
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol. , 08 January 2024
Sec. Thyroid Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1277961
 Rafael Luccas1,2
Rafael Luccas1,2 Cinthia Minatel Riguetto3,4
Cinthia Minatel Riguetto3,4 Monica Alves5
Monica Alves5 Denise Engelbrecht Zantut-Wittmann3
Denise Engelbrecht Zantut-Wittmann3 Fabiano Reis2*
Fabiano Reis2*Graves’ ophthalmopathy (GO) affects up to 50% of patients with Graves’ disease (GD) ranging from mild ocular irritation to vision loss. The initial diagnosis is based on clinical findings and laboratory tests. Orbital imaging, such as magnetic resonance imaging (MRI) and computed tomography (CT), is an important tool to assess orbital changes, being also useful for understanding disease progression and surgical planning. In this narrative review, we included 92 studies published from 1979 to 2020 that used either MRI and/or CT to diagnose and investigate GO, proposing new methods and techniques. Most of the methods used still need to be corroborated and validated, and, despite the different methods and approaches for thyroid eye disease (TED) evaluation, there is still a lack of standardization of measurements and outcome reports; therefore, additional studies should be performed to include these methods in clinical practice, facilitating the diagnosis and approach for the treatment of TED.
Graves’ disease (GD), the most common causes of hyperthyroidism in iodine-replete areas, is characterized by the excess of thyroid hormones associated with loss of the negative feedback between the hypothalamic–pituitary axis and the thyroid gland due to circulating thyroid-stimulating anti-thyrotropin receptor antibodies (TRAb) (1). TRAb mimic the action of hormone, excessively activating thyroid gland follicular cells and inducing its growth and vascularization (2). GD has an approximate incidence of 40 cases, each with 100,000 persons, being more frequent in women and patients between 30 and 50 years old, and may include extrathyroidal features, including Graves’ ophthalmopathy (GO) (3, 4).
GO affects up to 50% of the patients, varying from mild ocular irritation to vision loss (2). Patients may experience conjunctival redness, conjunctival and eyelid swelling, proptosis, retrobulbar pain, ocular dryness, photophobia, and reduced visual acuity secondary to optic nerve compression and cornea erosion. From a mechanical point of view, these signs and symptoms are due to an enlargement of orbital fat tissue and extraocular muscles, compressing the surrounding structures (5). Although the diagnosis of GO is based on clinical findings such as inflammation of the orbit and proptosis, imaging exams, including magnetic resonance imaging (MRI), computed tomography (CT), and ultrasonography, are useful in the identification and follow-up of clinically active GO (6) as well as unusual cases of unilateral ophthalmopathy, optic neuropathies, and optic nerve compression (7).
Imaging exams are not an essential tool to diagnose GO in clinical practice; however, they can add valuable information on tissue microstructure, leading to new findings on actual disease progress and status, which is vital for planning treatment and interventions (8). Imaging in patients with GO may reveal an increase in orbital fibroadipose tissue, enlargement of extraocular muscles, and optic-nerve compression. Imaging is especially warranted in cases of asymmetric proptosis and for differential diagnosis (9, 10).
Orbital imaging is an important tool to assess disease progression and for surgical planning. MRI and CT can be used individually or mutually for these applications. The enlargement of extraocular muscles is the main characteristic of GO. Still, it is challenging to determine if the muscle is volumetrically enlarged in the scenario of symmetric mild disease, where the patient-specific normal measure parameter is lost (4). On the other hand, there has been developed normative data that define an average for normal extraocular muscle measurements (11–14) as a guide, but not as a norm, because it represents variations and overlap cases on both healthy and diseased muscles.
The inferior rectus muscle is the most frequently involved in clinical myopathy, followed by medial, superior, and lateral rectus muscles, respectively. In GO, multiple muscles can be involved simultaneously and/or bilaterally in 76% to 90% of the cases. Extraocular muscle enlargement is the most common sign among these patients, usually affecting younger and older patients differently. According to Su et al. (15), younger patients are less affected by motility restriction despite developing more proptosis even with enlarged muscles, whereas older patients suffer from more motility restriction and diplopia due to the muscle bellies enlargement posterior in the orbit. Proptosis is mainly related to the most enlarged muscle position than the size itself; however, imaging analysis for muscle enlargement is not precise or sensitive and should be used as adjuvant evidence for diagnosis (16).
Another remarkable characteristic of GO is the fat expansion associated with proptosis, younger patients, and a longer GO duration. Visually, fat expansion can expand the brow, galeal, and premalar regions but may also be identified and measured by imaging. Both fat expansion and muscle enlargement are usually measured in volume individually.
Exophthalmos is usually measured during clinical evaluations by a Hertel exophthalmometer, but imaging techniques can be also used for this measurement, tracing a reference line between the anterior extents of each zygomatic bone in a mid-orbital axial section and then measuring the distance from this reference line to the posterior aspect of the ocular globe. A distance of 10 mm or less indicates exophthalmos (9). The level of proptosis is indicated by grades: grade 1 when more than two-thirds of the anteroposterior diameter of the eyeball is projected to the front of the line, grade 2 when the posterior pole of the globe border the line, and grade 3 when the entire eyeball is projected in front of this line (17).
Due to the difficulties in accessing GO image changes, our aim was to review systematically studies that used imaging approaches to diagnose or investigate the disease, proposing new methods and techniques or further investigating the usual ones.
The search for these studies occurred on the main databases such as PubMed, Embase, Scopus, and Web of Science in September 2021. This review used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (18) as a reference for the article structure.
Publications with no year restriction until the search date were considered, involving CT or MRI approaches in patients with GD who did not undergo clinical or surgical treatment to evaluate clinical activity or severity of the disease. Studies without a control group were also considered because the objective of this review is also to give the full scenario of the current state of the studies and research works being done with imaging in GO and how the study designs differ from each other. Due to the large number of results generated by the search strategy (Supplementary Material), the following exclusion criteria were considered for better selection of the studies: being related to other ocular diseases instead of GD; other imaging approaches than CT or MRI; studies with animals; case reports, reviews, meta-analysis, and treatment outcome investigation studies; and publication in other languages than English.
All studies were evaluated separately by Rafael Luccas (RL) and Cinthia Minatel Riguetto (CMR), considering the inclusion and exclusion criteria. A total of 2,032 publications were initially retrieved, and 1,703 and 1,733 were excluded by the reviewer RL and CR, respectively, based on the title or abstract. The difference between the selected publications by the reviewers was revised jointly by the reviewers to decide on the inclusion. Three hundred twenty-nine articles were read, of which 234 studies were excluded and 95 studies were considered for the review across CT and MRI modalities, as shown in Figure 1.
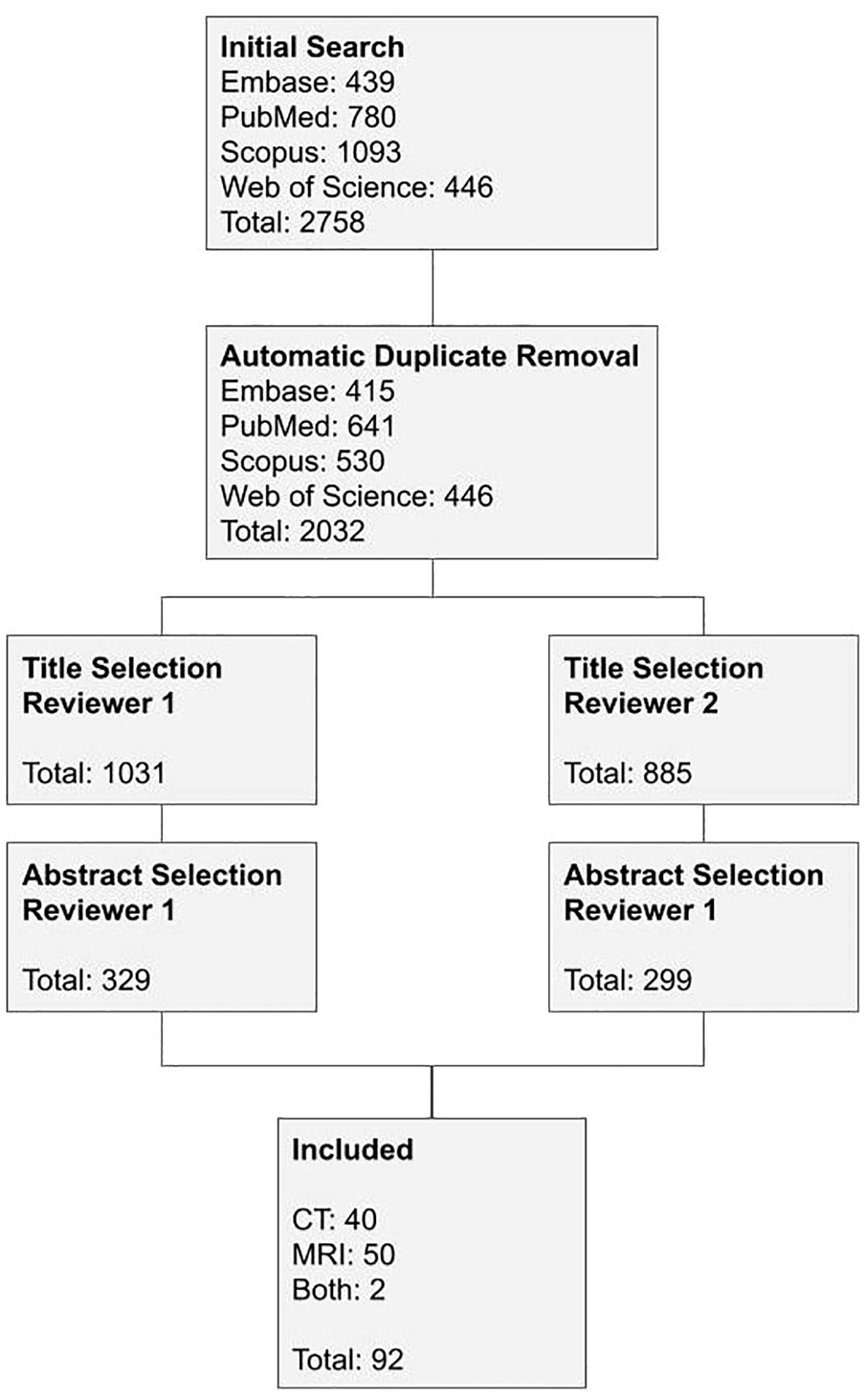
Figure 1 Studies selection flowchart.
The following information was retrieved from the publications and summarized in tables, one for each imaging modality detailed: number of subjects, sex, if the subjects were divided into groups on the study, use of control group, mean age with standard deviation, age range, evaluation area, acquisition details (thickness in mm for CT studies and magnetic field intensity in T for MRI studies), evaluation method, software used for imaging analysis, if the proposed method was able to evaluate GO activity or severity, and if the study used any classification for the disease activity.
The study was approved by the local ethical committee (CAAE number 92689218.8.0000.5404).
There were 42 publications included on the CT modality from 1979 to 2020 (Table 1). A total of 3,228 subjects were assessed, of which 1,973 were women, representing 61.12% of the sample, whereas male subjects represented 27.14%. In only three studies, the number of male subjects surpassed the number of women. Some studies did not specify the patients’ sex; therefore, 21.43% of the sample is undefined regarding this category. The age of the subjects ranged from 5 to 89 years old, but only 19.05% of the studies included the juvenile population. Of the studies included in this modality, only 38.10% had a control group, and three subclassified the subjects regarding GO activity [e.g., active thyroid eye disease (TED), inactive TED, and GD without ophthalmopathy].
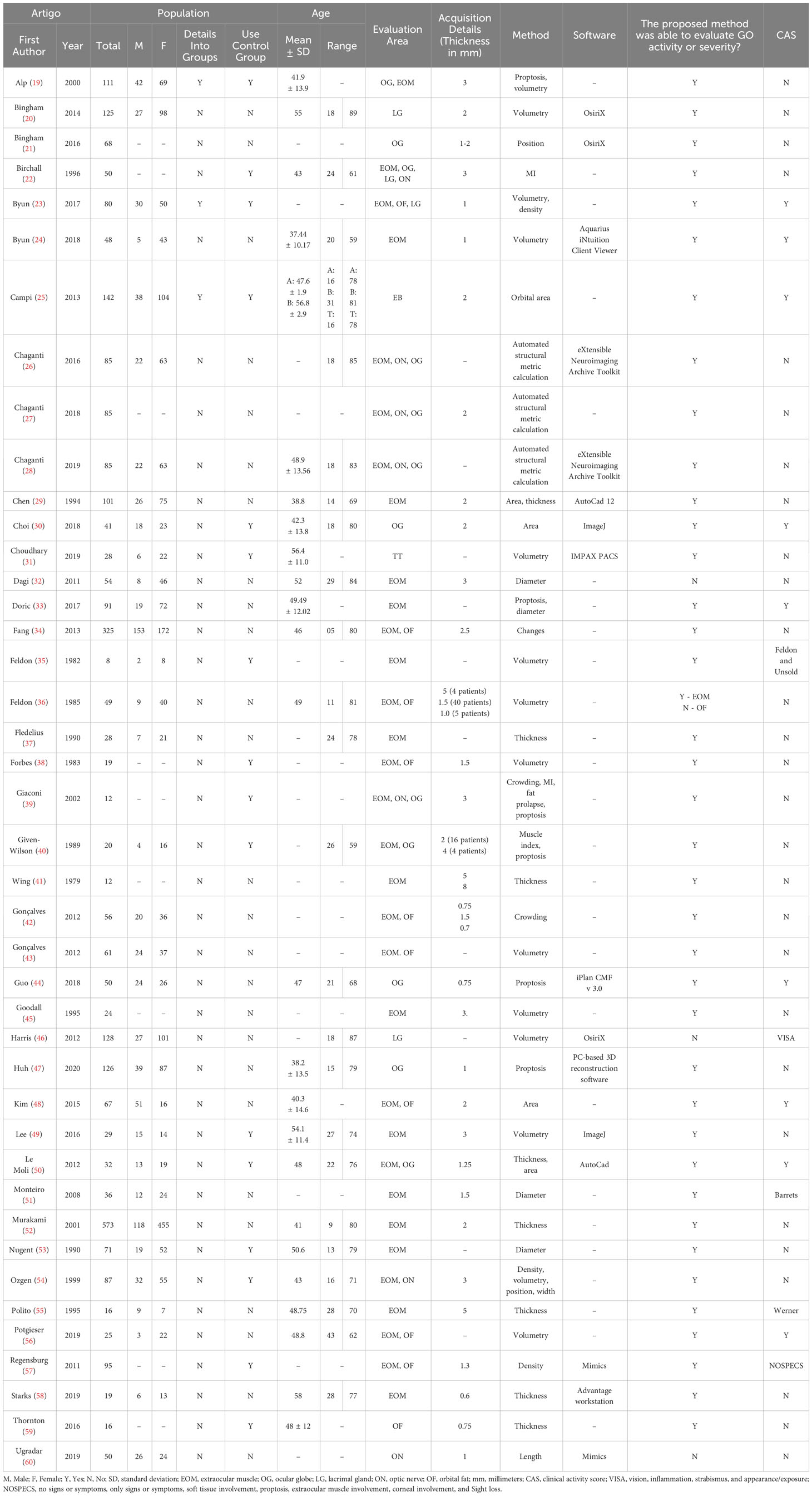
Table 1 Studies that used CT as an imaging method to investigate thyroid eye disease.
Different ocular regions were evaluated by these studies, such as extraocular muscles (78.57%), ocular globe (30.95%), orbital fat (23.81%), optic nerve (16.67%), and lacrimal gland (9.52%). Different methods were also applied to assess these areas, including volumetry (30.95%); thickness (19.05%); proptosis (14.29%); area and diameter (9.52% each); automated structural metric calculation (7.14%); position, muscle index, and crowding (4.76% each); and density, changes in general, fat prolapse, diffusion tensor imaging, width, and length (2.38% each).
For CT studies, the acquisition details more frequently reported was the slice thickness, which ranged from 0.6 to 8 mm, with a mean thickness of 3 mm. Ten studies did not specify acquisition details. Only 38.10% of the studies reported the software used for imaging analysis, not considering the publications that indicated that the analysis was done on the workstation.
The study’s proposed methods were able to evaluate GO activity or severity, with 95.24% of them considering that the method demonstrated a promising way of diagnosing or assessing the disease. Only 9.52% reporting the results were not satisfying. A total of 21.43% of the studies evaluated disease activity through the Clinical Activity Score (CAS), whereas 11.90% used other classifications [NOSPECS (no signs or symptoms, only signs or symptoms, soft tissue involvement, proptosis, extraocular muscle involvement, corneal involvement, and sight loss), Werner, Barrets, VISA (vision, inflammation, strabismus, and appearance/exposure), and Feldon and Unsold], and 66.67% did not use any method for disease activity classification.
Fifty-two publications from 1988 to 2021 were included in the MRI group (Table 2). One thousand nine hundred forty-two subjects were analyzed, of which 1,253 were women, and 591 were men, representing 64.52% and 30.43% of the sample, respectively. In only four studies, the number of male subjects surpassed the number of women. Like in the CT studies, some of them did not specify the patients’ sex; therefore, 5.05% of the sample was undefined. The age of the subjects ranged from 4 to 83 despite 53.85% of them not specifying the age range. Only 7.69% of the studies included the juvenile population. Of the studies included, 67.31% had a control group, and 25% subclassified the subjects according to disease activity (e.g., active TED, inactive TED, and GD without ophthalmopathy).
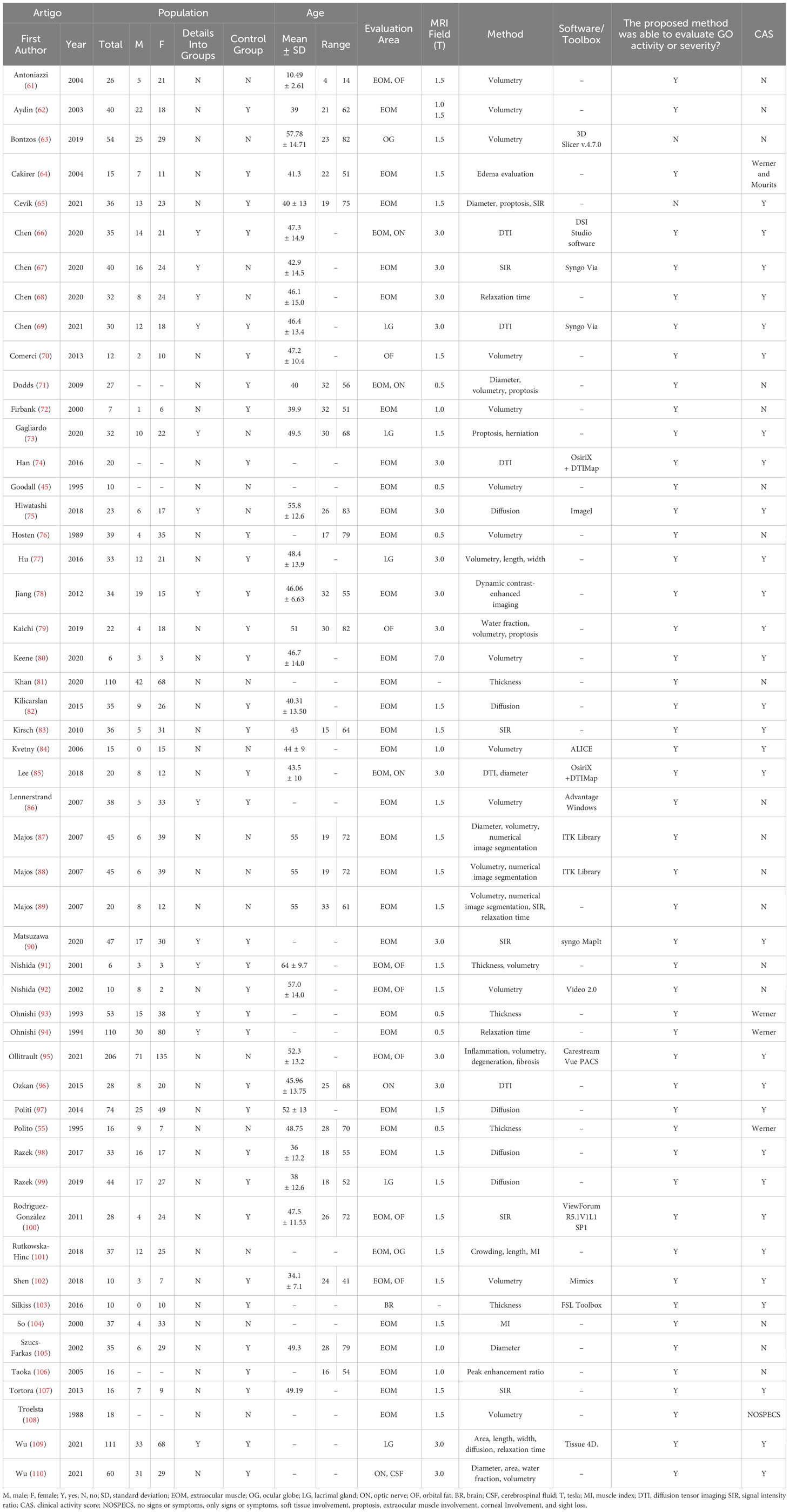
Table 2 Studies that used MR as an imaging method to investigate thyroid eye disease.
Different ocular regions were assessed, such as extraocular muscles (78.85%), orbital fat (15.38%), lacrimal gland and optic nerve (9.62% each), ocular globe (3.85%), and brain and cerebrospinal fluid (1.92% each). Different methods were also applied to evaluate these areas, including volumetry (40.38%); diameter, diffusion, and signal intensity ratio (11.54% each); diffusion tensor imaging (9.62%); proptosis, thickness, and relaxation time (7.69% each); length and numerical image segmentation (5.77% each); muscle index, area, width, and water fraction (3.85% each); and crowding, edema, herniation, dynamic contrast-enhanced imaging, inflammation, degeneration, fibrosis, and peak enhancement ratio (1.92% each).
The acquisition detail, more frequently, was the magnetic field, ranging from 0.5 T to 7.0 T, with a mean field of 1.5 T. Only 34.62% of the studies reported the software used for imaging analysis, not considering the publications that indicated that the analysis was done on the workstation.
The study’s proposed methods were able to evaluate GO activity or severity, with 96.15% considering the used method demonstrated a promising way of diagnosing or evaluating the disease. Only 3.85% reported that the results were not satisfying. The disease activity was assessed through CAS by 59.62% of the studies, whereas 9.62% used other classifications (NOSPECS and Werner), and 32.69% did not use any method for disease classification.
GO can be diagnosed at different stages, and it is crucial to identify the stage in order to guide treatment approaches (111). Unfortunately, only a small percentage of the studies included herein identified the stages and evaluated them according to subgroups. Studies seeking to evaluate diagnostic methods and disease grading would better consider disease stage to evidence which method is more sensitive for each distinct stage, as shown by Chen et al. (65–69). In this MRI study, all findings suggested that the methods used can help to identify the disease activity and staging, providing a better perspective on treatment options. Gagliardo et al. (73) also evaluated the subjects into different groups regarding the disease activity, and their findings pointed to an easy method for daily practice to diagnose and identify the disease stage.
Across the included studies, there were seven areas investigated. In the CT studies, the investigators analyzed the extraocular muscle, the ocular globe, the lacrimal gland, the optic nerve, and the orbital fat. The extraocular muscles were the most investigated area, with 76.74% of the studies analyzing it, mostly its volumetry, thickness, and diameter because it is reported as the most affected area by the disease (112) and considered an important factor to determine the disease diagnosis and its activity. Han et al. (74), different from other studies, used diffusion tensor imaging to measure the fractional anisotropy, mean, axial, and radial diffusivities of the muscles. The authors not only stated that diffusion imaging allows the identification of the disease stage, as acute or chronic, but also recognized its limitations on reflecting the disease activity according to the CAS. Dagi et al. (32) and Su et al. (15) found a weak correlation between extraocular muscle diameters and motility in younger subjects but stronger in older patients with active TED. The studies varied in affirming which extraocular muscle is the most affected by the disease, if the inferior rectus muscle (19), the medial (36) or lateral rectus muscles (37), but all agree on muscle involvement in general. Potgieser et al. (56) also found that the extraocular muscle involvement decreases in regard to volume over the years of natural disease history, inversely proportional to orbital fat that increases the volume over the years. Orbital fat was also investigated by CT (23.26%), and as related to ophthalmopathy as the extraocular muscles. Feldon et al. (36) state that the orbital fat does not play an essential role in the disease; however, others (31, 34, 39, 57) demonstrated the relation of the orbital fat with the disease progress and the importance on imaging findings to diagnose and evaluate this condition, by measuring the orbital fat density, ratio with orbital area, or volume. The ocular globe was mostly assessed by its position and proptosis or better methods to do these measures (44), also correlating the extraocular muscles and orbital fat involvement (19, 21).
Harris et al. (46) found lacrimal gland enlargement in GO with a weak correlation with proptosis or inflammation, contested by Bingham et al. (20), who affirmed that the lacrimal gland enlargement was positively correlated with proptosis.
MRI studies investigated the extraocular muscle, the ocular globe, the lacrimal gland, the optic nerve, the orbital fat, the cerebrospinal fluid, and the brain. Similarly to the CT studies, the extraocular muscles were evaluated by 78.85% of the studies using mainly volumetry, diameter, thickness, diffusion (weighted and tensor imaging), and signal intensity ratio. The findings of volumetry, diameter, and thickness were very similar to the ones with CT; however, the use of MRI allows the investigator to approach the disease with other methods, such as diffusion and signal intensity ratio, used together by 32.69% of the studies. Diffusion tensor imaging studies (66, 69) can assess microstructural changes in the extraocular muscles and indicate the disease activity with mean diffusivity metrics of medial extraocular muscles, whereas Han et al. (74) agreed with the advantages of this method remarking that the fractional anisotropy and radial diffusivity are better markers for the disease activity. The diffusion-weighted imaging was evaluated (82, 98) using the apparent diffusion coefficient as a metric on the extraocular muscles stating to diagnosis. The study highlights that the medial rectus muscle is the better one to obtain the metric, and the study by Kilicarslan et al. (82) found that the metric also correlates to ophthalmologic tests, making the method a promising option because the diffusion-weighted imaging sequence can be obtained on routine MRI, improving information about the disease. The signal intensity ratio of T1 and T2 images was also promising in indicating disease activity (83, 97). Both studies pointed out the method used to indicate disease activity in extraocular muscles, helping to determine the best treatment approach, because T1 and T2 images are sequences collected routinely.
Orbital fat findings in MRI are similar to the findings in CT studies (92, 102). The degree of exophthalmos and the volume rate obtained with MRI were both accurate and reliable. The sum of all the findings regarding orbital fat indicates that not only the extraocular muscles but also the orbital fat should be routinely when evaluating GO. The optic nerve and lacrimal gland were assessed by MRI mainly by diffusion methods. Chen et al. (66), Lee et al. (85), and Ozkan et al. (96) used diffusion tensor imaging to evaluate the optic nerve indicating fractional anisotropy and mean diffusivity as the main metrics to assess the nerve, whereas Chen et al. (69) used the method to evaluate the lacrimal gland, showing that the metrics, particularly the fractional anisotropy, can be useful to reveal the disease activity. Razek et al. (99) and Wu et al. (109) also evaluated the lacrimal gland but using diffusion-weighted imaging and signal intensity ratio, respectively, which both demonstrated promising results for diagnosing and predicting disease activity.
Interestingly, two studies investigated unusual areas of TED: brain and cerebrospinal fluid. Wu et al. (110) evaluated the volume of cerebrospinal fluid in the optic nerve sheath by applying a semi-automatic segmentation algorithm based on water images and stated that the cerebrospinal fluid was causing the enlargement of the optic nerve sheath, concluding that these measurements were sensitive for dysthyroid optic neuropathy. Silkiss et al. (103) evaluated the brain anatomy in patients with thyroid ophthalmopathy using an automatic cortical segmentation algorithm to estimate the thickness of the subject’s grey matter and found changes in six locations on the right hemisphere and two on the left hemisphere, possibly associated with the cognitive changes reported by the patients. These two studies showed that new approaches not only in methods but also on sites of investigation could be very promising for a better understanding and management of GO.
Most methods have not achieved sufficient scientific evidence regarding their reproducibility. Studies performed with CT were the least specific when describing the acquisition methods, 23.26% of them did not specify the image acquisition details, and others mostly indicated the thickness of the slices. Otherwise, MRI studies showed the field potency, highly relevant due to this information directly reflecting on the quality of the acquired image and, consequently, the quality of the outcomes. Thus, regarding reproducibility, only a few studies (36.84%) across CT and MRI reported the software used for the image analysis, and they were different among them, indicating that, despite the method used, there is no standard procedure for evaluating the disease when it comes to imaging analysis of non-dimensional metrics.
One of the most critical factors to validate a method was the correlation with the assessments already established as standard procedures in medical practice, such as CAS when it comes to TED. In CT studies, 65.12% did not use any disease activity assessments, whereas, in MRI studies, the percentage found was 32.69%. The use of such assessments in clinical studies to determine their validity and to increase the chance for the method to become implemented in the hospital routine is relevant.
This review demonstrated that, despite the fact that several studies have been performed using different methods and approaches for TED evaluation, there is still a lack of standardization of measurements and outcome reports. Indeed, important information related to method implementation or reproducibility and specifications about the software used for analysis or the imaging acquisition parameter have not been reported. Enhancement of reproducibility and methodological heterogeneity will set the stage for more robust studies to define its clinical relevance. As discussed before, there is also a need for studies about TED that relate common practice and disease management to achieve more effective and realistic measurements and direct treatment strategies.
Regarding the scope of the studies, there was a considerable discrepancy between the ones evaluating extraocular muscles and those evaluating other areas. Orbital fat comes right after the extraocular muscles, but these studies showed that other areas also have promising results when it comes to diagnosing and identifying the disease activity, highlighting the studies with lacrimal gland, optic nerve, and the brain.
Considering the study designs, even using different methods, several attention points should be considered. For more homogeneous, reproducible, and reliable study designs, we propose that:
● the investigators consider using control groups to increase the reliability of the results because the disease diagnosis is the focus and should be, whenever possible, compared to healthy subjects for a better understanding of the alterations between groups;
● the acquisition of the image be best possible within the study site capabilities for a guaranteed quality of data obtained on image analysis;
● relate the results with scores of approved and validated assessment methods such as CAS for the GO;
● better description of the study design, methods, and data or image acquisition on the published papers, indicating, for example, which software was used for imaging analysis and statistical results, acquisition protocols, metrics for imaging, and equipment details.
In the revised studies, it was possible to notice that most of the methods used still need to be corroborated and validated; therefore, more studies should be performed to include these methods in clinical practice, facilitating the diagnosis and approach for the treatment of TED.
RL: Conceptualization, Data curation, Formal Analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. CMR: Validation, Writing – review & editing. MA: Conceptualization, Writing – review & editing. DEZ-W: Conceptualization, Writing – review & editing. FR: Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We would like to thank to Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for funding this study under the process CAPES (AUXPE) 88881.859210/2023-01 and make it possible to be published.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1277961/full#supplementary-material
1. Riguetto CM, Neto AM, Tambascia MA, Zantut-Wittmann DE. The relationship between quality of life, cognition, and thyroid status in Graves’ disease. Endocrine (2019) 63(1):87–93. doi: 10.1007/s12020-018-1733-y
2. Łacheta D, Miśkiewicz P, Głuszko A, Nowicka G, Struga M, Kantor I, et al. Immunological aspects of graves’ Ophthalmopathy. BioMed Res Int (2019) 12:2019. doi: 10.1155/2019/7453260
3. Ehlers M, Schott M, Allelein S. Graves’ disease in clinical perspective. Front Biosci (Landmark Ed) (2019) 24(1):35–47. doi: 10.2741/4708
4. Smith TJ, Hegedüs L. Graves’ Disease. N Engl J Med (2016) 375(16):1552–65. doi: 10.1056/NEJMra1510030
5. Genere N, Stan MN. Current and emerging treatment strategies for graves’ Orbitopathy. Drugs (2019) 79(2):109–24. doi: 10.1007/s40265-018-1045-9
6. Fox TJ, Anastasopoulou C. Graves orbitopathy. In: StatPearls. Treasure Island (FL: StatPearls Publishing (2022). Available at: https://www.ncbi.nlm.nih.gov/books/NBK549889/.
7. Müller-Forell W, Kahaly GJ. Neuroimaging of graves’ orbitopathy. Best Pract Res Clin Endocrinol Metab (2012) 26(3):259–71. doi: 10.1016/j.beem.2011.11.009
8. Edmunds MR, Boelaert K. Knowledge of thyroid eye disease in graves’ Disease patients with and without orbitopathy. Thyroid (2019) 29(4):557–62. doi: 10.1089/thy.2018.0665
9. Lo C, Ugradar S, Rootman D. Management of graves myopathy: Orbital imaging in thyroid-related orbitopathy. J AAPOS (2018) 22(4):256.e1–9. doi: 10.1016/j.jaapos.2018.06.002
10. Wémeau JL, Klein M, Sadoul J, Briet C, Vélayoudom-Céphise F. Graves’ disease: Introduction, epidemiology, endogenous and environmental pathogenic factors. Ann Endocrinol (Paris) (2018) 79(6):599–607. doi: 10.1016/j.ando.2018.09.002
11. Ozgen A, Ariyurek M. Normative measurements of orbital structures using CT. AJR Am J Roentgenol (1998) 170(4):1093–6. doi: 10.2214/ajr.170.4.9530066
12. Wolf A, Jaafar M, Olsen C, Kadom N. Normative values for pediatric extraocular muscle position. Invest Ophthalmol Vis Sci (2008) 49(13):1805.
13. Zhang ZH, Chen Y, Wang Y, Meng W, Fang H-Y, Xu D-D, et al. Normative measurements of extraocular musculature by multislice computed tomography. Chin Med Sci J (2013) 27(4):232–6. doi: 10.1016/s1001-9294(13)60007-3
14. Rana K, Juniat V, Rayan A, Patel S, Selva D. Normative measurements of orbital structures by magnetic resonance imaging. Int Ophthalmol (2022) 42(12):3869–75. doi: 10.1007/s10792-022-02407-1
15. Su Y, Liu X, Fang S, Huang Y, Li Y, Zhong S, et al. Age-related difference in extraocular muscles and its relation to clinical manifestations in an ethnically homogenous group of patients with Graves’ orbitopathy. Graefes Arch Clin Exp Ophthalmol (2022) 260(2):583–9. doi: 10.1007/s00417-021-05377-9
16. North VS, Freitag SK. A review of imaging modalities in thyroid-associated orbitopathy. Int Ophthalmol Clin (2019) 59(4):81–93. doi: 10.1097/IIO.0000000000000289
17. Baptista AC, Marchiori E, Boasquevisque E, Cabral CEL. Proptose ocular como manifestação clínica de tumores Malignos extra-orbitários: estudo pela tomografia computadorizada. Radiol Bras (2003) 36:81–8. doi: 10.1590/S0100-39842003000200006
18. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (2021) 372:n71. doi: 10.1136/bmj.n71
19. Alp MN, Ozgen A, Can I, Cakar P, Gunalp I. Colour Doppler imaging of the orbital vasculature in Graves’ disease with computed tomographic correlation. Br J Ophthalmol (2000) 84(9):1027–30. doi: 10.1136/bjo.84.9.1027
20. Bingham CM, Harris MA, Realini T, Nguyen J, Hogg JP, Sivak-Callcott JA. Calculated computed tomography volumes of lacrimal glands and comparison to clinical findings in patients with thyroid eye disease. Ophthalmic Plast Reconstructive Surg (2014) 30(2):116–8. doi: 10.1097/iop.0000000000000015
21. Bingham CM, Sivak-Callcott JA, Gurka MJ, Nguyen J, Hogg JP, Feldon SE, et al. Axial globe position measurement: A prospective multicenter study by the international thyroid eye disease society. Ophthalmic Plast Reconstr Surg (2016) 32(2):106–12. doi: 10.1097/iop.0000000000000437
22. Birchall D, Goodal KL, Noble JL, Jackson A. Graves ophthalmopathy: Intracranial fat prolapse on CT images as an indicator of optic nerve compression. Radiology (1996) 200(1):123–7. doi: 10.1148/radiology.200.1.8657899
23. Byun JS, Moon NJ, Lee JK. Quantitative analysis of orbital soft tissues on computed tomography to assess the activity of thyroid-associated orbitopathy. Graefes Arch Clin Exp Ophthalmol (2017) 255(2):413–20. doi: 10.1007/s00417-016-3538-0
24. Byun JS, Lee JK. Relationships between eyelid position and levator-superior rectus complex and inferior rectus muscle in patients with Graves’ orbitopathy with unilateral upper eyelid retraction. Graefes Arch Clin Exp Ophthalmol (2018) 256(10):2001–8. doi: 10.1007/s00417-018-4056-z
25. Campi I, Vannucchi GM, Minetti AM, Pignataro L, Beck-Peccoz P, Salvi M. A quantitative method for assessing the degree of axial proptosis in relation to orbital tissue involvement in graves’ Orbitopathy. Ophthalmology (2013) 120(5):1092–8. doi: 10.1016/j.ophtha.2012.10.041
26. Chaganti S, Nelson K, Mundy K, Luo Y, Harrigan RL, Damon S, et al. Structural functional associations of the orbit in thyroid eye disease: kalman filters to track extraocular rectal muscles. Spie-Int Soc Optical Eng (2016) 9784. doi: 10.1117/12.2217299
27. Chaganti S, Nelson K, Mundy K, Harrigan R, Galloway R, Mawn LA, et al. Imaging biomarkers in thyroid eye disease and their clinical associations. J Med Imag (2018) 5(4):44001. doi: 10.1117/1.jmi.5.4.044001
28. Chaganti S, Mundy K, DeLisi MP, Nelson KM, Harrigan RL, Galloway RL, et al. Assessment of orbital computed tomography (CT) imaging biomarkers in patients with thyroid eye disease. J Digital Imag (2019) 32(6):987–94. doi: 10.1007/s10278-019-00195-2
29. Chen YL, Chang TC, Huang KM, Tzeng SS, Kao SCS. Relationship of eye movement to computed tomographic findings in patients with Graves’ ophthalmopathy. Acta Ophthalmologica (1994) 72(4):472–7. doi: 10.1111/j.1755-3768.1994.tb02800.x
30. Choi KJ, Lee MJ. Comparison of exophthalmos measurements: Hertel exophthalmometer versus orbital parameters in 2-dimensional computed tomography. Can J Ophthalmology-Journal Canadien D Ophtalmologie (2018) 53(4):384–90. doi: 10.1016/j.jcjo.2017.10.015
31. Choudhary MM, Zhang KR, Johnson S, Hwang CJ, Chon BH, Perry JD. Temporal fat pad volume in patients with thyroid eye disease. Ophthalmic Plast Reconstr Surg (2020) 36(2):194–7. doi: 10.1097/iop.0000000000001511
32. Dagi LR, Zoumalan CI, Konrad H, Trokel SL, Kazim M. Correlation between extraocular muscle size and motility restriction in thyroid eye disease. Ophthalmic Plast Reconstr Surg (2011) 27(2):102–10. doi: 10.1097/IOP.0b013e3181e9a063
33. Dorić I, Žarković M, Radojičić Z, Repac N, Janićijević A, Rotim K, et al. The value of multidetector computed tomography of orbits in globe protrusion in comparison to hertel exophthalmometry. Acta Clinica Croatica (2017) 56(1):21–7. doi: 10.20471/acc.2017.56.01.04
34. Fang ZJ, Zhang JY, He WM. CT features of exophthalmos in Chinese subjects with thyroid-associated ophthalmopathy. Int J Ophthalmol (2013) 6(2):146–9. doi: 10.3980/j.issn.2222-3959.2013.02.07
35. Feldon SE, Weiner JM. Clinical significance of extraocular muscle volumes in graves’ Ophthalmopathy: A quantitative computed tomography study. Arch Ophthalmol (1982) 100(8):1266–9. doi: 10.1001/archopht.1982.01030040244006
36. Feldon SE, Lee CP, Muramatsu SK, Weinar JM. Quantitative computed tomography of graves’ Ophthalmopathy: extraocular muscle and orbital fat in development of optic neuropathy. Arch Ophthalmol (1985) 103(2):213–5. doi: 10.1001/archopht.1985.01050020065021
37. Fledelius HC, Nielsen H. Graves’ orbitopathy: Clinical features and imaging results, by ultrasound and CT-scan. Orbit (1990) 9(4):235–40. doi: 10.3109/01676839009019290
38. Forbes G, Gorman CA, Gehring D, Baker HL Jr. Computer analysis of orbital fat and muscle volumes in Graves ophthalmopathy. Am J Neuroradiol (1983) 4(3):737–40.
39. Giaconi JA, Kazim M, Rho T, Pfaff C. CT scan evidence of dysthyroid optic neuropathy. Ophthalmic Plast Reconstructive Surg (2002) 18(3):177–82. doi: 10.1097/00002341-200205000-00005
40. Givenwilson R, Pope RM, Michell MJ, Cannon R, McGregor AM. The use of real-time orbital ultrasound in graves ophthalmopathy - A comparison with computed-tomography. Br J Radiol (1989) 62(740):705–9. doi: 10.1259/0007-1285-62-740-705
41. Wing SD, Hunsaker JN, Anderson RE, Van Dyk HJ, Osborn AG. Direct sagittal computed tomography in Graves’ ophthalmopathy. J Comput Assist Tomogr (1979) 3(6):820–4. doi: 10.1097/00004728-197912000-00020
42. Gonçalves ACP, Silva LN, Gebrim EMMS, Monteiro MLR. Quantification of orbital apex crowding for screening of dysthyroid optic neuropathy using multidetector CT. AJNR Am J Neuroradiol (2012) 33(8):1602–7. doi: 10.3174/ajnr.A3029
43. Gonçalves AC, Silva LN, Gebrim EMMS, Matayoshi S, Monteiro MLR. Predicting dysthyroid optic neuropathy using computed tomography volumetric analyses of orbital structures. Clinics (Sao Paulo) (2012) 67(8):891–6. doi: 10.6061/clinics/2012(08)06
44. Guo J, Qian J, Yuan Y. Computed tomography measurements as a standard of exophthalmos? Two-dimensional versus three-dimensional techniques. Curr Eye Res (2018) 43(5):647–53. doi: 10.1080/02713683.2018.1431285
45. Goodall KL, Jackson A, Leatherbarrow B, Whitehouse RW. Enlargement of the tensor intermuscularis muscle in graves’ Ophthalmopathy: A computed tomographic and magnetic resonance imaging study. Arch Ophthalmol (1995) 113(10):1286–9. doi: 10.1001/archopht.1995.01100100074032
46. Harris MA, Realini T, Hogg JP, Sivak-Callcott JA. CT dimensions of the lacrimal gland in Graves orbitopathy. Ophthalmic Plast Reconstr Surg (2012) 28(1):69–72. doi: 10.1097/IOP.0b013e31823c4a3a
47. Huh J, Park SJ, Lee JK. Measurement of proptosis using computed tomography based three-dimensional reconstruction software in patients with Graves’ orbitopathy. Sci Rep (2020) 10(1):14554. doi: 10.1038/s41598-020-71098-4
48. Kim HC, Yoon SW, Lew H. Usefulness of the ratio of orbital fat to total orbit area in mild-to-moderate thyroid-associated ophthalmopathy. Br J Radiol (2015) 88(1053):20150164. doi: 10.1259/bjr.20150164
49. Lee JY, Bae K, Park KA, Lyu IJ, Oh SY. Correlation between extraocular muscle size measured by computed tomography and the vertical angle of deviation in thyroid eye disease. PloS One (2016) 11(1):e0148167. doi: 10.1371/journal.pone.0148167
50. Le Moli R, Pluchino A, Muscia V, Regalbuto C, Luciani B, Squatrito S, et al. Graves’ orbitopathy: extraocular muscle/total orbit area ratio is positively related to the Clinical Activity Score. Eur J Ophthalmol (2012) 22(3):301–8. doi: 10.5301/ejo.5000018
51. Monteiro MLR, Gonçalves ACP, Silva CTM, Moura JP, Ribeiro CS, Gebrim EMMS. Diagnostic ability of Barrett’s index to detect dysthyroid optic neuropathy using multidetector computed tomography. Clinics (Sao Paulo) (2008) 63(3):301–6. doi: 10.1590/s1807-59322008000300003
52. Murakami Y, Kanamoto T, Tuboi T, Maeda T, Inoue Y. Evaluation of extraocular muscle enlargement in dysthyroid ophthalmopathy. Japanese J Ophthalmol (2001) 45(6):622–7. doi: 10.1016/s0021-5155(01)00407-5
53. Nugent RA, Belkin RI, Neigel JM, Rootman J, Robertson WD, Spinelli J, et al. Graves orbitopathy: correlation of CT and clinical findings. Radiology (1990) 177(3):675–82. doi: 10.1148/radiology.177.3.2243967
54. Ozgen A, Alp MN, Ariyürek M, Tütüncü NB, Can I, Günalp I. Quantitative CT of the orbit in Graves’ disease. Br J Radiol (1999) 72(860):757–62. doi: 10.1259/bjr.72.860.10624341
55. Polito E, Leccisotti A. MRI in Graves orbitopathy: recognition of enlarged muscles and prediction of steroid response. Ophthalmologica (1995) 209(4):182–6. doi: 10.1159/000310609
56. Potgieser PW, Win MMML, Wiersinga WM, Mourits MP. Natural course of mild graves orbitopathy: increase of orbital fat but decrease of muscle volume with increased muscle fatty degeneration during a 4-year follow-up. Ophthalmic Plast Reconstr Surg (2019) 35(5):456–60. doi: 10.1097/iop.0000000000001319
57. Regensburg NI, Wiersinga WM, Berendschot TTJM, Saeed P, Mourits MP. Densities of orbital fat and extraocular muscles in graves orbitopathy patients and controls. Ophthalmic Plast Reconstructive Surg (2011) 27(4):236–40. doi: 10.1097/IOP.0b013e31820365d5
58. Starks VS, Reinshagen KL, Lee NG, Freitag SK. Visual field and orbital computed tomography correlation in dysthyroid optic neuropathy due to thyroid eye disease. Orbit-the Int J Orbital Disorders-Oculoplastic Lacrimal Surg (2020) 39(2):77–83. doi: 10.1080/01676830.2019.1600150
59. Thornton IL, Clark J, Sokol JA, Hite M, Nunnery WR. Radiographic evidence of prominent retro and suborbicularis oculi fat in thyroid-associated orbitopathy. Orbit-an Int J Orbital Disord Facial Reconstructive Surg (2016) 35(1):35–8. doi: 10.3109/01676830.2015.1099689
60. Ugradar S, Rootman DB. Quantification of optic nerve length and tortuosity in thyroid eye disease. Can J Ophthalmol (2019) 54(5):611–4. doi: 10.1016/j.jcjo.2019.01.007
61. Antoniazzi F, Zamboni G, Cerini R, Lauriola S, Dall’Agnola A, Tatò L. Graves ophthalmopathy evolution studied by MRI during childhood and adolescence. J Pediatr (2004) 144(4):527–31. doi: 10.1016/j.jpeds.2004.01.033
62. Aydin K, Güven K, Sencer S, Cıkım A, Gül N, Minareci O. A new MRI method for the quantitative evaluation of extraocular muscle size in thyroid ophthalmopathy. Neuroradiology (2003) 45(3):184–7. doi: 10.1007/s00234-002-0930-8
63. Bontzos G, Papadaki E, Mazonakis M, Maris GT, Kapsala Z, Blazaki S, et al. Quantification of effective orbital volume and its association with axial length of the eye. A 3D-MRI study Rom J Ophthalmol (2019) 63(4):360–6.
64. Cakirer S, Cakirer D, Basak M, Durmaz S, Altuntas Y, Yigit U. Evaluation of extraocular muscles in the edematous phase of graves ophthalmopathy on contrast-enhanced fat-suppressed magnetic resonance imaging. J Comput Assisted Tomogr (2004) 28(1):80–6. doi: 10.1097/00004728-200401000-00013
65. Cevik Y, Sekeroglu HT, Ozgen B, Turan KE, Sanac AS. Clinical and radiological findings in patients with newly diagnosed graves’ Ophthalmopathy. Int J Endocrinol (2021) 2021:1–7. doi: 10.1155/2021/5513008
66. Chen HH, Hu H, Chen W, Cui D, Xu XQ, Wu FY, et al. Thyroid-associated orbitopathy: evaluating microstructural changes of extraocular muscles and optic nerves using readout-segmented echo-planar imaging-based diffusion tensor imaging. Korean J Radiol (2020) 21(3):332–40. doi: 10.3348/kjr.2019.0053
67. Chen L, Chen W, Chen H-H, Wu Q, Xu X-Q, Hu H, et al. Radiological staging of thyroid-associated ophthalmopathy: comparison of T1 mapping with conventional MRI. Int J Endocrinol (2020) 2020:1–6. doi: 10.1155/2020/2575710
68. Chen W, Hu H, Chen H-H, Su G-Y, Yang T, Xu X-Q, et al. Utility of T2 mapping in the staging of thyroid-associated ophthalmopathy: efficiency of region of interest selection methods. Acta Radiologica (2020) 61(11):1512–1519. 0284185120905032. doi: 10.1177/0284185120905032
69. Chen L, Hu H, Chen W, Wu Q, Zhou J, Chen H-H, et al. Usefulness of readout-segmented EPI-based diffusion tensor imaging of lacrimal gland for detection and disease staging in thyroid-associated ophthalmopathy. BMC Ophthalmol (2021) 21(1):281. doi: 10.1186/s12886-021-02044-9
70. Comerci M, Elefante A, Strianese D, Senese R, Bonavolontà P, Alfano B, et al. Semiautomatic regional segmentation to measure orbital fat volumes in thyroid-associated ophthalmopathy. A validation study. Neuroradiol J (2013) 26(4):373–9. doi: 10.1177/197140091302600402
71. Dodds NI, Atcha AW, Birchall D, Jackson A. Use of high-resolution MRI of the optic nerve in Graves’ ophthalmopathy. Br J Radiol (2009) 82(979):541–4. doi: 10.1259/bjr/56958444
72. Firbank MJ, Coulthard A. Evaluation of a technique for estimation of extraocular muscle volume using 2D MRI. Br J Radiol (2000) 73(876):1282–9. doi: 10.1259/bjr.73.876.11205672
73. Gagliardo C, Radellini S, Morreale Bubella R, Falanga G, Richiusa P, Vadalà M, et al. Lacrimal gland herniation in Graves ophthalmopathy: a simple and useful MRI biomarker of disease activity. Eur Radiol (2020) 30(4):2138–41. doi: 10.1007/s00330-019-06570-5
74. Han JS, Seo HS, Lee YH, Lee H, Suh S, Jeong E-K, et al. Fractional anisotropy and diffusivity changes in thyroid-associated orbitopathy. Neuroradiology (2016) 58(12):1189–96. doi: 10.1007/s00234-016-1764-0
75. Hiwatashi A, Togao O, Yamashita K, Kikuchi K, Momosaka D, Honda H. Diffusion-weighted magnetic resonance imaging of extraocular muscles in patients with Grave’s ophthalmopathy using turbo field echo with diffusion-sensitized driven-equilibrium preparation. Diagn Interventional Imag (2018) 99(7-8):457–63. doi: 10.1016/j.diii.2018.02.007
76. Hosten N, Sander B, Cordes M, Schubert CJ, Schörner W, Felix R. Graves ophthalmopathy: MR imaging of the orbits. Radiology (1989) 172(3):759–62. doi: 10.1148/radiology.172.3.2772184
77. Hu H, Xu X-Q, Wu F-Y, Chen H-H, Su G-Y, Shen J, et al. Diagnosis and stage of Graves’ ophthalmopathy: Efficacy of quantitative measurements of the lacrimal gland based on 3-T magnetic resonance imaging. Exp Ther Med (2016) 12(2):725–9. doi: 10.3892/etm.2016.3389
78. Jiang H, Wang Z, Xian J, Li J, Chen Q, Ai L. Evaluation of rectus extraocular muscles using dynamic contrast enhanced MR imaging in patients with Graves’ ophthalmopathy for assessment of disease activity. Acta Radiologica (2012) 53(1):87–94. doi: 10.1258/ar.2011.110431
79. Kaichi Y, Tanitame K, Terada H, Itakura H, Ohno H, Yoneda M, et al. Thyroid-associated orbitopathy: quantitative evaluation of the orbital fat volume and edema using IDEAL-FSE. Eur J Radiol Open (2019) 6:182–6. doi: 10.1016/j.ejro.2019.05.003
80. Keene KR, Vught L, Velde NM, Ciggaar IA, Notting IC, Genders SW, et al. The feasibility of quantitative MRI of extraocular muscles in myasthenia gravis and Graves’ orbitopathy. NMR Biomed (2021) 34(1):1–11. doi: 10.1002/nbm.4407
81. Khan TP, Qayyum S, Abbas Q, Arshad M, Arshad Z. Pathophysiology changes in extraocular muscles in thyroid eye disease: ophthalmic and radiological correlation in our population. Pakistan J Med Health Sci (2020) 14(4):1226–7.
82. Kilicarslan R, Alkan A, Ilhan MM, Yetis H, Aralasmak A, Tasan E. Graves’ ophthalmopathy: the role of diffusion-weighted imaging in detecting involvement of extraocular muscles in early period of disease. Br J Radiol (2015) 88(1047):20140677. doi: 10.1259/bjr.20140677
83. Kirsch E, Kaim AH, De Oliveira MG, von Arx GG. Correlation of signal intensity ratio on orbital MRI-TIRM and clinical activity score as a possible predictor of therapy response in graves’ orbitopathy-a pilot studyat 1. 5 t. Neuroradiol (2011) 53:S99. doi: 10.1007/s00234-011-0913-8
84. Kvetny J, Puhakka KB, Rohl L. Magnetic resonance imaging determination of extraocular eye muscle volume in patients with thyroid-associated ophthalmopathy and proptosis. Acta Ophthalmologica Scandinavica (2006) 84(3):419–23. doi: 10.1111/j.1600-0420.2005.00617.x
85. Lee H, Lee YH, Suh S, Jeong E-K, Baek S, Seo HS. Characterizing intraorbital optic nerve changes on diffusion tensor imaging in thyroid eye disease before dysthyroid optic neuropathy. J Comput Assisted Tomogr (2018) 42(2):293–8. doi: 10.1097/rct.0000000000000680
86. Lennerstrand G, Tian S, Isberg B, Landau Högbeck I, Bolzani R, Tallstedt L, et al. Magnetic resonance imaging and ultrasound measurements of extraocular muscles in thyroid-associated ophthalmopathy at different stages of the disease. Acta Ophthalmologica Scandinavica (2007) 85(2):192–201. doi: 10.1111/j.1600-0420.2006.00807.x
87. Majos A, Grzelak P, Młynarczyk W, Stefańczyk L. Eyeball muscles’ diameters versus volume estimated by numerical image segmentation. Eur J Ophthalmol (2007) 17(3):287–93. doi: 10.1177/112067210701700302
88. Majos A, Grzelak P, Młynarczyk W, Stefańczyk L. Numerical segmentation image technique (NSI) in estimation of extraocular muscles volume in Graves’ ophthalmology. Polish J Radiol (2007) 72(2):75–81.
89. Majos A, Grzelak P, Młynarczyk W, Stefańczyk L. Magnetic Resonance evaluation of disease activity in Graves’ ophthalmopathy: T2-time and signal intensity of extraocular muscles. Med Sci Monit (2007) 13 Suppl 1:44–8.
90. Matsuzawa K, Izawa S, Kato A, Fukaya K, Matsumoto K, Okura T, et al. Low signal intensities of MRI T1 mapping predict refractory diplopia in Graves’ ophthalmopathy. Clin Endocrinol (2020) 92(6):536–44. doi: 10.1111/cen.14178
91. Nishida Y, Tian S, Isberg B, Tallstedt L, Lennerstrand G. MRI measurements of orbital tissues in dysthyroid ophthalmopathy. Graefes Arch Clin Exp Ophthalmol (2001) 239(11):824–31. doi: 10.1007/s004170100352
92. Nishida Y, Tian S, Isberg B, Hayashi O, Tallstedt L, Lennerstrand G. Significance of orbital fatty tissue for exophthalmos in thyroid-associated ophthalmopathy. Graefes Arch Clin Exp Ophthalmol (2002) 240(7):515–20. doi: 10.1007/s00417-002-0498-3
93. Ohnishi T, Noguchi S, Murakami N, Nakahara H, Hoshi H, Jinnouchi S, et al. Levator palpebrae superioris muscle: MR evaluation of enlargement as a cause of upper eyelid retraction in Graves disease. Radiology (1993) 188(1):115–8. doi: 10.1148/radiology.188.1.8511284
94. Ohnishi T, Noguchi S, Murakami N, Tajiri J, Harao M, Kawamoto H, et al. Extraocular muscles in Graves ophthalmopathy: usefulness of T2 relaxation time measurements. Radiology (1994) 190(3):857–62. doi: 10.1148/radiology.190.3.8115640
95. Ollitrault A, Charbonneau F, Herdan M-L, Bergès O, Zuber K, Giovansili L, et al. Dixon-T2WI magnetic resonance imaging at 3 tesla outperforms conventional imaging for thyroid eye disease. Eur Radiol (2021) 31(7):5198–205. doi: 10.1007/s00330-020-07540-y
96. Ozkan B, Anik Y, Katre B, Altintaş Ö, Gençtürk M, Yüksel N. Reply re: “quantitive assessment of optic nerve with diffusion tensor imaging in patients with thyroid orbitopathy”. Ophthalmic Plast Reconstructive Surgery (2015) 31(6):486–7. doi: 10.1097/IOP.0000000000000551
97. Politi LS, Godi C, Cammarata G, Ambrosi A, Iadanza A, Lanzi R, et al. Magnetic resonance imaging with diffusion-weighted imaging in the evaluation of thyroid-associated orbitopathy: getting below the tip of the iceberg. Eur Radiol (2014) 24(5):1118–26. doi: 10.1007/s00330-014-3103-3
98. Razek AAA, El-Hadidy M, Moawad MR, El-Metwaly N, El-Said AA. Performance of apparent diffusion coefficient of medial and lateral rectus muscles in Graves’ orbitopathy. Neuroradiol J (2017) 30(3):230–4. doi: 10.1177/1971400917691993
99. Razek AAA, El-Hadidy M, Moawad MR, El-Metwaly N, El-Said AA. Assessment of lacrimal glands in thyroid eye disease with diffusion-weighted magnetic resonance imagin. Polish J Radiol (2019) 84:e142–6. doi: 10.5114/pjr.2019.84096
100. Rodríguez-González N, Pérez-Rico C, López-Para Giménez R, Arévalo-Serrano J, Del Amo García B, Calzada Domingo L, et al. Short-tau inversion-recovery (STIR) sequence magnetic resonance imaging evaluation of orbital structures in Graves’ orbitopathy. Archivos la Sociedad Espanola Oftalmologia (2011) 86(11):351–7. doi: 10.1016/j.oftal.2011.06.010
101. Rutkowska-Hinc B, Maj E, Jabłońska A, Milczarek-Banach J, Bednarczuk T, Miśkiewicz P, et al. Prevalence of radiological signs of dysthyroid optic neuropathy in magnetic resonance imaging in patients with active, moderate-to-severe, and very severe graves orbitopathy. Eur Thyroid J (2018) 7(2):88–94. doi: 10.1159/000486828
102. Shen J, Jiang W, Luo Y, Cai Q, Li Z, Chen Z, et al. Establishment of magnetic resonance imaging 3D reconstruction technology of orbital soft tissue and its preliminary application in patients with thyroid-associated ophthalmopathy. Clin Endocrinol (2018) 88(5):637–44. doi: 10.1111/cen.13564
103. Silkiss RZ, Wade AR. Neuroanatomic variations in graves’ dysthyroid ophthalmopathy as studied with MRI. Trans Am Ophthalmological Soc (2016) 114:T9–1-T9-10.
104. So NM, Lam WW, Cheng G, Metreweli C, Lam D. Assessment of optic nerve compression in Graves’ ophthalmopathy - The usefulness of a quick T1-weighted sequence. Acta Radiologica (2000) 41(6):559–61. doi: 10.1080/028418500127346207
105. Szucs-Farkas Z, Toth J, Balazs E, Galuska L, Burman KD, Karanyi Z, et al. Using morphologic parameters of extraocular muscles for diagnosis and follow-up of Graves’ ophthalmopathy: diameters, areas, or volumes? AJR Am J Roentgenol (2002) 179(4):1005–10. doi: 10.2214/ajr.179.4.1791005
106. Taoka T, Sakamoto M, Nakagawa H, Fukusumi A, Iwasaki S, Taoka K, et al. Evaluation of extraocular muscles using dynamic contrast enhanced MRI in patients with chronic thyroid orbitopathy. J Comput Assist Tomogr (2005) 29(1):115–20. doi: 10.1097/01.rct.0000146112.56194.24
107. Tortora F, Cirillo M, Ferrara M, Belfiore MP, Carella C, Caranci F, et al. Disease activity in Graves’ ophthalmopathy: diagnosis with orbital MR imaging and correlation with clinical score. Neuroradiol J (2013) 26(5):555–64. doi: 10.1177/197140091302600509
108. Troelstra A, Rijnevekd WJ, Kooijman AC, Houtman WA. Correlation between NMR scans of extraocular muscles and clinical symptoms in Graves’ ophthalmopathy. Documenta Ophthalmologica (1988) 70(2-3):243–9. doi: 10.1007/BF00154461
109. Wu D, Zhu H, Hong S, Li B, Zou M, Ma X, et al. Utility of multi-parametric quantitative magnetic resonance imaging of the lacrimal gland for diagnosing and staging Graves’ ophthalmopathy. Eur J Radiol (2021) 141:109815. doi: 10.1016/j.ejrad.2021.109815
110. Wu H, Luo B, Yuan G, Wang Q, Liu P, Zhao Y, et al. The diagnostic value of the IDEAL-T2WI sequence in dysthyroid optic neuropathy: a quantitative analysis of the optic nerve and cerebrospinal fluid in the optic nerve sheath. Eur Radiol (2021) 31(10):7419–28. doi: 10.1007/s00330-021-08030-5
111. Davies TF, Andersen S, Latif R, Nagayama Y, Barbesino G, Brito M, et al. Graves’ disease. Nat Rev Dis Primers (2020) 6(1):52. doi: 10.1038/s41572-020-0184-y
Keywords: Graves’ ophthalmopathy, Graves’ disease, imaging analysis, magnetic resonance imaging, computed tomography
Citation: Luccas R, Riguetto CM, Alves M, Zantut-Wittmann DE and Reis F (2024) Computed tomography and magnetic resonance imaging approaches to Graves’ ophthalmopathy: a narrative review. Front. Endocrinol. 14:1277961. doi: 10.3389/fendo.2023.1277961
Received: 15 August 2023; Accepted: 12 December 2023;
Published: 08 January 2024.
Edited by:
Terry Francis Davies, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Jeehee Yoon, Chonnam National University Bitgoeul Hospital, Republic of KoreaCopyright © 2024 Luccas, Riguetto, Alves, Zantut-Wittmann and Reis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabiano Reis, ZmFiaWFub3JlaXMyQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.