 Huiling An1,2,3
Huiling An1,2,3 Jun Zhai
Jun Zhai
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 19 February 2024
Sec. Reproduction
Volume 15 - 2024 | https://doi.org/10.3389/fendo.2024.1314432
Background: Although in vitro fertilization (IVF) in infertile patients with endometrial hyperplasia is common after drug treatment, the pregnancy outcomes are often unsatisfactory. Till date, no studies have reported the outcome of patients with endometrial hyperplasia treated using early-follicular long (EL) protocol and midluteal long (ML) protocol.
Objective: To evaluate the pregnancy outcomes and disease prognosis of patients with endometrial hyperplasia with or without atypia undergoing IVF treatment with EL protocol or ML protocol.
Methods: This was a retrospective study in university-affiliated reproductive medical center. A total of 138 patients with endometrial hyperplasia undergoing IVF treatment were included to compare the pregnancy outcomes and disease prognosis between EL and ML protocols. We further matched 276 patients with normal endometrium to compare the pregnancy outcomes between patients with endometrial hyperplasia and patients with normal endometrium under different controlled ovarian stimulation (COS) protocol.
Results: In patients with endometrial hyperplasia, the clinical pregnancy rate (CPR) and live birth rate (LBR) were significantly higher in EL protocol than in ML protocol (61.8% vs. 43.5%, P=0.032; 50.0% vs. 30.6%, P= 0.022). In the ML protocol, patients with endometrial hyperplasia had significantly lower CPR and LBR than those with normal endometrium (43.5% vs. 59.7%, P=0.037; 30.6% vs. 49.2%, P=0.016). While in the EL protocol, they achieved similar CPR and LBR as patients with normal endometrium (61.8% vs. 69.7%, P=0.232; 50.0% vs. 59.9%, P=0.156). In patients with endometrial hyperplasia, COS protocol was an independent factor affecting clinical pregnancy (adjusted odds ratio [OR] 2.479; 95% confidence interval [CI] 1.154-5.327) and live birth (adjusted OR 2.730; 95% CI 1.249-5.966). After 1–10 years of follow-up, no significant difference was found in the recurrence rate of endometrial lesions between both treatment groups.
Conclusions: For patients with endometrial hyperplasia undergoing IVF treatment, the EL protocol is superior to ML protocol, and in the EL protocol, they can achieve similar pregnancy outcomes as patients with normal endometrium.
Endometrial hyperplasia is defined as irregularity and cystic expansion of glands (simple) or crowding and budding of glands (complex) without worrisome changes in the appearance of individual gland cells (1, 2). The underlying cause of the hyperplasia is a relative predominance of estrogen combined with insufficient progesterone levels (2). In 2014, based on the presence or absence of cellular atypia, endometrial hyperplasia was categorized into two types by the World Health Organization: endometrial hyperplasia without atypia (EH) and endometrial atypical hyperplasia (EAH) (1). EAH is a recognized precancerous condition called endometrial intraepithelial neoplasia (EIN) (1, 3). The frequency of endometrial hyperplasia found in infertile women undergoing in vitro fertilization (IVF) treatment for the first time is approximately 3% (4). Prior studies have reported that complete remission of endometrial hyperplasia can be achieved in up to 80% - 90% patients using high-efficiency progesterone treatment (5, 6).
Patients with endometrial hyperplasia complicated with infertility often need assisted reproductive technology (ART) for achieving pregnancy, but studies found that irrespective of the use of midluteal long (ML) protocol or gonadotropin-releasing hormone (GnRH) antagonist protocol for controlled ovarian stimulation (COS), the pregnancy outcomes of the patients with endometrial hyperplasia were significantly lower than those of the patients with normal endometrium (7, 8). At the same time, due to concerns that the increase in estrogen (E2) level during COS would increase the risk of recurrence of endometrial lesions, Azim et al. (9) suggested to choose the mild stimulation protocol or the combination of letrozole during COS to reduce E2 level. However, the mild stimulation protocol usually resulted in fewer oocytes retrieved and embryos available. For protecting the endometrium, Chen et al. adopted progestin primed ovarian stimulation (PPOS) protocol, and compared the curative effect with the mild stimulation protocol in the freeze-thaw cycle (10). They found that PPOS protocol provided higher clinical pregnancy rate (CPR) compared to mild stimulation protocol (40.54%vs. 9.38%) (10). However, the disadvantage of the PPOS protocol is that fresh embryo transfer cannot be performed, which increases the economic burden of the patients and delays the time for the patients to reach pregnancy. Therefore, further research is urgently needed to explore the optimal COS protocol for these patients.
In recent years, because the early-follicular long (EL) protocol has shown better pregnancy outcomes and can reduce the risk of ovarian hyperstimulation syndrome (OHSS), it has gradually become the predominant choice in many reproductive centers in China. Xu et al. (11) showed that in the normal population, the LBR of EL protocol was significantly higher than that of ML protocol and GnRH antagonist protocol in fresh embryo transfer cycles (62.6% vs. 52.1% vs. 45.6%). In the process of COS, since the E2 level on trigger day was lower in the EL protocol than ML protocol, it may be more beneficial to patients with endometrial hyperplasia. To the best of our knowledge, till date, no studies have reported pregnancy outcomes of patients with endometrial hyperplasia treated using EL protocol. This study retrospectively collected the data of infertile patients with endometrial hyperplasia undergoing IVF/ICSI treatment in the Reproductive Medicine Center of our hospital, and compared the effects of EL protocol and ML protocol on pregnancy outcomes and disease prognosis, to optimize a COS protocol for these patients.
In this retrospective cohort study, we analyzed the clinical data of patients undergoing their first IVF cycle at Reproductive Medicine Center of the public university hospital between January 2011 and January 2021. This research was approved by Institutional Review Board (2023-KY-0236-001). The requirement for informed consent was waived due to the retrospective character of this study.
Inclusion criteria: 1. age 20–40 years, 2. underwent the first IVF cycle and fresh embryo transfer. Exclusion criteria: 1. uterine malformation; 2. uterine submucosal fibroids; 3. intrauterine adhesions; 4. endometriosis or adenomyosis; 5. serious endocrine diseases; 6. untreated hydrosalpinx; 7. preimplantation genetic testing, and 8. severe oligozoospermia or teratozoospermia in the male partner.
A total of 138 patients with endometrial hyperplasia (EH: 114 cases; EAH/EIN: 24 cases) who were completely relieved after drug treatment were included to compare the pregnancy outcomes and disease prognosis between EL and ML protocols. According to age ± 2 (years), body mass index (BMI) ± 2 (kg/m2), and COS protocol, we further matched 276 patients with normal endometrium to compare the pregnancy outcomes between patients with endometrial hyperplasia and patients with normal endometrium under different COS protocol. We defined patients with normal endometrium based on normal morphological diagnosis under hysteroscopy and normal pathological reports after endometrial biopsy. The flow chart of the study is presented in Figure 1.

Figure 1 Flowchart describing the study population.
Patients with EH were prescribed megestrol acetate (Qingdao Guohai Biological Pharmaceutical Co., Ltd., China), 160 mg/day orally, and ultrasound examination and endometrial biopsy were performed every 6 months during treatment until no endometrial lesions was found in two consecutive endometrial biopsies (12). Patients with EAH/EIN were treated with lesion resection under the guidance of hysteroscopy, followed by treatment with levonorgestrel intrauterine system (Mirena; Bayer Oy) and/or megestrol acetate (160–320 mg/day), and ultrasound examination and endometrial biopsy were performed every 3 months during treatment until no endometrial lesions was found in two consecutive endometrial biopsies (13). Patients were transferred to a reproductive center for treatment after complete remission.
EL protocol: On the 2nd or 3rd day of menstruation, patients were administered once 3.75 mg of the long-acting GnRH agonist (Diphereline; Beaufour Ipsen, Dreux, France). Serum follicle-stimulating hormone (FSH), luteinizing hormone (LH), estrogen (E2), and progesterone (P) were measured 28 days after injection. Follicle size was monitored using transvaginal ultrasound. ML protocol: On the 21st or 22nd day of the menstrual cycle, patients were administered 0.1 mg of the short-acting GnRH agonist (Triptorelin; IPSEN Biotechnology, France) for 14–16 days. Serum FSH, LH, E2, and P were measured after injection, meanwhile follicular size was monitored by vaginal ultrasound.
Gonadotropin (Gn) (Gonal-f; Merck Serono, Darmstadt, Germany) was used to promote multiple synchronized development and maturation of follicles once the downregulation criteria were reached in both protocols with serum FSH level suppressed to <5 mIU/mL, LH level <3 mIU/mL, E2 level <50 pg/mL, antral follicle diameter about 3–5 mm, and no ovarian cysts with diameter >10 mm. The dosage of Gn was adjusted in accordance with the blood hormone levels and follicle size.
When the diameter of three dominant follicles were ≥18 mm or the proportion of follicles with diameters >16 mm accounted for more than two-thirds of the total follicles, hCG (2000 IU, Livzon Pharmaceutical, China) were administered. Oocytes were extracted by puncture under the guidance of vaginal ultrasound at 36-37 h after the hCG trigger injection.
Embryo transfer was carried out 3-5 days following oocyte retrieval according to the embryo quality, endometrial status, and general health of the patients.
Follow-up was conducted through telephone until June 2022. Pregnancy outcomes, neonatal weight, and recurrence of endometrial lesions over 1–10 years were collected.
Pregnancy-induced hypertension (PIH): new onset of hypertension after 20 weeks of pregnancy (14); Low birth weight (LBW): birth weight less than 2,500 g; Recurrence of endometrial lesions: the reappearance of EH, EAH/EIN, or progression to endometrial carcinoma during IVF treatment or follow-up after IVF. Implantation rate (number of gestational sacs observed/number of embryos transplanted×100%); CPR (number of clinical pregnancies/number of transplant cycles×100%); LBR (number of deliveries that resulted in at least one live born baby/number of transplant cycles×100%) (15). Adverse pregnancy outcomes include abortion, preterm birth (PTB), gestational diabetes (GDM), PIH, premature rupture of membranes (PROM) (16); Adverse pregnancy outcomes rate (number of women with adverse pregnancy outcomes/number of clinical pregnancies×100%); LBW rate (number of deliveries with at least one LBW infant/number of deliveries×100%) (17, 18).
SPSS 25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp) was used for all analyses. Categorical variables are given as percentages, whereas continuous variables are expressed as the mean ± standard deviation (x ± s). To compare differences in the mean values of continuous variables, the t-test was used, while the Chi-square (X2) test was used to compare categorical variables. Univariate logistic regression was performed on variables that may affect clinical pregnancy and live birth in patients with endometrial hyperplasia, and multivariate logistic regression was performed on variables found to be significant after univariate logistic regression and variables considered significant in previous literature. The threshold for statistical significance was set at P<0.050.
In patients with endometrial hyperplasia, the proportion of blastocyst stage embryo was significantly higher in EL protocol than in ML protocol (25.0%vs. 11.3%, P=0.040). In the EL protocol, the basal E2 level and the proportion of primary infertility were significantly higher in patients with endometrial hyperplasia than in patients with normal endometrium (51.85 ± 31.29vs. 39.69 ± 29.04 pg/ml, P=0.005; 68.4%vs. 54.6%, P=0.045) (Table 1).
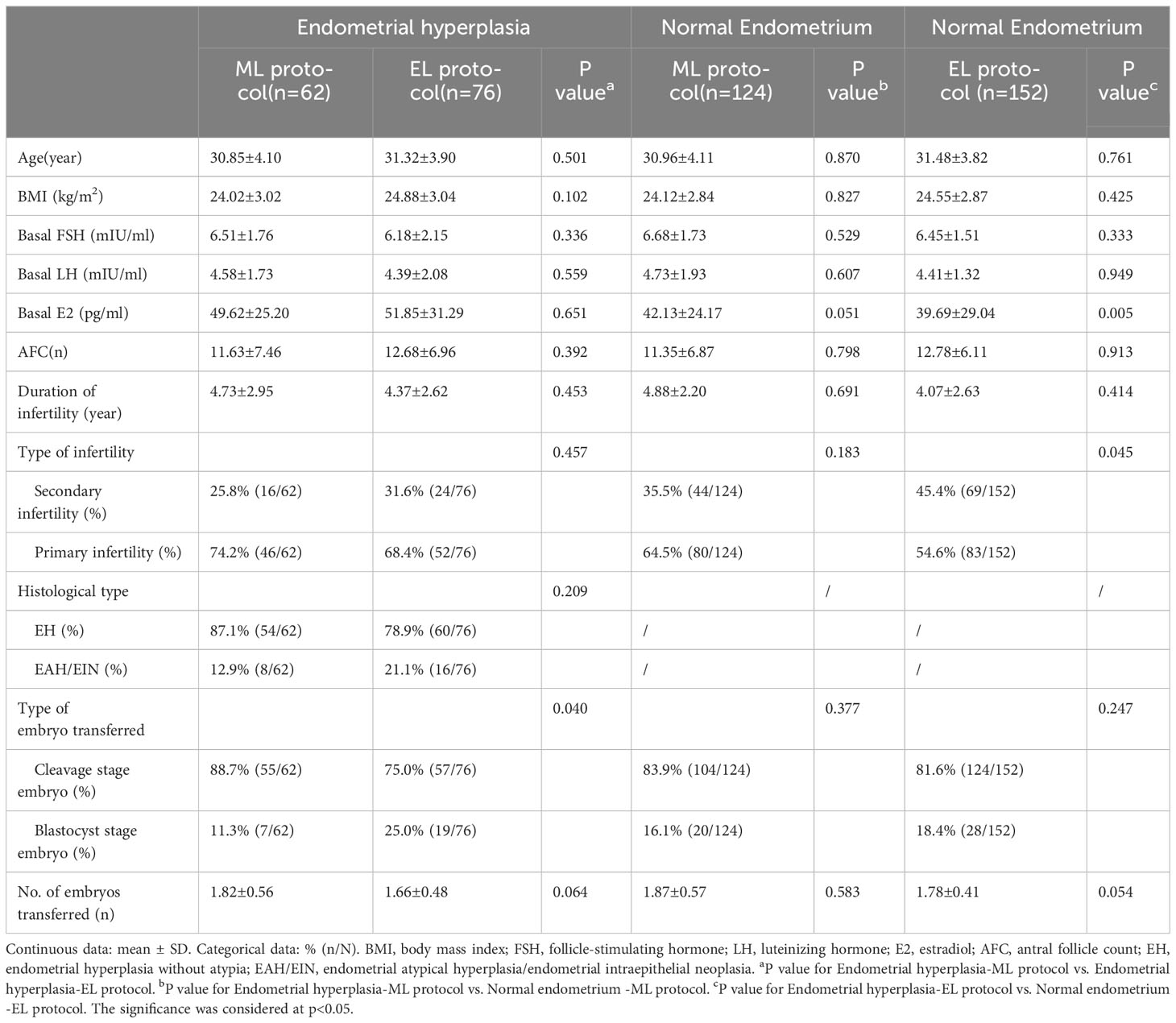
Table 1 Comparison of patients’ general characteristics.
In patients with endometrial hyperplasia, the implantation rate, the CPR and LBR were significantly higher in EL protocol than in ML protocol (49.2%vs. 31.9%, P=0.006; 61.8% vs. 43.5%, P=0.032; 50.0% vs. 30.6%, P= 0.022). There was no significant difference in the number of oocytes retrieved between EL and ML protocols, but the E2 level and LH level on trigger day of EL protocol were significantly lower (2133.91 ± 1329.37vs. 4152.90 ± 2431.81 pg/ml, P=0.001; 0.73 ± 0.68mIU/mL vs. 1.83 ± 0.87mIU/mL, P=0.001). In the ML protocol, patients with endometrial hyperplasia had significantly lower CPR and LBR than those with normal endometrium (43.5% vs. 59.7%, P=0.037; 30.6% vs. 49.2%, P=0.016). While in the EL protocol, patients with endometrial hyperplasia achieved similar CPR and LBR as patients with normal endometrium (61.8% vs. 69.7%, P=0.232; 50.0% vs. 59.9%, P=0.156). No matter in ML or EL protocol, the endometrial thickness on trigger day of patients with endometrial hyperplasia was significantly thinner than that of patients with normal endometrium (11.26 ± 2.08vs. 12.50 ± 2.74 mm, P=0.001; 11.43 ± 2.48vs. 12.73 ± 2.48 mm, P=0.001). No significant differences were found in terms of the number of high-quality embryos, adverse pregnancy outcomes rate, neonatal weight, or recurrence rate of endometrial lesions (Table 2).
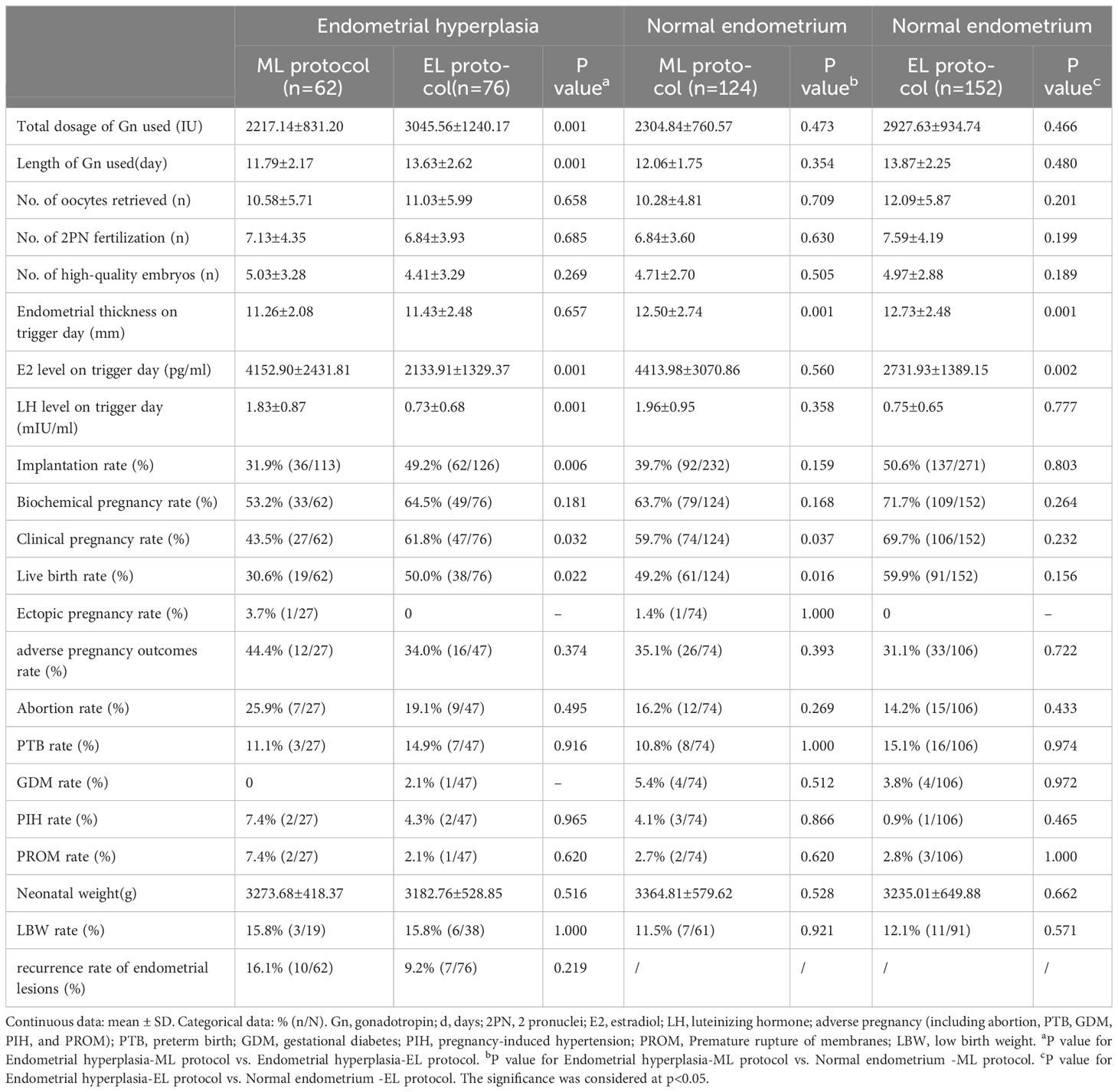
Table 2 Comparison of laboratory parameters and clinical outcomes.
Age, type of infertility (reference: secondary infertility), COS protocol (reference: ML protocol), endometrial thickness on trigger day, type of embryo transferred (reference: cleavage stage embryo), histological type (reference: EH), and number of embryos transferred were included for the multivariate logistic regression. The multivariate logistic regression results are shown in Figures 2, 3. COS protocol (adjusted odds ratio [OR] 2.479; 95% confidence interval [CI] 1.154-5.327), type of embryo transferred (adjusted OR 5.622; 95% CI 1.199-26.362), and number of embryos transferred (adjusted OR 8.542; 95% CI 2.319-31.466) were independent factors affecting clinical pregnancy. COS protocol (adjusted OR 2.730; 95% CI 1.249-5.966), number of embryos transferred (adjusted OR 4.298; 95% CI 1.316-14.035) were independent factors affecting live birth.
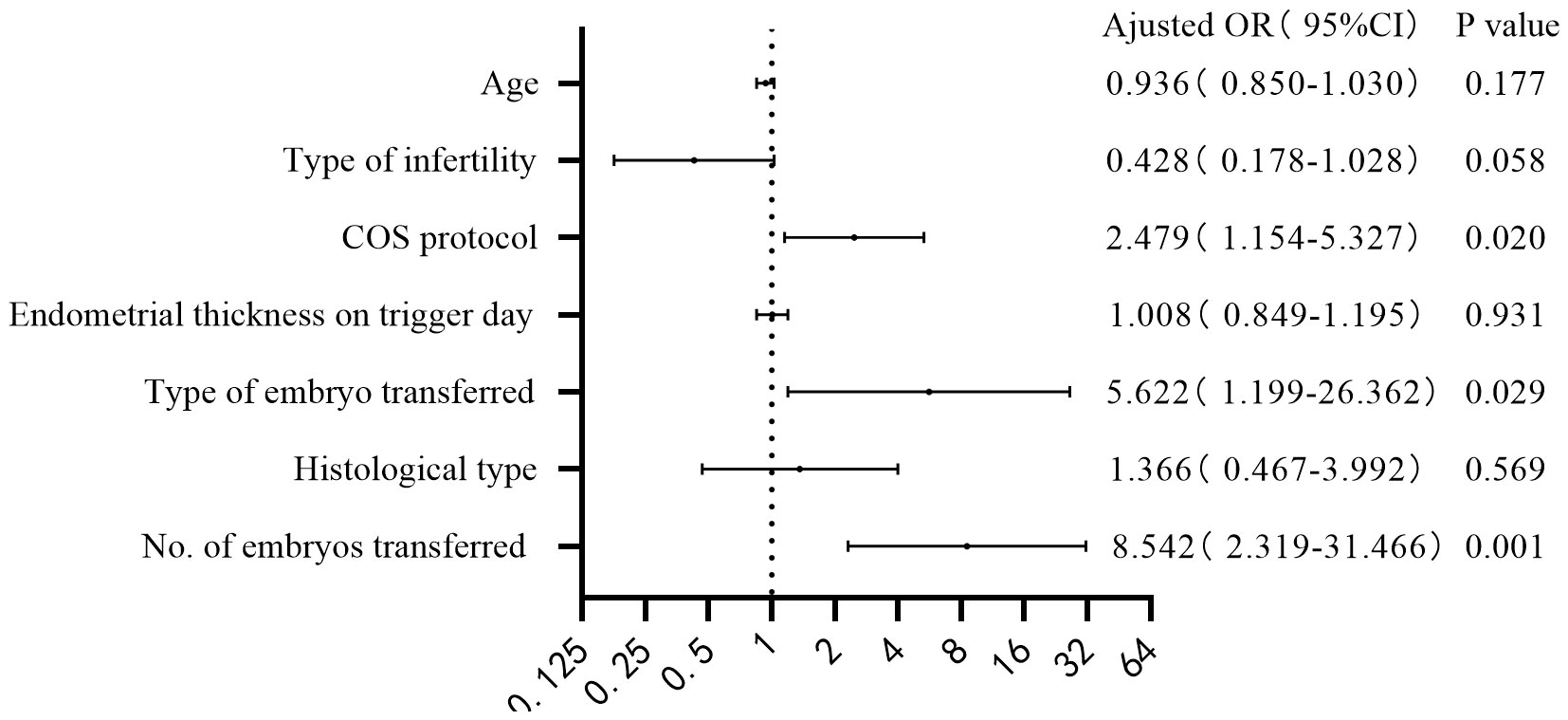
Figure 2 Forest plot: multivariate logistic regression performed for clinical pregnancy.
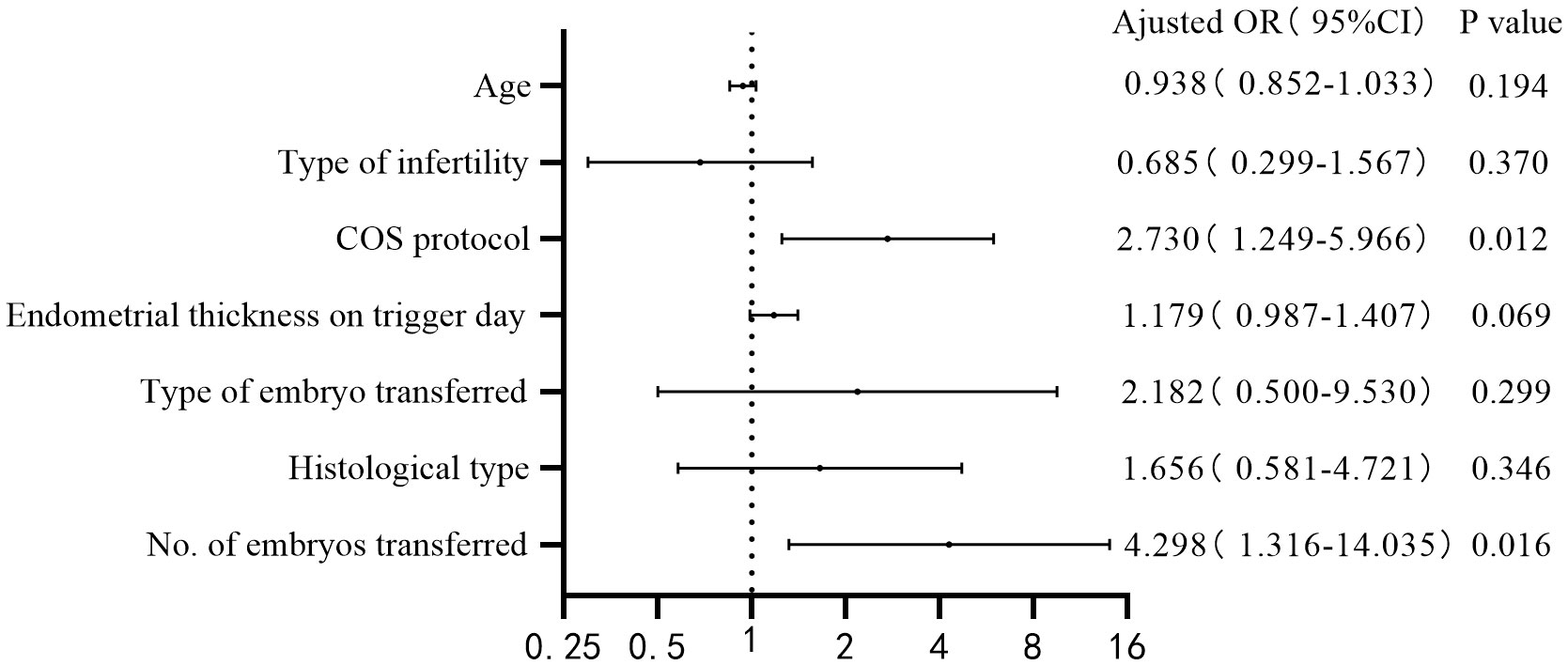
Figure 3 Forest plot: multivariate logistic regression performed for live birth.
Seven of 76 patients in the EL protocol relapsed, with a recurrence rate of 9.2% (7/76). Ten of 62 patients in the ML protocol relapsed, with a recurrence rate of 16.1% (10/62). Eleven of 114 EH patients relapsed, with a recurrence rate of 9.6% (11/114). Six of 24 EAH/EIN patients relapsed, with a recurrence rate of 25.0% (6/24). After the relapse of eleven patients with EH, eight patients remained as endometrial hyperplasia without atypia, while three patients progressed to endometrial atypical hyperplasia/endometrial intraepithelial neoplasia. After the relapse of six patients with EAH/EIN, three patients remained as endometrial atypical hyperplasia/endometrial intraepithelial neoplasia, two patients were endometrial hyperplasia without atypia, and one patient progressed to carcinoma.
The risk factors of endometrial lesions are also common causes of infertility. Since patients with endometrial hyperplasia are often accompanied by ovulation disorders, the proportion of primary infertility among such patients in this study was as high as 71.0%. At the same time, endometrial lesions, in turn, would have a negative effect on embryo implantation, thereby aggravating infertility.
Although ART assisted pregnancy in patients with endometrial hyperplasia is common after drug treatment, the pregnancy outcomes are often unsatisfactory (7, 8, 19, 20). Fujimoto et al. (7) showed that when using ML protocol for COS, the CPR was significantly lower in patients with EAH/EIN than patients with normal endometrium (9.5%vs. 35.7%). This study showed that, in the ML protocol, the CPR and LBR of patients with endometrial hyperplasia were significantly lower than those of patients with normal endometrium (43.5% vs. 59.7%; 30.6% vs. 49.2%), consistent with the findings of Fujimoto et al. In another study, which investigated the GnRH antagonist protocol for COS, patients with endometrial hyperplasia also had significantly lower LBR than those with normal endometrium (8). The possible reasons for this result are as follows:1. High-efficiency progesterone can cause a reduction in the number of glandular cells in the endometrium and the endometrium atrophy (21, 22). 2. During drug therapy, frequent endometrial scrapings are required to assess the effect of treatment, which may lead to endometritis and thinning of endometrial damage in some patients (22, 23).
Selecting the best COS protocol for patients with endometrial hyperplasia and improving the pregnancy outcomes of these patients warrants clinical attention. Due to its higher CPR and lower risk of OHSS compared to other protocols, the EL protocol is more widely used in current clinical practice (11, 24, 25). Therefore, for the first time, we investigated the pregnancy outcomes of infertile patients with endometrial hyperplasia using EL protocol for COS, and compared them with the outcomes of the ML protocol. The results showed that, in patients with endometrial hyperplasia, treatment using EL protocol provided higher CPR and LBR compared to the ML protocol (61.8% vs. 43.5%; 50.0% vs. 30.6%). This study found that the number of oocytes retrieved and high-quality embryos were similar between two COS protocols, so the improvement in pregnancy outcomes of patients using EL protocol is more likely due to the increased endometrial receptivity. Due to the administration of long-acting GnRH agonist, the EL protocol provides the endometrium with a longer rest time, which may be beneficial to the recovery of endometrial tissue function (26). Studies have revealed that the expression of endometrial receptivity markers was significantly higher in patients treated with EL protocol than patients treated with ML protocol, including homeobox A10 and leukemia inhibitory factor (11). In the EL protocol, patients with endometrial hyperplasia achieved similar CPR and LBR as patients with normal endometrium (61.8% vs. 69.7%; 50.0% vs. 59.9%), which may be attributed to the improvement of endometrium by the long-acting GnRH agonist.
Current study shows that ART treatment does not increase the risk of recurrence of endometrial lesions (27, 28). In this study, the recurrence rate of patients with EAH/EIN after ART treatment was 25%, which was similar to the recurrence rate of endometrial lesions (26%-32.4%) without ART for assisted pregnancy (29–31). Additionally, patients in the EL protocol were administered the long-acting GnRH agonist, resulting in increased suppression of LH. The LH level on trigger day is significantly lower in the EL protocol than that in the ML protocol (0.73 ± 0.68 mIU/mL vs. 1.83 ± 0.87 mIU/mL, P=0.001). According to the classic bicellular bigonadal hormone theory, the relative deficiency of LH weakens the process of estrogen synthesis in granulosa cells, resulting in a lower level of E2 on trigger day in the EL protocol and less stimulation to the endometrium, which enhances safety of patients with endometrial hyperplasia.
This study comprehensively compared the pregnancy outcomes, perinatal outcomes, and disease prognosis of patients with endometrial hyperplasia treated with EL protocol and ML protocol for the first time. The results suggest that the EL protocol maybe a better COS protocol for patients with endometrial hyperplasia, which has certain guiding significance for the selection of COS protocols for patients with endometrial hyperplasia. The limitation of this study is that this is a retrospective study conducted in a single center. The results of our study need to be confirmed by large-sample, multi-center, and prospective studies in the future.
For patients with endometrial hyperplasia undergoing IVF treatment, the EL protocol is superior to ML protocol, and in the EL protocol, they can achieve similar pregnancy outcomes as patients with normal endometrium.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: DOI: 10.5281/zenodo.10417109.
This retrospective cohort study was approved by the Ethics Review Committee of the First Affiliated Hospital of Zhengzhou University (2023-KY-0236-001). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because The requirement for informed consent was waived due to the retrospective character of this study.
HA: Data curation, Investigation, Methodology, Writing –original draft. TL: Investigation, Writing – review & editing. KH: Writing – review & editing. HS: Writing – review & editing. CW: Writing – review & editing. TC: Writing – review & editing. JZ: Conceptualization, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the National Natural Science Foundation of China (Grant No. 82071649) and the Key Scientific Research Projects of Higher Education Institutions in Henan Province (Grant No. 22A320025).
We appreciate the medical staff at the First Affiliated Hospital of Zhengzhou University for helping us to collect the data.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kurman RJ, Carcangiu ML, Herrington CS. World Health Organisation classification of tumours of the female reproductive organs. Int agency Res Cancer (2014) 125–6.
2. Emons G, Beckmann MW, Schmidt D, Mallmann P. Uterus commission of the gynecological oncology working group (AGO). New WHO Classification Endometrial Hyperplasias. Geburtshilfe Frauenheilkd (2015) 75(2):135–6. doi: 10.1055/s-0034-1396256
3. Mutter GL, Baak JP, Crum CP, Richart RM, Ferenczy A, Faquin WC. Endometrial precancer diagnosis by histopathology, clonal analysis, and computerized morphometry. J Pathol (2000) 190(4):462–9. doi: 10.1002/(SICI)1096-9896(200003)190:4<462::AID-PATH590>3.0.CO;2-D
4. Tian Y, Liu Y, Wang G, Lv Y, Zhang J, Bai X, et al. Endometrial hyperplasia in infertile women undergoing IVF/ICSI: A retrospective cross-sectional study. J Gynecol Obstet Hum Reprod (2020) 49(9):101780. doi: 10.1016/j.jogoh.2020.101780
5. Chandra V, Kim JJ, Benbrook DM, Dwivedi A, Rai R. Therapeutic options for management of endometrial hyperplasia. J Gynecol Oncol (2016) 27(1):e8. doi: 10.3802/jgo.2016.27.e8
6. Lucchini SM, Esteban A, Nigra MA, Palacios AT, Alzate-Granados JP, Borla HF. Updates on conservative management of endometrial cancer in patients younger than 45 years. Gynecol Oncol (2021) 161(3):802–9. doi: 10.1016/j.ygyno.2021.04.017
7. Fujimoto A, Ichinose M, Harada M, Hirata T, Osuga Y, Fujii T. The outcome of infertility treatment in patients undergoing assisted reproductive technology after conservative therapy for endometrial cancer. J Assist Reprod Genet (2014) 31(9):1189–94. doi: 10.1007/s10815-014-0297-x
8. Friedlander H, Blakemore JK, McCulloh DH, Fino ME. Fertility-sparing treatment and assisted reproductive technology in patients with endometrial carcinoma and endometrial hyperplasia: pregnancy outcomes after embryo transfer. Cancers (Basel) (2023) 15(7):Undefined. doi: 10.3390/cancers15072123
9. Azim A, Oktay K. Letrozole for ovulation induction and fertility preservation by embryo cryopreservation in young women with endometrial carcinoma. Fertil Steril (2007) 88(3):657–64. doi: 10.1016/j.fertnstert.2006.12.068
10. Chen J, Cheng Y, Fu W, Peng X, Sun X, Chen H, et al. PPOS protocol effectively improves the IVF outcome without increasing the recurrence rate in early endometrioid endometrial cancer and atypical endometrial hyperplasia patients after fertility preserving treatment. Front Med (Lausanne) (2021) 8:581927(Undefined). doi: 10.3389/fmed.2021.581927
11. Xu B, Geerts D, Hu S, Yue J, Li Z, Zhu G, et al. The depot GnRH agonist protocol improves the live birth rate per fresh embryo transfer cycle, but not the cumulative live birth rate in normal responders: a randomized controlled trial and molecular mechanism study. Hum Reprod (2020) 35(6):1306–18. doi: 10.1093/humrep/deaa086
12. Ren F, Ma Y, Cai L, Yang S, Han P, Zhang F, et al. Analysis of factors related to conservative treatment of endometrial hyperplasia and delivery outcome (in Chinese). J Pract Obstetrics Gynecology (2020) 36(11):843–7.
13. Yuan W, Shi H. Prognosis analysis of fertility maintenance in women with complex endometrial hyperplasia or endometrial cancer (in Chinese). Chin J OF Family Plann GYNECOTOKOLOGY (2018) 10(1):23–7. doi: 10.3969/j.issn.1674-4020.2018.01.07
14. Tranquilli AL, Brown MA, Zeeman GG, Dekker G, Sibai BM. The definition of severe and early-onset preeclampsia. Statements from the international society for the study of hypertension in pregnancy (ISSHP). Pregnancy Hypertens (2013) 3(1):44–7. doi: 10.1016/j.preghy.2012.11.001
15. Zegers-Hochschild F, Adamson GD, de Mouzon J, Ishihara O, Mansour R, Nygren K, et al. International Committee for Monitoring Assisted Reproductive Technology; World Health Organization. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril (2009) 92(5):1520–4. doi: 10.1016/j.fertnstert.2009.09.009
16. Yu T, Wu D, Cao Y, Zhai J. Association between menstrual patterns and adverse pregnancy outcomes in patients with polycystic ovary syndrome. Front Endocrinol (Lausanne) (2021) 12:740377(Undefined). doi: 10.3389/fendo.2021.740377
17. Li Y, Ruan X, Wang H, Li X, Cai G, Du J, et al. Comparing the risk of adverse pregnancy outcomes of Chinese patients with polycystic ovary syndrome with and without antiandrogenic pretreatment. Fertil Steril (2018) 109(4):720–7. doi: 10.1016/j.fertnstert.2017.12.023
18. Liu S, Mo M, Xiao S, Li L, Hu X, Hong L, et al. Pregnancy outcomes of women with polycystic ovary syndrome for the first in vitro fertilization treatment: A retrospective cohort study with 7678 patients. Front Endocrinol (Lausanne) (2020) 25:575337(11). doi: 10.3389/fendo.2020.575337
19. Zong X, Guo Y, Li H, Li R, Qiao J. Obstetric and perinatal outcomes following frozen and fresh embryo transfer in patients with endometrial hyperplasia and carcinoma: a retrospective study in a high-volume reproductive center. BMC Pregnancy Childbirth (2023) 23(1):92. doi: 10.1186/s12884-023-05418-7
20. Li M, Song J, Zhao Y, Wu S, Liu H, Tang R, et al. Fertility outcomes in infertile women with complex hyperplasia or complex atypical hyperplasia who received progestin therapy and in vitro fertilization. J Zhejiang Univ Sci B (2017) 18(11):1022–5. doi: 10.1631/jzus.B1600523
21. Mentrikoski MJ, Shah AA, Hanley KZ, Atkins KA. Assessing endometrial hyperplasia and carcinoma treated with progestin therapy. Am J Clin Pathol (2012) 138(4):524–34. doi: 10.1309/AJCPM2TSDDF1MHBZ
22. Inoue O, Hamatani T, Susumu N, Yamagami W, Ogawa S, Takemoto T, et al. Factors affecting pregnancy outcomes in young women treated with fertility-preserving therapy for well-differentiated endometrial cancer or atypical endometrial hyperplasia. Reprod Biol Endocrinol (2016) 14(Undefined):2. doi: 10.1186/s12958-015-0136-7
23. Guo Y, Zong X, Li H, Qiao J. Analysis of IVF/ICSI outcomes in infertile women with early-stage endometrial cancer and atypical endometrial hyperplasia after conservative treatment. J Assist Reprod Genet (2022) 39(7):1643–51. doi: 10.1007/s10815-022-02475-3
24. Wang D, Chu T, Yu T, Zhai J. Is early-follicular long-acting GnRH agonist protocol an alternative for patients with polycystic ovary syndrome undergoing in vitro fertilization? Reprod Biol Endocrinol (2022) 20(1):137. doi: 10.1186/s12958-022-01007-z
25. Wang X, Li W, Chen X, Zhang W, Chu M, Yin S, et al. Is the long-acting gonadotropin-releasing hormone agonist long protocol better for patients with endometriosis undergoing IVF? Int J Gynaecol Obstet (2023) 162(1):325–32. doi: 10.1002/ijgo.14690
26. Edwards RG. Clinical approaches to increasing uterine receptivity during human implantation. Hum Reprod (1995) 10(Suppl 2):60–66. doi: 10.1093/humrep/10.suppl_2.60
27. Ichinose M, Fujimoto A, Osuga Y, Minaguchi T, Kawana K, Yano T, et al. The influence of infertility treatment on the prognosis of endometrial cancer and atypical complex endometrial hyperplasia. Int J Gynecol Cancer (2013) 23(2):288–93. doi: 10.1097/IGC.0b013e31827c18a1
28. Fan Y, Li X, Wang J, Wang Y, Tian L, Wang J. Analysis of pregnancy-associated factors after fertility-sparing therapy in young women with early stage endometrial cancer or atypical endometrial hyperplasia. Reprod Biol Endocrinol (2021) 19(1):118. doi: 10.1186/s12958-021-00808-y
29. Vaugon M, Peigné M, Phelippeau J, Gonthier C, Koskas M. IVF impact on the risk of recurrence of endometrial adenocarcinoma after fertility-sparing management. Reprod BioMed Online (2021) 43(3):495–502. doi: 10.1016/j.rbmo.2021.06.007
30. Gallos ID, Yap J, Rajkhowa M, Luesley DM, Coomarasamy A, Gupta JK. Regression, relapse, and live birth rates with fertility-sparing therapy for endometrial cancer and atypical complex endometrial hyperplasia: a systematic review and metaanalysis. Am J Obstet Gynecol (2012) 207(4):266. doi: 10.1016/j.ajog.2012.08.011
Keywords: endometrial hyperplasia, early-follicular, midluteal, long protocol, in vitro fertilization, pregnancy outcomes
Citation: An H, Li T, Huang K, Shi H, Wang C, Chu T and Zhai J (2024) Pregnancy outcomes in infertile patients with endometrial hyperplasia with or without atypia undergoing in vitro fertilization: the early-follicular long protocol is superior to midluteal long protocol. Front. Endocrinol. 15:1314432. doi: 10.3389/fendo.2024.1314432
Received: 10 October 2023; Accepted: 29 January 2024;
Published: 19 February 2024.
Edited by:
Etienne Marbaix, Université Catholique de Louvain, BelgiumReviewed by:
Hiroshi Kishi, The Jikei University School of Medicine, JapanCopyright © 2024 An, Li, Huang, Shi, Wang, Chu and Zhai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jun Zhai, YmVzdHpoYWkyMDA1QDE2My5jb20=
†ORCID: Jun Zhai, orcid.org/0000-0001-9566-865X
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.