 Margaret West1
Margaret West1 Risa M. Wolf
Risa M. Wolf
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Endocrinol. , 10 October 2023
Sec. Clinical Diabetes
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1288215
This article is part of the Research Topic Developing Strategies to Improve Diabetes Management in College-Going Young Adults View all 12 articles
The process of transitioning from pediatric to adult diabetes care for adolescents and young adults is challenging. This transition period may include many life changes, and can be fraught with worsening glycemic control leading to increased risk for diabetes-related hospitalizations and complications. Research has demonstrated that increased support during this period can help maintain engagement in diabetes care. Transition guidelines highlight the importance of preparation and readiness for transition. In this article, we discuss the development, implementation and content of a workshop for patients and parents/caregivers preparing for the transition to college, the workforce and adult diabetes care.
The process of transitioning from pediatric to adult health care for adolescents and young adults with chronic conditions is challenging. This period is a time of major changes in school, work and living environment. Young adults with type 1 diabetes face even greater challenges during this transition period with the additional stress of managing their disease and maintaining glycemic control. Almost 50% of young adults report difficulties in transitioning from pediatric to adult diabetes care, and almost 30% disengage from medical care during this period (1–3). Attendance at follow-up appointments declines and there is often an associated rise in hemoglobin A1c levels (4, 5). In general, hemoglobin A1c levels during this age group are at their peak, and thus there is increased risk for hospitalization and diabetes-related complications (5, 6).
Studies have identified the need for more support during the transition period for young adults with type 1 diabetes (7). Trials implementing care navigators and intensive transition coordinator support have shown promising results in facilitating engagement and clinic attendance in this age group (8, 9). The American Diabetes Association (ADA) and others have developed transition guidelines to help guide providers during this period (10–12). The importance of transition preparation through education and counseling promotes transition readiness for both patients and their caregivers (11).
In 2018, we developed a workshop for young adults and their parents/caregivers to help prepare them for transitioning into the workforce, moving out of their parents’ home, or going to college. We hosted this event in collaboration with key stakeholders including the JDRF and The DiabetesLink (formerly College Diabetes Network (CDN)). (Appendix A: Event flyer). Workshop invitations were directed to high school juniors and seniors, as well as young adults who recently graduated from high school or were entering the workforce, with both type 1 and type 2 diabetes. At our institution, patients are usually transitioned to adult diabetes care one-year after high school, but can remain in the pediatric practice at the discretion of the provider based upon transition readiness.
The workshop was structured as a 2-hour event where the first hour included a series of brief presentations hosted by faculty, followed by a panel discussion featuring students who already transitioned to college or the workforce, and some with their parents/caregivers as dyads. (Appendix B: Agenda) The platform for this event was initially an in-person workshop, but due to the COVID-19 pandemic beginning in 2020, the workshop was switched to a virtual (zoom) platform. Both formats have been successful and engaging, but an in-person workshop allows for either small group discussions (one for the students and one for the parents), or panel discussions; whereas on the zoom platform a panel discussion has been easier to facilitate. In order to engage participants in the workshop, the hosts prepared a list of questions to get the panel started, and then the attendants were requested to submit questions to the host, which were then asked of the panel discussants. At the completion of the workshop, attendees were able to provide feedback through a brief survey of what was most helpful and what could be improved in the program.
The first year that we hosted this event in 2018, the event was held on a Sunday in May, but feedback from parents was that it felt too close to the time the students were leaving for college or moving out of the house and felt that more preparation time would have been helpful. Based on this feedback, in subsequent years, this event has been held on a Sunday in March.
This presentation is given by an adult endocrinologist. During this portion of the presentation, we emphasize to patients and their parents that the overall goals of care are similar between adult and pediatric providers, namely, to help the patient achieve the best control of blood glucose that is possible for them, and to ensure good health now and in the future. The adult provider’s perspective includes more focus on control of cardiovascular risk factors and management of microvascular complications. However, unlike tertiary care pediatric centers, many adult providers do not have onsite nutritionists, psychologists and diabetes educators so often separate appointments for these providers have to be made. To ensure good continuity of care, the participants are reminded that they should identify potential adult providers 6-9 months ahead of time since adult clinics often have long waits for new patient appointments and that a good time for such an appointment could be soon after graduation from high school, or later depending on the planned transition time. At the first appointment with their new provider it’s important to identify key clinical and administrative staff in the office, as well as procedures for obtaining refills. If the patient is going away for college, we discuss that some individuals choose to have a second provider at their college, while maintaining a provider in their hometown. Regardless of diabetes provider location, we recommend setting up an appointment with the college student health center for the student to be aware of local resources for diabetes care and management.
This presentation discusses the process of registering at their school’s Disability Services office prior to the start of classes to facilitate reasonable accommodations for diabetes management in the classroom and on campus. While some students are hesitant to self-identify as having a disability, and are comfortable with informal accommodations provided in high school, they are encouraged to register with Disability Services prior to an issue arising to ensure equal opportunity to succeed in college. Students are encouraged to share a list of proposed accommodations and rationales with their medical team for submission. In this presentation, we review commonly requested accommodations such as ability to pause exams in case of hypoglycemia or hyperglycemia, continuous access to diabetes technology including cell phones for continuous glucose monitoring, and permission to keep a minifridge in the dorm room for insulin storage. As an example, the speaker will demonstrate how to navigate a local college website to identify the Disability services office and find the appropriate forms and contact information.
This presentation encourages students to maintain frequent communication with their primary pediatric or adult diabetes team while in college, and have their team’s contact information readily accessible for urgent or after-hours needs. We also suggest students identify the nearest emergency room in case of an emergency, and also determine the capabilities and limitations of the student health office if unable to reach their primary endocrinology team.
Students and parents should also develop a plan for obtaining prescriptions and supplies, and whether these will be picked up locally or shipped from their parents’ home. Prescription plan logistics will depend on the student’s insurance as well as proximity to home. We highlight the importance of developing a system for the student to identify when to begin the reordering process to avoid running out of medications or supplies. Families are encouraged to transition the responsibility for medication and supply management to the student during senior year of high school so that parents can provide oversight and guidance before the student moves away from home. This is especially important given the frequent confusion on whether supplies are coming from a pharmacy or DME company, and who to contact for refills. Patients are also encouraged to identify a local pharmacy near the college in case of an urgent medication need.
This presentation is given by a dietitian (RD), who discusses navigating the dining hall in college and adjusting to a variable eating schedule typical in college or in the workforce. Nutrition choices and food intake often change when young adults leave home and live at college. Dining halls and cafeterias can be challenging to navigate for both food choices and carbohydrate counting. During this presentation, the RD discusses strategies on carbohydrate counting in dining halls and college food establishments. Some colleges have nutrition information on their dining websites, or have phone apps available so that students can see menus and associated nutrition information. The speaker demonstrates how to navigate a school nutrition website for a local college as an example, and how to contact the campus dietitian for additional information. An email/letter template is shared for contacting the school dietitian with request for carbohydrate information and possibly food additions or modifications to the cafeteria menu (e.g. sugar-free pancake syrup, high protein yogurt).
College dining halls often have many food options for main courses, sides, and desserts. The RD discusses how to make healthy food choices for balanced meals, in order to avoid large glycemic excursions, promote overall heart healthy food intake and healthy weight management. Estimating portions is also reviewed as the college student is unlikely to use measuring cups in the dining hall. Sample serving sizes are visualized with images and objects for different food types to help students estimate carbohydrate content.
The speaker also discusses managing meals with a variable schedule of classes and activities in college, and managing late-night eating. The dietitian reviews tips such as planning meals and snacks, which may include packing food to go, or learning about different dining halls on campus and their hours of operation. The RD provides suggestions for complex carbohydrates and protein sources to keep in their dorm room, which can be eaten as a quick meal or on-the-go.
In the last part of the nutrition presentation, the dietitian discusses the benefits of physical activity and ways to stay physically active on campus while also managing blood glucose with exercise. The speaker reviews exercise management with multiple daily injection verses insulin pumps (including hybrid closed loop systems). The discussion includes utilizing exercise functions on pumps, modifying insulin doses at meals prior to exercise, and food choices to help maintain blood glucose levels during activity. The RD provides guidance on complex carbohydrate and protein consumption to help optimize athletic performance, with examples such as peanut butter sandwich on whole wheat bread, or protein granola bar. The speaker also discusses differing carbohydrate needs for blood glucose maintenance and treatment of hypoglycemia depending on type of insulin delivery (injections, pumps, and hybrid-closed loop systems).
This presentation reviews hyperglycemia, sick day management and hypoglycemia management. This includes a review of when to check for ketones, managing hyperglycemia when sick, and the signs and symptoms of DKA. A list of scenarios of when to seek help are reviewed. Hypoglycemia management is also reviewed. Importantly, if students have roommates, we remind them to demonstrate to the roommate where the glucagon is stored and how to give glucagon in an emergency. The list of contents for an “emergency diabetes kit” are outlined. In this discussion, wearing a medical alert bracelet is reinforced, as well as setting up a Medical ID on the phone for emergency responders to access if needed.
This presentation reviews responsible behavior, and effects of alcohol and other substances on diabetes. While consumption of alcohol is not condoned, it is a likely exposure after high school or in college, and thus it is important to discuss the effects of alcohol on diabetes. This presentation reviews that alcohol is predominantly metabolized by the liver, and with alcohol consumption, the liver’s ability to perform gluconeogenesis and glycogenolysis is reduced and can lead to hypoglycemia. Thus, it is recommended to drink alcohol responsibly and limit to 1-2 drinks, always eat carbohydrates while drinking alcohol, and monitor blood sugars closely for potential delayed hypoglycemia (13).
In some states, recreational cannabis is legal for young adults 18 years of age and over. Recreational cannabis use can result in acute adverse events with increased risk for DKA and higher hemoglobin A1c. In this presentation, we review the effects of marijuana, and the increased food consumption typically associated with cannabis use that can lead to hyperglycemia.
This presentation is usually given by a psychologist at our center, but can be given by anyone on the diabetes team. Upon arrival to college, students should share their diabetes diagnosis with their roommate, resident assistant, and other important adults such as coaches. For those joining the workforce, it is important to inform co-workers and bosses. While these individuals are not expected to participate in the student’s diabetes management, they should know how to identify an emergency and respond when the student with diabetes needs assistance. In this presentation, the students are encouraged to practice having these conversations, as these initial conversations can be a source of anxiety. As an example, the speaker may role-play how to open this conversation with a new roommate, or start a conversation about diabetes with their athletic coach. Further, advice on seeking mental health resources and peer support on campus is discussed.
Parents and students are also encouraged to discuss expectations regarding communication, and set up a schedule for touching base about diabetes management successes or issues. With the advent of continuous glucose monitoring, families must establish boundaries around outreach to their college students regarding blood glucose management. Some families identify blood sugar thresholds above or below which parents will contact the student and/or other individuals such as roommate or resident assistants, while some families opt not to use glucose sharing technology. Students are also encouraged to utilize other resources and apps that connect to their continuous glucose monitors and notify them of an untreated low. The speaker also reminds parents to avoid focusing every conversation around diabetes when speaking with their children at college.
The series of presentations (Table 1) concludes with an overview of resources available from diabetes organizations, including JDRF and DiabetesLink (formerly College Diabetes Network, CDN). These resources are shared with the participants by email after the event.
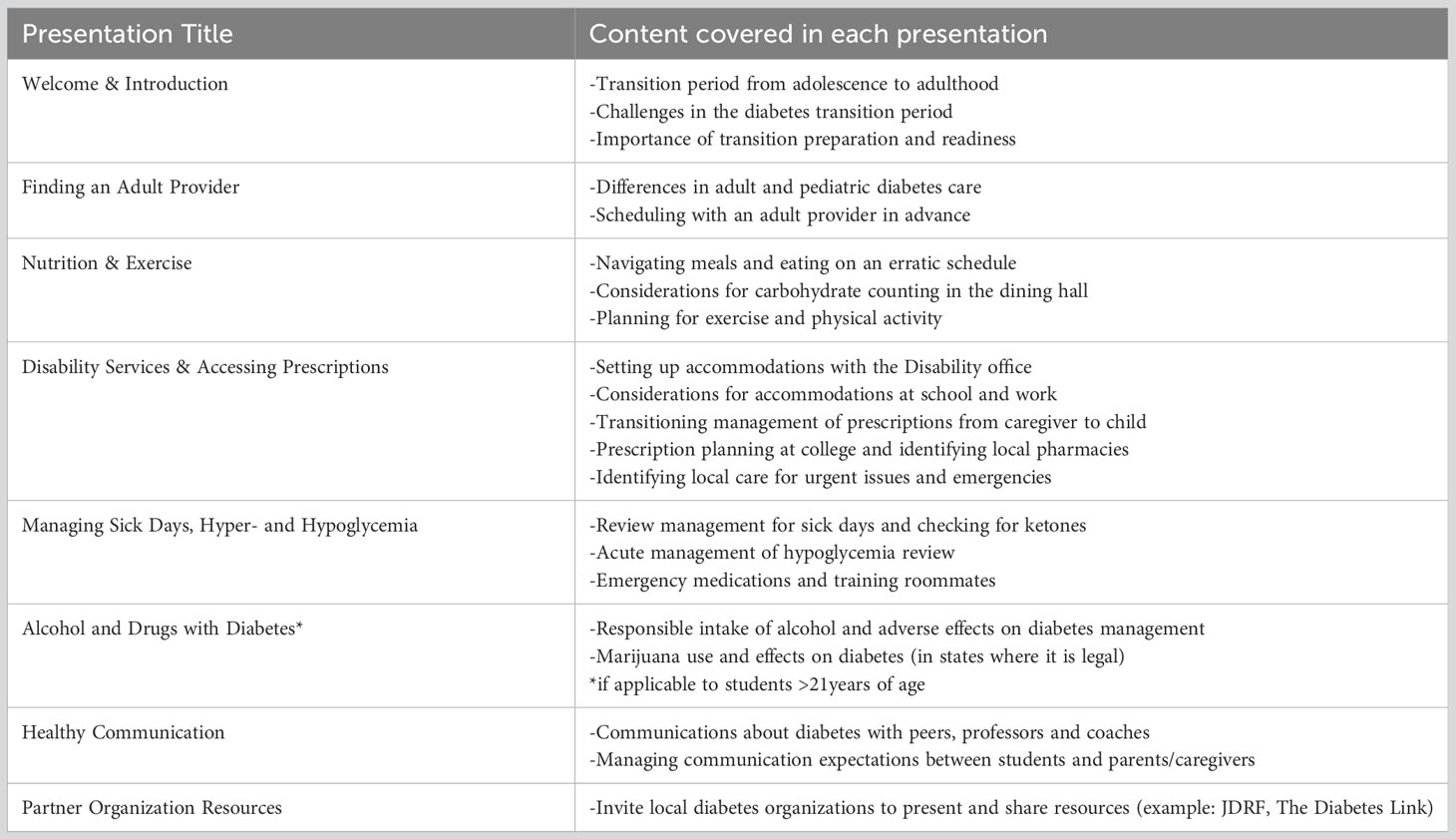
Table 1 Diabetes transition and off to college workshop content.
Transition preparation and readiness are important to ensure a smooth transition process from pediatric to adult diabetes care that occurs during a time of many life-transitions. Readiness should apply to both adolescents and young adults, as well as their parents and caregivers (9). The implementation of a workshop to prepare and ready patients and caregivers for the upcoming transition to college or into the workforce, and leaving the home has been a successful addition to our transition program for all young adults with diabetes. Feedback from patients and caregivers has reflected important knowledge acquisition, and insight on how to set-up accommodations at college or work, eating on a variable schedule, and ideal communication patterns among all stakeholders. We hope this article provides a framework for other diabetes programs to establish and host a similar program for their young adults and patients transitioning to college or the work-force.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
RW: Conceptualization, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. MW: Conceptualization, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing. AS: Conceptualization, Project administration, Resources, Writing – original draft, Writing – review & editing. MT: Conceptualization, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1288215/full#supplementary-material
1. Insabella G, Grey M, Knafl G, Tamborlane W. The transition to young adulthood in youth with type 1 diabetes on intensive treatment. Pediatr Diabetes (2007) 8:228–34. doi: 10.1111/j.1399-5448.2007.00266.x
2. Sparud-Lundin C, Ohrn I, Danielson E, Forsander G. Glycaemic control and diabetes care utilization in young adults with Type 1 diabetes. Diabetes Med (2008) 25:968–73. doi: 10.1111/j.1464-5491.2008.02521.x
3. Kipps S, Bahu T, Ong K, Ackland FM, Brown RS, Fox CT, et al. Current methods of transfer of young people with Type 1 diabetes to adult services. Diabetes Med (2002) 19:649–54. doi: 10.1046/j.1464-5491.2002.00757.x
4. Cadario F, Prodam F, Bellone S, Trada M, Binotti M, Trada M, et al. Transition process of patients with type 1 diabetes (T1DM) from paediatric to the adult health care service: a hospital-based approach. Clin Endocrinol (Oxf) (2009) 71:346–50. doi: 10.1111/j.1365-2265.2008.03467.x
5. Foster NC, Beck RW, Miller KM, Clements MA, Rickels MR, DiMeglio LA, et al. State of type 1 diabetes management and outcomes from the T1D exchange in 2016-2018. Diabetes Technol Ther (2019) 21:66–72. doi: 10.1089/dia.2018.0384
6. Bryden KS, Dunger DB, Mayou RA, Peveler RC, Neil HA. Poor prognosis of young adults with type 1 diabetes: a longitudinal study. Diabetes Care (2003) 26:1052–7. doi: 10.2337/diacare.26.4.1052
7. Hynes L, Byrne M, Dinneen SF, McGuire BE, O'Donnell M, Mc Sharry J., et al. Barriers and facilitators associated with attendance at hospital diabetes clinics among young adults (15-30 years) with type 1 diabetes mellitus: a systematic review. Pediatr Diabetes (2016) 17:509–18. doi: 10.1111/pedi.12198
8. Spaic T, Robinson T, Goldbloom E, Gallego P, Hramiak I, Lawson ML, et al. Closing the gap: results of the multicenter canadian randomized controlled trial of structured transition in young adults with type 1 diabetes. Diabetes Care (2019) 42:1018–26. doi: 10.2337/dc18-2187
9. White M, O'Connell MA, Cameron FJ. Clinic attendance and disengagement of young adults with type 1 diabetes after transition of care from paediatric to adult services (TrACeD): a randomised, open-label, controlled trial. Lancet Child Adolesc Health (2017) 1:274–83. doi: 10.1016/S2352-4642(17)30089-5
10. Association AD. Standards of medical care in diabetes—2019 abridged for primary care providers. Clin Diabetes (2019) 37:11–34. doi: 10.2337/cd18-0105
11. Lindholm Olinder A, DeAbreu M, Greene S, Haugstvedt A, Lange K, Majaliwa ES, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Diabetes education in children and adolescents. Pediatr Diabetes (2022) 23:1229–42. doi: 10.1111/pedi.13418
12. Peters A, Laffel L, American Diabetes Association Transitions Working, Diabetes care for emerging adults: recommendations for transition from pediatric to adult diabetes care systems: a position statement of the American Diabetes Association, with representation by the American College of Osteopathic Family Physicians, the American Academy of Pediatrics, the American Association of Clinical Endocrinologists, the American Osteopathic Association, the Centers for Disease Control and Prevention, Children with Diabetes, The Endocrine Society, the International Society for Pediatric and Adolescent Diabetes, Juvenile Diabetes Research Foundation International, the National Diabetes Education Program, and the Pediatric Endocrine Society (formerly Lawson Wilkins Pediatric Endocrine Society). Diabetes Care (2011) 34:2477–85. doi: 10.2337/dc11-1723
Keywords: type 1 diabetes, continuous glucose monitors, prescriptions, transition, young adult
Citation: West M, Sidhaye A, Thivierge M and Wolf RM (2023) Development and implementation of a workshop for young adults with diabetes entering college and the workforce. Front. Endocrinol. 14:1288215. doi: 10.3389/fendo.2023.1288215
Received: 04 September 2023; Accepted: 14 September 2023;
Published: 10 October 2023.
Edited by:
Mridusmita Saikia, Cornell University, United StatesReviewed by:
Jeniece Ilkowitz, New York University, United StatesCopyright © 2023 West, Sidhaye, Thivierge and Wolf. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Risa M. Wolf, UldvbGZAamh1LmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.