1.71-2.16), hypertension(OR: 1.74, 95% CI=1.52-2.00), microvascular disease(OR: 2.14, 95% CI=1.61-2.85), vascular disease(OR: 2.75, 95% CI=2.35-3.21), nephropathy(OR: 2.67, 95% CI=2.06-3.46), depression(OR: 1.82, 95% CI=1.04-3.20), atherogenic dyslipidemia(OR: 2.22, 95% CI=1.98-2.49), metabolic syndrome(OR: 2.22, 95% CI=1.98-2.49), and diuretic treatment(OR: 2.42, 95% CI=1.38-4.22) revealed that these factors pose a significant risk for ED in diabetic men. Analyses of factors such as hypertension, microvascular disease, depression, and diuretic treatment exhibited considerable heterogeneity(I2 = 63.3%, 77.8%,87.7% and 68.6%, respectively). Conversely, analyses of factors such as CVD, vascular disease, nephropathy, atherogenic dyslipidemia, and metabolic syndrome demonstrated no significant heterogeneity. As a result, fixed-effect models were employed in these cases(I2 = 25.3%, 0%,30.0%, 46.0%, and 0%, respectively). No evidence of publication bias was detected in the results pertaining to the hypertension and microvascular disease factors(P = .527, = .296, respectively). The results of all meta-analyses involving medical history and symptomatology factors are presented in Supplementary Figures 26-38.
Subgroup analysis and sensitivity analyses
Ration could possibly serve as a contributing factor to the observed heterogeneity in BMI, HbA1C, and microvascular disease factors. Furthermore, the utilization of medication for DM may be a potential source of heterogeneity in the relationship between smoking status factors, hypertension factors, and the development of ED. Lastly, the study design employed could be a plausible source of heterogeneity in the associations between BMI, smoking status, and microvascular disease factors. Significantly, we observed a notably higher incidence of ED within the African subgroup of the diabetic population, particularly in relation to mean age(OR: 2.38, 95% CI=1.52-5.26), duration of DM(OR: 3.16, 95% CI=1.41-7.08), and hypertension(OR: 2.23, 95% CI=1.50-3.31) factors. In addition, sensitivity analysis showed that our findings were reliable.
Discussion
Our study, a Comprehensive Systematic Review and Meta-Analysis, has shed light on the multitude of risk factors associated with ED in men with DM. Notably, we have identified several key risk factors, including mean age, HbA1C levels, duration of DM, presence of diabetic neuropathy, retinopathy, foot complications, CVD, hypertension, microvascular complications, vascular disease, nephropathy, depression, metabolic syndrome, and diuretic treatment. Our findings significantly emphasize the heightened incidence of ED among individuals within the African subgroup of the diabetic population. Notably, mean age, duration of DM, and hypertension emerge as influential contributing factors to this phenomenon.
Heterogeneity was observed in the meta-analysis of certain factors, including mean age, smoking status, and others. To explore the potential sources of heterogeneity, we conducted subgroup analyses based on various parameters. In the subgroup analysis encompassing BMI, smoking status, HbA1C, hypertension, and microvascular disease factors, our observations indicate that heterogeneity in the meta-analysis results of these factors may stem from the subgroups of region, diabetes types, and study design. Regrettably, our analyses did not reveal a significant source of heterogeneity in the results of subgroup analyses regarding mean age and duration of DM factors. In the context of conducting a meta-analysis that encompasses a substantial number of studies, it is inevitable to encounter high heterogeneity. On one hand, the vast number of studies reflects the inclusion of diverse possibilities from various sources. On the other hand, in our pursuit of incorporating a comprehensive range of risk factors to provide a broader perspective, certain quality control measures had to be relaxed, which may have introduced heterogeneity due to the inclusion of lower-quality studies under less standardized study designs. We have acknowledged and outlined the limitations of our study, which detail the reasons behind the heterogeneity. Upon thorough examination of our data, we have identified the presence of publication bias in the meta-analysis pertaining to mean age, HbA1C, and duration of DM factors. To mitigate this issue, we firstly expanded our literature search to include not only mainstream academic databases but also gray literature, unpublished studies, and conference proceedings. Then, we used the trim and filling method to validate the results, which showed that the results were still stable after applying the necessary adjustments.
Our subgroup analysis revealed a significant increase in the incidence of ED among African subgroups of the diabetic population, particularly in relation to factors such as mean age (OR: 2.38, 95% CI = 1.52 – 5.26), duration of diabetes (OR: 3.16, 95% CI = 1.41 – 7.08), and hypertension (OR: 2.23, 95% CI = 1.50 – 3.31). Several factors contribute to this increased risk of ED in African populations. Firstly, the high prevalence of chronic diseases, including CVD and hypertension, along with infectious diseases like malaria and AIDS, in specific African regions, collectively contribute to the development of ED. These diseases pose a significant burden on African regions, exacerbating the incidence of ED (76). Furthermore, it is worth noting that certain regions experience a significant economic disparity when compared to developed regions in Europe and the US. This disparity has far-reaching implications, encompassing various aspects such as the quality of medical and healthcare services, education, and food safety (77). Previous studies have established a strong correlation between these factors and the prevalence of ED (78). Finally, cultural and social contexts also play a role in the higher risk of ED among African populations. In certain African cultures, male sexual competence is considered a symbol of honor and dignity. Consequently, men may experience anxiety and stress regarding their sexual ability, which can further affect their sexual function (79).
The relationship between DM and ED has garnered significant attention in the realm of ED-related research. Conducted as a comprehensive exploration of the medical and psychosocial factors associated with erectile dysfunction, the Massachusetts Male Aging Study uncovered a significant finding: diabetic patients exhibited a threefold age-adjusted likelihood of developing ED compared to non-diabetic patients (80). In 2017, Kouidrat et al. carried out an extensive meta-analysis consisting of 145 studies. The analysis revealed prevalence rates of 37.5%, 66.3%, and 57.7% for ED in individuals with type 1, type 2, and both types of diabetes, respectively (81). Recently, a review conducted by Giuseppe Defeudis and colleagues (82) on the definition and incidence of ED in patients with DM, the influence of DM complications and treatment on ED, served as inspiration for our study. Building upon this research, we employed more objective statistical tools to delve deeper into the distinct impact of these influencing factors on ED.
Advancing age is associated with a notable decline in organ function as well as reductions in male sex hormones. Additionally, the aging process often coincides with the simultaneous presence of other risk factors for ED. There exist misconceptions suggesting that advancing age leads to diminished sexual interest and desire. However, despite a reduction in sexual activity attributable to declining physical vigor associated with aging, engagement in sexual behavior remains prevalent among older demographics (83). In an epidemiological study carried out in the UK, results indicated that as many as 84.5% of men aged 60–69 years reported participating in sexual activity, while the percentage stood at 59.3% for men aged 70–79 years (84). Our study not only provides compelling evidence for this perspective, but our subgroup analysis also reveals a noteworthy finding: populations from Africa may exhibit a heightened susceptibility to the impact of advancing age on ED (Table 3).

Table 3 Subgroup analysis of the correlation between risk factors for erectile dysfunction and diabetes mellitus.
In contrast to prior research regarding risk factors for ED (85), our study identified that BMI does not significantly contribute to ED risk. Likewise, physical activity was found to have limited efficacy in mitigating the development of ED. On one hand, it is plausible that BMI may not accurately reflect the extent of obesity in individuals, and on the other hand, managing body size and fat content may not effectively reduce ED risk in diabetic individuals without adequate glycemic control. Our findings align with this interpretation, as they underscore the significance of diabetic complications and glycemic control in relation to ED (86). Notably, the influence of smoking on ED remains considerable, underscoring its ongoing relevance. Therefore, quitting smoking represents an effective strategy for preventing and managing ED, even among individuals with DM.
Sufficient levels of androgens are crucial for erectile function. Androgens act peripherally, influencing erectile mechanisms by upholding the integrity of penile structures and regulating vasodilation in the penis (87). Two comprehensive meta-analyses, encompassing 850 diabetic men and 2000 non-diabetic individuals (88), as well as 1,822 diabetic men and 10,009 non-diabetic individuals, revealed markedly lower total testosterone levels in diabetic men compared to controls (89). This association has been linked to reduced levels of sex hormone binding globulin in individuals with DM. Our findings indicate that testosterone may not be a significant risk factor, aligning with previous reviews by Corona et al. (90), which suggest that testosterone replacement improves sexual symptoms in patients with prediabetes or newly diagnosed DM, but not in subjects with established diabetes. This phenomenon is attributed to the masking effect of diabetes-related vascular disease and neuropathy on the impact of replacement therapy.
Our observations indicate that the risk of experiencing ED is more prominently associated with diabetic complications rather than the duration of diabetes itself. These findings suggest that the duration of DM should not be perceived as the sole determinant of ED, and that the key factors contributing to heightened risk are inadequate glycemic control and the development of complications stemming from suboptimal treatment approaches. A randomized controlled study substantiates our perspective, which examined the impact of intensive glucose control on the risk of subsequent ED in 280 men with a history of diabetes ranging from 1 to 15 years and minor complications. Those initially randomized to intensive glucose control demonstrated a significantly reduced risk of ED compared to the usual care group (OR 0.33; 95% CI 0.18, 0.60) (91).
Previous animal and human studies have demonstrated that glycemic control plays a crucial role in regulating levels of systemic testosterone and Derived Factor-1 alpha. Notably, diabetic animals and humans exhibited significantly reduced levels of these two factors, whereas glycemic control effectively reversed this decline. This finding suggests that maintaining proper glycemic control mitigates the risk of ED in diabetic individuals by improving endothelial damage and enhancing protective mechanisms (92).We regret to note that only one study has investigated the outcomes of poor glycemic control as a risk factor. Consequently, we were unable to conduct a meta-analysis on this aspect. However, it is inferred that individuals with complications may be more prone to also have poor glycemic control. In individuals with diabetic retinopathy, there is an up-regulation of pro-inflammatory cytokines, which also hasten the progression of atherosclerosis. This leads to compromised blood flow to penile arterioles. Moreover, diabetic retinopathy signifies a more severe peripheral nerve complication of diabetes, undeniably exerting a detrimental impact on the erectile nerve (26). Similarly, the development of diabetic neuropathy is intricately linked to the underlying processes of microangiopathy and neurotoxicity, which manifest through a multitude of mechanisms (93). These mechanisms encompass heightened oxidative stress, accumulation of advanced glycation end products, impaired axonal transport, elevated flow through the polyol pathway, and the resulting detrimental impact on vascular nerve injury (94).
Penile erection is a complex process that involves the intricate interplay of neurovascular and psychological factors, regulating the balance between cavernous smooth muscle contraction and relaxation (95). The etiology of ED encompasses organic factors (such as neurogenic, vasogenic, steroid-induced, and drug-induced) as well as psychological factors (96). Vascular diseases, including CVD, microvascular and peripheral vascular sclerosis, and injury, are recognized as the primary organic causes of ED (97), while psychogenic ED is primarily attributed to psychological factors, social interpersonal relationships, and psychiatric diseases, all of which can exacerbate the occurrence of psychogenic ED. Hyperglycemia is frequently linked to impaired vasodilator signals, excessive smooth muscle cell contraction, and venous occlusive disorders—all of which are mechanisms contributing to ED in patients with DM (98). In addition, prolonged hyperglycemia leads to elevated oxidative stress due to factors such as inflammation, heightened production of reactive oxygen species, hyperhomocysteinemia, and reduced cellular antioxidants (99). These effects may be exacerbated by the presence of additional risk factors associated with both organic and psychological causes of ED. Our findings strongly align with this perspective, and through our meta-analysis of medical histories, we consistently observed significant impact results.
In our review of current published literature, we have identified certain risk factors that were not addressed in our article. This was due to the fact that some studies did not align with our inclusion and exclusion criteria, and others were not designed for quantitative meta-analysis. It is important to note that despite their omission from our study, these risk factors are of significance. Specifically, we would like to highlight risk factors such as abdominal obesity (100); waist circumference (101);Hypogonadism (102); Cardiovascular medications (103) encompass a range of pharmacological interventions, such as angiotensin-converting enzyme (ACE) inhibitors, calcium channel blockers, beta-blockers, and diuretics (5) that were not covered in our analysis. We recommend that future high-quality longitudinal studies with wide-ranging scopes investigate the association of these factors with ED.
A notable strength of this study lies in its status as the most comprehensive meta-analysis to date examining the risk of ED in diabetic men. Initially, our study produced noteworthy findings in African subgroups with multiple risk factors. Nevertheless, to date, there is a lack of published studies stratified by different racial/ethnic populations to ascertain the impact of diverse demographics on the incidence of ED in diabetic men. Secondly, it is important to acknowledge the significant heterogeneity observed across several of our studies. While we have attempted to address this through subgroup analysis, it is vital to recognize the limitations inherent in our interpretation of these findings. Finally, the exclusive inclusion of English literature introduces the potential for selection bias, thereby possibly limiting the ability of certain studies to conduct meta-analyses and confining them to providing solely original data.
Conclusion
Our study indicates that in men with DM, several risk factors for ED have been identified, including mean age, HbA1C, duration of DM, diabetic neuropathy, diabetic retinopathy, diabetic foot, cardiovascular disease, hypertension, microvascular disease, vascular disease, nephropathy, depression, metabolic syndrome, and diuretic treatment. By clarifying the connection between these risk factors and ED, clinicians and scientific experts can intervene and address these risk factors, ultimately reducing the occurrence of ED and improving patient management.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethics statement
In our current study, we solely relied on publicly accessible summary studies, and ethical approval as well as consent from participants were obtained through the original studies.
Author contributions
DD: Conceptualization, Investigation, Methodology, Resources, Writing – original draft. AW: Investigation, Methodology, Resources, Writing – original draft. AT: Investigation, Methodology, Resources, Writing – original draft. LWT: Investigation, Methodology, Resources, Writing – original draft. AZ: Conceptualization, Funding acquisition, Supervision, Writing – review & editing. MR: Conceptualization, Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by Xinjiang Uygur Autonomous Region Regional Collaborative Innovation Special Science and Technology Assistance Program FOUNDATION(No.2022E02129); National Natural Science Foundation of China (NSFC 82260139).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2024.1368079/full#supplementary-material
References
1. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of type 2 diabetes - global burden of disease and forecasted trends. J Epidemiol Glob Health. (2020) 10:107–11. doi: 10.2991/jegh.k.191028.001
2. GBD. 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. (2016) 388:1545–602. doi: 10.1016/S0140-6736(16)31678-6
3. Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. (2019) 157:107843. doi: 10.1016/j.diabres.2019.107843
4. Pellegrino F, Sjoberg DD, Tin AL, Benfante NE, Briganti A, Montorsi F, et al. Relationship between age, comorbidity, and the prevalence of erectile dysfunction. Eur Urol Focus. (2023) 9:162–7. doi: 10.1016/j.euf.2022.08.006
5. Maiorino MI, Bellastella G, Esposito K. Diabetes and sexual dysfunction: current perspectives. Diabetes Metab Syndr Obes. (2014) 7:95–105. doi: 10.2147/DMSO.S36455
6. Malavige LS, Levy JC. Erectile dysfunction in diabetes mellitus. J Sex Med. (2009) 6:1232–47. doi: 10.1111/j.1743-6109.2008.01168.x
7. Saigal CS, Wessells H, Pace J, Schonlau M, Wilt TJ, Urologic Diseases in America Project. Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch Intern Med. (2006) 166:207–12. doi: 10.1001/archinte.166.2.207
8. Akter S, Choubey M, Arbee S, Mohib MM, Tirumalasetty MB, Minhaz N, et al. Safeguarding intimate health: decoding the interplay of diabetes and erectile dysfunction. Preprints. (2023). doi: 10.20944/preprints202308.1440.v1
9. Esposito K, Giugliano D, Nappo F, Marfella R, Campanian Postprandial Hyperglycemia Study Group. Regression of carotid atherosclerosis by control of postprandial hyperglycemia in type 2 diabetes mellitus. Circulation. (2004) 110:214–9. doi: 10.1161/01.CIR.0000134501.57864.66
10. De Angelis L, Marfella MA, Siniscalchi M, Marino L, Nappo F, Giugliano F, et al. Erectile and endothelial dysfunction in Type II diabetes: a possible link. Diabetologia. (2001) 44:1155–60. doi: 10.1007/s001250100616
11. McMahon CG. Current diagnosis and management of erectile dysfunction. Med J Aust. (2019) 210:469–76. doi: 10.5694/mja2.50167
12. Salonia A, Bettocchi C, Boeri L, Capogrosso P, Carvalho J, Cilesiz NC, et al. European association of urology guidelines on sexual and reproductive health-2021 update: male sexual dysfunction. Eur Urol. (2021) 80:333–57. doi: 10.1016/j.eururo.2021.06.007
13. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
14. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–5. doi: 10.1007/s10654-010-9491-z
15. Shekelle PG, Ortiz E, Rhodes S, Morton SC, Eccles MP, Grimshaw JM, et al. Validity of the Agency for Healthcare Research and Quality clinical practice guidelines: how quickly do guidelines become outdated? JAMA. (2001) 286:1461–7. doi: 10.1001/jama.286.12.1461
16. Alon L, Corica B, Raparelli V, Cangemi R, Basili S, Proietti M, et al. Risk of cardiovascular events in patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis. Eur J Prev Cardiol. (2022) 29:938–46. doi: 10.1093/eurjpc/zwab212
17. Fu X, Xu J, Zhang R, Yu J. The association between environmental endocrine disruptors and cardiovascular diseases: A systematic review and meta-analysis. Environ Res. (2020) 187:109464. doi: 10.1016/j.envres.2020.109464
18. Abeway S, Dagne K, Zegeye T. Erectile dysfunction and correlates among diabetic men at dessie referral hospital: North Central Ethiopia, 2020. Diabetes Metab Syndr Obes. (2020) 13:4201–8. doi: 10.2147/DMSO.S278384
19. Al-Hunayan A, Al-Mutar M, Kehinde EO, Thalib L, Al-Ghorory M. The prevalence and predictors of erectile dysfunction in men with newly diagnosed with type 2 diabetes mellitus. BJU Int. (2007) 99:130–4. doi: 10.1111/j.1464-410X.2006.06550.x
20. Almigbal TH. Erectile dysfunction in men with type 2diabetes: ls it associated with poor glycemic control? J Men’s Health. (2019) 15:12–22. doi: 10.22374/jomh.v15i1.104
21. Almigbal TH, Schattner P. The willingness of Saudi men with type 2 diabetes to discuss erectile dysfunction with their physicians and the factors that influence this. PloS One. (2018) 13:e0201105. doi: 10.1371/journal.pone.0201105
22. Bortolotti A, Fedele D, Chatenoud L, Colli E, Coscelli C, Landoni M, et al. Cigarette smoking: a risk factor for erectile dysfunction in diabetics. Eur Urol. (2001) 40:392–6. doi: 10.1159/000049805
23. Burke JP, Jacobson DJ, McGree ME, Nehra A, Roberts RO, Girman CJ, et al. Diabetes and sexual dysfunction: results from the Olmsted County study of urinary symptoms and health status among men. J Urol. (2007) 177:1438–42. doi: 10.1016/j.juro.2006.11.059
24. Chaudhary RK, Shamsi BH, Tan T, Chen H-M, Xing J-P. Study of the relationship between male erectile dysfunction and type 2 diabetes mellitus/metabolic syndrome and its components. J Int Med Res. (2016) 44:735–41. doi: 10.1177/0300060515623122
25. Chew K-K, Bremner A, Stuckey B, Earle C, Jamrozik K. Sex life after 65: how does erectile dysfunction affect ageing and elderly men? Aging Male. (2009) 12:41–6. doi: 10.1080/13685530802273400
26. Chew SKH, Taouk Y, Xie J, Nicolaou TE, Wang JJ, Wong TY, et al. Relationship between diabetic retinopathy, diabetic macular oedema and erectile dysfunction in type 2 diabetics. Clin Exp Ophthalmol. (2013) 41:683–9. doi: 10.1111/ceo.12099
27. Chuang Y-C, Chung M-S, Wang P-W, Lee W-C, Chen C-D, Chang H-W, et al. Albuminuria is an independent risk factor of erectile dysfunction in men with type 2 diabetes. J Sex Med. (2012) 9:1055–64. doi: 10.1111/j.1743-6109.2011.02586.x
28. Bacon CG, Hu FB, Giovannucci E, Glasser DB, Mittleman MA, Rimm EB. Association of type and duration of diabetes with erectile dysfunction in a large cohort of men. Diabetes Care. (2002) 25:1458–63. doi: 10.2337/diacare.25.8.1458
29. Fedele D, Coscelli C, Santeusanio F, Bortolotti A, Chatenoud L, Colli E, et al. Erectile dysfunction in diabetic subjects in Italy. Gruppo Italiano Studio Deficit Erettile nei Diabetici. Diabetes Care. (1998) 21:1973–7. doi: 10.2337/diacare.21.11.1973
30. Demir T, Cömlekci A, Demir O, Gülcü A, Caliskan S, Argun L, et al. A possible new risk factor in diabetic patients with erectile dysfunction: homocysteinemia. J Diabetes Complications. (2008) 22:395–9. doi: 10.1016/j.jdiacomp.2007.04.001
31. El Saghier EO, Shebl SE, Fawzy OA, Eltayeb IM, Bekhet LM, Gharib A. Androgen deficiency and erectile dysfunction in patients with type 2 diabetes. Clin Med Insights Endocrinol Diabetes. (2015) 8:55–62. doi: 10.4137/CMED.S27700
32. Musa E, El-Bashir JM, Sani-Bello F, Bakari AG. Clinical and biochemical correlates of hypogonadism in men with type 2 diabetes mellitus. Pan Afr Med J. (2021) 38:292. doi: 10.11604/pamj.2021.38.292.25719
33. Fedele D, Bortolotti A, Coscelli C, Santeusanio F, Chatenoud L, Colli E, et al. Erectile dysfunction in type 1 and type 2 diabetics in Italy. On behalf of Gruppo Italiano Studio Deficit Erettile nei Diabetici. Int J Epidemiol. (2000) 29:524–31. doi: 10.1093/intjepid/29.3.524
34. Furukawa S, Sakai T, Niiya T, Miyaoka H, Miyake T, Yamamoto S, et al. Self-reported sitting time and prevalence of erectile dysfunction in Japanese patients with type 2 diabetes mellitus: The Dogo Study. J Diabetes Complications. (2017) 31:53–7. doi: 10.1016/j.jdiacomp.2016.10.011
35. Furukawa S, Sakai T, Niiya T, Miyaoka H, Miyake T, Yamamoto S, et al. Nocturia and prevalence of erectile dysfunction in Japanese patients with type 2 diabetes mellitus: The Dogo Study. J Diabetes Investig. (2016) 7:786–90. doi: 10.1111/jdi.12503
36. Furukawa S, Sakai T, Niiya T, Miyaoka H, Miyake T, Yamamoto S, et al. Diabetic peripheral neuropathy and prevalence of erectile dysfunction in Japanese patients aged <65 years with type 2 diabetes mellitus: The Dogo Study. Int J Impot Res. (2017) 29:30–4. doi: 10.1038/ijir.2016.40
37. Furukawa S, Sakai T, Niiya T, Miyaoka H, Miyake T, Yamamoto S, et al. Depressive symptoms and prevalence of erectile dysfunction in Japanese patients with type 2 diabetes mellitus: the Dogo Study. Int J Impot Res. (2017) 29:57–60. doi: 10.1038/ijir.2016.45
38. García-Malpartida K, Mármol R, Jover A, Gómez-Martínez MJ, Solá-Izquierdo E, Victor VM, et al. Relationship between erectile dysfunction and silent myocardial ischemia in type 2 diabetic patients with no known macrovascular complications. J Sex Med. (2011) 8:2606–16. doi: 10.1111/j.1743-6109.2011.02365.x
39. Giugliano F, Maiorino MI, Bellastella G, Autorino R, De Sio M, Giugliano D, et al. Adherence to Mediterranean diet and erectile dysfunction in men with type 2 diabetes. J Sex Med. (2010) 7:1911–7. doi: 10.1111/j.1743-6109.2010.01713.x
40. Gobena MB, Abdosh T, Dheresa M, Dechasa DB. Erectile dysfunction and associated factors among patients with diabetes attending follow-up at a public hospital, Harar, Eastern Ethiopia. A cross-sectional study design. Front Endocrinol (Lausanne). (2023) 14:1131555. doi: 10.3389/fendo.2023.1131555
41. Habibi A, Kalbasi S, Saadatjoo SA, Arefi MG. Evaluation of erectile dysfunction and associated factors in type-II diabetic patients in birjand, Iran in 2008-2009. J Res Health Sci. (2011) 11:97–102.
42. Henis O, Shahar Y, Steinvil A, Finn T, Heruti R, Loewenstein A, et al. Erectile dysfunction is associated with severe retinopathy in diabetic men. Urology. (2011) 77:1133–6. doi: 10.1016/j.urology.2011.01.009
43. Hurisa AD, Negera GZ. Erectile dysfunction among diabetic patients in a tertiary hospital of Southwest Ethiopia. Open Public Health J. (2020) 13:240–5. doi: 10.2174/1874944502013010240
44. Jamieson F, Chalmers J, Duncan C, Prescott RJ, Campbell IW. Erectile dysfunction in type 1 diabetic males. Br J Diabetes Vasc Dis. (2008) 8:232–4. doi: 10.1177/1474651408094536
45. Kalter-Leibovici O, Wainstein J, Ziv A, Harman-Bohem I, Murad H, Raz I, et al. Clinical, socioeconomic, and lifestyle parameters associated with erectile dysfunction among diabetic men. Diabetes Care. (2005) 28:1739–44. doi: 10.2337/diacare.28.7.1739
46. Kamenov ZA, Christov VG, Yankova TM. Erectile dysfunction in diabetic men is linked more to microangiopathic complications and neuropathy than to macroangiopathic disturbances. J Men’s Health Gender. (2007) 4:64–73. doi: 10.1016/j.jmhg.2006.12.004
47. Katsimardou A, Patoulias D, Zografou I, Siskos F, Stavropoulos K, Imprialos K, et al. The impact of metabolic syndrome components on erectile function in patients with type 2 diabetes. Metabolites. (2023) 13:617. doi: 10.3390/metabo13050617
48. Klein R, Klein BE, Lee KE, Moss SE, Cruickshanks KJ. Prevalence of self-reported erectile dysfunction in people with long-term IDDM. Diabetes Care. (1996) 19:135–41. doi: 10.2337/diacare.19.2.135
49. Klein R, Klein BEK, Moss SE. Ten-year incidence of self-reported erectile dysfunction in people with long-term type 1 diabetes. J Diabetes Complications. (2005) 19:35–41. doi: 10.1016/j.jdiacomp.2003.12.005
50. Lo WH, Fu SN, Wong CKH, Chen ES. Prevalence, correlates, attitude and treatment seeking of erectile dysfunction among type 2 diabetic Chinese men attending primary care outpatient clinics. Asian J Androl. (2014) 16:755–60. doi: 10.4103/1008-682X.127823
51. Lu C-C, Jiann B-P, Sun C-C, Lam H-C, Chu C-H, Lee J-K. Association of glycemic control with risk of erectile dysfunction in men with type 2 diabetes. J Sex Med. (2009) 6:1719–28. doi: 10.1111/j.1743-6109.2009.01219.x
52. Malavige LS, Jayaratne SD, Kathriarachchi ST, Sivayogan S, Fernando DJ, Levy JC. Erectile dysfunction among men with diabetes is strongly associated with premature ejaculation and reduced libido. J Sex Med. (2008) 5:2125–34. doi: 10.1111/j.1743-6109.2008.00907.x
53. Zeleke M, Hailu D, Daka D. Erectile dysfunction and associated factors among diabetic patients at, Hawassa, Southern, Ethiopia. BMC Endocr Disord. (2021) 21:139. doi: 10.1186/s12902-021-00807-5
54. Minami H, Furukawa S, Sakai T, Niiya T, Miyaoka H, Miyake T, et al. Physical activity and prevalence of erectile dysfunction in Japanese patients with type 2 diabetes mellitus: The Dogo Study. J Diabetes Investig. (2018) 9:193–8. doi: 10.1111/jdi.12660
55. Miyata Y, Shindo K, Matsuya F, Noguchi M, Nishikido M, Koga S, et al. Erectile dysfunction in hemodialysis patients with diabetes mellitus: association with age and hemoglobin A1c levels. Int J Urol. (2004) 11:530–4. doi: 10.1111/j.1442-2042.2004.00838.x
56. Mutagaywa RK, Lutale J, Aboud M, Kamala BA. Prevalence of erectile dysfunction and associated factors among diabetic men attending diabetic clinic at Muhimbili National Hospital in Dar-es-Salaam, Tanzania. Pan Afr Med J. (2014) 17:227. doi: 10.11604/pamj.2014.17.227.2695
57. Naya Y, Mizutani Y, Ochiai A, Soh J, Kawauchi A, Fujito A, et al. Preliminary report of association of chronic diseases and erectile dysfunction in middle-aged men in Japan. Urology. (2003) 62:532–6. doi: 10.1016/s0090-4295(03)00383-2
58. Ndang Ngou Milama S, Mougougou A, Olagui SG, Mbethe D, Nsame D, Boundama HG, et al. Analysis of the factors associated with ED in type 2 diabetics at the university hospital of libreville. Sex Med. (2022) 10:100564. doi: 10.1016/j.esxm.2022.100564
59. Nisahan B, Kumanan T, Rajeshkannan N, Peranantharajah T, Aravinthan M. Erectile dysfunction and associated factors among men with diabetes mellitus from a tertiary diabetic center in Northern Sri Lanka. BMC Res Notes. (2019) 12:210. doi: 10.1186/s13104-019-4244-x
60. Nutalapati S, Ghagane SC, Nerli RB, Jali MV, Dixit NS. Association of erectile dysfunction and type II diabetes mellitus at a tertiary care centre of south India. Diabetes Metab Syndr. (2020) 14:649–53. doi: 10.1016/j.dsx.2020.04.039
61. Moulik PK, Hardy KJ. Hypertension, anti-hypertensive drug therapy and erectile dysfunction in diabetes. Diabetes Med. (2003) 20:290–3. doi: 10.1046/j.1464-5491.2003.00911.x
62. Palmer MR, Holt SK, Sarma AV, Dunn RL, Hotaling JM, Cleary PA, et al. Longitudinal patterns of occurrence and remission of erectile dysfunction in men with type 1 diabetes. J Sex Med. (2017) 14:1187–94. doi: 10.1016/j.jsxm.2017.07.012
63. Pitta RM, de Lima Queiroga L, Louzada ACS, Ritti-Dias RM, Kaufmann OG, Wolosker N. What are the main risk factors associated with erectile dysfunction in the elderly? A cross-sectional study of 2436 Brazilian elderly men. Clin Interv Aging. (2023) 18:1047–54. doi: 10.2147/CIA.S405121
64. Rosen RC, Wing RR, Schneider S, Wadden TA, Foster GD, West DS, et al. Erectile dysfunction in type 2 diabetic men: relationship to exercise fitness and cardiovascular risk factors in the Look AHEAD trial. J Sex Med. (2009) 6:1414–22. doi: 10.1111/j.1743-6109.2008.01209.x
65. Sasaki H, Yamasaki H, Ogawa K, Nanjo K, Kawamori R, Iwamoto Y, et al. Prevalence and risk factors for erectile dysfunction in Japanese diabetics. Diabetes Res Clin Pract. (2005) 70:81–9. doi: 10.1016/j.diabres.2005.02.018
66. Seid A, Gerensea H, Tarko S, Zenebe Y, Mezemir R. Prevalence and determinants of erectile dysfunction among diabetic patients attending in hospitals of central and northwestern zone of Tigray, northern Ethiopia: a cross-sectional study. BMC Endocr Disord. (2017) 17:16. doi: 10.1186/s12902-017-0167-5
67. Shiri R, Ansari M, Falah Hassani K. Association between comorbidity and erectile dysfunction in patients with diabetes. Int J Impot Res. (2006) 18:348–53. doi: 10.1038/sj.ijir.3901432
68. Siu SC, Lo SK, Wong KW, Ip KM, Wong YS. Prevalence of and risk factors for erectile dysfunction in Hong Kong diabetic patients. Diabetes Med. (2001) 18:732–8. doi: 10.1046/j.0742-3071.2001.00557.x
69. Tridiantari DK, Saraswati LD, Udiyono A. Epidemiology of erectile dysfunction in men with diabetes mellitus: a study in a primary health care center in Indonesia. Med J Indonesia. (2020) 29:82–7. doi: 10.13181/mji.oa.192070
70. Van Cauwenberghe J, Enzlin P, Nefs G, Ruige J, Hendrieckx C, De Block C, et al. Prevalence of and risk factors for sexual dysfunctions in adults with type 1 or type 2 diabetes: Results from Diabetes MILES - Flanders. Diabetes Med. (2022) 39:e14676. doi: 10.1111/dme.14676
71. Walle B, Lebeta KR, Fita YD, Abdissa HG. Prevalence of erectile dysfunction and associated factors among diabetic men attending the diabetic clinic at Felege Hiwot Referral Hospital, Bahir Dar, North West Ethiopia, 2016. BMC Res Notes. (2018) 11:130. doi: 10.1186/s13104-018-3211-2
72. Weinberg AE, Eisenberg M, Patel CJ, Chertow GM, Leppert JT. Diabetes severity, metabolic syndrome, and the risk of erectile dysfunction. J Sex Med. (2013) 10:3102–9. doi: 10.1111/jsm.12318
73. Wessells H, Penson DF, Cleary P, Rutledge BN, Lachin JM, McVary KT, et al. Effect of intensive glycemic therapy on erectile function in men with type 1 diabetes. J Urol. (2011) 185:1828–34. doi: 10.1016/j.juro.2010.12.098
74. Yang G, Pan C, Lu J. Prevalence of erectile dysfunction among Chinese men with type 2 diabetes mellitus. Int J Impot Res. (2010) 22:310–7. doi: 10.1038/ijir.2010.21
75. Zheng H, Fan W, Li G, Tam T. Predictors for erectile dysfunction among diabetics. Diabetes Res Clin Pract. (2006) 71:313–9. doi: 10.1016/j.diabres.2005.07.011
76. Geldsetzer P, Ortblad K, Bärnighausen T. The efficiency of chronic disease care in sub-Saharan Africa. BMC Med. (2016) 14:127. doi: 10.1186/s12916-016-0675-6
77. Tadesse AW, Gurmu KK, Kebede ST, Habtemariam MK. Analyzing efforts to synergize the global health agenda of universal health coverage, health security and health promotion: a case-study from Ethiopia. Global Health. (2021) 17:53. doi: 10.1186/s12992-021-00702-7
78. Allen MS, Walter EE. Erectile dysfunction: an umbrella review of meta-analyses of risk-factors, treatment, and prevalence outcomes. J Sex Med. (2019) 16:531–41. doi: 10.1016/j.jsxm.2019.01.314
79. Mesfin T, Tekalegn Y, Adem A, Seyoum K, Geta G, Sahiledengle B, et al. Magnitude of erectile dysfunction and associated factors among adult diabetic men on follow-up at Goba and Robe hospitals, Bale Zone, South East Ethiopia: hospital-based cross-sectional study. BMC Endocr Disord. (2023) 23:236. doi: 10.1186/s12902-023-01489-x
80. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. (1994) 151:54–61. doi: 10.1016/s0022-5347(17)34871-1
81. Kouidrat Y, Pizzol D, Cosco T, Thompson T, Carnaghi M, Bertoldo A, et al. High prevalence of erectile dysfunction in diabetes: a systematic review and meta-analysis of 145 studies. Diabetes Med. (2017) 34:1185–92. doi: 10.1111/dme.13403
82. Defeudis G, Mazzilli R, Tenuta M, Rossini G, Zamponi V, Olana S, et al. Erectile dysfunction and diabetes: A melting pot of circumstances and treatments. Diabetes Metab Res Rev. (2022) 38:e3494. doi: 10.1002/dmrr.3494
83. Jackson SE, Yang L, Koyanagi A, Stubbs B, Veronese N, Smith L. Declines in sexual activity and function predict incident health problems in older adults: prospective findings from the english longitudinal study of ageing. Arch Sex Behav. (2020) 49:929–40. doi: 10.1007/s10508-019-1443-4
84. Liu H, Waite LJ, Shen S, Wang DH. Is sex good for your health? A national study on partnered sexuality and cardiovascular risk among older men and women. J Health Soc Behav. (2016) 57:276–96. doi: 10.1177/0022146516661597
85. Corona G, Rastrelli G, Monami M, Saad F, Luconi M, Lucchese M, et al. Body weight loss reverts obesity-associated hypogonadotropic hypogonadism: a systematic review and meta-analysis. Eur J Endocrinol. (2013) 168:829–43. doi: 10.1530/EJE-12-0955
86. Corona G, Rastrelli G, Balercia G, Lotti F, Sforza A, Monami M, et al. Hormonal association and sexual dysfunction in patients with impaired fasting glucose: a cross-sectional and longitudinal study. J Sex Med. (2012) 9:1669–80. doi: 10.1111/j.1743-6109.2012.02717.x
87. Morales A. Androgens are fundamental in the maintenance of male sexual health. Curr Urol Rep. (2011) 12:453–60. doi: 10.1007/s11934-011-0202-4
88. Ding EL, Song Y, Malik VS, Liu S. Sex differences of endogenous sex hormones and risk of type 2 diabetes: a systematic review and meta-analysis. JAMA. (2006) 295:1288–99. doi: 10.1001/jama.295.11.1288
89. Corona G, Monami M, Rastrelli G, Aversa A, Sforza A, Lenzi A, et al. Type 2 diabetes mellitus and testosterone: a meta-analysis study. Int J Androl. (2011) 34:528–40. doi: 10.1111/j.1365-2605.2010.01117.x
90. Corona G, Maggi M. The role of testosterone in male sexual function. Rev Endocr Metab Disord. (2022) 23:1159–72. doi: 10.1007/s11154-022-09748-3
91. Enzlin P, Rosen R, Wiegel M, Brown J, Wessells H, Gatcomb P, et al. Sexual dysfunction in women with type 1 diabetes: long-term findings from the DCCT/EDIC study cohort. Diabetes Care. (2009) 32:780–5. doi: 10.2337/dc08-1164
92. Castela A, Gomes P, Silvestre R, Guardão L, Leite L, Chilro R, et al. Vasculogenesis and diabetic erectile dysfunction: how relevant is glycemic control? J Cell Biochem. (2017) 118:82–91. doi: 10.1002/jcb.25613
93. Sima AA, Sugimoto K. Experimental diabetic neuropathy: an update. Diabetologia. (1999) 42:773–88. doi: 10.1007/s001250051227
94. Yagihashi S, Yamagishi S-I, Wada R. Pathology and pathogenetic mechanisms of diabetic neuropathy: correlation with clinical signs and symptoms. Diabetes Res Clin Pract. (2007) 77 Suppl 1:S184–9. doi: 10.1016/j.diabres.2007.01.054
95. de Souza ILL, Ferreira EDS, Vasconcelos LHC, Cavalcante F de A, da Silva BA. Erectile dysfunction: key role of cavernous smooth muscle cells. Front Pharmacol. (2022) 13:895044. doi: 10.3389/fphar.2022.895044
96. Burnett AL, Nehra A, Breau RH, Culkin DJ, Faraday MM, Hakim LS, et al. Erectile dysfunction: AUA guideline. J Urol. (2018) 200:633–41. doi: 10.1016/j.juro.2018.05.004
97. Assar ME, Angulo J, García-Rojo E, Sevilleja-Ortiz A, García-Gómez B, Fernández A, et al. Early manifestation of aging-related vascular dysfunction in human penile vasculature-A potential explanation for the role of erectile dysfunction as a harbinger of systemic vascular disease. Geroscience. (2022) 44:485–501. doi: 10.1007/s11357-021-00507-x
98. Phé V, Rouprêt M. Erectile dysfunction and diabetes: a review of the current evidence-based medicine and a synthesis of the main available therapies. Diabetes Metab. (2012) 38:1–13. doi: 10.1016/j.diabet.2011.09.003
99. Cayetano-Alcaraz AA, Tharakan T, Chen R, Sofikitis N, Minhas S. The management of erectile dysfunction in men with diabetes mellitus unresponsive to phosphodiesterase type 5 inhibitors. Andrology. (2023) 11:257–69. doi: 10.1111/andr.13257
100. Fillo J, Levcikova M, Ondrusova M, Breza J, Labas P. Importance of different grades of abdominal obesity on testosterone level, erectile dysfunction, and clinical coincidence. Am J Mens Health. (2017) 11:240–5. doi: 10.1177/1557988316642213
101. Corona G, Rastrelli G, Filippi S, Vignozzi L, Mannucci E, Maggi M. Erectile dysfunction and central obesity: an Italian perspective. Asian J Androl. (2014) 16:581–91. doi: 10.4103/1008-682X.126386
102. Kamenov ZA. A comprehensive review of erectile dysfunction in men with diabetes. Exp Clin Endocrinol Diabetes. (2015) 123:141–58. doi: 10.1055/s-0034-1394383
Keywords: diabetes mellitus, erectile dysfunction, risk factors, meta-analysis, sexual dysfuction
Citation: Dilixiati D, Waili A, Tuerxunmaimaiti A, Tao L, Zebibula A and Rexiati M (2024) Risk factors for erectile dysfunction in diabetes mellitus: a systematic review and meta-analysis. Front. Endocrinol. 15:1368079. doi: 10.3389/fendo.2024.1368079
Received: 09 January 2024; Accepted: 19 March 2024;
Published: 04 April 2024.
Edited by:
Katherine Esposito, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Mayank Choubey, NYU Grossman Long Island School of Medicine, United StatesGuiting Lin, University of California, San Francisco, United States
Copyright © 2024 Dilixiati, Waili, Tuerxunmaimaiti, Tao, Zebibula and Rexiati. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abudureheman Zebibula, MTE2MTgwMTBAemp1LmVkdS5jbg==; Mulati Rexiati, bXVyYXRyaXhhdEAxMjYuY29t
†These authors share first authorship