 Sylvie Epelboin1*†
Sylvie Epelboin1*† Julie Labrosse2†Jacques De Mouzon3Aviva Devaux4Marie-José Gervoise-Boyer5Laetitia Hesters6Philippe Jonveaux7
Julie Labrosse2†Jacques De Mouzon3Aviva Devaux4Marie-José Gervoise-Boyer5Laetitia Hesters6Philippe Jonveaux7 Rachel Levy8Nathalie Sermondade8
Rachel Levy8Nathalie Sermondade8 Patricia Fauque9Fabienne Pessione7
Patricia Fauque9Fabienne Pessione7- 1Department of Reproductive Medicine, Gynecology and Obstetrics, Hôpital Bichat-Claude Bernard, Assistance Publique-Hôpitaux de Paris Nord, Université de Paris, Paris, France
- 2Department of Reproductive Medicine, Gynecology and Obstetrics, American Hospital of Paris, Neuilly-sur-Seine, France
- 3Department of Reproductive Biology, Unilabs, Direction médicale, Clichy La Garenne, France
- 4Department of Reproductive Biology, Centre Hospitalier Universitaire, Amiens, France
- 5Department of Reproductive Medicine, Hôpital Saint Joseph, Marseille, France
- 6Department of Reproductive Biology, Hôpital Antoine Béclère, Hôpitaux Universitaires Paris-Sud, Assistance Publique - Hôpitaux de Paris, Clamart, France
- 7Department of Procreation, Agence de la biomédecine, La Plaine Saint Denis, France
- 8Department of Reproductive Biology, Hôpital Tenon, Hôpitaux Universitaires Est Parisien, Assistance Publique – Hôpitaux de Paris, Paris, France
- 9Department of Reproductive Biology, Université Bourgogne Franche-Comté - INSERM UMR1231, Dijon, France
Background: Risks of maternal morbidity are known to be reduced in pregnancies resulting from frozen embryo transfer (FET) compared to fresh-embryo transfer (fresh-ET), except for the risk of pre-eclampsia, reported to be higher in FET pregnancies compared to fresh-ET or natural conception. Few studies have compared the risk of maternal vascular morbidities according to endometrial preparation for FET, either with ovulatory cycle (OC-FET) or artificial cycle (AC-FET). Furthermore, maternal pre-eclampsia could be associated with subsequent vascular disorders in the offspring.
Methods: A 2013-2018 French nationwide cohort study comparing maternal vascular morbidities in 3 groups of single pregnancies was conducted: FET with either OC or AC preparation, and fresh-ET. Data were extracted from the French National Health System database. Results were adjusted for maternal characteristics and infertility (age, parity, smoking, obesity, history of diabetes or hypertension, endometriosis, polycystic ovary syndrome and premature ovarian insufficiency).
Results: A total of 68025 single deliveries were included: fresh-ET (n=48152), OC-FET (n=9500), AC-FET (n=10373). The risk of pre-eclampsia was higher in AC-FET compared to OC-FET and fresh-ET groups in univariate analysis (5.3% vs. 2.3% and 2.4%, respectively, P<0.0001). In multivariate analysis the risk was significantly higher in AC-FET compared to fresh-ET: aOR=2.43 [2.18-2.70], P<0.0001). Similar results were observed for the risk of other vascular disorders in univariate analysis (4.7% vs. 3.4% and 3.3%, respectively, P=0.0002) and in multivariate analysis (AC-FET compared to fresh-ET: aOR=1.50 [1.36-1.67], P<0.0001). In multivariate analysis, the risk of pre-eclampsia and other vascular disorders were comparable in OC-FET and fresh-ET: aOR=1.01 [0.87-1.17, P= 0.91 and aOR=1.00 [0.89-1.13], P=0.97, respectively).Within the group of FET, the risks of pre-eclampsia and other vascular disorders in multivariate analysis were higher in AC-FET compared to OC-FET (aOR=2.43 [2.18-2.70], P<0.0001 and aOR=1.5 [1.36-1.67], P<0.0001, respectively).
Conclusion: This nationwide register-based cohort study highlights the possibly deleterious role of prolonged doses of exogenous estrogen-progesterone supplementation on gestational vascular pathologies and the protective role of the corpus luteum present in OC-FET for their prevention. Since OC-FET has been demonstrated not to strain the chances of pregnancy, OC preparation should be advocated as first-line preparation in FET as often as possible in ovulatory women.
1 Introduction
The practice of frozen-thawed embryo transfer (FET) has increased over the past decades in connection with technological improvements resulting in higher cumulative live birth rates (1–5). FET enables single embryo transfer, reduces the risk of ovarian hyperstimulation syndrome, optimizes endometrial receptivity and facilitates fertility preservation (2–8). According to the 2020 annual report of the French Biomedicine Agency, FET was performed in up to 33 350 couples, representing 41.6% of in vitro Fertilization (IVF) transfers, of which 65% were transfers of frozen-thawed blastocysts. Although there is no transnational report on the type of protocol most frequently used for FET, it seems that the artificial cycle (AC) is the most performed worldwide since it facilitates the organization of ART centers compared with endometrial preparation by ovulatory cycles (OC), whether natural/modified natural or stimulated.
Assisted Reproductive Technologies (ART) have been associated to various maternal morbidities for which controlled ovarian stimulation regimens (9), embryo culture media (10, 11), and/or subfertility in itself might play a role (12–14). Risks of maternal and perinatal morbidity (placenta previa, placental abruption, premature birth, small for gestational age, and perinatal mortality) are known to be reduced in pregnancies resulting from FET compared to fresh embryo transfer (fresh-ET), except for the risk of pre-eclampsia and severe pre-eclampsia that were reported to be significantly higher in pregnancies resulting from FET compared to fresh-ET or natural conception (9, 15–21). Gestational hypertension is a disease of pregnancy that combines an increase in blood pressure > 140 mmHg and/or 90 mmHg occurring after the 20th week of amenorrhea, measured twice, with or without proteinuria > 0.3g/24h and/or oedemas and clinical other symptoms (22). The severe form of pre-eclampsia is defined by systolic pressure is ≥ 160 mmHg and/or diastolic pressure ≥ 110 mmHg or hypertension not controlled by treatment, more or less associated with impaired renal function with proteinuria ≥ 3g per 24 hours, oliguria, high blood levels of creatinine and/or liver enzymes, and low levels of blood platelets (22). Preeclampsia can lead to eclampsia, a serious complication that results in seizures.
Pre-eclampsia is considered as a multi-systemic disorder occurring in about 2-5% of pregnancies and as one of the leading causes of maternal and perinatal mortality and morbidity, particularly in developing countries (23). In France, although maternal mortality secondary to hypertensive pathologies in pregnancy has decreased by 50% in 10 years according to the latest report of the confidential national survey on maternal deaths, pre-eclampsia and severe pre-eclampsia remains one of the main causes of mortality (24). Moreover, beyond maternal mortality, pre-eclampsia can be the cause of significant severe maternal morbidity: in 10% of cases, pre-eclampsia progresses to a severe form, which can lead to organic dysfunctions, sometimes persistent in the medium and long term. Severe pre-eclampsia is a risk factor for postpartum thromboembolic complications. Pre-eclampsia is also responsible for a third of premature births in France (25). Therefore, it is important to prevent it by refining the knowledge of risk factors. An increased risk of pre-eclampsia might be explained by altered trophoblastic invasion leading to an inadequate remodelling of spiral arteries, insufficiently dilated vessels, an imbalance between angiogenic and anti-angiogenic factors or by endothelial dysfunction occurring after the release of placental factors into maternal circulation (26). Some causes of female infertility, such as diminished ovarian reserve or endometriosis may be a risk factor for pre-eclampsia and placental malperfusion lesions (27, 28).
Concerning the impact of the different types of endometrial preparation protocols for FET on the risk of pregnancy-induced vascular disorders, some studies have suggested that the presence of a corpus luteum (CL) in OC might be a protective factor, whereas the non-physiological and prolonged doses of the estrogen-progesterone combination in AC may have a deleterious impact (20, 29).Thus, as most recent studies demonstrate an equal live birth rate with endometrial preparation either by OC or AC, others have compared the risk of gestational vascular morbidities between the two types of protocols (20, 29). A systematic review of 2021 on hypertensive disorders in pregnancy following a FET cycle observed that hypertensive disorders were significantly increased after AC-FET when compared with natural cycle or mild OC-FET cycle (30). In a 2022 meta-analysis of 12 studies, Busneli et al. (31) observed a higher risk of pre-eclampsia, hypertensive disorders of pregnancy (HDP) and pregnancy-induced hypertension in AC-FET pregnancies compared to NC.
Many studies have also highlighted other manifestations of gestational vascular disorders, not only on pregnancy, but on the child’s growth, in case of assisted procreation techniques or treatments (30–35). Nevertheless, we have chosen to focus this study on the association between endometrial preparation protocols for ET and the incidence of pre-eclampsia and other maternal vascular disorders during pregnancy. The study of fetal growth disorders following medically assisted reproduction according to maternal context or techniques was specifically studied from the same national cohort by the same research group from the French Biomedecine Agency.
The objective of this extensive 5-year nationwide register-based cohort study was to evaluate, in the French population, the risk of pre-eclampsia and other gestational vascular disorders between FET, according to endometrial preparation by either ovulatory cycle (OC-FET) or artificial cycle (AC-FET) and fresh-ET. The aim was to report broad real-life data considering the numerous confounding factors accessible in the database, including underlying female infertility.
2 Materials and methods
This study is a nationwide register-based cohort study. Data were extracted from the French National Health System database (Système National des Données de Santé – SNDS) that includes > 99% of national deliveries, in which all outpatients and hospitalizations from 2008 to 2018 (in any public hospital and private clinic) were registered. The database contains information on patient characteristics, diagnoses and treatments registered in outpatient consultations. Maternal records were merged anonymously and with previous hospitalisations through a specific software making it impossible to retrieve patient identity but allowing to cross information through anonymized codes. The access to this database was legally approved.
We conducted a comparative analysis of the cohort of singleton births (deliveries ≥22 weeks of gestation (WG) and/or > 500g of birthweight) occurring in France and resulting from fresh-ET or FET from IVF and intracytoplasmic sperm injection (ICSI) cycles performed over a 5-year period (2013-2017). All women with a history of delivery from IVF with fresh-ET, intrauterine insemination or FET within the previous 5 years were excluded from the analysis As it was specified above, the database analysis made it possible to identify health events of our patients since the year 2008. Data available in the hospitalization database were parity, multiple pregnancy, maternal age, active smoking during pregnancy, obesity, maternal history of diabetes (type 1 or 2) or hypertension, diagnosis of endometriosis, polycystic ovary syndrome (PCOS) or premature ovarian insufficiency (POI), mode of conception (fresh-ET or FET) and term. Patients with twin deliveries or history of hypertensive disorders (pregnancy-induced or not) were excluded.
2.1 Comparison groups
Three comparison groups of singletons were analyzed: 1/pregnancies resulting from OC-FET (natural, modified natural or stimulated cycle); 2/pregnancies resulting from AC-FET; 3/pregnancies resulting from fresh-ET.
2.2 Endometrial preparation protocols
Endometrial preparation with OC included natural cycles, modified natural cycles (natural cycles with ovulation triggering by hCG and/or luteal phase support) and stimulated cycles (mild ovarian stimulation by gonadotropins). Luteal phase support with vaginal micronized progesterone (VMPg, 200 to 400 mg/day) was administered for 6 to 10 weeks of gestation (WG) in case of pregnancy.
Endometrial preparation by AC consisted in the sequential administration of exogenous estrogens and progesterone. According to ART centers, supplementation by estrogens was usually started on Day 1 (orally at 4-8 mg/day and/or transdermally at 200 µg/3days). In case of AC protocols with previous down regulation by GnRH-agonist, estrogen supplementation was started 10 to 15 days after GnRH-agonist introduction. Once adequate endometrial thickness was obtained, VMPg (600 to 1200 mg daily) was started and continued until the 12th WG in case of pregnancy.
Embryos were obtained from conventional IVF or ICSI cycles. In FET groups, embryos were frozen at cleavage stage or blastocyst stage (according to the evolution of laboratory policies).
2.3 Vascular disorders
Vascular disorders were classified into 2 groups according to the International Classification of Disease (ICD-10) codes: (i) hospitalization for pre-eclampsia and/or eclampsia (O14 and O15, grouped under the term pre-eclampsia), and (ii) hospitalization for other vascular disorders during pregnancy (gestational hypertension with or without proteinuria (O13, O16) or isolated proteinuria with oedema (O12). Although the terms used in literature are most often hypertensive disorders of pregnancy, (grouping pre-eclampsia and pregnancy induced hypertension with or without proteinuria), we made the choice to scrupulously follow the diagnoses according to the ICD10 codes internationally validated. We grouped under the term “other vascular disorders” the cases of hospitalization for isolated proteinuria with oedema with those for gestational hypertension with or without proteinuria, and distinguished them from pre-eclampsia/eclampsia, because of the difference in the severity of the maternal-fetal consequences. For isolated proteinuria with oedema, we make it clear that these are cases that have generated hospitalization.
2.4 Statistical analysis
Univariate and multivariate analyses were performed using logistic regression models to compare the risk of pregnancy-induced vascular disorders between fresh-ET and FET, and between the two types of endometrial preparation in FET cycles (OC-FET versus AC-FET). Two risk estimations were performed in multivariate analysis: the risk of pre-eclampsia and the risk of other pregnancy-induced vascular disorders, compared to pregnancies without any vascular disorder. Adjusted Odds Ratios (aOR) and their 95% confidence intervals (CI) were estimated.
3 Results
The study included 68 025 single deliveries following embryo transfer occurring nationwide from 2013 to 2017. A total of 48 152 were cases of fresh-ET and 19 873 were FET cycles, among which 9 500 were AC-FET and 10 373 were OC-FET.
3.1 Maternal characteristics
Comparison of maternal characteristics according to the type of treatment is presented in Table 1. Patients with fresh-ET were younger and more often primiparous (P < 0.0001 in the overall comparison). Within FET groups, in univariate analysis, women with AC were more often primiparous (56.1% vs. 54.5%, P = 0.03) and obese (4.3% vs. 3.6%, P =0.01) and were more often diagnosed with endometriosis (13.3% vs. 10.8%, P < 0.0001), PCOS (3.5% vs. 2.0%, P < 0.0001) and POI (1.4% vs. 0.6%, P < 0.0001).
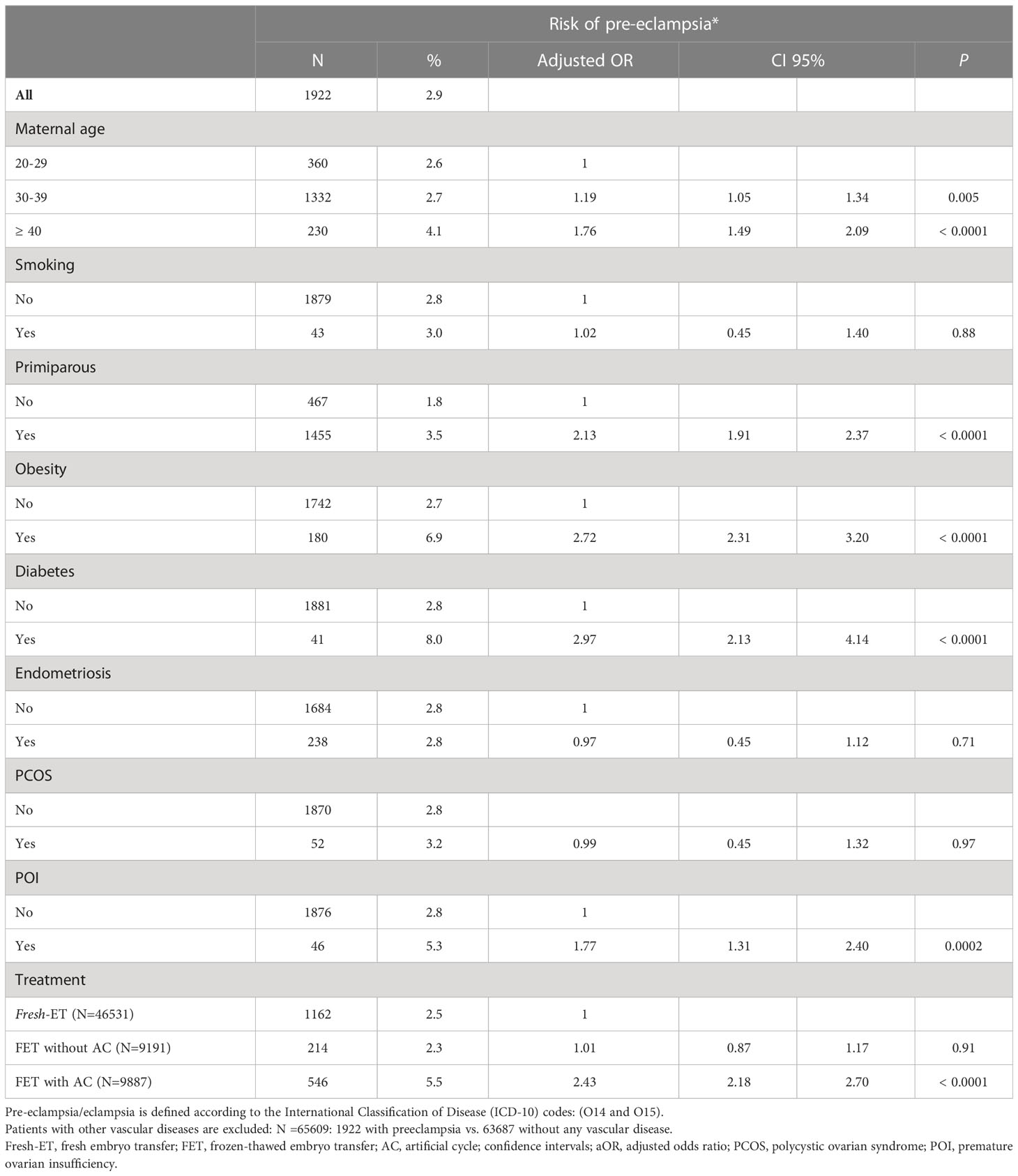
Table 1 Maternal characteristics according type of embryo transfer and endometrial preparation protocol.
3.2 Risk of pre-eclampsia and other vascular disorders
The frequency of hospitalizations for pre-eclampsia was 2.8% (n = 1 922) and 3.6% (n = 2 416) for other vascular disorders. A total of 63 687 (93.6%) women were not hospitalized for any vascular disorder.
Risk factors of pre-eclampsia and other vascular disorders compared to women without any vascular disorder in multivariate analysis are presented in Tables 2, 3, respectively. The risk of pre-eclampsia increased with age, primiparity, obesity, history of diabetes and POI (Table 2). There was no increased risk of pre-eclampsia in case of endometriosis or PCOS. The risk of vascular disorders other than pre-eclampsia increased with age, active smoking, primiparity, obesity and history of diabetes (Table 3). There was no increased risk based on any maternal infertility.
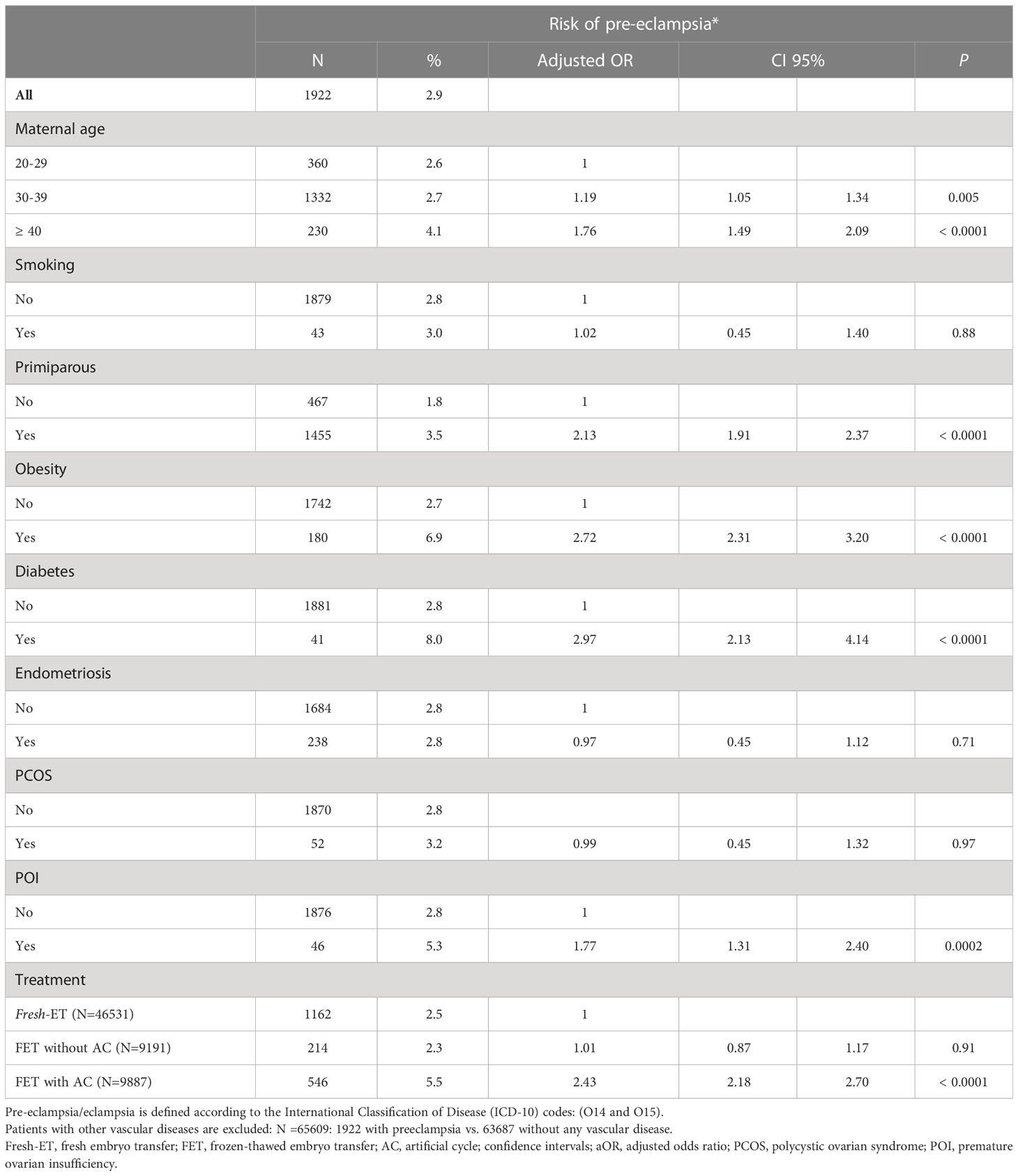
Table 2 Risk of pre-eclampsia compared to no vascular disease in multivariate analysis (N=65609).
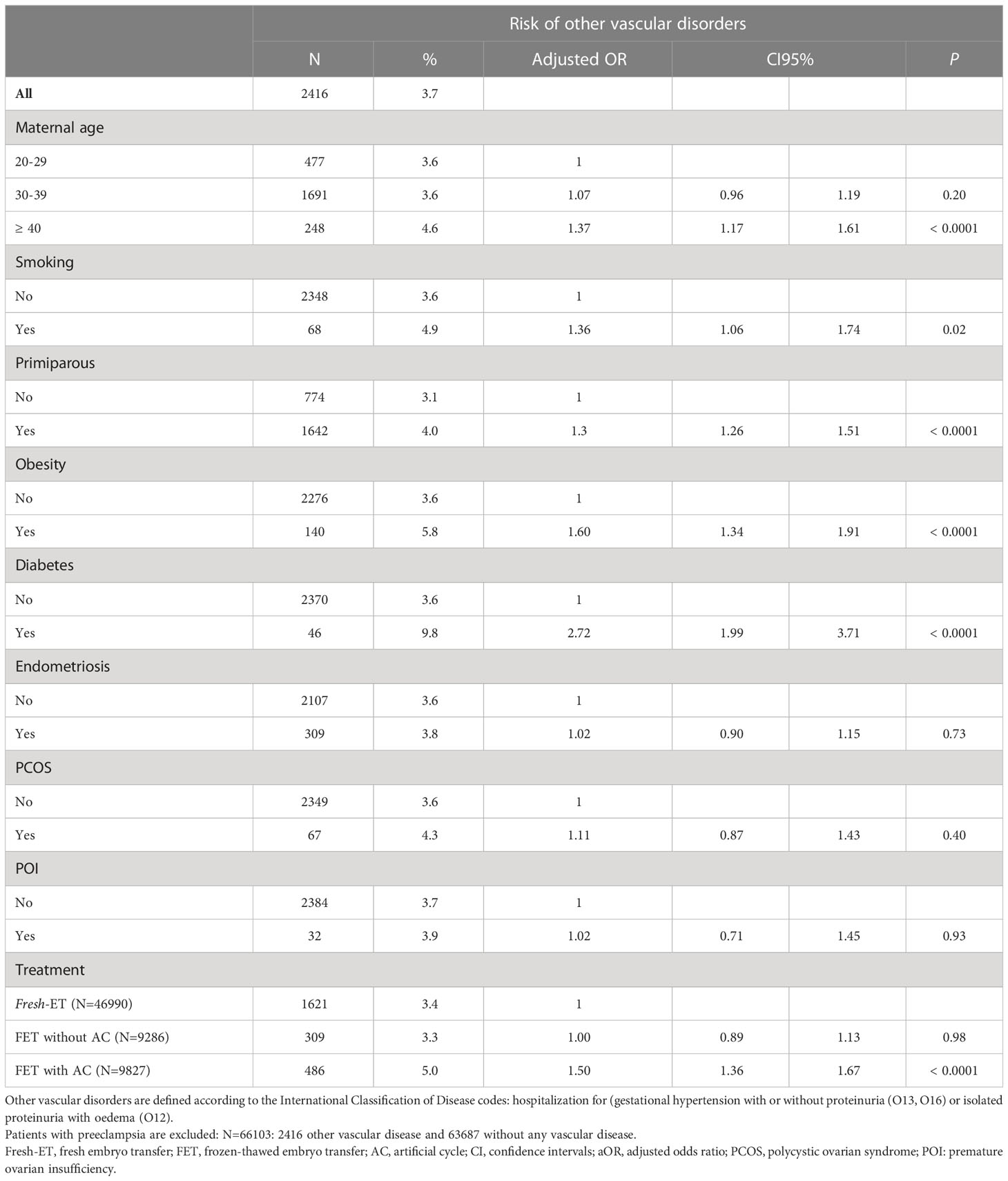
Table 3 Risk of other pregnancy-induced vascular diseases compared to no vascular disease in multivariate analysis (N =66103).
The risk of pre-eclampsia was significantly higher in the AC-FET group compared to OC-FET and fresh-ET groups in univariate analysis (5.3% vs. 2.3% and 2.4%, respectively, P < 0.0001). Similar results were observed for the risk of other vascular disorders in AC-FET compared to OC-FET and fresh-ET in univariate analysis (4.7% vs. 3.4% and 3.3%, P = 0.0002) (Table 1).
In multivariate analysis, the risk of pre-eclampsia compared to no vascular disease was significantly higher in AC-FET compared to fresh-ET (aOR = 2.43 [2.18-2.70], P < 0.0001) (Table 2). The risk was similar between OC-FET and fresh-ET: (aOR = 1.01 [0.87-1.17], P = 0.91) (Table 2).
In multivariate analysis, the risk of other vascular disease compared to no vascular disease was significantly higher in AC-FET compared to fresh-ET (aOR = 1.50 [1.36-1.67], P < 0.0001) (Table 3). The risk was similar between OC-FET and fresh-ET (aOR = 1.00 [0.89-1.13], P = 0.97, respectively) (Table 3).
To confirm the difference between the two endometrial preparation protocols for FET, the same multivariate analyses were performed excluding patients with fresh-ET. The risk of pre-eclampsia and other vascular disorders (compared to no vascular disease) was significantly higher after AC-FET compared to OC-FET: aOR=2.42 [2.06-2.85], P < 0.0001 and aOR=1.50 [1.29-1.74], P < 0.0001, respectively) (Figure 1).
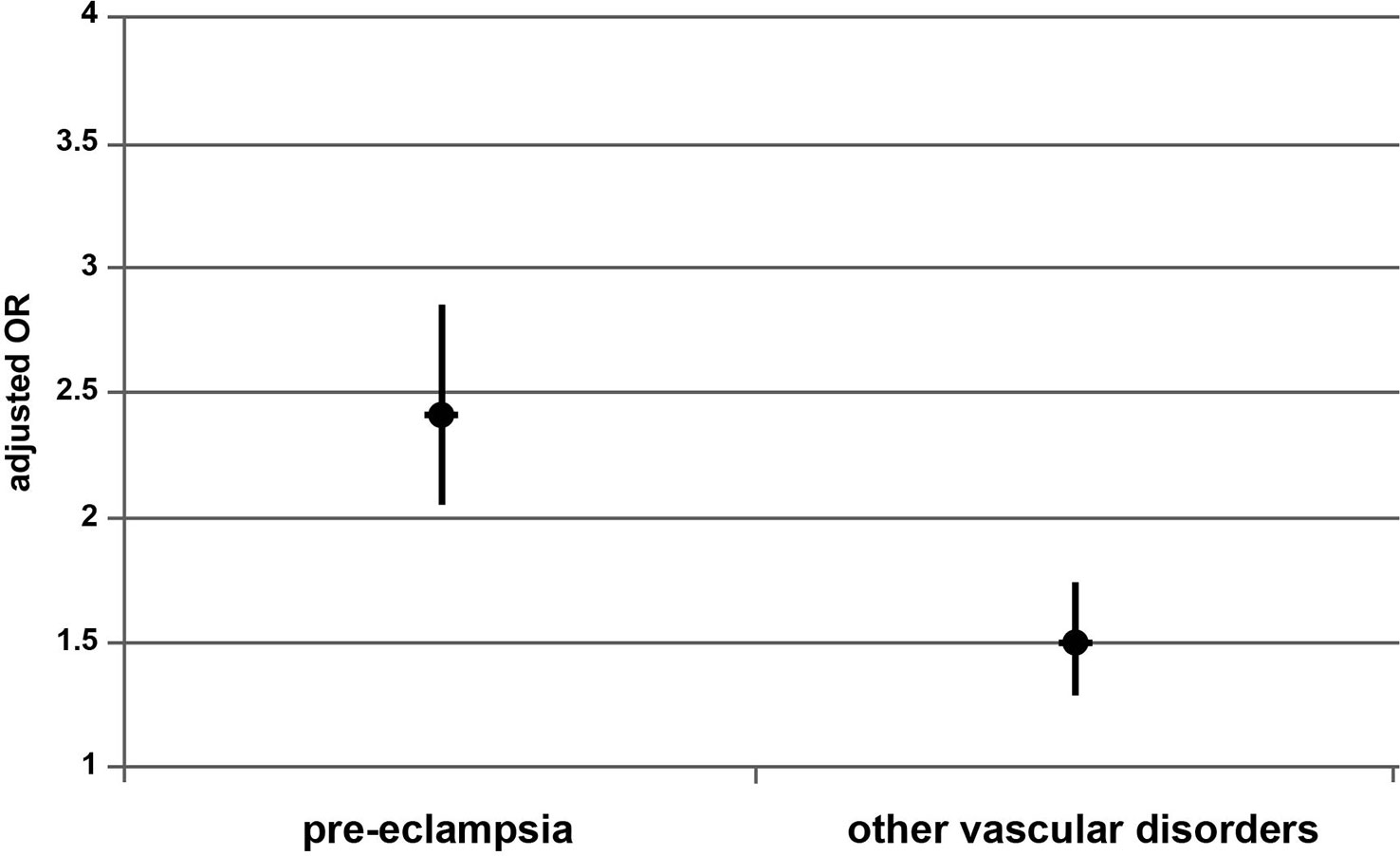
Figure 1 Risk of pre-eclampsia and other vascular disorders after AC-FET compared to OC-FET. AC-FET, artificial cycle for frozen-embryo transfer; OC-FET (line 1), ovulatory cycle for frozen-embryo transfer.
4 Discussion
In all, the findings from this large 5-year nationwide observational study demonstrated that endometrial preparation by AC was associated with an increased risk of pre-eclampsia and other vascular disorders compared to fresh-ET and OC-FET. These results remained significant after multivariate analysis adjusted on maternal characteristics. The risk was similar between OC-FET and fresh-ET.
Several recent publications are in line with our findings. A 2022 retrospective cohort study analysing the incidence of pre-eclampsia in 536 pregnant patients (from either autologous cycles or egg donation) after OC-FET (n = 325) or AC-FET (n= 211) showed that pre-eclampsia was significantly higher in AC cycles (11.8% vs. 3.7%, respectively, P < 0.001). Results remained significant after multivariate logistic regression analysis (AC-FET vs. OC-FET: OR: 2.9, 95% CI 1.4–6.0, P = 0.005) (36). Similarly, a 2022 meta-analysis including 9 studies (n= 8 327 patients with PCOS, pregnant after AC-FET or OC-FET) showed that preterm birth and pre-eclampsia rates were significantly higher with AC-FET compared to OC-FET (37). In addition to the obstetrical aspect, long-term consequences of pre-eclampsia are becoming a concern. A 2021 population-based cohort study using Danish national health registers including 2 491 340 individuals born in Denmark from 1977 to 2018 suggest that the existence of maternal hypertensive disorders during pregnancy is associated with a 23% increased risk of early-onset cardiovascular disease in children (32). Notably, results show an increased risk of specific cardiovascular diseases such as hypertension (HR = 2.11 [1.96-2.27]; P < 0.001), myocardial infarction (HR = 1.49 [1.12-1.98]; P = 0.007), pulmonary embolism (HR = 1.33 [1.11-1.58]; P = 0.002) and heart failure (HR = 1.30 [1.02-1.66]; P = 0.037). Moreover, a 2022 multinational population-based cohort study collecting data from Danish, Finnish and Swedish national registries (including 8 475 819 births, of which 188 670 (2.2%) were exposed to maternal pre-eclampsia) showed that children had an increased risk of ischemic heart disease (aOR = 1.33 [1.12-1.58]) and stroke (aOR = 1.34 [1.17-1.52]) in case of maternal pre-eclampsia (38). These associations were independent from preterm or small for gestational age, but dependent on the severity of pre-eclampsia.
In line with our findings, recent studies describe increased obstetrical risks in the absence of CL (18). The pathophysiology of vascular disorders found increased in the absence of CL seems to involve multiple factors. Indeed, the CL is a major source of estradiol, progesterone and their metabolites, as well as relaxin and vasoactive and angiogenic substances that might optimize implantation and placentation. Therefore, the presence of a CL in endometrial preparation by OC possibly leads to more physiological protein secretion profiles compared to AC (39, 40). A hypothesis for the increased risk of pre-eclampsia in the absence of CL could be the imbalance of steroid hormones and their metabolites influencing early physiological processes such as decidualisation, implantation, angiogenesis and maternal haemodynamic (41). Moreover, serum relaxin levels are almost undetectable in pregnant women without CL. This absence of circulating relaxin may also be at risk of abnormal placentation or compromised maternal cardiovascular adaptation. In 2019, Von Versen-Höynck et al. prospectively assessed rates of gestational vascular pathologies in relation to carotid-femoral pulse wave velocity and transit time before, during and after pregnancy, according to number of CL: 0 (n = 26), 1 (n = 23) or >1 (n = 22) (42). AC-FET cycles (0-CL) were associated with higher rates of pre-eclampsia (12.8% vs. 3.9%, P = 0.02) and severe pre-eclampsia (9.6% vs. 0.8%, P = 0.002) compared to modified natural FET cycles (1 CL). Authors suggested that altered vascular health in early pregnancy in women with 0 CL (AC cycles) might lead to insufficient cardiovascular adaptation contributing to an increased risk of pre-eclampsia (43). Moreover, within the same time, Boutet et al. published a case-control study on maternal and fetal concentrations of haemopexin, a glycoprotein protective of the vascular endothelium, in pre-eclamptic IVF-pregnancies according to presence or not of CL at embryo transfer (44). After adjustment, maternal haemopexin was higher in IVF with CL compared to natural conception in normotensive women (P = 0.04) and in case of pre-eclampsia (P = 0.01), and lower in case of pre-eclampsia in IVF pregnancies without CL compared to IVF pregnancies with CL (P = 0.002). In cord blood, in case of pre-eclampsia, hemopexin was higher in IVF with CL when compared to spontaneous pregnancies (P = 0.04). These physiological differences support the hypothesis that CL activity may influence perinatal outcomes.
The strength of our extensive 5-year nationwide register-based cohort study covering 68025 single deliveries including 19873 resulting from FET, almost equally between preparation by artificial (AC-FET: 10373) or ovulatory cycle (OC-FET: 9500), and 48152 fresh-ET controls, relies in the number and exhaustiveness of subjects analyzed. Moreover, our national database allows us to report broad real-life data considering the numerous confounding factors accessible in the database, including underlying detailed female infertility.
The limitations are linked to the register-based nature of the cohort data, which, although collected prospectively for the National Health Data System, were analyzed retrospectively according to a non-predetermined reading protocol. Therefore, it did not enable to refine the risk according to details of techniques (embryo stage, culture media, slow freezing or vitrification) and treatments (such as use or not of antiplatelet agents) in each group. Our national database provides some information on certain maternal characteristics (age, obesity, POI, PCOS, endometriosis, etc…) but does not enable to establish a possible link with the indication of FET (avoid fresh transfer to prevent the risk of OHSS, deferred transfer of supernumerary embryo after failure of fresh transfer or after a previous pregnancy). Nevertheless, except for POI, maternal underlying infertility (including PCOS) did not impact the incidence of gestational vascular disorders when comparing fresh-ET and both FET populations (Table 2). Therewith, we did not investigate the respective number of deliveries for the same mother over the period studied, which could result either from two successive IVFs with fresh-transfer if there are no supernumerary embryos after the first delivery, or FET for another child after successful IVF and fresh-transfer delivery, or FET for a child followed by IVF with fresh-transfer for the next one, or again2 deliveries after FET. The hypothesis of an increased risk of gestational vascular pathologies in the event of a prior history of gestational hypertensive disorder could be relevant. Nevertheless, the interpretation would be complex since a vascular gestational history induces a preventive therapeutic framework for the subsequent pregnancy, and because of the multiple possible successions of protocols. In this study, except for ET protocols, the risk of pre-eclampsia and other vascular disorders also increased with age, primiparity, obesity, history of diabetes and POI. Given the multicentric and retrospective nature of this national cohort, it was not possible for us to test the hypothesis of any association between those factors and the protocol choose for ET
In the growing trend of ART centers to practice more and more embryonic freeze-all, the choice of endometrial preparation in full knowledge of its side effects is of primary importance. The two lessons learned from these broad national data are as much warning information regarding the risk factor for preeclampsia and other vascular disorders represented by the artificial cycle preparation, than a reassuring message stemming from the data concerning the ovulatory cycle.
The choice of treatment for FET is possible in women whose ovarian function is present. Growing evidence highlights the possibly fundamental nature of the contribution of the CL in the prevention of adverse obstetrical and perinatal outcomes during pregnancy (45). Pereira et al. (41) stated that a better understanding of the critical roles of the secretory products of the CL during early pregnancy held the promise of improving the efficacy and safety of ART based on programmed FET cycles.
Until recently, the decision on the endometrial preparation protocol most often depended on center procedures, based on medical arguments, expected success rates, pregnancy loss rates, feasibility, organization and regulation of the center’s activity and women’s comfort. Medical arguments are essentially based on the possibility of ovulation of the woman. Obviously, dysovulations or anovulations determine a preparation with AC. If AC cycle with or without GnRH-agonist pre-treatment has long been the first choice for PCOS patients, current trends follow the principles of individualization, securitization and optimization in endometrial preparation, as mean endometrial thickness, implantation rates, clinical pregnancy rates, ongoing pregnancy rates and live birth rates are similar in artificial cycle and stimulated cycle for endometrial preparation prior to FET in PCOS (46, 47). Guo et al’s recent retrospective study on 1413 cases suggested that natural cycle, hormone replacement cycle, or hormone replacement treatment with GnRHa pretreatment showed no superiority or inferiority in pregnancy and perinatal outcomes in patients with endometriosis (48). Furthermore, the organizational argument has long prevailed in favor of AC-FET, which makes it possible to regulate transfers along the week. However, the use of antagonists in modified natural cycles allows an almost comparable flexibility. The argument of women’s comfort between a few days of subcutaneous injections in the stimulated protocols then about 6 weeks of progesterone (the vaginal route being the most used in France) in OC, and 3 months of oral estrogen intake and vaginal progesterone in AC protocol, is a very subjective consideration. The cost-effectiveness argument between the two protocols, including the cost of pregnancy concerns (such as hospitalization for pregnancy loss or pre-eclampsia and its complications), has poorly been studied and varies according to the country and the financial support. A recent retrospective study considering overweight/obese women with PCOS, suggested that midly stimulated preparation for FET demonstrated a higher LBR and a lower pregnancy loss rate than that in the AC-FET, and may be considered. as the most cost-effective treatment with the least adverse effects on patients (49). The argument for success has long been in favor of AC-FET, until considering the increased number of miscarriages and therefore the lower live birth rate (LBR) with AC when compared with OC.”
Zhang et al. (37) suggested that endometrial preparation by OC might be superior to AC, with significantly higher live birth rates and lower risks of miscarriage, preterm birth and pre-eclampsia, even for women with PCOS (37). Von Versen-Höynck et al. also concluded that pregnancy in the absence of CL could lead to adverse maternal and foetal risks and suggested that the existing evidence was already sufficient to discourage the use of AC-FET in women who ovulate, as they generate a deviation from physiology, exposing the patient and fetus to an avoidable health risk with no apparent benefit (42).
Hence, wider implications of this nationwide register-based cohort study are that it highlights two important information for physicians: i) the possible deleterious role of non-physiological and prolonged doses of exogenous estrogen-progesterone supplementation on gestational vascular pathologies ii) the protective role of the CL present in stimulated or spontaneous OC for their prevention. Our conclusions could help to change habits, especially since the possible addition of antagonists in OC allows a satisfactory programming of embryo transfer, which is the principal advantage of using AC in ART centers. Since results obtained by OC do not strain the chances of pregnancy, OC preparation could be advocated as first-line endometrial preparation in FET as often as the choice is possible in ovulatory women. Nevertheless, one must consider what specific management could be proposed for cases in which AC is unavoidable, as egg donation for pre-menopausal or menopausal women, or irreducible cases of anovulation or dysovulation generating a long and painful stimulation in women. Developing strategies to reduce the risk of pre-eclampsia are required. The preventive efficacy of antiplatelet agents in AC remains to be established. The present study should also be extended by a long-term follow-up of the cohort in order to evaluate the possible association of maternal pre-eclampsia with an increased risk of subsequent vascular pathologies in the offspring.
Data availability statement
The datasets presented in this article are not readily available because we used the French National hospitalization database (PMSI), included in the large French National Health System database (Système National des Données de Santé (SNDS), in which all hospitalizations (in any public hospital or private clinic) are registered, containing information on patient characteristics, diagnoses and treatments. Data were anonymized at data entry through a specific software making it impossible to retrieve patient identity but enabling to follow all hospitalizations through anonymized codes. Access to PMSI data and SNDS was legally approved in accordance with French Public Health Law (decree N° 2016-1871). Access to PMSI and SNDS data for organizations that do not have permanent access or matching with other databases already available goes through an authorization procedure that involves several organizations: the National Data Institute health (INDS, which in 2019 became the health data platform, the Expertise Committee for research, studies and evaluations in the field of health (CESREES). Consequently, data are available after obtaining legal authorization (at https://www.indsante.fr/) and from the CNIL (Commission Nationale Informatique et Liberte; CNIL, https://www.cnil.fr/). According to the French Public Health Law, non-interventional studies on humans do not require approval from an Institutional Review Board or written consent from participants. The study was conducted according to institutional and ethical rules concerning research on tissue specimens and patients. Requests to access the datasets should be directed toc3lsdmllLmVwZWxib2luQGFwaHAuZnI=.
Ethics statement
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
SE, FP: study conception and design. SE, JL, PF, FP: methodology and investigation. FP: formal analysis. JM, M-JG-B, LH, NS, RL, PJ: resources. SE, JL, PF, FP: writing—original draft preparation. SE, JL, PF, FP: writing—review and editing. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Groenewoud ER, Cohlen BJ, Macklon NS. Programming the endometrium for deferred transfer of cryopreserved embryos: hormone replacement versus modified natural cycles. Fertil Steril (2018) 109:768–74. doi: 10.1016/j.fertnstert.2018.02.135
2. Healy MW, Patounakis G, Connell MT, Devine K, DeCherney AH, Levy MJ, et al. Does a frozen embryo transfer ameliorate the effect of elevated progesterone seen in fresh transfer cycles? Fertil Steril (2016) 105:93–99.e1. doi: 10.1016/j.fertnstert.2015.09.015
3. Rienzi L, Gracia C, Maggiulli R, LaBarbera AR, Kaser DJ, Ubaldi FM, et al. Oocyte, embryo and blastocyst cryopreservation in ART: systematic review and meta-analysis comparing slow-freezing versus vitrification to produce evidence for the development of global guidance. Hum Reprod Update (2017) 23:139–55. doi: 10.1093/humupd/dmw038
4. Roque M, Valle M, Guimarães F, Sampaio M, Geber S. Freeze-all policy: fresh vs. frozen-thawed embryo transfer. Fertil Steril (2015) 103:1190–3. doi: 10.1016/j.fertnstert.2015.01.045
5. Roque M, Haahr T, Geber S, Esteves SC, Humaidan P. Fresh versus elective frozen embryo transfer in IVF/ICSI cycles: a systematic review and meta-analysis of reproductive outcomes. Hum Reprod Update (2019) 25:2–14. doi: 10.1093/humupd/dmy033
6. Devroey P, Polyzos NP, Blockeel C. An OHSS-free clinic by segmentation of IVF treatment. Hum Reprod (2011) 26:2593–7. doi: 10.1093/humrep/der251
7. Groenewoud ER, Cantineau AEP, Kollen BJ, Macklon NS, Cohlen BJ. What is the optimal means of preparing the endometrium in frozen-thawed embryo transfer cycles? a systematic review and meta-analysis. Hum Reprod Update (2017) 23:255–61. doi: 10.1093/humupd/dmw046
8. Racca A, Vanni VS, Somigliana E, Reschini M, Viganò P, Santos-Ribeiro S, et al. Is a freeze-all policy the optimal solution to circumvent the effect of late follicular elevated progesterone? a multicentric matched-control retrospective study analysing cumulative live birth rate in 942 non-elective freeze-all cycles. Hum Reprod (2021) 36:2463–72. doi: 10.1093/humrep/deab160
9. Vidal M, Vellvé K, González-Comadran M, Robles A, Prat M, Torné M, et al. Perinatal outcomes in children born after fresh or frozen embryo transfer: a Catalan cohort study based on 14,262 newborns. Fertil Steril (2017) 107:940–7. doi: 10.1016/j.fertnstert.2017.01.021
10. Maheshwari A, Kalampokas T, Davidson J, Bhattacharya S. Obstetric and perinatal outcomes in singleton pregnancies resulting from the transfer of blastocyst-stage versus cleavage-stage embryos generated through in vitro fertilization treatment: a systematic review and meta-analysis. Fertil Steril (2013) 100:1615–1621.e1–10. doi: 10.1016/j.fertnstert.2013.08.044
11. Wale PL, Gardner DK. The effects of chemical and physical factors on mammalian embryo culture and their importance for the practice of assisted human reproduction. Hum Reprod Update (2016) 22:2–22. doi: 10.1093/humupd/dmv034
12. Pinborg A, Wennerholm UB, Romundstad LB, Loft A, Aittomaki K, Söderström-Anttila V, et al. Why do singletons conceived after assisted reproduction technology have adverse perinatal outcome? systematic review and meta-analysis. Hum Reprod Update (2013) 19:87–104. doi: 10.1093/humupd/dms044
13. Luke B. Pregnancy and birth outcomes in couples with infertility with and without assisted reproductive technology: with an emphasis on US population-based studies. Am J Obstet Gynecol (2017) 217:270–81. doi: 10.1016/j.ajog.2017.03.012
14. Epelboin S, Labrosse J, Fauque P, Levy R, Gervoise-Boyer M-J, Devaux A, et al. Endometriosis and assisted reproductive techniques independently related to mother-child morbidities: a French longitudinal national study. Reprod BioMed Online (2021) 42:627–33. doi: 10.1016/j.rbmo.2020.11.017
15. Toner JP, Coddington CC, Doody K, Van Voorhis B, Seifer DB, Ball GD, et al. Society for assisted reproductive technology and assisted reproductive technology in the united states: a 2016 update. Fertil Steril (2016) 106:541–6. doi: 10.1016/j.fertnstert.2016.05.026
16. Maheshwari A, Pandey S, Amalraj Raja E, Shetty A, Hamilton M, Bhattacharya S. Is frozen embryo transfer better for mothers and babies? can cumulative meta-analysis provide a definitive answer? Hum Reprod Update (2018) 24:35–58. doi: 10.1093/humupd/dmx031
17. Qin J, Liu X, Sheng X, Wang H, Gao S. Assisted reproductive technology and the risk of pregnancy-related complications and adverse pregnancy outcomes in singleton pregnancies: a meta-analysis of cohort studies. Fertil Steril (2016) 105:73–85.e1–6. doi: 10.1016/j.fertnstert.2015.09.007
18. Saito K, Kuwahara A, Ishikawa T, Morisaki N, Miyado M, Miyado K, et al. Endometrial preparation methods for frozen-thawed embryo transfer are associated with altered risks of hypertensive disorders of pregnancy, placenta accreta, and gestational diabetes mellitus. Hum Reprod (2019) 34:1567–75. doi: 10.1093/humrep/dez079
19. Wei D, Liu J-Y, Sun Y, Shi Y, Zhang B, Liu J-Q, et al. Frozen versus fresh single blastocyst transfer in ovulatory women: a multicentre, randomised controlled trial. Lancet (2019) 393:1310–8. doi: 10.1016/S0140-6736(18)32843-5
20. Ginström Ernstad E, Wennerholm U-B, Khatibi A, Petzold M, Bergh C. Neonatal and maternal outcome after frozen embryo transfer: increased risks in programmed cycles. Am J Obstet Gynecol (2019) 221:126.e1–126.e18. doi: 10.1016/j.ajog.2019.03.010
21. Pessione F, De Mouzon J, Deveaux A, Epelboin S, Gervoise-Boyer M-J, Jimenez C, et al. Risques de morbidité maternelle et périnatale en fécondation in vitro : une étude nationale de cohorte française. Gynécol Obstétrique Fertilité Sénol (2020) 48:351–8. doi: 10.1016/j.gofs.2020.02.002
22. Bonnet M-P, Garnier M, Keita H, Compere V, Arthuis C, Raia-Barjat T, et al. Reprint of: severe pre-eclampsia: guidelines for clinical practice from the French society of anesthesiology and intensive care (SFAR) and the French college of gynaecologists and obstetricians (CNGOF). Gynecol Obstet Fertil Senol (2022) 50:2–25. doi: 10.1016/j.gofs.2021.11.003
23. Poon LC, Shennan A, Hyett JA, Kapur A, Hadar E, Divakar H, et al. The international federation of gynecology and obstetrics (FIGO) initiative on pre-eclampsia: a pragmatic guide for first-trimester screening and prevention. Int J Gynaecol Obstet (2019) 145 Suppl 1:1–33. doi: 10.1002/ijgo.12802
24. SPF. Les Morts maternelles en France: mieux comprendre pour mieux prévenir. 5e rapport de l’Enquête nationale confidentielle sur les morts maternelles (ENCMM), 2010-2012. Available at: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-cardiovasculaires-et-accident-vasculaire-cerebral/maladie-vasculaire-de-la-grossesse/les-morts-maternelles-en-france-mieux-comprendre-pour-mieux-prevenir.-5e-rapport-de-l-enquete-nationale-confidentielle-sur-les-morts (Accessed April 30, 2023).
25. Ancel P-Y, Goffinet F, EPIPAGE-2 Writing Group, Kuhn P, Langer B, Matis J, et al. Survival and morbidity of preterm children born at 22 through 34 weeks’ gestation in France in 2011: results of the EPIPAGE-2 cohort study. JAMA Pediatr (2015) 169:230–8. doi: 10.1001/jamapediatrics.2014.3351
26. Shanmugalingam R, Wang X, Motum P, Fulcher I, Lee G, Kumar R, et al. Clinical influence of nonadherence with prophylactic aspirin in preventing preeclampsia in high-risk pregnancies. Hypertension (2020) 75:1125–32. doi: 10.1161/HYPERTENSIONAHA.119.14107
27. Herman HG, Volodarsky-Perel A, Ton Nu TN, Machado-Gedeon A, Cui Y, Shaul J, et al. Diminished ovarian reserve is a risk factor for preeclampsia and placental malperfusion lesions. Fertil Steril (2023). doi: 10.1016/j.fertnstert.2023.01.029
28. Epelboin S, Labrosse J, Fauque P, Levy R, Gervoise-Boyer M-J, Devaux A, et al. Endometriosis and assisted reproductive techniques independently related to mother-child morbidities: a French longitudinal national study. Reprod Biomed Online (2021) 42:627–33. doi: 10.1016/j.rbmo.2020.11.017
29. Jing S, Li X, Zhang S, Gong F, Lu G, Lin G. Increased pregnancy complications following frozen-thawed embryo transfer during an artificial cycle. J Assist Reprod Genet (2019) 36:925–33. doi: 10.1007/s10815-019-01420-1
30. Mumusoglu S, Polat M, Ozbek IY, Bozdag G, Papanikolaou EG, Esteves SC, et al. Preparation of the endometrium for frozen embryo transfer: a systematic review. Front Endocrinol (Lausanne) (2021) 12:688237. doi: 10.3389/fendo.2021.688237
31. Busnelli A, Schirripa I, Fedele F, Bulfoni A, Levi-Setti PE. Obstetric and perinatal outcomes following programmed compared to natural frozen-thawed embryo transfer cycles: a systematic review and meta-analysis. Hum Reprod (2022) 37:1619–41. doi: 10.1093/humrep/deac073
32. Huang C, Li J, Qin G, Liew Z, Hu J, László KD, et al. Maternal hypertensive disorder of pregnancy and offspring early-onset cardiovascular disease in childhood, adolescence, and young adulthood: a national population-based cohort study. PloS Med (2021) 18:e1003805. doi: 10.1371/journal.pmed.1003805
33. Rosalik K, Carson S, Pilgrim J, Luizzi J, Levy G, Heitmann R, et al. Effects of different frozen embryo transfer regimens on abnormalities of fetal weight: a systematic review and meta-analysis. Hum Reprod Update (2021) 28:1–14. doi: 10.1093/humupd/dmab037
34. Asserhøj LL, Spangmose AL, Aaris Henningsen A-K, Clausen TD, Ziebe S, Jensen RB, et al. Adverse obstetric and perinatal outcomes in 1,136 singleton pregnancies conceived after programmed frozen embryo transfer (FET) compared with natural cycle FET. Fertil Steril (2021) 115:947–56. doi: 10.1016/j.fertnstert.2020.10.039
35. Makhijani R, Bartels C, Godiwala P, Bartolucci A, Nulsen J, Grow D, et al. Maternal and perinatal outcomes in programmed versus natural vitrified-warmed blastocyst transfer cycles. Reprod BioMed Online (2020) 41:300–8. doi: 10.1016/j.rbmo.2020.03.009
36. Roelens C, Blockeel C. Impact of different endometrial preparation protocols before frozen embryo transfer on pregnancy outcomes: a review. Fertil Steril (2022) 118:820–7. doi: 10.1016/j.fertnstert.2022.09.003
37. Zhang Y, Wu L, Li TC, Wang CC, Zhang T, Chung JPW. Systematic review update and meta-analysis of randomized and non-randomized controlled trials of ovarian stimulation versus artificial cycle for endometrial preparation prior to frozen embryo transfer in women with polycystic ovary syndrome. Reprod Biol Endocrinol (2022) 20:62. doi: 10.1186/s12958-022-00931-4
38. Yang F, Janszky I, Gissler M, Roos N, Wikström A-K, Yu Y, et al. Association of maternal preeclampsia with offspring risks of ischemic heart disease and stroke in Nordic countries. JAMA Netw Open (2022) 5:e2242064. doi: 10.1001/jamanetworkopen.2022.42064
39. Casper RF, Yanushpolsky EH. Optimal endometrial preparation for frozen embryo transfer cycles: window of implantation and progesterone support. Fertil Steril (2016) 105:867–72. doi: 10.1016/j.fertnstert.2016.01.006
40. Fauser BC, de Jong D, Olivennes F, Wramsby H, Tay C, Itskovitz-Eldor J, et al. Endocrine profiles after triggering of final oocyte maturation with GnRH agonist after cotreatment with the GnRH antagonist ganirelix during ovarian hyperstimulation for in vitro fertilization. J Clin Endocrinol Metab (2002) 87:709–15. doi: 10.1210/jcem.87.2.8197
41. Pereira MM, Mainigi M, Strauss JF. Secretory products of the corpus luteum and preeclampsia. Hum Reprod Update (2021) 27:651–72. doi: 10.1093/humupd/dmab003
42. von Versen-Höynck F, Narasimhan P, Selamet Tierney ES, Martinez N, Conrad KP, Baker VL, et al. Absent or excessive corpus luteum number is associated with altered maternal vascular health in early pregnancy. Hypertension (2019) 73:680–90. doi: 10.1161/HYPERTENSIONAHA.118.12046
43. Conrad KP, von Versen-Höynck F, Baker VL. Risk of preeclampsia in artificial frozen embryo transfer as a result of insufficient corpus luteum hormone levels: a response. Am J Obstet Gynecol (2022) 227:676–7. doi: 10.1016/j.ajog.2022.06.011
44. Boutet ML, Youssef L, Erlandsson L, Hansson E, Manau D, Crispi F, et al. Maternal and fetal haemopexin and α1-microglobulin concentrations in pre-eclamptic IVF pregnancies according to presence of corpus luteum at embryo transfer. Reprod BioMed Online (2022) 45:135–45. doi: 10.1016/j.rbmo.2022.01.005
45. Singh B, Reschke L, Segars J, Baker VL. Frozen-thawed embryo transfer: the potential importance of the corpus luteum in preventing obstetrical complications. Fertil Steril (2020) 113:252–7. doi: 10.1016/j.fertnstert.2019.12.007
46. Yu J, Ma Y, Wu Z, Li Y, Tang L, Li Y, et al. Endometrial preparation protocol of the frozen-thawed embryo transfer in patients with polycystic ovary syndrome. Arch Gynecol Obstet (2015) 291:201–11. doi: 10.1007/s00404-014-3396-0
47. Bosdou JK, Anagnostis P, Kolibianakis EM. Is pretreatment with GnRH agonist necessary for endometrial preparation for frozen embryo transfer cycles in women with polycystic ovary syndrome? BJOG (2021) 128:675. doi: 10.1111/1471-0528.16473
48. Guo Y, Fang Z, Yu L, Sun X, Li F, Jin L. Which endometrial preparation protocol provides better pregnancy and perinatal outcomes for endometriosis patients in frozen-thawed embryo transfer cycles? a retrospective study on 1413 patients. J Ovarian Res (2023) 16:7. doi: 10.1186/s13048-023-01095-4
49. Guan L, Wu H, Wei C, Pang C, Liu D, Yu X, et al. The effect of mildly stimulated cycle versus artificial cycle on pregnancy outcomes in overweight/obese women with PCOS prior to frozen embryo transfer: a retrospective cohort study. BMC Pregnancy Childbirth (2022) 22:394. doi: 10.1186/s12884-022-04728-6
Keywords: pre-eclampsia, artificial cycle, ovulatory cycle, frozen embryo transfer, fresh embryo transfer, endometrial preparation
Citation: Epelboin S, Labrosse J, De Mouzon J, Devaux A, Gervoise-Boyer M-J, Hesters L, Jonveaux P, Levy R, Sermondade N, Fauque P and Pessione F (2023) Higher risk of pre-eclampsia and other vascular disorders with artificial cycle for frozen-thawed embryo transfer compared to ovulatory cycle or to fresh embryo transfer following in vitro fertilization. Front. Endocrinol. 14:1182148. doi: 10.3389/fendo.2023.1182148
Received: 08 March 2023; Accepted: 04 May 2023;
Published: 22 May 2023.
Edited by:
Zhen-Gao Sun, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, ChinaReviewed by:
Xiufeng Ling, Nanjing Medical University, ChinaBeihong Zheng, Fujian Women and Children Hospital, China
Copyright © 2023 Epelboin, Labrosse, De Mouzon, Devaux, Gervoise-Boyer, Hesters, Jonveaux, Levy, Sermondade, Fauque and Pessione. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sylvie Epelboin, c3lsdmllLmVwZWxib2luQGFwaHAuZnI=
†These authors have contributed equally to this work and share first authorship