 Daniele Carvalhal de Almeida Beltrão1,2†
Daniele Carvalhal de Almeida Beltrão1,2† Fabyan Esberard de Lima Beltrão2,3†
Fabyan Esberard de Lima Beltrão2,3† Giulia Carvalhal4
Giulia Carvalhal4 Fabyanna Lethicia de Lima Beltrão5Amanda da Silva Brito6Hatilla dos Santos Silva7
Fabyanna Lethicia de Lima Beltrão5Amanda da Silva Brito6Hatilla dos Santos Silva7 Helena Mariana Pitangueira Teixeira7Juliana Lopes Rodrigues8Camila Alexandrina Viana de Figueiredo8Ryan dos Santos Costa8Liana Clebia De Morais Pordeus1Giciane Carvalho Vieira1‡
Helena Mariana Pitangueira Teixeira7Juliana Lopes Rodrigues8Camila Alexandrina Viana de Figueiredo8Ryan dos Santos Costa8Liana Clebia De Morais Pordeus1Giciane Carvalho Vieira1‡ Helton Estrela Ramos5,8,9*‡
Helton Estrela Ramos5,8,9*‡- 1Postgraduate Program in Cognitive Neuroscience and Behavior, Center for Health Sciences, Federal University of Paraíba, João Pessoa, Paraíba, Brazil
- 2Department of Internal Medicine, University Centre of João Pessoa (UNIPE), João Pessoa, Paraíba, Brazil
- 3Department of Internal Medicine, Lauro Wanderley University Hospital, Federal University of Paraíba, João Pessoa, Paraíba, Brazil
- 4Center for Biological and Health Sciences, Federal University of Campina Grande, Campina Grande, Paraíba, Brazil
- 5Post-Graduate Program in Medicine and Health, Medical School of Medicine, Federal University of Bahia, Salvador, Brazil
- 6Department of Internal Medicine, Royal Portuguese Hospital of Beneficence, Recife, Pernambuco, Brazil
- 7Bioregulation Department, Health and Science Institut, Federal University of Bahia, Salvador, Bahia, Brazil
- 8Laboratory of Immunopharmacology and Molecular Biology, Health Sciences Institute, Federal University of Bahia, Salvador, Bahia, Brazil
- 9Postgraduate Program in Interactive Processes of Organs and Systems, Health and Science Institute, Federal University of Bahia, Salvador, Bahia, Brazil
Background: The Thr92Ala-DIO2 polymorphism has been associated with clinical outcomes in hospitalized patients with COVID-19 and neuropsychiatric diseases. This study examines the impact of the Thr92Ala-DIO2 polymorphism on neuropsychological symptoms, particularly depressive symptoms, in patients who have had moderate to severe SARS-CoV-2 infection and were later discharged.
Methods: Our prospective cohort study, conducted from June to August 2020, collected data from 273 patients hospitalized with COVID-19. This included thyroid function tests, inflammatory markers, hematologic indices, and genotyping of the Thr92Ala-DIO2 polymorphism. Post-discharge, we followed up with 68 patients over 30 to 45 days, dividing them into depressive (29 patients) and non-depressive (39 patients) groups based on their Beck Depression Inventory scores.
Results: We categorized 68 patients into three groups based on their genotypes: Thr/Thr (22 patients), Thr/Ala (41 patients), and Ala/Ala (5 patients). Depressive symptoms were less frequent in the Thr/Ala group (29.3%) compared to the Thr/Thr (59.1%) and Ala/Ala (60%) groups (p = 0.048). The Thr/Ala heterozygous genotype correlated with a lower risk of post-COVID-19 depression, as shown by univariate and multivariate logistic regression analyses. These analyses, adjusted for various factors, indicated a 70% to 81% reduction in risk.
Conclusion: Our findings appear to be the first to show that heterozygosity for Thr92Ala-DIO2 in patients with COVID-19 may protect against post-COVID-19 depression symptoms up to 2 months after the illness.
1 Introduction
Since the onset of the COVID-19 pandemic on 11 March 2020, concerns about the increased risk of neuropsychiatric disorders among survivors have risen. Long-term COVID, involving post-acute sequelae after SARS-CoV-2 infection, can lead to various dysfunctions of extrapulmonary organs, including neuroinflammation, which may contribute to the development of depression (1, 2).
The peripheral cytokines may potentially affect brain function through direct action or via afferent pathways. Individuals with autoimmune diseases and severe infections are more likely to experience depression, and therapeutic cytokines can trigger depressive symptoms. The cytokines under extensive study include interleukin (IL) (IL-1β, IL-5, IL-6, IL-12, and IL-17), tumor necrosis factor (TNF), and interferons (IFNs), representing the inflammatory aspect, and IL-10, associated with resolution (3).
Depression is a complex polygenic disorder influenced by environment. Depending on various studies, its heritability ranges from 30% to 50%, with stress and imbalances in the HPA axis being notable contributing factors. Genetic studies often neglect stress effects, contributing to inconsistent results (4, 5).
There is a statistically significant association between thyroid dysfunction and the development of mental distress, mood disorders, and depression (5, 6). A comprehensive meta-analysis of 12,315 individuals indicated that patients with subclinical hypothyroidism have a higher risk of depression compared to euthyroid controls (relative risk of 2.35, 95% CI: 1.84 to 3.02, p < 0.001) (7). Depression-related thyroid hormone (TH) level changes include increased reversed triiodothyronine (rT3) (8, 9) and decreased circulating T3 and TSH levels (10, 11).
The DIO2 gene encodes type 2 deiodinase (D2), a crucial enzyme in converting the pro-hormone T4 into its active form, T3. The Thr92Ala-DIO2 polymorphism is found in approximately half of the global population and has been linked to chronic diseases such as type 2 diabetes mellitus (12, 13), obesity (14), arterial hypertension (15), osteoporosis (16), mental distress (17, 18), and depression (19, 20).
Lately, we investigated 220 consecutive patients with moderate to severe COVID-19 that showed a protective role of the heterozygous state of the polymorphic variant DIO2 (Thr92Ala) in mortality and severity from COVID-19. The heterozygous genotype (Thr/Ala) was associated with a 47%–62% reduced in-hospital risk. The protective role of Thr92Ala’s heterozygous advantage was supported in a meta-analysis of 21 studies in more than 20,000 patients with diseases such as diabetes, obesity, ischemic stroke, myocardial infarction, and left ventricular hypertrophy (21).
This study aims to investigate the potential correlation between the Thr92Ala-DIO2 polymorphism and depressive symptoms 2 months after COVID-19 hospital discharge. Additionally, it aims to explore various metabolic and hormonal biomarkers alongside tomographic measurements evaluated upon hospital admission. The results of this study could help stratify patients and enable early identification of neuropsychiatric disorders in COVID-19 survivors, facilitating future interventions.
2 Materials and methods
This research was a branch of a broader prospective, longitudinal cohort study, designed to assess thyroid dysfunction in patients with moderate to severe COVID-19 requiring intensive or semi-intensive care. We evaluated 273 consecutive patients hospitalized with COVID-19 between June and August 2020 at the Hospital Metropolitano Dom José Maria Pires (a tertiary referral hospital for COVID-19) in João Pessoa, Paraíba, Brazil. Following discharge, 78 patients were assessed as outpatients for neuropsychiatric issues (Figure 1). Ethical approval was granted by the Hospital Universitário Lauro Wanderley’s Ethics Committee for Human Research (CAAE:31562720.9.0000.5183).
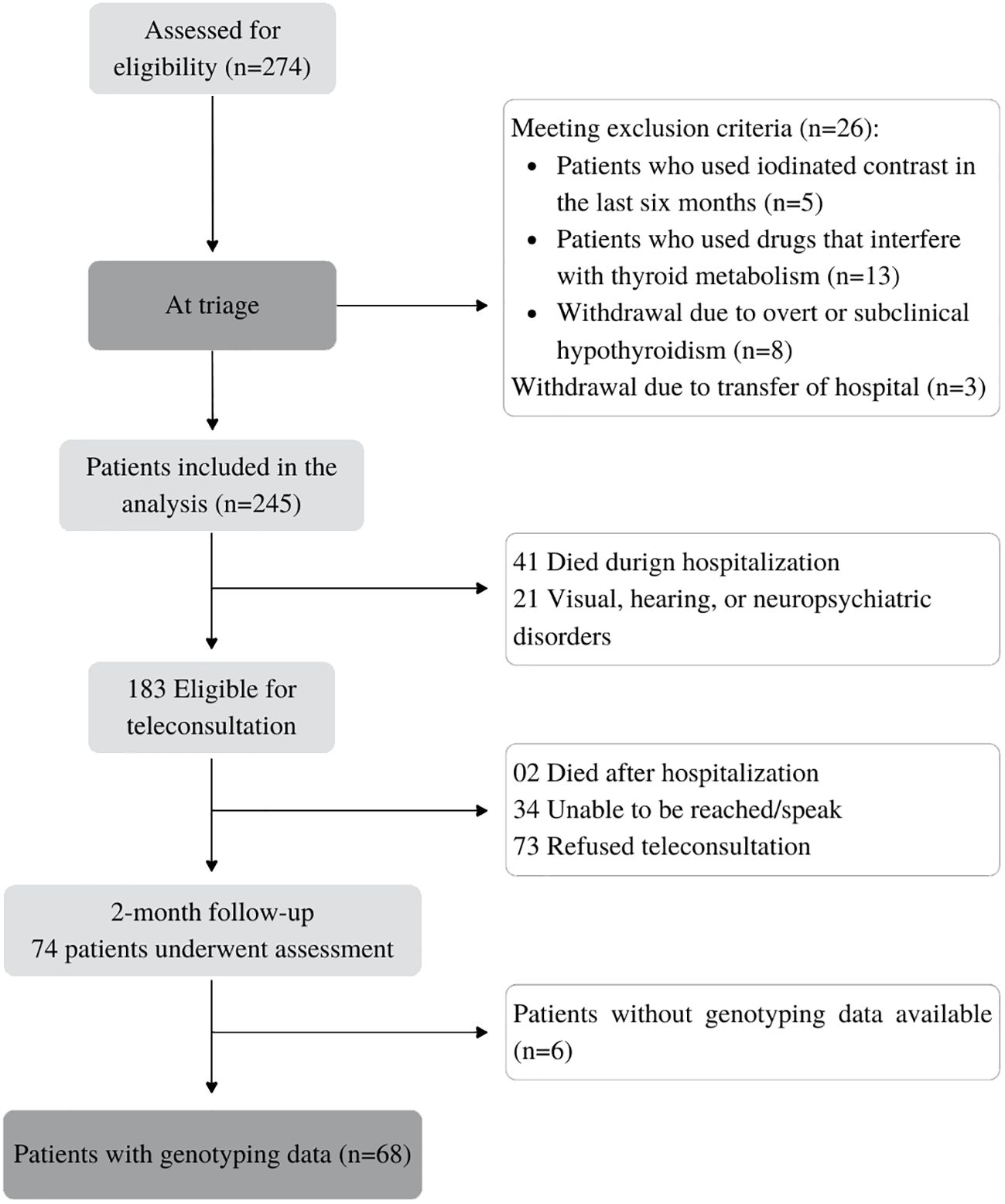
Figure 1 Flowchart of the study.
Inclusion criteria involved patients who tested positive for SARS-CoV-2 through quantitative real-time reverse transcription polymerase chain reaction (rRT-qPCR—Biomol OneStep/COVID-19, IBMP, Paraná, Brazil) with respiratory tract samples. In cases of negative rRT-qPCR, eligibility was determined based on clinical, radiological, and serological parameters (positive IgG for SARS-CoV-2). Exclusion criteria comprised patients with a history of thyroid disease or the use of drugs affecting thyroid metabolism, pregnancy, personal neuropsychiatric disorders, and the use of neuropsychiatric medications.
The primary outcomes were long-term depression symptomatology in previously hospitalized COVID-19 survivors according to the Thr92Ala-DIO2 polymorphism. Secondary outcomes were blood biochemistry, thyroid function tests, length of stay, comorbidities, complications, and severity scores according to Thr92Ala-DIO2 polymorphism and depressive symptomatology.
The research physicians gathered detailed clinical information on each patient within 48 h of admission using a standard questionnaire and severity scales (qSOFA and NEWS2). After discharge, patients were contacted and invited (30–45 days after discharge) by telephone for a medical consultation at the HULW, to evaluate post-COVID-19 symptoms and signs, including depression symptoms through Beck Depression Inventory (BDI). The BDI is a self-assessment instrument composed of 21 items with scores ranging from 0 to 63. The cutoff scores for the BDI were ≤9 (without depression) and >10 (with depression) (22).
Blood samples (50 mL) were collected within the first 48 h of hospital admission (before any interventions or therapy, including steroids and heparin). Laboratory tests performed included interleukin 6, D-dimer, alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatinine, high-sensitivity C-reactive protein (hs-PCR), and lactate dehydrogenase (LDH). The method used in all examinations was automated chemiluminescence (MAGLUMI-2000-PLUS; Shenzhen New Industries Biomedical Engineering Co., Shenzhen, China). The complete blood cell count with differential was performed on a MEK-7300 hematological analyzer (Nihon Kohden®, Tokyo, Japan).
Patients underwent chest CT to diagnose suspected SARS-CoV-2 pneumonia (ground-glass opacity, mosaic attenuation, and consolidation). A semiquantitative CT severity score proposed by Pan et al. was used in all cases (23).
Genomic DNA was extracted from peripheral blood leukocytes using standard techniques. In this study the polymorphism was determined by the TaqMan® SNP Genotyping method (7500 Real-Time PCR Systems, Applied Biosystems, Foster City, CA, USA), using the assay for genotyping with TaqMan® probes and primers, in a combination of hybridization and DNA polymerase activity, associated with fluorescence detection (24). We used the software Sequence Detection, version 1.3 (Applied Biosystems, CA) to analyze the data.
Statistical analysis: To determine the requisite sample size, we employed GPower 3.1.9.7 software, setting the significance level of α = 0.05, the desired statistical power of 0.95, and the effect size (F2) of 0.10. The outcome indicated a minimum sample size of 158 patients from the initial 273. Using the Cochran formula with finite population correction (population size n = 273) and aiming for a 95% confidence level and a margin of error within ±10% for prevalence estimation, the analysis required a minimum of 53 patients. Thus, our study group of 68 patients was sufficiently large for a comprehensive analysis.
The data were represented as the median ± interquartile range (IQR). Non-parametric tests were used for quantitative analysis, including the Mann–Whitney test for two-variable comparisons, and the Kruskal–Wallis test with Dunn’s post hoc test for multiple comparisons. Chi-square or Fisher’s exact test was used for qualitative analyses. Spearman’s rank correlation coefficient assessed the linear association between variables. Univariate and multivariate logistic regression analyses evaluated the risk of post-hospital discharge depressive symptoms among patients.
3 Results
Of the 274 adult patients admitted with COVID-19 to a referral hospital, 183 were initially selected for post-discharge assessment. Eligibility assessment led to the exclusion of 109 individuals: 2 due to post-hospitalization death, 34 were unreachable, and 73 declined participation. Furthermore, six patients were excluded due to incomplete genotype data, resulting in a final cohort of 68 patients (Figure 1).
The group of 68 patients was stratified into three subgroups based on genotype: Thr/Thr (n = 22), Thr/Ala (n = 41), and Ala/Ala (n = 5) (Figure 1). The Thr allele frequency was 0.62 and the Ala allele frequency was 0.37, with a distribution that was in Hardy–Weinberg equilibrium (p = 0.07; chi-square test). Baseline sociodemographic and clinical characteristics are summarized in Table 1. During follow-up, the median age of patients was 54.5 (45–67) years, 27 patients were over 60 years old (39.7%), and 48 patients (70.6%) were men. The median length of stay of patients in the hospital was 6 days (4.2–8), and seven patients (10.3%) were admitted to the ICU (Table 1).
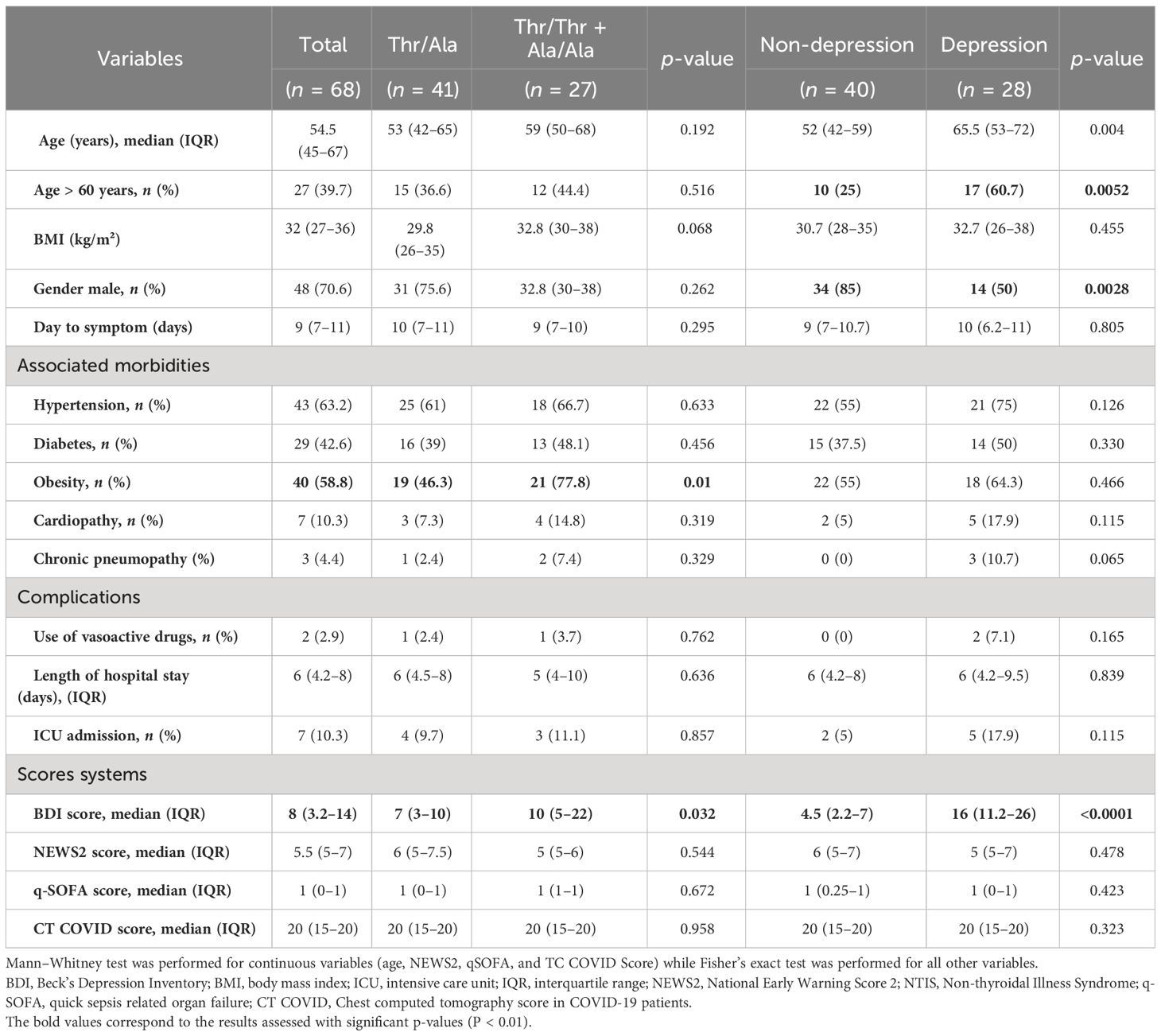
Table 1 Demographic and clinical characteristics of the patient cohort and their association with Thr92Ala-DIO2 polymorphism and depressive symptomatology (n = 68).
Risk factors for post-discharge depressive symptoms were analyzed using Mann–Whitney and Fisher’s tests. There was no significant difference between the risk factors (hypertension, diabetes mellitus, obesity, and heart disease), complications (use of vasoactive drugs, admission to the ICU, and hospital stay), and severity scores (NEWS2, q-SOFA, and CT-COVID). A higher percentage of non-depressed patients were younger than 60 (75%) and were men (85%) (Table 1).
Spearman correlation analysis (Figure 2A) revealed a direct correlation of BDI scores with age (r = 0.34, p = 0.005) and D-dimer (r = 0.35, p = 0.003). The strongest correlation was between D-dimer versus age (r = 0.45, p < 0.0001) and D-dimer versus IL-6 (r = 0.30, p < 0.01). The BDI scores, THs, and IL-6 showed no significant difference (Figure 2A).
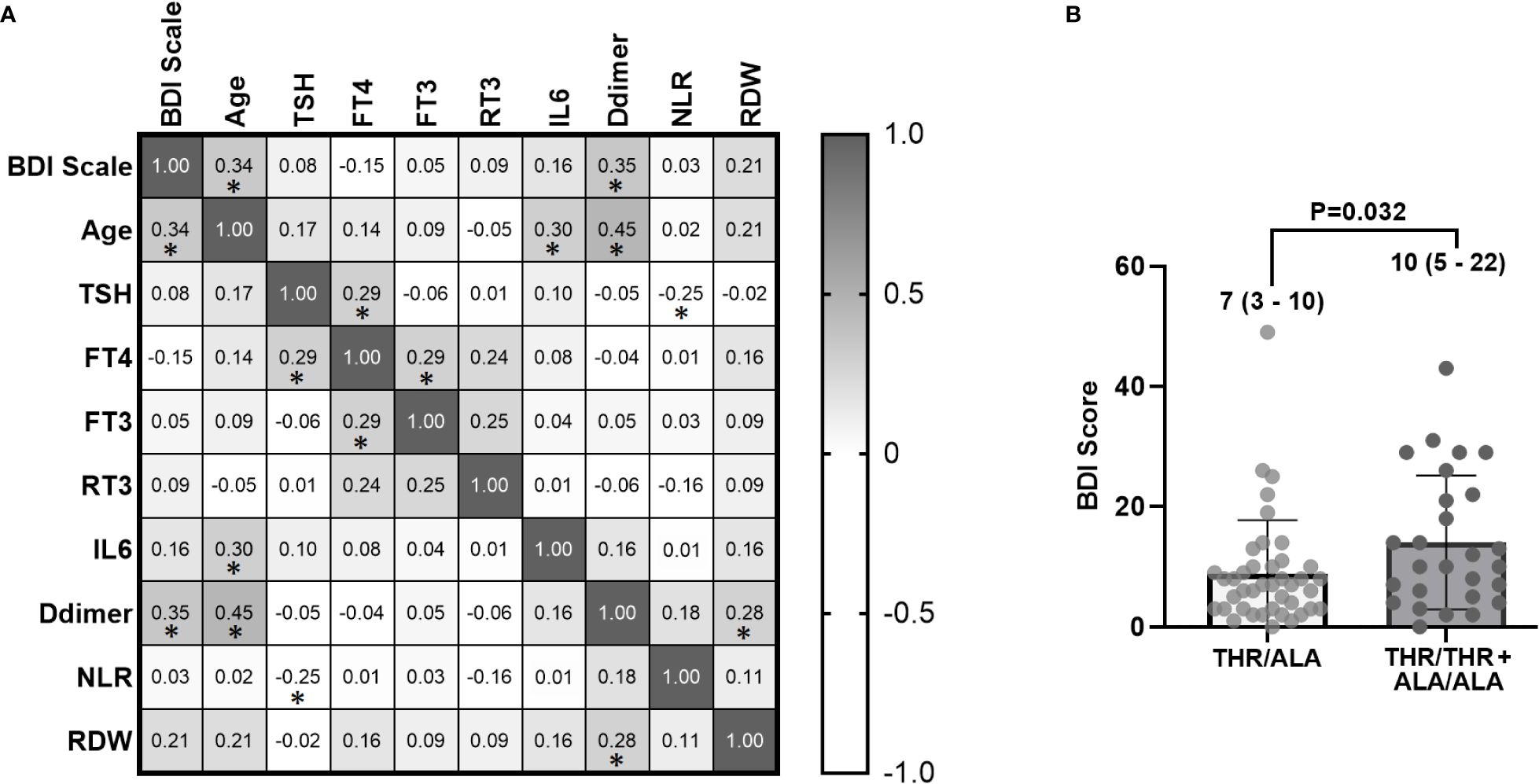
Figure 2 (A) Spearman correlation between laboratory variables of 68 hospitalized patients with COVID-19 collected within the first 48 h of admission and BDI scale scores after 30 to 45 days post-hospital discharge (* indicates p < 0.01). The numbers represent the correlation coefficient (r values). (B) Bar chart demonstrating higher BDI scores in homozygous patients (Thr/Thr + Ala/Ala) compared to heterozygous individuals (Thr/Ala) (p = 0.032). BDI, Beck Depression Inventory; TSH, thyroid-stimulating hormone; fT4, free tetraiodothyronine; fT3, free triiodothyronine; rT3: reverse triiodothyronine; IL-6, interleukin-6; NLR, neutrophil–lymphocyte ratio; RDW, red cell distribution width.
Regarding the BDI score, heterozygous patients (Thr92Ala) had lower scores than homozygous patients (p = 0.032) (Table 1 and Figure 2B).
The overall prevalence of depressive symptoms post-discharge was 41.2% (28 patients). Depressive symptoms were less common in Ala/Thr patients (29.3%) compared to Thr/Thr patients (59.1%) or Ala/Ala patients (60%) (p = 0.048) (Figure 3). Logistic regression analysis, adjusted for 15 comorbidities and other covariates, indicated that the Thr/Ala allele was associated with a reduced risk of depressive symptoms compared to the combined Thr/Thr + Ala/Ala genotype (overdominant model) (Table 2).
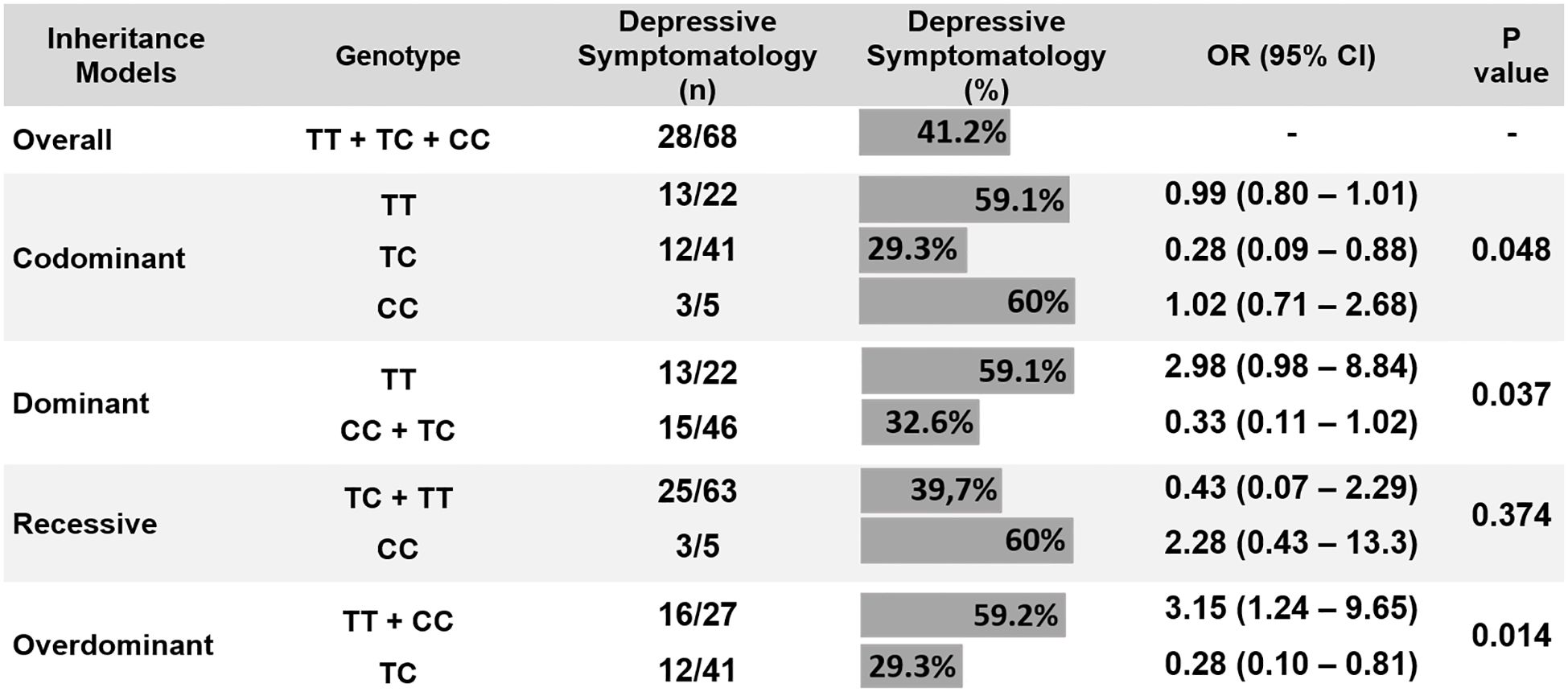
Figure 3 Correlation between DIO2 Thr92Ala polymorphism and depressive symptomatology (chi-square test). CI, confidence interval; OR, odds ratio.
Thyroid function tests, markers of inflammation, tissue damage, and hemochromocytometric parameters are shown in Table 2. There was no significant difference between laboratory parameters of the patient genotypes (Table 3). The only laboratory variable significantly different in patients with depressive symptoms was D-dimer levels, which were higher in these patients (p < 0.01).
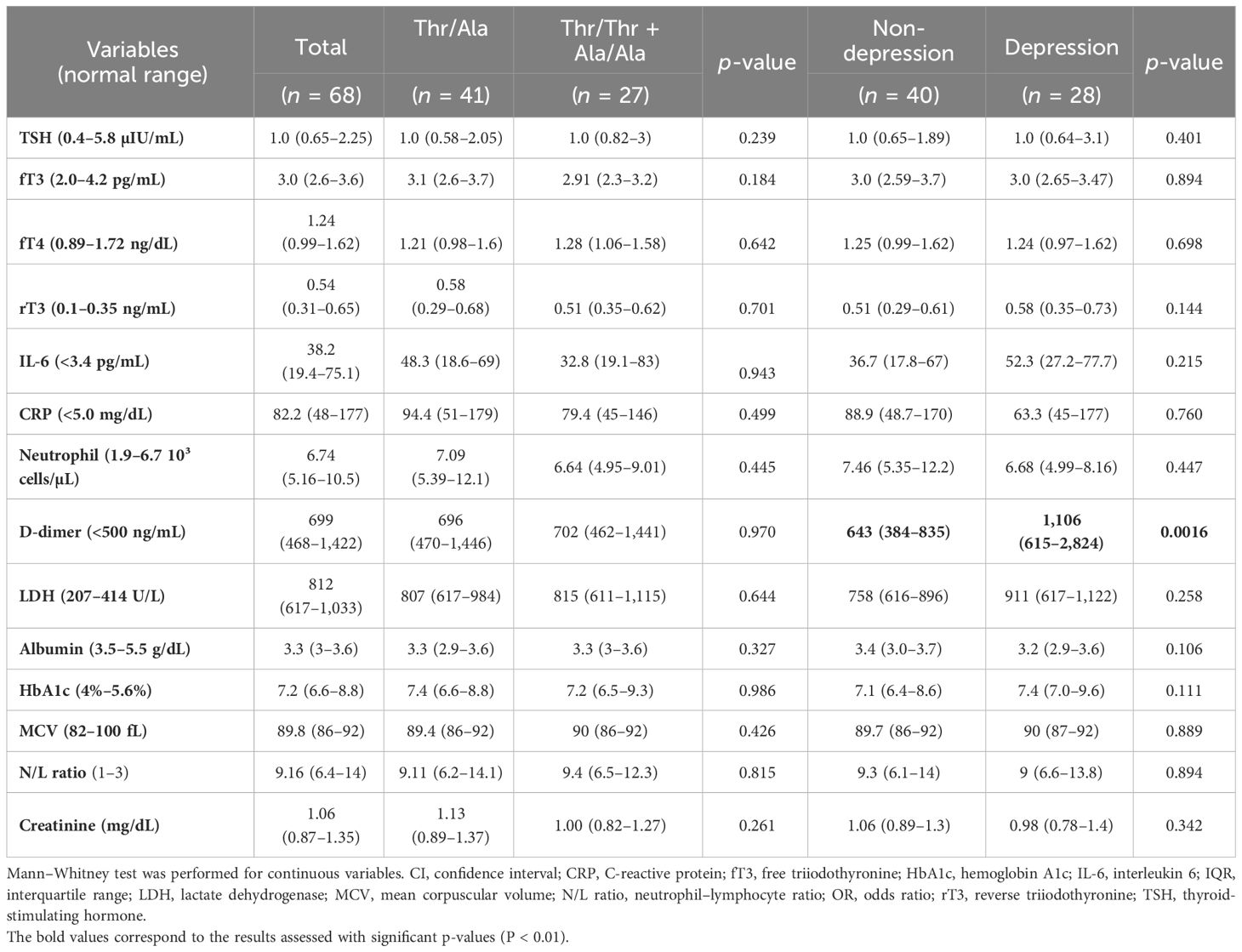
Table 2 Blood biochemistry in patients with COVID-19 and their association with Thr92Ala-DIO2 polymorphism and depressive symptomatology (n = 68).
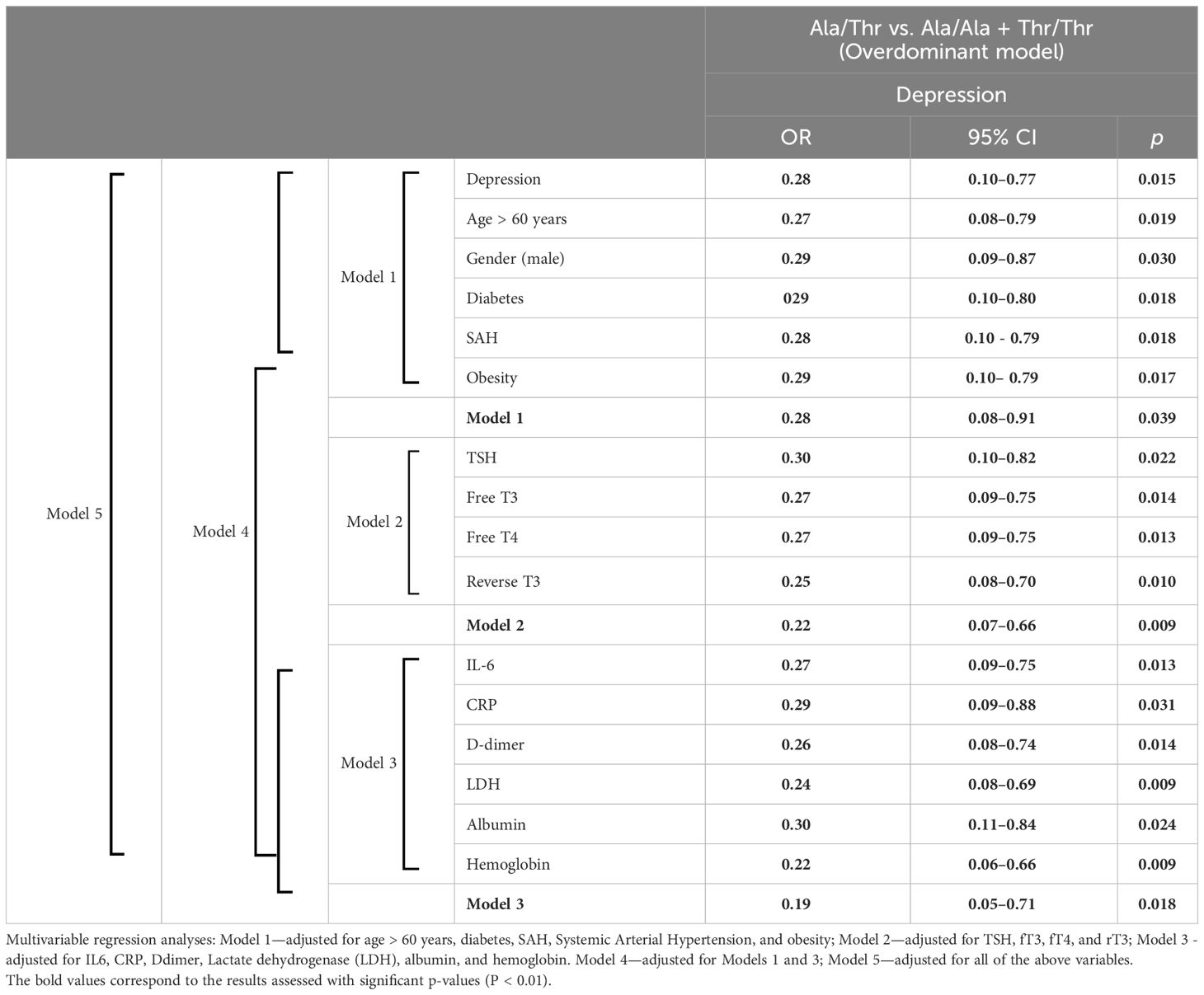
Table 3 Multivariable regression analyses between D2 Thr92Ala polymorphism (Thr/Thr, Thr/Ala, Ala/Ala, and overdominant model) and depressive symptomatology.
4 Discussion
To our knowledge, this study is the first of its kind to prospectively analyze the relationship between the Thr92Ala-DIO2 polymorphism and post-COVID-19 depression in hospitalized patients. Our findings indicate that the Thr/Ala genotype correlates with a significantly reduced risk of post-discharge depression, with risk reduction ranging between 70% and 81% as per univariate and multivariate logistic regression analyses adjusted for various covariates.
DIO2, essential for physiological function in the CNS, brown adipose tissue (25), and muscle (26), plays a pivotal role in local triiodothyronine (T3) production, influencing neurological development and function. Active T3 is produced within the brain by DIO2, predominantly by astrocytes, affecting genes associated with neuronal development, myelination, and synaptic transmission (27, 28). Notably, studies on mice that lack DIO2 revealed reduced brain T3 content with mild neurological effects, such as altered emotional behaviors and memory processing. Upregulation of DIO2 has been observed in various neurological disorders, influencing gene expression associated with inflammation and cell death.
The Thr92Ala D2 polymorphism has been associated with decreased TH activity in various end-organ targets. Research conducted in vitro and ex vivo suggests that the Ala allele is linked to enzyme dysfunction, impacting neurodegenerative mechanisms and oxidative stress within the central nervous system (29). Additionally, this polymorphism has been correlated with various neuropsychiatric conditions, including autism (Marcondes et al., 2021), schizophrenia (30), depression (19, 20), and cognitive impairment (31).
A Lithuanian study involving 168 participants investigated the link between 10 single-nucleotide polymorphisms (SNPs) in DIO1, DIO2, DIO3, and transmembrane TH transporters, specifically the organic anion transporter polypeptide 1C1 (OATP1C1), in relation to post-stroke depressive symptoms and anxiety. Among these SNPs, only the wild-type OATP1C1-rs974453 genotype (GG) showed a significant association with an increased likelihood for depression symptoms (OR = 2.73; 95% CI: 1.04–7.12; p = 0.041). In contrast, the Thr92Ala polymorphism did not demonstrate a statistically significant difference, even though it was more prevalent in the Thr/Thr genotype in patients with depression (20). Conversely, a study in Poland indicated that the Ala–Ala genotype of the Thr92Ala polymorphism was more common in healthy individuals compared to those with recurrent depression (7.2% vs. 0.6%, p = 0.03, respectively), suggesting its potential as a marker for reduced risk of recurrent depressive disorder (32).
This protection may be explained by the association of Thr92Ala-DIO2 gene expression with endoplasmic reticulum (ER) stress, inflammation, oxidative stress, apoptosis, and mitochondrial dysfunction (33). Disruption of ER homeostasis can lead to the accumulation of misfolded or unfolded proteins in the ER lumen, a condition referred to as ER stress. ER stress is associated with obesity, insulin resistance, type 2 diabetes (34), endothelial dysfunction (35), and low-grade chronic inflammation (36). These conditions have been associated with higher risk and worse prognosis of COVID-19 (37) and depression (38, 39).
Clinical studies have found associations between decreased levels of brain-derived neurotrophic factor (BDNF) and increased inflammatory markers, which are linked to the onset of depressive symptoms and various psychiatric disorders (40). In individuals with depression, one study revealed a correlation between elevated TSH levels, decreased serum BDNF levels, and a lower rise in BDNF during antidepressant treatment (41). A more recent study examining 50 patients undergoing their first episode of psychosis showed that high TSH levels were associated with low peripheral BDNF and reduced hippocampal volume, suggesting a potential neuroprotective effect of THs on the hippocampus (42).
Animal studies also contribute to our understanding by showing that BDNF has a protective effect against ER stress-induced cell death in brain neurons. This mechanism, which depends on PI3-K activation and inhibits caspase-12, highlights the importance of BDNF in maintaining neuronal integrity under stress (43). The connection between the Thr92Ala-DIO2 gene, ER stress, and BDNF regulation provides a comprehensive perspective on the biological mechanisms that protect against pathological conditions and depressive symptoms.
Research indicates a substantial genetic factor in depression, estimated to contribute approximately 30%–40% to its heritability (44, 45). A recent study found a significant link between the SIRT1 rs12415800 polymorphism, a gene associated with longevity, cellular defense against oxidative stress, and depressive symptoms in university students (46). This association was evident in both codominant (p = 0.0437) and overdominant (p = 0.0147) genetic models, demonstrating the heterozygous advantage (similar to our study) of this polymorphism against depressive symptoms (47).
Microglial cells, specific types of macrophages in the central nervous system, play a crucial role in neuroinflammation and are increasingly linked to the development of depression. Recent findings suggest a potential link between depression onset and viral infections like SARS-CoV-2, BoDV-1, ZIKV, HIV, and HHV6, which impact various glial cells, including astrocytes, oligodendrocytes, and microglia (48). Transcriptomic analysis [Gene Set Enrichment Analysis (GSEA)] of mice with the Thr92Ala polymorphism revealed increased gene expression related to neuroplasticity, cognition, apoptosis, and neuroinflammation. These results strongly suggest an association between Thr92Ala and neuroinflammation, involving astrocytes as the primary cell type expressing DIO2 in the central nervous system (49).
There are some limitations in this study. Our sample size was relatively small, and the observation time was short; we did not collect healthy people as controls, which may have some influence on the study results; we used mostly self-assessment scales, which may introduce recall bias; and we were unable to measure serum BDNF levels in our patients.
In this prospective study, we present evidence suggesting that possessing heterozygosity of Thr92Ala-DIO2 may have a protective role in preventing the occurrence of depressive symptoms after being discharged from the hospital. Additional research is needed to confirm these findings.
Data availability statement
The data presented in the study have been deposited in the figshare repository with the following accession number: https://doi.org/10.6084/m9.figshare.25118159.v1.
Ethics statement
The studies involving humans were approved by Hospital Universitario Lauro Wanderley’s Ethics Committee for Human Research. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DB: Data curation, Investigation, Methodology, Writing – original draft. FEB: Formal analysis, Investigation, Methodology, Software, Writing – original draft. GC: Data curation, Methodology, Writing – review & editing. FLB: Data curation, Methodology, Writing – review & editing. AB: Data curation, Writing – review & editing. HS: Data curation, Methodology, Writing – review & editing. HT: Data curation, Methodology, Writing – review & editing. JR: Data curation, Methodology, Writing – review & editing. CF: Data curation, Writing – review & editing. RC: Conceptualization, Validation, Writing – review & editing. LP: Investigation, Writing – review & editing, Methodology. GV: Conceptualization, Writing – review & editing. HR: Conceptualization, Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank all the patients who participated in this study and all the healthcare professionals at the Metropolitan Hospital Dom José Maria Pires for their efforts in taking care of these patients.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found onlineat: https://www.frontiersin.org/articles/10.3389/fendo.2024.1366500/full#supplementary-material
References
1. Peter RS, Nieters A, Kräusslich HG, Brockmann SO, Göpel S, Kindle G, et al. Post-acute sequelae of covid-19 six to 12 months after infection: population based study. BMJ. (2022) 379:e071050. doi: 10.1136/BMJ-2022-071050
2. Taquet M, Geddes JR, Husain M, Luciano S, Harrison PJ. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. (2021) 8:416–27. doi: 10.1016/S2215-0366(21)00084-5
3. Köhler CA, Freitas TH, Maes M, de Andrade NQ, Liu CS, Fernandes BS, et al. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatr Scand. (2017) 135:373–87. doi: 10.1111/ACPS.12698
4. Gonda X, Hullam G, Antal P, Eszlari N, Petschner P, Hökfelt TG, et al. Significance of risk polymorphisms for depression depends on stress exposure. Sci Rep. (2018) 8:1–10. doi: 10.1038/s41598-018-22221-z
5. Zięba A, Matosiuk D, Kaczor AA. The role of genetics in the development and pharmacotherapy of depression and its impact on drug discovery. Int J Mol Sci. (2023) 24:2946. doi: 10.3390/IJMS24032946
6. Müssig K, Künle A, Säuberlich AL, Weinert C, Ethofer T, Saur R, et al. Thyroid peroxidase antibody positivity is associated with symptomatic distress in patients with Hashimoto’s thyroiditis. Brain Behav Immun. (2012) 26:559–63. doi: 10.1016/J.BBI.2012.01.006
7. Loh HH, Lim LL, Yee A, Loh HS. Association between subclinical hypothyroidism and depression: An updated systematic review and meta-analysis. BMC Psychiatry. (2019) 19:1–10. doi: 10.1186/S12888-018-2006-2/FIGURES/5
8. Kjellman BF, Ljunggren JG, Beck-Friis J, Wetterberg L. Reverse T3 levels in affective disorders. Psychiatry Res. (1983) 10:1–9. doi: 10.1016/0165-1781(83)90022-7
9. Kirkegaard C, Faber J. Free thyroxine and 3,3’,5’-triiodothyronine levels in cerebrospinal fluid in patients with endogenous depression. Acta Endocrinol (Copenh). (1991) 124:166–72. doi: 10.1530/ACTA.0.1240166
10. Jia Y, Zhong S, Wang Y, Liu T, Liao X, Huang L. The correlation between biochemical abnormalities in frontal white matter, hippocampus and serum thyroid hormone levels in first-episode patients with major depressive disorder. J Affect Disord. (2015) 180:162–9. doi: 10.1016/J.JAD.2015.04.005
11. Ma J, Zhao M, Niu G, Wang Z, Jiang S, Liu Z. Relationship between thyroid hormone and sex hormone levels and non-suicidal self-injury in male adolescents with depression. Front Psychiatry. (2022) 13:1071563. doi: 10.3389/FPSYT.2022.1071563
12. Estivalet AAF, Leiria LB, Dora JM, Rheinheimer J, Bouças AP, Maia AL, et al. D2 Thr92Ala and PPARγ2 pro12ala polymorphisms interact in the modulation of insulin resistance in type 2 diabetic patients. Obesity. (2011) 19:825–32. doi: 10.1038/oby.2010.231
13. Dora JM, MaChado WE, Rheinheimer J, Crispim D, Maia AL. Association of the type 2 deiodinase Thr92Ala polymorphism with type 2 diabetes: case–control study and meta-analysis. Eur J Endocrinol. (2010) 163:427–34. doi: 10.1530/EJE-10-0419
14. Wang X, Chen K, Zhang C, Wang H, Li J, Wang C, et al. The type 2 deiodinase thr92Ala polymorphism is associated with higher body mass index and fasting glucose levels: A systematic review and meta-analysis. BioMed Res Int. (2021) 2021:9914009. doi: 10.1155/2021/9914009
15. van der Deure WM, Peeters RP, Uitterlinden AG, Hofman A, Breteler MM, Witteman J, et al. Impact of thyroid function and polymorphisms in the type 2 deiodinase on blood pressure: the Rotterdam Study and the Rotterdam Scan Study. Clin Endocrinol (Oxf). (2009) 71:137–44. doi: 10.1111/J.1365-2265.2008.03447.X
16. Kang YE, Kang YM, Park B, Shong M, Yi HS. Type 2 deiodinase Thr92Ala polymorphism is associated with a reduction in bone mineral density: A community-based korean genome and epidemiology study. Clin Endocrinol (Oxf). (2020) 93:238–47. doi: 10.1111/cen.14206
17. Marcondes AAE, Gomez TGB, Ravache TT, Batistuzzo A, Lorena FB, de Paula CS, et al. Assessment of children in the autistic spectrum disorder that carry the Thr92Ala-DIO2 polymorphism. J Endocrinol Invest. (2021) 44:1775–82. doi: 10.1007/S40618-020-01497-X
18. Taroza S, Rastenytė D, Podlipskytė A, Patamsytė V, Mickuvienė N. Deiodinases, organic anion transporter polypeptide polymorphisms and ischemic stroke outcomes. J Neurol Sci. (2019) 407:116457. doi: 10.1016/j.jns.2019.116457
19. Gałecka E, Talarowska M, Orzechowska A, Górski P, Bieńkiewicz M, Szemraj J. Association of the DIO2 gene single nucleotide polymorphisms with recurrent depressive disorder. Acta Biochim Pol. (2015) 62:297–302. doi: 10.18388/abp.2014_1002
20. Taroza S, Rastenytė D, Burkauskas J, Podlipskytė A, Kažukauskienė N, Patamsytė V, et al. Deiodinases, organic anion transporter polypeptide polymorphisms and symptoms of anxiety and depression after ischemic stroke. J Stroke Cerebrovascular Dis. (2020) 29:105040. doi: 10.1016/j.jstrokecerebrovasdis.2020.105040
21. Beltrão FEL, Beltrão DCA, Carvalhal G, de Lima Beltrão FE, de Souza Braga Filho J, de Brito Oliveira J, et al. Heterozygote advantage of the type II deiodinase thr92Ala polymorphism on intrahospital mortality of COVID-19. J Clin Endocrinol Metab. (2022) 107:E2488–501. doi: 10.1210/CLINEM/DGAC075
22. Andrade L, Gorenstein C, Vieira Filho AH, Tung TC, Artes R. Psychometric properties of the Portuguese version of the State-Trait Anxiety Inventory applied to college students: Factor analysis and relation to the Beck Depression Inventory. Braz J Med Biol Res. (2001) 34:367–74. doi: 10.1590/S0100-879X2001000300011
23. Pan F, Ye T, Sun P, Gui S, Liang B, Li L, et al. Time course of lung changes at chest CT during recovery from Coronavirus disease 2019 (COVID-19). Radiology. (2020) 295:715–21. doi: 10.1148/radiol.2020200370
24. De La Vega FM, Lazaruk KD, Rhodes MD, Wenz MH. Assessment of two flexible and compatible SNP genotyping platforms: TaqMan® SNP Genotyping Assays and the SNPlexTM Genotyping System. Mutat Res - Fundam Mol Mech Mutagenesis. (2005) 573:111–35. doi: 10.1016/J.MRFMMM.2005.01.008
25. Strączkowski M, Nikołajuk A, Stefanowicz M, Matulewicz N, Fernandez-Real JM, Karczewska-Kupczewska M. Adipose tissue and skeletal muscle expression of genes associated with thyroid hormone action in obesity and insulin resistance. Thyroid (2022) 32:206–14. doi: 10.1089/THY.2021.0351
26. Marsili A, Tang D, Harney JW, Singh P, Zavacki AM, Dentice M, et al. Type II iodothyronine deiodinase provides intracellular 3,5,3’-triiodothyronine to normal and regenerating mouse skeletal muscle. Am J Physiol Endocrinol Metab. (2011) 301:818–24. doi: 10.1152/AJPENDO.00292.2011/ASSET/IMAGES/LARGE/ZH10101163430005.JPEG
27. Richard S, Flamant F. Regulation of T3 availability in the developing brain: The mouse genetics contribution. Front Endocrinol (Lausanne). (2018) 9:265/BIBTEX. doi: 10.3389/FENDO.2018.00265/BIBTEX
28. Salas-Lucia F, Fekete C, Sinkó R, Egri P, Rada K, Ruska Y, et al. Axonal T3 uptake and transport can trigger thyroid hormone signaling in the brain. Elife. (2023) 12:e82683. doi: 10.7554/ELIFE.82683
29. Butler PW, Smith SM, Linderman JD, Brychta RJ, Alberobello AT, Dubaz OM, et al. The thr92Ala 5′ Type 2 deiodinase gene polymorphism is associated with a delayed triiodothyronine secretion in response to the thyrotropin-releasing hormone–stimulation test: A pharmacogenomic study. Thyroid. (2010) 20:1407. doi: 10.1089/THY.2010.0244
30. Colak A, Akan G, Oncu F, Yanbay H, Acar S, Yesilbursa D, et al. 1508– Association study of the dio2 gene as a susceptibility candidate for schizophrenia in the turkish population; a case-control study. Eur Psychiatry. (2013) 28:1. doi: 10.1016/S0924-9338(13)76526-X
31. Wouters HJCM, Van Loon HCM, van der Klauw MM, Elderson MF, Slagter SN, Kobold AM, et al. No effect of the thr92Ala polymorphism of deiodinase-2 on thyroid hormone parameters, health-related quality of life, and cognitive functioning in a large population-based cohort study. Thyroid. (2017) 27:147–55. doi: 10.1089/THY.2016.0199
32. Gałecka E, Talarowska M, Orzechowska A, Górski P, Szemraj J. Polymorphisms in the type I deiodinase gene and frontal function in recurrent depressive disorder. Adv Med Sci. (2016) 61:198–202. doi: 10.1016/J.ADVMS.2015.12.008
33. Jo S, Fonseca TL, Bocco BMLC, Fernandes GW, McAninch EA, Bolin AP, et al. Type 2 deiodinase polymorphism causes ER stress and hypothyroidism in the brain. J Clin Invest. (2019) 129:230. doi: 10.1172/JCI123176
34. Özcan U, Cao Q, Yilmaz E, Lee AH, Iwakoshi NN, Özdelen E, et al. Endoplasmic reticulum stress links obesity, insulin action, and type 2 diabetes. Science. (2004) 306:457–61. doi: 10.1126/SCIENCE.1103160/SUPPL_FILE/OZCAN.SOM.REV.PDF
35. di Pietro N, Marcovecchio ML, di Silvestre S, de Giorgis T, Cordone VGP, Lanuti P, et al. Plasma from pre-pubertal obese children impairs insulin stimulated Nitric Oxide (NO) bioavailability in endothelial cells: Role of ER stress. Mol Cell Endocrinol. (2017) 443:52. doi: 10.1016/J.MCE.2017.01.001
36. Kim S, Joe Y, Jeong SO, Zheng M, Back SH, Park SW, et al. Endoplasmic reticulum stress is sufficient for the induction of IL-1β production via activation of the NF-κB and inflammasome pathways. Innate Immun. (2014) 20:799–815. doi: 10.1177/1753425913508593
37. Stefan N, Birkenfeld AL, Schulze MB. Global pandemics interconnected — obesity, impaired metabolic health and COVID-19. Nat Rev Endocrinol. (2021) 17:135–49. doi: 10.1038/s41574-020-00462-1
38. Mao J, Hu Y, Ruan L, Ji Y, Lou Z. Role of endoplasmic reticulum stress in depression (Review). Mol Med Rep. (2019) 20:4774–80. doi: 10.3892/MMR.2019.10789
39. Behnke J, Mann MJ, Scruggs FL, Feige MJ, Hendershot LM. Members of the Hsp70 family recognize distinct types of sequences to execute ER quality control. Mol Cell. (2016) 63:739. doi: 10.1016/J.MOLCEL.2016.07.012
40. Lima Giacobbo B, Doorduin J, Klein HC, Dierckx RAJO, Bromberg E, de Vries EFJ. Brain-derived neurotrophic factor in brain disorders: focus on neuroinflammation. Mol Neurobiol. (2019) 56:3295. doi: 10.1007/S12035-018-1283-6
41. Baek JH, Kang ES, Fava M, Mischoulon D, Nierenberg AA, Lee D, et al. Thyroid stimulating hormone and serum, plasma, and platelet brain-derived neurotrophic factor during a 3-month follow-up in patients with major depressive disorder. J Affect Disord. (2014) 169:112–7. doi: 10.1016/J.JAD.2014.08.009
42. Toll A, Blanco-Hinojo L, Berge D, Manzano A, El Abidi K, Perez-Solà V, et al. Relationship between thyroid-stimulating hormone, BDNF levels, and hippocampal volume in antipsychotic-naïve first-episode psychosis patients. Front Psychiatry. (2023) 14:1301714/BIBTEX. doi: 10.3389/FPSYT.2023.1301714/BIBTEX
43. Shimoke K, Utsumi T, Kishi S, Nishimura M, Sasaya H, Kudo M, et al. Prevention of endoplasmic reticulum stress-induced cell death by brain-derived neurotrophic factor in cultured cerebral cortical neurons. Brain Res. (2004) 1028:105–11. doi: 10.1016/J.BRAINRES.2004.09.005
44. Wray NR, Ripke S, Mattheisen M, Trzaskowski M, Byrne EM, Abdellaoui A, et al. Genome-wide association analyses identify 44 risk variants and refine the genetic architecture of major depression. Nat Genet. (2018) 50:668. doi: 10.1038/S41588-018-0090-3
45. Sullivan PF, Neale MC, Kendler KS. Genetic epidemiology of major depression: Review and meta-analysis. Am J Psychiatry. (2000) 157:1552–62. doi: 10.1176/APPI.AJP.157.10.1552/ASSET/IMAGES/LARGE/Q42F1.JPEG
46. Kilic U, Gok O, Bacaksiz A, Izmirli M, Elibol-Can B, Uysal O. SIRT1 gene polymorphisms affect the protein expression in cardiovascular diseases. PloS One. (2014) 9:90428. doi: 10.1371/JOURNAL.PONE.0090428
47. Wang C, Ji L, Ren D, Yuan F, Liu L, Bi Y, et al. Personality traits as mediators in the association between SIRT1 rs12415800 polymorphism and depressive symptoms among Chinese college students. Front Psychiatry. (2023) 14:1104664/BIBTEX. doi: 10.3389/FPSYT.2023.1104664/BIBTEX
48. Yu X, Wang S, Wu W, Chang H, Shan P, Yang L, et al. Exploring new mechanism of depression from the effects of virus on nerve cells. Cells. (2023) 12:1767. doi: 10.3390/CELLS12131767
Keywords: post-COVID-19, Thr92Ala-DIO2 polymorphism, thyroid function, biomarkers, depression
Citation: Beltrão DCdA, Beltrão FEdL, Carvalhal G, Beltrão FLdL, Brito AdS, Silva HdS, Teixeira HMP, Rodrigues JL, de Figueiredo CAV, Costa RdS, Pordeus LCDM, Vieira GC and Ramos HE (2024) The Thr92Ala polymorphism in the type 2 deiodinase gene is linked to depression in patients with COVID-19 after hospital discharge. Front. Endocrinol. 15:1366500. doi: 10.3389/fendo.2024.1366500
Received: 06 January 2024; Accepted: 20 February 2024;
Published: 07 June 2024.
Edited by:
Jeff M. P. Holly, University of Bristol, United KingdomReviewed by:
Miriam Oliveira Ribeiro, Mackenzie Presbyterian University, BrazilAdriano Martimbianco De Assis, Catholic University of Pelotas, Brazil
Copyright © 2024 Beltrão, Beltrão, Carvalhal, Beltrão, Brito, Silva, Teixeira, Rodrigues, de Figueiredo, Costa, Pordeus, Vieira and Ramos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helton Estrela Ramos, cmFtb3NoZWx0b25AZ21haWwuY29t
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship