
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 06 December 2023
Sec. Thyroid Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1301620
 Nan Liang1
Nan Liang1 Han Zhang2
Han Zhang2 Chengqiu Sui1
Chengqiu Sui1 Rui Du1
Rui Du1 Canxiao Li1
Canxiao Li1 Jingting Li1
Jingting Li1 Gianlorenzo Dionigi3
Gianlorenzo Dionigi3 Daqi Zhang1*
Daqi Zhang1* Hui Sun1*†
Hui Sun1*†Background: Despite improvements in overall survival, the recurrence of differentiated thyroid cancer (DTC) is becoming more common and remains a challenge necessitating accurate reappraisal of the patient. This study aimed to describe the characteristics, reasons, morbidity, and strategies of second operations for DTC.
Methods: This was a retrospective observational study of patients with DTC who underwent a second surgery between June 2008 and June 2021 in the Department of Thyroid Surgery at China–Japanese Union Hospital, Jilin University, P.R. China. All clinical characteristics were recorded, and the analysis was estimated using SPSS.
Results: Second surgeries were detected in 683 patients. The proportion of second operations changed with the update of international guidelines from 2015 (P < 0.001). The true recurrence rate progressively increased from 21.3% to 61.5%. The rate of an “absence of preoperative FNA” or an “absence of intraoperative pathology at first surgery” decreased from 49.8% to 12.7%, while that of a “misdiagnosis of preoperative FNA at second surgery” decreased from 10% to 1.8%. The most common tumor location during the second surgery was the lateral lymph nodes (n = 104, 36.5%), with a median time to relapse of 36 months. Completion of thyroidectomy and lymph node dissection correlated with the second operation.
Conclusion: After 2015, second surgeries were more standardized, the incidence of complications decreased, and real recurrence became the most common reason for a second DTC surgery.
The incidence of thyroid cancer has been increasing all over the world (1). Differentiated thyroid cancer (DTC) is the principal histologic type of thyroid gland cancer, accounting for the majority of thyroid malignancies (2). In addition, outcomes related to various treatment options can vary significantly based on different clinicopathologic factors, tumor size, and genetic variants related to tumor biology. Regardless of etiology and treatment strategy, DTC can recur (3). As such, postoperative surveillance is warranted, and when recurrence is detected, the reassessment of disease status and treatment options is necessary. Within this context, the incidence of second DTC surgeries has also increased (3).
Treatment algorithms and data on the management of recurrent DTC are critical to guide clinical decisions. Due to the advances in early diagnosis, improvements in guidelines, and the optimization of treatment options, patients with recurrent DTC now have better prognoses (3). Furthermore, due to altered anatomy, the risk of complications such as hypoparathyroidism and vocal fold paralysis following a second surgery is higher than that after the initial surgery (4). Moreover, with the further improvement of DTC guidelines and the standardization of diagnosis and treatment, the reasons for DTC second surgery have also changed. Meanwhile, the diagnosis and treatment strategy of DTC second surgery are affected by many factors (5). The effective and standard treatments are worthy studied (6). In this context, further investigation of the epidemiologic, treatment, and clinical features of recurrent DTC is essential. This study aims to clarify the status of the second surgeries by analyzing the features, reasons and surgical strategies of the second surgery of DTC patients in our center, so as to provide a theoretical basis for the standardized treatment of the second surgeries.
This was a retrospective observational study.
This single-center study was carried out at the China–Japan Union Hospital of Jilin University, China.
This study lasted for 13 years, i.e., from June 2008 to June 2021.
The institutional ethics committee of the China–Japan Union Hospital of Jilin University approved this study (20220506023). All included patients signed informed consent forms.
Patients of either sex were included if they had a cytological diagnosis of DTC, had experienced just one thyroid surgery procedure before, and were indicated to undergo a redo surgery, and the second operation was offered at the Thyroid Surgery Division of the China–Japan Union Hospital of Jilin University.
Patients with benign histology, undetermined malignant potential tumors, medullary thyroid cancer, non-thyroidal malignancies, incomplete information, or previous tumor ablation were excluded. We also did not include any individual who had received prior anti-tumor treatment, including chemotherapy, radiotherapy, or immunotherapy, or who was participating in an interventional trial with an expected impact on the outcome of the present study. Finally, any patient with a contraindication to redo surgery; who was not available for follow-up; who did not undergo primary tumor resection at initial surgery, i.e., only experienced local incision or palliative treatment; who did not provide informed consent.
According to Duren ‘s criteria, relapses of thyroidal carcinoma were classified as either local (may present itself in the residual thyroid lobe or in the thyroid bed where surgery was performed), loco-regional (may present in the cervical lymph nodes of the central compartment or lateral-cervical nodes), or distant (distant metastasis) more than one year after the previous operation (7).
Persistent disease was defined by a positive Tg result, an abnormal neck ultrasound image, or persistently increased levels of TgAb.
Patients were considered disease-free when they showed (1) no clinical evidence of a tumor, (2) no evidence of a tumor on radioactive iodine imaging and/or cervical ultrasound, or (3) an unstimulated serum Tg concentration of <0.2 ng/mL or stimulated Tg concentration of <1 ng/mL in the absence of interfering antibodies (Abs) (8).
All included patients underwent thyroid function tests (including serum T3, T4, and TSH; Tg; and TgAbs), neck ultrasound (US) imaging, preoperative fine-needle aspiration cytology, FNA-Tg (if suspected LNM), subsequently postoperative pathology analyses. Some patients took the CT scan, MRI, PET when necessary (8).
During the second surgery, we routinely obtained tumor tissue samples for histological analysis by surgical resection. Recruited DTC patients were divided into papillary thyroid cancer (PTC) and follicular thyroid cancer (FTC) groups.
Before their second surgery, each patient underwent a new laryngoscopy examination to determine the condition of their laryngeal recurrent nerve. In addition, iPTH, calcitonin, and blood calcium tests were routinely performed.
The follow-up for patients after the second surgery is similar to that following the primary surgery; specifically, US imaging was performed, and biochemical indicators (e.g., Tg; serum T3, T4, and TSH; and blood calcium) were measured.
A total of 1557 patients undergoing re-operation were identified. After applying the exclusion criteria, 683 (43.8%) patients were included in this study (Figure 1).
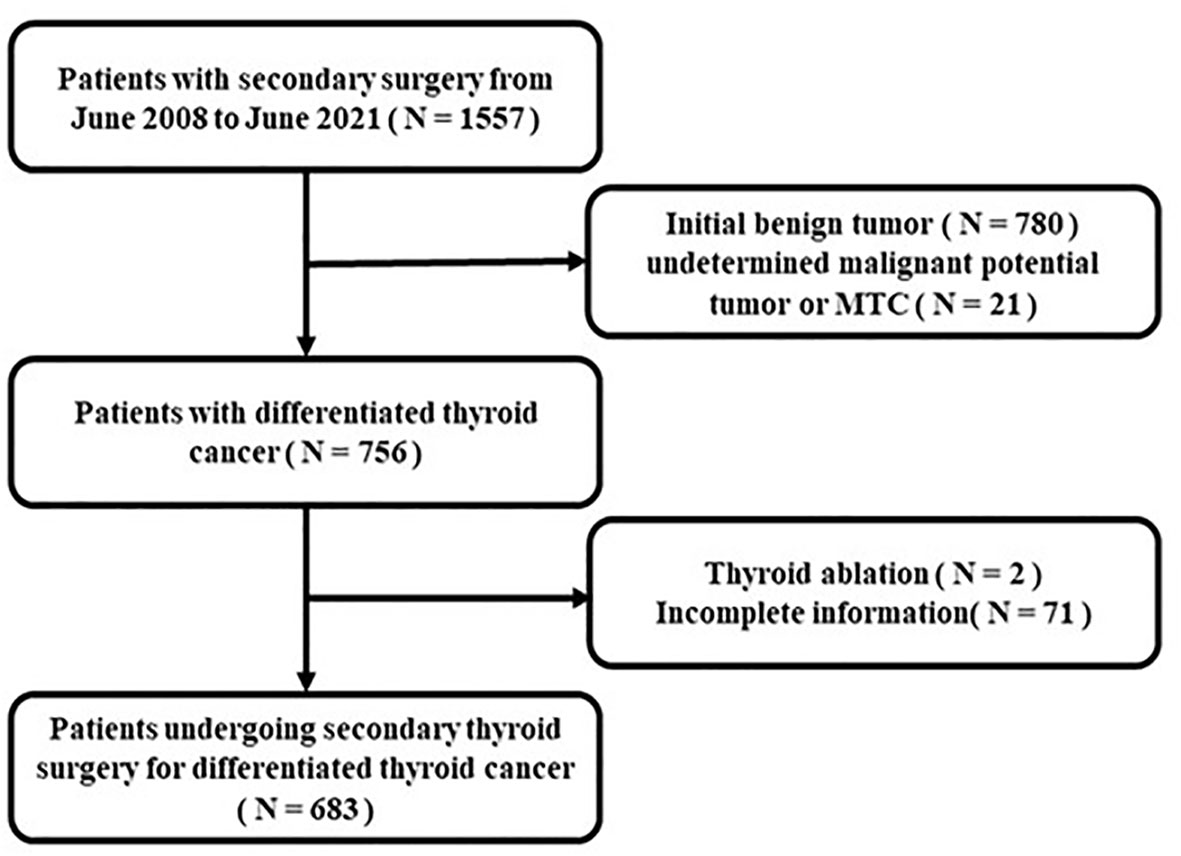
Figure 1 Flowchart of the inclusion and exclusion criteria.
Thyroid: Total thyroidectomy (TT); near TT; sub-TT; lobectomy + isthmusectomy; <lobectomy (i.e., nodulectomy) (9).
Lymph node: central lymph node dissection (CLND); unilateral lateral lymph node dissection (LLND); CLND +unilateral LLND; bilateral LLND; CLND + bilateral LLND (9).
We collected and reviewed the initial pathology using the patients’ medical history. The reasons for the second surgery were classified into five groups and also divided into objective reasons, subjective reasons, and real recurrence. Objective reasons included “lack of preoperative FNA or intraoperative pathology in the initial surgery” and “lack or misdiagnosis of preoperative FNA in the second surgery.” Subjective reasons included “less-experienced surgeons” and a “less-experienced paramedical team.” The time of recurrence was measured from the date of the previous neck operation.
We segmented the timing of reoccurrence into three parts according to the 2012 Chinese expert consensus and 2015 ATA guidelines, as follows: June 2008 to December 2012, January 2013 to December 2015, and January 2016 to June 2021 (8).
We analyzed all data using SPSS version 23.0 (IBM Corporation, Armonk, NY, USA). All results are shown as mean ± standard deviation, median, and interquartile range or count (percentage) values. Continuous variables were analyzed by Fisher’s exact test and the rank-sum test. Categorical variables were analyzed with an analysis of variance test, or, in the case of non-normal distribution, using the Kruskal–Wallis test. P < 0.05 was considered statistically significant. Charts were generated using GraphPad Prism version 8.0 (GraphPad Software, San Diego, CA, USA).
A total of 683 patients were enrolled, comprising 172 men (25.2%) and 511 women (74.8%). The male-to-female ratio was 1:2.97 (Table 1). Patients’ mean age at the initial and second surgeries was 37.94 ± 11.39 and 40.74 ± 11.25 years, respectively. The median body mass index was 24.2 (21.8; 26.7). The majority of tumors were PTC (97.2%), with just 2.8% being FTC. Total thyroidectomy was the most common operation among both initial surgeries (n = 222, 32.5%) and second surgeries (n = 317, 46.4%). As for cervical lymph node dissection during the second surgery, CLND + unilateral LLND was performed most often (n = 252, 36.9%). The median operative time for the second operation was 180 (135; 232) min. Thirty-six patients (5.3%) developed vocal cord paralysis, and 73 subjects (10.7%) had transient hypoparathyroidism.
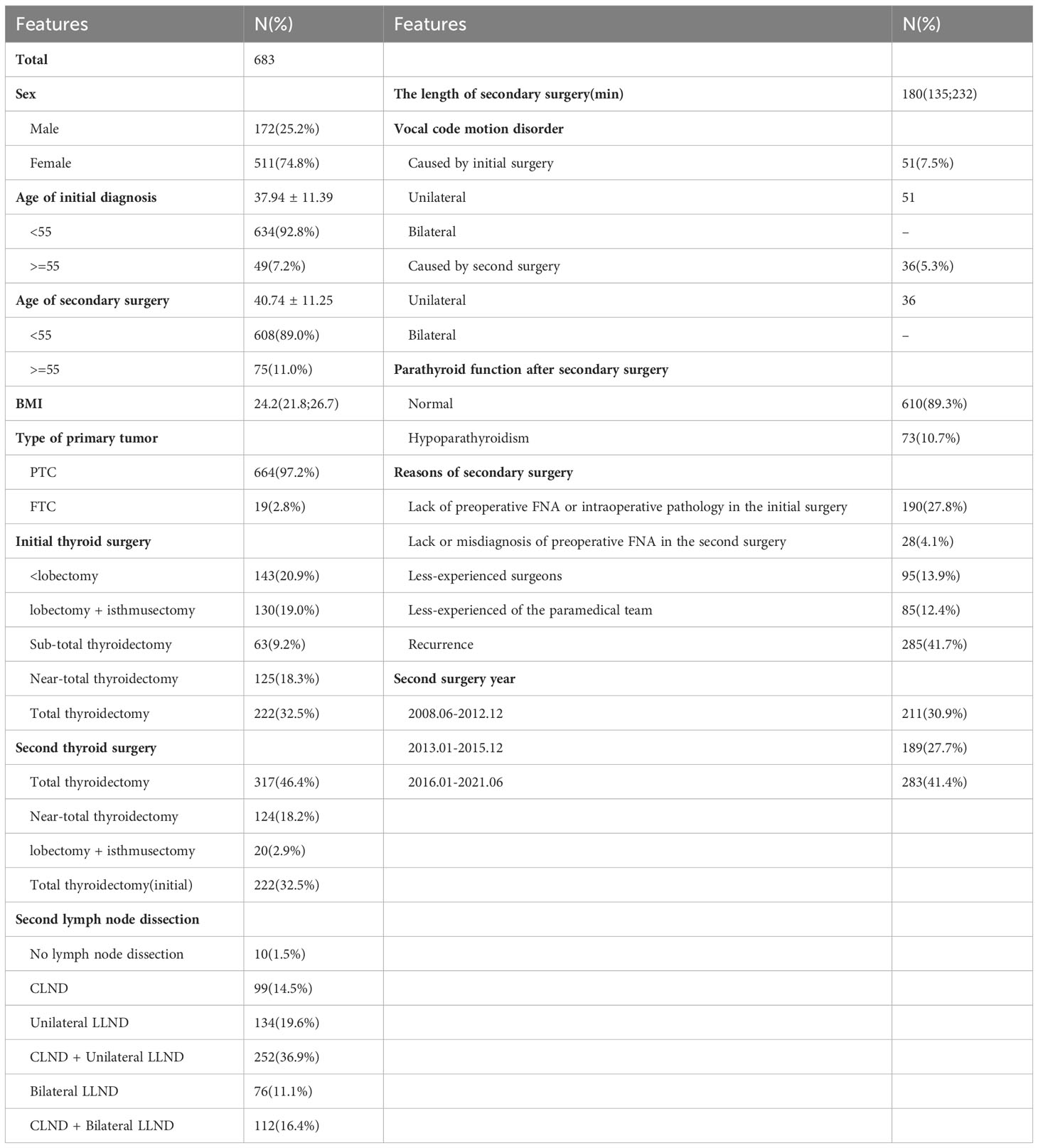
Table 1 Clinical features of second-surgery DTC patients.
54.1% of patients who underwent re-operation suffered from persistent disease, and 41.7% of patients experienced true recurrence after an initial disease-free interval.
Every patient’s clinical information was critically reviewed thoroughly, and the specific inferred the reasons were analyzed and classified. Objective reasons included “lack of preoperative FNA or intraoperative pathology in the initial surgery” (n = 188, 27.5%) and “lack or misdiagnosis of preoperative FNA in the second surgery” (n = 19, 2.8%). Subjective reasons included “less-experienced surgeons” (n = 99, 14.5%) and a “less-experienced paramedical team” (n = 92, 13.5%). In fact, the “less-experienced surgeons” refer to improper surgical procedures during the initial operation, and similarly, the so-called “low experienced paramedical team” refer to the incomplete or inaccurate evaluation results during the initial evaluation. A total of 285 patients (41.7%) experienced “real recurrence.”
Further analysis found that, with the continuous updating of guidelines (Table 2), the proportion of different reasons for the second surgery changed (P < 0.001). The percentage of patients with true recurrence gradually increased from 21.3% (first stage) to 34.9% (second stage) and 61.5% (third stage), while the percentage of second surgeries performed due to objective reasons gradually decreased (P < 0.001), with operations attributed to a “lack of preoperative FNA or intraoperative pathology in the initial surgery” decreasing from 49.8% in the first stage to 12.7% in the third stage and those attributed to a “lack or misdiagnosis of preoperative FNA in the second surgery” dropping from 10% in the first stage to 1.8% in the third stage. However, there was no significant difference in the proportion of operations performed for subjective reasons among the three stages. Supplementary Table 1 shows the differences in clinicopathological characteristics of patients who underwent second surgeries in each of the three stages. Total thyroidectomy (P < 0.001) became the main option for the second thyroid surgery. The length of the second surgery was also gradually shortened (225 vs. 180 vs. 150 min, P < 0.001).
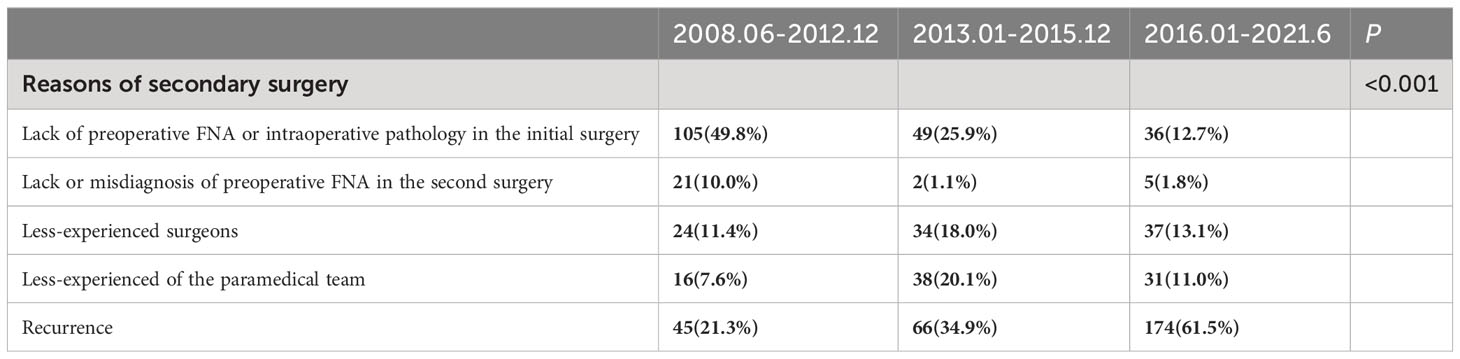
Table 2 Different reasons of second-surgery DTC patients in different stages.
We compiled the tumor location from the second surgery in cases of real recurrence (Figure 2A); the main tumor location during second surgeries was the lateral lymph nodes (n = 104, 36.5%), followed by the central + lateral lymph nodes (n = 72, 25.3%) and the thyroid lobe + lymph node (n = 64, 22.5%). In addition, there were 30 patients with recurrence in the contralateral thyroid lobe, accounting for 10.5% of all cases. We further studied the recurrence time of DTC patients among 285 cases with real recurrence (Figure 2B). More than 50% of the cohort experienced relapse within 36 months, and the majority of recurrence cases (71.5%) occurred within the first 5 years after the initial surgery. The follow-up duration ranges from 12 months to 264 months, with a median re-operation time of 36 months.
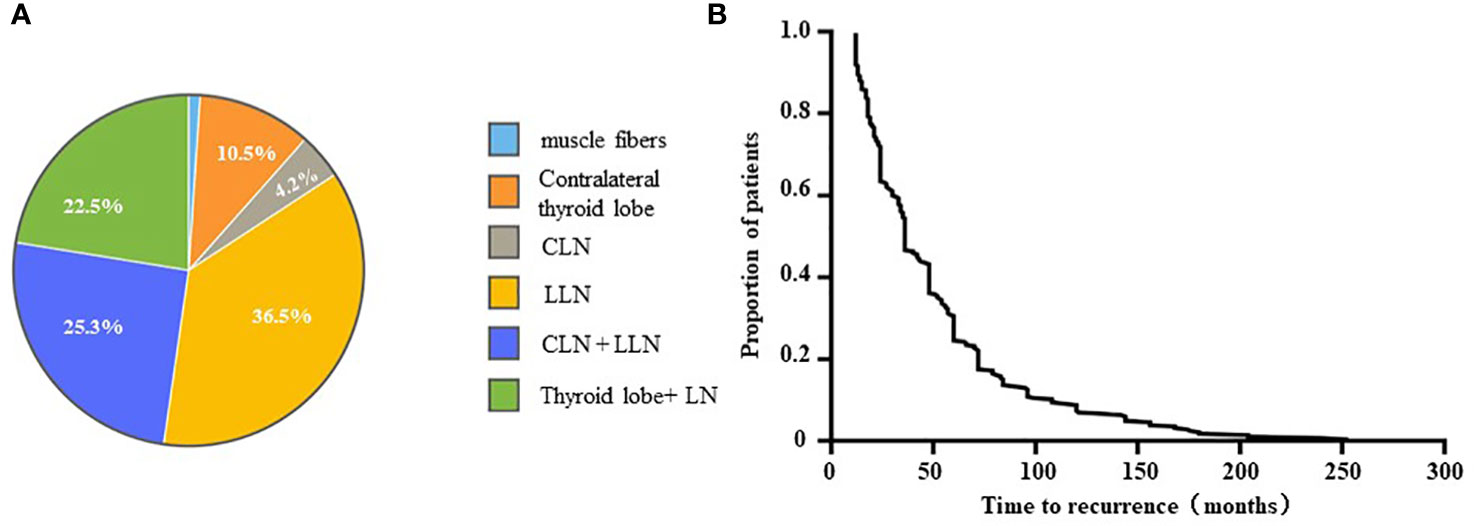
Figure 2 The tumor location of secondary surgery (A) and the recurrence time curve (B).
The reason for the second surgery is an important factor in the selection of second surgical procedures. Table 3 shows that in cases re-treated due to a “l Lack of preoperative FNA or intraoperative pathology in the initial surgery,” total thyroidectomy (n = 102, 54.3%) and near-total thyroidectomy (n = 74, 39.4%) each accounted for half of the second thyroid surgeries. CLND + unilateral LLND was the routine second lymph node dissection procedure (n = 104, 55.3%). In case re-treated due to a “Lack or misdiagnosis of preoperative FNA in the second surgery”, near-total thyroidectomy (n = 12, 63.2%) was the main type of second thyroid surgery. Among cases re-treated due to “less-experienced surgeons” or a “less-experienced paramedical team,” total thyroidectomy was the most common type of second thyroid surgery. However, there were some differences in CLND procedures during second lymph node dissection for two reasons: first, the “less-experienced paramedical team” group mostly performed lateral lymph node dissection; second, among patients with real recurrence, total thyroidectomy (n = 259,91.1%) was the major type of second thyroid surgery. The majority second lymph node dissection types were CLND + unilateral LLND (n = 98, 34.4%) and unilateral LLND (n = 75, 26.3%).
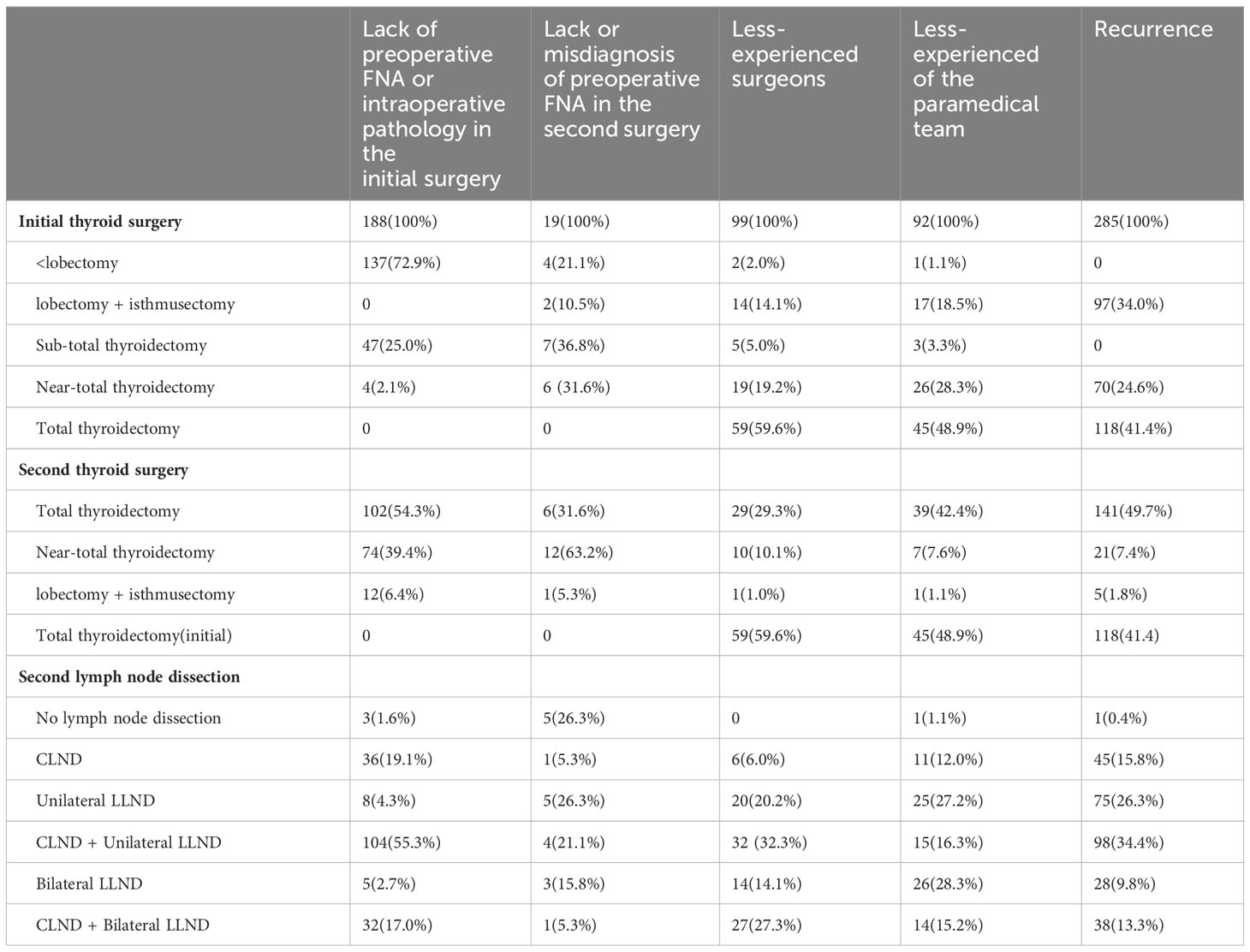
Table 3 Different surgical strategy in “second surgery” reasons of DTC.
The rate of second surgeries for thyroid cancer is increasing year by year, and the recurrence rate of well-DTC has reached 30% (10, 11). Radioactive iodine has been an important adjuvant treatment for persistent/recurrent DTC, but it may not be able to improve the prognosis very well (12, 13). Therefore, it is essential to have a standard second surgery for DTC at hand (14). This study enrolled all patients who experienced second surgeries for DTC at a single center over 13 years to summarize the re-operation reasons, strategies, and development trends among them.
In addition to recurrence, reasons for a second surgery among DTC patients also include persistent diseases and both subjective and objective factors. Bates et al. (15) indicated that about 77.2% of second surgeries may be attributed to persistent disease rather than true disease recurrence. Similarly, we found that, before the release of the Chinese expert consensus in 2012, the proportion of second surgeries performed due to subjective and objective reasons at our center was about 78.7%. However, with the improvement of the guidelines, real recurrence (61.5%) became the most common reason for second surgeries among DTC patients at our center, especially after the release of the 2015 guideline, and the percentage of second surgeries performed for subjective and objective reasons has decreased to 38.5%. This also means that real recurrence has become the main reason for second surgeries at this stage, and the difficulty of the second surgery has also increased. In our true recurrence group, lateral cervical lymph nodes (36.5%) were the main tumor sites during the second surgery, followed by the central + lateral cervical lymph nodes (26.3%) and the thyroid lobe + lymph nodes (22.5%), while contralateral thyroid lobe recurrence accounted for 10% of cases. The results reported by Xu et al. (16) differ slightly from ours. They pointed out that, in 232 patients with persistent/recurrent DTC, 43.1% had lesions in the lymph nodes, 17.7% had lesions in the remnant thyroid or thyroid bed, and 39.2% had lesions in both locations. This difference may be due to a slight variation in the study methods and populations, but both our study and that by Xu et al. each pointed out that the second operation focuses more on lymph node dissection, which increases the difficulty of the operation.
In terms of complications, Medas et al. (17) observed that, in 152 patients with second surgeries for benign or malignant recurrent diseases, the rates of permanent hypoparathyroidism (10%) and transient RLN injury (4.6%) were greater than those following the initial surgery. A 2009 review (18) reported rates of 9.5% and 6.4% for permanent hypoparathyroidism and vocal fold disease, respectively, with both being significantly higher than those following initial thyroidectomy. Michael P et al. (19) reported a 31% rate of inadvertent partial or complete parathyroid resection. Similarly, in our center, patients with hypoparathyroidism and vocal code motion disorders totaled 10.7% and 5.3% of the population after second surgeries, respectively. After 2015, the proportion of patients with postoperative hypoparathyroidism declined to 7.4%. This phenomenon suggests that our surgical technique improved after the 2015 ATA guidelines were published.
In patients with DTC, the decision about the method of secondary surgery is mainly determined by US, computed tomography, and MRI (20, 21). However, the choice of second surgery modality is closely related to the reason for the second surgery (22) and is also typically inseparable from the cause of the initial surgery. Therefore, we need to conduct in-depth analyses of the causes and auxiliary medical examinations of patients and then decide on the parameters of the second surgery (23).
There were several limitations in this study. First, though this was a single center and retrospective study, it was a relative large cohort. In addition, since majority of those patients were taken the initial surgery at some other hospitals. It was difficult to obtain the complete information about initial surgery, such as pathological subtype, tumor invasion, high-volume lymph node metastasis, et al. Finally, there was no further follow up information for after the second surgery.
Significant changes have occurred in the features of DTC patients undergoing second surgeries with updates to the guidelines. The reasons for the second surgery and the procedure of the initial surgery are key factors determining the strategy of the second surgery among DTC patients. With the development of the surgical standard, skill proficiency, and intraoperative nerve monitoring (IONM) technology improvements, the proportion of second surgeries attributed to subjective and objective reasons declined. In the new era, real recurrence became the primary reason for second surgeries for DTC. We look forward to more accurate and unified guidelines for DTC second surgeries.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The institutional ethics committee of the China–Japan Union Hospital of Jilin University approved this study (20220506023). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
NL: Writing – review & editing, Conceptualization, Data curation, Funding acquisition, Methodology, Supervision. HZ: Writing – original draft, Conceptualization, Data curation, Formal Analysis, Methodology. CS: Resources, Writing – review & editing. RD: Resources, Writing – review & editing. CL: Resources, Writing – review & editing. JL: Resources, Writing – review & editing. GD: Writing – review & editing, Methodology, Supervision, Visualization. DZ: Writing – review & editing, Conceptualization, Methodology, Resources, Supervision. HS: Writing – review & editing, Conceptualization, Data curation, Funding acquisition, Project administration, Resources, Supervision, Visualization.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Jilin Province Science and Technology Development Program (20210402011GH, YDZJ202201ZYTS112); and the Program of Jilin Provincial Finance Department (2021SCZ23, 2022SCZ09), the project of China-Japan Union Hospital (2023CL01).
We would like to thank many clinicians from our department for their support. This study was funded by the National Nature Science Foundation of China [81972499]; the Jilin Province Science and Technology Development Program [20210402011GH, YDZJ202201ZYTS112]; and the Program of Jilin Provincial Finance Department [2021SCZ23], the Jilin University Bethune Project [2020B14].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1301620/full#supplementary-material
1. Cabanillas ME, McFadden DG, Durante C. Thyroid cancer. Lancet (2016) 388(10061):2783–95. doi: 10.1016/S0140-6736(16)30172-6
2. Kitahara CM, Sosa JA. The changing incidence of thyroid cancer. Nat Rev Endocrinol (2016) 12(11):646–53. doi: 10.1038/nrendo.2016.110
3. Semrad TJ, Keegan THM, Semrad A, Brunson A, Farwell DG. Predictors of neck reoperation and mortality after initial total thyroidectomy for differentiated thyroid cancer. Thyroid (2018) 28(9):1143–52. doi: 10.1089/thy.2017.0483
4. Patel KN, Yip L, Lubitz CC, Grubbs EG, Miller BS, Shen W, et al. The American Association of Endocrine Surgeons Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults. Ann Surg (2020) 271(3):e21–93. doi: 10.1097/SLA.0000000000003580
5. Lamartina L, Borget I, Mirghani H, Al Ghuzlan A, Berdelou A, Bidault F, et al. surgery for neck recurrence of differentiated thyroid cancer: outcomes and risk factors. J Clin Endocrinol Metab (2017) 102(3):1020–31. doi: 10.1210/jc.2016-3284
6. Zhu J, Wang X, Zhang X, Li P, Hou H. Clinicopathological features of recurrent papillary thyroid cancer. Diagn Pathol (2015) 10:96. doi: 10.1186/s13000-015-0346-5
7. Duren M, Duh QY, Siperstein AE, Clark OH. Recurrent or persistent thyroid cancer of follicular cell origin. Curr Treat Options Oncol (2000) 1(4):339–43. doi: 10.1007/s11864-000-0049-2
8. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid (2016) 26(1):1–133. doi: 10.1089/thy.2015.0020
9. American Thyroid Association Surgery Working G, American Association of Endocrine S, American Academy of O-H, Neck S, American H, Neck S, Carty SE, Cooper DS, et al. Consensus statement on the terminology and classification of central neck dissection for thyroid cancer. Thyroid (2009) 19(11):1153–8. doi: 10.1089/thy.2009.0159
10. Urken ML, Milas M, Randolph GW, Tufano R, Bergman D, Bernet V, et al. Management of recurrent and persistent metastatic lymph nodes in well-differentiated thyroid cancer: a multifactorial decision-making guide for the Thyroid Cancer Care Collaborative. Head Neck (2015) 37(4):605–14. doi: 10.1002/hed.23615
11. Weslley Rosario P, Franco Mourao G, Regina Calsolari M. Role of adjuvant therapy with radioactive iodine in patients with elevated serum thyroglobulin after neck reoperation due to recurrent papillary thyroid cancer: a monoinstitutional comparative study. Endocrine (2020) 68(1):144–50. doi: 10.1007/s12020-019-02165-8
12. Hung ML, Wu JX, Li N, Livhits MJ, Yeh MW. Association of radioactive iodine administration after reoperation with outcomes among patients with recurrent or persistent papillary thyroid cancer. JAMA Surg (2018) 153(12):1098–104. doi: 10.1001/jamasurg.2018.2659
13. Bouvet C, Barres B, Kwiatkowski F, Batisse-Lignier M, Chafai El Alaoui M, Kauffmann P, et al. Re-treatment with adjuvant radioactive iodine does not improve recurrence-free survival of patients with differentiated thyroid cancer. Front Endocrinol (Lausanne) (2019) 10:671. doi: 10.3389/fendo.2019.00671
14. Scharpf J, Tuttle M, Wong R, Ridge D, Smith R, Hartl D, et al. Comprehensive management of recurrent thyroid cancer: An American Head and Neck Society consensus statement: AHNS consensus statement. Head Neck (2016) 38(12):1862–9. doi: 10.1002/hed.24513
15. Bates MF, Lamas MR, Randle RW, Long KL, Pitt SC, Schneider DF, et al. Back so soon? Is early recurrence of papillary thyroid cancer really just persistent disease? Surgery (2018) 163(1):118–23. doi: 10.1016/j.surg.2017.05.028
16. Xu S, Li Q, Wang Z, Huang H, Wang X, Liu S, et al. Evaluating the risk of re-recurrence in patients with persistent/recurrent thyroid carcinoma after initial reoperation. Surgery (2021) 169(4):837–43. doi: 10.1016/j.surg.2020.09.033
17. Medas F, Tuveri M, Canu GL, Erdas E, Calo PG. Complications after reoperative thyroid surgery: retrospective evaluation of 152 consecutive cases. Updates Surg (2019) 71(4):705–10. doi: 10.1007/s13304-019-00647-y
18. Ondik MP, Dezfoli S, Lipinski L, Ruggiero F, Goldenberg D. Secondary central compartment surgery for thyroid cancer. Laryngoscope (2009) 119(10):1947–50. doi: 10.1002/lary.20589
19. Ondik MP, McGinn J, Ruggiero F, Goldenberg D. Unintentional parathyroidectomy and hypoparathyroidism in secondary central compartment surgery for thyroid cancer. Head Neck (2010) 32(4):462–6. doi: 10.1002/hed.21205
20. Liu Z, Xun X, Wang Y, Mei L, He L, Zeng W, et al. MRI and ultrasonography detection of cervical lymph node metastases in differentiated thyroid carcinoma before reoperation. Am J Transl Res (2014) 6(2):147–54.
21. Kim HK, Ha EJ, Han M, Lee J, Soh EY. Reoperations for structurally persistent or recurrent disease after thyroidectomy: analysis via preoperative CT. Sci Rep (2020) 10(1):12376. doi: 10.1038/s41598-020-69398-w
22. Ruggiero FP, Fedok FG. Outcomes in reoperative thyroid cancer. Otolaryngol Clin North Am (2008) 41(6):1261–8. doi: 10.1016/j.otc.2008.06.003
23. Gambardella C, Offi C, Romano RM, De Palma M, Ruggiero R, Candela G, et al. Transcutaneous laryngeal ultrasonography: a reliable, non-invasive and inexpensive preoperative method in the evaluation of vocal cords motility-a prospective multicentric analysis on a large series and a literature review. Updates Surg (2020) 72(3):885–92. doi: 10.1007/s13304-020-00728-3
Keywords: thyroid cancer, recurrence, surgery, morbidity, second surgery
Citation: Liang N, Zhang H, Sui C, Du R, Li C, Li J, Dionigi G, Zhang D and Sun H (2023) Surgical resection of recurrent differentiated thyroid cancer: patterns, detection, staging, and treatment of 683 patients. Front. Endocrinol. 14:1301620. doi: 10.3389/fendo.2023.1301620
Received: 25 September 2023; Accepted: 15 November 2023;
Published: 06 December 2023.
Edited by:
Akira Sugawara, Tohoku University, JapanReviewed by:
Khawla S. Al-Kuraya, King Faisal Specialist Hospital and Research Centre, Saudi ArabiaCopyright © 2023 Liang, Zhang, Sui, Du, Li, Li, Dionigi, Zhang and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hui Sun, c19oQGpsdS5lZHUuY24=; Daqi Zhang, emhhbmdkcUBqbHUuZWR1LmNu
†ORCID: Hui Sun, orcid.org/0000-0001-8348-4933
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.