 Ana Lúcia Danielewicz1,2†
Ana Lúcia Danielewicz1,2† Stefano Lazzer3,4*†
Stefano Lazzer3,4*† Alice Marra1†Laura Abbruzzese5†
Alice Marra1†Laura Abbruzzese5† Mattia D’Alleva3,4†Maria De Martino3†
Mattia D’Alleva3,4†Maria De Martino3† Miriam Isola3†
Miriam Isola3† Núbia Carelli Pereira Avelar2†Vanessa Amaral Mendonça6†
Núbia Carelli Pereira Avelar2†Vanessa Amaral Mendonça6† Ana Cristina Rodrigues Lacerda6†
Ana Cristina Rodrigues Lacerda6† Alessandro Sartorio1††
Alessandro Sartorio1††- 1Istituto Auxologico Italiano, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Experimental Laboratory for Auxo-endocrinological Research, Piancavallo-Verbania, Italy
- 2Department of Health Sciences, Graduate Program in Rehabilitation Sciences, Federal University of Santa Catarina, Araranguá, Santa Catarina, Brazil
- 3Department of Medicine, University of Udine, Udine, Italy
- 4School of Sport Science, University of Udine, Udine, Italy
- 5Istituto Auxologico Italiano, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Division of Eating and Nutrition Disorders, Piancavallo-Verbania, Italy
- 6Department of Physiotherapy, Federal University of the Jequitinhonha and Mucuri Valleys, Diamantina, Minas Gerais, Brazil
Background: In the last decade a large number of studies proposed and/or validated equations to estimate the Resting Energy Expenditure (REE) in adults and/or older adults, however, no equation currently available showed good accuracy for older adults with severe obesity. Thus, this study aimed to develop and validate new predictive equations for REE, based on data from the indirect calorimetry, in Italian older adults with severe obesity.
Methods: A retrospective study was as conducted with 764 Caucasian older adults with severe obesity (age range: 60-74 years and BMI ≥ 35 kg/m/²). Four models were used to test the accuracy of anthropometry and body composition variables in multivariable prediction of REE. All models were derived by stepwise multiple regression analysis using a calibration group of 382 subjects [295 females and 87 males] and the equations were cross-validated in the remaining 382 subjects [295 females and 87 males] as validation group. The new prediction equations and the other published equations were tested using the Bland-Altman method. Prediction accuracy was defined as the percentage of subjects whose REE was predicted within ± 10% of measured REE.
Results: All the equations analyzed predicted higher energy requirements for males than females, and most of them underestimated the energy requirement values of our sample. The highest accuracy values were observed in the new equations, with 62% in the anthropometric model and 63% in the body composition model.
Conclusion: Although the accuracy of our equations was slightly higher in comparison with the other taken into consideration, they cannot be considered completely satisfactory for predicting REE in Italians older adults with severe obesity. When predicting equations cannot guarantee precise or acceptable values of REE, the use of indirect calorimetry (if available) should be always recommended, especially in clinical practice.
1 Introduction
The aging population is increasing worldwide and, in parallel, it is also observed an increase in the prevalence of older people with obesity (1), which is caused by a chronic energy imbalance wherein energy intake regularly exceeds energy expenditure (2).
An important factor to be considered in older adults with obesity is the pronounced body composition changes, with greater deposition of fat mass in visceral organs, at the expense of the amount of fat-free mass, particularly muscle mass (3). These age-related changes are due to the interplay between aging, inflammation, bad eating habits, metabolic disorders, and oxidative stress (4).
It is well established that both aging and obesity, contribute to altering the Resting Energy Expenditure (REE), which represents in most individuals around 50-70% of the total daily energy expenditure (5), which also includes energy consumed during food thermogenesis and physical activity. REE is considered an important parameter to provide a proper caloric intake essential to maintain the ideal energy balance and/or to determine weight loss in subjects with obesity (6).
The most common method of measuring REE in clinical is Indirect Calorimetry (IC) (7) which measures oxygen and carbon dioxide concentrations in the expired air, and then calculates the energy expenditure with equations based on the concentration values of these gases (8). Although the IC is a non-invasive and reliable method, its application is limited because it requires specialized equipment and trained personnel, which can be costly in daily clinical practice (9).
Thus, several predictive equations developed to calculate the REE have already been created in the last 10 years, and a large number of studies proposed new equations and/or validated the existing ones. However, they included data analysis considering adults with obesity without age differentiation (10–13), normal weight and/or older adults (10, 14–16). Other equations were proposed considering groups of people classified by gender (17–19), ethnicity (20, 21), hospitalization (22) and the presence of chronic diseases (23). Despite being widely referenced, these equations were designed for the general population, without considering existing divergences related to age groups and other epidemiological and body composition variables.
In a recent systematic review, Cioffi et al. (24) evaluated the prediction accuracy of REE in healthy older adults according to the group level, and after analyzing 14 included studies, they concluded that, to date, no equation could be recommended because of the criteria limitation. To the best of our knowledge, to date, two equations for older adults with obesity have been validated. The study performed by Noreik et al. (5) found the best accuracy for estimating REE in the equation proposed by Lührmann et al. (3) (0.876, p = 0.0001), which however was elaborated only with body weight and did not take into account body composition variables. In another recent validation study performed by Griffith et al. (6), the best accuracy (59%) for older adults with obesity was observed in the equation proposed by FAO/WHO/ONU (1985), which however was not considered completely satisfactory.
Given the above findings, it remains important to investigate new accurate predictive equations to determine the REE in older adults with obesity, considering their differences according to subgroups (age, gender, ethnicity, and body composition), since these results could help to improve the health strategies in this population at-risk. Thus, this study aimed to develop and validate new predictive equations for REE, based on data from indirect calorimetry, in Italian older adults with severe obesity.
2 Subjects and methods
2.1 Study sample and design
A retrospective study was performed on 764 Caucasian older adults with severe obesity (590 females and 174 males) hospitalized between January 2016 and January 2019 at the Division of Metabolic Diseases, Italian Institute for Auxology, IRCCS, Piancavallo (VB), Italy, for a 3-week multidisciplinary integrated body weight reduction program (BWRP). Briefly, the BWRP entailed an energy-restricted diet in combination with physical rehabilitation (moderate aerobic activity), psychological counseling, and nutritional education (25).
The inclusion criteria were: 1) age between 65 and 74 years; and 2) Body Mass Index (BMI) calculated as weight (kg)/height² (m) ≥ 35 kg/m2, according to the cut-off for obesity in older people recommended by the Pan American Health Organization (2001). Individuals who had overt metabolic and/or endocrine diseases (i.e. diabetes, hypothyroidism, hypertension, amenorrhea), acute or chronic kidney/liver diseases, acute or chronic infection or inflammatory conditions, autoimmune diseases, malignant diseases, neurodegenerative diseases, hematological and/or oncological disorders, and those taking medications regularly or using any drugs known to influence energy metabolism were excluded. For each participant, anthropometric and instrumental measurements, such as the evaluation of body composition by bioimpedance analysis (see below for details), were collected.
This study was approved by the Ethical Committee of Istituto Auxologico Italiano, IRCCS, Milan Italy (code: 2023_03_21_06; research code: 01C311, acronym: EQUASTIMET60). Written informed consent was signed by all participants at the admission to the Hospital.
2.2 Anthropometric measurements and body composition
All the anthropometric measurements, REE, and body composition analysis were taken before the beginning of the BWRP by the same trained operators, according to the Anthropometric Standardization Manual (26).
The body weight (BW) was measured to the nearest 0.1 kg using an electronic scale (Ro WU 150, Wunder Sa.bi., Trezzo sull’Adda, Italy). Standardizing height was determined by a Harpenden Stadiometer (Holtain Limited, Crymych, Dyfed, UK).
Body composition was measured by using a multifrequency tetrapolar impedancemeter (BIA, Human-IM Scan, DS-Medigroup, Milan, Italy) with a delivered current of 800 A at a frequency of 50 kHz. To reduce errors of measurement, attention was paid to the standardization of the variables that affect measurement validity, reproducibility, and precision. Measurements were performed according to the method of Lukaski et al. (27) after 20 minutes of rest in a supine position with relaxed arms and legs without any contact with other body parts. Fat-free mass (FFM) was estimated using the prediction equation for adults developed by Bedogni et al. (28). Fat Mass (FM) was obtained by subtracting FFM from body weight (BW) and % FM as (FM/BW) × 100.
2.3 Resting energy expenditure
REE was determined in a 22 to 25°C room in the morning (between 08:00 and 10:00 a.m.) and after an overnight fast using an open-circuit, indirect computerized calorimetry with a rigid, transparent, ventilated canopy (Vmax 29, Sensor Medics, Yorba Linda, CA), periodically undergone to quality control tests to ensure the reliability of the measurements. Before each test, the gas analyzers were calibrated using a reference gas mixture (15.00% O2 and 5.00% CO2). The subjects were fasting from at least 8 hours, were not smoking for at least 1 hour, and waited 30 minutes in a sitting position before undergoing REE measurement. After achieving a steady state in the lying position, the REE of individuals was measured for 30 minutes. The data relative to the acclimation period were discarded. The steady state was defined as at least 5 minutes< 5% variation in the respiratory quotient,< 10% variation in O2, and< 10% variation in minute ventilation (29). Oxygen consumption and carbon dioxide production, standardized for temperature, barometric pressure and, humidity, were recorded at 1-min intervals for a minimum of 30 min and averaged over the whole measurement period. Energy expenditure was derived from the measured oxygen uptake and carbon dioxide output according to the equation of Weir (30).
2.4 Statistical analysis
Values of continuous variables are given as mean and standard deviation or median and interquartile range (IQR), according to the data distribution. The data were analyzed using the Kolmogorov–Smirnov test to verify the normal distribution. Student’s t-test or Mann–Whitney U test was used to compare continuous variables between groups, as appropriate. For the development and cross-validation of new equations for predicting REE, the data set of 764 measured REE values was randomly split into two groups: a calibration group (n: 382, 295 females and 87 males) for the development of predictive equations, and a cross-validation group (n: 382, 295 females and 87 males) for the validation of the predictive equations. In the calibration group, the univariable relationships between REE and continuous predictors (age, body weight, height, FFM, and FM) were first studied using scatterplots and non-parametric regression plots. A first-degree linear model was as accurate as more complex models to describe all the REE-predictor relationships and was thus chosen as the reference model for all univariable analyses. Four pre-specified models were used to test the accuracy of anthropometry and body composition in multivariable prediction of REE. Model 1 was based on body weight, age, and gender; Model 2 added height to the predictors of Model 1; Model 3 was based on age, gender and FFM; Model 4 added FM to the predictors of Model 3. Standard diagnostic plots were used to test univariable and multivariable model fit. The adjusted coefficient of determination (R2adj) and the root mean squared error of the estimate (RMSE) were used as measures of model fit.
The new prediction equations and the other published equations were tested in the cross-validation group by using the Bland-Altman method (31) to ascertain the degrees of systematic and magnitude of bias when predicted REE was compared with measured REE. In addition, prediction accuracy was defined as the percentage of subjects whose REE was predicted to be within ±10% of measured REE. This error limit on prediction accuracy was accepted empirically as being consistent with calorimetry measurement errors of 5% or less (32). Differences between predicted REE and measured REE higher than ±10% were considered prediction errors and are reported as percentages of subjects whose REE was overestimated or underestimated.
Statistical analysis was performed using STATA 18.0 (STATA Corp, College Station, TX, USA).
3 Results
The main characteristics of 764 older adults with severe obesity (590 females and 174 males) are shown in Table 1. Female and male subjects with obesity had a comparable age between 65 and 74 years and showed a mean BMI of 40.3 kg/m2 [37.4 - 44.8] for females and 38.5 kg/m2 [35.5 - 41.5] for males (p-value< 0.001). Male subjects with obesity were significantly taller (+8.9%, p-value< 0.001) and had the highest FFM values compared to females (+39.5%, p-value< 0.001), while female subjects with obesity showed a higher amount of FM (+19.7%, p-value< 0.001). The REE obtained with indirect computerized calorimetry was significantly higher in males (+20.8%, p-value< 0.001) compared to female patients, but REE normalized for FFM was significantly lower in males than females (-13.7%, p-value< 0.001).
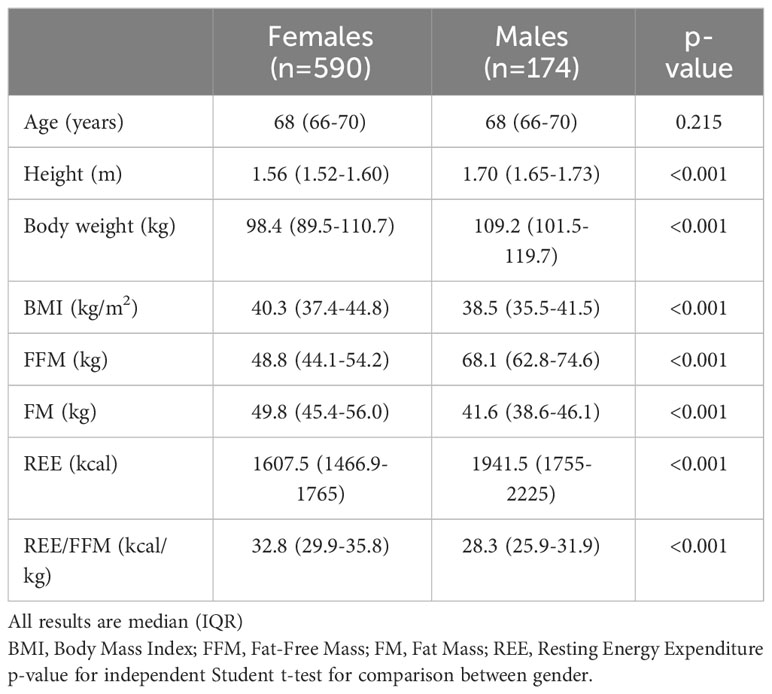
Table 1 Physical characteristics of the sample (n:764).
The association between the obtained REE and the physical variables was analyzed through univariate regression analysis (Table 2). A significant association was observed between the REE and all the tested variables: male gender, age, height, BW, BMI, FFM and FM.
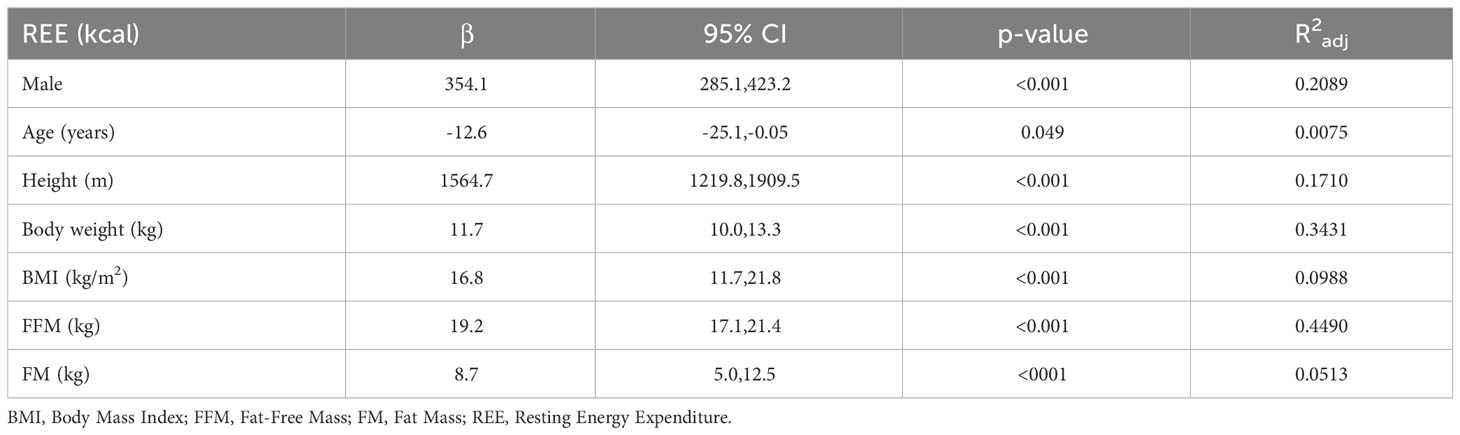
Table 2 Univariable regression analysis between anthropometric and body composition variables and Resting Energy Expenditure (REE) in the calibration group (n: 382, 295 females and 87 males).
Table 3 shows that all models of multivariable regression analysis had similar accuracy for predicting REE in the analyzed sample (R2adj ~ 0.46; p< 0.001). The insertion of the height variable (Model 2) did not significantly modify the model of simple anthropometric measurements based on BW, age and gender (Model 1). Similarly, the insertion of the FM variable (Model 4) did not substantially change the fit value of the model for body composition based on age, gender and FFM (Model 3).
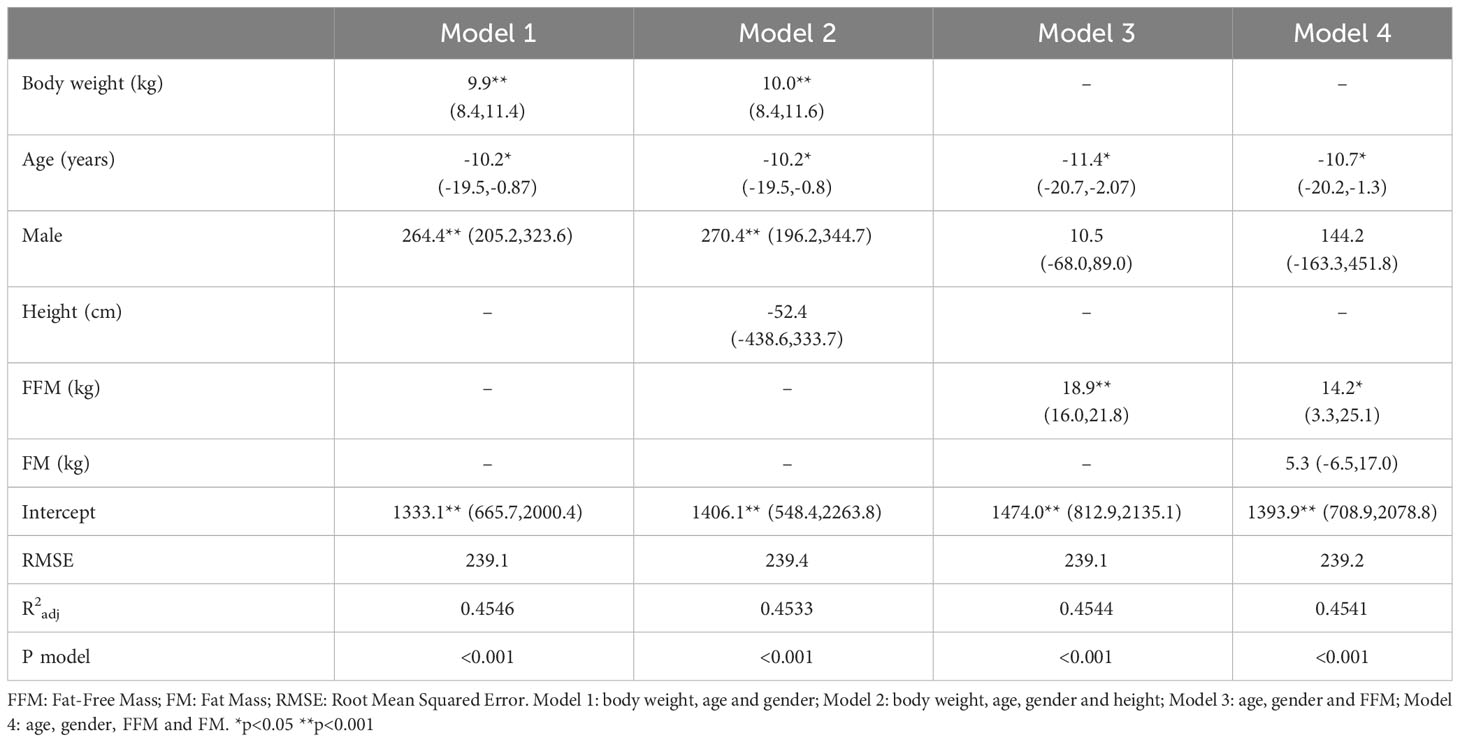
Table 3 Multivariable regression analysis between anthropometric and body composition variables and Resting Energy Expenditure (REE) in the calibration group (n: 382, 295 females and 87 males).
Therefore, the new equations for the prediction of REE in older adults with severe obesity are the following:
where gender = 1 for males and 0 for females, age in years, BW and FFM in kg.
All equations, with both anthropometric and body composition measurements, predicted higher energy requirements for males than females (p<0.001) (Table 4).
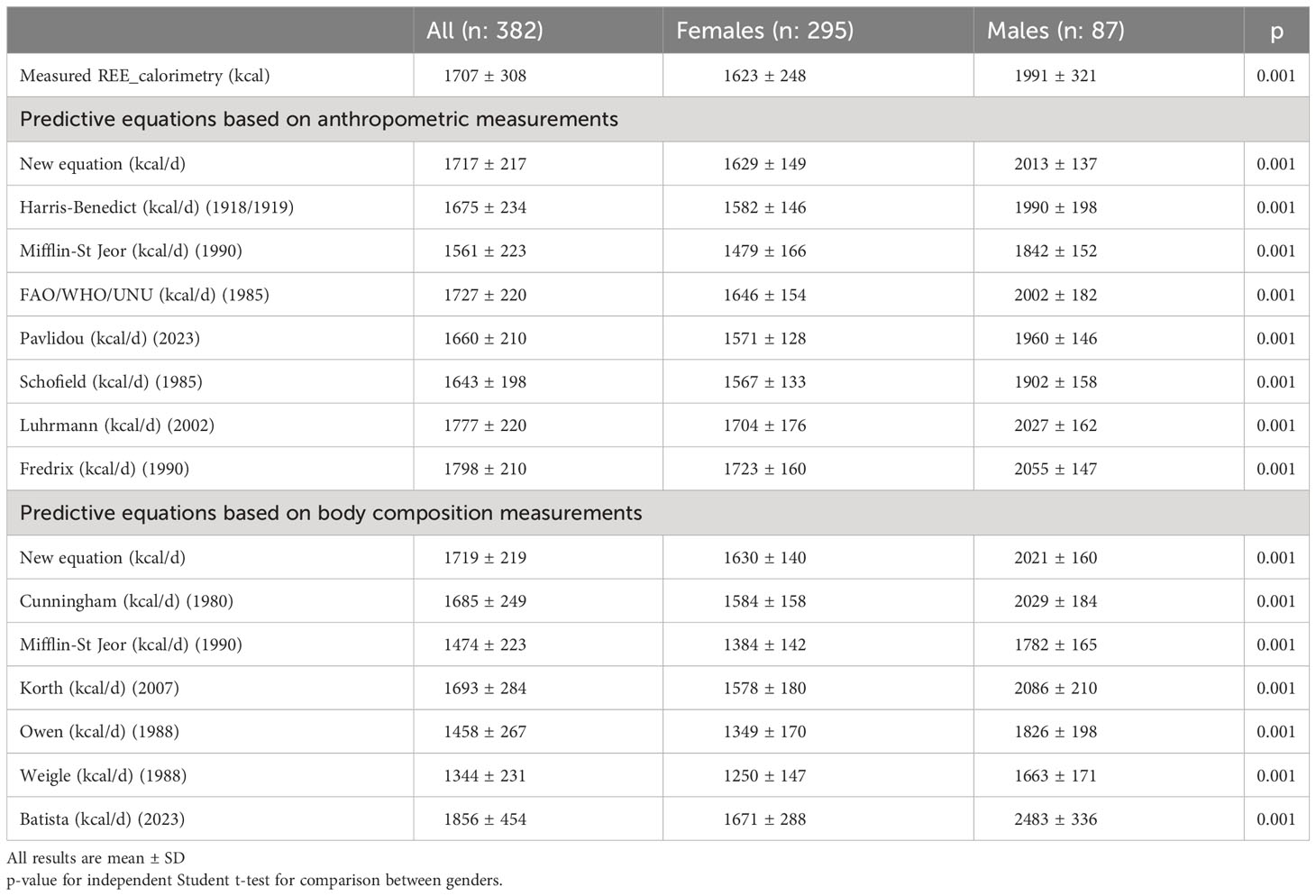
Table 4 Resting Energy Expenditure (REE) measured by calorimetry and estimated by predictive equations in the validation group (n: 382).
Comparing the REE estimated by indirect calorimetry and the prediction equations analyzed based on anthropometric measurements, it was found that only the new equation proposed and the equation proposed by FAO/WHO/UNU (33) did not show a significant difference (Table 5). All other equations were significantly different, with most of them underestimating the energy requirement. Significant overestimations were observed in the equations proposed by Luhrmann et al. (3) and Fredrix et al. (37).
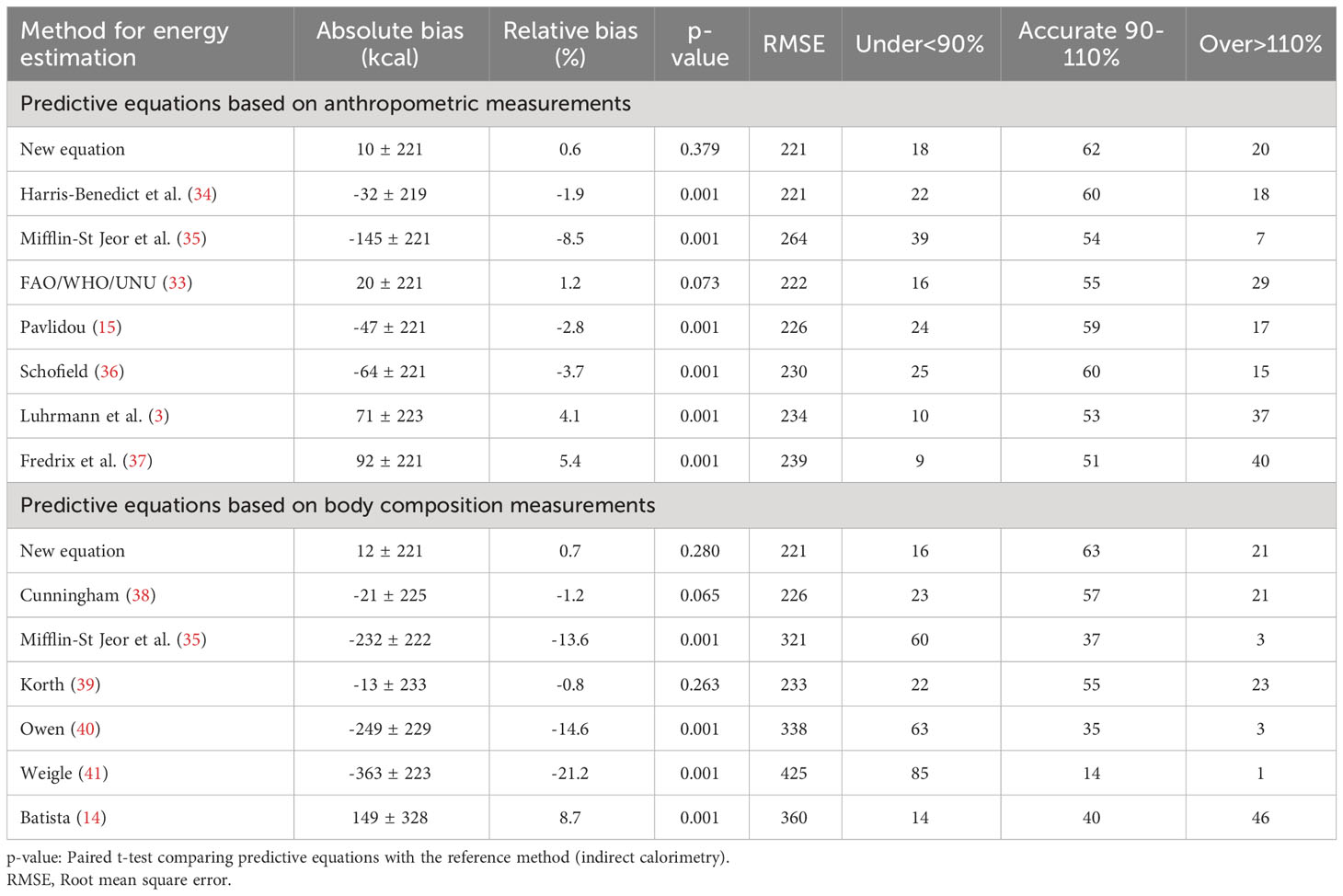
Table 5 Accuracy of predictive equations for resting energy estimation compared to Resting Energy Expenditure by indirect calorimetry in the validation group (n: 382).
Considering prediction equations based on body composition measurements, the new equation and equations proposed by Cunningham (38) and Korth et al. (39) did not show a significant difference from REE. However, the equations proposed by Mifflin et al. (35), Owen (1988), Weigle et al. (41) and Batista et al. (14) showed a significant underestimation of REE (Table 5).
The new proposed equations had accuracies of 62% and 63%, considering anthropometric and body composition models, respectively. Considering the other equations analyzed, the most accurate was the equation proposed by Harris-Benedict (34) and Schofield (36) with 60%, followed by Pavlidou et al. (15) with 59% (Table 5).
Most of the analyzed equations presented a systematic bias for underestimation of energy requirements, as observed in Figure 1. The smallest values of relative bias were found in the new equation, in the FAO/WHO/UNU (33) (1.2%) and in the Harris-Benedict (34) (-1.9%) considering anthropometric models, and in the Korth et al. (39) (-0.8%) and the Cunningham (38) (-1.2%) considering body composition models.
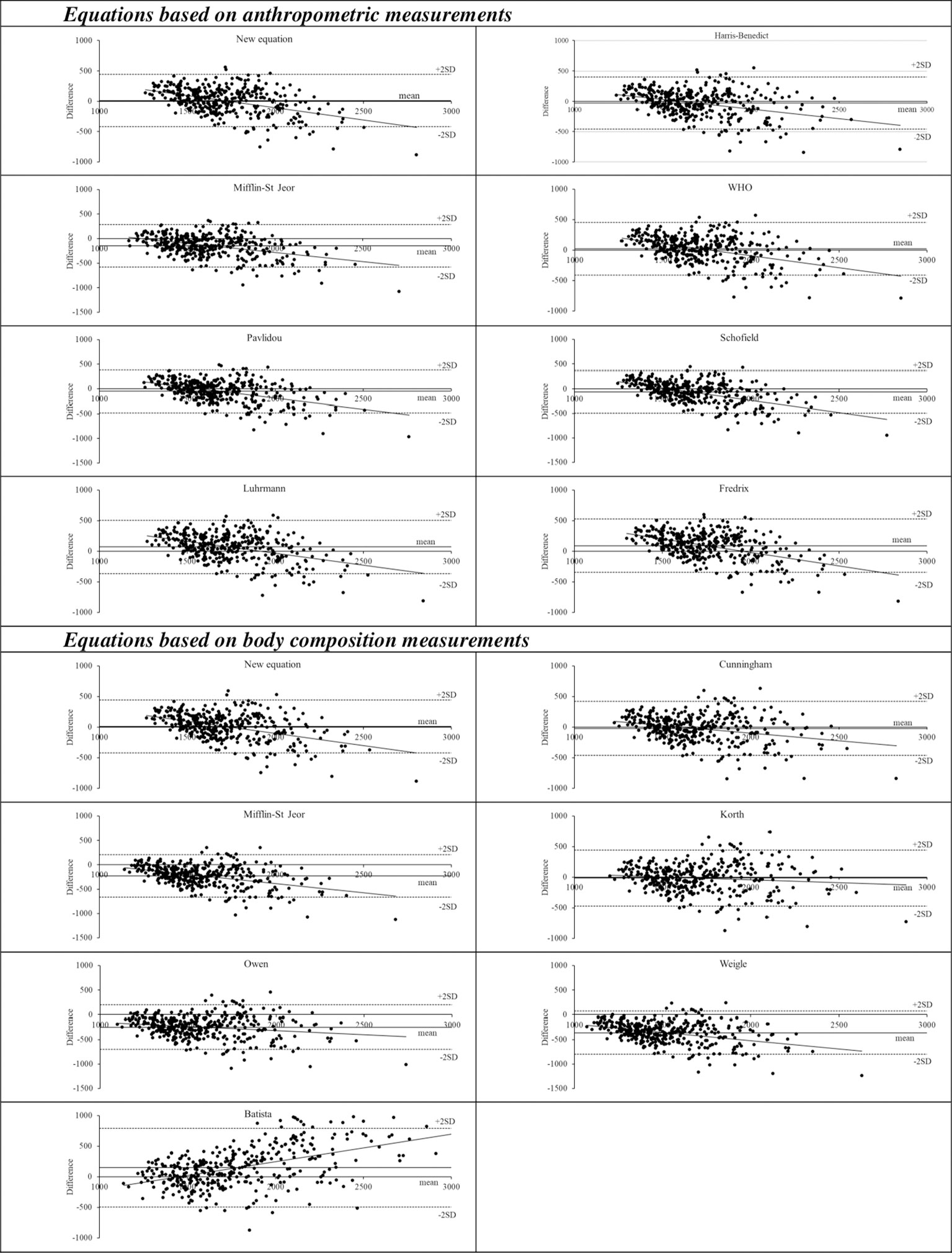
Figure 1 Bland-Altman plots of energy expenditure measured by indirect calorimetry and predicted by fifteen tested equations. The dashed lines represent the mean difference between Resting Energy Expenditure (REE) predicted by each of the tested equations and REE measured by indirect calorimetry and ±1.96 standard deviations (SD) of the mean (limits of agreement), with a 95% confidence interval (dotted lines).
4 Discussion
In the present study we proposed new equations to estimate REE in older adults with severe obesity based on data of indirect calorimetry and also, we validated them and other main equations already proposed in the literature. In summary, there was a variation in the previously proposed equations to predict REE in our sample, in which most of them underestimated the energy requirement and had poor accuracy. The best accuracies were found in the new proposed equations, with 62% and 63%, respectively, considering the anthropometric and body composition in the models.
Our results showed that only the new equations and the equation proposed by FAO/WHO/UNU (33) (for anthropometric models) and by Cunningham (38) and Korth et al. (39) (for body composition models) did not show a significant difference between the estimated values and those obtained by using the indirect calorimetry of REE. This evidence contradicts that found by Noreik et al. (5) in which a better accuracy for REE estimation in older adults with obesity was observed in the equation proposed by Lührmann et al. (3). However, this equation was tested in a sample of not hospitalized patients with a mean BMI value of 26 kg/m², which is far lower than the one considered for our sample of severely obese. Moreover, other studies that analyzed samples of old people (3, 14, 15, 36, 37) also included non-obese individuals, making extremely difficult the comparison of the results.
It is important to highlight that advanced aging alters the body composition, with an increase in adipose tissue and a decrease in lean tissues (42), and changes in both the quantity and quality of lean mass which are key factors to determine the REE precision of prediction equations. Due to their greater body mass, individuals with severe obesity require a higher REE than eutrophic people, to maintain their essential body functions (17). However, the weight excess in individuals with obesity has a significant impact on the age-related declines in terms of REE, with a mean decline almost 1.5 times greater than normal weight individuals (43).
Recently, Griffith et al. (6) validated four equations commonly used to guide weight loss interventions in a sample of older adults with obesity (≥ 65 years and BMI ≥ 30kg/m²) and found that FAO/WHO/UNU (33) also had the best accuracy for REE estimation. However, none of them obtained values above 60%. In the present study, although the highest accurate values were observed in the models with anthropometric variables, only the new equation with body composition variables achieved an accuracy of 62%. Other body composition-based prediction models compared in our study had a lower agreement, including the study by Batista et al. (14) with 40%, which was the only one that analyzed a sample of older adults, however non-obese. This finding is in agreement with other studies where FFM values were more pertinent than isolated anthropometric variables during energy requirements estimations (38, 39, 41).
In the present study, the REE obtained by indirect calorimetry was higher in men than in women, and in the same way, all equations predicted higher energy requirements for men. However, when REE values were normalized to the FFM, higher REE values were observed in women. The greater amount of fat mass in older women than in men could lead to a lower basal metabolic rate and, consequently, lower energy (18), thus reinforcing the importance of considering FFM values during REE estimations. Also, it is important to note that the inclusion of the FM variable in our prediction model did not substantially change the predictive estimation of REE calculated only with the FFM. Although our model explained less than 50% of the variance, it is in agreement with other studies that found FFM as the major factor related to REE (38, 44).
Most of the body composition equations tested in our study presented a tendency to underestimate the REE values. As previously mentioned, body composition, especially the FFM values of the sample and other measures of nutritional status are the main factors that influence the REE. In addition to the differences in clinical characteristics of the samples, the methods used in each study to calculate body composition should be considered to explain these variations. While we used BIA measurements, other tested equations were created based on skinfold measurements (38, 40) or densitometry methods (i.e. DXA) (14). It is also important to mention that other variables not included in our analysis may contribute to the variations observed in the REE of older adults with severe obesity. According to Martin et al. (45), the race can significantly affect REE variability. In fact, these authors demonstrated that black individuals typically have lower REE than white participants. Another anthropometric characteristic described in the literature is waist circumference, which has been shown to tend to increase in women with aging (46).
Some limitations of our study should be considered while interpreting the results. The new equations might not be entirely representative of European older adults with obesity being the average BMI of our sample considered representative of a severe obesity condition. Also, the sample was recruited in a hospital setting, and patients with serious illnesses were excluded. Therefore, body composition variables were measured by BIA, while DXA is still considered the gold standard method for the estimation of fat mass and fat-free mass.
Nevertheless, REE was measured by indirect calorimetry with a highly accurate method. To the best of our knowledge, our study was the first to propose specific equations for European older adults with severe obesity, with a mean BMI of 40.3 kg/m² for women and 38.5 kg/m² for men. Furthermore, our equation based on body composition measurements achieved an accuracy greater than 60%, which had not been found in previous studies. The validation analysis considered all the main equations used in the last decades, highlighting the importance of using specific equations for each population.
In conclusion, although the accuracy of our equations was slightly higher (62% and 63% considering anthropometric and body composition models, respectively) in comparison with the other available equations taken into consideration, they cannot be considered completely satisfactory for predicting REE in Italians older adults with severe obesity. To date, we cannot exclude that the use of these equations in other different populations might provide more accurate results than those obtained in the Italian population from which formulas have been developed. When predicting equations cannot guarantee precise or acceptable values of REE, the use of indirect calorimetry (if available) should be always recommended, especially in clinical practice.
Data availability statement
The raw data supporting the conclusions of this article will be uploaded on Zenodo.org immediately after the publication of the manuscript and they will be available upon a reasonable request to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethical Committee of Istituto Auxologico Italiano, IRCCS, Milan Italy (code: 2023_03_21_06; research code: 01C311, acronym: EQUASTIMET60). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AD: Conceptualization, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. SL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing, Resources, Visualization. AM: Data curation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. LA: Data curation, Validation, Visualization, Writing – review & editing. MD: Data curation, Formal Analysis, Validation, Visualization, Writing – review & editing. MDM: Data curation, Formal Analysis, Validation, Visualization, Writing – review & editing. MI: Data curation, Formal Analysis, Validation, Visualization, Writing – review & editing. NP: Validation, Visualization, Writing – review & editing. VM: Writing – review & editing. AL: Visualization, Writing – review & editing. AS: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Italian Ministry of Health - ricerca corrente. We also thank CNPq for Universal grant - CNPq-402574/2021-4.
Acknowledgments
The authors thank the nursing staff at the Division of Metabolic Diseases, Istituto Auxologico Italiano, Piancavallo-Verbania, Italy. The authors also thank the subjects for their participation in this research, and the Brazilian National Council for Scientific and Technological Development (CNPq – Brazil), which financed the scholarship for the postdoctoral abroad of AD.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Aging and Health (2022). Available at: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (Accessed 29 September 2023).
2. Malandrino N, Bhat SZ, Alfaraidhy M, Grewal RS, Kalyani RR. Obesity and aging. Endocrinol Metab Clin North Am (2023) 52(2):317–39. doi: 10.1016/j.ecl.2022.10.001
3. Lührmann PM, Herbert BM, Krems C, Neuhäuser-Berthold M. A new equation especially developed for predicting resting metabolic rate in the elderly for easy use in practice. Eur J Nutr (2002) 41:108–13. doi: 10.1007/s003940200016
4. Polyzos SA, Kountouras J, Mantzoros CS. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism (2019) 92:82–97. doi: 10.1016/j.metabol.2018.11.014
5. Noreik M, Maurmann M, Meier V, Becker I, Röhrig G, Polidori MC, et al. Resting energy expenditure (REE) in an old-old population: implications for metabolic stress. Exp Gerontol (2014) 59:47–50. doi: 10.1016/j.exger.2014.06.009
6. Griffith R, Shean R, Petersen CL, Al-Nimr RI, Gooding T, Roderka MN, et al. Validation of resting energy expenditure equations in older adults with obesity. J Nutr Gerontol Geriatr (2022) 41(2):126–39. doi: 10.1080/21551197.2022.2070320
7. Müller M, Selberg O, Süttmann U, Weimann A, KUSE E-R. Schätzung und Messung des Energieverbrauches: Methoden und Stellenwert in der klinischen Diagnostik. Intensivmedizin+ Notfallmedizin (1992) 29(8):411–26.
8. Kruizenga HM, Hofsteenge GH, Weijs PJ. Predicting resting energy expenditure in underweight, normal weight, overweight, and obese adult hospital patients. Nutr Metab (Lond) (2016) 13:85. doi: 10.1186/s12986-016-0145-3
9. Mtaweh H, Tuira L, Floh AA, Parshuram CS. Indirect calorimetry: History, technology, and application. Front Pediatr (2018) 6:257. doi: 10.3389/fped.2018.00257
10. Itoi A, Yamada Y, Yokoyama K, Adachi T, Kimura M. Validity of predictive equations for resting metabolic rate in healthy older adults. Clin Nutr ESPEN (2017) 22:64–70. doi: 10.1016/j.clnesp.2017.08.010
11. Lorenzo A, Renzo L, Morini P, Miranda RC, Romano L, Colica C. New equations to estimate resting energy expenditure in obese adults from body composition. Acta Diabetol (2018) 55(1):59–66. doi: 10.1007/s00592-017-1061-3
12. Orozco-Ruiz X, Pichardo-Ontiveros E, Tovar AR, Torres N, Medina-Vera I, Prinelli F, et al. Development and validation of new predictive equation for resting energy expenditure in adults with overweight and obesity. Clin Nutr (2018) 37(6 Pt A):2198–205. doi: 10.1016/j.clnu.2017.10.022
13. Marra M, Sammarco R, Cioffi I, Morlino D, Di Vincenzo O, Speranza E, et al. New predictive equations for estimating resting energy expenditure in subjects with normal weight and overweight. Nutrition (2021) 84:111105. doi: 10.1016/j.nut.2020.111105
14. Batista LD, Valentini Neto J, Grande de França NA, Lima Ribeiro SM, Fisberg RM. Body composition affects the accuracy of predictive equations to estimate resting energy expenditure in older adults: An exploratory study. Clin Nutr ESPEN (2023) 53:80–6. doi: 10.1016/j.clnesp.2022.11.021
15. Pavlidou E, Papadopoulou SK, Seroglou K, Giaginis C. Revised harris-benedict equation: new human resting metabolic rate equation. Metabolites (2023) 13(2):1–12. doi: 10.3390/metabo13020189
16. Porter J, Ward LC, Nguo K, Davidson Z, Gibson S, Prentice R, et al. Development and validation of new predictive equations for the resting metabolic rate of older adults aged ≥ 65 y. Am J Clin Nutr (2023) 117(6):1164–73. doi: 10.1016/j.ajcnut.2023.04.010
17. Oliveira BAP, Nicoletti CF, Oliveira CC, Pinhel MAS, Quinhoneiro DCG, Noronha NY, et al. A new resting metabolic rate equation for women with class III obesity. Nutrition (2018) 49:1–6. doi: 10.1016/j.nut.2017.11.024
18. Sgambato MR, Wahrlich V, Anjos LAD. Validity of basal metabolic rate prediction equations in elderly women living in an urban tropical city of Brazil. Clin Nutr ESPEN (2019) 32:158–64. doi: 10.1016/j.clnesp.2019.03.003
19. Maury-Sintjago E, Muñoz-Mendoza C, Rodríguez-Fernández A, Ruíz-De la Fuente M. Predictive equation to estimate resting metabolic rate in older Chilean women. Nutrients (2022) 14(15):1–10. doi: 10.3390/nu14153199
20. Ikeda K, Fujimoto S, Goto M, Yamada C, Hamasaki A, Ida M, et al. A new equation to estimate basal energy expenditure of patients with diabetes. Clin Nutr (2013) 32(5):777–82. doi: 10.1016/j.clnu.2012.11.017
21. Camps SG, Wang NX, Tan WS, Henry CJ. Estimation of basal metabolic rate in Chinese: are the current prediction equations applicable? Nutr J (2016) 15(1):79. doi: 10.1186/s12937-016-0197-2
22. Barcellos PS, Borges N, Torres DPM. New equation to estimate resting energy expenditure in non-critically ill patients. Clin Nutr ESPEN (2020) 37:240–6. doi: 10.1016/j.clnesp.2020.02.006
23. Buch A, Diener J, Stern N, Rubin A, Kis O, Sofer Y, et al. Comparison of equations estimating resting metabolic rate in older adults with type 2 diabetes. J Clin Med (2021) 10(8):1–11. doi: 10.3390/jcm10081644
24. Cioffi I, Marra M, Pasanisi F, Scalfi L. Prediction of resting energy expenditure in healthy older adults: A systematic review. Clin Nutr (2021) 40(5):3094–103. doi: 10.1016/j.clnu.2020.11.027
25. Guerrini Usubini A, Bottacchi M, Bondesan A, Caroli D, Castelnuovo G, Sartorio A. A three-week in-hospital multidisciplinary body weight reduction program exerts beneficial effects on physical and mental health and fatiguability of elderly patients with obesity. Front Aging Neurosci (2022) 14:1054941. doi: 10.3389/fnagi.2022.1054941
26. Gilbride J. Anthropometric standardization reference manual. J Am Dietetic Assoc (1989) 89(6):872–4.
27. Lukaski HC, Bolonchuk WW, Hall CB, Siders WA. Validation of tetrapolar bioelectrical impedance method to assess human body composition. J Appl Physiol (1986) 60(4):1327–321985. doi: 10.1152/jappl.1986.60.4.1327
28. Bedogni G, Agosti F, De Col A, Marazzi N, Tagliaferri A, Sartorio A. Comparison of dual-energy X-ray absorptiometry, air displacement plethysmography and bioelectrical impedance analysis for the assessment of body composition in morbidly obese women. Eur J Clin Nutr (2013) 67(11):1129–32. doi: 10.1038/ejcn.2013.159
29. McClave SA, Lowen CC, Kleber MJ, McConnell JW, Jung LY, Goldsmith LJ. Clinical use of the respiratory quotient obtained from indirect calorimetry. J Parenter Enteral Nutr (2003) 27(1):21–6. doi: 10.1177/014860710302700121
30. Weir JB. New methods for calculating metabolic rate with special reference to protein metabolism. J Physiol (1949) 109(1-2):1–9. doi: 10.1113/jphysiol.1949.sp004363
31. Bland JM, Altman D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet (1986) 327:307–108476. doi: 10.1016/S0140-6736(86)90837-8
32. Phang PT, Rich T, Ronco J. A validation and comparison study of two metabolic monitors. J Parenter Enteral Nutr (1990) 14(3):259–61. doi: 10.1177/0148607190014003259
33. FAO/WHO/UNU. Energy and protein requirements. Report of a joint FAO/WHO/UNU Expert Consultation. World Health Organ Tech Rep Ser (1985) 724:1–206.
34. Harris JA, Benedict FG. A Biometric Study of Human Basal Metabolism. Proc Natl Acad Sci USA (1918) 4(12):370–3. doi: 10.1073/pnas.4.12.370
35. Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, Koh YO. A new predictive equation for resting energy expenditure in healthy individuals. Am J Clin Nutr (1990) 51(2):241–7. doi: 10.1093/ajcn/33.11.2372
36. Schofield WN. Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr (1985) 39 Suppl 1:5–41.
37. Fredrix EW, Soeters PB, Deerenberg IM, Kester AD, von Meyenfeldt MF, Saris WH. Resting and sleeping energy expenditure in the elderly. Eur J Clin Nutr (1990) 44(10):741–7.
38. Cunningham JJ. A reanalysis of the factors influencing basal metabolic rate in normal adults. Am J Clin Nutr (1980) 33(11):2372–4. doi: 10.1093/ajcn/33.11.2372
39. Korth O, Bosy-Westphal A, Zschoche P, Glüer C, Heller M, Müller M. Influence of methods used in body composition analysis on the prediction of resting energy expenditure. Eur J Clin Nutr (2007) 61(5):582–9. doi: 10.1038/sj.ejcn.1602556
40. Owen OE. Resting metabolic requirements of men and women. ; 63(5):503-10. In Mayo Clinic Proceedings (1988) 63(5):503–10.
41. Weigle DS, Sande KJ, Iverius PH, Monsen ER, Brunzell JD. Weight loss leads to a marked decrease in nonresting energy expenditure in ambulatory human subjects. Metabolism (1988) 37(10):930–6. doi: 10.1016/0026-0495(88)90149-7
42. Shlisky J, Bloom DE, Beaudreault AR, Tucker KL, Keller HH, Freund-Levi Y, et al. Nutritional considerations for healthy aging and reduction in age-related chronic disease. Adv Nutr (2017) 8(1):17–26. doi: 10.3945/an.116.013474
43. Siervo M, Oggioni C, Lara J, Celis-Morales C, Mathers JC, Battezzati A, et al. Age-related changes in resting energy expenditure in normal weight, overweight and obese men and women. Maturitas (2015) 80(4):406–13. doi: 10.1016/j.maturitas.2014.12.023
44. Karlsson M, Olsson E, Becker W, Karlström B, Cederholm T, Sjögren P. Ability to predict resting energy expenditure with six equations compared to indirect calorimetry in octogenarian men. Exp Gerontol (2017) 92:52–5. doi: 10.1016/j.exger.2017.03.013
45. Martin K, Wallace P, Rust PF, Garvey WT. Estimation of resting energy expenditure considering effects of race and diabetes status. Diabetes Care (2004) 27(6):1405–11. doi: 10.2337/diacare.27.6.1405
Keywords: energy expenditure, predictive equations, indirect calorimetry, obesity, older adults, aging
Citation: Danielewicz AL, Lazzer S, Marra A, Abbruzzese L, D’Alleva M, Martino MD, Isola M, Avelar NCP, Mendonça VA, Lacerda ACR and Sartorio A (2023) Prediction of resting energy expenditure in Italian older adults with severe obesity. Front. Endocrinol. 14:1283155. doi: 10.3389/fendo.2023.1283155
Received: 25 August 2023; Accepted: 23 October 2023;
Published: 08 November 2023.
Edited by:
Xilin Yang, Tianjin Medical University, ChinaReviewed by:
Ann Kristine Jansen, Federal University of Minas Gerais, BrazilIolanda Cioffi, University of Milan, Italy
Copyright © 2023 Danielewicz, Lazzer, Marra, Abbruzzese, D’Alleva, Martino, Isola, Avelar, Mendonça, Lacerda and Sartorio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefano Lazzer, c3RlZmFuby5sYXp6ZXJAdW5pdWQuaXQ=
†ORCID: Ana Lúcia Danielewicz, orcid.org/0000-0003-1563-0470
Stefano Lazzer, orcid.org/0000-0003-0067-2221
Alice Marra, orcid.org/0000-0002-3181-634X
Laura Abbruzzese, orcid.org/0000-0003-3855-1599
Mattia D’Alleva, orcid.org/0000-0001-9179-1618
Maria De Martino, orcid.org/0000-0002-0445-9578
Miriam Isola, orcid.org/0000-0002-6391-1720
Núbia Carelli Pereira de Avelar, orcid.org/0000-0003-4212-4039
Vanessa Amaral Mendonça, orcid.org/0000-0002-1696-6091
Ana Cristina Rodrigues Lacerda, orcid.org/0000-0001-5366-3754
Alessandro Sartorio, orcid.org/0000-0002-9620-4133