 Lídice Tavares Puglia1
Lídice Tavares Puglia1 Gianluca Tamagno
Gianluca Tamagno
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol. , 21 November 2023
Sec. Pituitary Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1269781
This article is part of the Research Topic Insights in Hyperprolactinemia View all 6 articles
Background: Vitex agnus castus (VAC), also known as chaste tree, is a plant from the Mediterranean area, Crimea, and central Asia. Its fruit has been used for more than 2500 years as phytotherapic agent. In the last century, VAC has been mostly used for the treatment of premenstrual syndrome (PMS), menstrual irregularities, fertility disorders, and symptoms of menopause. Since some degree of hyperprolactinaemia may be observed in patients with such disorders, VAC effects on hyperprolactinaemia have been assessed in a small number of studies and in some patient series or single case reports. It has been postulated that the diterpenes contained in VAC extract may interact with dopamine D2 receptors (D2R) and inhibit prolactin release via dopamine D2R activation in the anterior pituitary. Most of the published papers focus on the use of VAC for the management of PMS or infertility. However, due to its action on D2R, VAC could have a role in the treatment of mild hyperprolactinaemia, including patients with idiopathic hyperprolactinaemia, microprolactinoma, drug-induced hyperprolactinaemia, or polycystic ovary syndrome.
Methods: We have reviewed and analysed the data from the literature concerning the use of VAC extracts in patients with hyperprolactinaemia.
Results: Some evidence suggests a possible role of VAC for the management of hyperprolactinaemia in selected patients, though in an inhomogeneous way. However, there are not any large randomized controlled trials supporting the same and the precise pharmacological aspects of VAC extract in such a clinical setting still remain obscure.
Conclusion: It appears that VAC may represent a potentially useful and safe phytotherapic option for the management of selected patients with mild hyperprolactinaemia who wish to be treated with phytotherapy. However, larger studies of high quality are needed to corroborate it.
The genus Vitex comprises nearly 250 species distributed worldwide, mostly in the tropical and temperate zones (1). Several species, such as Vitex agnus castus (VAC), Vitex trifolia, Vitex negundo, and Vitex rotundifolia have been used as traditional medicinal plants. More than 20 Vitex species have been investigated with regard to their chemical and biological properties with nearly 200 compounds described so far (2).
VAC lamiaceae, formerly verbenaceae, is a deciduous tree or a large shrub native to central Asia and Mediterranean Europe. VAC is also known as chaste tree, chaste berry, or monk’s pepper. The dried fruits of VAC have been used for more than 2500 years for medicinal purposes, mostly for a variety of gynaecological conditions (3). In history, almost all VAC organs have been pharmacologically used and many contradictions have appeared with regard to VAC medicinal use even in modern times. In the late Middle Ages in Europe, the use of VAC was introduced also to celibate clerics for its supposed usefulness in reducing undesired sexual libido. After vanishing in the 19th century, the pharmacological use of VAC has reemerged in Europe in the last six decades as a treatment for some gynaecological conditions such as premenstrual syndrome (PMS), cyclical mastalgia, menstrual cycle irregularities, corpus luteum insufficiency, dysfunctional uterine bleeding, and some symptoms of menopause, such as hot flushes (3–8). A recent review established that there is a role for VAC in the treatment of polycystic ovary syndrome (PCOS) (9). In fact, VAC has been approved by the German Commission E for the treatment of irregularities of the menstrual cycle, cyclical mastalgia and PMS, and such medication can be prescribed by family physicians and gynaecologists in Germany (10, 11).
As hyperprolactinaemia can occur in these gynaecological conditions, we have assessed all studies that evaluated the role of VAC on prolactin (PRL) regardless of the study outcome.
Phytotherapic drugs contain a number of pharmacological properties acting through various mechanisms and pathways. The final result is a complex set of synergistic and antagonistic interactions operating at biochemical, cellular, and physiological level (12, 13). This is particularly relevant in the context of the increasing use of complementary and alternative medicine, with current rates of use ranging between 26% and 91% (14, 15). In the USA, sales increased by 6.8% in 2014 for the eleventh consecutive year (16). An European study reported that 18.8% of the population use at least one plant supplement (17). Systematic reviews and meta-analyses on phytotherapic products have increased in number and, in the last 4 years, a considerable number of manuscripts of consistent quality assessing the clinical effectiveness of herbal remedies have been published (18). Although the majority of the publications to date have come from Western countries, there has also been an increase in interest in this area in Asiatic countries (19–22).
To date, 24 distinct phytoconstituents have been isolated from the fruits of VAC, including 10 flavonoids, 5 terpenoids, 4 phenolic, 3 neolignans compounds, 1 glyceride, and 1 labdane-diterpene (23). Although the pharmacological mechanism of action of VAC has yet to be fully elucidated, its extract appears to act, at least in part, through the binding with estrogen receptors, dopamine receptors, and opiate receptors. These actions would result in changes to levels of PRL in the body, potentially leading to an improvement in the control of symptoms of menopause and PMS. More recent studies suggest a role for VAC extract in potentiating antioxidants in cancer chemoprevention and bone fracture healing. However, further research in this field is still ongoing (24–26).
Mild hyperprolactinaemia is a condition in which PRL is slightly increased and occurs for a variety of reasons, including also normal physiological response to stress in patients without a prolactinoma (Table 1) (27–29).
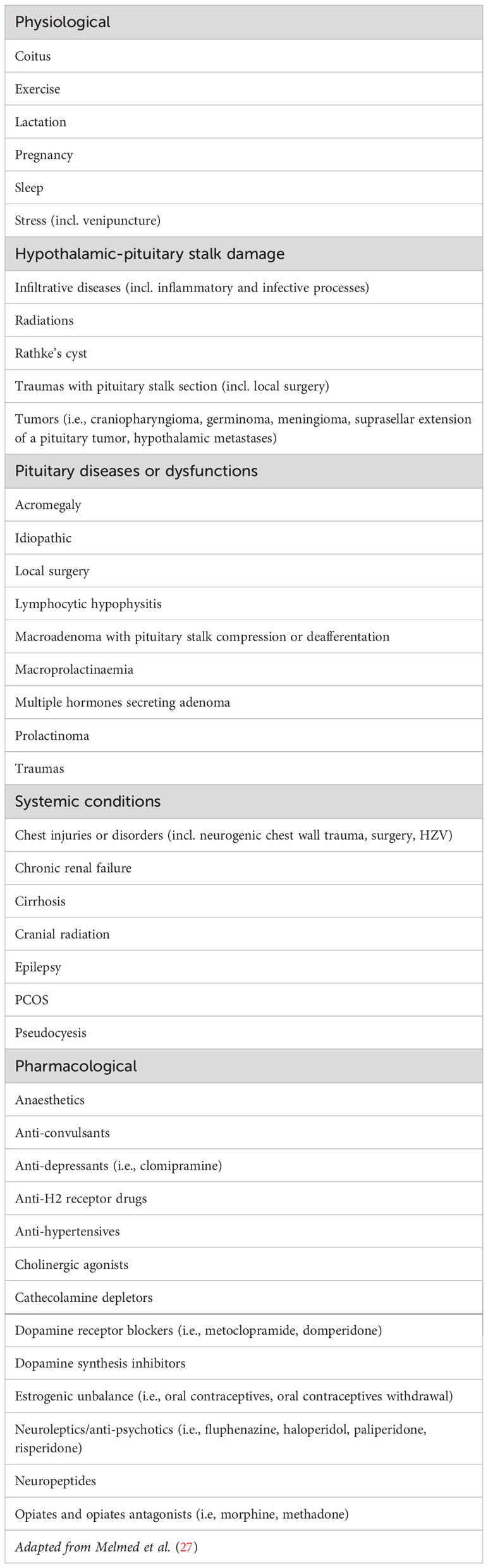
Table 1 Causes of hyperprolactinaemia.
PRL release from the pituitary is regulated by hypothalamic dopamine inhibition. Dopamine is secreted by the tuberoinfundibular dopaminergic neurons into the portal vessels that connect the hypothalamus with the pituitary. In the late luteal phase, women have a relative increase in serum PRL (28). Such an event is due to the decrease, to some extent, of the dopaminergic inhibition at the time of the premenstrual period (29). Increased PRL levels have been linked with mastalgia and some symptoms of PMS (30–34). One study showed that bromocriptine, a commercially available dopamine agonist, can improve breast pain and this was associated with a decrease in PRL levels (35). A study on the effects of lisuride, another dopamine agonist, demonstrated not only an improvement in symptoms of mastalgia but also on the psychological and somatic symptoms of PMS, including depression, sadness, irritability, emotional changes, and sensorial sensitivity (36). This suggests that multiple dopaminergic regions within the brain, such as the nigrostriatal and the mesolimbic system, play a role in PMS (29).
VAC exerts a central dopaminergic activity in vitro and in vivo (29, 37–42). The PRL-suppressive effect of VAC is thought to be due to a number of diterpenes, including clerodadienols, which bind to dopamine D2 receptor (37). The dopaminergic bicyclic diterpenes that have been identified are able to inhibit cAMP formation and PRL release in rat pituitary cell cultures (41). Such dopaminergic action inhibits both basal and thyrotropin releasing hormone (TRH)-stimulated PRL release (37, 38).
VAC may also bind to estrogen receptor (ER) and, as per an investigation of phytotherapy safety and efficacy in the USA, it has been evidenced that methanol extract of VAC shows significant competitive binding to ERα and ERβ (7). In addition, linoleic acid was identified as an ER ligand in VAC extracts (43). ERα or ERβ binding assays have been used to guide fractionation of VAC, which resulted in the isolation of apigenin and its identification as an ERβ-selective phytoestrogen (44). The administration of VAC extract and estradiol valerate to ovariectomized rats significantly improved learning and memory performance in both groups and the findings in each group were comparable (45). VAC extract significantly increased the expression of ERα mRNA in the hippocampus. Additionally, VAC extract at the dose of 80 mg/kg significantly increased the uterine weight in the ovariectomized rats.This result was similar to that observed in the estradiol-treated group (45). However, these data contradict the findings from a previous study, in which VAC dry extract did not induce vaginal cornification or an increase in uterine weight in rats, suggesting that it does not exert in vivo estrogenic properties (46).
VAC opioid activity can be beneficial in diminishing the symptoms of PMS such as depression, irritability, anxiety, mastalgia, fatigue, and headache (47, 48). Extracts of VAC have been reported to have an affinity for the opioid μ, δ, and κ receptors (MOR, DOR, and KOR, respectively). One study showed that VAC has a high affinity for MOR and KOR, and a weak affinity for DOR (39). In addition, two VAC methanol extracts have been found to activate MOR (8). Whereas a study reported an antagonist opioid activity of some flavonoids, a more recent study determined that these compounds have dose-dependent affinity for MOR and DOR resulting in the activation of these two receptors, but not in the activation of KOR (49, 50).
The possible impact of VAC on the pituitary-thyroid axis and the pituitary-adrenal axis was assessed by the administration of VAC essential oil to rats. In treated rats, the gland functional morphology showed that the relative volume density of thyrotrophic cells and thyrocytes was increased. By contrast, a decrease of pituitary corticotrophic cells associated with no changes on the adrenal tissue was observed. Consistently with the cytological findings, TSH, total thyroxine, and triiodothyronine had an increment while ACTH was lower than at the baseline and corticosterone was unaltered (51).
A possible chemopreventive activity of some VAC components (vitetrifolim D and vitexlatam) has also been hypothesized and assessed. These components may be able to stimulate NADP(H): quinone oxidoreductase type 1 (QR1) (26). QR1 is an important phase II detoxification enzyme that can protect cells against the harmful effects caused by free radicals and reactive oxygen species by catalyzing the reduction of quinones to hydroquinones. Therefore, an increased activity of the enzyme might protect cells from potential carcinogenicity (26, 52).
Additionally, VAC has been shown to exert some beneficial effects in the process of the bone healing after a long bone fracture in premenopausal women (25). Osteogenic and angiogenic factors and callus formation were assessed in a double-blind randomized placebo-controlled trial. In this study, vascular endothelial growth factor (VEGF), which is known to induce vascular invasion in fracture gap and enhance angiogenesis, was significantly increased in the VAC-treated group compared with the baseline (25, 53). Thus, phytoestrogens could exert a positive effect in the process of angiogenesis and promote the early stage of fracture healing. The VAC-treated group also showed an improved callus formation. When VAC was co-administered with magnesium, a significant elevation of osteocalcin, an osteogenic marker, has been reported (25).
The therapeutic effects of VAC impact on the endocrine physiology through their action on various hormones, such as PRL and female sex hormones. These effects appear to be dose-dependent. Low dose VAC resulted in lower estrogen levels and higher progesterone and PRL levels, possibly caused by the inhibition of the release of FSH and stimulation of LH (13, 54). In a study using different VAC doses, the highest VAC dose decreased the levels of PRL while FSH and LH remained unchanged (37). This dose-dependent relationship may clarify why low VAC doses stimulate breast milk production, while high doses have the opposite effect (5).
The preparations and dosage of VAC are wide-ranging. Dried, ripened, or fresh ripe fruits (berries) can be used to produce the phytotherapic medications in the form of liquid extract, dried fruit, or as a tablet or capsule. Fluid extract (40 drops daily) and tincture (35 to 45 drops, 3 times a day) have also been used (13, 55). VAC-enriched food supplements are also available. The variability in preparation and dosage was noted in the different clinical studies. Though the dosage of VAC dry extract is often 20 to 40 mg per day, in some cases higher doses (up to 1800 mg per day) were used (11, 13, 48). The appropriate dose may be best determined by the purpose for which it is being applied. For isolated mastalgia, a low VAC dosage could be appropriate (56, 57). For the treatment of PMS, a higher dosage might be necessary (58). The prescription of 4 mg/day of an extract standardized to 6% of the constituent agnuside is one of the formulations sold in the USA and this dose has been used in some studies (5).
The Committee on the Herbal Medicinal Products (HMPC), a sub-organization of the European Medicines Agency, published a final report on VAC in 2010 (59). They stated that VAC should contain the dry extract of the crude drug, which is extracted with 60% ethanol aqueous solution at the drug-extract-ratio of 6-12:1, equivalent to 180 mg of the crude herbal substance (mg/d). The specified contents of 0.05% agnuside and 0.08% casticin in the crude drug quantified by high performance liquid chromatography (HPLC) are considered to be the minimum pharmacological requirement. A medicinal product equivalent to 180 mg/d of the crude drug, as recommended by HMPC, contains at least 0.09 mg/d of agnuside and 0.144 mg/d of casticin, respectively (59). By this definition, two commercial VAC-derived drugs have been labeled for “well-established use” in 2014 and five other VAC-derived compounds have been considered as traditional products (22).
An assessment of the quality of medicinal products and health supplements that contain VAC in the European, Japanese, and American markets was published in 2014 (22). In Europe, only VAC extracts classified as drugs are commercialized. By contrast, in Japan and the USA, there are VAC-containing health foods with no such strict specifications like those of HPMC (59). The majority of health supplements assessed failed to reach the minimum standard of not less than 0.05% agnuside and 0.08% (22).
VAC is usually well tolerated, with infrequent, mild, and reversible adverse effects, such as nausea, headache, gastrointestinal disturbances, menstrual disorders, acne, itch, and rash (60, 61).
There are no known drug interactions with VAC but, due to its dopaminergic effects, its derivatives could interfere with certain Parkinson’s disease medications, such as dopamine agonists and dopaminergic antagonists, like metoclopramide (37, 38). Importantly, VAC has not been found to interact with oral contraceptives (OCP) and its use in treating PMS symptoms among women taking the OCP has been shown (62). However, given the significance of any interaction between OCP and VAC, this aspect should be addressed independently.
VAC is contraindicated during pregnancy and there is controversy with regard to its use during lactation. The caution is due, at least in part, to the absence of clear data and the pharmacologically varied activity of phytotherapic drugs (63, 64). Without clear evidence in terms of safety and efficacy VAC extracts will remain contraindicated during pregnancy for the general safety of mother and child (18). Similarly, VAC use during lactation is not encouraged (55).
In this manuscript, we aimed to review and analyse the data as well as the clinical implications of the effects of VAC on PRL secretion. The use of VAC in the treatment of a number of gynaecological conditions has been quite extensively reviewed and assessed (57, 65–67). However, VAC has been proposed as a therapeutic alternative for a number of other indications, including the therapeutic management of hyperprolactinaemia. The use of VAC in the treatment of hyperprolactinaemia has not been precisely defined yet. There is a limited number of small clinical studies from which only a few concrete conclusions can be drawn. Given the explosion of the alternative remedies market, a full understanding of the physiology and pharmacology of VAC impact on PRL levels is of relevance to endocrinologists and gynaecologists and, ultimately to the patients taking these over-the-counter medications (16, 18, 67). In particular, patients with mild to moderate elevation of PRL who wish to avoid conventional medications may choose to use phytotherapic medications that appear to be safe and well tolerated, and actually may have a role in the inhibition of PRL hypersecretion (5, 37, 60, 61, 68). With regard to the administration of VAC extract to patients with prolactinoma, only a handful of case reports have been published (69, 70). Therefore, we wonder if a role for the use of VAC in the treatment of hyperprolactinaemia may finally exist.
We have reviewed and analysed the studies that evaluate the effects of VAC on PRL secretion published up to February 2019. We have included the studies that considered this target either directly or indirectly, thus including those studies that looked at the effect of VAC on mild hyperprolactinaemia. The studies in which VAC was assessed in association with other medication were excluded.
The terms used were vitex agnus castus, agnus castus, chaste berry, and monk’s pepper both independently and cross-referenced with hyperprolactinaemia, premenstrual syndrome, polycystic ovary syndrome, and mastalgia. Additionally, further relevant papers were identified using the “related articles” function in PubMed and by exploring the reference lists of the relevant articles. We did not restrict the search to randomized controlled studies because the number of suitable papers would be extremely limited. On the other side, we have included single case reports or series.
The electronic databases explored were Pubmed, ClinicalTrials.gov, and The Cochrane Library.
Altogether, we have identified a total of nine published papers. Among these, six were prospective studies (Table 2) (19, 54, 56, 71–73). Three published papers were case reports of patients with hyperprolactinaemia who have received treatment with a VAC extract (Table 3) (69, 70, 74).
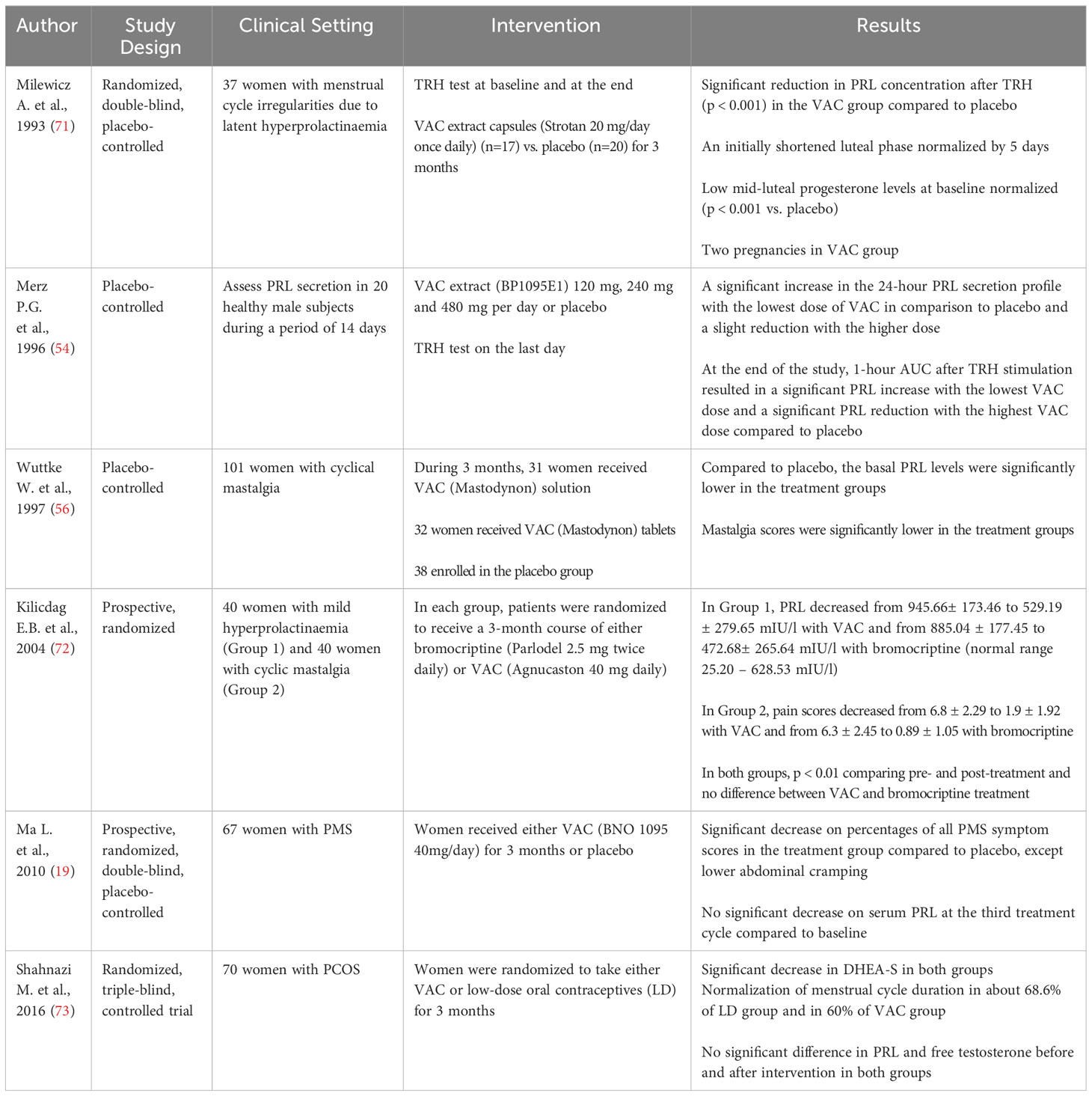
Table 2 Prospective studies where PRL levels were assessed in patients taking a VAC extract.
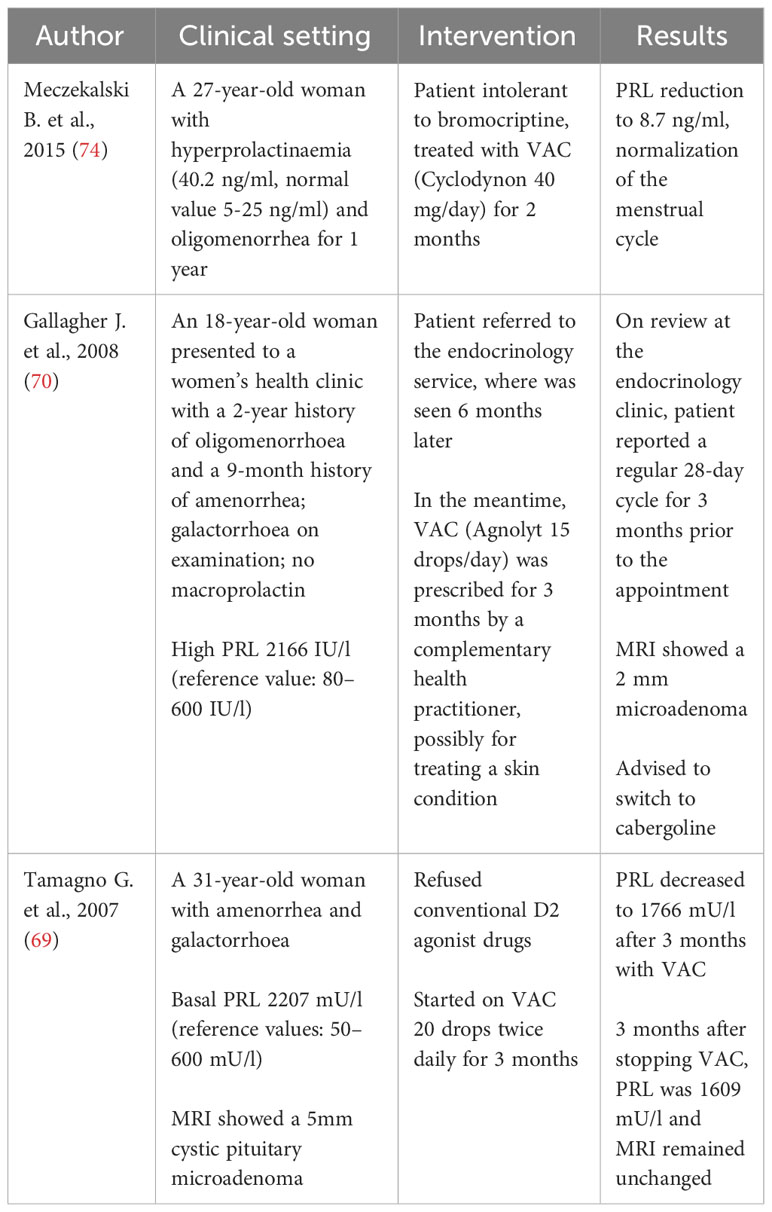
Table 3 Case reports of patients with hyperprolactinaemia who have been treated with a VAC extract.
Though there is some evidence suggesting a role of VAC in the management of hyperprolactinaemia in selected patients, the lack of large randomized controlled trials and the still unclear pharmacological aspects through which VAC extract might work affect the possibility of reaching solid enough conclusions. Unfortunately, the variety of the methodological aspects and of the design of the studies prevent from drawing any reproducible conclusions. However, it appears that VAC can be able to impact on PRL secretion in selected patients, especially those with only mild hyperprolactinaemia, and in general terms seems to be a safe and well tolerated phytotherapic agent.
Hyperprolactinaemia is a relatively common condition in the female population. In addition, the popularity of non-conventional medications, including phytotherapic drugs, has progressively increased in the recent years. VAC has been proposed as a phytotherapic medication with a potential to reduce PRL levels in vivo. Against the beliefs held by monks in the middle ages, VAC may actually have a role in increasing, as opposed to decreasing, male libido. The available literature on the effect of VAC, although limited in number, suggests a potential role of VAC in the treatment of mild hyperprolactinaemia. All but two of the published studies included in our data analysis report a decrease of the PRL levels as a result of the use of VAC extracts. One of the studies that failed to demonstrate a decrease in PRL did not provide reference ranges for PRL, stating only that it did not significantly change, and the results are therefore difficult to draw conclusions from (19). In the other manuscript that found no significant changes on PRL levels after three cycles of treatment with VAC, the authors stated that the result might be explained by the different methods used for measuring the PRL levels (ELISA, versus specific chemiluminescence assay method) (71, 73). Moreover, VAC effects might be dose-dependent and also this aspect can contribute to the heterogeneity of the results among the various studies. For example, a low VAC dose has been found to increase PRL while, in the same study, a higher dose decreased the PRL levels (54). This observation may highlight further the complicated pharmacology of the active constituents of VAC.
In our opinion, the systematic characterization and assessment of the single molecular constituents of VAC extract is the only possible way for discriminating which of them, alone or in combination, are able to exert a pharmacological effect on PRL secretion and, therefore, on the circulating PRL levels. However, we understand that such an approach would require a significant financial investment and a heavy dedicated workload for the researchers. Possibly these practical aspects have contributed to the limited research carried out on this topic to date. In fact, we shall keep in mind that there is already a good number of well-established, effective, and reasonably safe conventional medications available on the market (cabergoline and bromocriptine, for citing the two most widely used dopamine agonists in the treatment of hyperprolactinaemia). A comparison of VAC and bromocriptine use on PRL levels in women with mild hyperprolactinaemia found a comparable reduction in both groups (72). Although arising from a small study, these findings are interesting and warrant further evaluation. The reduction of PRL after VAC administration has been demonstrated elsewhere, including a decrease in TRH-stimulated PRL release and among women with mastalgia (56, 71).
Unfortunately, the assessment of a possible correlation between the changes of the PRL levels, when documented, and the changes of the signs and symptoms reported by the patients enrolled in the various studies cannot be performed in a valid way considering the inhomogeneous collection of data and observations from study to study.
In addition to the few studies where the changes of specific symptoms and signs were assessed, some case reports described a reduction in the symptoms of hyperprolactinaemia, such as galactorrhea and menstrual cycle irregularities, in women taking VAC. Interestingly, in two of these case reports, the patient had a pituitary microadenoma (69, 70).
Unfortunately, the small number of studies and case reports published to date and included in this analysis of the published clinical data are significantly heterogeneous. Many of these works lack a robust enough methodology, often with a small number of enrolled patients and with a short duration of the treatment and/or observation time. Moreover, the different types of VAC extract and doses used in the reported studies inevitably impact in a significant way on the possibility of carrying out a solid and reliable analysis of the results. There are also some obvious difficulties usually encountered by the researchers when studying the physiological levels of PRL in vivo. For example, physiological stressors, such as venipuncture, may impact on the findings and should also be accounted for in any study design. A quite recent meta-analysis focusing on the VAC in PMS highlighted the paucity of well-structured studies (66). Moreover, there is a generic risk of selection bias associated with the meta-analyses. The poor homogeneity and the paucity of the published data unfortunately prevents from a statistical analysis of the published findings.
Therefore, it is not possible to reach any solid conclusions on the potential role of VAC extract in the treatment of hyperprolactinaemia. Additionally, a direct link between VAC and decreased PRL levels has been not undoubtedly identified yet.
We think that further investigations, both in vitro and in vivo and including also more stringently designed studies and high quality trials, should be encouraged on the basis of the currently available data from the literature.
However, for the moment the possible pharmacological use of VAC extractin patients with hyperprolactinaemia should remain strictly limited to the few patients who are looking for non-conventional forms of treatment and, in our opinion, also in these cases the well-established dopamine agonists should be initially offered as first-line treatment and, then, re-offered during the follow-up within a reasonable observation time, if no evidence of satisfactory therapeutic effects will be achieved with VAC.
The precise characterization of one or more VAC extract molecules able to therapeutically impact on the PRL levels and proving that such VAC component or components are effective and safe in vivo is, in our opinion, the only option for possibly considering the use of VAC, in the form of specific component or components, for the treatment of hyperprolactinaemia. Probably, the well-established presence on the market of valuable and reliable dopamine agonists contributes to leave a very little room only to non-conventional alternatives in the pharmacological armamentarium of the treatment of hyperprolactinaemia.
The interest in phytotherapic drugs has lately increased worldwide, both among patients and in the scientific community. VAC is a well-known phytotherapic drug with a relatively proven role in some gynaecological conditions and, in particular, in the treatment of PMS. The efficacy of VAC extracts in the treatment of other conditions, like hyperprolactinaemia, is still a matter of debate. There are no published studies which produce unequivocal evidence of VAC efficacy in this clinical setting and, indeed, the complexity of the physiological, pharmacological, and clinical aspects of VAC and hyperprolactinaemia does not help. Even in this context affected by a significant degree of uncertainty, the available laboratory and clinical findings seem to support the existence of some effects of VAC on PRL secretion with a possible therapeutic impact in selected patients. Larger and higher quality studies are required for exploring the VAC effects on hyperprolactinaemia and, possibly, confirming the hypothesis of a role of this phytotherapic medication in such a clinical setting. Some important questions, for example related to the therapeutic VAC dosage and the target patient population, are still unanswered. However, we think that VAC might represent a potentially reasonable and safe phytotherapic option for the management of selected patients with mild hyperprolactinaemia who wish to be treated with phytotherapy.
LP: Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft. JL: Data curation, Resources, Validation, Visualization, Writing – review & editing. GT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The preliminary findings of this review and analysis of published data have been presented as poster at the 17th Congress of the European Neuroendocrine Association, Milan, Italy.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. P'ei C, Chen S, Fang W, Liou S, Fu L, Sheng G, et al. Delectis Florae Reipublicae Popularis Sinicae Agendae Academiae Sinicae Edita. In: Fl Reipubl Popularis Sin, (Science Press) vol. 65. p. 131–50.
2. Li SH. Studies on the chemical and biological constituents of three Taxaceae plants, Vitex agnus-castus and Isodon xerophilus [dissertation]. Kunming, China: Kunming Institute of Botany, the Chinese Academy of Sciences (2001).
3. Niedenthal T, Uehleke B, Puchtler E. Mönchspfeffer: Kritische Notizen zur Arzneipflanze des Jahres 2022. Z für Phytotherapie (2022) 43(6):255–61.
4. Madaus G. Lehrbuch der biologischen Arzneimittel, Abteilung I: Heilpflanzen. Georg Thieme Verlag (1938) Vol. I:441–6.
6. Merz PG, Schrödter A, Rietbrock S, Gorkow C, Löw D. Prolactin secretion and tolerance during treatment with an Agnus castus extract (BP1095E1) - Effect on prolactin secretion. Phytopharmaka Forschung und Klinischer Anwendung (1995), 93–7. doi: 10.1007/978-3-642-85434-7_7
7. Liu JH, Burdette JE, Xu HY, Gu C, van Breemen RB, Bhat KP, et al. Evaluation of estrogenic activity of plant extracts for the potential treatment of menopausal symptoms. J Agric Food Chem (2001) 49:2472–2479. doi: 10.1021/jf0014157
8. Webster DE, Lu J, Chen SN, Farnsworth NR, Wang ZJ. Activation of the mu-opiate receptor by Vitex agnus-castus methanol extracts: implication for its use in PMS. J Ethnopharmacol (2006) 106(2):216–21. doi: 10.1016/j.jep.2005.12.025
9. Arentz S, Abbott JA, Smith CA, Bensoussan A. Herbal medicine for the management of polycystic ovary syndrome (PCOS) and associated oligo/amenorrhoea and hyperandrogenism; a review of the laboratory evidence for effects with corroborative clinical findings. BMC Complement Altern Med (2014) 14:511. doi: 10.1186/1472-6882-14-511
10. Kommission E. Monographie BGA/BfArM, Agni casti fructus (Keuschlamm-früchte). Bundesanzeiger (1992) 226.
11. Blumenthal M. German Federal Institute for Drugs and Medical Devices. Commission E. Herbal Medicine: expanded Commission E monographs. 1st ed. Newton (MA: Integrative Medicine Communications (2000).
12. Williamson E. Synergy and other interactions in phytomedicines. Phytomedicine (2001) 8(5):401–9. doi: 10.1078/0944-7113-00060
13. Mills S, Bone K. Principles and practice of phytotherapy. London: Churchill Livingstone Harcourt Publishers (2000).
14. Holden S, Davis R, Yeh G. Pregnant women’s use of complementary & alternative medicine in the United States. J Altern Compl Med (2014) 20(5):A120. doi: 10.1089/acm.2014.5319.abstract
15. Smith CA, Bateson DJ, Weisberg E. A survey describing the use of complementary therapies and medicines by women attending a family planning clinic. BMC Complement Altern Med (2013) 13(1):224. doi: 10.1186/1472-6882-13-224
16. Smith T, Lynch ME, Johnson J, Kawa K, Bauman H, Blumenthal M. Herbal and dietary supplement sales in the US increase 6.8% in 2014. Herbal Gram (2015) 107:52–9.
17. Garcia-Alvarez A, Egan B, de Klein S, Dima L, Maggi FM, Isoniemi M, et al. Usage of plant food supplements across six European countries: findings from the PlantLIBRA consumer survey. PloS One (2014) 9(3):e92265. doi: 10.1371/journal.pone.0092265
18. Izzo AA, Hoon-Kim S, Radhakrishnan R, Williamson EM. A critical approach to evaluating clinical efficacy, adverse events and drug interactions of herbal remedies. Phytother Res (2016) 30:691–700. doi: 10.1002/ptr.5591
19. Ma L, Lin S, Chen R, Zhang Y, Chen F, Wang X. Evaluating therapeutic effect in symptoms of moderate-to-severe premenstrual syndrome with Vitex agnus castus (BNO 1095) in Chinese women. Aust N Z J Obstet Gynaecol (2010) 50:189–93. doi: 10.1111/j.1479-828X.2010.01137.x
20. Zamani M, Neghab N, Torabian S. Therapeutic effect of Vitex Agnus castus in patients with premenstrual syndrome. Acta Med Iran (2012) 50:101–6.
21. Momoeda M, Sasaki H, Tagashira E, Takano Y, Ochiai K. Efficacy and safety of Vitex agnus-castus extract for treatment of premenstrual syndrome in Japanese patients: a prospective, open-label study. Adv Ther (2014) 31(3):362–73. doi: 10.1007/s12325-014-0106-z
22. Fukahori M, Kobayashi S, Naraki Y, Sasaki T, Oka H, Seki M, et al. Quality evaluation of medicinal products and health foods containing chaste berry (Vitex agnus-castus) in Japanese, European and American markets. Chem Pharm Bull (2014) 62(4):379–85. doi: 10.1248/cpb.c13-00588
23. Chen SN, Friesenb JB, Webster D, Nikolic D, van Breemen RB, Wang ZJ, et al. Phytoconstituents from Vitex agnus-castus fruits. Fitoterapia (2011) 82(4):528–33. doi: 10.1016/j.fitote.2010.12.003
24. Maltas E, Uysal A, Ylldiz S, Durak Y. Evaluation of antioxidant and antimicrobial activity of Vitex agnus castus L. Fresen Environ Bull (2010) 19:3094–9.
25. Eftekhari MH, Rostami ZH, Emami MJ, Tabatabaee HR. Effects of “vitex agnus castus” extract and magnesium supplementation, alone and in combination, on osteogenic and angiogenic factors and fracture healing in women with long bone fracture. J Res Med Sci (2014) 19(1):1–7.
26. Li S, Qiu S, Yao P, Sun H, Fong HHS, Zhang H. Compounds from the fruits of the popular European medicinal plant Vitex agnus-castus in chemoprevention via NADP(H): quinone oxidoreductase type 1 induction. Evid Based Complement Alternat Med (2013) 2013:432829. doi: 10.1155/2013/432829
27. Melmed S, Kleinberg D. 2008 Anterior pituitary. In: Kronenberg HM, Melmed S, Polonsky KS, Larsen PR, editors. Williams textbook of endocrinology 11th ed, vol. p . Philadelphia (PA: Saunders Elsevier (2008). p. 185–261.
28. Jarry H, Leonhardt S, Wuttke W, Spengler B, Christoffel V. Auf der Suche nach dopaminergen substanzen in Agni-casti-fructus-präparaten: warum eigentlich. Z Phytother (1999) 20:150–2. doi: 10.1078/094471103322004866
29. Wuttke W, Jarry H, Christoffel V, Spengler B, Seidlová-Wuttke D. Chaste tree (Vitex agnus-castus) – pharmacology and clinical indications. Phytomedicine (2003) 10:348–57. doi: 10.1078/094471103322004866
30. Kumar S, Mansel RE, Scanlon MF, Hughes LE, Edwards CA, Woodhead JS, et al. Altered responses of prolactin, luteinizing hormone and follicle stimulating hormone secretion to thyrotrophin releasing hormone/gonadotrophin releasing hormone stimulation in cyclical mastalgia. Br J Surg (1984) 71(11):870–3. doi: 10.1002/bjs.1800711123
31. Peters F, Schuth W, Scheurich B, Breckwoldt M. Serum prolactin levels in patients with fibrocystic breast disease. Obstet Gynecol (1984) 64(3):381–5.
32. Halbreich U, Ben-David M, Assael M, Bornstein R. Serum-prolactin in women with premenstrual syndrome. Lancet (1976) 7987:654–6. doi: 10.1016/S0140-6736(76)92465-X
33. Carroll BJ, Steiner MP. The psychobiology of premenstrual dysphoria: the role of prolactin. Psychoneuroendocrinology (1978) 3(2):171–80. doi: 10.1016/0306-4530(78)90005-7
34. Jarry H, Leonhardt S, Wuttke W, Behr B, Gorkow C. Agnus-castus als dopaminerges wirkprinzip in Mastodynon N. Z für Phytotherapie (1991) 3:77–82.
35. Mansel RE, Dogliotti L. European multicentre trial of bromocriptine in cyclical mastalgia. Lancet (1990) 335(8683):190–3. doi: 10.1016/0140-6736(90)90278-D
36. Schwibbe M, Becker D, Wuttke W. EEG and psychological effects of lisuride in women with premenstrual tension. In: Calne DB, editor. Lisuride and other dopamine agonists. New York (NY: Raven Press (1983). p. 345–55.
37. Sliutz G, Speiser P, Schultz AM, Spona J, Zeillinger R. Agnus castus extracts inhibit prolactin secretion of rat pituitary cells. Horm Metab Res (1993) 25(5):253–5. doi: 10.1055/s-2007-1002090
38. Jarry H, Leonhardt S, Gorkow C, Wuttke W. In vitro prolactin but not LH and FSH release is inhibited by compounds in extracts of Agnus castus: direct evidence for a dopaminergic principle by the dopamine receptor assay. Exp Clin Endocrinol (1994) 102(6):448–54. doi: 10.1055/s-0029-1211317
39. Wuttke W. Dopaminergic action of extracts of Agnus Castus. Forsch Komplementmed (1996) 3:329–30.
40. Meier B, Berger D, Hoberg E, Sticher O, Schaffner W. Pharmacological activities of Vitex agnus-castus extracts in vitro. Phytomedicine (2000) 7(5):373–81. doi: 10.1016/S0944-7113(00)80058-6
41. Ibrahim N, Shalaby AS, Farag RS, Elbaroty GS, Nofal SM, Hassan EM. Gynecological efficacy and chemical investigation of Vitex agnus-castus L. fruits growing in Egypt. Nat Prod Res (2008) 22(6):537–46. doi: 10.1080/14786410701592612
42. Jarry H, Spengler B, Wuttke W, Christoffel V. In vitro assays for bioactivity-guided isolation of endocrine active compounds in Vitex agnus-castus. Maturitas (2006) 55S:S26–36. doi: 10.1016/j.maturitas.2006.06.014
43. Liu J, Burdette JE, Sun Y, Deng S, Schlecht SM, Zheng W, et al. Isolation of linoleic acid as an estrogenic compound from the fruits of Vitex agnus-castus L. (chaste-berry). Phytomedicine (2004) 11:18–23. doi: 10.1078/0944-7113-00331
44. Jarry H, Spengler B, Porzel A, Schmidt J, Wuttke W, Christoffel V. Evidence for estrogen receptor beta-selective activity of Vitex agnus-castus and isolated flavones. Planta Med (2003) 69:945–7. doi: 10.1055/s-2003-45105
45. Allahtavakoli M, Honari N, Pourabolli I, Kazemi AI, Ghafarian H, Roohbakhsh A, et al. Vitex agnus castus extract improves learning and memory and increases the transcription of estrogen receptor α in hippocampus of ovariectomized rats. Basic Clin Neurosci (2015) 6(3):185–92.
46. Cavieres MF, Castillo R. Evaluation of the estrogenicity of vitex agnus castus. Toxicol Lett (2011) 205S:S250. doi: 10.1016/j.toxlet.2011.05.853
47. Lauritzen C, Reuter HD, Repges R, Böhnert KJ, Schmidt U. Treatment of premenstrual tension syndrome with Vitex agnus- castus. Controlled, double-blind study versus pyridoxine. Phytomedicine (1997) 4:183–9. doi: 10.1016/S0944-7113(97)80066-9
48. Schellenberg R. Treatment for the premenstrual syndrome with agnus castus fruit extract: prospective, randomized, placebo controlled study. BMJ (2001) 322:134–7. doi: 10.1136/bmj.322.7279.134
49. Katavic PL, Lamb K, Navarro H, Prisinzano TE. Flavonoids as opioid receptor ligands: identification and preliminary structure-activity relationships. J Nat Prod (2007) 70(8):1278–82. doi: 10.1021/np070194x
50. Webster DE, He Y, Chen SN, Pauli GF, Farnsworth NR, Wang ZJ. Opioidergic mechanisms underlying the actions of Vitex agnus-castus L. Biochem Pharmacol (2011) 81(1):170–7. doi: 10.1016/j.bcp.2010.09.013
51. Šošić-Jurjević B, Ajdžanović V, Filipović B, Miloševi V. Functional morphology of pituitary -thyroid and -adrenocortical axes in middle-aged male rats treated with Vitex agnus castus essential oil. Acta Histochem (2016) 118(7):736–45. doi: 10.1016/j.acthis.2016.07.007
52. Li R, Bianchet MA, Talalay P, Amzel LM. The three-dimensional structure of NAD(P)H:quinone reductase, a flavoprotein involved in cancer chemoprotection and chemotherapy: mechanism of the two-electron reduction. Proc Natl Acad Sci USA (1995) 92(18):8846–50. doi: 10.1073/pnas.92.19.8846
53. Street J, Bao M, deGuzman L, Bunting S, Peale FV Jr, Ferrara N, et al. Vascular endothelial growth factor stimulates bone repair by promoting angiogenesis and bone turnover. Proc Natl Acad Sci USA (2002) 99:9656–61. doi: 10.1073/pnas.152324099
54. Merz PG, Gorkow C, Schördter A, Rietbrock S, Sieder C, Loew D, et al. The effects of a special Agnus castus extract (BP 1095E1) on prolactin secretion in healthy male subjects. Exp Clin Endocrinol Diabetes (1996) 104:447–53. doi: 10.1055/s-0029-1211483
55. Upton R. Chaste tree fruit: Vitex agnus-castus: standards of analysis, quality control, and therapeutics. American Herbal Pharmacopoeia and therapeutic compendium. Santa Cruz (CA: American Herbal Pharmacopoeia (2001).
56. Wuttke W, Splitt G, Gorkow C, Sieder C. Behandlung zyklusabhängiger Brustschmerzen mit einem Agnus castus-haltigen arzneimittel – egebnisse einer randomisierten plazebokontrollierten doppelblindstudie. Geburtshilfe Frauenheilkd (1997) 57:569–74. doi: 10.1055/s-2007-1023139
57. Halaska M, Beles P, Gorkow C, Sieder C. Treatment of cyclical mastalgia with a solution containing a Vitex agnus castus extract: results of a placebo-controlled double-blind study. Breast (1999) 8(4):175–81. doi: 10.1054/brst.1999.0039
58. Schellenberg R, Zimmermann C, Drewe J, Hoexter G, Zahner C. Dose-dependent efficacy of the Vitex agnus castus extract Ze 440 in patients suffering from premenstrual syndrome. Phytomedicine (2012) 19:1325–31. doi: 10.1016/j.phymed.2012.08.006
59. Committee on Herbal Medicinal Products. EMA/HMPC/144006/2009. London: European Medicines Agency (2010).
60. McCaleb R, Leigh E, Morien K. The encyclopedia of popular herbs: your complete guide to the leading medicinal plants. Roseville (CA: Prima Health (2000).
61. Daniele C, Thompson CJ, Pittler MH, Pittler MH, Ernst E. Vitex agnus castus: a systematic review of adverse events. Drug Saf (2005) 28:319–32. doi: 10.2165/00002018-200528040-00004
62. Braun L, Cohen M. Herbs and natural supplements - an evidence-based guide. 4th ed Vol. 2. Australia: Elselvier (2015).
63. Ernst E. Herbal medicinal products during pregnancy: are they safe? BJOG (2002) 109:227–35. doi: 10.1111/j.1471-0528.2002.t01-1-01009.x
64. Smeriglio A, Tomaino A, Trombetta D. Herbal products in pregnancy: experimental studies and clinical reports. Phytother Res (2014) 28:1107–16. doi: 10.1002/ptr.5106
65. Dante G, Facchinetti F. Herbal treatments for alleviating premenstrual symptoms: a systematic review. J Psychosom Obstet Gynaecol (2011) 32(1):42–51. doi: 10.3109/0167482X.2010.538102
66. Verkaik S, Kamperman AM, van Westrhenen R, Schulte PFJ. The treatment of premenstrual syndrome with preparations of Vitex agnus castus: a systematic review and meta-analysis. Am J Obstret Gynecol (2017) 217(2):150–66. doi: 10.1016/j.ajog.2017.02.028
67. Franco OH, Chowdhury R, Troup J, Voortman T, Kunutsor S, Kavousi M, et al. Use of plant-based therapies and menopausal symptoms: a systematic review and meta-analysis. JAMA (2016) 315(23):2554–63. doi: 10.1001/jama.2016.8012
68. Tamagno G. Are changes of prolactin levels the effectors of vitex agnus castus beneficial effects on the pre-menstrual syndrome? Maturitas (2009) 63:369. doi: 10.1016/j.maturitas.2009.07.004
69. Tamagno G, Burlacu MC, Daly AF, Beckers A. Vitex agnus castus might enrich the pharmacological armamentarium for medical treatment of prolactinoma. Eur J Obstet Gynecol Reprod Biol (2007) 135:136–41. doi: 10.1016/j.ejogrb.2007.05.004
70. Gallagher J, Lynch FW, Barragry J. A prolactinoma masked by a herbal remedy. Eur J Obstet Gynecol Reprod Biol (2008) 137:247–61. doi: 10.1016/j.ejogrb.2006.12.020
71. Milewicz A, Gejdel E, Sworen H, Sienkiewicz K, Jedrzejak J, Teucher T, et al. Vitex agnus castus extract in the treatment of luteal phase defects due to latent hyperprolactinemia. Results of a randomized placebo-controlled double-blind study. Arzneimittelforschung (1993) 43(7):752–6.
72. Kilicdag EB, Tarim E, Bagisa T, Erkanli S, Aslan E, Ozsahin K, et al. Fructus agni casti and bromocriptine for treatment of hyperprolactinemia and mastalgia. Int J Gynaecol Obstet (2004) 85:292–3. doi: 10.1016/j.ijgo.2004.01.001
73. Shahnazi M, Khalili AF, Hamdi K, Ghahremaninasab P. The effects of combined low-dose oral contraceptives and vitex agnus on the improvement of clinical and paraclinical parameters of polycystic ovarian syndrome: A triple-blind, randomized, controlled clinical trial. Iran Red Crescent Med J (2016) 18(12):e37510. doi: 10.5812/ircmj.37510
Keywords: Vitex agnus castus, hyperprolactinaemia, dopamine agonist, phytotherapy, premenstrual syndrome, mastalgia
Citation: Puglia LT, Lowry J and Tamagno G (2023) Vitex agnus castus effects on hyperprolactinaemia. Front. Endocrinol. 14:1269781. doi: 10.3389/fendo.2023.1269781
Received: 30 July 2023; Accepted: 02 November 2023;
Published: 21 November 2023.
Edited by:
Xiang’En Shi, Capital Medical University, ChinaReviewed by:
Craig Stiles, Barts Health NHS Trust, United KingdomCopyright © 2023 Puglia, Lowry and Tamagno. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gianluca Tamagno, Z2lhbmx1Y2F0YW1hZ25vQHRpc2NhbGkuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.