 Jonas Seibold
Jonas Seibold Mario Hönemann
Mario Hönemann Anke Tönjes
Anke Tönjes Benjamin Sandner
Benjamin Sandner
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Endocrinol. , 19 February 2024
Sec. Adrenal Endocrinology
Volume 15 - 2024 | https://doi.org/10.3389/fendo.2024.1294415
While suggested, surgery is not always possible as a first-line treatment of Cushing’s Disease (CD). In such cases, patients require medical therapy in order to prevent complications resulting from hypercortisolism. Although there has been a wide expansion in pharmacological options in recent years, mitotane was the agent of choice for treating hypercortisolism decades ago. Due to the introduction of other therapies, long-term experience with mitotane remains limited. Here, we report the case of a woman with CD who was treated with mitotane for 37 years. During the treatment period, biochemical and clinical disease control was achieved and the patient had two uncomplicated pregnancies. Drug-related side effects remained moderate and could be controlled by several dose adjustments. Our case highlights the ability of mitotane to allow an effective control of hypercortisolism and to represent a safe treatment option in special situations where CD requires an alternative therapeutic approach. Furthermore, we provide a literature review of the long-term use of mitotane and reported cases of pregnancy in the context of mitotane therapy.
The majority of cases of endogenous hypercortisolism (Cushing’s syndrome) occur due to an ACTH (adrenocorticotropic hormone) producing adenoma of the pituitary gland (so-called Cushing’s disease (CD)) (1).
For all etiologies of Cushing’s Syndrome, resection of the causal lesion(s) represents the treatment of choice (2). However, certain situations may require an alternative therapeutic approach. Medical therapy can be used as a primary or adjunctive option if the primary lesion is not fully resectable (e.g., due to size/location of the tumor or metastatic disease), if a surgical approach is not feasible due to severe comorbidities, or in line with the patient’s preference (1, 3).
Furthermore, drugs may help to control hypercortisolism in patients who suffer acute complications by severe hypercortisolism as well as in situations with persistent or recurrent symptoms after pituitary surgery, which may be the case in up to 20% of patients (4).
Various medical agents with different points of action have been identified for the treatment of hypercortisolism. Pituitary-directed drugs (e.g. pasireotide, cabergolin) inhibit central ACTH-secretion, whereas adrenal-directed drugs (e.g. ketoconazole, metyrapone) directly disrupt adrenal steroidogenesis. Recently, several new steroidogenesis inhibitors have been under investigation. Osilodrostat and levoketoconazole (the 2S, 4R enantiomer of ketoconazole), whose efficacy has now been demonstrated in several studies, offer certain advantages such as improved pharmacokinetics and reduced toxicity (3, 5, 6). Glucocorticoid receptor antagonists do not alter hormone production but inhibit the glucocorticoid receptor (7).
Mitotane (o,p’-dichlorodiphenyldichloroethane, o,p’-DDD), a derivate of the insecticide DDT (dichlorodiphenyltrichloroethane) (8), exhibits both adrenolytic and adrenostatic effects (9–11). Discovered in the 1950s, its cytotoxic effects were soon utilized for the treatment of adrenocortical carcinoma, where it showed beneficial effects on survival and long-term remission (12–14). Though not fully understood, the cytotoxic effects are thought to be mediated by the inhibition of mitochondrial respiratory chain complexes and the induction of endoplasmic reticulum (ER) stress. Subsequently, this leads to cell apoptosis and impairment of overall steroidogenesis with an almost mandatory necessity of glucocorticoid replacement therapy (11, 15–18). In contrast, mineralocorticoid deficiency is less frequent, as glomerulosa cells appear to be less affected by mitotane. Therefore, fludrocortisone replacement therapy was commenced in only 20 – 65% of patients usually due to orthostatic hypotension or dizziness. In addition, mineralocorticoid insufficiency occurred later, typically 6 – 9 months after initiation of mitotane (10, 19, 20).
At lower concentrations, mitotane predominantly inhibits several steps in adrenal steroid synthesis (e.g., cholesterol side-chain cleavage enzyme and 11-beta-hydroxylase), whereas cytolytic effects are reduced (9, 11, 19). Moreover, by an enhanced cortisol clearance through induction of cytochrome P450 3A4 (CYP3A4), and through increased levels of corticosteroid-binding globulin (CBG, transcortin), mitotane reduces the levels of biologically active cortisol (18, 20–22).
Hence, it can be used as an adrenostatic agent in ACTH-dependent hypercortisolism, where it has not only proven to be one of the most effective drugs in normalizing cortisol levels but also to have beneficial effects on clinical features, even in long-term treatment (7, 23–25). However, experience with mitotane in the treatment of CD is limited, especially regarding long-term treatment and its use under special circumstances.
The patient first presented as a 9-year-old girl at Leipzig University Hospital with cushingoid habitus, acne, and hirsutism in 1969. She was overweight and below average height for her age. Elevated levels of 17-ketosteroids and hydroxycorticosteroids were found in the patient’s urine, whereas imaging of the adrenal glands and the pituitary region (aortography of the adrenal glands and sella x-ray) showed no pathological findings. Clinical symptoms worsened throughout the next visits, in particular persistent growth retardation and development of a buffalo hump. Furthermore, an impaired glucose tolerance developed. Based on the loss of the physiological circadian rhythm of cortisol serum levels and a lack of suppression of cortisol in the 1 mg dexamethasone suppression test (DST), the diagnosis of endogenous hypercortisolism was established. Since ACTH assays as well as CT or MRI scans were not available at the hospital at that time, no further diagnostic workup was possible. Due to her religious beliefs (being Jehovah’s Witnesses), the patient’s mother decided against the recommended adrenalectomy, and the patient was discharged without any treatment.
At 16 years of age, as an operative treatment was still strictly rejected by the patient’s parents, medication with mitotane was initiated at a loading dose of 2 grams per day. At that time the patient weighed 65 kilograms, resulting in a weight-for-age above the 75th percentile. Within 3 months she lost 8 kilograms in weight and showed a normalisation of steroid levels. Mitotane treatment was monitored by periodical evaluation of the plasmatic concentration. The drug, by then downscaled to 1 gram per day, was well tolerated and, with the exception of elevated transaminases, no biochemical abnormalities were found. Within 12 months, the symptoms of hypercortisolism improved, her weight dropped to 47 kilograms, and a normal menstrual cycle developed. Laboratory analyses confirmed a normalization of transaminases and glucose metabolism.
Over the next years, further therapy was conducted in an outpatient setting closer to the patient’s hometown. During the first months, two hospitalizations became necessary due to gastroenteritis and malaise with vertigo, requiring short-term discontinuation of the drug with a subsequent dose adjustment. However, no overt signs of adrenal insufficiency were reported.
At the age of 23, with a daily dose of 750 mg mitotane, the patient gave birth to a boy via an uncomplicated primary cesarean delivery in the 35th week of gestation. Neither the mother nor the boy showed signs of adrenal insufficiency. Perioperatively, the mother was given prednisolone as a substitute. In response to slightly elevated serum cortisol levels after discharge, mitotane was titrated to the personal maximum dose of 1250 mg daily. At age 31 and still on the same amount of mitotane, the patient gave birth to another healthy boy. Both boys developed normally during infancy and adolescence and showed no signs of adrenal insufficiency to this day (being 40 and 32 years old at the time of this article).
At the age of 36, new features of hypercortisolism developed under 500 mg of mitotane per day. Further diagnostic workup for CD showed a lack of suppression in the 1 mg DST with elevated ACTH levels and a CRH stimulation test with a typical increase in ACTH and cortisol levels. As pituitary MRI showed no adenoma, petrosal sinus sampling was performed and excluded the ectopic origin of hypercortisolism (pituitary/peripheral gradient for ACTH was 35-fold on the left and 15-fold on the right). Subsequently, the patient consented to the proposed transsphenoidal surgery. Similarly to previous findings, no adenoma could be detected intraoperatively, and a central 1/3 resection of the pituitary was carried out. The histological examination showed discrete hyperplasia of ACTH-producing cells. As the symptoms of CD persisted, mitotane was continued. Even after a later hospitalization with sepsis in the context of massively elevated mitotane levels, the patient decided against radiation of the pituitary, as well as alternative medication with pasireotide, but insisted on continuing to take mitotane on her own responsibility. Over the long period of treatment serum concentrations of mitotane were very regularly monitored and consistently found within the target range.
In early 2013, the patient suffered a right-sided middle cerebral artery (MCA) stroke, and just a few months later, she was hospitalized due to an acute adrenal insufficiency in the context of an urosepsis. In the same year, she was admitted to our intensive care unit with an acute adrenal insufficiency and a massive exsiccosis. Clearly reduced morning serum cortisol levels (24 nmol/l) and a subsequently performed ACTH stimulation test revealed a primary adrenal insufficiency (reference range (RR) > 500 nmol/l). Replacement therapy with hydrocortisone and fludrocortisone was established due to a concomitant mineralocorticoid deficiency, whereas mitotane was stopped at a plasma level of 18.6 mg/l. Follow-up blood samples taken two months after discharge showed persistent primary adrenal insufficiency.
When the patient once again presented with symptoms of hypercortisolism in 2018, midnight cortisol levels were within normal ranges (42 nmol/l, ULN < 207). Although daytime cortisol values showed a circadian dynamic, the basal ACTH on the other hand was elevated to 31.45 pmol/l (RR 1.04 – 10.8). As the DST and brain MRI findings were unremarkable, the symptoms were not considered to require a specific treatment, even though the continuously elevated ACTH levels may suggest the persistence of central hypercortisolism. Since then, there have been regular endocrinological diagnostic work-ups, including regular MRI examinations, and the clinical situation remained unaltered. Moreover, no severe medical conditions have developed thus far.
Mitotane is the first-line treatment for adrenal carcinoma. One of its complex modes of action is its adrenolytic effect, resulting in a reduction of cortisol levels. Therefore, it presents one second-line treatment option also for CD. However, data from long-term applications is missing (2). A review of the literature revealed less than 200 reported cases with long-term use of mitotane (Table 1), with the longest reported intake period being 11.5 years (26).
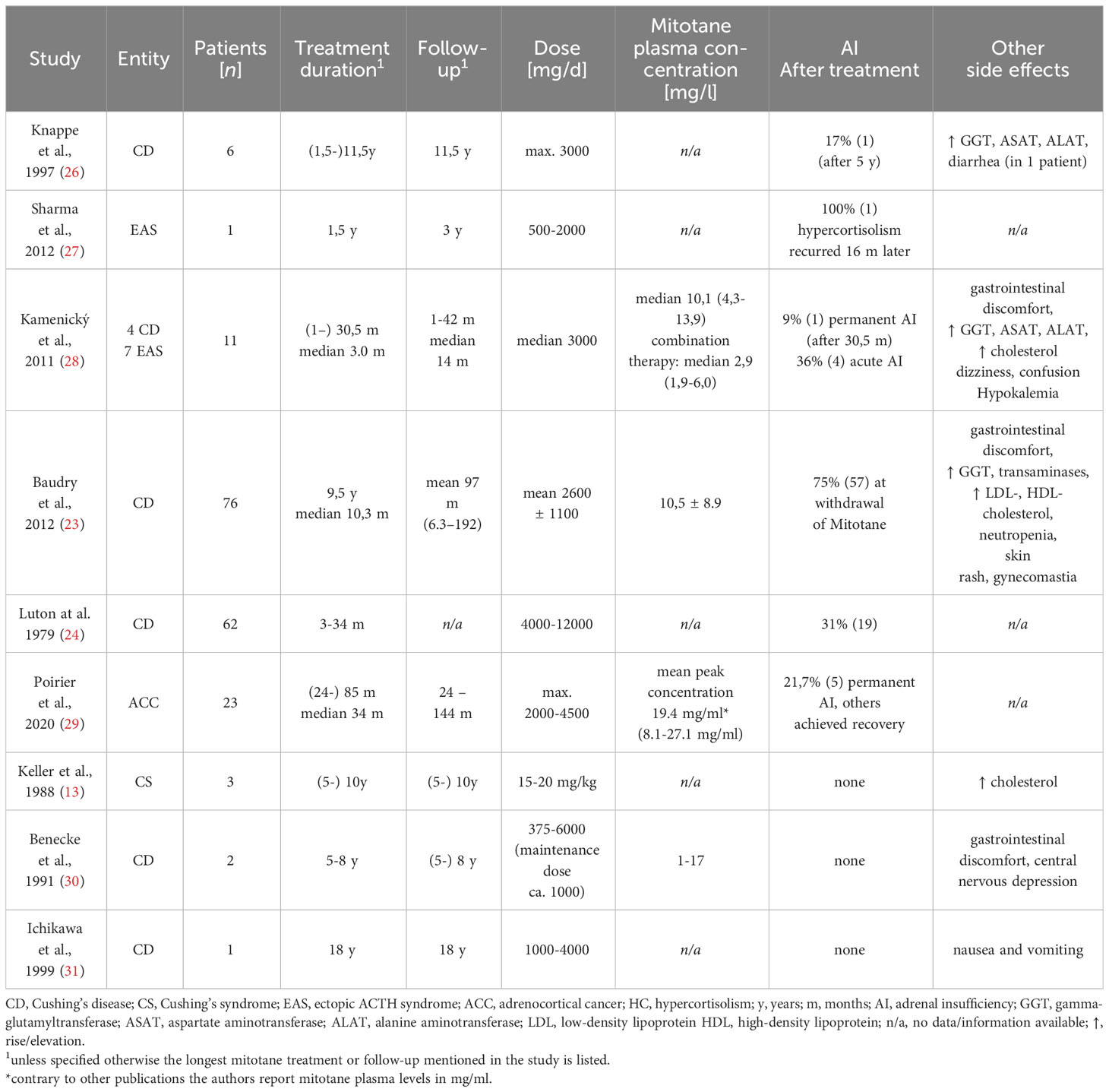
Table 1 Published case reports of long-term treatment with mitotane.
To the best of our knowledge, we hereby reported the longest documented treatment using mitotane, with a total duration of 37 years. This exceedingly long exposure allowed an exceptional insight into the potentials and challenges of therapy with mitotane. Contrary to many other reported cases, we saw a patient on exclusive single-drug therapy with mitotane, allowing us to examine the drug’s efficacy and side effects without any interference from other medication.
In our patient, the signs and symptoms of hypercortisolism regressed and a normalization of steroid levels was achieved within months after the initiation of mitotane. As specified by a recent meta-analysis by Broersen et al. (25), mitotane provides an effective control of cortisol levels in 80% of CD patients, and in that respect is the most effective drug among pasireotide, cabergoline, ketoconazole, and metyrapone.
In comparison, our patient’s daily dose of 125 to 1250 mg was lower than what was reported in other studies, e.g., 2600 ± 1100 mg described by Baudry et al. (23). Even though several dose adjustments were made due to side effects, the regimen could be maintained without the need for a dosage escalation over time. This underlines that, contrary to adrenostatic drugs, mitotane does not tend to treatment escape (4).
However, while the adrenolytic effects of mitotane are reduced at lower doses, adrenal insufficiency (AI) occurs regularly. Subsequently, glucocorticoid replacement becomes necessary in most of the patients (Table 1) (7, 10). Nonetheless, mitotane therapy without simultaneous steroid replacement was possible in our patient by performing both close clinical and laboratory monitoring.
It may be difficult to maintain the balance between beneficial and adverse drug effects. Mitotane shows high accumulation in adipose tissue, causing a half-life of up to 5 months (32). Differences in the individual intestinal metabolism and a correlation between free mitotane levels, considering the active fraction, and individual cholesterol and triglyceride concentrations fuel variability in drug levels (33). The drug`s toxic effects are hard to predict as they vary considerably and do not necessarily correlate with plasma levels. Furthermore, mitotane has a high potential for drug-drug interactions and an inductive effect on several CYP-enzymes (15). Therefore, side effects occurred in most of the reported patients and made permanent discontinuation of mitotane necessary in one-third of the cases (20, 23).
Over the years, our patient experienced a wide range of the most commonly reported toxic drug effects (Table 1), such as elevation of transaminases, gastrointestinal and neurological toxicities, as well as recurrent severe infections, which may indicate immune deficiency (23, 26, 34, 35). However, as the main part of the side effects appears to be dose-dependent and reversible (26, 34), they could be managed by several dose adjustments.
A remarkable aspect of our patient’s history is that she repeatedly developed severe anemia, which resolved within a few weeks after the withdrawal of mitotane. Even if rarely reported, observations from animals exposed to DDT isomers suggest a causal relationship, possibly due to inflammation-associated hypoferremia, inhibition of hematopoietic tissue, or an estrogenic inhibitory effect on red blood cells (15, 36, 37).
Taken together, our case highlights that through close collaboration with well-informed patients and regular evaluations of the dosage, toxic drug effects are manageable and long-term treatment is safe and effective.
The latest follow-up examinations of our patient revealed a physiological cortisol circadian dynamic, suggesting an at least partial, recovery of the adrenal function. Hypothalamus-pituitary-adrenal axis recovery after discontinuation of mitotane was also observed by other authors in up to 80% of their patients with a mean time to recovery of 2.7 years (28, 29). Although no predictors for recovery have been identified so far, this further supports the theory that adrenocortical tissue remains viable and normal adrenal function can be regained with lower drug concentrations (29).
One of the unique aspects of the presented case is that the patient gave birth to two healthy children while being treated with mitotane. This is remarkable, as not only hypercortisolism (38, 39) but also exposure to DDT and its isomers may affect fertility and pregnancy outcomes negatively (40–42).
Even though the majority of women with CD suffer from oligo- or amenorrhea (39), the history of our patient points out that mitotane provides sufficient control of cortisol levels. Therefore, a normal menstrual cycle and fertility could be restored.
Furthermore, despite the negative effects of DDT/DDD on gonadal function, which was established in an animal model (43) as well as in humans (20, 34), our case underlines that even at therapeutic levels of mitotane (14 – 20 mg/l), conception is possible (35).
Due to the negative impact of DDT and its derivates on pregnancy and fetal outcomes observed in animal and environmental studies (40, 44, 45), experts recommend avoiding pregnancy when taking mitotane (2). Consequently, the influence of mitotane on fetal development remains poorly understood and it is not clear whether the effects observed in DDT will occur in humans exposed to o,p’-DDD. Overall, we found a total of 21 documented pregnancies in association with mitotane intake (Table 2), the majority of which were terminated by therapeutic abortion.
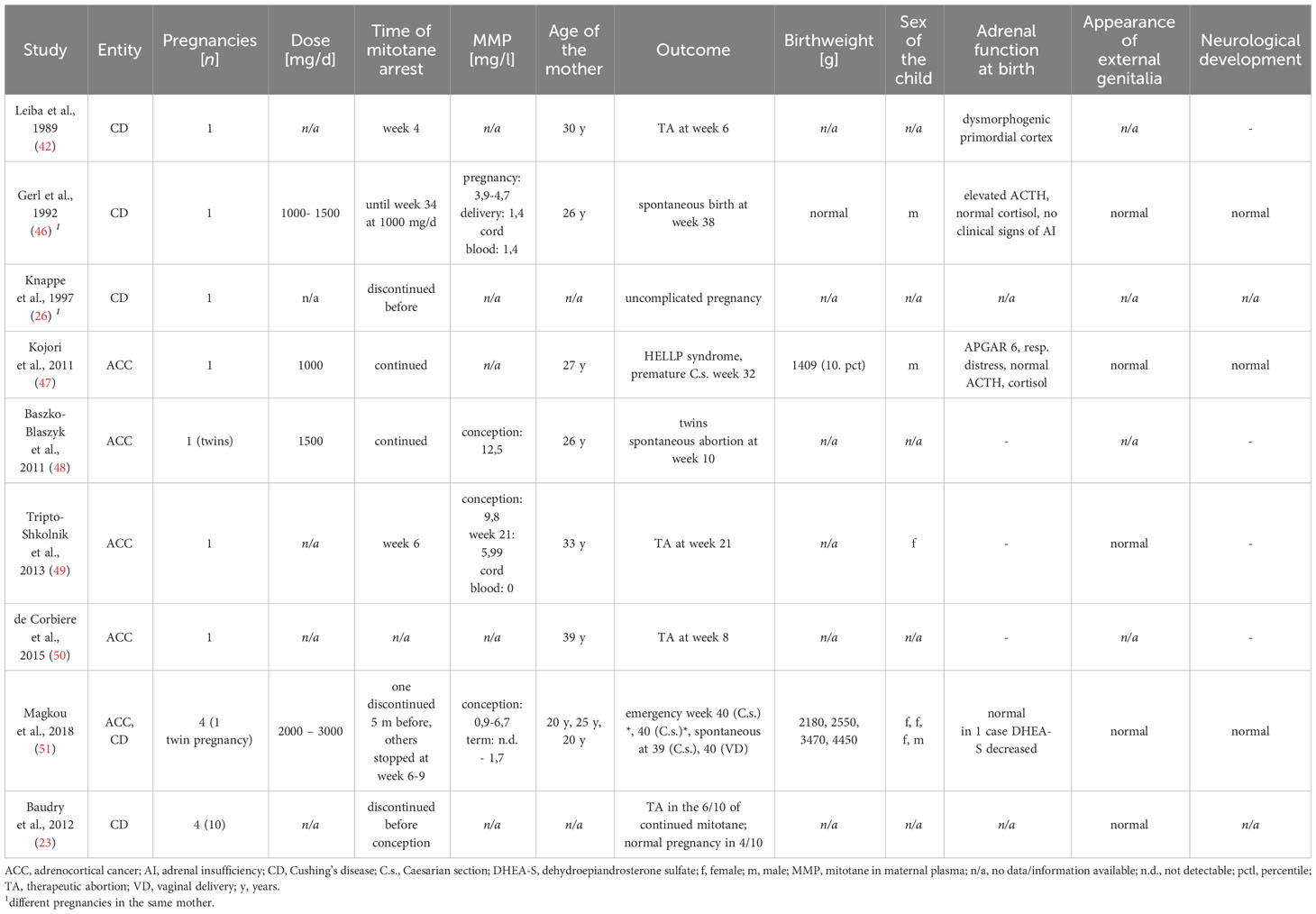
Table 2 Published case reports of pregnancy under mitotane intake.
Whereas several investigations suggest a negative impact of maternal exposure to DDT isomers on fetal neurologic development (52–54), in the context of mitotane, only Leiba et al. found a nervous system malformation in a fetus after abortion (42). In contrast, our patient’s sons, as well as the other live births, reported in Table 2, showed no neurologic impairments. Their normal educational and vocational development thus extends the findings of Magkou et al. (51), showing normal neurocognitive development throughout early childhood after exposure to mitotane in pregnancy.
Acute adrenal insufficiency, due to cytolytic effects on the fetus’ adrenal glands, was neither observed in our patient’s sons nor described in the other cases. This indicates that there is no impact on the offspring’s adrenal glands, or at least the possible impact remains tolerable at the applied doses. However, toxicity at higher plasma levels with an underlying dose-effect relationship, as seen in acute toxicity of mitotane, cannot be ruled out according to the available data.
In the examined studies, continued intake of mitotane was described only for one other case with a premature operative delivery subsequent to the development of a HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count) (47). In another case, a healthy infant was born after mitotane cessation at the 34th gestational week, with detectable maternal plasma levels at birth (26). In all the other live births, mitotane was either stopped before conception or in the first trimester. There was no regular evaluation of o,p’-DDD-plasma levels throughout pregnancy in most of the presented cases and there are inconsistent findings regarding the extent to which mitotane is transferred from the mother to the fetus (26, 49, 51).
Moreover, due to the small number of natural pregnancies, it is not possible to assess whether the increased risk of premature delivery, spontaneous abortion, or small-for-gestational-age that are associated with exposure to DDT/DDE, are also present in the case of mitotane exposure (45, 55, 56).
In summary, the data on the use of mitotane during pregnancy is incomplete. However there is also very little experience with other adrenostatic medications for pregnant women (2). Mitotane represents a possible therapy for patients for whom surgical therapy is not possible or desirable, also in long-term application.
In conclusion, we report the case of the longest documented application of mitotane in a patient with CD. In addition, we highlight the ability of mitotane to provide an efficient control of levels of cortisol, while adverse effects of the drug are manageable. Our patient’s medical history, underlined by the uncomplicated pregnancy and parturition of two healthy children, suggests that mitotane may be a long-term alternative if surgery or other therapeutic options are not feasible.
JS: Writing – original draft. MH: Writing – original draft, Writing – review & editing. AT: Writing – review & editing. BS: Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors acknowledge support from the German Research Foundation (DFG) and Universität Leipzig within the program of Open Access Publishing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Fleseriu M, Auchus R, Bancos I, Ben-Shlomo A, Bertherat J, Biermasz NR, et al. Consensus on diagnosis and management of Cushing’s disease: a guideline update. Lancet Diabetes Endocrinol (2021) 9:847–75. doi: 10.1016/S2213-8587(21)00235-7
2. Nieman LK, Biller BM, Findling JW, Murad MH, Newell-Price J, Savage MO, et al. Treatment of Cushing’s syndrome: an endocrine society clinical practice guideline. J Clin Endocrinol Metab (2015) 100:2807–31. doi: 10.1210/jc.2015-1818
3. Tritos NA. Adrenally directed medical therapies for cushing syndrome. J Clin Endocrinol Metab (2021) 106:16–25. doi: 10.1210/clinem/dgaa778
4. Pivonello R, De Leo M, Cozzolino A, Colao A. The treatment of Cushing’s disease. Endocrine Rev (2015) 36:385–486. doi: 10.1210/er.2013-1048
5. Pivonello R, Fleseriu M, Newell-Price J, Bertagna X, Findling J, Shimatsu A, et al. Efficacy and safety of osilodrostat in patients with Cushing’s disease (LINC 3): a multicentre phase III study with a double-blind, randomised withdrawal phase. Lancet Diabetes Endocrinol (2020) 8:748–61. doi: 10.1016/S2213-8587(20)30240-0
6. Pivonello R, Elenkova A, Fleseriu M, Feelders RA, Witek P, Greenman Y, et al. Levoketoconazole in the treatment of patients with cushing’s syndrome and diabetes mellitus: results from the SONICS phase 3 study. Front Endocrinol (Lausanne) (2021) 12:595894. doi: 10.3389/fendo.2021.595894
7. Pivonello R, Ferrigno R, De Martino MC, Simeoli C, Di Paola N, Pivonello C, et al. Medical treatment of cushing’s disease: an overview of the current and recent clinical trials. Front Endocrinol (Lausanne) (2020) 11:648–. doi: 10.3389/fendo.2020.00648
8. Fassnacht M, Kroiss M, Allolio B. Update in adrenocortical carcinoma. J Clin Endocrinol Metab (2013) 98:4551–64. doi: 10.1210/jc.2013-3020
9. Brown RD, Nicholson WE, Chick WT, Strott CA. Effect of o,p’DDD on Human Adrenal Steroid llβ-Hydroxylation Activity. J Clin Endocrinol Metab (1973) 36:730–3. doi: 10.1210/jcem-36-4-730
10. Bianchini M, Puliani G, Chiefari A, Mormando M, Lauretta R, Appetecchia M. Metabolic and endocrine toxicities of mitotane: A systematic review. Cancers (2021) 13:5001. doi: 10.3390/cancers13195001
11. Hescot S, Amazit L, Lhomme M, Travers S, DuBow A, Battini S, et al. Identifying mitotane-induced mitochondria-associated membranes dysfunctions: metabolomic and lipidomic approaches. Oncotarget (2017) 8:109924–40. doi: 10.18632/oncotarget.18968
12. Hutter AM Jr., Kayhoe DE. Adrenal cortical carcinoma: Results of treatment with o, p’DDD in 138 patients. Am J Med (1966) 41:581–92. doi: 10.1016/0002-9343(66)90220-8
13. Keller E, Benecke R, Vetter B, Willgerodt H. LONG-TERM TREATMENT OF HYPOTHALAMIC-PITUITARY CUSHING SYNDROME WITH o,p’-DDD IN LOW DOSAGE. Pediatr Res (1988) 23:129. doi: 10.1203/00006450-198801000-00170
14. Becker D, Schumacher OP. o, p’DDD therapy in invasive adrenocortical carcinoma. Ann Internal Med (1975) 82:677–9. doi: 10.7326/0003-4819-82-5-677
15. Corso CR, Acco A, Bach C, Bonatto SJR, de Figueiredo BC, de Souza LM. Pharmacological profile and effects of mitotane in adrenocortical carcinoma. Br J Clin Pharmacol (2021) 87:2698–710. doi: 10.1111/bcp.14721
16. Poli G, Guasti D, Rapizzi E, Fucci R, Canu L, Bandinelli A, et al. Morphofunctional effects of mitotane on mitochondria in human adrenocortical cancer cells. Endocrine-Related Cancer (2013) 20:537–50. doi: 10.1530/ERC-13-0150
17. Lo Iacono M, Puglisi S, Perotti P, Saba L, Petiti J, Giachino C, et al. Molecular mechanisms of mitotane action in adrenocortical cancer based on in vitro studies. Cancers (2021) 13:5255. doi: 10.3390/cancers13215255
18. Chortis V, Taylor AE, Schneider P, Tomlinson JW, Hughes BA, O’Neil DM, et al. Mitotane therapy in adrenocortical cancer induces CYP3A4 and inhibits 5α-reductase, explaining the need for personalized glucocorticoid and androgen replacement. J Clin Endocrinol Metab (2013) 98:161–71. doi: 10.1210/jc.2012-2851
19. Hart MM, Reagan RL, Adamson RH. The effect of isomers of DDD on the ACTH-induced steroid output, histology and ultrastructure of the dog adrenal cortex. Toxicol Appl Pharmacol (1973) 24:101–13. doi: 10.1016/0041-008X(73)90185-3
20. Daffara F, De Francia S, Reimondo G, Zaggia B, Aroasio E, Porpiglia F, et al. Prospective evaluation of mitotane toxicity in adrenocortical cancer patients treated adjuvantly. Endocrine-Related Cancer (2008) 15:1043–53. doi: 10.1677/ERC-08-0103
21. Bae YJ, Kratzsch J. Corticosteroid-binding globulin: modulating mechanisms of bioavailability of cortisol and its clinical implications. Best Pract Res Clin Endocrinol Metab (2015) 29:761–72. doi: 10.1016/j.beem.2015.09.001
22. Alexandraki KI, Kaltsas GA, Le Roux CW, Fassnacht M, Ajodha S, Christ-Crain M, et al. Assessment of serum-free cortisol levels in patients with adrenocortical carcinoma treated with mitotane: a pilot study. Clin Endocrinol (2010) 72:305–11. doi: 10.1111/j.1365-2265.2009.03631.x
23. Baudry C, Coste J, Bou Khalil R, Silvera S, Guignat L, Guibourdenche J, et al. Efficiency and tolerance of mitotane in Cushing’s disease in 76 patients from a single center. Eur J Endocrinol (2012) 167:473–81. doi: 10.1530/EJE-12-0358
24. Luton J, Mahoudeau J, Bouchard P, Thieblot P, Hautecouverture M, Simon D, et al. Treatment of Cushing’s disease by o, p′ DDD: survey of 62 cases. New Engl J Med (1979) 300:459–64. doi: 10.1056/NEJM197903013000903
25. Broersen LHA, Jha M, Biermasz NR, Pereira AM, Dekkers OM. Effectiveness of medical treatment for Cushing’s syndrome: a systematic review and meta-analysis. Pituitary (2018) 21:631–41. doi: 10.1007/s11102-018-0897-z
26. Knappe G, Gerl H, Ventz M, Rohde W. Langzeit-Therapie des hypothalamisch-hypophysären Cushing-Syndroms mit Mitotan (o, p’-DDD). DMW-Deutsche Medizinische Wochenschrift (1997) 122:882–6. doi: 10.1055/s-2008-1047704
27. Sharma S, Nieman L. Prolonged remission after long-term treatment with steroidogenesis inhibitors in Cushing’s syndrome caused by ectopic ACTH secretion. Eur J endocrinology/European Fed Endocrine Societies (2012) 166:531. doi: 10.1530/EJE-11-0949
28. Kamenický P, Droumaguet C, Salenave S, Blanchard A, Jublanc C, Gautier J-F, et al. Mitotane, metyrapone, and ketoconazole combination therapy as an alternative to rescue adrenalectomy for severe ACTH-dependent Cushing’s syndrome. J Clin Endocrinol Metab (2011) 96:2796–804. doi: 10.1210/jc.2011-0536
29. Poirier J, Gagnon N, Terzolo M, Puglisi S, Ghorayeb NE, Calabrese A, et al. Recovery of adrenal insufficiency is frequent after adjuvant mitotane therapy in patients with adrenocortical carcinoma. Cancers (2020) 12:639. doi: 10.3390/cancers12030639
30. Benecke R, Keller E, Vetter B, de Zeeuw RA. Plasma level monitoring of mitotane (o,p’-DDD) and its metabolite (o,p’-DDE) during long-term treatment of cushing’s disease with low doses. Eur J Clin Pharmacol (1991) 41:259–61. doi: 10.1007/BF00315440
31. Ichikawa Y, Kaburaki J, Yoshida T, Kawai S. 18 years mitotane therapy for intractable Cushing’s disease. Lancet (1999) 354:951. doi: 10.1016/S0140-6736(05)75699-3
32. Moolenaar A, Van Slooten H, Van Seters A, Smeenk D. Blood levels of o, p′-DDD following administration in various vehicles after a single dose and during long-term treatment. Cancer Chemother Pharmacol (1981) 7:51–4. doi: 10.1007/BF00258213
33. Kroiss M, Plonné D, Kendl S, Schirmer D, Ronchi CL, Schirbel A, et al. Association of mitotane with chylomicrons and serum lipoproteins: practical implications for treatment of adrenocortical carcinoma. Eur J Endocrinol (2016) 174:343–53. doi: 10.1530/EJE-15-0946
34. Kerkhofs TM, Baudin E, Terzolo M, Allolio B, Chadarevian R, Mueller HH, et al. Comparison of two mitotane starting dose regimens in patients with advanced adrenocortical carcinoma. J Clin Endocrinol Metab (2013) 98:4759–67. doi: 10.1210/jc.2013-2281
35. Haak HR, Hermans J, van de Velde CJH, Lentjes E, Goslings BM, Fleuren GJ, et al. Optimal treatment of adrenocortical carcinoma with mitotane: results in a consecutive series of 96 patients. Br J Cancer (1994) 69:947–51. doi: 10.1038/bjc.1994.183
36. Fourie FR, Hattingh J. DDT administration: haematological effects observed in the crowned Guinea-fowl (Numida meleagris). J Environ Pathol Toxicol (1979) 2:1439–46.
37. Tomita M, Yoshida T, Fukumori J, Yamaguchi S, Kojima S, Fukuyama T, et al. p,p’-DDT induces microcytic anemia in rats. J Toxicol Sci (2013) 38:775–82. doi: 10.2131/jts.38.775
38. Lindsay JR, Jonklaas J, Oldfield EH, Nieman LK. Cushing’s syndrome during pregnancy: personal experience and review of the literature. J Clin Endocrinol Metab (2005) 90:3077–83. doi: 10.1210/jc.2004-2361
39. Caimari F, Valassi E, Garbayo P, Steffensen C, Santos A, Corcoy R, et al. Cushing’s syndrome and pregnancy outcomes: a systematic review of published cases. Endocrine (2017) 55:555–63. doi: 10.1007/s12020-016-1117-0
40. Lysodren - EPAR. Scientific Discussion (2006). Available at: https://www.ema.europa.eu/documents/scientific-discussion/lysodren-epar-scientific-discussion_en.pdf.
41. Guo H, Jin Y, Cheng Y, Leaderer B, Lin S, Holford TR, et al. Prenatal exposure to organochlorine pesticides and infant birth weight in China. Chemosphere (2014) 110:1–7. doi: 10.1016/j.chemosphere.2014.02.017
42. Leiba S, Weinstein R, Shindel B, Lapidot M, Stern E, Levavi H, et al. The protracted effect of o, p’-DDD in Cushing’s disease and its impact on adrenal morphogenesis of young human embryo. Ann Endocrinol (Paris) (1989) 50(1):49–53.
43. Rhouma KB, Tebourbi O, Krichah R, Sakly M. Reproductive toxicity of DDT in adult male rats. Hum Exp Toxicol (2001) 20:393–7. doi: 10.1191/096032701682692946
44. Fabro S, McLachlan J, Dames N. Chemical exposure of embryos during the preimplantation stages of pregnancy: mortality rate and intrauterine development. Am J Obstetrics Gynecol (1984) 148:929–38. doi: 10.1016/0002-9378(84)90535-0
45. Longnecker MP, Klebanoff MA, Zhou H, Brock JW. Association between maternal serum concentration of the DDT metabolite DDE and preterm and small-for-gestational-age babies at birth. Lancet (2001) 358:110–4. doi: 10.1016/S0140-6736(01)05329-6
46. Gerl H, Benecke R, Knappe G, Rohde W, Stahl F, Amendt P. Pregnancy and partus in Cushing’s disease treated withoff, p’-DDD. Acta Endocrinol (Copenh) (1992) 126:133.
47. Kojori F, Cronin CMG, Salamon E, Burym C, Sellers EAC. Normal adrenal function in an infant following a pregnancy complicated by maternal adrenal cortical carcinoma and mitotane exposure. J Pediatr Endocrinol Metab (2011) 24:203–4. doi: 10.1515/jpem.2011.123
48. Baszko-Błaszyk D, Ochmańska K, Waśko R, Sowiński J. Pregnancy in a patient with adrenocortical carcinoma during treatment with Mitotane—a case report. Endokrynologia Polska (2011) 62:186–8.
49. Tripto-Shkolnik L, Blumenfeld Z, Bronshtein M, Salmon A, Jaffe A. Pregnancy in a patient with adrenal carcinoma treated with mitotane: a case report and review of literature. J Clin Endocrinol Metab (2013) 98:443–7. doi: 10.1210/jc.2012-2839
50. de Corbière P, Ritzel K, Cazabat L, Ropers J, Schott M, Libé R, et al. Pregnancy in women previously treated for an adrenocortical carcinoma. J Clin Endocrinol Metab (2015) 100:4604–11. doi: 10.1210/jc.2015-2341
51. Magkou D, Do Cao C, Bouvattier C, Douillard C, de Marcellus C, Cazabat L, et al. Foetal exposure to mitotane/Op’DDD: Post-natal study of four children. Clin Endocrinol (2018) 89:805–12. doi: 10.1111/cen.13854
52. Bornman M, Pretorius E, Marx J, Smit E, van der Merwe C. Ultrastructural effects of DDT, DDD, and DDE on neural cells of the chicken embryo model. Environ Toxicol: Int J (2007) 22:328–36. doi: 10.1002/tox.20261
53. Torres-Sánchez L, Rothenberg SJ, Schnaas L, Cebrián ME, Osorio E, del Carmen Hernández M, et al. In utero p, p′-DDE exposure and infant neurodevelopment: a perinatal cohort in Mexico. Environ Health Perspectives (2007) 115:435–9. doi: 10.1289/ehp.9566
54. Ribas-Fitó N, Torrent M, Carrizo D, Muñoz-Ortiz L, Júlvez J, Grimalt JO, et al. In utero exposure to background concentrations of DDT and cognitive functioning among preschoolers. Am J Epidemiol (2006) 164:955–62. doi: 10.1093/aje/kwj299
55. Korrick SA, Chen C, Damokosh AI, Ni J, Liu X, Cho S-I, et al. Association of DDT with spontaneous abortion: a case-control study. Ann Epidemiol (2001) 11:491–6. doi: 10.1016/S1047-2797(01)00239-3
Keywords: mitotane, Cushing’s syndrome, pregnancy, long-term treatment, adrenostatic drug
Citation: Seibold J, Hönemann M, Tönjes A and Sandner B (2024) Safe long-term therapy of Cushing’s syndrome over 37 years with mitotane. Front. Endocrinol. 15:1294415. doi: 10.3389/fendo.2024.1294415
Received: 14 September 2023; Accepted: 29 January 2024;
Published: 19 February 2024.
Edited by:
Giuseppe Reimondo, University of Turin, ItalyReviewed by:
Rosa Maria Paragliola, Saint Camillus International University of Health and Medical Sciences, ItalyCopyright © 2024 Seibold, Hönemann, Tönjes and Sandner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Benjamin Sandner, YmVuamFtaW4uc2FuZG5lckBtZWRpemluLnVuaS1sZWlwemlnLmRl
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.