 Guangyao Lin
Guangyao Lin Xiufang Zhong2
Xiufang Zhong2 Lianwei Xu
Lianwei Xu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Endocrinol. , 07 November 2023
Sec. Reproduction
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1215755
This article is part of the Research Topic Growth Hormone in Fertility and Infertility: Physiology, Pathology, Diagnosis and Treatment, Volume II View all 8 articles
Objective: To appraise the current randomized clinical trials (RCTs) for evidence of the association of growth hormone (GH) with improved outcomes in infertile women with diminished ovarian reserve (DOR) undergoing in vitro fertilization (IVF).
Methods: Relevant RCTs published in Chinese or English were identified through a comprehensive search of nine databases from the period of database inception to April 20, 2023. We included trials investigating adjuvant GH during ovarian stimulation and reported the subsequent outcomes. The group with adjuvant GH treatment and the group without adjuvant GH treatment were set up as the trial and control groups, respectively. The quality of RCTs was measured according to the Cochrane Collaboration Handbook.
Results: Of the 579 studies initially identified, 10 RCTs comprising 852 infertile women with DOR were included. The GH dose of individual trials ranged between 3 and 5 IU/day. Overall, we judged the trials to be at high risk of bias in the blinding domain. Pooled results showed that GH was associated with an increased clinical pregnancy rate (RR = 1.63, 95%CI [1.31, 2.03], p < 0.0001) and a greater number of oocytes retrieved (MD = 0.91, 95%CI [0.47, 1.35], p < 0.0001). Favorable associations were also observed when ovarian stimulation was combined with GH therapy for improving the optimal embryos rate (RR = 1.84, 95%CI [1.30, 2.59], p = 0.0005) and the number of optimal embryos (MD = 0.28, 95%CI [0.08, 0.48], p = 0.005) along with reducing the cycle cancellation rate (RR = 0.46, 95%CI [0.24, 0.89], p = 0.02). Moreover, GH resulted in an increase in the fertilization rate (RR = 1.33, 95%CI [1.18, 1.50], p < 0.00001) and the embryo implantation rate (RR = 1.56, 95%CI [1.21, 2.01], p = 0.0006). In addition, there was a significant enhancement in estradiol levels (SMD = 1.18, 95%CI [0.46, 1.91], p = 0.001) and endometrial thickness (MD = 0.75, 95%CI [0.41, 1.09], p < 0.0001) on the day of hCG. With regard to the total number of days and total dose of gonadotrophins used, GH treatment was correlated with shorter days (MD = -0.26, 95%CI [-0.46, -0.06], p = 0.01) and lower dose (MD = -460.97, 95%CI [-617.20, -304.73], p < 0.00001) of gonadotrophins applied during ovarian stimulation. Furthermore, GH in conjunction with the GnRH antagonist protocol was more conducive to improving the number of oocytes retrieved when compared with the GnRH agonist protocol (p < 0.0001). Moreover, a notable association was also seen in IVF combined with GH more than or equal to 4.5 IU/day to increase the number of optimal embryos and estradiol levels on the day of hCG (p < 0.05).
Conclusion: For infertile women with DOR undergoing IVF, adjuvant treatment with GH during ovarian stimulation protocols showed better clinical outcomes, shorter days and lower dosages of gonadotrophin required. Furthermore, well-designed RCTs are needed to verify our results in the future.
Systematic review registration: https://www.crd.york.ac.uk PROSPERO (CRD42023421739)
Diminished ovarian reserve (DOR) is one of the leading problems affecting women’s reproductive health. It is a clinical syndrome characterized by reduced anti-Müllerian hormone (AMH) levels, elevated follicle-stimulating hormone (FSH) levels, and decreased antral follicle count (AFC). DOR is also highly associated with low fertility and even infertility due to the concomitant decrease in oocyte quality with quantity (1, 2). Therefore, assisted reproductive technology (ART) is often considered for infertile women with DOR. Statistics derived from 181,536 ART cycles showed that the incidence of DOR was approximately 19% to 26% in the US ART population (3). Women with DOR are closely correlated with a reduced probability of pregnancy in ART as well (4). Meanwhile, the negative consequences of DOR include a higher incidence of preeclampsia (5), elevated odds of recurrent pregnancy loss (6), and a higher risk of miscarriage (7). An increase in the prevalence of infertility caused by DOR has tremendously influenced quality of life in women. Although various adjuvant reagents and stimulation protocols have been applied to promote outcomes in infertile women with DOR undergoing IVF, effective treatment remains a clinical challenge.
Growth hormone (GH), secreted by the pituitary gland, is involved in metabolism, cell growth, and development (8). Growing evidence in the literature demonstrated the expression of GH in female oocytes, ovarian granulosa, placenta, and uterus, which reveals that GH may play a distinct role in women’s reproduction (9, 10). Clinically, a decrease in GH levels tends to correlate with poor ovarian response, low oocyte quality and cleavage rate in IVF (11). The beneficial role of GH supplementation during ovarian stimulation may facilitate the implantation process by improving endometrial receptivity and promoting the maturation process of luteinization through regulating the number of receptors in granulosa cells of patients with DOR, such as bone morphogenetic hormone receptor, FSH receptor, and LH receptor (11, 12). Recently, the number of randomized controlled trials (RCTs) of GH for infertile patients with DOR receiving IVF has been increasing. However, several clinical studies have yielded controversial results. For example, Shi et al. (13) reported that the GH co-treatment with IVF was related to promoting the clinical pregnancy rate but not to reducing the dose and the duration of gonadotropin application, which was contrary to Zhao’s study (14). Furthermore, Kang et al. (15) confirmed that a greater number of oocytes were retrieved in the GH group compared to the control group. Still, the optimal embryos rate between the two groups illustrated no difference. While Zhang et al. (16) demonstrated that though the number of optimal embryos was improved by GH adjuvant therapy, the number of oocytes retrieved was not enhanced. Therefore, this meta-analysis of RCTs was conducted to inform clinical practice. The study’s concerns were as follows: (1) Does GH improve the outcomes in infertile women with DOR undergoing IVF?; (2) Is the GH co-treatment associated with a reduction in gonadotropin required during ovarian stimulation?
We conducted this study according to the preferred reporting items for systematic review and meta-analysis (PRISMA) statement (17) and registered on PROSPERO (registration number: CRD42023421739)
We systematically searched nine databases, namely, Web of Science, Sinomed, EBSCO, Scopus, PubMed, China National Knowledge Infrastructure (CNKI), Cochrane Library, Wanfang, and VIP Information, from the database inception to April 20, 2023. The search strategy was conducted using the following three components: clinical condition (infertility, diminished ovarian reserve, decreased ovarian reserve, declined ovarian reserve), intervention (growth hormone, in vitro fertilization, assisted reproductive technology, intracytoplasmic sperm injection, intrauterine insemination), and study type (randomized clinical trial). No search filters or restrictions were applied. To identify additional papers, we also manually checked the reference lists of the retrieved documents.
Two reviewers (G.Y.L. and X.F.Z.) independently checked the titles, abstracts, and full text of comprehensive searches to establish eligibility. Any ambiguity for inclusion was discussed with the other authors (S.N.L. and L.W.X.).
Studies were included if (1) infertility was associated with DOR; (2) DOR was defined as AMH<1.1ng/mL or FSH≥10IU/L or AFC<5~7 follicles (18, 19); (3) infertile women underwent IVF regardless of ovarian stimulation protocol; (4) GH was administered during ovarian stimulation; (5) they were RCTs (including propensity score matching studies); (6) there were no geographical restrictions; (7) the study was published in the Chinese or English language.
Studies were excluded if (1) women had a history of polycystic ovary syndrome, ovarian surgery, endometriosis, or other autoimmune or endocrine dysfunction; (2) the study involved DHEA and other adjuvant treatment; (3) the study was duplicate publication, review, case report, meta-analysis, study protocol, and animal experiment; (4) the full text of the study was not accessible.
Two authors (G.Y.L. and X.F.Z.) independently recorded all articles using standardized forms. The following data were collected: methodological characteristics, study population characteristics, details of the treatments, and outcomes in each group. An ultimate form was generated from the two assessment forms. Two reviewers (G.Y.L. and S.N.L.) independently estimated the quality of the studies based on the Cochrane Collaboration Handbook (http://handbook.cochrane.org), and any disagreements between the reviewers were resolved by discussing with the corresponding author (L.W.X). Each RCT was assigned to six specific domains: sequence generation, allocation concealment, blinding of participants and outcome assessment, incomplete outcome data, selective outcome reporting, and other potential threats. The risk of bias for each domain was rated as low, high, or unclear bias based on the information identified from the included articles.
The Revman software 5.3 was adopted to perform statistical analysis. Continuous variables were measured by the mean difference (MD) or standardized mean difference (SMD) with 95% confidence intervals (CIs). Dichotomous results were evaluated by the risk ratio (RR) with 95% CI. p-value < 0.05 was considered statistically significant. Additionally, heterogeneity among the studies was reported as I2. The random effect model was applied when the heterogeneity was substantial (I2 > 50%). Otherwise, the fixed effect model was adopted. To investigate potential sources of heterogeneity, subgroup analysis was applied. Where appropriate and possible, planned subgroup analyses included GH dose (≥4.5 IU/d or <4.5 IU/d) and stimulation protocol (GnRH antagonist protocol or GnRH agonist protocol). A sensitivity analysis was performed to verify the robustness of the results by omitting individual studies.
Our literature searches yielded 579 potentially relevant citations through database searches, of which 243 duplicates were removed. After screening the titles and abstracts, 321 articles against our inclusion criteria were excluded. Then, after a full-texts review, five publications were excluded as their full texts were not available to access or the studies were compared with DHEA treatment. Finally, 10 RCTs were included for qualitative synthesis (Figure 1).
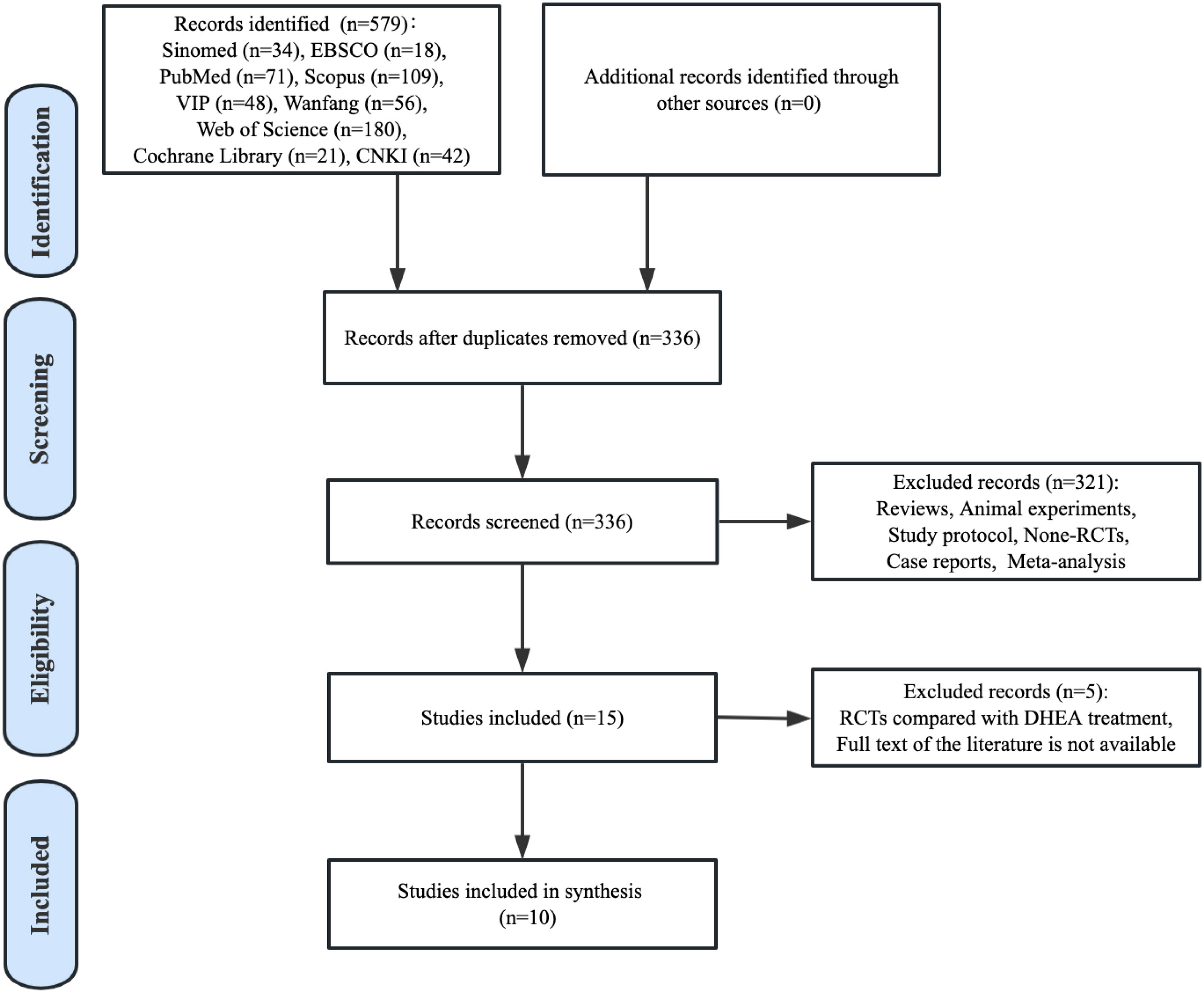
Figure 1 Paper selection flowchart.
We included 10 RCTs reporting on 852 infertile women with DOR undergoing IVF. Of these, 427 were divided into the trial group receiving GH co-treatment during ovarian stimulation and 425 into the control group without GH co-treatment. All the included studies were conducted in China and published from 2017 to 2023. Two studies used the median (25th percentile, 75th percentile) for continuous variables. One study (16) stated that the dose of GH used depended on individual AFC development. In addition, one study (20) compared the combination of GH with minimal stimulation; six (13–15, 21–23) compared with GnRH antagonist protocol; one (24) compared with long GnRH agonist protocol; and two (16, 25) compared with short GnRH agonist protocol. Seven trials (13–15, 21–23, 25) applied GH during ovarian stimulation until the trigger day; one study (24) utilized GH during ovarian stimulation for five days and two studies (16, 20) used GH until the leading follicle reached a diameter of 18mm or greater. The study characteristics are presented in Table 1.
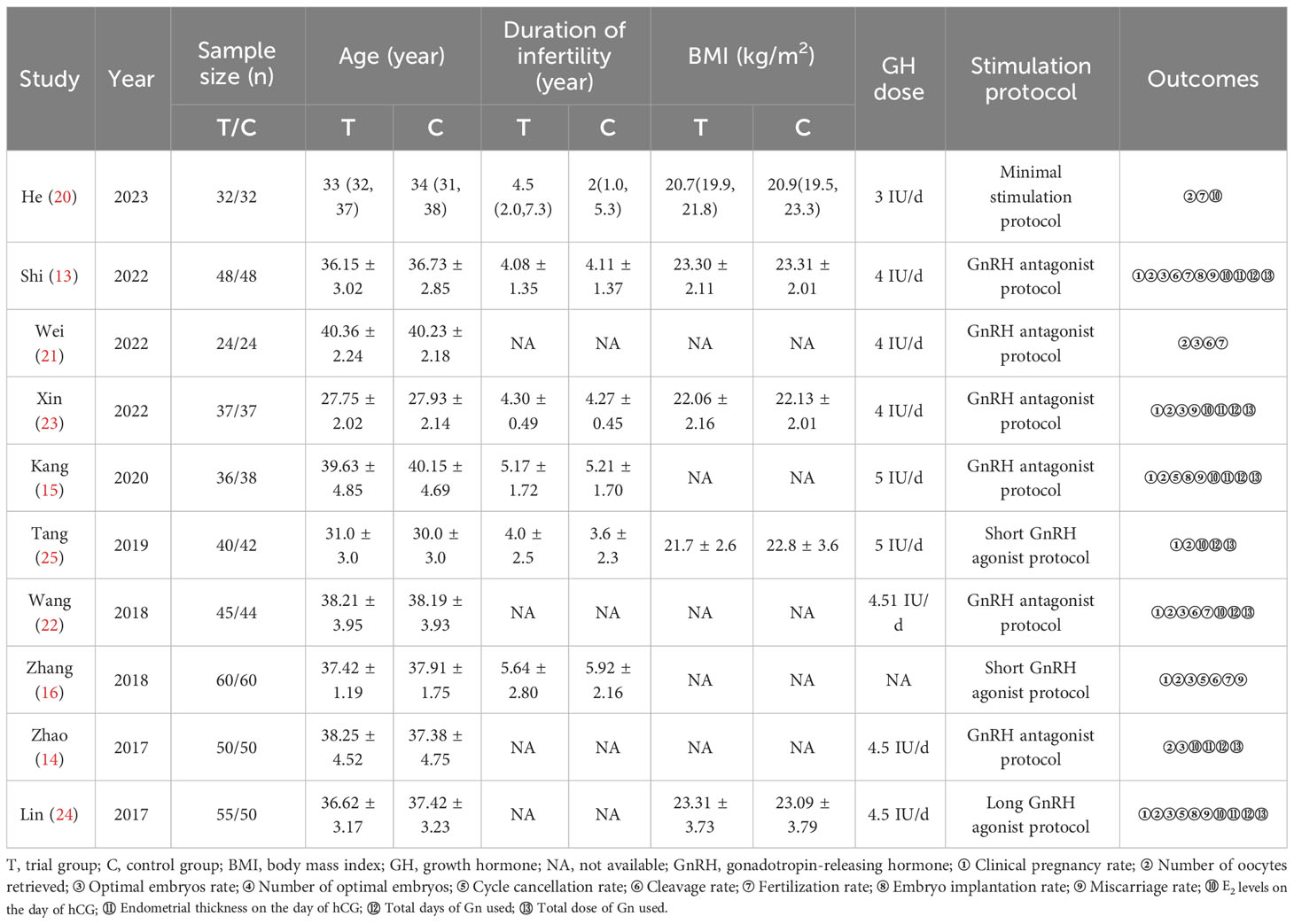
Table 1 Study characteristics.
The methodological quality of five documents (13, 15, 16, 21, 23) provided detailed procedures on how patients were randomized. Furthermore, one study (20) adopted propensity score matching and was rated as a low risk of bias. Four trials (14, 22, 24, 25) were unclear about random sequence generation. Furthermore, ten studies presented information on the allocation concealment methods, all of which were rated as having a low risk of bias. All studies failed to state the blinding of the participants, investigator, and assessor, which was considered to have a high risk of bias. The incomplete outcome was reported in three studies (15, 16, 24) and was judged as having a low risk of bias. The methods of selected reporting were presented in all studies. No potential bias was detected among the ten studies and, thus, an unclear risk of bias was rated (Figure 2).
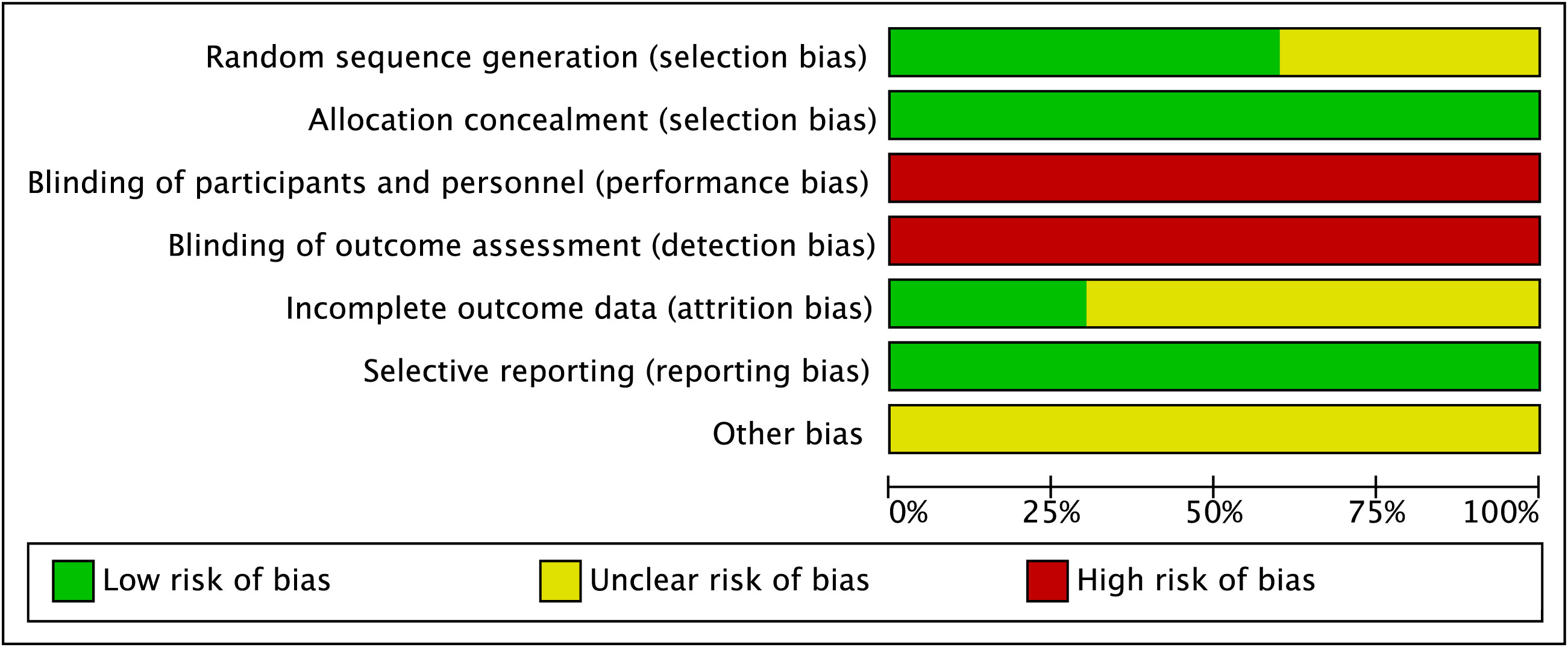
Figure 2 Risk of bias assessment.
Seven RCTs involving 593 women reported clinical pregnancy rates through IVF were meta-analyzed. Pooling the findings of these trials demonstrated that GH co-treatment on IVF significantly improved the clinical pregnancy rate in infertile patients with DOR (RR = 1.63, 95%CI [1.31, 2.03], p < 0.0001, I2 = 0%). Regarding the number of oocytes retrieved, patients receiving GH achieved a greater number of oocytes retrieved compared with those not receiving GH (MD = 0.91, 95%CI [0.47, 1.35], p < 0.0001, I2 = 90%) (Table 2). The pooled results were robust after checking by sensitivity analysis.
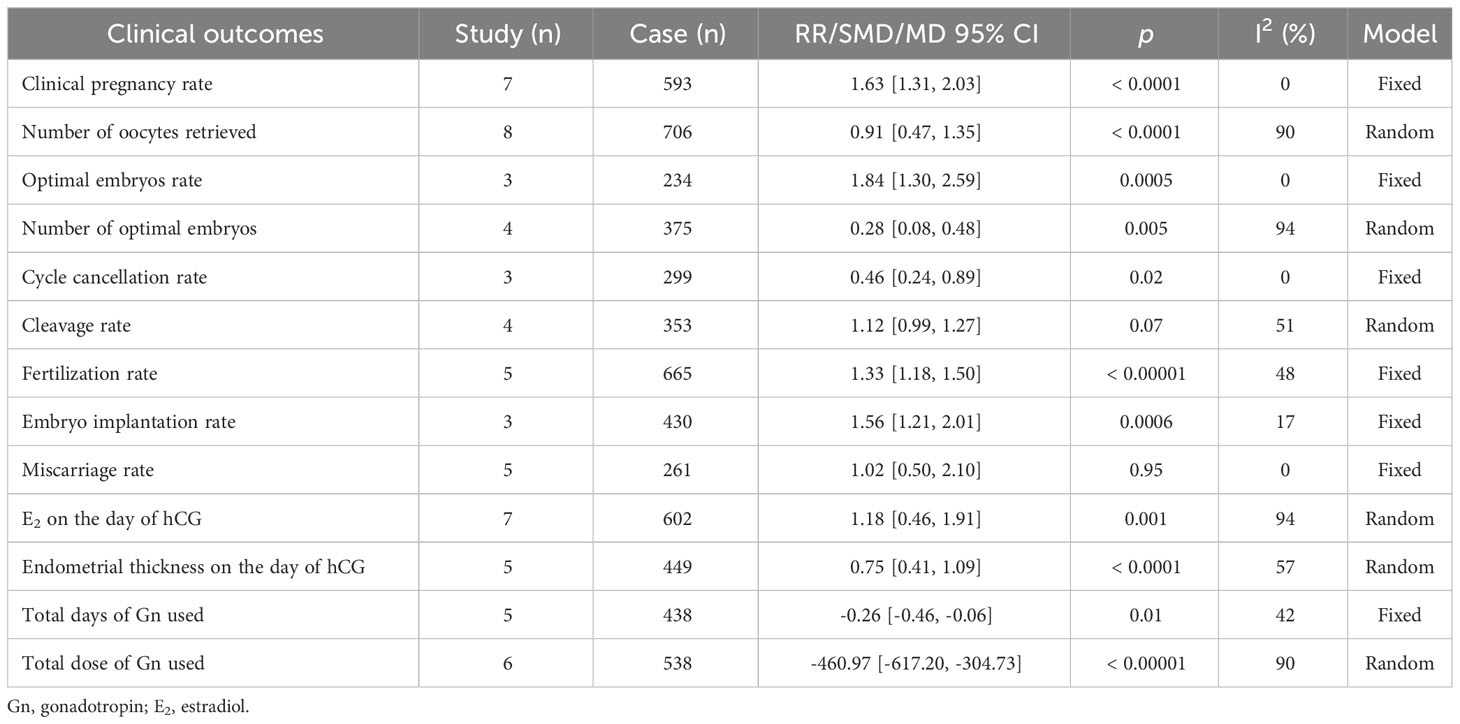
Table 2 The pooled results of the forest plot for clinical outcomes.
It was noteworthy that the rate of optimal embryos was significantly higher (RR = 1.84, 95%CI [1.30, 2.59], p = 0.0005, I2 = 0%), and the number of optimal embryos was also higher (MD = 0.28, 95%CI [0.08, 0.48], p = 0.005, I2 = 94%) in women with GH co-treatment. In addition, three studies involving 299 patients observed the cycle cancellation rate according to whether or not they received GH supplementation. We noted a decrease in cycle cancellation rate in women with GH treatment (RR = 0.46, 95%CI [0.24, 0.89], p = 0.02, I2 = 0%) (Table 2). The sensitivity analysis verified that no individual study impacted the pooled estimates.
However, no statistically significant difference in cleavage rate (RR = 1.12, 95%CI [0.99, 1.27], p = 0.07, I2 = 51%) and miscarriage rate (RR = 1.02, 95%CI [0.50, 2.10], p = 0.95, I2 = 0%) was detected between the GH group and the control group (Table 2). The results were not modified after the sensitivity analysis.
Five RCTs, including 665 patients, were identified to evaluate the effect of GH addition on fertilization rate. We observed a remarkable increase in the fertilization rate of infertile women receiving GH treatment (RR = 1.33, 95%CI [1.18, 1.50], p < 0.00001, I2 = 48%). In addition, three studies recruiting 430 patients reported embryo implantation rates. The meta-analysis revealed a considerable increase in the embryo implantation rate in the GH group (RR = 1.56, 95%CI [1.21, 2.01], p = 0.0006, I2 = 17%) (Table 2). No individual study affected the results after examination by sensitivity analysis.
With respect to the E2 levels on the day of hCG, data from seven studies comprising 602 patients showed that the improvement in E2 levels on the day of hCG was connected with a combination of GH (SMD = 1.18, 95%CI [0.46, 1.91], p = 0.001, I2 = 94%). Meanwhile, five studies including 449 patients reported the endometrial thickness on the day of hCG. The result implied an enormous increase in the endometrial thickness on the day of hCG with the administration of GH (MD = 0.75, 95%CI [0.41, 1.09], p < 0.0001, I2 = 57%) (Table 2). The sensitivity analysis proved that our results were robust.
Six studies focused on the total days of Gn used. After omitting one study (14) via sensitivity analysis, the heterogeneity decreased from 93% to 42%. The pooled result from five studies involving 438 patients presented a significant reduction in the total days of Gn used in the GH group (MD = -0.26, 95%CI [-0.46, -0.06], p = 0.01, I2 = 42%). Additionally, six studies provided sufficient data to compare the total dose of Gn used in women with GH treatment and those without GH treatment. Pooling of these data indicated a striking association between GH treatment and the total dose of Gn used (MD = -460.97, 95%CI [-617.20, -304.73], p < 0.00001, I2 = 90%) (Table 2).
Given the three pooled results on the number of oocytes retrieved, the number of optimal embryos, and the level of E2 on the day of hCG were detected with substantial heterogeneity (I2 > 60%), subgroup analysis was performed according to GH dose and GnRH protocol during ovarian stimulation. However, when comparing the association of different GnRH protocols with the number of optimal embryos and level of E2 on the day of hCG, only one study reported available data on GnRH agonist protocol. Therefore, we conducted subgroup analysis according to GH dose for the two outcomes only.
In the subgroup analysis for GH dose, there was no statistical difference in the outcome of the number of oocytes retrieved between women with GH dose ≥4.5 IU/d treatment and GH dose <4.5 IU/d treatment. However, the result showed that the GnRH antagonist protocol combined with GH supplementation was more favorable in improving the number of oocytes retrieved compared to the GnRH agonist protocol (MD = 1.09, 95%CI [0.59, 1.58], p < 0.0001, I2 = 90%) (Table 3).
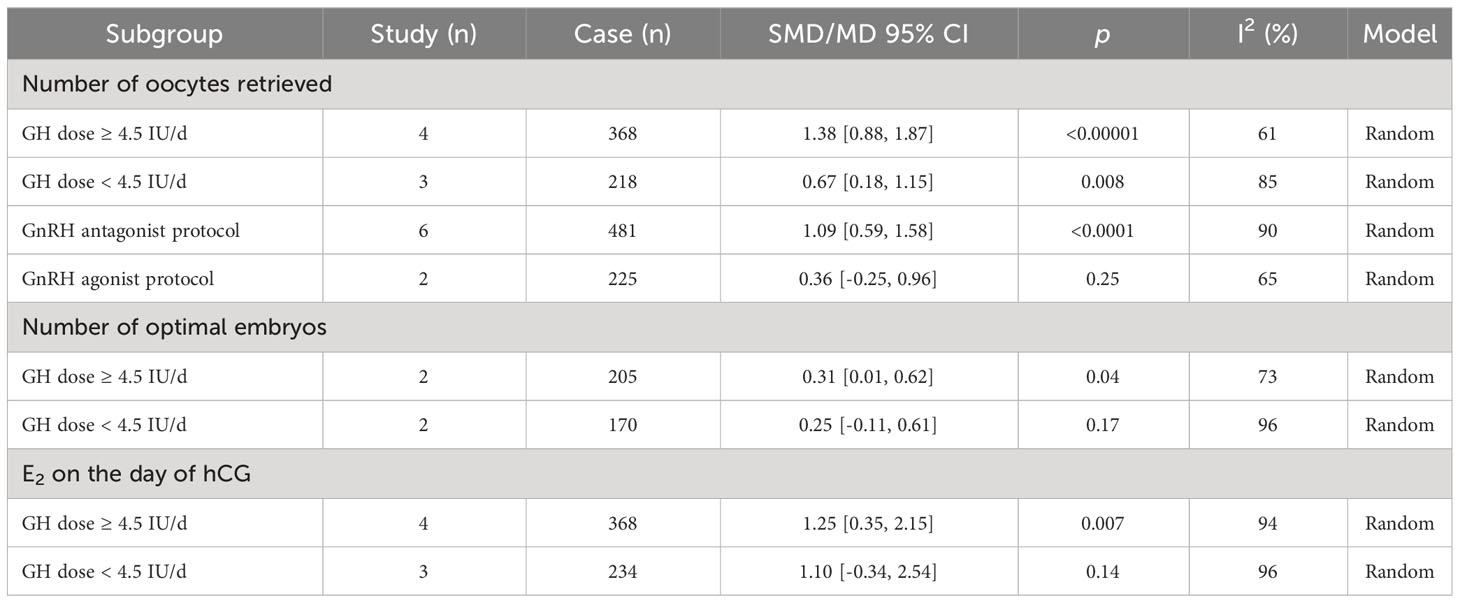
Table 3 The subgroup analysis of the correlation of GH with clinical outcomes.
Subgroup analysis performed according to the GH dose indicated a statistically significant difference between the two outcomes. The number of optimal embryos (MD = 0.31, 95%CI [0.01, 0.62], p = 0.04, I2 = 73%) and the level of E2 on the day of hCG (SMD = 1.25, 95%CI [0.35, 2.15], p = 0.007, I2 = 94%) were remarkably increased when GH dose ≥4.5 IU/d was adopted, whereas trials with GH dose < 4.5 IU/d showed uncertain efficacy (Table 3).
Infertility is a widespread reproductive health problem globally. Approximately 12.7% of reproductive-age females suffered from infertility in the US, and 25% of cases of infertility were diagnosed as ovulatory disorders (2). One of the major causes of infertility is DOR (2). Nevertheless, the etiology of DOR is uncertain due to the various complicated factors involved. Abundant literature has elucidated the association of DOR with some pathogenic factors, including environmental influences (triclosan and arsenic exposure, per- and polyfluoroalkyl substances intake) (26–28), unhealthy habits (cigarette, alcohol, and addictive drug consumption) (29), medical complications (gynecological surgery, radiotherapy, and chemotherapy) (30, 31), maternal exposures (intrauterine nutrition restriction, chronic gestational hypoxia) (32, 33), autoimmune diseases (HIV infection, thyroid hormone imbalance) (34, 35), and so forth. Notably, the deterioration of gamete quality and the progressive loss of oocytes occur naturally with older age. Therefore, a burgeoning number of women with DOR are seeking ART treatment for infertility yearly (36). Despite recent advances in ART, the outcomes of natural cycle IVF for DOR are unsatisfying due to the high cycle cancellation rate. For this reason, diverse stimulation interventions and protocols have been recommended to ameliorate IVF outcomes in infertile women with DOR. These schemes used for ovulation induction include the addition of adjuvant therapy, increased gonadotropin dosages, and different procedures for pituitary suppression during ovarian stimulation (37–39). However, high doses of gonadotrophins are often associated with a range of unexpected side effects (40). Hence, exploring an optimal adjuvant treatment remains an ongoing clinical challenge.
GH treatment in conjunction with ovarian stimulation has been considered an efficient strategy for enhancing the outcomes of IVF in infertile women (41). The molecular mechanisms of GH in the reproductive field are rather complex. Substantial evidence has demonstrated that GH could improve oocyte developmental competence by alleviating apoptosis and elevating mitochondrial membrane potential through activating the PI3K-AKT and the Sirt3-Sod2 signaling pathway in granulosa cells; meanwhile, GH may also promote cell proliferation and participate in the steroidogenic process via PI3K-AKT and PLC-PKC signaling to interact with LHR and FSHR and then regulate the functions of granulosa cells and the follicle development (42). Additionally, Liu et al., using in vitro and in vivo experiments, revealed that GH could significantly ameliorate the decline of oocyte quality and depletion of ovarian reserve associated with advanced age via decreasing the expression of γH2AX and inhibiting Fos and Jun signaling pathways in oocytes (43). In terms of uterine receptivity, GH may mediate endometrial thickness and increase endometrial blood perfusion by upregulating IGF-1 and VEGF together with ITGB3 in the uterus (44, 45).
A previous meta-analysis (46) focusing on GH for patients with poor ovarian responders undergoing IVF suggested that GH is beneficial for women in increasing the number of oocytes retrieved and MII oocytes, along with the clinical pregnancy rate and the number of embryos available to transfer. However, they failed to estimate the association of GH supplementation with cycle cancellation rate, cleavage rate, fertilization rate, E2 levels on the day of hCG, endometrial thickness on the day of hCG, total days of Gn used, and total dose of Gn applied. Furthermore, the previous study didn’t distinguish the effects of GH for women with different ovarian reserves. Therefore, to provide a more specific reflection on the significance of GH in a unique population, we focused our study on women with DOR.
In this systematic review, we estimated a potential association of GH treatment in infertile women with DOR undergoing IVF to provide evidence for informing clinical practice. Our research extended and replicated former reviews on the effectiveness of GH in fertility, which, however, generally focused on poor responders. According to our meta-analysis, adjuvant GH not only increased the clinical pregnancy rate, the number of oocytes retrieved, the optimal embryos rate, and the number of optimal embryos but also decreased the cycle cancellation rate of infertile women with DOR, which was the most critical outcome for women undergoing IVF. Moreover, GH co-treatment was more beneficial in improving the fertilization rate and embryo implantation rate. In particular, the administration of GH resulted in an obvious increase in the E2 levels and endometrial thickness on the day of hCG, which may be a novel therapeutic option for women with a thin endometrium. Similarly, a significant decrease in the total days and dose of gonadotropin applied was observed when GH was added during ovarian stimulation. Based on subgroup analyses, we also noted there was no dose-dependent connection between adjuvant GH and the number of oocytes retrieved, whereas an increased dose of GH (≥4.5 IU/d) was superior in improving the number of optimal embryos and E2 levels on the day of hCG. Furthermore, the combination of the GnRH antagonist protocol with GH significantly promoted the number of oocytes retrieved compared to the GnRH agonist protocol.
To the best of our knowledge, this is the first systematic review and meta-analysis evaluating the impact of GH on the outcomes in infertile women with DOR undergoing IVF. Some limitations ought to be noted in the interpretation of our findings. First, although 10 RCTs were included in this analysis, two studies (20, 24) adopted the median (25th percentile, 75th percentile) for continuous variables and one study (14) just reported the percentages without detailed data on clinical pregnancy rate and cleavage rate. As a result, we were unable to integrate the corresponding results into our analysis. The second limitation is that the ovarian stimulation protocols varied in each study, including GnRH antagonist protocol, minimal stimulation protocol, long GnRH agonist protocol, and short GnRH agonist protocol. Therefore, we were forced to divide these protocols into GnRH antagonist protocol and GnRH agonist protocol for subgroup analysis. For this reason, we could not estimate the correlation of GH plus different ovarian stimulation protocols with the outcomes of IVF. The third limitation is that all studies incorporated poor descriptions of their methodologies. For example, they did not report blinding of the participants, investigators, and assessors throughout the trial, which substantially impaired the strength of the evidence. However, since study populations are diverse in the real world of clinical practice, non-blinded pragmatic studies have been proposed to obtain clinically relevant outcomes (47). The fourth limitation is that publication bias cannot be evaluated by Begg’s and Egger’s tests, as less than ten studies were included in each outcome. Nevertheless, to accommodate this limitation, we conducted a sensitivity analysis for each estimate, and it verified that our results were robust. The fifth limitation is that the age of patients is believed to lead to differences in IVF efficacy, with younger infertile women with DOR possibly achieving greater improvement. Unfortunately, none of the studies reported outcomes based on different ages. Therefore, we can’t perform subgroup analysis to compare the clinical significance of GH co-treatment among different age groups. Lastly, our meta-analysis focused on GH in infertile women with DOR undergoing IVF. Hence, our pooled results may not be appropriate for those not diagnosed with DOR.
In conclusion, GH supplementation has significant clinical efficacy in improving the outcomes in infertile women with DOR undergoing IVF, including increasing the clinical pregnancy rate, number of oocytes retrieved, optimal embryos rate and number of optimal embryos, fertilization rate, embryo implantation rate, E2 levels, and endometrial thickness on the day of hCG, along with decreasing cycle cancellation rate, total days, and total dose of gonadotropin applied. However, our findings are insufficient to offer clinical recommendations due to the high risk of bias and heterogeneity. Therefore, well-designed studies are needed to certify our results in the future.
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
GYL and LWX designed the study. GYL implemented the methods and conducted the experiments. GYL, XFZ, and SNL analyzed and presented the results. GYL completed an initial draft. All authors contributed to the article and approved the submitted version.
This study received funding from the Shanghai Three-year Plan on Promoting Traditional Chinese Medicine Development (2021-2023) [grant numbers ZY(2021-2023)-0209-01].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Jaswa EG, McCulloch CE, Simbulan R, Cedars MI, Rosen MP. Diminished ovarian reserve is associated with reduced euploid rates via preimplantation genetic testing for aneuploidy independently from age: evidence for concomitant reduction in oocyte quality with quantity. Fertil Steril (2021) 115(4):966–73. doi: 10.1016/j.fertnstert.2020.10.051
2. Carson SA, Kallen AN. Diagnosis and management of infertility: A review. JAMA (2021) 326(1):65–76. doi: 10.1001/jama.2021.4788
3. Devine K, Mumford SL, Wu M, DeCherney AH, Hill MJ, Propst A. Diminished ovarian reserve in the United States assisted reproductive technology population: diagnostic trends among 181,536 cycles from the Society for Assisted Reproductive Technology Clinic Outcomes Reporting System. Fertil Steril (2015) 104(3):612–19.e3. doi: 10.1016/j.fertnstert.2015.05.017
4. Esteves SC, Roque M, Bedoschi GM, Conforti A, Humaidan P, Alviggi C. Defining low prognosis patients undergoing assisted reproductive technology: POSEIDON criteria-the why. Front Endocrinol (Lausanne) (2018) 9:461. doi: 10.3389/fendo.2018.00461
5. Ganer Herman H, Volodarsky-Perel A, Ton Nu TN, Machado-Gedeon A, Cui Y, Shaul J, et al. Diminished ovarian reserve is a risk factor for preeclampsia and placental malperfusion lesions. Fertil Steril (2023) 119(5):794–801. doi: 10.1016/j.fertnstert.2023.01.029
6. Bunnewell SJ, Honess ER, Karia AM, Keay SD, Al Wattar BH, Quenby S. Diminished ovarian reserve in recurrent pregnancy loss: a systematic review and meta-analysis. Fertil Steril (2020) 113(4):818–827.e3. doi: 10.1016/j.fertnstert.2019.11.014
7. Busnelli A, Somigliana E, Cirillo F, Levi-Setti PE. Is diminished ovarian reserve a risk factor for miscarriage? Results of a systematic review and meta-analysis. Hum Reprod Update (2021) 27(6):973–88. doi: 10.1093/humupd/dmab018
8. Donato J, Wasinski F, Furigo IC, Metzger M, Frazão R. Central regulation of metabolism by growth hormone. Cells (2021) 10(1):129. doi: 10.3390/cells10010129
9. Sirotkin AV. Control of reproductive processes by growth hormone: extra- and intracellular mechanisms. Vet J (2005) 170(3):307–17. doi: 10.1016/j.tvjl.2004.05.014
10. Skowronski MT, Mlotkowska P, Tanski D, Lepiarczyk E, Oklinski MK, Nielsen S, et al. Pituitary gonadotropins, prolactin and growth hormone differentially regulate AQP1 expression in the porcine ovarian follicular cells. Int J Mol Sci (2017) 19(1):5. doi: 10.3390/ijms19010005
11. Chang CW, Sung YW, Hsueh YW, Chen YY, Ho M, Hsu HC, et al. Growth hormone in fertility and infertility: Mechanisms of action and clinical applications. Front Endocrinol (Lausanne) (2022) 13:1040503. doi: 10.3389/fendo.2022.1040503
12. Regan SLP, Knight PG, Yovich JL, Arfuso F, Dharmarajan A. Growth hormone during in vitro fertilization in older women modulates the density of receptors in granulosa cells, with improved pregnancy outcomes. Fertil Steril (2018) 110(7):1298–310. doi: 10.1016/j.fertnstert.2018.08.018
13. Shi A, Cao Y, Ge Z, Jiao Y, Zhang L. Effect of adding recombinant human growth hormone during ovulation induction on IVF-ET outcome and influencing factors discussion of pregnancy outcome in patients with diminished ovarian reserve. Prog Modern Biomedicine (2022) 22(15):2965–70. doi: 10.13241/j.cnki.pmb.2022.15.032
14. Zhao C, Qi R, Liang Y, Zhou L, Wu X, Gao X, et al. An application research of growth hormone on ovarian reserve dysfunction patients in IVF cycle. Chin J Birth Health Heredity (2017) 25(1):125–6.
15. Kang W, Liang X. Application of growth hormone injection in luteal phase in IVF-ET assisted pregnancy in aged infertile patients with diminished ovarian reserve. Hainan Med J (2020) 31(7):875–8. doi: 10.3969/j.issn.1003-6350.2020.07.018
16. Zhang J, Wang C, Zhang Z, Zhang C. Pregnancy outcome of patients ≥ 35 years old with diminished ovarian reserve treated with growth hormone. J Chin Physician (2018) 20(8):1167–70. doi: 10.3760/cma.j.issn.1008-1372.2018.08.013
17. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (2021) 372:n71. doi: 10.1136/bmj.n71
18. Cohen J, Chabbert-Buffet N, Darai E. Diminished ovarian reserve, premature ovarian failure, poor ovarian responder–a plea for universal definitions. J Assist Reprod Genet (2015) 32(12):1709–12. doi: 10.1007/s10815-015-0595-y
19. Expert Group of Consensus on Clinical Diagnosis & Management of Diminished Ovarian Reserve and Reproductive Endocrinology & Fertility Preservation Section of Chinese Society on Fertility Preservation under Chinese Preventive Medicine Association. Consensus on clinical diagnosis and management of diminished ovarian reserve. J Reprod Med (2022) 31(4):425–34. doi: 10.3969/j.issn.1004-3845.2022.04.001
20. He F, Wang F, Yang Y, Uan Z, Sun C, Zou H, et al. The effect of growth hormone on the metabolome of follicular fluid in patients with diminished ovarian reserve. Reprod Biol Endocrinol (2023) 21(1):21. doi: 10.1186/s12958-023-01073-x
21. Wei X, Liu Z. Effect of follicular phase pretreatment with growth hormone for advanced diminished ovarian reserve patients following the controlled ovarian hyperstimulation. Lab Med Clinic (2022) 19(12):1596–8. doi: 10.3969/j.issn.1672-9455.2022.12.004
22. Wang S. Effect of growth hormone combined with antagonists on the outcome of IVF-ET in patients with diminished ovarian reserve. J Shandong Med Coll (2018) 40(6):409–10. doi: 10.3969/j.issn.1674-0947.2018.06.004
23. Xin X. Effect of growth hormone on in vitro fertilization embryo transfer in young patients with decreased ovarian reserve. Med Innovation China (2022) 19(28):20–3. doi: 10.3969/j.issn.1674-4985.2022.28.005
24. Lin S, Li X, Liu D, Wu Z, Tan S. The effect of growth hormone on the IVF-ET outcome of the patients with diminished ovarian reserve. Chin J Birth Health Heredity (2017) 25(6):105–106,19.
25. Tang X, Hu W, Song H, Ding X, Huang Y. Effect of growth hormone on in vitro fertilization-embryo transfer outcomes in young patients with diminished ovarian reserve. Maternal Child Health Care China (2019) 34(7):1614–6. doi: 10.7620/zgfybj.j.issn.1001-4411.2019.07.51
26. Mínguez-Alarcón L, Christou G, Messerlian C, Williams PL, Carignan CC, Souter I, et al. Urinary triclosan concentrations and diminished ovarian reserve among women undergoing treatment in a fertility clinic. Fertil Steril (2017) 108(2):312–9. doi: 10.1016/j.fertnstert.2017.05.020
27. Chen Y, Sun Y, Zhao A, Cai X, Yu A, Xu Q, et al. Arsenic exposure diminishes ovarian follicular reserve and induces abnormal steroidogenesis by DNA methylation. Ecotoxicol Environ Saf (2022) 241:113816. doi: 10.1016/j.ecoenv.2022.113816
28. Ding N, Harlow SD, Randolph JF, Calafat AM, Mukherjee B, Batterman S, et al. Associations of perfluoroalkyl substances with incident natural menopause: the study of women's health across the nation. J Clin Endocrinol Metab (2020) 105(9):e3169–82. doi: 10.1210/clinem/dgaa303
29. de Angelis C, Nardone A, Garifalos F, Pivonello C, Sansone A, Conforti A, et al. Smoke, alcohol and drug addiction and female fertility. Reprod Biol Endocrinol (2020) 18(1):21. doi: 10.1186/s12958-020-0567-7
30. Goodman LR, Goldberg JM, Flyckt RL, Gupta M, Harwalker J, Falcone T. Effect of surgery on ovarian reserve in women with endometriomas, endometriosis and controls. Am J Obstet Gynecol (2016) 215(5):589.e1–6. doi: 10.1016/j.ajog.2016.05.029
31. Spears N, Lopes F, Stefansdottir A, Rossi V, De Felici M, Anderson RA, et al. Ovarian damage from chemotherapy and current approaches to its protection. Hum Reprod Update (2019) 25(6):673–93. doi: 10.1093/humupd/dmz027
32. Richardson MC, Guo M, Fauser BC, Macklon NS. Environmental and developmental origins of ovarian reserve. Hum Reprod Update (2014) 20(3):353–69. doi: 10.1093/humupd/dmt057
33. Aiken CE, Tarry-Adkins JL, Spiroski AM, Nuzzo AM, Ashmore TJ, Rolfo A, et al. Chronic gestational hypoxia accelerates ovarian aging and lowers ovarian reserve in next-generation adult rats. FASEB J (2019) 33(6):7758–66. doi: 10.1096/fj.201802772R
34. Santulli P, de Villardi D, Gayet V, Lafay Pillet MC, Marcellin L, Blanchet V, et al. Decreased ovarian reserve in HIV-infected women. AIDS (2016) 30(7):1083–8. doi: 10.1097/QAD.0000000000001025
35. Bahri S, Tehrani FR, Amouzgar A, Rahmati M, Tohidi M, Vasheghani M, et al. Overtime trend of thyroid hormones and thyroid autoimmunity and ovarian reserve: a longitudinal population study with a 12-year follow up. BMC Endocr Disord (2019) 19(1):47. doi: 10.1186/s12902-019-0370-7
36. Inhorn MC, Patrizio P. Infertility around the globe: new thinking on gender, reproductive technologies and global movements in the 21st century. Hum Reprod Update (2015) 21(4):411–26. doi: 10.1093/humupd/dmv016
37. Lin G, Zhong X, Li S, Liu X, Xu L. The clinical value of progestin-primed ovarian stimulation protocol for women with diminished ovarian reserve undergoing IVF/ICSI: a systematic review and meta-analysis. Front Endocrinol (Lausanne) (2023) 14:1232935. doi: 10.3389/fendo.2023.1232935
38. Pandian Z, McTavish AR, Aucott L, Hamilton MP, Bhattacharya S. Interventions for 'poor responders' to controlled ovarian hyper stimulation (COH) in in-vitro fertilisation (IVF). Cochrane Database Syst Rev (2010) 1):CD004379. doi: 10.1002/14651858
39. Zhang Y, Zhang C, Shu J, Guo J, Chang HM, Leung PCK, et al. Adjuvant treatment strategies in ovarian stimulation for poor responders undergoing IVF: a systematic review and network meta-analysis. Hum Reprod Update (2020) 26(2):247–63. doi: 10.1093/humupd/dmz046
40. Singh R, Kaur S, Yadav S, Bhatia S. Gonadotropins as pharmacological agents in assisted reproductive technology and polycystic ovary syndrome. Trends Endocrinol Metab (2023) 34(4):194–215. doi: 10.1016/j.tem.2023.02.002
41. Sood A, Mohiyiddeen G, Ahmad G, Fitzgerald C, Watson A, Mohiyiddeen L. Growth hormone for in vitro fertilisation (IVF). Cochrane Database Syst Rev (2021) 11(11):CD000099. doi: 10.1002/14651858
42. Pan P, Huang X. The clinical application of growth hormone and its biological and molecular mechanisms in assisted reproduction. Int J Mol Sci (2022) 23(18):10768. doi: 10.3390/ijms231810768
43. Liu C, Li S, Li Y, Tian J, Sun X, Song T, et al. Growth hormone ameliorates the age-associated depletion of ovarian reserve and decline of oocyte quality via inhibiting the activation of Fos and Jun signaling. Aging (Albany NY) (2021) 13(5):6765–81. doi: 10.18632/aging.202534
44. Altmäe S, Aghajanova L. Growth hormone and endometrial receptivity. Front Endocrinol (Lausanne) (2019) 10:653. doi: 10.3389/fendo.2019.00653
45. Bondy CA, Zhou J. Growth hormone, insulin-like growth factors and the female reproductive system. Adv Exp Med Biol (2005) 567:91–115. doi: 10.1007/0-387-26274-1_4
46. Cozzolino M, Cecchino GN, Troiano G, Romanelli C. Growth hormone cotreatment for poor responders undergoing in vitro fertilization cycles: a systematic review and meta-analysis. Fertil Steril. (2020) 114(1):97–109. doi: 10.1016/j.fertnstert.2020.03.007
Keywords: diminished ovarian reserve, growth hormone, infertility, in vitro fertilization, meta-analysis
Citation: Lin G, Zhong X, Li S and Xu L (2023) Clinical evidence of growth hormone for infertile women with diminished ovarian reserve undergoing IVF: a systematic review and meta-analysis. Front. Endocrinol. 14:1215755. doi: 10.3389/fendo.2023.1215755
Received: 02 May 2023; Accepted: 16 October 2023;
Published: 07 November 2023.
Edited by:
Hannu Kullervo Martikainen, University of Oulu, FinlandReviewed by:
Giuliano Marchetti Bedoschi, University of Sao Paulo, BrazilCopyright © 2023 Lin, Zhong, Li and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lianwei Xu, eHVfbGlhbndlaTI4MDBAc2h1dGNtLmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.