
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 30 January 2024
Sec. Clinical Diabetes
Volume 15 - 2024 | https://doi.org/10.3389/fendo.2024.1302013
This article is part of the Research TopicEarly Detection and Combination Therapy for Diabetic Peripheral Neuropathy: What does the Future Look Like?View all 6 articles
 Anna E. Körei†
Anna E. Körei† Magdolna Békeffy†
Magdolna Békeffy† Adrienn MenyhártKarola OsgyánIldikó Istenes
Adrienn MenyhártKarola OsgyánIldikó Istenes Viktor J. Horváth*
Viktor J. Horváth* Péter Kempler*
Péter Kempler*Introduction: Autonomic and sensory neuropathy have been observed in both prediabetes and manifest diabetes mellitus. However, there is a lack of available data regarding whether patients at a moderate or high risk of developing diabetes, yet without a current diagnosis of prediabetes or diabetes, exhibit an increased prevalence of neuropathy.
Methods: FINDRISC (Finnish Diabetes Risk Score) was used to classify individuals at risk (≥12 points, n = 44; control <12 points, n = 28). HbA1c levels >5.6% served as exclusion criteria, and patients with known medical conditions predisposing to neuropathy were also excluded. Cardiac autonomic function (Ewing tests) and peripheral sensory neuropathy (Neurometer and Q-sense) were assessed by standardized protocols, and their potential association with increased FINDRISC points was analyzed using a regression model.
Results: Mean age was 46.7 ± 14.3 years in the control and 55.7 ± 14.1 years in the increased risk group. Male/female ratio did not differ. Individuals with increased risk of diabetes were more obese (BMI: 29.9 ± 12.5 kg/m2 vs. 25.9 ± 8.9 kg/m2). Additionally, hypertension was more frequent among them (68.2% vs. 17.9%), and their lipid parameters were also less favorable. Parasympathetic neuropathy was present in both groups (56.8% vs. 32.1%, respectively). Sympathetic neuropathy was not found. Sensory nerve dysfunction was of low prevalence in the high-risk group and did not occur in healthy controls. In multiple logistic regression analysis, HbA1c exhibited an independent association with parasympathetic neuropathy (OR: 5.9; 95% CI: 1.08–32.68; p < 0.041).
Discussion: An increased risk of developing prediabetes/diabetes does not appear to have a strong correlation with an increased likelihood of developing autonomic or sensory neuropathy. However, the etiology behind the occurrence of parasympathetic autonomic neuropathy in healthy individuals remains unknown.
The global prevalence of prediabetes and diabetes mellitus is rapidly increasing (1, 2). The two conditions are strongly interrelated with up to 70% of individuals diagnosed with prediabetes progressing to diabetes (3). Both diabetes and prediabetes are associated with an increased risk of developing sensory (DSPN) and cardiac autonomic (CAN) neuropathy (3–6), both of which are independent risk factors for mortality in diabetic patients (7, 8).
Although the diagnosis of incident diabetes or prediabetes is based on laboratory tests, identifying individuals at a higher risk of developing diabetes is also possible with non-invasive approaches (3). The FINDRISC (Finnish Diabetes Risk Score) questionnaire stands out as widely utilized. It demonstrates the capacity to predict the onset of incident diabetes with an acceptable sensitivity and specificity (9). Non-invasive models for predicting diabetes include mostly similar risk factors, but they weigh the components differently. Notably, an elevated fasting plasma glucose level within the normoglycemic range emerges as an independent risk factor for type 2 diabetes in young men (10). In addition, increased glucose values were observed as early as 13 years prior to the diagnosis of diabetes (11). These data indicate that patients with normal blood glucose levels but at higher risk for diabetes may exhibit an altered metabolic status, potentially representing an increased susceptibility to microvascular complications as well. Also, certain risk factors in non-invasive prediction models [e.g., age, higher body mass index (BMI), high blood pressure] are associated with the development of neuropathy even in the absence of abnormal glucose metabolism (12). As high-risk diabetes, prediabetes, and manifest diabetes represent a glycaemic continuum and the latter two entities are clearly associated with different types of neuropathies, our study aimed to determine whether an increased risk of diabetes is associated with a higher prevalence of neuropathy or neuropathy-related symptoms.
We enrolled adult patients (aged 18 years and older) who attended the diabetes and general medicine outpatient clinic of the Department of Internal Medicine and Oncology, Semmelweis University from 2020 to 2023. The clinic serves as a secondary referral center for a suburban area of Budapest, Hungary, with approximately a hundred thousand inhabitants. We included patients referred to our clinic by general practitioners, exhibiting an increased risk of developing type 2 diabetes (FINDRISC ≥12 points) but no known history of glucose metabolism abnormalities.
This group of patients served as our primary focus. Patients referred with other, general health problems unrelated to any glucose metabolism abnormalities were included in the control group (FINDRISC <12 points). HbA1c levels higher than 5.6% (and fasting blood glucose equal or higher than 5.9 mmol/l) served as exclusion criteria and patients with diseases known to cause neuropathy were also excluded from further investigation. Furthermore, to exclude any potential glucose metabolism abnormalities, a 75-g oral glucose tolerance test was administered to patients with a FINDRISC ≥12 points. In addition to an assessment of CAN and DSPN, demographic data, anthropometrics, lifestyle information (including smoking habits and alcohol consumption, eating habits, and physical activity), current and previous chronic illnesses, current (temporary or continuous) medications and laboratory data were collected on a standardized data entry form. The study protocol was approved by the local ethical committee, and all participants gave written informed consent.
Subclinical and clinical DSPN and CAN were diagnosed in accordance with the Toronto Diabetic Neuropathy Expert Group recommendation (13) and were performed using standardized protocols (7, 14, 15). DSPN was evaluated by Neurometer CPT (Neurotron Inc., Baltimore, MD, USA), Medoc Q-Sense device (Ramat Yishay, Israel), calibrated 128-Hz tuning fork, and Semmes-Weinstein monofilament. Current perception threshold (CPT) was measured at the median and peroneal nerves (digital branches) by the Neurometer device at three different frequencies (2000 Hz, 250 Hz, and 5 Hz) assessing large myelinated, small myelinated and small unmyelinated sensory fiber function, respectively. Cold and heat detection thresholds were assessed using a thermal sensory analyser from the Q-Sense instrument. Diagnosis of DSPN was confirmed when abnormal results were found bilaterally using the same diagnostic method.
Symptoms consistent with painful diabetic neuropathy were assessed using the Neuropathy Total Symptoms Score–6 (NTSS-6) questionnaire.
CAN was assessed by the standard cardiovascular reflex tests (CARTs) using Ewing’s battery (13), except the handgrip test (15). Briefly, the parasympathetic function was assessed by heart rate responses to deep breathing and standing (30:15 ratio) and by performing the Valsalva maneuver (Valsalva ratio). The results of the deep-breathing test were expressed as the difference of the highest heart rate during inspiration and the lowest heart rate during expiration (beat-to-beat variation; beats/min). Sympathetic autonomic function was assessed by blood pressure responses to standing (orthostatic hypotension test). Diagnosis of CAN was defined as the presence of at least two pathological reflex test results, or alternatively, one that is clearly abnormal and two that fall within the borderline range. Patients taking antihypertensive medications (especially beta-blockers and non-dihidropyridin type Ca-antagonist), which could affect CART results derived from analysis of heart rate changes, were requested to stop medications at least 24h prior to investigations. Patients were also asked to avoid consuming coffee, other caffeinated beverages, alcohol, smoking, and strenuous exercise at least 6h before testing.
Consistent with recent guidelines, age-related reference values were used for the interpretation of heart rate–based tests. To evaluate severity of CAN, an autonomic neuropathy score (CAN score) was obtained by scoring the results of the reflex tests: 0, 1, and 2 for normal, borderline, and abnormal test results.
After we determined eligibility including sex at birth and age, height and weight were measured by calibrated instruments. Smoking burden was defined as package year. Weekly alcohol consumption (beer, wine, and spirits) was recorded and considered to be high if the level of consumption was >14 units/week. All the laboratory measurements were completed by using standardized protocols of the Department of Laboratory Medicine, Semmelweis University.
Available medical records were screened for the following medical conditions: a possible previous documentation of diabetes, diagnosis of hypertension and hyperlipidaemia, previous major cardiovascular event (including myocardial infarction, heart failure, peripheral vascular disease, and cerebrovascular accident), known dementia, thyroid disease, chronic obstructive pulmonary disease, connective tissue diseases, inflammatory bowel disease, chronic liver disease, chronic kidney disease (CKD III–V), chronic anaemia, radiologically confirmed vertebral disc herniation, and malignancies. Information collected from medical records was supplemented with direct information from the participants.
The Kolmogorov–Smirnov test for normality was performed on all variables. Normally distributed data were presented as means ± SD, while non-normally distributed data, such as triglycerides, cholesterol, blood pressure, and sensory and autonomic measures were expressed as median (interquartile range). Categorical data were reported as n (%).
For comparison between groups, Mann-Whitney U-test or paired t-test for continuous variables and χ2 test for categorical data were used based on the variable’s normality of distribution. To investigate the explanatory variables of cardiovascular autonomic neuropathy (CAN) (only parasympathetic autonomic dysfunction was detected within the study population), a multiple logistic regression model was employed using cardiovascular parasympathetic autonomic neuropathy as dependent variable. All variables that exhibited a univariate association (p < 0.1) with parasympathetic autonomic neuropathy were included in the analysis. Consequently, the model incorporated age, the presence of hypertension as a comorbidity, HbA1c, and the risk of developing type 2 diabetes represented by the total score of FINDRISC questionnaire. Explanatory factors of sensory impairment could not be analyzed due to the very limited occurrence of sensory neuropathy as outcome measure within this study population. P < 0.05 was considered as statistically significant. All analyses were performed using SPSS version 27.0.
A total of 44 patients with an increased risk of diabetes (FINDRISC ≥12 points, referred as high-risk group) were investigated, along with 28 control patients (FINDRISC <12 points, referred as control group). The total score difference between the two groups was approximately 10 points, indicating a significant disparity. Participants of the high-risk group were older; their weight, waist, and hip circumference was higher; their height was lower; and their BMI was also significantly higher. On the other hand, the waist-to-hip ratio (WHR) did not differ significantly and no gender difference could be seen. Hypertension was more prevalent in the high-risk group, leading to a higher frequency of antihypertensive medication usage. There was no difference in the use of non-steroidal anti-inflammatory drug medication between the two groups. Family history of diabetes and hypertension was also more frequent among members of the high-risk group. There was no difference in the smoking habit and alcohol consumption (>14 units/week) between the two groups.
Average diastolic blood pressure was higher in the high-risk group, but no difference was found in systolic blood pressure and resting heart rate. HbA1c was mild; fasting blood glucose was considerably higher (both significantly different) in the high-risk group. Low-desity lipoprotein (LDL; measured) and high-density lipoprotein (HDL) did not exhibit differences; however, there were significant disparities in total cholesterol, triglyceride levels, and triglyceride/HDL ratio, all of which were higher in the high-risk group. No difference in kidney function and sedimentation rate was detected between the two groups.
Beat-to-beat variation being a sensitive marker for parasympathetic neuropathy was significantly lower, and cardiovascular autonomic score was significantly higher in the high-risk group when compared to healthy controls. Parasympathetic neuropathy occurred more frequently among patients with a moderate to high risk of developing diabetes. The 30:15 ratio and the Valsalva ratio (the latter controlled partially by sympathetic nerves) remained within the normal range in both groups, and no cases of sympathetic neuropathy were diagnosed in either the high-risk or control group.
Sensory neuropathy only occured in the high-risk group, but in only eight patients. Regarding the symptoms associated with DSPN, sensations of pricking and lancinating nature were more frequently reported in the high-risk group. However, there was no difference in the frequency of aching and burning pain, numbness, and allodynia between groups. Regarding NTSS, there was a trend toward higher scores in the high-risk group, but the difference did not reach statistical significance. Similarly, protective sensation assessed by the monofilament in the lower limbs was found not significantly different between the high-risk and healthy control groups. In contrast, reduced vibration sensation as measured with a tuning fork was found in the high-risk group compared to healthy control subjects with the differences being significant on all extremities except the right arm. Comparing CPTs between groups, a significant difference was detected only in CPTs of large and small myelinated nerve fibers of the median nerves. However, assessing CPT abnormality between high risk for diabetes and healthy control groups, a pathological CPT was detected more frequently in the large myelinated fibers of the peroneal nerve in the high-risk group.
Finally, when comparing thermal sensation thresholds between groups, warm sensation thresholds were found significantly higher in the high-risk group. Regarding cold thermal sensation, high-risk patients had consistently lower cold detection thresholds on all limbs. Yet, the differences were found significant only for thresholds measured on the lower limbs.
The main features of the study participants are shown in Tables 1–4.
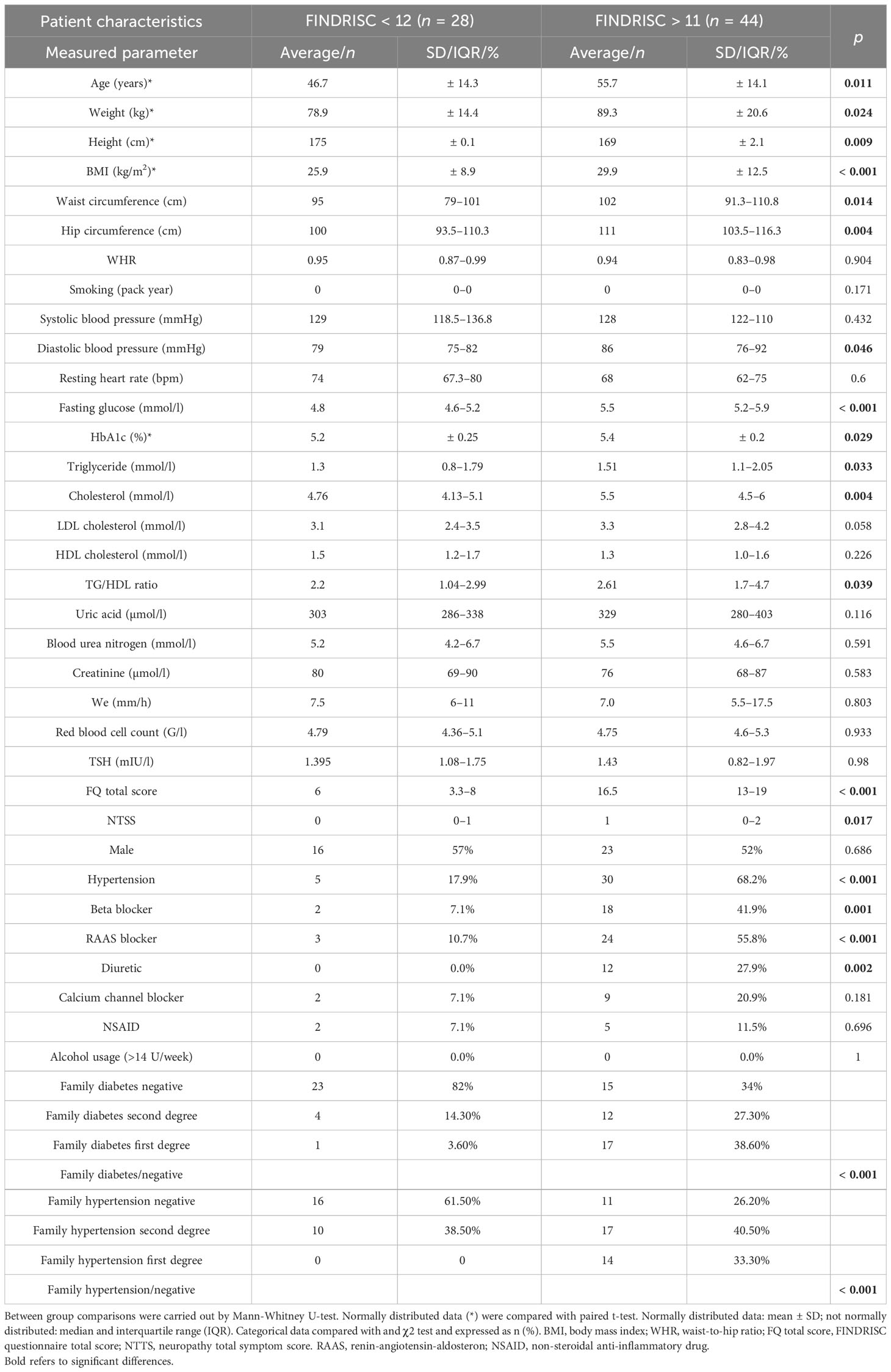
Table 1 Anthropometric and clinical characteristics of the participants.
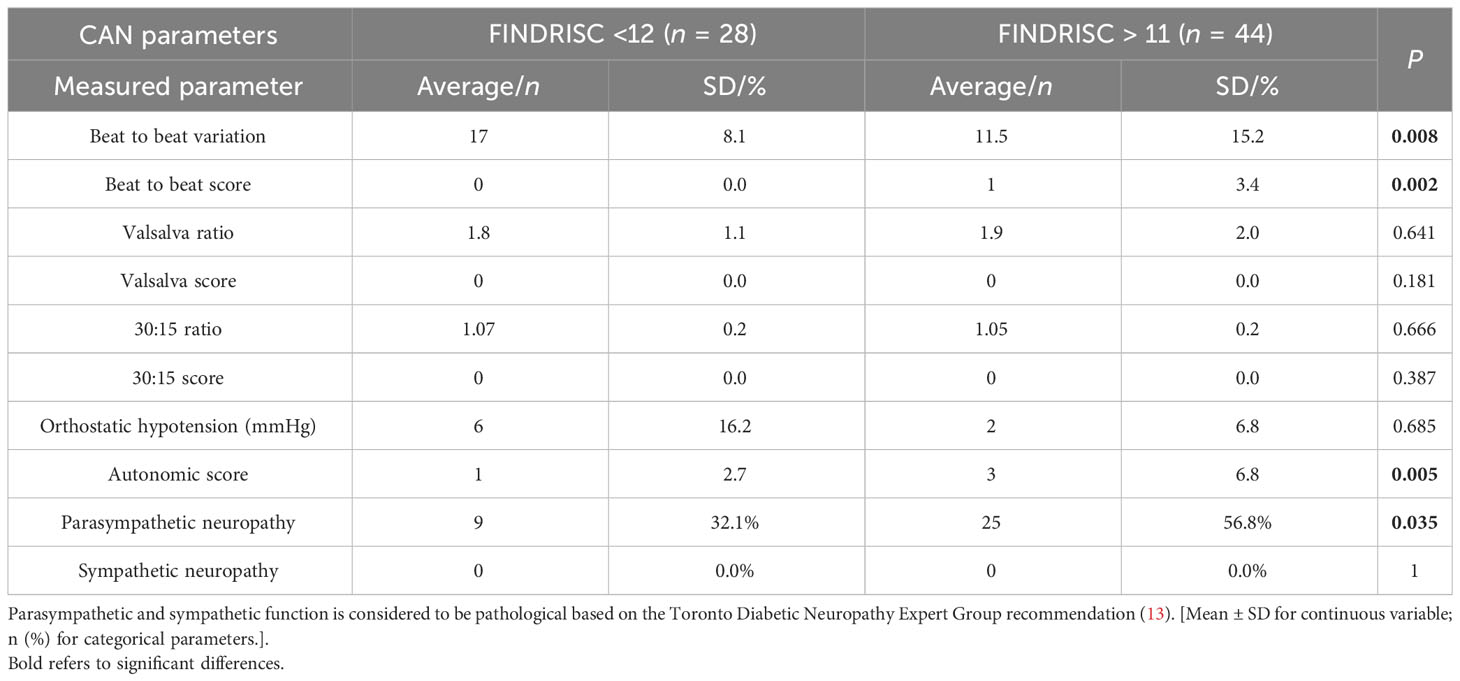
Table 2 Cardiac autonomic (CAN) markers of the different populations (unadjusted data).
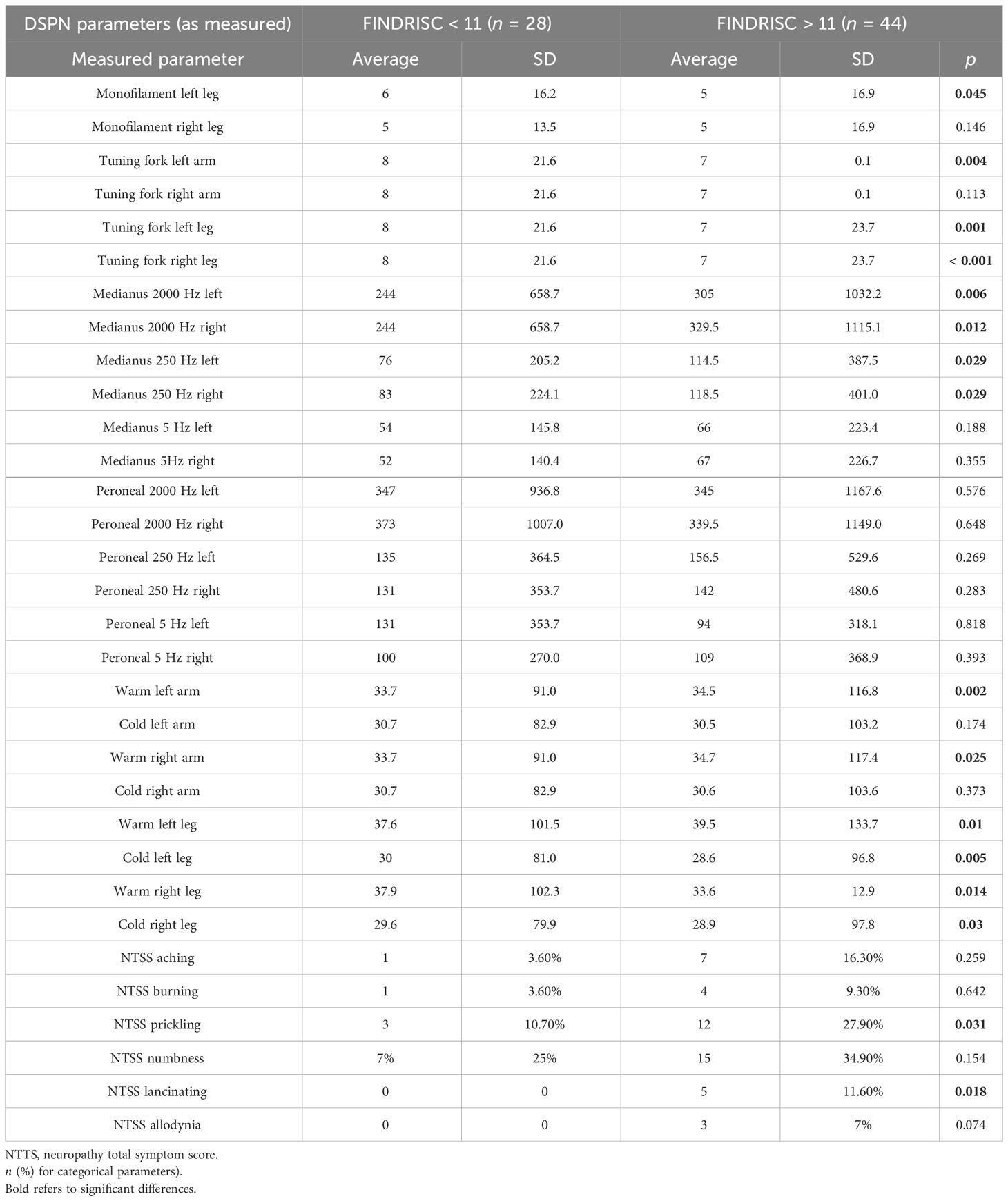
Table 3 Results of peripheral sensory neural function measurement and neural sensation alterations in the different groups (unadjusted data; mean ± SD for continuous.
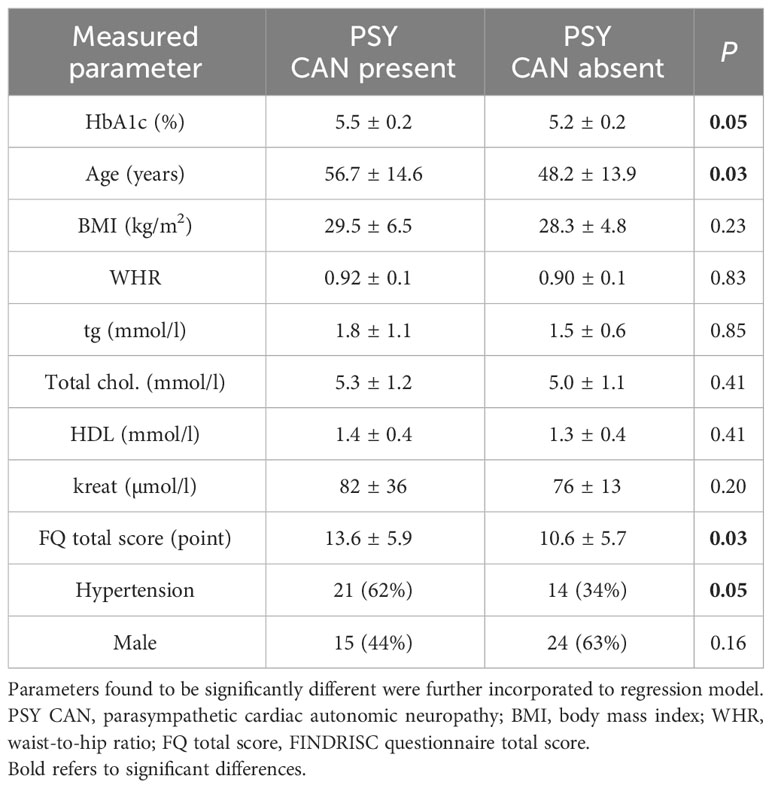
Table 4 Parameters determine the presence or absence of parasympathetic cardiac autonomic neuropathy in both groups.
In order to explore the explanatory variables for cardiovascular autonomic neuropathy CAN, clinical and laboratory data of study participants with and without CAN were compared (Table 4). Significant differences between groups were detected in respect of age, HbA1c, the presence of hypertension as comorbidity, and the total score obtained in the FINDRISC questionnaire reflecting type 2 diabetes risk. No significant differences between participants with and without CAN were found regarding BMI; WHR; serum lipid levels, such as triglyceride (TG); total cholesterol; HDL; and serum creatinine. In multiple logistic regression analysis, glycaemia (indicated by HbA1c levels) emerged as the only and independent factor associated with CAN (OR: 5.9; 95% CI: 1.08–32.68; p < 0.041) (Table 5).
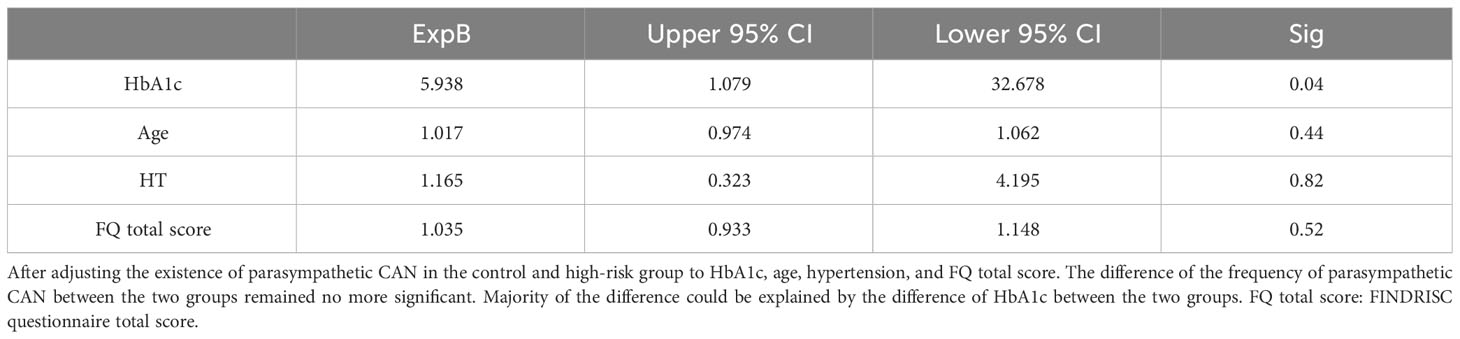
Table 5 Association between the presence of parasympathetic CAN and their determinants.
Variables underlying sensorimotor neuropathy could not be assessed given their low incidence rate observed in this study.
The main objective of this study was to evaluate whether patients with an increased risk for type 2 diabetes (FINDRISC ≥ 12 points) without clinically manifest glucose metabolism disorders have an increased prevalence of neuropathy. CAN is more frequent in patients with an increased risk of developing type 2 diabetes when compared to healthy control subjects, and it shows independent association with HbA1c levels within the normal range. As for sensorimotor polyneuropathy, only some slight alterations hinting to early DSPN could be verified in high-risk patients. However, parasympathetic neuropathy was documented in both the control and the increased risk groups. This finding needs further attention.
It is reasonable to assume that patients at risk of developing diabetes or prediabetes (without clinically manifested glucose metabolism disorder) may exhibit various forms of neuropathy with variability in their characteristics (4). Higher mean fasting plasma glucose levels within the normoglycemic range in young individuals is an independent risk factor for type 2 diabetes (10). Additionally, increased glucose values were observed in the Whitehall II study as early as 13 years before the diagnosis of diabetes (11). Although we have no direct evidence that the FINDRISC questionnaire identifies these people, we cannot exclude it. Some pathophysiological aspects may support our findings on slight autonomic and sensory dysfunction in patients being at higher risk for type 2 diabetes. Enhanced polyol pathway activity and increased oxidative and nitrosative stress are well-known mechanisms related to the development of neuropathy and are associated with hyperglycaemia (16). Higher quartile of glucose (or HbA1c) levels even within the normal range might have an impact on neuronal function in high-risk individuals.
In the present study, glycaemia within the normal range emerged as the only independent factor associated with CAN. Age and hypertension are addressed by the FINDRISC questionnaire itself and, assumably, their effects were eradicated by incorporating the score results into the regression model. Glycaemia, age, and hypertension are proven risk factors of autonomic neuropathy (4, 17). Similarly to the present study, glycaemia was found the only independent explaining measure for sensory nerve dysfunction, as observed in our previous study involving patients with impaired glucose tolerance (14).
We assessed CAN by standard CARTs. CARTs are still the gold standard of CAN assessment. Short-term heart rate variability (HRV) indices might be additional resources being easier, perhaps more sensitive and patient independent compared to CARTs (18). Also, primary sympathovagal imbalance was suggested a common pathway to the development of hypertension and diabetes mellitus (19). Large epidemiological studies also support the hypothesis that autonomic dysfunction may predict the development of future type 2 diabetes (5). Orthostatic hypotension is a late and insensitive marker of CAN. Accordingly, no instances of sympathetic CAN could be detected in this study. One can speculate that sudomotor tests would provide a more precise assessment of CAN in our study. However, no strong evidence on diagnostic accuracy of sudomotor function assessment in prediabetic and diabetic sympathetic neuropathy is available (18).
It should also be noted that a limited number of patients (n = 9; 32.1%) had parasympathetic neuropathy in the control group. It may be associated with the high prevalence of cardiovascular risk factors (hypertension, hyperlipidaemia, etc.) being also known as predictors of CAN. The presence of an early stage neuropathy in, otherwise, healthy individuals underscores the importance of investigating factors that may contribute to the development of neuropathy.
The assessment of peripheral neural dysfunction with the Neurometer is also a matter of debate. We have three decades of experience with this instrument (14, 20–30), and it seems to be a reliable and reproducible method to detect early changes of sensory dysfunction. Our recent meta-analysis also confirmed its usefulness and comparability with other sensory assessment tools (8). Using the Neurometer and quantitative sensor testing (Q-Sense), only very slight differences between individuals at high risk of type 2 diabetes and healthy controls could be observed: high-risk patients tended to have diminished vibration, current, and thermal perception with the thresholds remaining in the normal reference ranges. Whether these changes have clinical significance or predict future decline in sensory function remain open. Gold standard methods of small-fiber neuropathy such as CCM (corneal confocal microscopy) and punch biopsy may be more sensitive (31). However, CCM and IENFD (intraepithelial nerve fiber density) assessments through punch biopsy were not accessible to us during the study. Furthermore, the clinical utility of IENFD assessment is limited by its invasive nature.
In this study, the risk of diabetes was assessed using the FINDRISC questionnaire (32–35). The FINDRISC is able to identify not only diabetes but also milder forms of glucose abnormalities depending on the cutoff point chosen (32, 33, 35). In our study, we opted for a cutoff value of >11 points to identify patients at a moderate to high risk of developing diabetes, a threshold slightly lower than the cutoff values used by most studies (>13 and >15 points). However, in a previous study, lowering the cutoff value to ≥11 in the FINDRISC questionnaire yielded an enhanced sensitivity of 73%, a specificity of 67%, and an excellent negative predictive value of 98.5% for detecting diabetes (34). Moreover, a cross-sectional analysis of the National Health and Nutrition Examination Survey spanning 1999–2010 recommended an optimal cutoff point of 10 for men and 12 for women in detecting diabetes and 9 for men and 10 for women in detecting prediabetes (35). Considering our aim to assess the neuropathy burden of individuals at a higher risk of diabetes yet without prediabetes or diabetes, the chosen cutoff value of >11 seemed to be appropriate. The score of >11 was also shown to be a reasonable cutoff for the optimal utilization of OGTT in screening for abnormal glucose metabolism in the population (35).
Certain limitations of the present study need to be addressed. An important limitation is the small sample size that restricts our ability to adjust our data for potentially confounding factors and conduct subgroup analyses. A further important confounding factor is the usage of beta-blockers. Nonetheless, patients followed our instructions to discontinue heart rate–modifying drugs 24h before the investigation. Usage of diuretics would primarily affect the orthostatic hypotension test. In our study, no participant had orthostatic hypotension and, therefore, the clinically significant effect of diuretics can be excluded. Due to our inability to continuously monitor glucose concentration (even for a limited duration), no precise assessment of the effect of total glycaemic burden on neural function was possible and further investigations are required to explore this aspect in detail. Given the cross-sectional design of the present study, no causative relationship between CAN and HbA1c could be concluded. The overall atherosclerotic cardiovascular risk was low or moderate among the patients and, therefore, we did not collect information on the integrity of the coronary circulation, although the presence of coronary disease could potentially influence our results. As our cohort included participants referred to a university center, referral bias cannot be excluded. We assessed obesity by BMI and waist circumference, but these parameters do not address the visceral fat tissue, which is associated with an increased risk of metabolic syndrome, diabetes, and cardiovascular diseases (36) potentially leading to neuropathy.
Our study has notable strengths as well. This was the first attempt to demonstrate an association between an increased risk of type 2 diabetes risk and the presence of neuropathy. The utilization of gold standard measures of diabetic autonomic neuropathy and validated instruments for sensory neuropathy assessment constitutes a valuable strength rendering our study easily reproducible. The fact that all tests and examinations were conducted in the same laboratory, using the same methodology for both groups reduces the risk related to the methods applied. Key risk factors for neuropathy were systematically collected at the time of patient selection. Additionally, electronic medical records were available for all patients, ensuring comprehensive data retrieval without missing values.
In summary, our study did not demonstrate clear evidence of an elevated risk of autonomic and sensory neuropathy among patients with an increased risk of developing diabetes but without a manifest glucose metabolism disorder (FINDRISC >11 points). However, the more common presence of parasympathetic neuropathy and subtle sensory alterations found in this patient population underscores the need for further investigations to clarify the factors contributing to the development of parasympathetic and sensory dysfunction and warrants further prospective studies to reveal their clinical significance and long-term consequences.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Semmelweis University Regional and Institutional Committee of Science and Research Ethics. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
AK: Data curation, Formal analysis, Investigation, Writing – review & editing. MB: Data curation, Investigation, Writing – review & editing. AM: Data curation, Investigation, Writing – review & editing. KO: Data curation, Investigation, Project administration, Writing – review & editing. II: Investigation, Writing – review & editing. VH: Data curation, Investigation, Writing – original draft. PK: Conceptualization, Funding acquisition, Methodology, Resources, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The research was supported by the Hungarian Diabetes Association.
The authors would like to thank Erika Gulyásné Gáspár for her enormous contribution in data collection and her dedicated work as a specialist nurse at the Neuropathy Laboratory of the Department of Internal Medicine and Oncology, Semmelweis University Faculty of Medicine.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rawshani AN, Rawshani AR, Franzén S, Sattar N, Eliasson B, Svensson A-M, et al. Risk factors, mortality, and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med (2018) 379(7):633–44. doi: 10.1056/NEJMoa1800256
2. Centers for Disease Control and Prevention. National Diabetes Fact Sheet: national estimates and general information on diabetes and prediabetes in the United States. Available at: https://www.cdc.gov/diabetes/data/statistics-report/index.html.
3. Tabák AG, Herder C, Rathmann W, Brunner EJ, Kivimäki M. Prediabetes: a high-risk state for diabetes development. Lancet (2012) 379(9833):2279–90. doi: 10.1016/S0140-6736(12)60283-9
4. Gerritsen J, Dekker JM, TenVoorde BJ, Bertelsmann FW, Kostense PJ, Stehouwer CD, et al. Glucose tolerance and other determinants of cardiovascular autonomic function: the Hoorn Study. Diabetologia (2000) 43(5):561–70. doi: 10.1007/s001250051344
5. Schroeder EB, Chambless LE, Liao D, Prineas RJ, Evans GW, Rosamond WD, et al. Diabetes, glucose, insulin, and heart rate variability: the Atherosclerosis Risk in Communities (ARIC) study. Diabetes Care (2005) 28(3):668–74. doi: 10.2337/diacare.28.3.668
6. Putz Z, Tabák AG, Tóth N, Istenes I, Németh N, Gandhi RA, et al. Noninvasive evaluation of neural impairment in subjects with impaired glucose tolerance. Diabetes Care (2009) 32(1):181–3. doi: 10.2337/dc08-1406
7. Vági OE, Svébis MM, Domján BA, Körei AE, Istenes I, Putz Z, et al. Association of cardiovascular autonomic neuropathy and distal symmetric polyneuropathy with all-cause mortality: A retrospective cohort study. J Diabetes Res (2021) 2021:6662159. doi: 10.1155/2021/6662159
8. Vági OE, Svébis MM, Domján BA, Körei AE, Tesfaye S, Horváth VJ, et al. The association between distal symmetric polyneuropathy in diabetes with all-cause mortality - a meta-analysis. Front Endocrinol (Lausanne) (2023) 14:1079009. doi: 10.3389/fendo.2023.1079009
9. Lindström J, Tuomilehto J. The diabetes risk score: a practical tool to predict type 2 diabetes risk. Diabetes Care (2003) 26(3):725–31. doi: 10.2337/diacare.26.3.725
10. Tirosh A, Shai I, Tekes-Manova D, Israeli E, Pereg D, Shochat T, et al. Normal fasting plasma glucose levels and type 2 diabetes in young men. N Engl J Med (2005) 353(14):1454–62. doi: 10.1056/NEJMoa050080
11. Tabák AG, Jokela M, Akbaraly TN, Brunner EJ, Kivimäki M, Witte DM. Trajectories of glycaemia, insulin sensitivity, and insulin secretion before diagnosis of type 2 diabetes: an analysis from the Whitehall II study. Lancet (2009) 373(9682):2215–21. doi: 10.1016/S0140-6736(09)60619-X
12. Callaghan BC, Xia R, Reynolds E, Banerjee M, Rothberg AE, Burant CF, et al. Association between metabolic syndrome components and polyneuropathy in an obese population. JAMA Neurol (2016) 73(12):1468–76. doi: 10.1001/jamaneurol.2016.3745
13. Tesfaye S, Boulton AJM, Dyck PJ, Freeman R, Horowitz M, Kempler P, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care (2010) 33(10):2285–93. doi: 10.2337/dc10-1303
14. Németh N, Putz Z, Istenes I, Körei AE, Vági OE, Kempler M, et al. Is there a connection between postprandial hyperglycemia and IGT related sensory nerve dysfunction? Nutr Metab Cardiovasc Dis (2017) 27(7):609–14. doi: 10.1016/j.numecd.2017.05.001
15. Körei AE, Kempler M, Istenes I, Vági OE, Putz Z, Horváth VJ, et al. Why not to use the handgrip test in the assessment of cardiovascular autonomic neuropathy among patients with diabetes mellitus? Curr Vasc Pharmacol (2017) 15(1):66–73. doi: 10.2174/1570161114666160822154351
16. Schreiber AK, Nones CF, Reis RC, Chichorro JG, Cunha JM. Diabetic neuropathic pain: Physiopathology and treatment. World J Diabetes (2015) 6(3):432–44. doi: 10.4239/wjd.v6.i3.432
17. Ziegler D, Voss A, Rathmann W, Strom A, Perz S, Roden M, et al. Increased prevalence of cardiac autonomic dysfunction at different degrees of glucose intolerance in the general population: the KORA S4 survey. Diabetologia (2015) 58(5):1118–28. doi: 10.1007/s00125-015-3534-7
18. Spallone V. Update on the impact, diagnosis and management of cardiovascular autonomic neuropathy in diabetes: what is defined, what is new, and what is unmet. Diabetes Metab J (2019) 43(1):3–30. doi: 10.4093/dmj.2018.0259
19. Frontoni S, Bracaglia D, Gigli F. Relationship between autonomic dysfunction, insulin resistance and hypertension, in diabetes. Nutr Metab Cardiovasc Dis (2005) 15(6):441–9. doi: 10.1016/j.numecd.2005.06.010
20. Masson EA, Veves A, Fernando D, Boulton AJ. Current perception thresholds: a new, quick, and reproducible method for the assessment of peripheral neuropathy in diabetes mellitus. Diabetologia (1989) 32(10):724–8. doi: 10.1007/BF00274531
21. Pitei DL, Watkins PJ, Stevens MJ, Edmonds ME. The value of the Neurometer in assessing diabetic neuropathy by measurement of the current perception threshold. Diabetes Med (1994) 11(9):872–6. doi: 10.1111/j.1464-5491.1994.tb00371.x
22. Barkai L, Kempler P, Vámosi I, Lukács K, Marton A, Keresztes K. Peripheral sensory nerve dysfunction in children and adolescents with Type 1 diabetes mellitus. Diabetic Med (1998) 15:228–33. doi: 10.1002/(SICI)1096-9136(199803)15:3<228::AID-DIA551>3.0.CO;2-8.
23. Barkai L, Kempler P. Puberty as a risk factor for diabetic neuropathy. Diabetes Care (2000) 23:1044–45. doi: 10.2337/diacare.23.7.1044
24. Keresztes K, Istenes I, Hermányi ZS, Vargha P, Barna I, Kempler P. Risk factors of autonomic and sensory nerve dysfunction in patients with newly diagnosed type 1 diabetes. Diabetes Care (2003) 26:2213–4. doi: 10.2337/diacare.26.7.2213
25. Keresztes K, Istenes I, Folhoffer A, Lakatos PL, Horváth A, Csák T, et al. Autonomic and sensory nerve dysfunction in primary biliary cirrhosis. World J Gastroenterol (2004) 10:3039–43. doi: 10.3748/wjg.v10.i20.3039
26. Kempler P, Váradi A, Kádár É, Szalay F. Autonomic and peripheral neuropathy in primary biliary cirrhosis:evidence of small sensory fibre damage and prolongation of the QT interval. J Hepatol (1994) 21:1150–1. doi: 10.1016/s0168-8278(05)80640-3
27. Várkonyi TT, Tóth F, Rovó L, Lengyel CS, Kiss JG, Kempler P, et al. Impairment of the auditory brainstem function in diabetic neuropathy. Diabetes Care (2002) 25:631–2. doi: 10.2337/diacare.25.3.631
28. Várkonyi TT, Pető T, Dégi R, Keresztes K, Lengyel CS, Janáky M, et al. Impairment of visual evoked potentials. An early central manifestation of diabetic neuropathy? Diabetes Care (2002) 25:1661–2. doi: 10.2337/diacare.25.9.1661
29. Várkonyi TT, Börcsök É, Tót F, Fülöp ZS, Takács R, Rovó L, et al. Severity of autonomic and sensory neuropathy and the impairment of visual- and auditory-evoked potentials in Type 1 diabetes. Diabetes Care (2006) 29:2325–6. doi: 10.2337/dc06-1174
30. Kempler P, Menyhárt A, Horváth V, Kiss ÁT, Körei AE. Editorial: Frontiers in diagnostic and therapeutic approaches in diabetic sensorimotor neuropathy. Front Endocrinol (2023) 14:1228101 PMID:37396189. doi: 10.3389/fendo.2023.1228101
31. Gad H, Petropoulos IN, Khan A, Ponirakis G, MacDonald R, Alam U, et al. Corneal confocal microscopy for the diagnosis of diabetic peripheral neuropathy: A systematic review and meta-analysis. J Diabetes Investig (2022) 13:134–47. doi: 10.1111/jdi.13643
32. Saaristo T, Peltonen M, Lindström J, Saarikoski L, Sundvall J, Eriksson JG, et al. Cross-sectional evaluation of the Finnish Diabetes Risk Score: a tool to identify undetected type 2 diabetes, abnormal glucose tolerance and metabolic syndrome. Diabetes Vasc Dis Res (2005) 2(2):67–72. doi: 10.3132/dvdr.2005.011
33. Schwarz PEH, Li J, Reimann M, Schutte AE, Bergmann A, Hanefeld M, et al. The Finnish Diabetes Risk Score is associated with insulin resistance and progression towards type 2 diabetes. J Clin Endocrinol Metab (2009) 94(3):920–6. doi: 10.1210/jc.2007-2427
34. Jølle A, Midthjell K, Holmen J, Carlsen SM, Tuomilehto J, Bjørngaard JH, et al. Validity of the FINDRISC as a prediction tool for diabetes in a contemporary Norwegian population: a 10-year follow-up of the HUNT study. BMJ Open Diabetes Res Care (2019) 7(1):e000769. doi: 10.1136/bmjdrc-2019-000769
35. Zhang L, Zhang Z, Zhang Y, Hu G, Chen L. Evaluation of Finnish Diabetes Risk Score in screening undiagnosed diabetes and prediabetes among U.S. adults by gender and race: NHANES 1999-2010. PloS One (2014) 9(5):e97865. doi: 10.1371/journal.pone.0097865
Keywords: diabetes, prediabetes, increased risk of diabetes, autonomic neuropathy, sensory neuropathy
Citation: Körei AE, Békeffy M, Menyhárt A, Osgyán K, Istenes I, Horváth VJ and Kempler P (2024) No clear evidence of neuropathy among patients with high risk for the development of prediabetes/diabetes—a pilot study. Front. Endocrinol. 15:1302013. doi: 10.3389/fendo.2024.1302013
Received: 25 September 2023; Accepted: 03 January 2024;
Published: 30 January 2024.
Edited by:
Rayaz A. Malik, Weill Cornell Medicine-Qatar, QatarReviewed by:
Triantafyllos Didangelos, University General Hospital of Thessaloniki AHEPA, GreeceCopyright © 2024 Körei, Békeffy, Menyhárt, Osgyán, Istenes, Horváth and Kempler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Viktor J. Horváth, aG9ydmF0aGp2aWt0b3JAZ21haWwuY29t; Péter Kempler, a2VtcGxlci5wZXRlckBtZWQuc2VtbWVsd2Vpcy11bml2Lmh1
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.