
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 14 August 2023
Sec. Clinical Diabetes
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1237832
This article is part of the Research TopicCOVID-19 and Diabetes: Current Findings and Future PerspectivesView all 17 articles
 Xiao-ying Zhou1
Xiao-ying Zhou1 Shao-feng Huang1Jun-xu Lin2Hai-ni Zhi2Lu Xiao3Xiang-zhu Wang1Kai-heng Guo1
Shao-feng Huang1Jun-xu Lin2Hai-ni Zhi2Lu Xiao3Xiang-zhu Wang1Kai-heng Guo1 Lin Zhou1
Lin Zhou1 Tao Long1Hui-min You1Ming-run Lin1Xiang-ya Luo1Wei-ping Sun3*
Tao Long1Hui-min You1Ming-run Lin1Xiang-ya Luo1Wei-ping Sun3* Chun-ping Zeng1*
Chun-ping Zeng1*Aims: This study aims to describe the clinical characteristics, laboratory data and complications of hospitalized COVID-19 patients with type 2 diabetes mellitus (T2DM) since epidemic prevention and control optimization was adjusted in December 2022 in China.
Methods: This retrospective multicenter study included 298 patients with confirmed type 2 diabetes mellitus with or without COVID-19. We collected data from the first wave of the pandemic in The Fifth Affiliated Hospital of Guangzhou Medical University, Loudi Central Hospital and The First People’s Hospital of Xiangtan from December 1, 2022 to February 1, 2023. We extracted baseline data, clinical symptoms, acute complications, laboratory findings, treatment and outcome data of each patient from electronic medical records.
Results: For among 298 hospitalized patients with type 2 diabetes, 136 (45.6%) were COVID-19 uninfected, and 162 (54.4%) were COVID-19 infected. We found that the incidence of cough, fatigue, fever, muscle soreness, sore throat, shortness of breath, hyposmia, hypogeusia and polyphagia (all p<0.01) were significantly higher in the exposure group. They showed higher levels of ketone (p=0.04), creatinine (p<0.01), blood potassium (p=0.01) and more diabetic ketoacidosis (p<0.01). Patients with COVID-19 less use of metformin (p<0.01), thiazolidinediones (p<0.01) and SGLT2 (p<0.01) compared with patients without COVID-19.
Conclusion: COVID-19 patients with diabetes showed more severe respiratory and constitutional symptoms and an increased proportion of hyposmia and hypogeusia. Moreover, COVID-19 patients with diabetes have a higher incidence of acute complications, are more prone to worsening renal function, and are more cautious about the use of antidiabetic drugs.
Since the optimization and adjustment of epidemic prevention and the orderly restoration of production and living in December 2022, COVID-19 has started the first wave of the pandemic in China. At present, SARS-CoV-2 Omicron BA.5.2 variants is progressively displacing other variants in southern CHINA, which displays a higher transmissibility than other Omicron subvariants (1). Since China no longer requires nucleic acid detection of SARS-CoV-2, the infection rate of the novel coronavirus is not available. The Centers for Disease Control and Prevention (CDC) in Sichuan (a province in southern CHINA) estimated the prevalence of COVID-19 approximately 65.5% as of December 26, 2022. According to the big data model of the National School of Development, as of January 11, 2023, the cumulative infection rate of COVID-19 in China is approximately 64%, and the cumulative number of infected people is approximately 900 million.
Several studies have reported that COVID-19 patients are more susceptible to type 2 diabetes, and the severity and mortality of COVID-19 in diabetes patients are higher than those in patients without diabetes (2, 3). In China, the reported prevalence of diabetes in patients with COVID-19 is similar to the national prevalence of T2DM, approximately 11% (4, 5). In New Delhi, India, the prevalence of diabetes among people with COVID-19 is 47%, which is far higher than the prevalence of T2DM in this region (6). Although the prevalence of diabetes among COVID-19 patients varies by region, studies have reported that the proportion of COVID-19 patients with diabetes is relatively high (7, 8). Moreover, COVID-19 patients with diabetes might be at increased risk of acute metabolic complications, especially an increase in diabetic ketoacidosis during the COVID-19 pandemic (9). The patients with diabetes also had abnormal blood glucose levels and increased the dose of insulin during hospitalization, which indicated their poor glycemic control (10). The increased prevalence, severity, and complications of type 2 diabetes in COVID-19 patients may be related to human angiotensin-converting enzyme 2 (ACE2) and transmembrane serine protease 2 receptors, which are expressed on pancreatic beta cells (11). SARS-CoV-2 infection has been shown to reduce insulin secretion levels and induce pancreatic β cell apoptosis (12).
We conducted a multicenter retrospective study in southern China, aiming to compare the basic information, laboratory examinations, clinical symptoms, acute complications, and medication in patients with diabetes with or without COVID-19, and ascertain the impact of COVID-19 on diabetes.
This retrospective multicenter study included 298 patients with confirmed type 2 diabetes mellitus with or without COVID-19. We collected data from the first wave of the pandemic in The Fifth Affiliated Hospital of Guangzhou Medical University, Loudi Central Hospital and The First People’s Hospital of Xiangtan from December 1, 2022 to February 1, 2023. This research was conducted with approval from the Fifth Affiliated of Guangzhou Medical University Research Ethics Committee. (GYWY-L2023-64).
Patients fulfilling the following criteria were included in this study: physician diagnosis of T2DM and aged over 18 years. Gravidas and patients with severe multi-organ dysfunction were excluded. We divided all patients into two groups depending on whether they were confirmed with COVID-19 after novel coronavirus nucleic acid testing or novel coronavirus antigen detection. All the enrolled patients were hospitalized due to poor blood glucose control or new-onset diabetes, among which the T2DM patients with COVID-19 had been clearly infected before hospitalization.
We extracted baseline data, clinical symptoms, acute complications, laboratory findings, treatment and outcome data of each patient from electronic medical records. All data collected were reviewed by the research team and double checked by experienced physicians. Patients with missing data or unknown medical records were excluded.
We used SPSS (version 26.0; IBM) statistical software to analyze and process the data. Quantitative data were expressed as x±s and differences between groups were compared using independent sample t-test if they were normally distributed. Quantitative data that did not conform to a normal distribution and ordinal data were expressed as medians or quartile ranges and differences between groups were compared using nonparametric tests. Qualitative data were described by frequency or percentage and differences between groups were compared using the χ2 test. For all the statistical analyses, a p-value < 0.05 was considered statistically significant.
A total of 298 hospitalized patients with type 2 diabetes were included in this retrospective study. Among these patients, 136 (45.6%) were COVID-19 uninfected and 162 (54.4%) were COVID-19 infected, respectively. Of all hospitalized patients, the median age was 64 years (IQR, 49-67) and the median duration of diabetes was 8.0 (IQR, 3.0-14.0). Compared with patients without COVID-19, patients with COVID-19 infected had older age (68.5 [IQR, 59.0-76.0]), longer diabetes duration (10.0 [IQR, 4.0-19.0]), and had no significant differences in either systolic blood pressure or diastolic blood pressure. The most common symptoms were cough (143 [48.0%]), fatigue (132 [44.3%]), fever (61[20.5%]), dizziness (77 [25.8%]), shortness of breath (61 [20.5%]), nausea (67 [22.5%]), polyuria (75[25.2%]) and polydipsia (132 [44.3]) at illness onset. Less common symptoms included muscle soreness, runny nose, sore throat, chest distress, diarrhea, hyposmia, hypogeusia, polyphagia and weight loss. We found that the incidence of cough (37[27.2%] vs 106[65.4%]; p<0.01), fatigue (37[27.3%] vs 95[58.6%]; p<0.01), fever (16[11.8%] vs 45[27.8%]; p<0.01), muscle soreness (3[2.2%] vs 22[13.6%]; p<0.01), sore throat (8[5.9%] vs 23[14.2%]; p=0.02), shortness of breath (18[13.2%] vs 43[26.5%]; p<0.01), hyposmia (0[0%] vs 14[8.6%]; p<0.01), hypogeusia (1[0.7%] vs 17[10.5%]; p<0.01) and polyphagia (1[0.7% vs 25[15.4%]; p<0.01) were significantly higher in the exposure group than in the non- exposure group (Table 1).
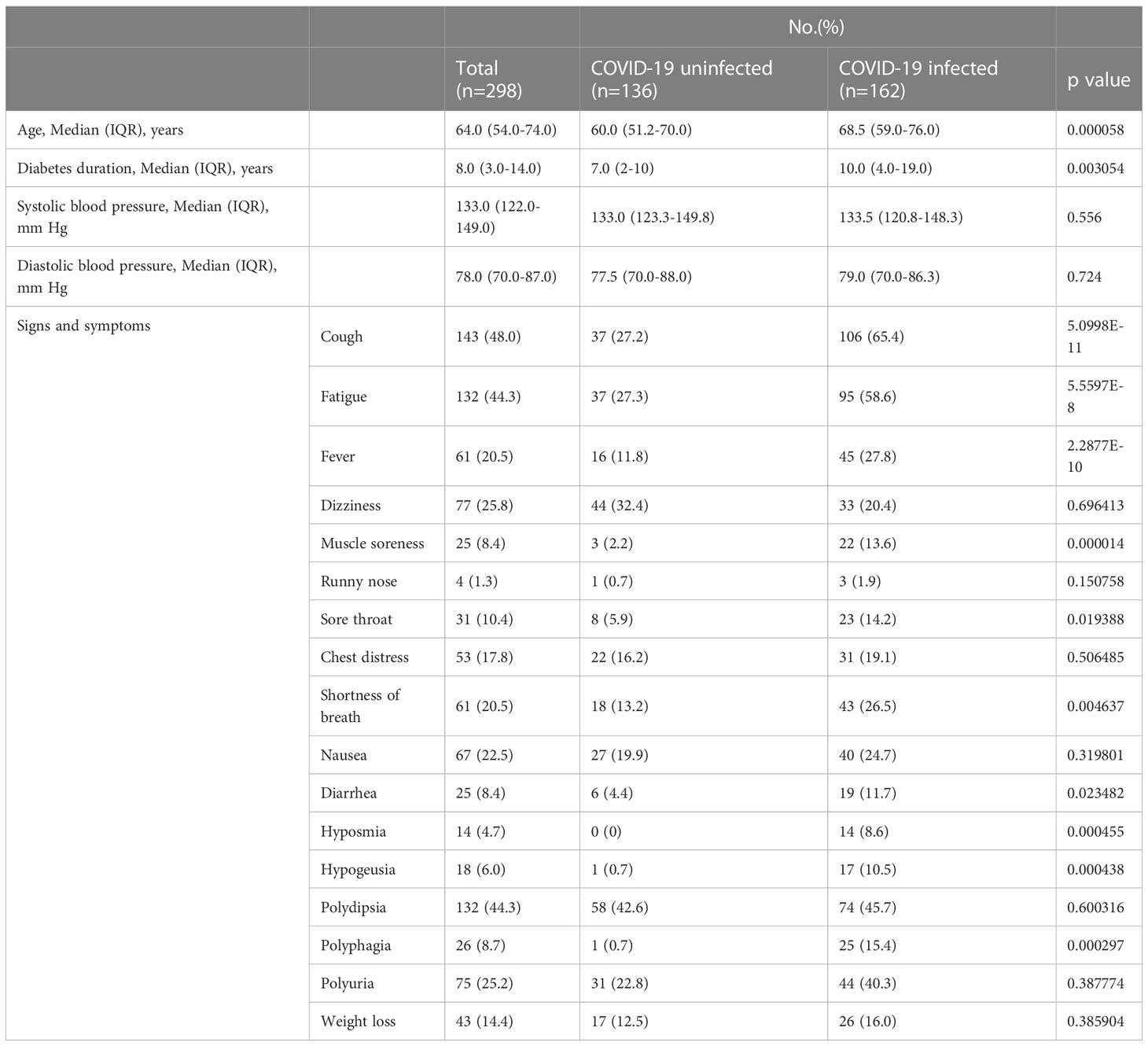
Table 1 Baseline characteristic and clinical signs and symptoms of patients infected with COVID-19.
The laboratory test results and the incidence of acute complications at admission are shown in Table 2. In all the patients, glycosylated hemoglobin and fasting plasma glucose were above the normal range, while the values of other laboratory indicators were within the normal range. Compared to non-exposure group, the exposure group showed higher levels of ketone (0.2 [IQR, 0.1-0.3] vs 0.2 [IQR, 0.1-0.9]; p=0.04), creatinine (69.3 [IQR, 53.7-89.3] vs 86.5 [IQR, 63.3-121.0]); p<0.01), blood potassium (4.0[IQR, 3.7-4.3] vs 4.2[IQR, 3.7-4.6], p=0.01) and more diabetic ketoacidosis (8[5.9%] vs 34[21.0]; p<0.01). These laboratory data indicated that the COVID-19 patients with diabetes are more likely to develop diabetic ketoacidosis and are at greater risk of developing renal insufficiency than those without COVID-19 infection (Table 2).

Table 2 Comparison of laboratory parameters and complication between COVID-19 infected and uninfected diabetic patients.
During hospitalization, most patients were treated with insulin (192[64.1%]), followed by metformin (98[32.9%]), SGLT2 (71[23.8%]), glucosidase inhibitors (48[15.4%]), DPP4 (41[13.8%]), thiazolidinediones (30[10.1%]), GLP1 (20[6.7%]), sulfnoylureas (7[2.3%]) and glinides (3[1.0%]). There was no significant difference in the total daily dose of insulin used between patients with T2DM with and without COVID-19 infection. Compared with T2DM patients without COVID-19 infection, patients with COVID-19 were less likely to use metformin (88[64.7%] vs 10[6.2%]; p<0.01), thiazolidinediones (30[22.1%] vs 0[0%]; p<0.01) and SGLT2 (66[48.5%] vs 5[3.2%]; p<0.01) (Table 3).
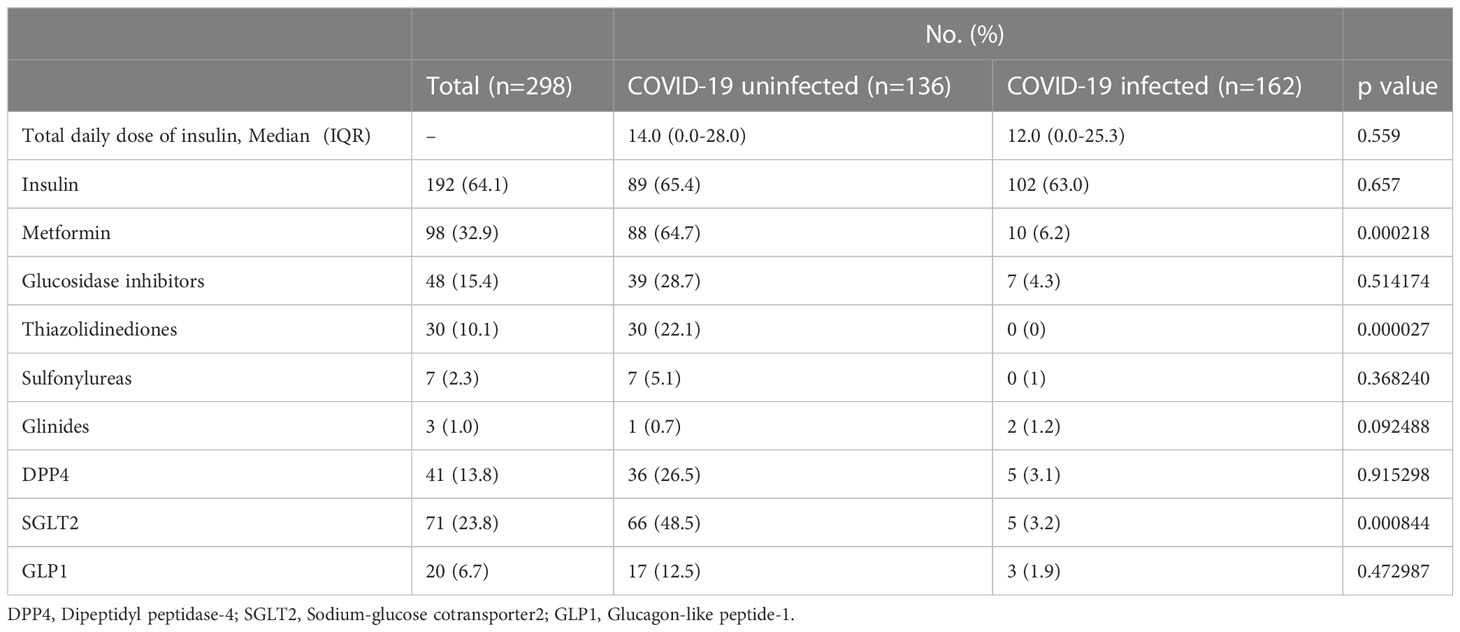
Table 3 Comparison of treatments between COVID-19 infected and uninfected diabetic patients.
This study was a retrospective study of 298 hospitalized T2DM patients with or without COVID-19 infection, and analyzed baseline data, clinical symptoms, acute complications, laboratory findings, treatment measures and outcome data. From the present results, the severity of T2DM patients with COVID-19 would be higher than those without COVID-19. This may be related to angiotensin-converting enzyme 2 (ACE2), whose expression is elevated in T2DM patients. SARS-CoV-2 binds to ACE2 receptors and can cause multiple organ damage. Moreover, high blood glucose activates inflammatory pathways and increases oxidative damage, impairing immune cell function (13, 14).
In many COVID-19 epidemic studies, COVID-19 with diabetes mostly occurred in the elderly (12, 15)..Recent studies have also indicated that the older the age of T2DM patients with COVID-19 is, the higher the incidence of severe clinical courses and increased mortality (16, 17). In the study, T2DM patients with COVID-19 had a longer duration of diabetes, indicating that this group of people was at higher risk from COVID-19 infection, which was consistent with the characteristics of such patients in other articles (18, 19). The cause was partly attributed to the immune system being impaired due to metabolic inflammation and the body’s ability to deal with infections being reduced in patients with diabetes.
Diabetes is associated with hyperglycemia, and the common symptoms are polyuria, polydipsia, polyphagia and weight loss (20). Consistently, the data of this study showed that these symptoms were the most common in T2DM patients with or without COVID-19. Our study also found that cough was also common in T2DM patients with or without COVID-19, and we speculated that type 2 diabetes may be related to an increased prevalence of respiratory symptoms (21).
Hyperglycemia can trigger an inflammatory response, which leads to structural changes in lung tissue and impaired lung function (22). Such structural changes may also be associated with an increased risk of hospitalization for pneumonia in patients with diabetes (23). The occurrence of fatigue in T2DM patients is also related to the inflammatory response (24), and they showed high levels of inflammatory markers including IL-6, CRP, and neopterin, which plays a role in causing fatigue in T2DM patients (25). Compared to T2DM patients without COVID-19, T2DM patients with COVID-19 had significantly more cough, fatigue, fever, muscle soreness, sore throat and shortness of breath. Studies have shown that patients with COVID-19 have significantly higher numbers of neutrophils (10) and elevated levels of inflammation-related biomarkers (26), which suggests that patients with diabetes are prone to develop an inflammatory storm that ultimately leads to worse symptoms of COVID-19. In addition, oxidative stress caused by persistent hyperglycemia was considered to be the main cause of lung injury in diabetes (27). Patients with diabetes tend to have lower forced vital capacity (FVC) and forced expiratory volume within one second, as well as lower diffusion capacity, which contributes to more severe COVID-19 symptoms (28). Dizziness and nausea were also common in T2DM patients with or without COVID-19, which could be partly explained by diabetic autonomic neuropathy and hypoglycemia caused by T2DM (29, 30). Compared with T2DM patients without COVID-19, hyposmia and hypogeusia were almost exclusively found in COVID-19 patients. Previous studies have shown that 41% and 38% of patients with COVID-19 have hyposmia and hypogeusia, respectively (31). The exact mechanism of hypogeusia and hyposmia in COVID-19 infected patients is not clear, and studies have noted that it may be related to the neuroinvasive potential of SARS-CoV-2 (32). Interestingly, the eating habits of T2DM patients with COVID-19 also changed - they became more polyophagous. This may be related to the COVID-19 lockdown and hyposmia. In a study from Italy, patients experienced a significant increase in appetite due to disruptions in daily work due to the COVID-19 lockdown and stress caused by reading news about COVID-19 from the media (33). Another study showed that patients were unable to perceive taste and flavor, resulting in no sensation of satiation and thus increased appetite (34).
Laboratory findings indicated that the level of creatinine significantly increased in patients with COVID-19, suggesting that kidney damage may have occurred. In a previous cohort study of 5,449 patients admitted to the hospital with COVID-19, 1,993(36.6%) patients developed AKI (35). However, the exact mechanism of COVID-19 on the kidney is unknown, and may be related to the direct damage of SARS-CoV-2 to renal tubules. SARS coronaviruses (including SARS-CoV-2) are detected in urine by PCR, which indicates that the virus interacts directly with or is exposed to renal tubules (36, 37). Furthermore, ACE as a viral receptor is only expressed in the proximal renal tubules, which is parallel to the damaged site of the kidney in patients with SARS-CoV infection (37, 38). Although the median values of creatinine in our study were still within the normal range, they were far from the extent of AKI. However, the difference between the exposure group and the non-exposure group was large, and the present study identified elevated creatinine as a significant predictor of all outcomes of interest (mortality, ICU admission and intubation), which needs to be considered (39).
We found higher ketones and higher rates of diabetic ketoacidosis in T2DM patients with COVID-19 infected, as has been reported in other research. Ketosis occurred in 6.4% of patients with COVID-19 and increased to 11.6% in patients with COVID-19 and diabetes, resulting in a higher mortality rate (33.3%) (40). In a CORONADO study, 11.1% of participants reported diabetes-related disorders at admission, including 40 cases of ketosis, 19 of which were ketoacidosis (2). ACE receptors are expressed in pancreatic tissue and β-cells, and SARS-CoV-2 has been found to bind to ACE2 receptors. Therefore, the metabolic disorders, including DKA may be caused by decreased insulin secretion due to severe insulin resistance and β-cell dysfunction (41, 42). For an unusually high number of patients with COVID-19 developing diabetic ketoacidosis and a hyperosmolar hyperglycemic state, a guideline has been released for the management of DKA (43).
In fact, T2DM patients with COVID-19 are most recommended to be treated with insulin (44). However, our results showed no significant difference between the exposure group and non-exposure group, which may be related to the fact that the proportion of hospitalized patients using insulin therapy was already quite high. From the reported results, T2DM patients with COVID-19 were less likely to use metformin, sodium-glucose transporter-2 inhibitor (SGLT-2i) and thiazolidinediones than patients without COVID-19 infection. This may be associated with insulin therapy reduced expression of ACE2, while metformin, glucagon-like peptide-1 agonists and thiazolidinediones up-regulate ACE2 expression (45). Furthermore, practical recommendations indicated that discontinuing of metformin and SGLT-2i is recommended in patients with diabetes who have a severe course of COVID-19 (42). In randomized controlled trials, the risk of DKA after SGLT2 use was two times higher in patients with T2DM than in controls (46). In our results patients with DKA and increased creatinine were numerous in the exposure group and the use of metformin required close monitoring for acidosis and decreased renal function, so there was a decrease in metformin use. However, previous studies have shown that metformin and SGLT-2i are associated with reduced mortality in patients with COVID-19 and type 2 diabetes, possibly due to reduced release of inflammatory cytokines, so metformin and SGLT-2i can be used for asymptomatic and mild COVID-19 patients (42, 47). Thiazolidinediones have been found to reduce markers of inflammation in COVID-19 patients (48). However, as a second or even third line treatment, metformin is not explicitly recommended for T2DM patients with COVID-19, which may be the reason why it was not used in the exposure group in our study.
The strengths of this study are that it was a multicenter study with an adequate sample size and comprehensive clinical records. Furthermore, to the best of our knowledge, this is the first study to investigate the clinical characteristics and outcomes of hospitalized COVID-19 patients with diabetes in southern China since the COVID-19 policy adjustment. Our study also has certain limitations. First, it is difficult to assess risk factors for poor prognosis due to short-term outcome follow-up. Second, cases with mild symptoms who were treated at home were missed, so this study only represents patients with more severe COVID-19.
In conclusion, COVID-19 patients with diabetes showed more severe respiratory and constitutional symptoms and an increased proportion of hyposmia and hypogeusia. Moreover, T2DM patients with COVID-19 have a higher incidence of acute complications, are more prone to worsening renal function, and are more cautious about the use of antidiabetic drugs.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Fifth Affiliated of Guangzhou Medical University Research Ethics Committee (GYWY-L2023-64). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
C-pZ and W-pS performed the general development and design of the study and contributed to critical revisions. X-yZ is the first author who contributed to the design, statistical analysis and manuscript writing of the study. S-fH wrote sections of the manuscript. S-fH, J-xL, H-nZ, LX, X-zW, K-hG, LZ, TL, H-mY, M-rL, and X-yL contributed to data collection and helped perform the analysis with constructive discussion. All authors contributed to the article and approved the submitted version.
We thank all staff in department of endocrinology in The Fifth Affiliated Hospital of Guangzhou Medical University, Loudi Central Hospital and The First People’s Hospital of Xiangtan.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Tian D, Nie W, Sun Y, Ye Q. The epidemiological features of the SARS-CoV-2 omicron subvariant BA.5 and its evasion of the neutralizing activity of vaccination and prior infection. Vaccines (Basel) (2022) 10(10):6. doi: 10.3390/vaccines10101699
2. Cariou B, Hadjadj S, Wargny M, Pichelin M, Al-Salameh A, Allix I, et al. Phenotypic characteristics and prognosis of inpatients with COVID-19 and diabetes: the CORONADO study. Diabetologia (2020) 63(8):1500–15. doi: 10.1007/s00125-020-05180-x
3. Shi Q, Zhang X, Jiang F, Zhang X, Hu N, Bimu C, et al. Clinical characteristics and risk factors for mortality of COVID-19 patients with diabetes in Wuhan, China: A two-center, retrospective study. Diabetes Care (2020) 43(7):1382–91. doi: 10.2337/dc20-0598
4. Singh AK, Khunti K. COVID-19 and diabetes. Annu Rev Med (2022) 73:129–47. doi: 10.1146/annurev-med-042220-011857
5. Wang L, Gao P, Zhang M, Huang Z, Zhang D, Deng Q, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA (2017) 317(24):2515–23. doi: 10.1001/jama.2017.7596
6. Mithal A, Jevalikar G, Sharma R, Singh A, Farooqui KJ, Mahendru S, et al. High prevalence of diabetes and other comorbidities in hospitalized patients with COVID-19 in Delhi, India, and their association with outcomes. Diabetes Metab Syndr (2021) 15(1):169–75. doi: 10.1016/j.dsx.2020.12.029
7. Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA (2020) 323(20):2052–9. doi: 10.1001/jama.2020.6775
8. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (2020) 395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5
9. Kamrath C, Monkemoller K, Biester T, Rohrer TR, Warncke K, Hammersen J, et al. Ketoacidosis in children and adolescents with newly diagnosed type 1 diabetes during the COVID-19 pandemic in Germany. JAMA (2020) 324(8):801–4. doi: 10.1001/jama.2020.13445
10. Guo W, Li M, Dong Y, Zhou H, Zhang Z, Tian C, et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab Res Rev (2020) 36(7):e3319. doi: 10.1002/dmrr.3319
11. Wu CT, Lidsky PV, Xiao Y, Lee IT, Cheng R, Nakayama T, et al. SARS-CoV-2 infects human pancreatic beta cells and elicits beta cell impairment. Cell Metab (2021) 33(8):1565–1576 e5. doi: 10.1016/j.cmet.2021.05.013
12. Muller JA, Gross R, Conzelmann C, Kruger J, Merle U, Steinhart J, et al. SARS-CoV-2 infects and replicates in cells of the human endocrine and exocrine pancreas. Nat Metab (2021) 3(2):149–65. doi: 10.1038/s42255-021-00347-1
13. Aluganti Narasimhulu C, Singla DK. Mechanisms of COVID-19 pathogenesis in diabetes. Am J Physiol Heart Circ Physiol (2022) 323(3):H403–20. doi: 10.1152/ajpheart.00204.2022
14. Pelle MC, Zaffina I, Provenzano M, Moirano G, Arturi F. COVID-19 and diabetes-Two giants colliding: From pathophysiology to management. Front Endocrinol (Lausanne) (2022) 13:974540. doi: 10.3389/fendo.2022.974540
15. Chen Y, Yang D, Cheng B, Chen J, Peng A, Yang C, et al. Clinical characteristics and outcomes of patients with diabetes and COVID-19 in association with glucose-lowering medication. Diabetes Care (2020) 43(7):1399–407. doi: 10.2337/dc20-0660
16. Yan Y, Yang Y, Wang F, Ren H, Zhang S, Shi X, et al. Clinical characteristics and outcomes of patients with severe covid-19 with diabetes. BMJ Open Diabetes Res Care (2020) 8(1). doi: 10.1136/bmjdrc-2020-001343
17. McGurnaghan SJ, Weir A, Bishop J, Kennedy S, Blackbourn LAK, McAllister DA, et al. Risks of and risk factors for COVID-19 disease in people with diabetes: a cohort study of the total population of Scotland. Lancet Diabetes Endocrinol (2021) 9(2):82–93. doi: 10.1016/S2213-8587(20)30405-8
18. Baidya A, Singh SK, Bajaj S, Zargar AH, Singh P, Das S, et al. Diabetes and COVID-19: A review. J ASEAN Fed Endocr Soc (2020) 35(1):40–8. doi: 10.15605/jafes.035.01.06
19. Conway J, Gould A, Westley R, Raju SA, Oklopcic A, Broadbent A, et al. Characteristics of patients with diabetes hospitalised for COVID-19 infection-a brief case series report. Diabetes Res Clin Pract (2020) 169:108460. doi: 10.1016/j.diabres.2020.108460
20. Vieira R, Souto SB, Sanchez-Lopez E, Machado AL, Severino P, Jose S, et al. Sugar-lowering drugs for type 2 diabetes mellitus and metabolic syndrome-strategies for in Vivo administration: Part-II. J Clin Med (2019) 8(9):1. doi: 10.3390/jcm8091332
21. De Santi F, Zoppini G, Locatelli F, Finocchio E, Cappa V, Dauriz M, et al. Type 2 diabetes is associated with an increased prevalence of respiratory symptoms as compared to the general population. BMC Pulm Med (2017) 17(1):101. doi: 10.1186/s12890-017-0443-1
22. Glaser S, Kruger S, Merkel M, Bramlage P, Herth FJ. Chronic obstructive pulmonary disease and diabetes mellitus: a systematic review of the literature. Respiration (2015) 89(3):253–64. doi: 10.1159/000369863
23. Klein OL, Smith LJ, Tipping M, Peng J, Williams MV. Reduced diffusion lung capacity in patients with type 2 diabetes mellitus predicts hospitalization for pneumonia. Diabetes Res Clin Pract (2011) 92(1):e12–5. doi: 10.1016/j.diabres.2010.12.012
24. Bi Y, Zhang L, Li X, Kan Y, Li S, Zou Y, et al. Contributing factors of fatigue in patients with type 2 diabetes: A systematic review. Psychoneuroendocrinology (2021) 130:105280. doi: 10.1016/j.psyneuen.2021.105280
25. Stewart KJ. Role of exercise training on cardiovascular disease in persons who have type 2 diabetes and hypertension. Cardiol Clin (2004) 22(4):569–86. doi: 10.1016/j.ccl.2004.06.007
26. Wang Z, Du Z, Zhu F. Glycosylated hemoglobin is associated with systemic inflammation, hypercoagulability, and prognosis of COVID-19 patients. Diabetes Res Clin Pract (2020) 164:108214. doi: 10.1016/j.diabres.2020.108214
27. Zheng H, Wu J, Jin Z, Yan LJ. Potential biochemical mechanisms of lung injury in diabetes. Aging Dis (2017) 8(1):7–16. doi: 10.14336/AD.2016.0627
28. Klein OL, Krishnan JA, Glick S, Smith LJ. Systematic review of the association between lung function and Type 2 diabetes mellitus. Diabetes Med (2010) 27(9):977–87. doi: 10.1111/j.1464-5491.2010.03073.x
29. Freeman J. Management of hypoglycemia in older adults with type 2 diabetes. Postgrad Med (2019) 131(4):241–50. doi: 10.1080/00325481.2019.1578590
30. Vinik AI, Maser RE, Mitchell BD, Freeman R. Diabetic autonomic neuropathy. Diabetes Care (2003) 26(5):1553–79. doi: 10.2337/diacare.26.5.1553
31. Agyeman AA, Chin KL, Landersdorfer CB, Liew D, Ofori-Asenso R. Smell and taste dysfunction in patients with COVID-19: A systematic review and meta-analysis. Mayo Clin Proc (2020) 95(8):1621–31. doi: 10.1016/j.mayocp.2020.05.030
32. Li YC, Bai WZ, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol (2020) 92(6):552–5. doi: 10.1002/jmv.25728
33. Di Renzo L, Gualtieri P, Pivari F, Soldati L, Attina A, Cinelli G, et al. Eating habits and lifestyle changes during COVID-19 lockdown: an Italian survey. J Transl Med (2020) 18(1):229. doi: 10.1186/s12967-020-02399-5
34. Hoier A, Chaaban N, Andersen BV. Possibilities for maintaining appetite in recovering COVID-19 patients. Foods (2021) 10(2):13. doi: 10.3390/foods10020464
35. Hirsch JS, Ng JH, Ross DW, Sharma P, Shah HH, Barnett RL, et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int (2020) 98(1):209–18. doi: 10.1016/j.kint.2020.05.006
36. Chu KH, Tsang WK, Tang CS, Lam MF, Lai FM, To KF, et al. Acute renal impairment in coronavirus-associated severe acute respiratory syndrome. Kidney Int (2005) 67(2):698–705. doi: 10.1111/j.1523-1755.2005.67130.x
37. Soleimani M. Acute kidney injury in SARS-coV-2 infection: Direct effect of virus on kidney proximal tubule cells. Int J Mol Sci (2020) 21(9):2. doi: 10.3390/ijms21093275
38. Soler MJ, Wysocki J, Batlle D. ACE2 alterations in kidney disease. Nephrol Dial Transplant (2013) 28(11):2687–97. doi: 10.1093/ndt/gft320
39. Alguwaihes AM, Al-Sofiani ME, Megdad M, Albader SS, Alsari MH, Alelayan A, et al. Diabetes and Covid-19 among hospitalized patients in Saudi Arabia: a single-centre retrospective study. Cardiovasc Diabetol (2020) 19(1):205. doi: 10.1186/s12933-020-01184-4
40. Li J, Wang X, Chen J, Zuo X, Zhang H, Deng A. COVID-19 infection may cause ketosis and ketoacidosis. Diabetes Obes Metab (2020) 22(10):1935–41. doi: 10.1111/dom.14057
41. Hamming I, Timens W, Bulthuis ML, Lely AT, Navis G, van Goor H, et al. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol (2004) 203(2):631–7. doi: 10.1002/path.1570
42. Bornstein SR, Rubino F, Khunti K, Mingrone G, Hopkins D, Birkenfeld AL, et al. Practical recommendations for the management of diabetes in patients with COVID-19. Lancet Diabetes Endocrinol (2020) 8(6):546–50. doi: 10.1016/S2213-8587(20)30152-2
43. Rayman G, Lumb A, Kennon B, Cottrell C, Nagi D, Page E, et al. Guidance on the management of Diabetic Ketoacidosis in the exceptional circumstances of the COVID-19 pandemic. Diabetes Med (2020) 37(7):1214–6. doi: 10.1111/dme.14328
44. Lim S, Bae JH, Kwon HS. COVID-19 and diabetes mellitus: from pathophysiology to clinical management. Nat Rev Endocrinol (2021) 17(1):11–30. doi: 10.1038/s41574-020-00435-4
45. Sinha S, Cheng K, Schaffer AA, Aldape K, Schiff E, Ruppin E, et al. In vitro and in vivo identification of clinically approved drugs that modify ACE2 expression. Mol Syst Biol (2020) 16(7):e9628. doi: 10.15252/msb.20209628
46. Scheen AJ. SGLT2 inhibition during the COVID-19 epidemic: Friend or foe? Diabetes Metab (2020) 46(5):343–4. doi: 10.1016/j.diabet.2020.06.003
47. Nguyen NN, Ho DS, Nguyen HS, Ho DKN, Li HY, Lin CY, et al. Preadmission use of antidiabetic medications and mortality among patients with COVID-19 having type 2 diabetes: A meta-analysis. Metabolism (2022) 131:155196. doi: 10.1016/j.metabol.2022.155196
Keywords: COVID-19, diabetes, clinical characteristics, acute complications, renal insufficiency
Citation: Zhou X-y, Huang S-f, Lin J-x, Zhi H-n, Xiao L, Wang X-z, Guo K-h, Zhou L, Long T, You H-m, Lin M-r, Luo X-y, Sun W-p and Zeng C-p (2023) Clinical characteristics and acute complication of COVID-19 patients with diabetes: a multicenter, retrospective study in Southern China. Front. Endocrinol. 14:1237832. doi: 10.3389/fendo.2023.1237832
Received: 10 June 2023; Accepted: 27 July 2023;
Published: 14 August 2023.
Edited by:
Pranav Kumar Prabhakar, Lovely Professional University, IndiaReviewed by:
Naina Mohamed Pakkir Maideen, Dubai Health Authority, United Arab EmiratesCopyright © 2023 Zhou, Huang, Lin, Zhi, Xiao, Wang, Guo, Zhou, Long, You, Lin, Luo, Sun and Zeng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chun-ping Zeng, emNwMTkzQDE2My5jb20=; Wei-ping Sun, c3Vud3AwN0AxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.