
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 17 May 2024
Sec. Clinical Diabetes
Volume 15 - 2024 | https://doi.org/10.3389/fendo.2024.1344007
This article is part of the Research Topic Preventing cardiovascular complications of type 2 diabetes View all 13 articles
 Amanda Jiménez1,2,3†
Amanda Jiménez1,2,3† Bogdan Vlacho4,5†
Bogdan Vlacho4,5† Manel Mata-Cases4,5
Manel Mata-Cases4,5 Jordi Real4
Jordi Real4 Dídac Mauricio4,5,6,7
Dídac Mauricio4,5,6,7 Josep Franch-Nadal4,5,8*‡
Josep Franch-Nadal4,5,8*‡ Emilio Ortega1,2,3*‡
Emilio Ortega1,2,3*‡Aims: We aimed to describe and compare the incidence of the first cardiovascular event and its major subtypes, coronary heart disease (CHD), cerebrovascular disease, heart failure (HF), or peripheral artery disease (PAD), according to age and sex in a population-based cohort of individuals with type 2 diabetes (T2D) from a Mediterranean region.
Material and methods: We used linked primary care electronic medical reports, pharmacy-invoicing data, and hospital admission disease registry records from the SIDIAP database, which contains linked data for 74% of the Catalonian population. We selected individuals with T2D aged 30 to 89 years free of cardiovascular disease (CVD). The primary outcome was the first presentation of CVD.
Results: The study cohort included 247,751 individuals (48.6% women, 66.8 ± 11.9 years). During a 6.99-year follow-up, the cumulative incidence of the first cardiovascular event was 23.4%. Men were at higher risk for CVD (hazard ratio [HR]: 1.47 95%CI: 1.45-1.50), CHD (HR: 1.52 95%CI: 1.47-1.57), cerebrovascular disease (HR:1.07 95%CI: 1.03-1.10) and PAD (HR: 2.30 95%CI: 2.21-2.39) than women but at a lower risk for HF (HR:0.70 95%CI: 0.68-0.73). CHD and PAD were the most frequent CVD presentations among men (28.1% and 27.5%) and HF (40.1%) in women. CHD predominated among young participants of both sexes, while HF predominated among women older than 65 and men older than 75.
Conclusions: In individuals with T2D, the overall risk and the type of first CVD manifestation largely varied by sex and age. This epidemiological evidence should be considered in clinical practice.
Patients with type 2 diabetes (T2D) are at a higher risk for a wide range of cardiovascular diseases (1). Although a substantial reduction in incidence rates of cardiovascular complications has been observed over the last two decades, cardiovascular disease (CVD) risk in T2D remains higher than in age and sex-matched controls. Furthermore, despite steadily decreasing rates for atherosclerotic diseases, the decline in heart failure (HF) incidence has plateaued in recent years (2).
Given the varied impact of modifiable cardiovascular risk factors on different manifestations of CVD, acquiring a comprehensive understanding of the epidemiology surrounding initial cardiovascular events in individuals with T2D could foster the creation of more personalized primary prevention approaches (2). This might be especially relevant among young adults, as evidenced by recent data from the Global Burden of Disease (GBD) study, which highlights an increasing trend in cardiovascular morbidity and mortality in this age cohort over the last three decades (3).
In this context, there is a growing acknowledgment that CVD pathophysiology and presentation exhibit variations based on sex and age (4). Of note, within the general population, CVD predominantly presents as coronary heart disease (CHD) in men, whereas women are more prone to experiencing cerebrovascular disease or HF as their primary event, with these manifestations typically occurring more frequently at older ages (5). Whether such age and sex differences in the first CVD event are also present in individuals with T2D has seldom been explored.
Several studies and meta-analyses have demonstrated a stronger association between T2D and HF, CHD, and cerebrovascular disease in women than in men (6–11). Fewer studies have explored sex differences in absolute risk for the various forms of CVD manifestation, and none focused on first events (2, 6, 12). In addition, whether age modulates sex-specific risks for the different CVD subtypes in men and women with T2D is poorly defined as most previous studies applied broad age groups or did not consider the various CVD components separately (2, 6, 12).
In this work, we aimed to describe and compare the incidence rates of the first cardiovascular event and its major subtypes (CHD, PAD, cerebrovascular disease, and HF) according to sex and age in a large cohort of individuals with T2D from a primary care setting.
We performed a longitudinal, retrospective cohort study. Data for this study was obtained from the Sistema d’Informació per al Desenvolupament de l’Investigació en Atenció Primària (SIDIAP) database (www.sidiap.org). This database, created in 2010 for research purposes, contains pseudo-anonymous, routinely collected healthcare information of over 5,000,000 patients registered by 3,414 general practitioners at 274 different primary care practices in Catalonia (a northeast area of Spain). The population in the SIDIAP database corresponds to more than 74% of the Catalonian population, providing a representative sample of the primary care population.
The SIDIAP database contains information on clinical diagnoses, anthropometric measures, and laboratory tests. In addition, the CMBD database (data from hospitalisation discharge statistics and specialised out-patient care from the hospitals of the National Health System) and pharmacological treatments (data from the pharmacy-invoicing system provided by the CatSalut) are automatically collected and linked to the SIDIAP database. The Ethics Committee of the Primary Healthcare University Research Institute (IDIAP), Jordi Gol (Barcelona, Spain), approved the study (code P17/087).
For this analysis, we selected all individuals with a registered diagnosis of T2D (n=333,036) on January 1st, 2010 (study index date). T2D diagnosis was based on the presence of the diagnostic codes (International Statistical Classification of Diseases and Related Health Problems 10th Revision-ICD-10): E11, E13, and E14. Subjects with other types of diabetes, such as type 1, secondary, or gestational diabetes (ICD-10: E10, E12, O24), were excluded from the analysis.
Individuals with previous cardiovascular events (n=68,982, 20.7%) or known atrial fibrillation (n=22,673, 6.8%) were excluded, as well as those aged under 27 or above 89 years (n=8,310, 2.4%) for whom cardiovascular risk evaluation was not systematically recommended or CVD prevention of a first event was not a clinical priority. The remaining participants (n=247,751) were followed until the cardiovascular event, death, or the end of the study (December 2016). Study flow charts are included in the Supplementary material (Supplementary Figure 1).
The study population was divided into five different age groups according to baseline age and sex (young (Y): <35 years; early adulthood (EA): 35-55 for men and 35-60 for women; middle adulthood (MA): 55-65 for men and 60-65 for women; young old (YO): 65-75 years; middle-to-very old (MVO): >75 years). This age grouping was selected considering the age range at which systematic cardiovascular risk evaluation is recommended (Framingham-REGICOR strategy 35-75 years) in our Health Care System, and also according to the age limit to define premature events according to sex, i.e., <55 years for men and <60 years for women (13).
At the study index date, the following data were collected from the SIDIAP database: age, sex, socioeconomic condition, the presence of diagnoses and comorbidities, including microvascular complications (retinopathy, nephropathy, polyneuropathy), and hypertension (based on registers of ICD-9/ICD-10 diagnostic codes recorded in the database) use of concomitant medications (based on the Anatomical Therapeutic Chemical-ATC classification system), blood pressure, anthropometric (body weight, height, and body mass index) and laboratory data [lipids, creatinine, urinary albumin excretion (UAE)].
Specific diagnosis codes for retinopathy, nephropathy, polyneuropathy, and hypertension are displayed in Supplementary Table 1.
Any microvascular complication was defined as the presence of a diagnostic code of retinopathy or/and nephropathy or/and polyneuropathy. Obesity was described as a body mass index ≥30 Kg/m2. The socioeconomic condition was evaluated by the MEDEA index. The MEDEA index is a socioeconomic deprivation index based on indicators recorded by census tract and validated in the Spanish population. Higher index values correspond to greater deprivation (14). The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.
Cardiovascular events involving four major conditions occurring after the index date and before the end of the study period were recorded and reported as CHD, cerebrovascular disease, PAD, and HF. CHD was defined as fatal or non-fatal myocardial infarction, angina or unstable angina, undetermined ischemic heart disease, and coronary revascularisation (coronary artery bypass grafting, percutaneous coronary intervention). Cerebrovascular disease was defined as fatal or non-fatal ischemic or hemorrhagic stroke, transient ischemic attack, and intracerebral revascularisation. PAD was defined as intermittent claudication, extracerebral artery stenosis, and carotid or peripheral revascularisation (endovascular, stenting, or surgical bypass). HF included congestive/acute HF and other HF diagnoses (systolic and diastolic, chronic, or undetermined). Diagnoses were based on ICD-9/ICD-10 codes. Specific diagnosis codes for CVD can be found in the online Supplementary information (Supplementary Table 2).
The overall mortality during the study period was also retrieved from the SIDIAP database. However, specific causes of death were not available in this study.
The baseline characteristics were described as frequencies and percentages for categorical variables, while for continuous variables, the mean and standard deviation (SD) or median and quartiles were calculated. In comparing groups (sex), the p-value was calculated using the Fisher exact test for qualitative variables and the independent samples t-test for quantitative variables. Fisher exact test and ANOVA analysis were applied when comparing age categories.
Cumulative incidence and incidence rates of cardiovascular manifestations were computed using the exact method. For each event of interest, the overall incidence rate and age-sex-specific incidence rate were calculated as the number of incident events divided by the persons-years (PY) during the follow-up and were expressed as per 100 PY. Hazard ratios (HR) and 95% confidence intervals (95% CI) were computed for each baseline characteristic. The compare Groups R Package (Version 4.6.0) 10 was used to perform group descriptions for several variables and to estimate each HR. Cox proportional hazard models were used to evaluate time to death according to the type of first-ever cardiovascular disease presentation. Hazard ratios (HR) in these models were adjusted by age and sex.
All statistical analyses were performed using the free R statistical software version 3.6.1 (https://www.r-project.org/).
The study cohort included 247,751 individuals (48.6% women) with T2D. Table 1 displays the clinical characteristics at baseline for the whole cohort and stratified by age.
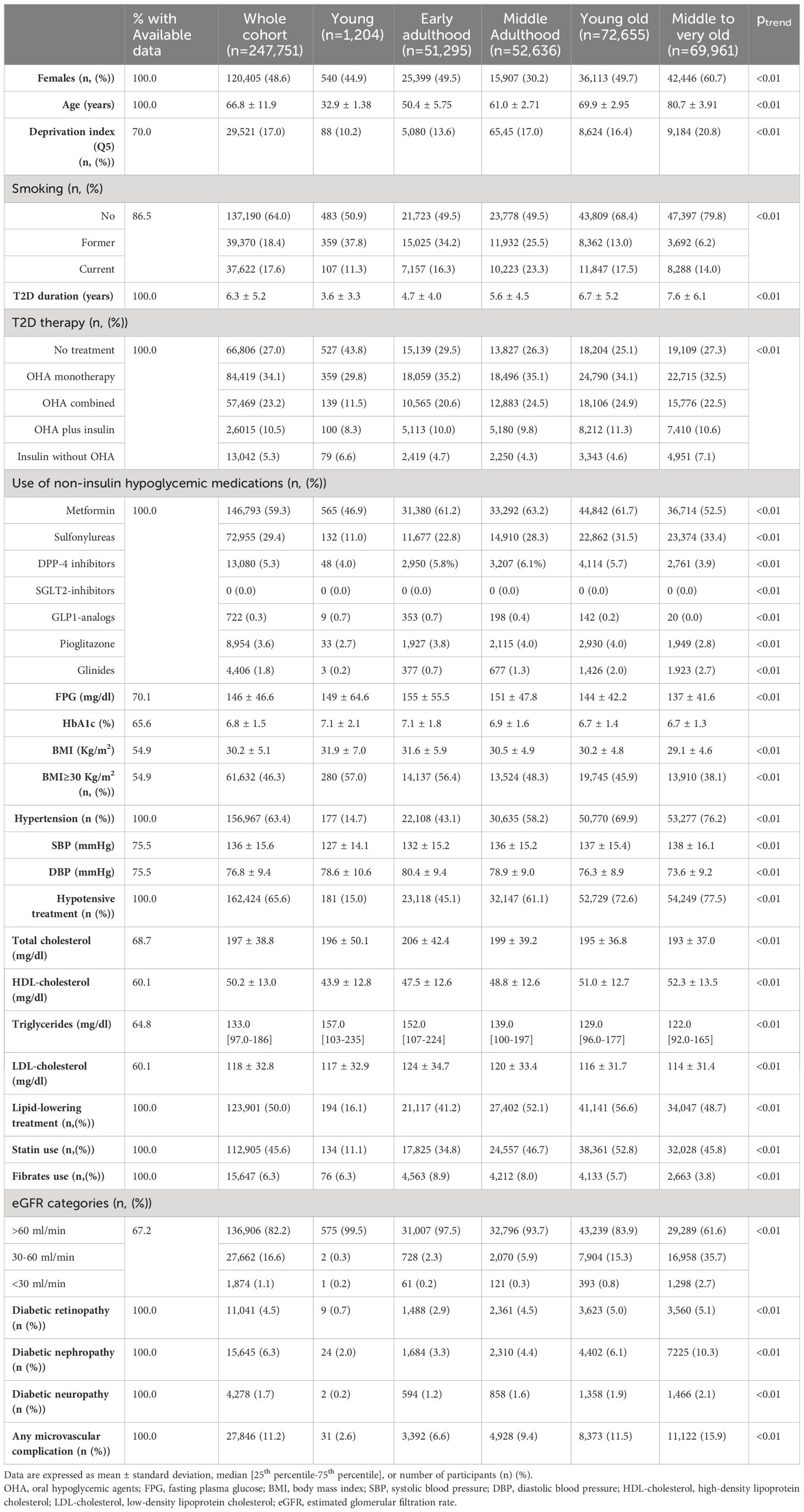
Table 1 Clinical characteristics at baseline for the whole cohort and stratified by age.
The mean age was 66.8 ± 11.9 years, HbA1c was 6.8 ± 1.5%, and body mass index (BMI) was 30.2 ± 5.1 Kg/m2. The most common treatment modalities were oral hypoglycemic agents in monotherapy or combined. Metformin (59.3%) and sulfonylureas (29.5%) were the most frequently prescribed hypoglycemic medications. In contrast, a mere 0.3% of participants utilized glucagon-like peptide 1 analogs, and none were prescribed sodium glucose transporter inhibitors (SGLT2-i). The prevalence of hypertension, statin use, current smoking, and microvascular complications was 63.4%, 45.6%, 17.6%, and 11.2%, respectively.
Compared to the older age groups, the younger groups had a higher proportion of males, a shorter diabetes duration, were less often treated with insulin, and had a lower prevalence of hypertension and microvascular complications. In contrast, they showed worse glycemic control and lipid profile, had a higher prevalence of obesity, and were less frequently treated with lipid-lowering therapies. The prevalence of active smokers was the lowest among the young, increasing until middle adulthood and decreasing after that (Table 1).
The cumulative incidence of overall CVD and its major components in men and women according to age category is displayed in Figure 1.
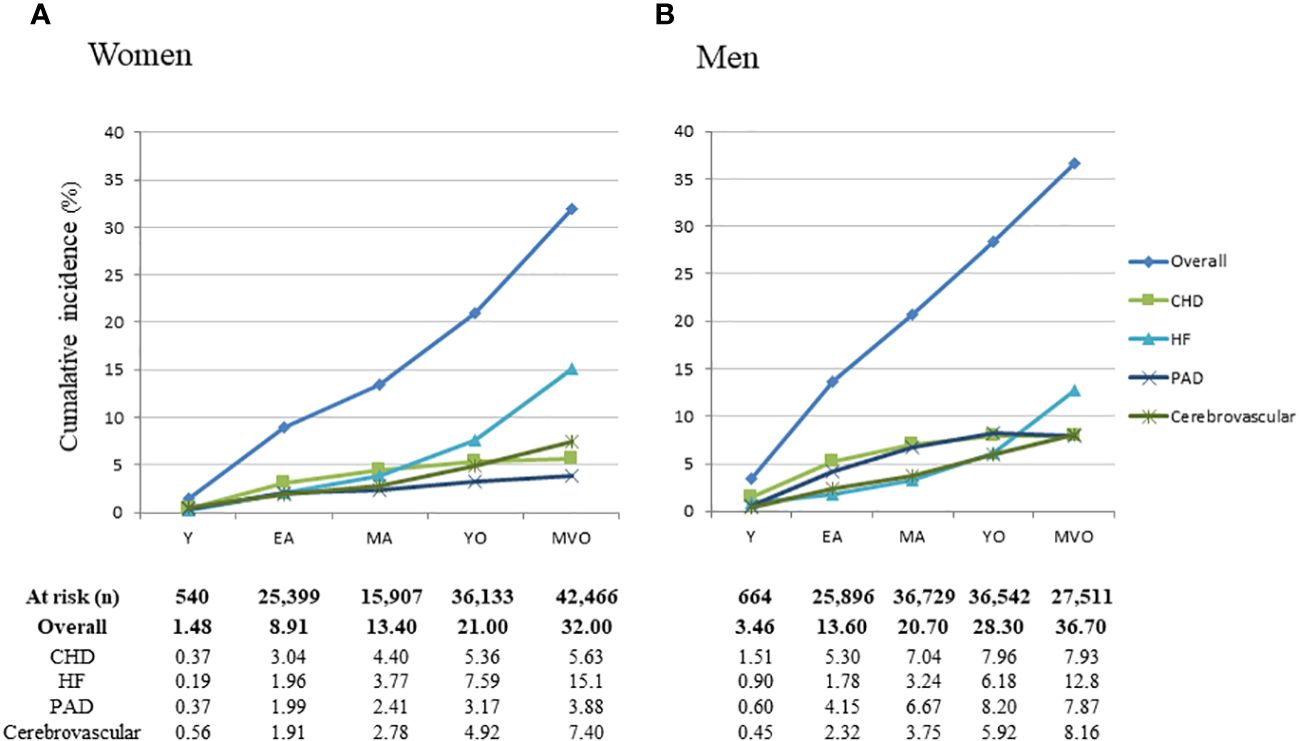
Figure 1 Cumulative incidence rates for first cardiovascular events in women (A) and men (B) by age categories. CVD, cardiovascular disease; CHD, coronary heart disease; HF, heart failure; PAD, peripheral artery disease; Y, young; EA, early adulthood; MA, middle-adulthood; YO, young old; MVO, middle to very old.
During 1,435,568 person-years, first-time cardiovascular events occurred in 57,152 individuals, corresponding to a cumulative incidence of 21.2% in women and 24.8% in men and a crude incidence rate of 3.61% per year in women and 4.34% in men (p<0.01).
The incidence of cardiovascular events increased across age categories in both men and women (ptrend<0.01), with a maximum incidence among middle to very-old adults (HR: 4.03, 95%CI: 3.91-4.16, with young as the reference). Men were at a higher absolute risk than women. The excess risk for men was the highest in young adults (HR: 2.38 (95%CI: 1.06 to 5.32) and the lowest among middle to very-old adults (HR: 1.25; 95%CI: 1.22 to 1.28).
When different CVD subtypes were considered individually, men were at higher risk than women for CHD, PAD, and cerebrovascular disease (p<0.01). In contrast, women showed a higher risk than men for HF (p<0.01) (Figures 1, 2).
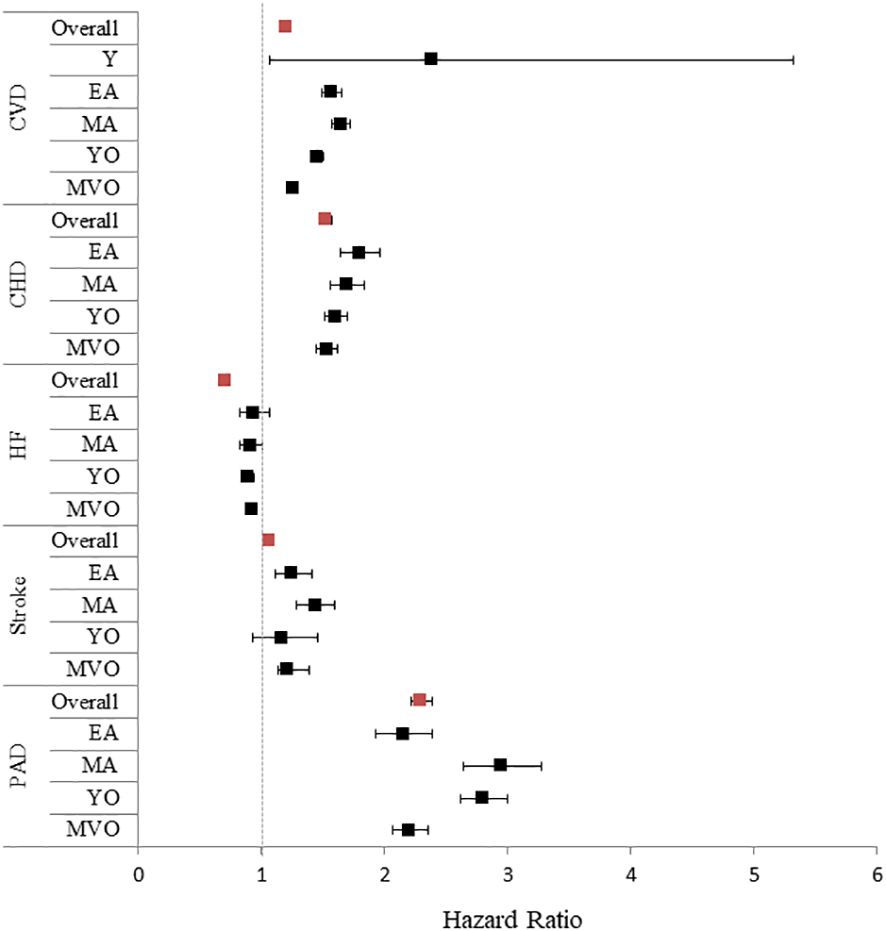
Figure 2 Forrest plot for a first cardiovascular event stratified by age in women vs. men Women were considered as the reference. Given the low number of events among the young age category, the hazard ratios for cardiovascular disease subtypes were not included in the figure. Red squares: whole cohort; black squares: pre-defined age subgroups. Y, young; EA, early adulthood; MA, middle-adulthood; YO, young old; MVO, middle to very old. CVD, cardiovascular disease; CHD, coronary heart disease; HF, heart failure; PAD, peripheral artery disease.
Figure 3; Supplementary Figure 2 display the relative contribution of cardiovascular disease main categories and specific subtypes to the first CVD event in men and women for the entire cohort and stratified by age.
In men, the most frequent CVD presentation was CHD (28.7%), followed by PAD (27.5%), while in women, HF clearly predominated (40.1%).
Furthermore, the first CVD event differed according to age in both men and women. Although more frequent among men, CHD was the most frequent first CVD manifestation in both men and women during early and middle adulthood, decreasing after that and becoming less common in older groups. Despite this reducing incidence with age, CHD remained the most frequent presentation of CVD among men below 75 years and women below 65 years. Similar trends were observed for PAD, which was much more common among men than women and more frequent among younger than older groups.
The opposite was observed for HF, which, although more common in women than men at any age, was relatively infrequent in younger age categories but markedly increased in the older groups. In women, the contribution of HF to overall CVD doubled between EA and MVO (22.0% to 47.1%), while in men, it tripled (13.3% to 34.8%), representing the most common presentation of CVD in the YO and MVO groups among women (i.e., >65 years), and the MVO group among men (i.e., >75 years). The proportion of cerebrovascular disease as the first cardiovascular event varied less with age and between sexes (18.7% to 22.7%) (Figure 3).
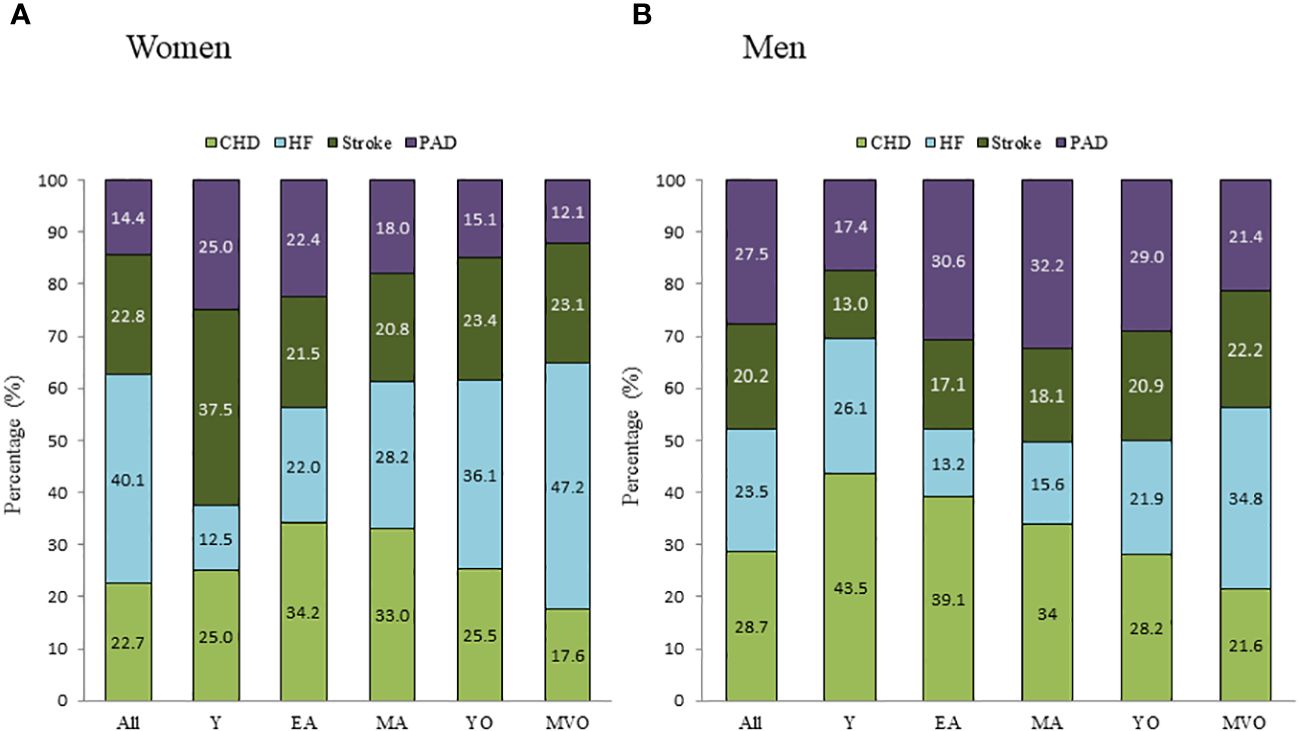
Figure 3 Distribution of the first-ever cardiovascular event subtype stratified by sex in the different age categories. (A): women; (B): men. Y, young; EA, early adulthood; MA, middle-adulthood; YO, young old; MVO, middle to very old; CVD, cardiovascular disease; CHD, coronary heart disease; HF, heart failure; PAD, peripheral artery disease.
The baseline characteristics of individuals with or without cardiovascular events during the follow-up are shown in Supplementary Table 3.
In sex-stratified analyses adjusted by age, most CVD risk factors were significantly and similarly associated with CVD in both men and women. However, compared to men, women had a higher negative impact of deprivation [HR: 1.24 (95%CI: 1.17-1.30) vs. HR: 1.12 (95%CI: 1.07-1.17)], obesity [(HR: 1.31 (95%CI: 1.26-1.35) vs. HR: 1.13 (95%CI: 1.10-1.17)], and hypertension (HR: 1.43 (95%CI: 1.38-1.47) vs. HR: 1.27 (95%CI: 1.24-1.30)] (Supplementary Figure 3), Factors more strongly associated with CVD in these analyses were those related to T2D duration, control, and complications.
In age-stratified analyses, we observed a higher relative risk associated with classical cardiovascular risk factors, metabolic control, and end-organ damage in younger vs. older individuals (Supplementary Figure 4).
During the follow-up, 20,811 men (16.3%) and 18,866 women (15.7%) died. The mean age at the time of death was 73.7 ± 10.2 years in men and 78.4 ± 8.5 years in women. Before the death date, 52.7% of deceased men and 47.9% of dead women had had a previous first cardiovascular event. The specific cause of death was not available.
In Cox regression analysis, experiencing a cardiovascular event, regardless of type, was found to be associated with elevated all-cause mortality. However, the initial occurrence of heart failure (HF) was linked to a greater risk, independently of age and sex, compared to coronary heart disease (CHD), peripheral artery disease (PAD), or cerebrovascular disease (Figure 4).
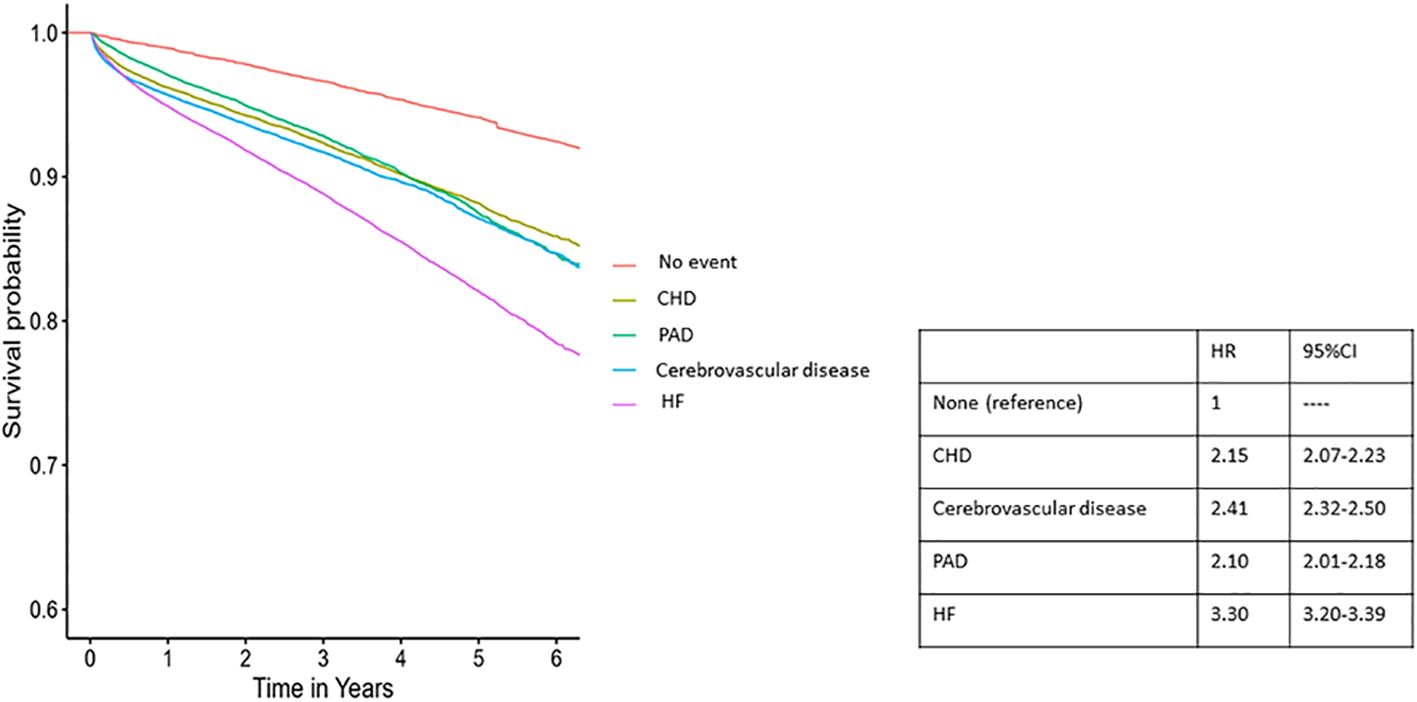
Figure 4 Survival plot for all-cause mortality according to first cardiovascular event form of manifestation and the corresponding hazard ratios CHD, coronary heart disease; HF, heart failure; PAD, peripheral artery disease.
In this longitudinal retrospective analysis of a large cohort of individuals with T2D diabetes in primary prevention from a primary care setting in a western Mediterranean region, we found that HF and PAD substantially contribute to CVD. We also observed a considerable influence of sex and age on overall cardiovascular risk and the form of the initial clinical presentation of CVD. Within our cohort, we observed that men exhibited a higher susceptibility to overall CVD, CHD, cerebrovascular disease, and PAD compared to women. However, men demonstrated a lower risk for HF across all age groups. CHD emerged as the predominant CVD presentation among men and younger individuals, whereas HF predominated among women and older participants.
We found an annual incidence rate of CVD of around 4%. This rate was similar to that reported by Shah et al. in a recent study that included 34,198 individuals with T2D free of cardiovascular disease from primary care settings in England but higher than the 1 to 2% per year observed in other studies (1, 15–20). Several factors could explain the variability between studies; however, one of the most relevant might be the number and type of outcomes included in the CVD definition. As in the study mentioned above by Shah et al. (1), we applied a broad definition that included HF and PAD. Notably, both conditions combined accounted for more than 50% of the first-ever individual events in our cohort and 1 in 3 in the study of Shah et al. (1). In contrast, in most previous works, CVD was restricted to coronary and cerebrovascular events. Only a few studies included HF (17), and even fewer included PAD (17, 19).
Our findings that HF and PAD are leading contributors to T2D cardiovascular burden reinforce the importance of considering them in routine clinical practice and risk estimation strategies.
That being said, there were considerable variations in the absolute risk for the various manifestations of CVD by sex and age.
First, as in previous studies, we observed that women had lower overall CVD risk and lower risk for atherosclerotic diseases than men, independent of age (6). In contrast, we found higher incidence rates for HF in women than men at any age. Previous studies assessing sex differences in absolute HF risk in individuals with T2D are conflicting. In older studies, a higher absolute risk was observed in men (21, 22), whereas, in more contemporary works, women showed numerically higher rates for HF than men (12, 21–23). Nonetheless, none of these studies focused primarily on first events or considered the full effect of age. Thus, our results further reinforce the importance of HF as a primary driver of CVD in women with T2D. Mechanisms explaining a higher HF risk in women are not yet fully elucidated and might include differences in cardiac structure, function, and metabolism, differential myocardial response to classical cardiovascular risk factors, and exposure in women to unique risks, such as pre-eclampsia (24–26). It should also underscored that, in our cohort, the presentation of cardiovascular disease as HF was associated with a higher risk for all-cause mortality than other CVD subtypes, independently of age and sex. These results, which are in line with previous literature suggesting a profound impact of HF on overall survival, might further reinforce the importance of strategies primarily addressing its prevention (27).
Second, although sex patterns for CVD’s first manifestation were consistent across age groups, atherosclerotic diseases, mainly CHD, accounted for most premature events in both men and women. In contrast, HF predominated in the aging population of both sexes. This finding agrees with previous epidemiological studies conducted in the general population, showing that HF is disproportionally distributed among older adults, with a prevalence that doubles for each decade of life (28).
Finally, we observed a sex-differential association between hypertension, obesity, socio-economic status, and incident cardiovascular disease. In our work, as in previous studies, the relative contribution of these factors was higher for women than for men (29, 30). Similarly, as in earlier cohort studies, in our work, the relative risk associated with classical cardiovascular risk factors, metabolic control, and end-organ damage was higher in younger vs. older individuals (31). These data have important clinical implications. First, it should help evaluate and discuss cardiovascular risks and preventive strategies in the clinical setting and facilitate shared decision-making from a more individualised perspective. Second, the evidence of large sex and age differences in CVD epidemiology and the possibility of a sex and age-differential impact of classical and non-classical cardiovascular risk factors among individuals with T2D should prompt us to evaluate the ongoing cardiovascular preventive strategies. Of note, current cardiovascular risk management in T2D is based on evidence from clinical trials mainly focused on coronary and cerebrovascular disease prevention conducted in predominantly middle-aged populations where women were frequently underrepresented (32–36). Although this approach has been proven to be highly effective in diminishing cardiovascular morbidity and mortality, T2D-related cardiovascular burdens might be further reduced by considering sex and age-specific risks and by modulating medical interventions in accordance.
In this regard, hypertension treatment dramatically reduces the incidence of HF and stroke but has a smaller impact on CHD (37, 38). Furthermore, observational data suggested that cardiovascular risk in women rises at lower blood pressure thresholds and that hypertension might confer a greater risk for HF in women than in men (30). In this same line, the recent Systolic Blood Pressure Intervention Trial (SPRINT), which unfortunately excluded participants with T2D, suggested a more significant benefit of lowering blood pressure goals in older vs. younger participants (37). On the other hand, lowering LDL-cholesterol dose-dependently decreases the incidence of atherosclerotic events, especially CHD (39). However, statin treatment is associated with limited improvements in preventing first non-fatal HF hospitalisations (40). Finally, the relative benefits of the newest T2D therapies vary. While sodium-glucose transport type 2 inhibitors have been shown to significantly impact HF, the cardiovascular benefits of glucagon-like peptide 1 agonists mostly rely on preventing atherosclerotic diseases (41). Thus, it could be speculated that the absolute cardiovascular benefits of these newer therapies might also vary by age and sex. Unfortunately, no clinical trials have been designed to primarily explore sex or age-specific targets or therapies for CVD prevention. Our findings further reinforce the need to fill this lack of evidence on these clinically relevant issues.
Our study has several limitations. First, diagnoses were recorded by treating physicians based on ICD-9/ICD-10 codes. Thus, some inter-individual variability in definitions cannot be excluded. Also, over 23% of Catalonians receive health care outside the National Health Care System (Institut Català de la Salut) due to health agreements between the government and the private sector. This population is not included in the SIDIAP database. Nonetheless, the data quality of the SIDIAP database has been previously validated, and more specifically, data on CVD has proven to be of high quality and suitable for epidemiological studies (42, 43). Second, there was a substantial proportion of missing values for some variables (including BMI, blood pressure, or lipid profile). Therefore, the analysis assessing the association between risk factors and cardiovascular disease should be interpreted cautiously. Thirdly, it’s important to note that in Spain, sodium-glucose transporters 2 inhibitors and long-acting glucagon-like 1 peptide analogs were not accessible at the baseline study date, and our dataset does not extend beyond 2016. Therefore, we cannot assess whether these newer agents’ prescriptions might impact cardiovascular disease incidence and presentation. However, it is worth highlighting that the utilization of these advanced therapies remains minimal within the Catalonian population. As of 2018, their usage had stayed within 5% (41). Further studies comparing cardiovascular disease and its main subtypes incidence before and after full implementation of SGLT2-i and GLP1-analogs in the clinical practice help to delineate their impact in a real-world setting. Finally, the specific cause of death was only available for a limited proportion of study participants.
In conclusion, our study demonstrated that HF and PAD are significant contributors to cardiovascular disease burden in subjects with T2D and that, as in the general population, in women and older individuals, CVD more frequently manifests as HF. This epidemiological evidence should be considered in clinical practice and risk estimation strategies and might be relevant in designing future clinical trials.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
The Ethics Committee of the Primary Healthcare University Research Institute (IDIAP), Jordi Gol (Barcelona, Spain), approved the study (code P17/087). The study was conducted in accordance with the local legislation and institutional requirements. Minimal risk research permitted the authors to conduct the investigation without obtaining informed consent from patients. Data was anonymized and is untraceable.
AJ: Writing – original draft. BV: Data curation, Methodology, Writing – review & editing. MM: Conceptualization, Investigation, Writing – review & editing. JR: Formal analysis, Methodology, Writing – review & editing. DM: Conceptualization, Funding acquisition, Investigation, Writing – review & editing. JF: Conceptualization, Funding acquisition, Investigation, Writing – review & editing. EO: Conceptualization, Funding acquisition, Investigation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This project has been funded by Generalitat de Catalunya, Departament de Salut, Pla estratègic de recerca i innovació en salut 2016-2020 (SLT002/16/00095). This research was also supported by the Center for Biomedical Research on Diabetes and Associated Metabolic Diseases (CIBERDEM; group CB15/00071) and the Center for Biomedical Research on Physiopathology of Obesity and Nutrition (CIBEROBN), both from Instituto de Salud Carlos III, Barcelona, Spain.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2024.1344007/full#supplementary-material
BMI, body mass index; CHD, coronary heart disease; CVD, cardiovascular disease; EA, early adulthood; eGFR, estimated glomerular filtration rate; HF, heart failure; HR, hazard ratio; MA, middle adulthood; MVO, middle to very old; PAD, peripheral artery disease; UAE, urinary albumin excretion; Y, young; YO, young, old.
1. Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1·9 million people. Lancet Diabetes Endocrinol. (2015) 3:105–13. doi: 10.1016/S2213-8587(14)70219-0
2. Sattar N, McMurray J, Boren J, Rawshani A, Omerovic E, Berg N, et al. Years of cardiovascular complications and risk factors in patients with type 2 diabetes: A nationwide Swedish cohort study. Circulation. 147(25):1872–86. doi: 10.1161/CIRCULATIONAHA.122.063374
3. Lababidi H, Salerno PR, Wass SY, Shafiabadi Hasani N, Bourges-Sevenier B, Al-Kindi S. The Global Burden of premature cardiovascular disease, 1990-2019. Int J Cardiol Cardiovasc Risk Prev. (2023) 19:200212. doi: 10.1016/j.ijcrp.2023.200212
4. Geraghty L, Figtree GA, Schutte AE, Patel S, Woodward M, Arnott C. Cardiovascular disease in women: from pathophysiology to novel and emerging risk factors. Heart Lung Circ. (2021) 30:9–17. doi: 10.1016/j.hlc.2020.05.108
5. Leening MJG, Ferket BS, Steyerberg EW, Kavousi M, Deckers JW, Nieboer D, et al. Sex differences in lifetime risk and first manifestation of cardiovascular disease: prospective population based cohort study. BMJ. (2014) 349. doi: 10.1136/bmj.g5992
6. Malmborg M, Schmiegelow MDS, Nørgaard CH, Munch A, Gerds T, Schou M, et al. Does type 2 diabetes confer higher relative rates of cardiovascular events in women compared with men? Eur Heart J. (2020) 41:1346–53. doi: 10.1093/eurheartj/ehz913
7. Al-Salameh A, El bouzegaoui N, Saraval-Gross M. Diabetes and cardiovascular risk according to sex: An overview of epidemiological data from the early Framingham reports to the cardiovascular outcomes trials. Ann Endocrinol (Paris). (2023) 84:57–68. doi: 10.1016/j.ando.2022.09.023
8. Kalyani RR, Lazo M, Ouyang P, Turkbey E, Chevalier K, Brancati F, et al. Sex differences in diabetes and risk of incident coronary artery disease in healthy young and middle-aged adults. Diabetes Care. (2014) 37:830–8. doi: 10.2337/dc13-1755
9. Chase-Vilchez AZ, Chan IHY, Peters SAE, Woodward M. Diabetes as a risk factor for incident peripheral arterial disease in women compared to men: a systematic review and meta-analysis. Cardiovasc Diabetol. (2020) 19:151. doi: 10.1186/s12933-020-01130-4
10. Dong X, Cai R, Sun J, Huang R, Wang P, Sun H, et al. Diabetes as a risk factor for acute coronary syndrome in women compared with men: a meta-analysis, including 10 856 279 individuals and 106 703 acute coronary syndrome events. Diabetes Metab Res Rev. (2017) 33(5). doi: 10.1002/dmrr.2887
11. Peters TM, Holmes MV, Brent Richards J, Palmer T, Forgetta V, Lindgren CM, et al. Sex differences in the risk of coronary heart disease associated with type 2 diabetes: A mendelian randomization analysis. Diabetes Care. (2021) 44:556–62. doi: 10.2337/dc20-1137
12. Shen Y, Shi L, Nauman E, Katzmarzyk PT, Price-Haywood EG, Yin P, et al. Race and sex differences in rates of diabetic complications. J Diabetes. (2019) 11:449–56. doi: 10.1111/1753-0407.12869
13. Patel J, Al Rifai M, Scheuner MT, Shea S, Blumenthal RS, Nasir K, et al. Basic vs more complex definitions of family history in the prediction of coronary heart disease: the multi-ethnic study of atherosclerosis. Mayo Clin Proc. (2018) 93:1213–23. doi: 10.1016/j.mayocp.2018.01.014
14. Domínguez-Berjón MF, Borrell C, Cano-Serral G, Esnaola S, Nolasco A, Pasarín MI, et al. [Constructing a deprivation index based on census data in large Spanish cities(the MEDEA project)]. Gac Sanit. (2008) 22:179–87. doi: 10.1157/13123961
15. Basu S, Sussman JB, Berkowitz SA, Hayward RA, Yudkin JS. Development and validation of Risk Equations for Complications Of type 2 Diabetes (RECODe) using individual participant data from randomised trials. Lancet Diabetes Endocrinol. (2017) 5:788–98. doi: 10.1016/S2213-8587(17)30221-8
16. Berkelmans GFN, Gudbjörnsdottir S, Visseren FLJ, Wild SH, Franzen S, Chalmers J, et al. Prediction of individual life-years gained without cardiovascular events from lipid, blood pressure, glucose, and aspirin treatment based on data of more than 500 000 patients with Type 2 diabetes mellitus. Eur Heart J. (2019) 40:2899–906. doi: 10.1093/eurheartj/ehy839
17. Davis WA, Hellbusch V, Hunter ML, Bruce DG, Davis TME. Contemporary cardiovascular risk assessment for type 2 diabetes including heart failure as an outcome: the fremantle diabetes study phase II. J Clin Med. (2020) 9(5):1428. doi: 10.3390/jcm9051428
18. Mata-Cases M, De Prado-Lacueva C, Salido-Valencia V, Fernández-Bertolín E, Casermeiro-Cortés J, García-Durán M, et al. Incidence of complications and mortality in a type 2 diabetes patient cohort study followed up from diagnosis in a primary healthcare centre. Int J Clin Pract. (2011) 65:299–307. doi: 10.1111/ijcp.2011.65.issue-3
19. Piniés JA, González-Carril F, Arteagoitia JM, Irigoien I, Altzibar JM, Rodriguez-Murua JL, et al. Development of a prediction model for fatal and non-fatal coronary heart disease and cardiovascular disease in patients with newly diagnosed type 2 diabetes mellitus: the Basque Country Prospective Complications and Mortality Study risk engine (BASCORE). Diabetologia. (2014) 57:2324–33. doi: 10.1007/s00125-014-3370-1
20. Pylypchuk R, Wells S, Kerr A, Poppe K, Harwood M, Mehta S, et al. Cardiovascular risk prediction in type 2 diabetes before and after widespread screening: a derivation and validation study. Lancet. (2021) 397:2264–74. doi: 10.1016/S0140-6736(21)00572-9
21. Gottdiener JS, Arnold AM, Aurigemma GP, Polak JF, Tracy RP, Kitzman DW, et al. Predictors of congestive heart failure in the elderly: the Cardiovascular Health Study. J Am Coll Cardiol. (2000) 35:1628–37. doi: 10.1016/S0735-1097(00)00582-9
22. He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK. Risk factors for congestive heart failure in US men and women: NHANES I epidemiologic follow-up study. Arch Intern Med. (2001) 161:996–1002. doi: 10.1001/archinte.161.7.996
23. Zinman B, Inzucchi SE, Wanner C, Hehnke U, George JT, Johansen OE, et al. Empagliflozin in women with type 2 diabetes and cardiovascular disease – an analysis of EMPA-REG OUTCOME®. Diabetologia. (2018) 61:1522–7. doi: 10.1007/s00125-018-4630-2
24. Beale AL, Meyer PMD, Marwick TH, Lam CSP, Kaye DM. Sex differences in cardiovascular pathophysiology: why women are overrepresented in heart failure with preserved ejection fraction. Circulation. (2018) 138:198–205. doi: 10.1161/CIRCULATIONAHA.118.034271
25. Gori M, Lam CSP, Gupta DK, Santos ABS, Cheng S, Shah AM, et al. Sex-specific cardiovascular structure and function in heart failure with preserved ejection fraction. Eur J Heart Fail. (2014) 16:535–42. doi: 10.1002/ejhf.67
26. Scantlebury DC, Borlaug BA. Why are women more likely than men to develop heart failure with preserved ejection fraction? Curr Opin Cardiol. (2011) 26:562–8. doi: 10.1097/HCO.0b013e32834b7faf
27. Shah KS, Xu H, Matsouaka RA, Bhatt DL, Heidenreich PA, Hernandez AF, et al. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J Am Coll Cardiol. (2017) 70:2476–86. doi: 10.1016/j.jacc.2017.08.074
28. Ziaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nat Rev Cardiol. (2016) 13:368–78. doi: 10.1038/nrcardio.2016.25
29. Joseph JJ, Williams A, Azap RA, Zhao S, Brock G, Kline D, et al. Role of sex in the association of socioeconomic status with cardiovascular health in black Americans: the jackson heart study. J Am Heart Assoc. (2023) 12(23):e030695. doi: 10.1161/JAHA.123.030695
30. Ji H, Niiranen TJ, Rader F, Henglin M, Kim A, Ebinger JE, et al. Sex differences in blood pressure associations with cardiovascular outcomes. Circulation. (2021) 143:761–3. doi: 10.1161/CIRCULATIONAHA.120.049360
31. Antza C, Gallo A, Boutari C, Ershova A, Gurses KM, Lewek J, et al. Prevention of cardiovascular disease in young adults: Focus on gender differences. A collaborative review from the EAS Young Fellows. Atherosclerosis. (2023) 384:117272. doi: 10.1016/j.atherosclerosis.2023.117272
32. Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, Reaven PD, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. (2009) 360:129–39. doi: 10.1056/NEJMoa0808431
33. Patel A, ADVANCE Collaborative Group, MacMahon S, Chalmers J, Neal B, Woodward M, Billot L, et al. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet. (2007) 370:829–40. doi: 10.1016/S0140-6736(07)61303-8
34. ADVANCE Collaborative Group, Patel A, MacMahon S, Chalmers J, Neal B, Billot L, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. (2008) 358:2560–72. doi: 10.1056/NEJMoa0802987
35. Action to Control Cardiovascular Risk in Diabetes Study Group, Gerstein HC, Miller ME, Byington RP, Goff DC Jr, Bigger JT, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. (2008) 358:2545–59. doi: 10.1056/NEJMoa0802743
36. Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HAW, Livingstone SJ, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): Multicentre randomised placebo-controlled trial. Lancet. (2004) 364:685–96. doi: 10.1016/S0140-6736(04)16895-5
37. SPRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. (2015) 373:2103–16. doi: 10.1056/NEJMoa1511939
38. Mefford MT, Goyal P, Howard G, Durant RW, Dunlap NE, Safford MM, et al. The association of hypertension, hypertension duration, and control with incident heart failure in black and white adults. J Clin Hypertens. (2020) 22:857–66. doi: 10.1111/jch.13856
39. Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. (2010) 376:1670–81. doi: 10.1016/S0140-6736(10)61350-5
40. Preiss D, Campbell RT, Murray HM, Ford I, Packard CJ, Sattar N, et al. The effect of statin therapy on heart failure events: a collaborative meta-analysis of unpublished data from major randomized trials. Eur Heart J. (2015) 36:1536–46. doi: 10.1016/j.atherosclerosis.2015.04.086
41. Palmer SC, Tendal B, Mustafa RA, Vandvik PO, Li S, Hao Q, et al. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ. (2021) 372:m4573. doi: 10.1136/bmj.m4573
42. Ramos R, Balló E, Marrugat J, Elosua R, Sala J, Grau M, et al. Validity for use in research on vascular diseases of the SIDIAP (Information System for the Development of Research in Primary Care): the EMMA study. Rev Esp Cardiol (Engl Ed). (2012) 65:29–37. doi: 10.1016/j.rec.2011.07.016
Keywords: first cardiovascular event, primary prevention, heart failure, peripheral artery disease, sex difference, age-related, cumulative incidence
Citation: Jiménez A, Vlacho B, Mata-Cases M, Real J, Mauricio D, Franch-Nadal J and Ortega E (2024) Sex and age significantly modulate cardiovascular disease presentation in type 2 diabetes: a large population-based cohort study. Front. Endocrinol. 15:1344007. doi: 10.3389/fendo.2024.1344007
Received: 24 November 2023; Accepted: 01 May 2024;
Published: 17 May 2024.
Edited by:
Maria Pompea Antonia Baldassarre, G. d’Annunzio University of Chieti and Pescara, ItalyReviewed by:
Anoop Titus, Houston Methodist Hospital, United StatesCopyright © 2024 Jiménez, Vlacho, Mata-Cases, Real, Mauricio, Franch-Nadal and Ortega. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emilio Ortega, RU9SVEVHQTFAY2xpbmljLmNhdA==; Josep Franch-Nadal, am9zZXAuZnJhbmNoQGdtYWls
†These authors contributed equally to this work and shared first authorship
‡These authors contributed equally to this work and shared senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.