 Jeffrey R. Garber
Jeffrey R. Garber Andrea Frasoldati
Andrea Frasoldati Vivek Patkar
Vivek Patkar Enrico Papini
Enrico Papini
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
EDITORIAL article
Front. Endocrinol., 05 September 2023
Sec. Thyroid Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1276323
This article is part of the Research TopicThyroid Nodule Evaluation: Current, Evolving, and Emerging ToolsView all 16 articles
Editorial on the Research Topic
Thyroid nodule evaluation: current, evolving, and emerging tools
Thyroid nodules are common, predominantly benign, asymptomatic on presentation, and most often remain so (Uppal et al.) (1). Moreover, those that are malignant are principally small low-risk neoplasms with an indolent course and minimal impact on survival (2). Hence, most patients do not benefit from extensive evaluation, treatment, and monitoring (2–5). On the contrary, costly diagnostic techniques and treatment may have a detrimental impact on a patient’s physical, emotional, and financial status (Uppal et al.). In the United States well over 500 000 fine-needle aspirations (FNAs) of thyroid nodules are performed yearly with as many as 40% likely unnecessary (6). In European countries, such as Germany and France, as well as well as in the United States, overtreatment is reflected by most thyroidectomies performed for nodular thyroid disease prove to be for benign disease while the minority that are malignant are principally comprised of low-risk thyroid cancers (7). Recommendations from professional societies such as the American Association of Clinical Endocrinologists (AACE), Associazione Medici Endocrinologi (AME) (2), American Thyroid Association (ATA) (3), European Thyroid Association (ETA) (4), and American College of Radiology (5) for reducing the collective burden of evaluating and treating thyroid nodules and low risk thyroid cancers have had limited impact on achieving this goal (6).
Over the past 3 decades narrative or written clinical practice guidelines (CPGs) have emerged as an increasingly important tool to aid clinicians in managing a host of medical conditions. Guidelines are regularly cited in publications and medical education forums and used as a basis for medical decision making in both clinical and administrative settings. Yet, despite their widespread clinical use, there is substantial room for improvement in the following ways:
● Establishing the cost effectiveness and validity of recommendations, which are often based on expert opinion, retrospective studies, and study populations that are not generalizable.
● Evaluating their impact on patient quality of life
● Routinely disseminating, distributing, and implementing guidelines
● Gauging their implementation by tracking their use and applicability
● Creating mechanisms for vetting guideline recommendations in various clinical situations and across different populations and cultures
● Addressing their often-formidable length and the wealth of information they contain, which makes them hard for physicians to navigate as well as absorb and retain (internalize)
● Providing timely updates of narrative multi-authored, highly validated documents
Advanced Clinical Decisions Support Systems (CDSS) addresses all the above-mentioned points by transforming CPGs into computer interpretable guidelines (CIGs). CIGs are derived from CPGs. They employ execution engines (programs) to analyze patient-specific data to electronically generate, document, and track recommendations (Garber and Patkar).
The articles in this Research Topic of Frontiers in Endocrinology are written by a diverse group of authors representing various specialties and regions. They cover the gamut of tools available for evaluating thyroid nodules. They also underscore the challenges in developing a streamlined, cost-effective approach that minimizes unnecessary evaluation and intervention that not only does not benefit patients but may harm them while maximizing the chances for identifying clinically significant disease that if left untreated would lead to significant morbidity.
The diagnostic tools available to clinicians caring for patients with thyroid nodules can be summarized in Table 1. Over time, history and physical examination have taken on a marginal role in evaluating thyroid nodules. This is due to several reasons. Many nodules are discovered incidentally on imaging that is not being performed to evaluate the thyroid gland. Since physical examination is not as reliable as ultrasound in establishing the presence, size, or characteristics of benign or malignant disease it is less frequently or carefully performed. Thus, it is not regularly used to follow patients with benign, inconsequential nodularity. This is not without a downside. Greater reliance on ultrasound as a monitoring tool and to facilitate fine needle aspiration of a candidate nodule leads to surveying the remainder of the thyroid gland for nodularity. While improving the yield and accuracy of fine needle aspiration, ultrasound often leads to the detection and evaluation of clinically inapparent nodules that are either diagnostically indeterminate or an inconsequential malignancy, resulting in surgery without clear benefit.
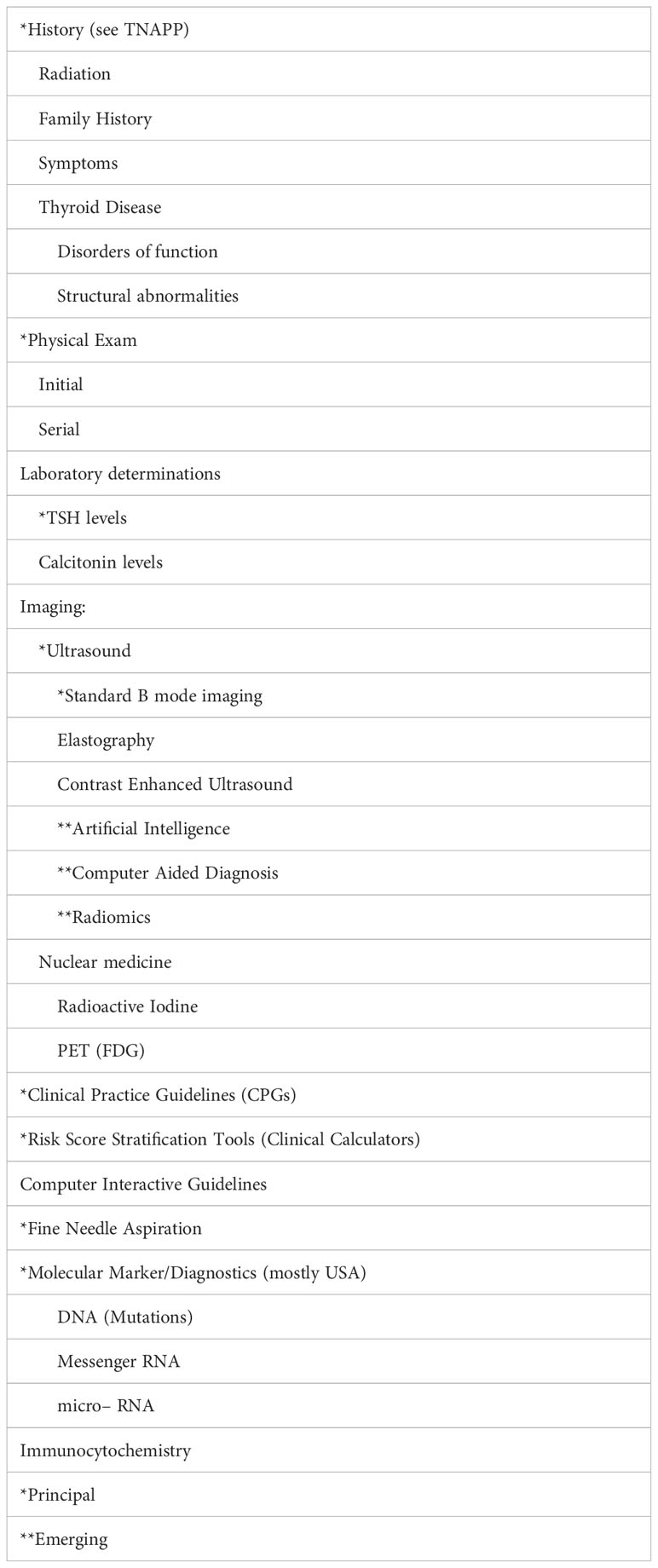
Table 1 Diagnostic Tools.
The current emphasis on evaluating thyroid nodules in addition to standard B-mode ultrasonography, are risk stratification tools such as ACR TIRADS, fine needle aspiration with Bethesda classification and molecular genetic markers (Patel et al.), where available. Additional tools that have not yet been standardized, widely adapted, or extensively studied, include ultrasound elastography (Li et al.), contrast enhanced ultrasound (Zhou et al.), emerging AI tools (Xu D. et al.) (8), and immunocytochemistry (Crescenzi and Baloch; Taccogna et al.). On a positive note, therapeutic advances promoted by professional societies (9–12) employing minimally invasive ablation procedures have been made. These techniques are being used more frequently. Compared with surgery, they are less expensive, cause less morbidity, and have fewer adverse effects on patient quality of life.
Challenges, however, remain. Tools for assessing risk vary, employing different characteristics underpinning a strong argument for universally accepted risk stratification tools (Majety et al.) (13, 14). Oftentimes, newer technology is complementary rather than substitutive, increasing cost without offering consistently substantial benefit (Uppal et al.). Yet reliable, relatively expensive, new AI tools may ultimately play a key role in resource poor regions that not only lack access to diagnostic tools, but do not have the professional expertise to interpret ultrasound (8).
A promising new development strongly supported by the editors of this Research Topic is the adaptation of CIGs to complement and facilitate the use of clinical practice guidelines and risk stratification systems. Using advanced CDSS to co–develop CIGs that complement conventional society guidelines, may not only increase the use of CPGs, but could serve as testing tools for assessing the efficacy and generalizability of a sequence of diagnostic tests (Triggiani et al.) (15). This could be accomplished by employing a range of assumptions and models for the respective sensitivity, specificity, accuracy, and costs of each tool being employed.
Our challenge is improving our approach to evaluating and managing thyroid nodules by increasingly employing minimally invasive techniques, and developing more specific, less costly molecular tests that not only diagnose malignancy but also provide prognostic information. Doing so will substantially reduce the number of preventable adverse effects of invasive diagnostic and non–surgical therapeutic procedures, surgical morbidity, and financial toxicity at the expense of only detecting the relatively small percentage that prove to be thyroid cancers that require treatment.
JG: Writing – original draft, Writing – review & editing. AF: Writing – review & editing, Writing – original draft. VP: Writing – review & editing. EP: Writing – review & editing.
VP is CMO of Deontics Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Durante C, Costante G, Lucisano G, Bruno R, Meringolo D, Paciaroni A, et al. The natural history of benign thyroid nodules. JAMA (2015) 313(9):926–35. doi: 10.1001/jama.2015.0956
2. Gharib H, Papini E, Garber JR, Duick DS, Harrell RM, Hegedüs L, et al. AACE/ACE/AME task force on thyroid nodules. American association of clinical endocrinologists, american college of endocrinology, and associazione medici endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules–2016 update. Endocr Pract (2016) 22(5):622–39. doi: 10.4158/EP161208.GL
3. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid (2016) 26(1):1–133. doi: 10.1089/thy.2015.0020
4. Durante C, Hegedus L, Czarniecka A, Paschke R, Russ G, Schmitt F, et al. 2023 European Thyroid Association clinical practice guidelines for thyroid nodule management. Eur Thyroid J (2023) 12(5):e230067. doi: 10.1530/ETJ–23–0067
5. Tessler FN, Middleton WD, Grant EG, Hoang JK, Berland LL, Teefey SA, et al. ACR thyroid imaging, reporting and data system (TI–RADS): white paper of the ACR TI–RADS committee. J Am Coll Radiol (2017) 14(5):587–95. doi: 10.1016/j.jacr.2017.01.046
6. White C, Weinstein MC, Fingeret AL, Randolph GW, Miyauchi A, Ito Y, et al. Is less more? A microsimulation model comparing cost–effectiveness of the revised american thyroid association’s 2015 to 2009 guidelines for the management of patients with thyroid nodules and differentiated thyroid cancer. Ann Surg (2020) 271(4):765–73. doi: 10.1097/SLA.0000000000003074
7. Bartsch DK, Dotzenrath C, Vorländer C, Zielke A, Weber T, Buhr HJ, et al. The stuDoQ/thyroid study group TSS. Current practice of surgery for benign goitre–an analysis of the prospective DGAV stuDoQ|Thyroid registry. J Clin Med (2019) 8(4):477. doi: 10.3390/jcm8040477
8. Tessler FN, Thomas J. Artificial intelligence for evaluation of thyroid nodules: A primer. Thyroid (2023) 33(2):150–8. doi: 10.1089/thy.2022.0560
9. Perros P, Hegedüs L, Nagy EV, Papini E, Hay HA, Abad–Madroñero J, et al. The impact of hypothyroidism on satisfaction with care and treatment and everyday living: results from E–mode patient self–assessment of thyroid therapy, a cross–sectional, international online patient survey. Thyroid (2022) 32(10):1158–68. doi: 10.1089/thy.2022.0324
10. Papini E, Monpeyssen H, Frasoldati A, Hegedüs L. 2020 European thyroid association clinical practice guideline for the use of image–guided ablation in benign thyroid nodules. Eur Thyroid J (2020) 9(4):172–85. doi: 10.1159/000508484
11. Orloff LA, Noel JE, Stack BC Jr, Russell MD, Angelos P, Baek JH, et al. Radiofrequency ablation and related ultrasound–guided ablation technologies for treatment of benign and Malignant thyroid disease: An international multidisciplinary consensus statement of the American Head and Neck Society Endocrine Surgery Section with the Asia Pacific Society of Thyroid Surgery, Associazione Medici Endocrinologi, British Association of Endocrine and Thyroid Surgeons, European Thyroid Association, Italian Society of Endocrine Surgery Units, Korean Society of Thyroid Radiology, Latin American Thyroid Society, and Thyroid Nodules Therapies Association. Head Neck (2022) 44(3):633–60. doi: 10.1002/hed.26960
12. Papini E, Hegedüs L. Minimally invasive ablative treatments for benign thyroid nodules: current evidence and future directions. Thyroid (2023) 30(8):890–3. doi: 10.1089/thy.2023.0263
13. Hoang JK, Asadollahi S, Durante C, Hegedüs L, Papini E, Tessler FN. An international survey on utilization of five thyroid nodule risk stratification systems: A needs assessment with future implications. Thyroid (2022) 32(6):675–81. doi: 10.1089/thy.2021.0558
14. Solymosi T, Hegedűs L, Bonnema SJ, Frasoldati A, Jambor L, Karanyi Z, et al. Considerable interobserver variation calls for unambiguous definitions of thyroid nodule ultrasound characteristics. Eur Thyroid J (2023) 12(2):e220134. doi: 10.1530/ETJ–22–0134
Keywords: thyroid nodule, clinical practice guideline, clinical calculators clinical decision support, computer interpretable guideline, evidence based care, guideline compliance, CDSS
Citation: Garber JR, Frasoldati A, Patkar V and Papini E (2023) Editorial: Thyroid nodule evaluation: current, evolving, and emerging tools. Front. Endocrinol. 14:1276323. doi: 10.3389/fendo.2023.1276323
Received: 11 August 2023; Accepted: 18 August 2023;
Published: 05 September 2023.
Edited and Reviewed by:
Terry Francis Davies, Icahn School of Medicine at Mount Sinai, United StatesCopyright © 2023 Garber, Frasoldati, Patkar and Papini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jeffrey R. Garber, amdhcmJlckBiaWRtYy5oYXJ2YXJkLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.