 Vince Fazekas-Pongor1†
Vince Fazekas-Pongor1† Mark M. Svébis2†
Mark M. Svébis2† David Major1
David Major1 Katalin Pártos1Norbert Dósa1
Katalin Pártos1Norbert Dósa1 Ágota Mészáros1Viktor J. Horváth2Beatrix A. Domján2László Zsirai3
Ágota Mészáros1Viktor J. Horváth2Beatrix A. Domján2László Zsirai3 Adam G. Tabák1,2,4*
Adam G. Tabák1,2,4*- 1Department of Public Health, Faculty of Medicine, Semmelweis University, Budapest, Hungary
- 2Department of Internal Medicine and Oncology, Faculty of Medicine, Semmelweis University, Budapest, Hungary
- 3Department of Gynecology and Family Planning, Istenhegyi Gene Diagnostic Center, Budapest, Hungary
- 4University College London (UCL) Brain Sciences, University College London, London, United Kingdom
Introduction: In 1989, the St Vincent declaration aimed to approximate pregnancy outcomes of diabetes to that of healthy pregnancies. We aimed to compare frequency and trends of outcomes of pregnancies affected by type 1 diabetes and controls in 1996–2018.
Methods: We used anonymized records of a mandatory nation-wide registry of all deliveries between gestational weeks 24 and 42 in Hungary. We included all singleton births (4,091 type 1 diabetes, 1,879,183 controls) between 1996 and 2018. We compared frequency and trends of pregnancy outcomes between type 1 diabetes and control pregnancies using hierarchical Poisson regression.
Results: The frequency of stillbirth, perinatal mortality, large for gestational age, caesarean section, admission to neonatal intensive care unit (NICU), and low Appearance, Pulse, Grimace, Activity, and Respiration (APGAR) score was 2-4 times higher in type 1 diabetes compared to controls, while the risk of congenital malformations was increased by 51% and SGA was decreased by 42% (all p<0.05). These observations remained significant after adjustment for confounders except for low APGAR scores. We found decreasing rate ratios comparing cases and controls over time for caesarean sections, low APGAR scores (p<0.05), and for NICU admissions (p=0.052) in adjusted models. The difference between cases and controls became non-significant after 2009. No linear trends were observed for the other outcomes.
Conclusions: Although we found that the rates of SGA, NICU care, and low APGAR score improved in pregnancies complicated by type 1 diabetes, the target of the St Vincent Declaration was only achieved for the occurrence of low APGAR scores.
Introduction
Type 1 diabetes mellitus affects approximately 0.3% of pregnancies (1), and studies indicate that it is associated with a more frequent occurrence of several unwanted pregnancy outcomes (2, 3). Estimates show that adverse fetal outcomes, such as congenital malformations, perinatal mortality, preterm delivery, and large for gestational age infants (LGA), occur 2-5-fold more often among pregnancies affected by type 1 diabetes compared to healthy pregnancies (3). Furthermore, type 1 diabetes is also associated with other pregnancy-related adverse conditions, such as polyhydramnios, oligohydramnios (4), or more common occurrence of gestational hypertension and preeclampsia (5). As a result, pregnancies with type 1 diabetes require closer observation, and prospective mothers also undergo Caesarean section (C-section) more often with estimates going as high as 50% of pregnancies ending in surgery (3). In turn, infants born to mothers affected by type 1 diabetes require closer attention, as they often exhibit lower Appearance, Pulse, Grimace, Activity and Respiration Scores (APGAR) compared to their healthy counterparts (6) with up to 50% of infants being admitted to neonatal intensive care units (NICU) after delivery (3).
Since the incidence and prevalence of type 1 diabetes are increasing worldwide (7, 8), and this is accompanied by underlying changes in sociodemographic factors (for instance the continuous increase in maternal age and more frequent occurrence of births at earlier gestations) (9, 10) and the use of novel insulins, insulin delivery devices, and continuous glucose measurement devices, these changes may in turn also affect the trends of pregnancy outcomes in this subpopulation.
More than 30 years ago, diabetes specialists and healthcare policy makers approved the St Vincent declaration that set very ambitious targets and goals to substantially decrease disease burden and mortality related to diabetes (11). One area of these goals covered pregnancies complicated by diabetes: participants of the meeting unanimously agreed and pledged to approximate pregnancy outcomes of diabetes to that of healthy pregnancies (11). Since the declaration, however, very few studies have been conducted to actually test whether these goals have been met or to investigate the trajectories of outcomes of pregnancies complicated by type 1 diabetes both nationally and internationally. Thus, we aimed to investigate time trends of pregnancy outcomes in Hungary between 1996 and 2018 and to examine whether the targets outlined in the St Vincent declaration were achieved by comparing pregnancies affected by type 1 diabetes with pregnancies uncomplicated by type 1 diabetes using data of an anonymous registry of all deliveries in Hungary.
Materials and methods
Study design
The current report is based on the Tauffer registry that is a mandatory nation-wide registry of all deliveries in Hungary since the 1930s (4). Attending physicians are required to fill in a standardized, anonymous form after all deliveries between gestational weeks 24 and 42. Given that the database contains anonymous records, the identification of repeated deliveries by the same woman was not possible. The database is accessible in an electronic format for the years 1994 to 2018. For our present analysis, we included all singleton births between 1996 and 2018. The time restriction was used because underlying diseases are coded using the International Classification of Diseases (ICD) system, and its 10th revision was introduced in Hungary in 1996 (12).
The legal basis of the anonymized registry is the 76/2004 ESzCsM decree (Decree on the Determination, Collection, Analysis of Health-related Unidentifiable data; Ministry of Health Social and Family Affairs, Hungary). Data presented in this report were made available through a data sharing agreement with the National Institute for Quality and Organizational Development in Healthcare and Medicines that confirmed that no ethical approval is required.
Participants
Of the total of 2,133,727 births included in the Tauffer database between 1994 and 2018, we excluded 115,518 as these happened before 1996. We further excluded 34,143 twin pregnancies, 1,894 deliveries that had a gestational age recorded <24 or >42 weeks. Of the eligible 1,980,464 births, we excluded 98,878 cases due to missing information on outcomes or covariables. Thus, the final analytical sample consisted of 1,883,274 pregnancies (95.1% of those eligible, 4,091 affected by type 1 diabetes and 1,879,183 control pregnancies) (Figure 1).
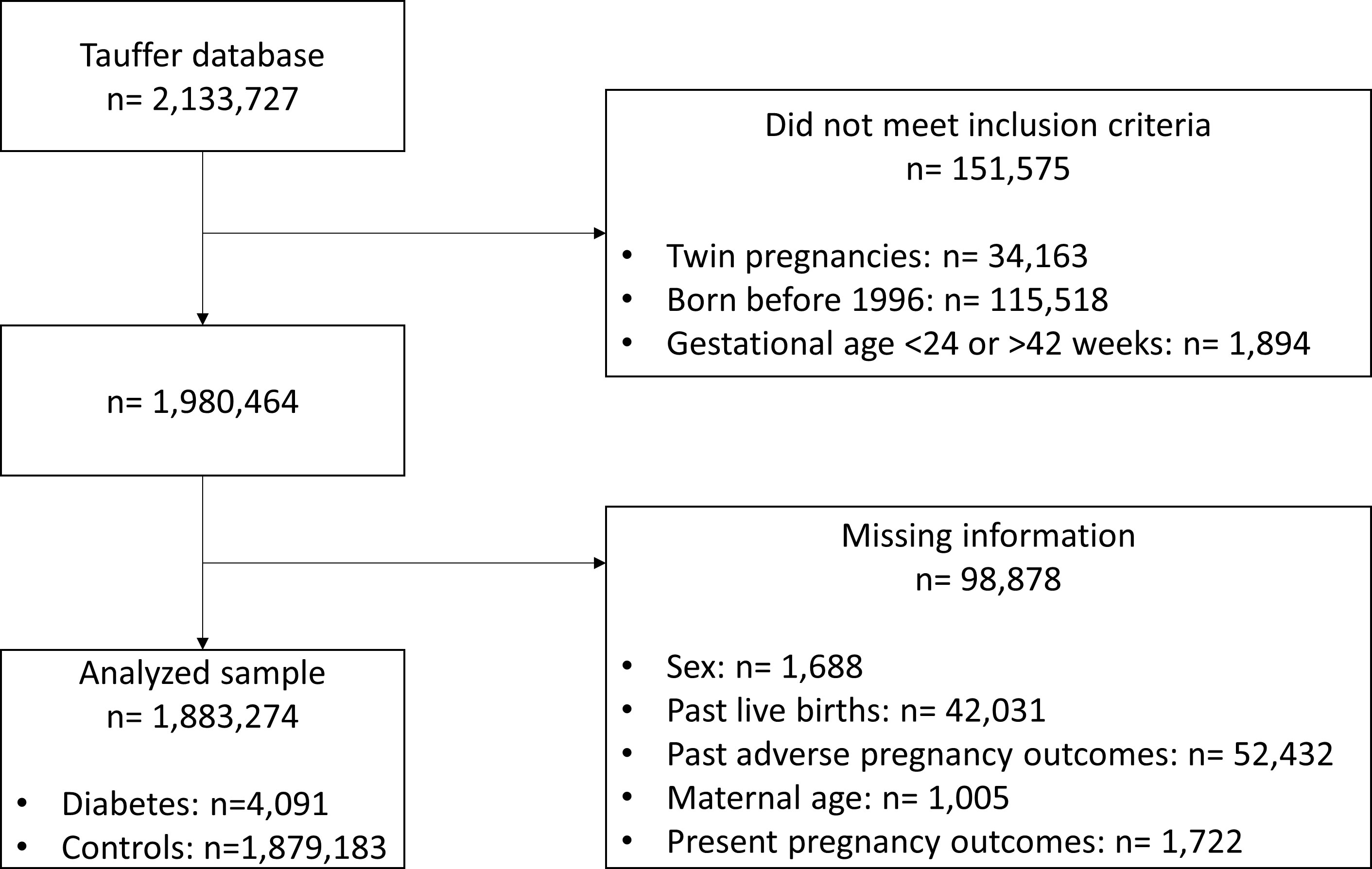
Figure 1 Flow chart of study participants.
Variables
Exposure
The main exposure for the current analysis is the presence of type 1 diabetes mellitus. For all information related to index pregnancies, data were extracted from hospital discharge reports. Data on known diseases/pathologies before and during the investigated pregnancy was based on ICD-10 codes. Type 1 diabetes was coded either as a preexisting disease (E10*) or as a complication of the index pregnancy (O240, O243, and O249). Controls were all pregnancies without a mention of the previous ICD-10 codes (13).
Outcomes
Regarding outcomes, there were separate dedicated questions for stillbirth, perinatal mortality (any death between week 24 of pregnancy and day 7 postpartum), C-section (elective or emergency), and admission to the neonatal intensive care unit (NICU). Congenital malformations (Q*) were recorded as a separate entry. Using birthweight, fetal sex, and gestational age at delivery, we calculated percentiles that were translated to small for gestational age (SGA, birthweight <10th percentile) and large for gestational age (LGA, birthweight >90th percentile) (14). Similarly, the 5-minute APGAR scores that were recorded in the database were coded as low APGAR scores if they were below 7.
Covariates
Maternal age was calculated as the difference between date of delivery and date of birth. Gestational age at delivery was based in most cases on the first trimester crown-rump length or was calculated from the date of the last menstrual period. Newborn sex was based on the phenotype at birth. From the detailed account of past pregnancy histories, we extracted the following variables: past induced and spontaneous abortions, past stillbirths, and past livebirths (all coded as yes/no variables). Using the previous variables, we created a variable describing prior adverse pregnancy outcome if the history contained either a stillbirth or an abortion. Primary maternal hypertension (I10*, I11*, I12*, I15*) was recorded as a preexisting disease or complication of the index pregnancy (O10*, O11*, O16*).
Statistical analysis
Given that the database contains anonymous records and thus the identification of repeated deliveries by the same woman cannot be identified, we assumed that outcomes could be correlated between repeated pregnancies and consequently the independence of observations may not hold true. Thus, for all estimations we used either bootstrapping or robust estimators.
Descriptive analysis
Descriptive statistics comparing pregnancies complicated by type 1 diabetes with control pregnancies was performed using independent sample t-tests for continuous variables and Chi-squared tests for categorical variables. Furthermore, we looked for temporal trends in descriptive variables within type 1 diabetes and control pregnancies. For this analysis, we decided to divide the 1996–2018 period into three periods (1996–2002, 2003–2010, 2011–2018). Heterogeneity and linear trends within the 3 periods were calculated with logistic regression for categorical variables and one-Way ANOVA for continuous variables.
Pregnancy outcome analysis
First, we compared pregnancy outcomes of pregnancies complicated by type 1 diabetes and controls using Poisson regression for the entire observation period. We calculated unadjusted and adjusted rate ratios (RR) with their respective 95% confidence intervals (95% CI). For the adjusted analysis, 2 different models were constructed. In Model 1, outcomes were adjusted for gestational age (linear, quadratic, and cubic terms), sex of the infant, and age of the mother (linear and quadratic terms). Model 2 was further adjusted for the presence of prior adverse pregnancy outcome, prior livebirth, and pre-pregnancy hypertension. Then, we calculated rate ratios with respective 95% CIs using Poisson regression for each of the 3 time periods and investigated whether there was any heterogeneity or a linear trend over time. For this analysis, we also provide unadjusted and adjusted estimates as described previously. For those outcomes where a linear trend was likely (p<0.10) in the adjusted models (meaning that the relative difference either increased or decreased between cases and controls over time), we ran an additional Poisson regression model where calendar time was treated as a continuous variable. For this model, we added calendar time (linear, quadratic, and cubic terms) and an interaction between calendar time and presence of type 1 diabetes (linear term) as covariates in addition to variables in Model 1. We then calculated estimated marginal means for the proportion of the given pregnancy outcomes for each calendar year with respective 95% CIs and present them as band charts.
Sensitivity analysis
To overcome the potential multilevel structure of the data, we ran a sensitivity analysis exclusively on first pregnancies (thus here we excluded records with a livebirth or abortion in the medical history).
All analyses were conducted in IBM SPSS Statistics version 28.0.1 (IBM, Armonk, NY, US). Significance was set at p<0.05.
Results
Descriptive statistics
Altogether, 0.22% of all pregnancies were affected by type 1 diabetes. The proportion was stable in the first two periods at 0.20% but increased by 36% (OR: 1.36 95% CI: 1.26-1.46) in the last period to 0.26%.
Mothers affected by type 1 diabetes were 2.7 years older and gave birth more than a week earlier, although the sex distribution of the newborns were similar in cases and controls. Past pregnancy history revealed that mothers affected by type 1 diabetes were 14% (OR: 0.86, 95% CI: 0.81-0.92) less likely to be primi- or multiparas, but more likely to have had pregnancies ending with stillbirth (OR: 2.61, 95% CI: 2.04-3.34) or to have undergone either spontaneous (OR: 1.75, 95% CI: 1.62-1.88) or induced abortions (OR: 1.10, 95% CI: 1.02-1.19). Primary hypertension occurred more than 4 times more often among pregnancies affected by type 1 diabetes compared to control pregnancies (OR: 4.81, 95% CI: 4.00-5.78) (Table 1).

Table 1 Baseline characteristics of pregnant women stratified by type 1 diabetes status in 1996–2018.
When investigating trends in descriptive characteristics in women with type 1 diabetes and controls over the three time periods, we found significant linear increases or decreases for all descriptive characteristics except for infant sex in controls and infant sex, primi- or multiparity, and history of induced abortions for type 1 diabetes. Maternal age increased by over 3 years, while the occurrence of primary hypertension more than doubled in both groups. The frequency of primi- or multiparity increased and past induced abortion decreased only in controls, while past stillbirth decreased, and history of spontaneous abortion increased in both cases and controls (Table 2).
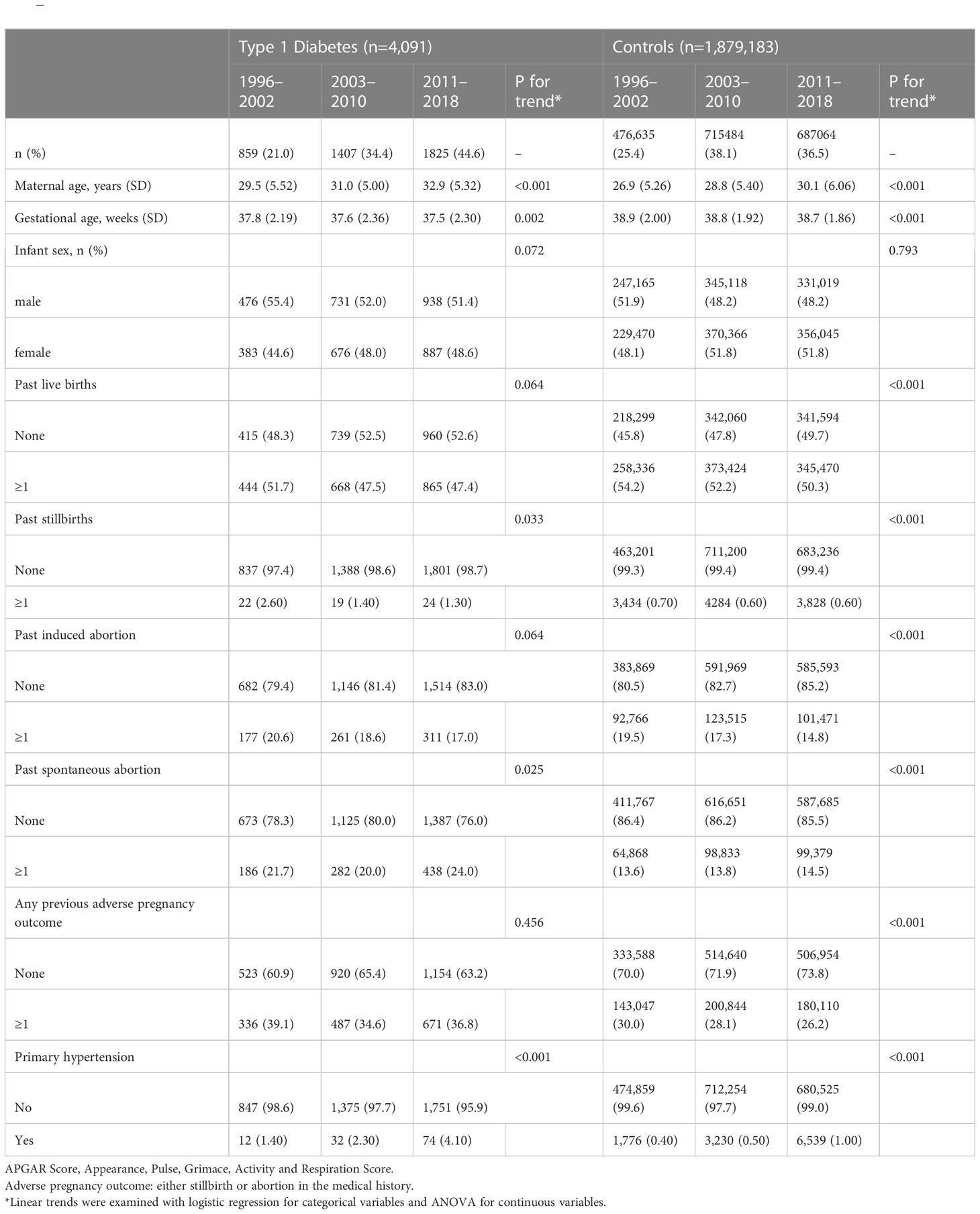
Table 2 Temporal trends in baseline characteristics of pregnant women by type 1 diabetes status over 3 time periods (1996–2002, 2003–2010, 2011–2018).
Pregnancy outcomes
According to our unadjusted analyses, the frequency of all outcomes was significantly different in cases and controls. The frequency of stillbirth, perinatal mortality, LGA, C-section, admission to NICU, and low APGAR score was 2-4 times higher in type 1 diabetes pregnancies compared to controls, while the risk of congenital malformations was increased by only 51% and the risk of SGA was decreased by 42%. These observations remained significant after adjustment for potential confounders across all outcomes except for low APGAR Scores, which showed similar risks in cases and controls in the full model. More marked attenuation was found for stillbirth, perinatal mortality, NICU treatment, and APGAR score (>50% reduction in model betas), while the change was smaller for the other outcomes (Table 3).
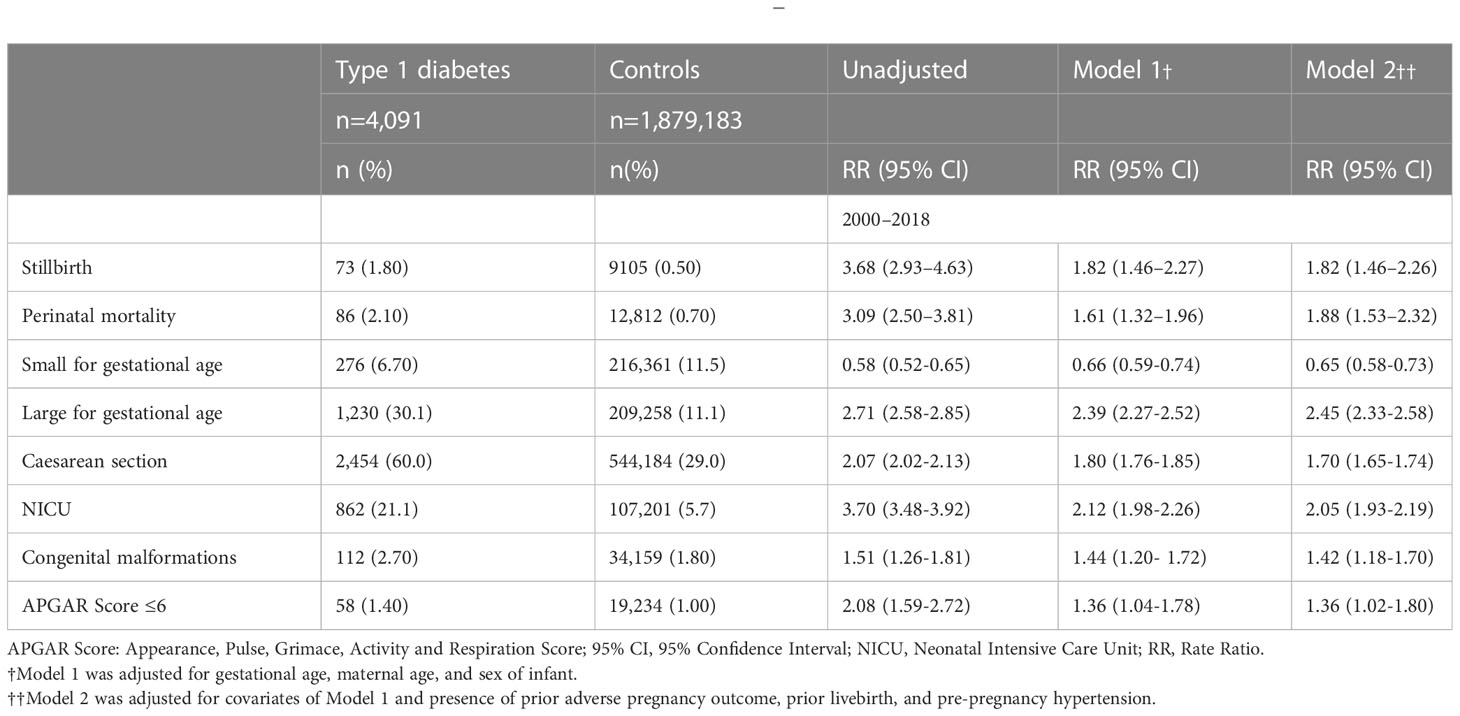
Table 3 Rate ratios for different pregnancy outcomes based on Poisson regression with hierarchical adjustment for potential confounders in singleton pregnancies affected by type 1 diabetes compared to controls in 1996–2018.
When we looked for time trends over the 3 time periods, we found significant linear trends for all outcomes in controls: decreasing trends for stillbirth, perinatal mortality, SGA, and NICU treatment, while increasing for LGA, C-section, congenital malformations, and low APGAR score. As for pregnancies affected by type 1 diabetes, decreasing trends were observed for low APGAR score and increasing trend for C-section, and non-significant (p<0.1) increase in LGA and decrease in SGA, NICU care, and low APGAR score (Tables 4, 5).
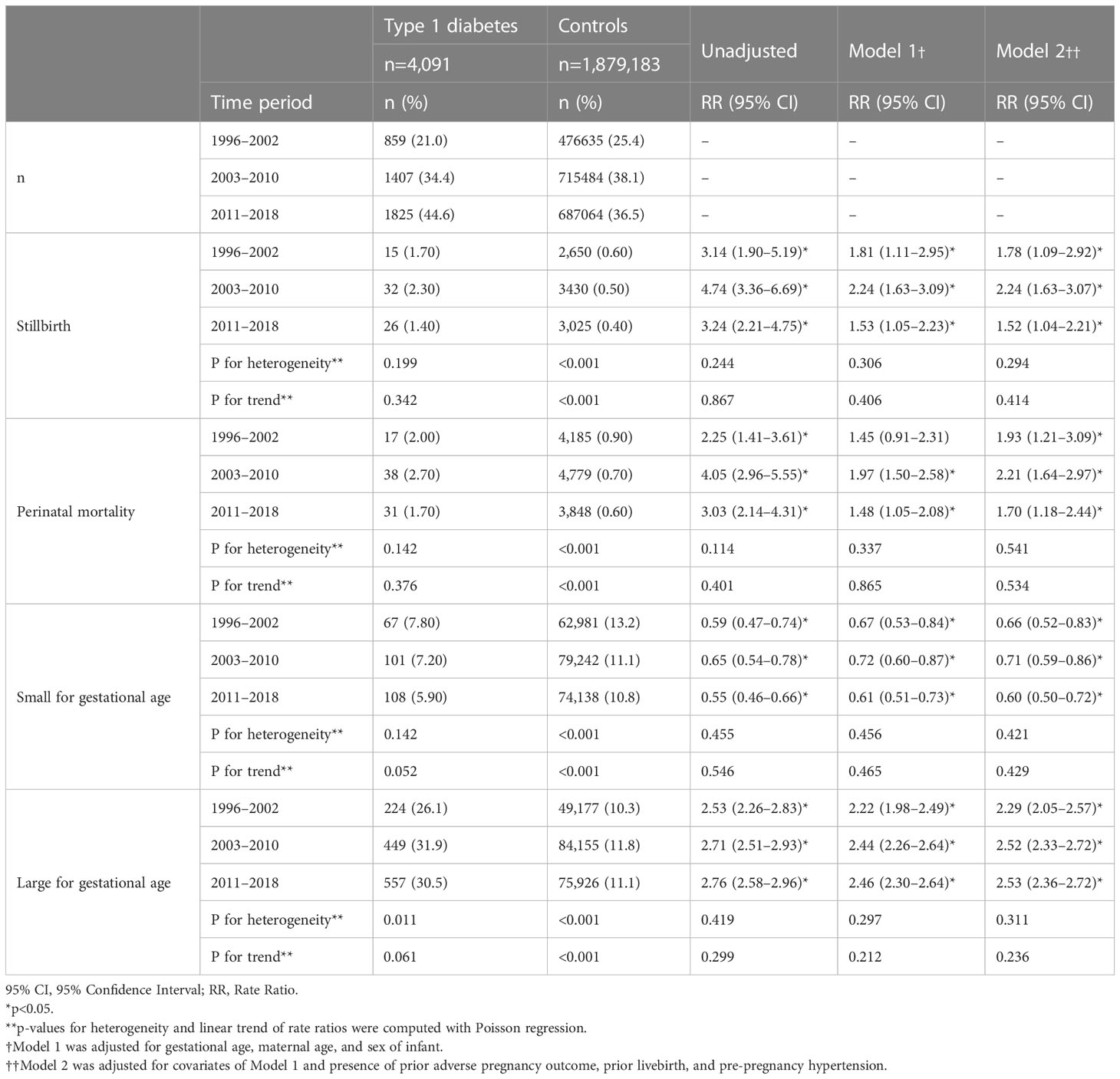
Table 4 Rate ratios for different pregnancy outcomes based on Poisson regression with hierarchical adjustment for potential confounders in singleton pregnancies affected by type 1 diabetes compared to controls over 3 time periods (1996–2002, 2003–2010, 2011–2018).
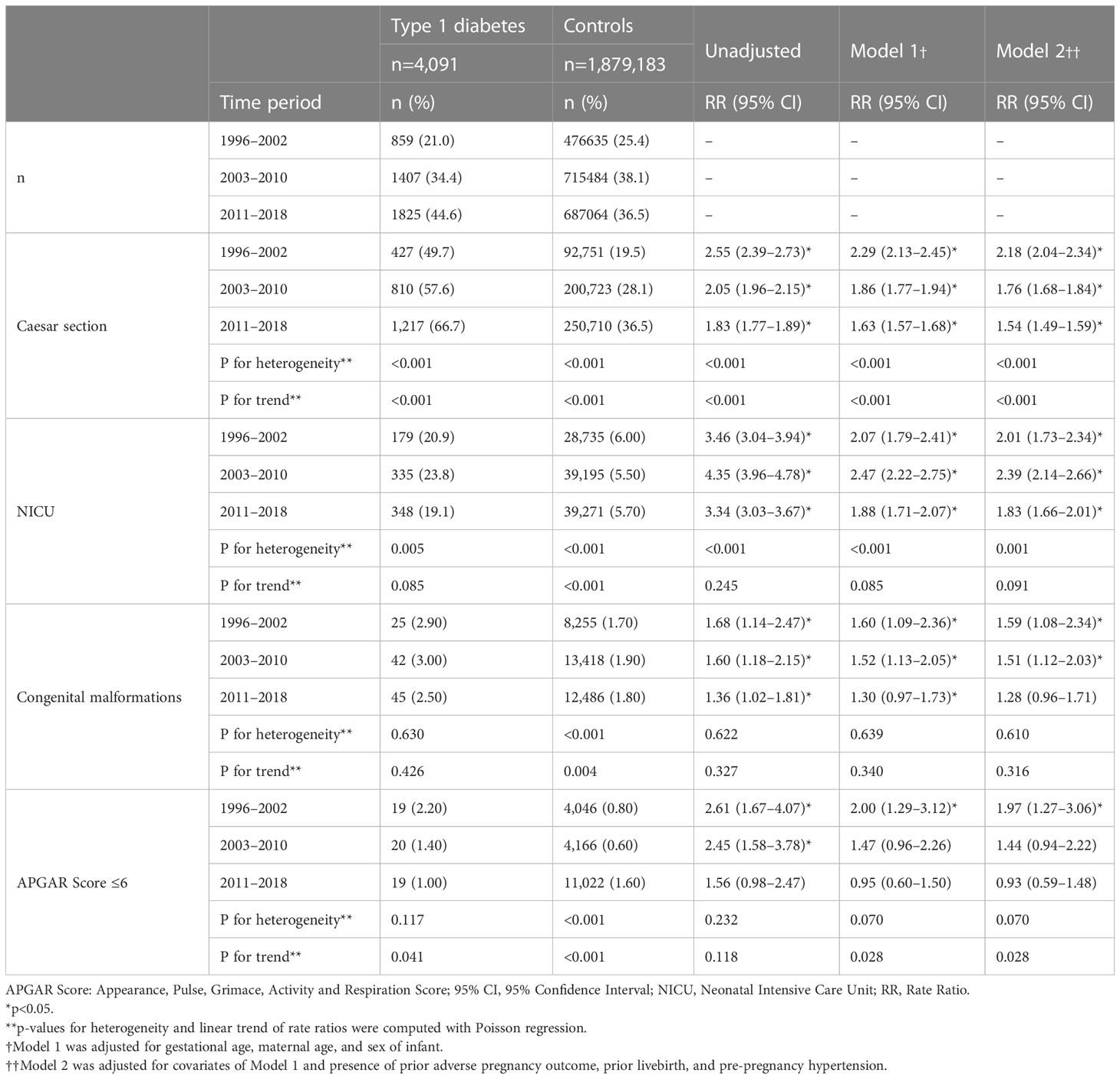
Table 5 Rate ratios for different pregnancy outcomes based on Poisson regression with hierarchical adjustment for potential confounders in singleton pregnancies affected by type 1 diabetes compared to controls over 3 time periods (1996–2002, 2003–2010, 2011–2018).
When investigating trends in the RRs comparing cases and controls, we found a significant decrease for only C-sections in unadjusted models showing that the difference between cases and controls decreased over the observation period although the risk remained elevated in cases compared to controls even at the end of the observation period. This observation still holds in the adjusted models. Furthermore, we found that the RRs significantly decreased for low APGAR scores in the adjusted models and became non-significant in the 3rd period. The figure showing the estimated marginal means shows that the gap decreased over the observation period and the confidence intervals were overlapping after 2009 (Tables 4, 5; Figures 2, 3). Although the gap decreased for admissions to NICU, the time by diabetes interaction term remained non-significant (p=0-052), indicating a possible power issue (Figure 4).
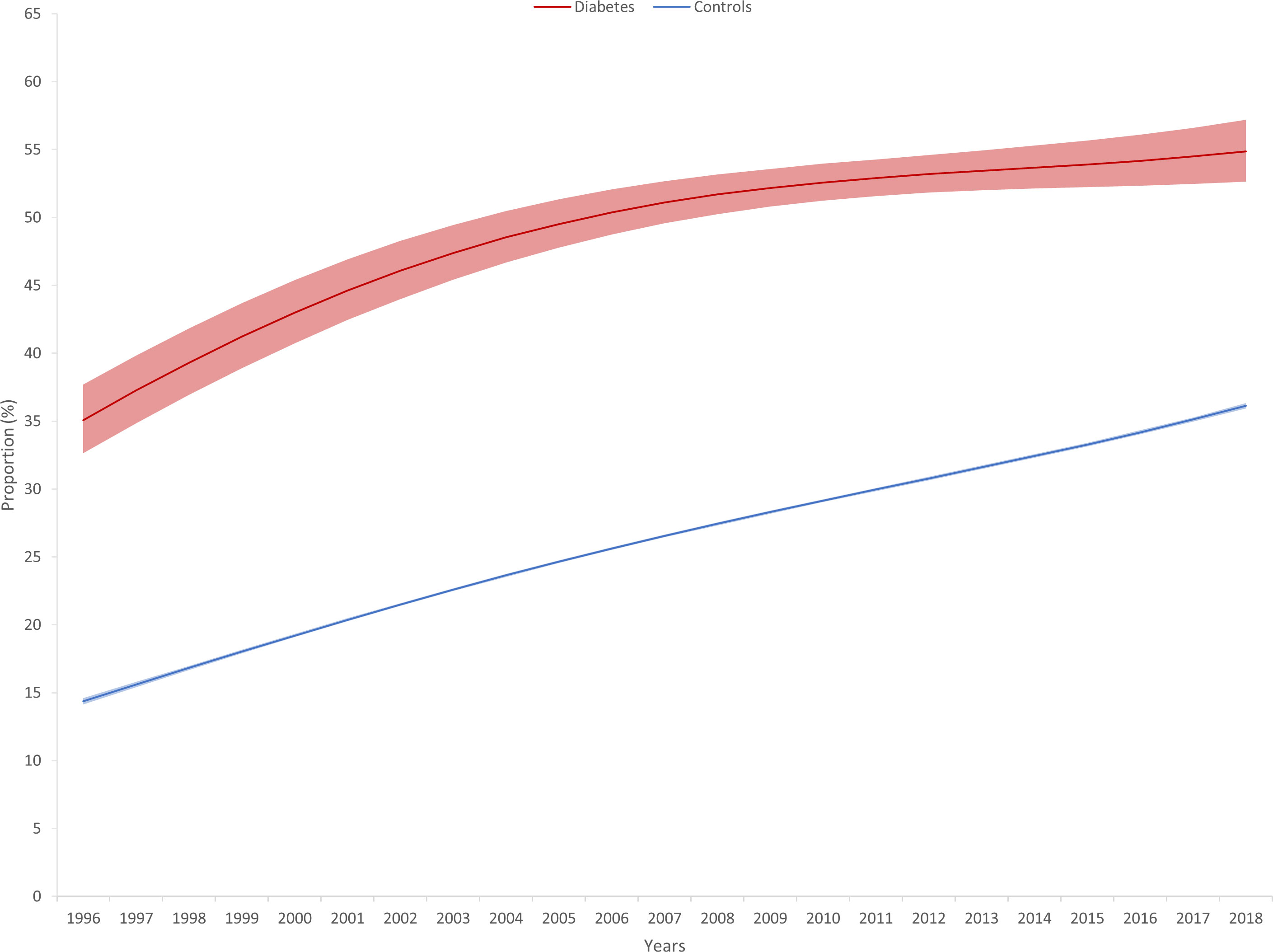
Figure 2 Estimated frequency of Caesarian sections (with 95% confidence intervals) based on Poisson regression with adjustment for gestational age at delivery, maternal age, and infant sex in singleton pregnancies affected by type 1 diabetes and controls from 1996 to 2018.
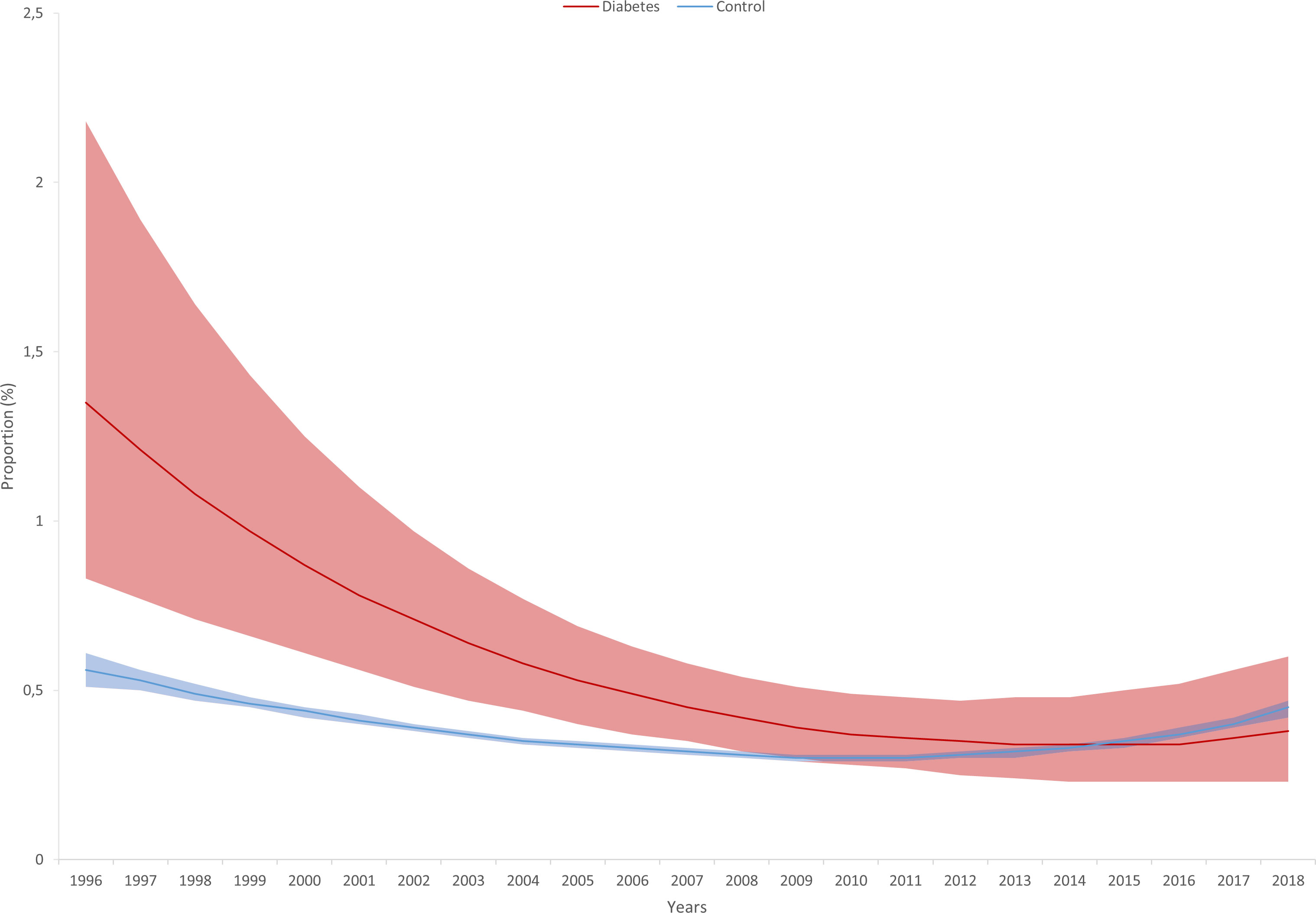
Figure 3 Estimated frequency of low APGAR (Appearance, Pulse, Grimace, Activity and Respiration) score (with 95% confidence intervals) based on Poisson regression with adjustment for gestational age at delivery, maternal age, and infant sex in singleton pregnancies affected by type 1 diabetes and controls from 1996 to 2018.
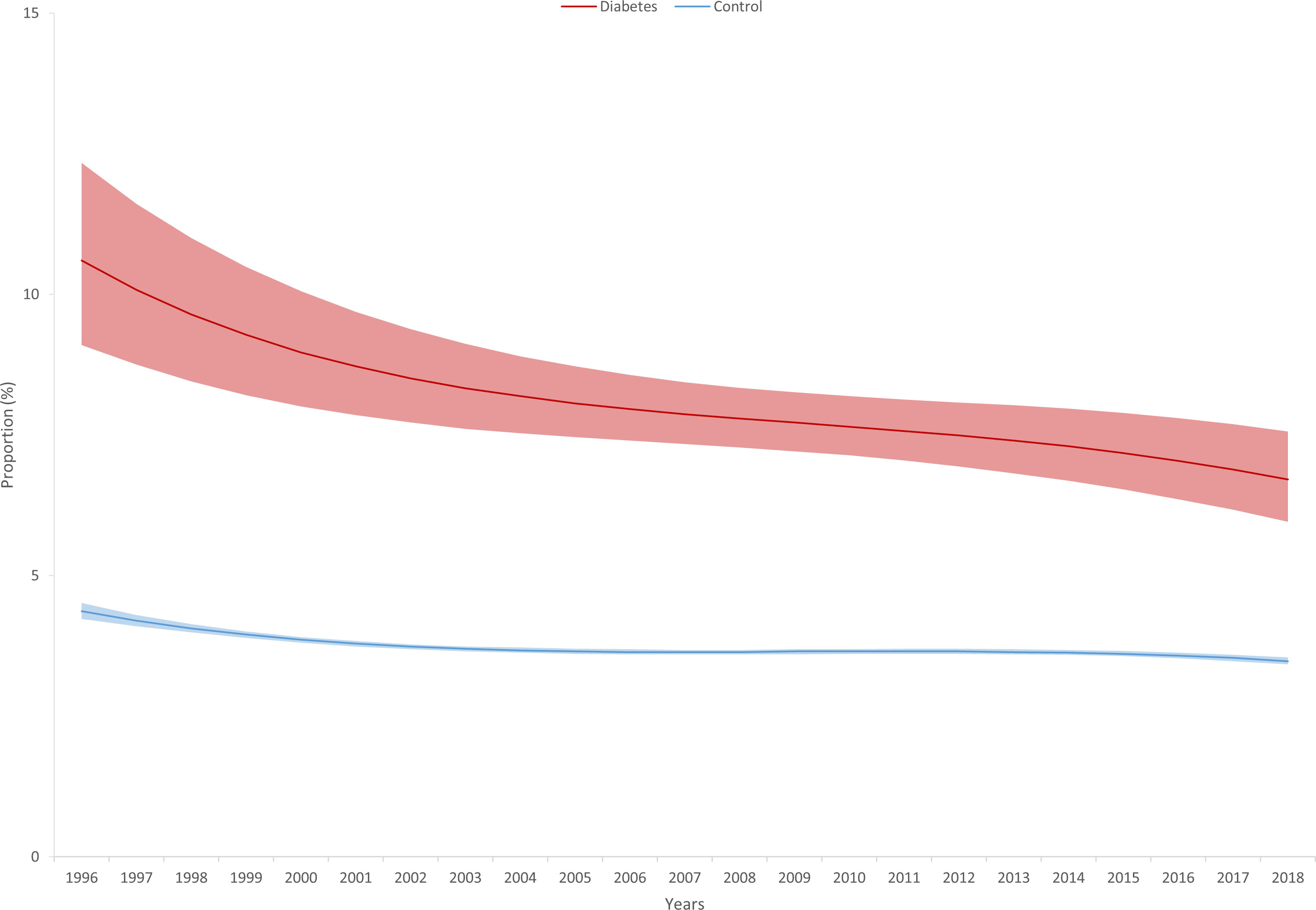
Figure 4 Estimated frequency of admission to neonatal infant care unit (with 95% confidence intervals) based on Poisson regression with adjustment for gestational age at delivery, maternal age, and infant sex in singleton pregnancies affected by type 1 diabetes and controls from 1996 to 2018.
Sensitivity analysis
Our sensitivity analysis on primiparas largely confirmed our main analysis on the point estimates, although, given the lower statistical power, some of the differences became non-significant (Supplement Tables 1, 2).
Discussion
Based on an analysis of approximately 4,000 singleton pregnancies complicated by type 1 diabetes and over 1.8 million controls over 23 years between 1996–2018, we found a 2-4 times elevated risk of stillbirth, perinatal mortality, LGA, C-section, requirement of NICU care, and low APGAR score in type 1 diabetes that was partly explained by the fact that type 1 diabetes patients were older, delivered earlier, and had a more frequently adverse pregnancy outcomes in their medical history. The risk of congenital malformations was only increased by approximately 50% and was less affected by adjustment. The risk of SGA was significantly lower by 42% compared to controls.
Over time, the risk of stillbirth, perinatal mortality, SGA, and NICU care improved for controls, while the risk of LGA, C-section, congenital malformation, and low APGAR score increased in unadjusted models. As for pregnancies affected by type 1 diabetes, the risk of LGA, C-section, and risk of NICU care changed in the same direction as in controls, while the risk of low APGAR scores decreased over time. Adjusted rate ratios that take into account changes of population characteristics over time, showed similar changes in both populations between 1996 and 2018 with the exception of decreasing rate ratios for C-section, low APGAR scores (p<0.05), and NICU treatment (p=0.052). While the difference between cases and controls for C-sections and NICU care remained significant throughout the observation period, the risk of low APGAR scores became similar in cases and controls after 2009.
Our results for the frequency of adverse pregnancy outcomes in the background population roughly support the observations made for Hungary in other studies. In our population, the occurrence of stillbirth was 1.8% in type 1 diabetes and 0.5% in control pregnancies. According to the results of the European Perinatal Health Report 2015–2019 (EPHR), Hungary ranks 25th in Europe with its 4.3 stillbirths per 1000 births (median: 3.2 per 1000 births, IQR: 2.8–3.8) (15). The occurrence of SGA was 8.2% in Hungary that was also high compared to the 4% to 11% range in Europe (15). Our findings showed an even higher rate of SGA (11.5%) that probably relates to the fact that we used a newer percentile chart on the whole population (14). Conversely, LGA affected approximately 10% of pregnancies based on a study summarizing the results of 15 European countries (16). In our study, LGA affected 11.1% of healthy pregnancies, again probably related to the use of the newest percentile tables. As for C-sections, Hungary ranks 25th in Europe with its 41.5 C-sections per 1000 births (median: 26 per 1000 births IQR: 20.7–32.1) (15).
Our observations made regarding the higher risk of all investigated pregnancy outcomes in the population affected by type 1 diabetes are corroborated by other studies. Specifically, both the absolute risk of stillbirth (1.8%) and the relative risk (3.7) compared to controls well corresponds to observations from other high income countries from the early 90s to 2010s (17–25). Similarly, the observed rates and relative risk of perinatal mortality of 2.1% and 3.09 completely overlaps with reports from the literature (17–22, 24, 25). In our study population, the risk of SGA was decreased in type 1 diabetes compared to controls. Although this outcome is relatively infrequently reported, there is some support for our finding (20). In our study, LGA affected 11.1% of healthy pregnancies, while for type 1 diabetes the estimate ran as high as 29.8% translating to a relative risk of 2.71. While the literature mostly confirms the increased risk of LGA in type 1 diabetes pregnancies, both the absolute and relative risks seem to be generally higher, with absolute risks going as high as 63% and RRs up to 11.5 (6, 20, 21, 25, 26). The risk of C-section was doubled in type 1 diabetes compared to controls in our study that is line with other observations of increased risks from other countries. However, the RRs are not easy to compare, given the wide range of C-sections in the general population across high income countries (6, 21, 26–28). Similarly, the risk of NICU admission is increased in type 1 diabetes according to both our observations and the literature (6, 28). In general, the rate of congenital anomalies was found to be elevated in type 1 diabetes pregnancies compared to controls both in our study and in previous observations. However, direct comparisons with the literature are hindered by the fact that we excluded deliveries terminating before 24 weeks of gestation leading to lower absolute and relative risks compared to the literature (17, 19, 21, 24, 28). Median APGAR scores are lower, as well as the risk of a low APGAR score is increased in type 1 diabetes compared to controls confirming our observations (27–29).
Major characteristics of our study population changed substantially from 1996 to 2018. The age of mothers with and without type 1 diabetes increased similarly by ~3 years. Similar observations are available for other high-income countries (15, 30–33). At the same time, we observed decreasing parity in both type 1 diabetes and controls, similarly to other European countries (15, 30). Furthermore, a decreasing gestational age at delivery seems to be universal finding in our and other studies (10, 15, 34). The increasing age of pregnant women is probably the driver of the more frequent occurrence of primary hypertension. Furthermore, measures of obesity (although we do not have this measure in our database) are also showing increasing trends both in people with and without type 1 diabetes concurrent with our study period in Hungary and elsewhere in Europe that may also increase the risk of adverse pregnancy outcomes and concurrent diseases (32, 35). As type 1 diabetes patients and controls have different baseline characteristics, and these characteristics may change differently in cases and controls, it is extremely important to eliminate their effect when examining temporal changes in comparative risks between cases and controls.
Among healthy pregnancies, we observed beneficial decreasing trends in the rates of stillbirth, perinatal mortality, SGA, and the risk of NICU care that well corresponds to European and worldwide trends (15, 36). In contrast, rates of C-section, low APGAR score, and congenital malformations increased over time. While the frequency of C-sections and its temporal changes shows high heterogeneity within Europe, the increasing trend in Hungary seems to be continuing also for the last 5 years (10, 15). Although these increases could be partially linked to the increasing age, BMI, and consequently higher risk of comorbidities of the mothers, changes in C-sections may also be explained by a more frequent choice of C-sections over natural birth by either patients or physicians.
The trends of pregnancy outcomes showed a somewhat different picture for pregnancies affected by type 1 diabetes compared to controls. We found no significant changes in the risk of stillbirth, perinatal mortality, and congenital malformation. While these findings could partly be related to the limited power of our analysis for these relatively rare outcomes, it is notable that stillbirth and perinatal mortality remained stubbornly persistent in the UK and Canada between the mid-nineties and early 2000s, probably partly explained by the decreasing participation in antenatal care of participants (37, 38). Another study found an initial increase followed by a decrease in stillbirth risk in Norway from 1985 to 1998 that was related to improving diabetes management of type 1 diabetes (22). The prevention of congenital malformations requires good glycemic control in the early pregnancy period that highlights the importance of pre-pregnancy counselling and care (25). There is some evidence in the literature of decreasing trends of congenital malformations, however the observed trends did not exceed those in the background population (38–40). While the risk of LGA increased parallel to control pregnancies, the literature is equivocal on this outcome. While two studies reported increasing rates of LGA (21, 41), another study found no change despite improving protocols and medication regimens between the nineties and early 2000s (42). To decrease macrosomia, proper glycemic control seems to be important especially in the first trimester along with proper weight control of participants (42, 43). We found somewhat improving rates of SGA, NICU care, and low APGAR scores in type 1 diabetes pregnancies that well correspond to the findings of a Polish tertiary care center (41).
While the above results show overall changes in the actual number of events, they provide little information on how the risk would change over time if the population would remain stable. Our analyses on the trends of rate ratios of the outcomes adjusted for confounders help us answer these questions. We found that the rate ratios between type 1 diabetes and controls decreased for three of the outcomes (C-section, NICU care, and low APGAR score), while for the rest, the changes were similar in cases and controls. The decrease in the occurrence of low APGAR scores was not only more pronounced in type 1 diabetes, but it decreased to an extent that it was no longer significantly different between cases and controls. For C-section rates that increased both in cases and controls, the increase was less pronounced in type 1 diabetes. Similarly, the decrease in NICU care was faster in cases compared to controls. These beneficial changes may reflect an improvement in overall pregnancy care protocols, glycemic control, and delivery procedures (41). It should be noted that these outcomes are less strongly related to early glycemic control compared to congenital malformations. Proper glycemic control has been linked to decreasing rates of other negative pregnancy outcomes: every 1% reduction of HbA1c is associated with an approximately 50% reduction in the risk of unwanted pregnancy outcomes (25). However HbA1c alone is not necessarily the only measure that should be used to monitor therapeutic goals, as mothers with normal HbA1c levels may still have a higher risk of adverse pregnancy outcomes (25). To approximate the pregnancy outcomes of the population affected by diabetes to that of healthy pregnancies, in addition to optimal glycemic control, participation in antenatal care, and administration of supplements, such as folic acid, should also be implemented as part of a multidisciplinary care program (25).
Our study has limitations that have to be acknowledged. Even though the included population is very large, for some rare outcomes, our trend analyses have a limited statistical power and thus important differences may remain unobserved. As we used registry data, misdiagnosis and misclassification of outcomes and predictors is a possibility. It should be noted, however that the Tauffer registry is not used for reimbursement purposes and thus selective misclassification (an important source of bias) is unlikely. Furthermore, we had no information on potentially important confounders, such as smoking, social status, measures of obesity. Given that we used anonymized data, we could not adjust for the multilevel structure of the data, although the use of bootstrapping and robust confidence intervals gives us some support that our findings are valid. Due to the lack of information on glycemic control, blood pressure, and other biological variables, we could not investigate causal biological factors behind the observed changes.
Major strengths of our study include its large sample size and long follow-up. Actually, ours is one of the longest studies investigating trends in pregnancy outcomes in type 1 diabetes compared to the background population. Given that most variables in our analysis are mandatory fields in the database, we could include almost all singleton births in Hungary between 1996 and 2018. Moreover, our main and sensitivity analyses showed similar findings that further confirm the robustness of our observations. Furthermore, the investigation of nulliparas allowed us to remove the multilevel structure of the data.
Conclusion
In conclusion, although we found that the rates of some outcomes (such as SGA, NICU care, and low APGAR score) improved in pregnancies complicated by type 1 diabetes, the risk of LGA and C-sections increased during the over 20-year observation period. Participating countries of the St Vincent Declaration, unanimously agreed to approximate pregnancy health outcomes of pregnancies complicated by type 1 diabetes to that of healthy pregnancies in 1989. However, we only found that this target was achieved for the occurrence of low APGAR scores. Furthermore, we found decreasing differences in terms of C-sections and NICU care but despite these beneficial trends, significant differences remained between type 1 diabetes cases and controls. To achieve all targets of the St Vincent Declaration, further improvements are required in pre-pregnancy and pregnancy management and care of women with type 1 diabetes.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
AT conceptualized and designed the study. Analysis and interpretation were handled by all authors. AT, VF-P, and MS wrote the first draft of the manuscript. All authors took critical part in the revision process. All authors provide approval for publication of the content and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This research did not receive and specific grant from funding agencies in the public, commercial, or not-for-profit sectors. AT was supported by the UK Medical Research Council (S011676). AT and VF-P were supported by project no. TKP2021-NKTA-47, implemented with the support provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund, financed under the TKP2021-NKTA funding scheme and a project through the National Cardiovascular Laboratory Program (RRF-2.3.1-21-2022-00003) provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund and the European University for Well-Being (EUniWell) program (grant agreement number: 101004093/EUniWell/EAC-A02-2019/EAC-A02-2019-1). The funding sources had no role in the interpretation of data, the writing of the report, and the decision to submit the article for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1232618/full#supplementary-material
References
1. Coton SJ, Nazareth I, Petersen I. A cohort study of trends in the prevalence of pregestational diabetes in pregnancy recorded in UK general practice between 1995 and 2012. BMJ Open (2016) 6(1):e009494. doi: 10.1136/bmjopen-2015-009494
2. Murphy HR, Howgate C, O’Keefe J, Myers J, Morgan M, Coleman MA, et al. Characteristics and outcomes of pregnant women with type 1 or type 2 diabetes: a 5-year national population-based cohort study. Lancet Diabetes Endocrinol (2021) 9(3):153–64. doi: 10.1016/S2213-8587(20)30406-X
3. McCance DR, Casey C. Type 1 diabetes in pregnancy. Endocrinol Metab Clin North Am (2019) 48(3):495–509. doi: 10.1016/j.ecl.2019.05.008
4. Zsirai L, Csákány GM, Vargha P, Fülöp V, Tabák ÁG. Breech presentation: its predictors and consequences. An analysis of the Hungarian tauffer obstetric database (1996–2011). Acta Obstetricia Gynecologica Scand (2016) 95(3):347–54. doi: 10.1111/aogs.12834
5. Holmes VA, Young IS, Patterson CC, Pearson DWM, Walker JD, Maresh MJA, et al. Optimal glycemic control, pre-eclampsia, and gestational hypertension in women with type 1 diabetes in the diabetes and pre-eclampsia intervention trial. Diabetes Care (2011) 34(8):1683–8. doi: 10.2337/dc11-0244
6. Seah JM, Kam NM, Wong L, Tanner C, Shub A, Houlihan C, et al. Risk factors for pregnancy outcomes in type 1 and type 2 diabetes. Intern Med J (2021) 51(1):78–86. doi: 10.1111/imj.14840
7. Mobasseri M, Shirmohammadi M, Amiri T, Vahed N, Hosseini Fard H, Ghojazadeh M. Prevalence and incidence of type 1 diabetes in the world: a systematic review and meta-analysis. Health Promot Perspect (2020) 10(2):98–115. doi: 10.34172/hpp.2020.18
8. Abela AG, Fava S. Why is the incidence of type 1 diabetes increasing? Curr Diabetes Rev (2021) 17(8):e030521193110. doi: 10.2174/1573399817666210503133747
9. Driscoll AK, Ely DM. Effects of changes in maternal age distribution and maternal age-specific infant mortality rates on infant mortality trends: united states, 2000-2017. Natl Vital Stat Rep (2020) 69(5):1–18.
10. Nassar N, Schiff M, Roberts CL. Trends in the distribution of gestational age and contribution of planned births in new south Wales, Australia. PloS One (2013) 8(2):e56238. doi: 10.1371/journal.pone.0056238
11. Platt MJ, Stanisstreet M, Casson IF, Howard CV, Walkinshaw S, Pennycook S, et al. St Vincent’s declaration 10 years on: outcomes of diabetic pregnancies. Diabetes Med (2002) 19(3):216–20. doi: 10.1046/j.1464-5491.2002.00665.x
12. Classification - BNO-X: Hungarian central statistics office. Available at: https://www.ksh.hu/classification_bno_x.
13. Organization WH. International statistical classification of diseases and related health problems. 10th revision. Fifth edition. Geneva: World Health Organization (2015).
14. Zsirai L, Csákány MG, Végh G, Tabák G. [Distribution of birth weights between 2011 and 2015 and changes in percentile figures between 1996 and 2015. analyis of the tauffer database. Orv Hetil (2019) 160(36):1426–36. doi: 10.1556/650.2019.31481
15. European Perinatal health report: EuroPeristat (2019). Available at: https://www.europeristat.com/images/Euro-Peristat_Fact_sheets_2022_for_upload.pdf.
16. Hocquette A, Durox M, Wood R, Klungsøyr K, Szamotulska K, Berrut S, et al. International versus national growth charts for identifying small and large-for-gestational age newborns: a population-based study in 15 European countries. Lancet Reg Health Eur (2021) 8:100167. doi: 10.1016/j.lanepe.2021.100167
17. Casson IF, Clarke CA, Howard CV, Mckendrick O, Pennycook S, Pharoah POD, et al. Outcomes of pregnancy in insulin dependent diabetic women: results of a five year population cohort study. BMJ (1997) 315(7103):275–8. doi: 10.1136/bmj.315.7103.275
18. Penney GC, Mair G, Pearson DWM. Outcomes of pregnancies in women with type 1 diabetes in Scotland: a national population-based study. BJOG: Int J Obstet Gynaecol (2003) 110(3):315–8. doi: 10.1046/j.1471-0528.2003.02067.x
19. Jensen DM, Damm P, Moelsted-Pedersen L, Ovesen P, Westergaard JG, Moeller M, et al. Outcomes in type 1 diabetic pregnancies: a nationwide, population-based study. Diabetes Care (2004) 27(12):2819–23. doi: 10.2337/diacare.27.12.2819
20. Silva IDS, Higgins C, Swerdlow AJ, Laing SP, Slater SD, Pearson DWM, et al. Birthweight and other pregnancy outcomes in a cohort of women with pre-gestational insulin-treated diabetes mellitus, Scotland, 1979-95. Diabetic Med (2005) 22(4):440–7. doi: 10.1111/j.1464-5491.2005.01434.x
21. Persson M, Norman M, Hanson U. Obstetric and perinatal outcomes in type 1 diabetic pregnancies. Diabetes Care (2009) 32(11):2005–9. doi: 10.2337/dc09-0656
22. Eidem I, Vangen S, Hanssen KF, Vollset SE, Henriksen T, Joner G, et al. Perinatal and infant mortality in term and preterm births among women with type 1 diabetes. Diabetologia (2011) 54(11):2771–8. doi: 10.1007/s00125-011-2281-7
23. Lauenborg J, Mathiesen E, Ovesen P, Westergaard JG, Ekbom P, Mølsted-Pedersen L, et al. Audit on stillbirths in women with pregestational type 1 diabetes. Diabetes Care (2003) 26(5):1385–9. doi: 10.2337/diacare.26.5.1385
24. Lapolla A, Dalfrà MG, Di Cianni G, Bonomo M, Parretti E, Mello G. A multicenter Italian study on pregnancy outcome in women with diabetes. Nutr Metab Cardiovasc Dis (2008) 18(4):291–7. doi: 10.1016/j.numecd.2006.12.001
25. Colstrup M, Mathiesen ER, Damm P, Jensen DM, Ringholm L. Pregnancy in women with type 1 diabetes: have the goals of st. Vincent declaration been met concerning foetal and neonatal complications? J Matern Fetal Neonatal Med (2013) 26(17):1682–6. doi: 10.3109/14767058.2013.794214
26. Stogianni A, Lendahls L, Landin-Olsson M, Thunander M. Obstetric and perinatal outcomes in pregnancies complicated by diabetes, and control pregnancies, in kronoberg, Sweden. BMC Pregnancy Childbirth (2019) 19(1):159. doi: 10.1186/s12884-019-2269-8
27. Mitrović M, Stojić S, Tešić DS, Popović D, Rankov O, Naglić DT, et al. The impact of diabetes mellitus on the course and outcome of pregnancy during a 5-year follow-up. Vojnosanit Pregl (2014) 71(10):907–14. doi: 10.2298/VSP1410907M
28. Owens LA, Sedar J, Carmody L, Dunne F. Comparing type 1 and type 2 diabetes in pregnancy- similar conditions or is a separate approach required? BMC Pregnancy Childbirth (2015) 15:69. doi: 10.1186/s12884-015-0499-y
29. Persson M, Fadl H. Perinatal outcome in relation to fetal sex in offspring to mothers with pre-gestational and gestational diabetes–a population-based study. Diabetes Med (2014) 31(9):1047–54. doi: 10.1111/dme.12479
30. Pearce D, Cantisani G, Laihonen A. Changes in fertility and family sizes in Europe. Popul Trends (1999) 95):33–40.
31. Nabukera S, Wingate MS, Alexander GR, Salihu HM. First-time births among women 30 years and older in the united states: patterns and risk of adverse outcomes. J Reprod Med (2006) 51(9):676–82.
32. Strauss A, Rochow N, Kunze M, Hesse V, Dudenhausen JW, Voigt M. Obesity in pregnant women: a 20-year analysis of the German experience. Eur J Clin Nutr (2021) 75(12):1757–63. doi: 10.1038/s41430-021-00981-8
33. Cundy T, Slee F, Gamble G, Neale L. Hypertensive disorders of pregnancy in women with type 1 and type 2 diabetes. Diabetes Med (2002) 19(6):482–9. doi: 10.1046/j.1464-5491.2002.00729.x
34. Tilstra AM, Masters RK. Worth the weight? recent trends in obstetric practices, gestational age, and birth weight in the united states. Demography (2020) 57(1):99–121. doi: 10.1007/s13524-019-00843-w
35. Giandalia A, Russo GT, Ruggeri P, Giancaterini A, Brun E, Cristofaro M, et al. The burden of obesity in type 1 diabetic subjects: a sex-specific analysis from the AMD annals initiative. J Clin Endocrinol Metab (2023). doi: 10.1210/clinem/dgad302
36. Hug L, You D, Blencowe H, Mishra A, Wang Z, Fix MJ, et al. Global, regional, and national estimates and trends in stillbirths from 2000 to 2019: a systematic assessment. Lancet (2021) 398(10302):772–85. doi: 10.1016/S0140-6736(21)01112-0
37. Tennant PW, Glinianaia SV, Bilous RW, Rankin J, Bell R. Pre-existing diabetes, maternal glycated haemoglobin, and the risks of fetal and infant death: a population-based study. Diabetologia (2014) 57(2):285–94. doi: 10.1007/s00125-013-3108-5
38. Feig DS, Hwee J, Shah BR, Booth GL, Bierman AS, Lipscombe LL. Trends in incidence of diabetes in pregnancy and serious perinatal outcomes: a Large, population-based study in Ontario, Canada, 1996–2010. Diabetes Care (2014) 37(6):1590–6. doi: 10.2337/dc13-2717
39. Liu S, Rouleau J, León JA, Sauve R, Joseph KS, Ray JG. Impact of pre-pregnancy diabetes mellitus on congenital anomalies, Canada, 2002-2012. Health Promot Chronic Dis Prev Can (2015) 35(5):79–84. doi: 10.24095/hpcdp.35.5.01
40. Bánhidy F, Acs N, Puhó EH, Czeizel AE. Congenital abnormalities in the offspring of pregnant women with type 1, type 2 and gestational diabetes mellitus: a population-based case-control study. Congenit Anom (Kyoto) (2010) 50(2):115–21. doi: 10.1111/j.1741-4520.2010.00275.x
41. Wender-Ozegowska E, Gutaj P, Mantaj U, Kornacki J, Ozegowski S, Zawiejska A. Pregnancy outcomes in women with long-duration type 1 diabetes-25 years of experience. J Clin Med (2020) 9(10):3223. doi: 10.3390/jcm9103223
42. Al-Agha R, Firth RG, Byrne M, Murray S, Daly S, Foley M, et al. Outcome of pregnancy in type 1 diabetes mellitus (T1DMP): results from combined diabetes-obstetrical clinics in Dublin in three university teaching hospitals (1995-2006). Ir J Med Sci (2012) 181(1):105–9. doi: 10.1007/s11845-011-0781-6
Keywords: type 1 diabetes mellitus, pregnancy, trend, stillbirth, perinatal mortality, cesarean section, neonatal intensive care, APGAR score
Citation: Fazekas-Pongor V, Svébis MM, Major D, Pártos K, Dósa N, Mészáros Á, Horváth VJ, Domján BA, Zsirai L and Tabák AG (2023) Trend of pregnancy outcomes in type 1 diabetes compared to control women: a register-based analysis in 1996-2018. Front. Endocrinol. 14:1232618. doi: 10.3389/fendo.2023.1232618
Received: 31 May 2023; Accepted: 19 June 2023;
Published: 12 July 2023.
Edited by:
Katrien Benhalima, University Hospitals Leuven, BelgiumReviewed by:
Angela Napoli, Saint Camillus International University of Health and Medical Sciences, ItalyEwa Wender-Ozegowska, Poznan University of Medical Sciences, Poland
Copyright © 2023 Fazekas-Pongor, Svébis, Major, Pártos, Dósa, Mészáros, Horváth, Domján, Zsirai and Tabák. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adam G. Tabák, dGFiYWsuYWRhbUBzZW1tZWx3ZWlzLmh1
†These authors share first authorship