
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Endocrinol. , 14 August 2023
Sec. Clinical Diabetes
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1177020
This article is part of the Research Topic Improving Outcomes in Diabetic Foot Care - A Worldwide Perspective View all 16 articles
 Virginie Blanchette1,2,3*
Virginie Blanchette1,2,3* Jérôme Patry3,4
Jérôme Patry3,4 Magali Brousseau-Foley1,5
Magali Brousseau-Foley1,5 Shweta Todkar6Solène Libier1Anne-Marie Leclerc6David G. Armstrong7Marie-Claude Tremblay2,4
Shweta Todkar6Solène Libier1Anne-Marie Leclerc6David G. Armstrong7Marie-Claude Tremblay2,4Introduction: Indigenous peoples in Canada face a disproportionate burden of diabetes-related foot complications (DRFC), such as foot ulcers, lower extremity amputations (LEA), and peripheral arterial disease. This scoping review aimed to provide a comprehensive understanding of DRFC among First Nations, Métis, and Inuit peoples in Canada, incorporating an equity lens.
Methods: A scoping review was conducted based on Arksey and O’Malley refined by the Joanna Briggs Institute. The PROGRESS-Plus framework was utilized to extract data and incorporate an equity lens. A critical appraisal was performed, and Indigenous stakeholders were consulted for feedback. We identified the incorporation of patient-oriented/centered research (POR).
Results: Of 5,323 records identified, 40 studies were included in the review. The majority of studies focused on First Nations (92%), while representation of the Inuit population was very limited populations (< 3% of studies). LEA was the most studied outcome (76%). Age, gender, ethnicity, and place of residence were the most commonly included variables. Patient-oriented/centered research was mainly included in recent studies (16%). The overall quality of the studies was average. Data synthesis showed a high burden of DRFC among Indigenous populations compared to non-Indigenous populations. Indigenous identity and rural/remote communities were associated with the worse outcomes, particularly major LEA.
Discussion: This study provides a comprehensive understanding of DRFC in Indigenous peoples in Canada of published studies in database. It not only incorporates an equity lens and patient-oriented/centered research but also demonstrates that we need to change our approach. More data is needed to fully understand the burden of DRFC among Indigenous peoples, particularly in the Northern region in Canada where no data are previously available. Western research methods are insufficient to understand the unique situation of Indigenous peoples and it is essential to promote culturally safe and quality healthcare.
Conclusion: Efforts have been made to manage DRFC, but continued attention and support are necessary to address this population’s needs and ensure equitable prevention, access and care that embraces their ways of knowing, being and acting.
Systematic review registration: Open Science Framework https://osf.io/j9pu7, identifier j9pu7.
The estimated population of Canada is 40 million and the diabetes rate is rising (1, 2). Canada’s Constitution Act (1982) recognizes three distinct groups of Indigenous peoples: First Nations, Inuit and Métis, and they account for around 5% in Canada’s total population (3, 4). Approximately 58% of the Indigenous population in Canada identifies as First Nations (5). The demographic of this population is growing rapidly, and young people are more exposed to diabetes and its complications (3, 6–8). Indigenous peoples are affected by type-2 diabetes 3 to 5 times higher than the general population and this chronic disease is one of the fastest increasing health issues among this population (7). Indigenous peoples worldwide, including in Canada, are disproportionately affected by diabetes due to many factors such as genetic predisposition, new environmental exposures, poverty, scarcity of resources and many other barriers that can affect an optimal diabetes care (e.g., geographical isolation, educational status, employment disadvantage, both cultural and linguistic differences) (9, 10). From an Indigenous perspective, rooted in a holistic understanding of health, diabetes is perceived as being associated with the processes of colonization, notably through the loss of traditional ways of life and spirituality, socio-economic marginalization, socio-cultural upheaval, stress and racism (11).
Indeed, Indigenous peoples are diagnosed with diabetes at a younger age, have greater severity of diagnosis, develop higher rates of complications and experience poorer treatment outcomes (12). These outcomes are greater with remote and rural populations (13). Compared to non-First Nations, older First Nations individuals with diabetes are at greater risk of diabetes-specific hospitalization and this can be challenged in regard to ethnocultural considerations and the geographical realities (14). They are also more at-risk of experiencing diabetes-related foot complications (DRFC) such as diabetic foot ulcer (DFU), lower extremity amputations (LEA), infections, foot deformities, Charcot neuroarthropathy, peripheral arterial disease (PAD) and neuropathy (12, 15).
Up to 34% of people with diabetes will develop a DFU during their lifetime which is a significant cause of disabilities, reduces quality of life and can lead to premature death (16). Moreover, LEAs, which are an estimated potential outcome for 1 in 5 DFUs, have an estimated 5-year mortality rate of 51% after a major LEA (16, 17). Personal, societal and economic outcomes of DRFC highlight the importance of supporting prevention strategies for the at-risk population and implementing effective team management approach (18, 19). It is even more important to act towards populations facing at time multiple and intersecting oppression, such as Indigenous peoples, since ethnicity has been identified as a predictor of worse outcomes such as LEAs and health care marginalization (15, 20, 21). It is even more appropriate to talk about the colonization and oppression rather than ethnicity which has led to the worst outcomes for this population and therefore this population has particular cultural needs (22). Thereafter, we refer to indigenous identity and not to ethnicity to respect these peoples. The effect of rurality is also closely associated especially for LEAs (15, 23, 24). Some evidence is published worldwide about diabetic foot disease and DRFC among Indigenous peoples (10, 25, 26), but the specific portrayal of DRFC for Indigenous peoples in Canada is lacking. It is recognized that there are health inequities and disparities as well as poor health care experience for this population (27, 28). Therefore, the aim of this scoping review is to map the existing literature related to diabetic foot disease among Indigenous peoples in Canada based on a western systematic methodology and incorporating an equity lens.
The present study will follow the six-stage approach developed by Arksey and O’Malley (29), refined by Levac and Colquhoun (30, 31), and also described by the Joanna Briggs Institute (32). Those stages are mentioned thereafter. Reporting will be compliant with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) Checklist (33). The iterative nature of scoping review includes refinement of specific sections of the method as the review progresses. This project has been registered on Open Science Framework (https://osf.io/j9pu7/).
Based on PICO strategy (34): What are the data regarding diabetes-related foot health outcomes (O) among Indigenous peoples in Canada (P), whether compared to the general population or not (C), for all types of health interventions including epidemiological surveillance data (I). Specific questions were:
● What is the available data on DRFC such as DFU, LEA, diabetic foot infection (DFI) experienced by Indigenous peoples in Canada?
● What is the available data on diabetes foot disease risk factors such as foot deformities, Charcot neuroarthropathy, PAD and neuropathy in Indigenous peoples in Canada?
● What is the available data on diabetic foot disease and DFRC on quality of life and mortality?
● What are other relevant variables such as patient-related outcomes and patient-related experiences related to this topic in Indigenous peoples in Canada?
● Does the reported data on this topic include demographic and equity factors based on the PROGRESS-Plus framework (35)?
● Do the included studies report any collaborations and/or partnerships with Indigenous peoples and/or community related to patient-oriented/centered research (36)?
The PROGRESS-Plus framework was developed for describing and assessing equity related to the social determinants of health within and across populations (37). Patient-oriented/centered research (POR) can support equity-focused health care research with Indigenous peoples, as the research findings are based on their needs, perspective and context as active stakeholders in the process (36, 38).
The broad concept of interest in this study was to identify the burdens of diabetic foot disease/DFRC experienced by Indigenous peoples in Canada. Diabetic foot disease/DFRC were mostly defined by the International Working Group on the Diabetic Foot (IWGDF) criteria and definitions (39). The “diabetic foot ulcer (DFU) “is defined as a break of the skin of the foot, that involves as a minimum the epidermis and part of the dermis, in a person with currently or previously diagnosed with diabetes and usually accompanied by neuropathy and/or peripheral arterial disease within the lower extremity; “neuropathy” is defined as the presence of symptoms or signs of nerve dysfunction in a person (a history of) with diabetes, after the exclusion of other causes. This can also include loss of protective sensation characterized by an inability to sense light pressure (10 g Semmes-Weinstein monofilament); “Peripheral artery disease” (PAD) is defined as an obstructive atherosclerotic vascular disease with clinical symptoms, signs, or abnormalities on non-invasive or invasive vascular assessment, resulting in disturbed or impaired circulation in one or more extremities. This can cause claudication and rest pain. “Infection” is defined as a pathological state caused by invasion and multiplication of microorganisms in host tissues accompanied by tissue destruction and/or a host inflammatory response; “lower extremity amputations (LEA)” is defined as a resection of a segment of a limb through a bone or through a joint; Charcot neuroarthropathy (Charcot foot) is a non-infectious destruction of bone(s) and joint(s) associated with neuropathy, which, in the acute phase, is associated with signs of inflammation (39). “Foot deformities” are defined as structural and functional foot deformities occurring with diabetes and motor neuropathy causing atrophy and muscle imbalances such as claw and hammer toes, prominent metatarsal heads, pes cavus, pes equinus, hallux limitus or rigidus and hallux abductovalgus (40). The Western “health-related quality of life” refers to an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. It is a broad-ranging concept affected in a complex way by the individual’s physical health, psychological state, level of independence, social relationships, and their relationships to salient features of their environment as they relate to the DRFC context (41).
The search protocol and strategies were developed by two members of the research team (VB and JP) and revised by another team member (MBF). The primary information source included systematic search from the following database: 1) MEDLINE, 2) CINAHL, 3) EMBASE, 4) Cochrane Library, 5) Native Health Database, 6) Government Health Indigenous Affairs Departments of the United States/Canada and 7) LiSSa. The secondary information source included reference lists as well as citation searches of related relevant citations. Canadian clinical guidelines from major organizations with an interest towards in diabetic population were reviewed. Grey literature was assessed through Google Scholar, Open Access Theses and Dissertations, ProQuest, ClinicalTrials.gov and Réseau Santécom. The search strategy, limited to articles in English and French, was developed for MEDLINE database (Supplement Material 1), with the assistance of a qualified librarian and involved a combination of key terms and concepts (MeSH, non-MeSH, key terms and free vocabulary). The search strategy was adapted for other databases and identical terms translated to French were used to search in selected French-language databases. This review had searched articles from inception up to August 29th, 2022. Citations from all information sources were merged and duplicates removed using EndNote (version 20.4, Clarivate Analytics, 2022).
Two independent reviewers (VB and JP) initially met to clarify the following inclusion criteria:
● Population: Adult (18 years and older) Indigenous peoples in Canada with either type-1 or type-2 diabetes with any DRFC or disease;
● Intervention: Any interventions including none;
● Comparator(s)/control: Other populations or none;
● Outcomes: Results pertaining or describing data about DRFC on DFU, LEA, DFI, quality of life, mortality, foot deformities, Charcot foot, PAD, neuropathy or other relevant data about DRFC (e.g., DFU recurrence, genetics, etc.);
● Settings: Any clinical settings or community;
● Languages: English or French
Exclusion criteria were:
● Publication/study design: Conference or meeting abstracts, commentaries, letters and correspondences, Editor’s response, protocol descriptions;
● Population: Individuals who were not considered as Indigenous in Canada (e.g., native from other countries); gestational diabetes; wounds, amputation or death in the absence of a diagnosis of either type-1 or type-2 diabetes.
The search strategy was completed by one of the authors (VB). Two arms of reviewers (VB/JP and VB/SL) have independently screened titles and abstracts using eligibility criteria. Then, relevant papers were read entirely, and eligibility criteria were systematically applied. Disagreement was settled using a consensus approach between reviewers and a third person intervened if required (MBF). Eligibility criteria were clarified following a training exercise on the first 300 citations and inter-rater agreement (kappa statistic) was greater than k=0.70, signifying substantial agreement, and then selection was completed (42).
A Microsoft Excel (Microsoft Corporation) spreadsheet served as the data extraction form developed by the two reviewers (VB and AML) and updated by an iterative manner during the full article revision process. The data-charting form includes the PICO elements, “PROGRESS-PLUS” factors (place of residence, race/ethnicity/identity/culture/language, occupation, gender/sex, religion, education, socioeconomic status, and social capital) including age and disabilities for the equity lens, year of publication, authors, study location, study design, type of data, sample sizes, aims of study and important results extracted from selected articles (35). We also identified whether a patient-oriented research strategy was integrated or not. The extraction of all information was conducted by one reviewer (VB) and double-checked by one of two reviewers (JP and SL).
A visual flow diagram (PRISMA) outlined the decision-making in the study selection process (33). Frequency measures such as numbers and their percentages numerical summary for the overall study characteristics and a narrative synthesis was conducted, centered on every variable aimed to answer our research sub-questions on Indigenous peoples in Canada. We have also aggregated the results in tables to identify the elements associated with equity, the integration of patient-oriented research, and the key findings from included studies. Risk of bias assessment is not mandatory in a scoping review, as many different study designs are included. However, two reviewers (VB and ST) conducted an appraisal based mixed methods appraisal tool (MMAT) and chose at posteriori according to the studies included (43).
Even though consultation of knowledge users (e.g., clinicians, citizens, patients and caregivers, decision makers, other researchers) is optional, it enhances the methodological rigor and the validity of the review. Thus, to gain appreciation of the review’s findings, the lead reviewer (VB) approached diabetic foot disease and Indigenous stakeholders in Canada to provide voluntary insights about our review.
A total of 5, 323 records were identified from bibliographic databases and 18 from additional searches. All duplicates were removed with Endnote and 2, 526 titles were screened. We retained 40 studies that reported data on diabetic foot disease for Indigenous peoples in Canada, as represented in the flow diagram (Figure 1) (44–81). Some included studies have described similar dataset/population [(75, 79) (80, 81) (48, 64) (44, 82); and (49, 78)] and therefore, they were merged and reported together for a same study design/similar outcomes or separately for significant differences (13, 52) and (50, 60) (Table 1).
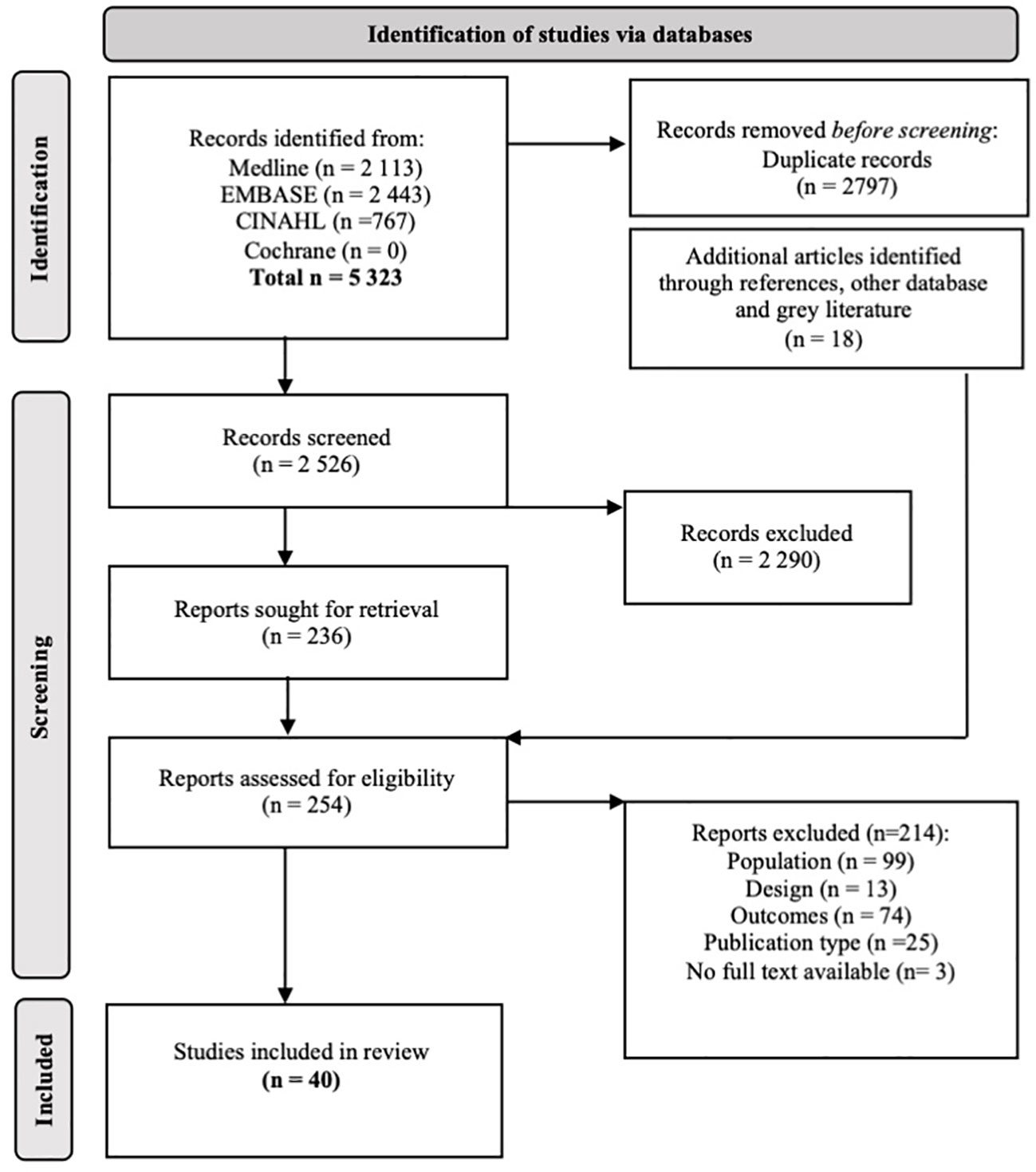
Figure 1 Study selection flowchart. Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Open Access.
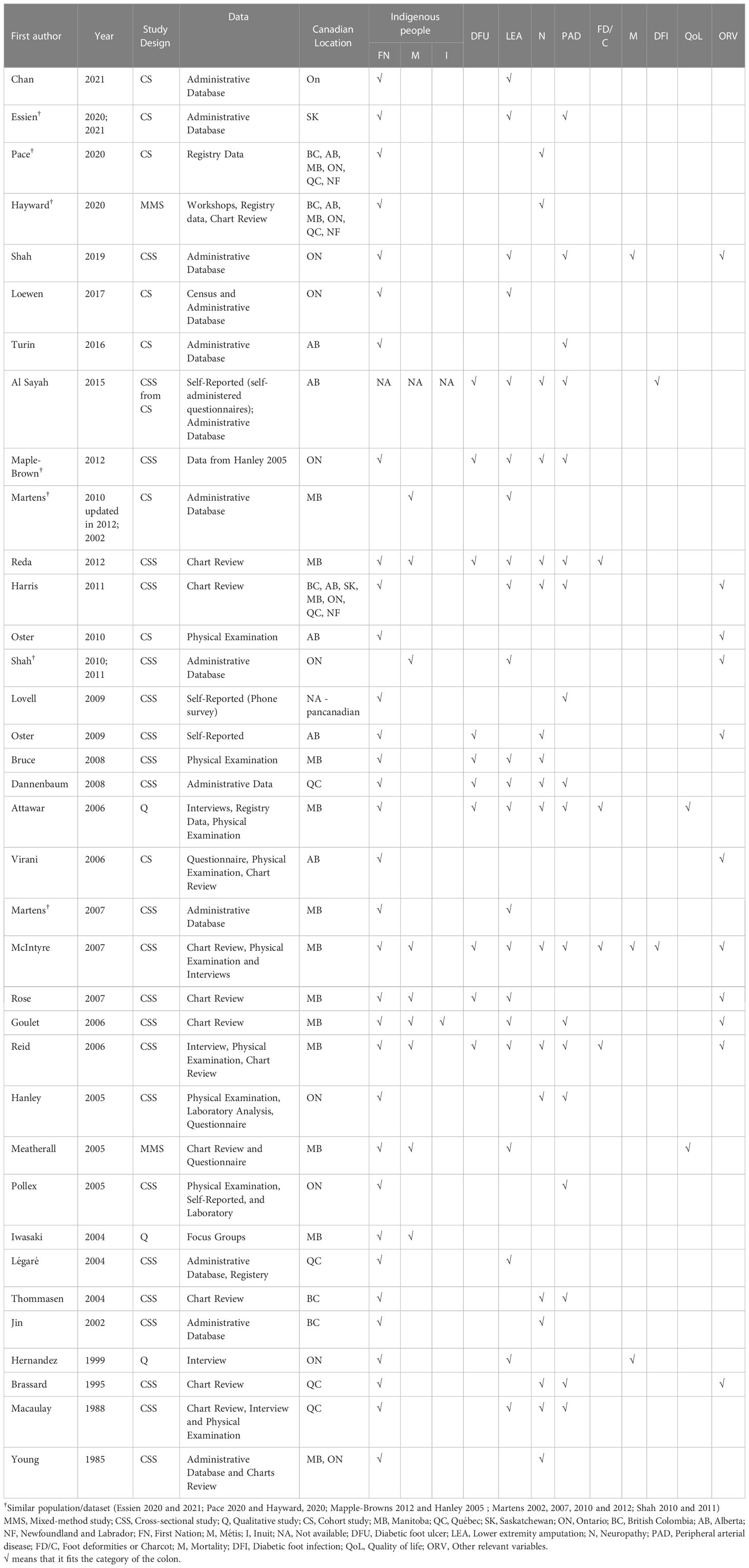
Table 1 Overview of included studies (n= 40).
General characteristics of the included studies and population are presented in the Table 1. The studies were published between 1985 and 2021. Most (51%) were published between 2000 and 2010 (52–70, 76, 82) and between 2010 and 2021 (39%) (44–51, 75, 77–79). Five percent were published between 1985 and 1990 (73, 74) and another five percent between 1991 and 2000 (71, 72). The majority of the studies were quantitative (86%), with the majority (61%) using a descriptive cross-sectional design (44, 47, 48, 50, 51, 53–57, 59–64, 66, 68–70, 72–74, 76) and the remainder (22%) using an observational cohort design (45, 46, 49, 52, 75–77, 80). There were also three qualitative studies (8%) (58, 67, 71) and two mixed-method studies (6%) (65, 81). Various types of data were reported such as administrative data (44, 46, 49, 53, 57, 59, 68, 70, 74, 75, 77, 79) and registry (58, 80, 81), self-reported data (47, 54, 55, 66), retrospective chart review data (50, 51, 61–63, 65, 69, 72–74), prospective data (e.g., physical examination, interviews, focus, questionnaires, etc.) (52, 56, 58, 60, 63–67, 71, 73, 76, 81) and data from a previous prospective study (48). The majority of studies were conducted in Indigenous population in Manitoba, followed by those living in Ontario. One study was pan-Canadian and the provinces and territories were not specified (54). No study included the Yukon, Nunavut and the Northwest Territories population. The Atlantic region was poorly represented with only three studies (but two with the same dataset) that included Newfoundland and Labrador in the overall study (51, 80, 81). The situation was similar for Saskatchewan (51, 75, 79).
Of the 40 studies included, the most published data were focused on First Nations (92%). Only one study (3%) did not distinguish specifically the identity of its population (i.e., First Nations, Métis, or Inuit) (47). Inuit were less represented, being included in only in one study (3%) (62). Métis were represented in a quarter of the studies (26%) (49, 50, 53, 60–63, 65, 67). All studies included at least 332,233 individuals from Indigenous peoples in Canada. The residential area of the community was mentioned for only 53% (19/36) of included studies from which eight studies clearly mentioned the population living on communities (i.e., on reserve) (52, 55, 56, 59, 64, 68, 77, 80, 81). Ten studies did not report demographic data about population with diabetes and/or Indigenous peoples only (47, 49, 50, 54, 62, 63, 66, 69, 70, 79). All details about the population are presented in Supplemental Material 2.
Nine studies did not present clear outcomes: microvascular disease including neuropathy, retinopathy and nephropathy (80, 81), surgery for leg circulation, including LEA (77), other atherosclerosis (including gangrene and other peripheral vascular disease) and neuropathy and amyotrophy (70), PAD (including ischemic feet, LEA and claudication) (73), microvascular disease including ischemic heart disease, cerebrovascular disease and peripheral vascular disease (72), ulcers or sores on their feet and legs (55), foot or leg ulcers or infection/gangrene or LEA (47) and precise type of amputation (i.e., lower, upper, traumatic, etc.) not mentioned (51). Therefore, their data are detailed in the Supplemental Material 2. and sparsely integrated. Studies that reported results for Indigenous peoples with comparators are presented in Table 2. The main results are also summarized in the following subsections.
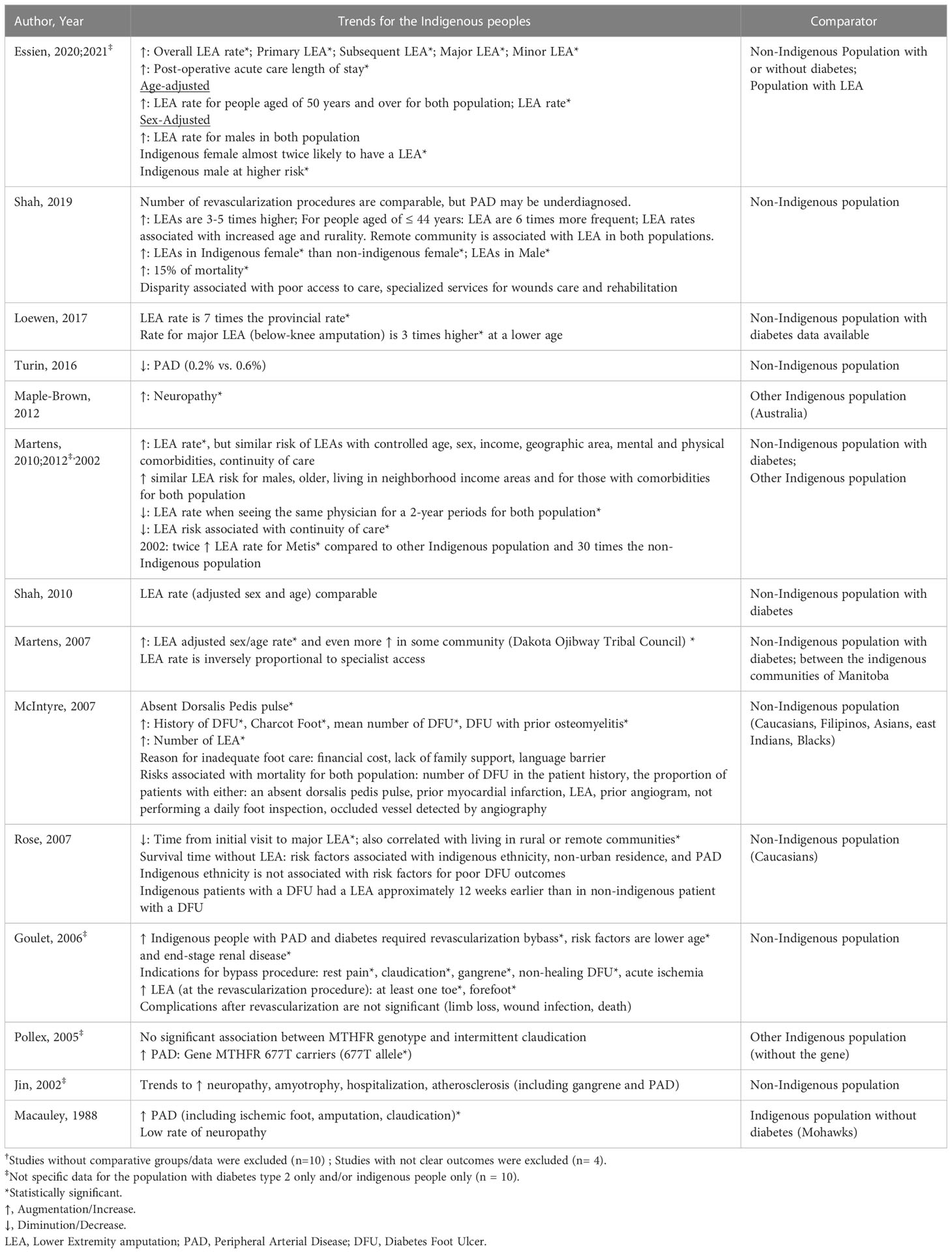
Table 2 Major findings concerning diabetic foot outcomes for Indigenous peoples†.
Ten studies provided data on DFUs (Table 1) (47, 48, 50, 55–58, 60, 61, 63). The prevalence of DFU ranged from 1% to 39% (47, 48, 50, 55, 57, 58, 60), and the prevalence of a history of DFU from 32% to 75% (58, 60). Only one person had a history of DFU in a population of 483 First Nations people (56). Six to fifteen percent of individuals had a history of DFU or had active DFU (13, 63).
Twenty-four studies provided data about LEAs, and thus it is the most studied outcome (44, 46–51, 53, 56–63, 65, 68, 71, 73, 75, 77–79). The incidence of LEA varied among communities and was estimated to range between 1.19 à 6.16 per 1,000 persons, and rates of LEA were inversely related to the access to specialists (59). The prevalence was estimated between 0 and 36% in this population (48, 49, 51, 57, 60). Studies have estimated that the prevalence of LEA was 7 to 49 times higher than the Indigenous population with diabetes than in the non-Indigenous population without diabetes (46, 49, 58, 78). A study identified that LEA’s frequency was 3 to 5 times higher to the non-Indigenous comparative across sex, age and location (44). Among people with diabetes, Ethnicity, or colonization, as experienced by people identifying as Indigenous would lead to a 1.7-fold increase in the risk of having LEA (75). Specifically, in the Métis population, the sex- and age-standardized LEA rate was equivalent to that of the entire population with diabetes (82). Their risk of LEA was similar compared to other Manitobans after controlling sex, age, income, geographic area, mental and physical comorbidities and continuity of care (49). However, a higher risk of LEA was identified in Métis male vs. female (59).
The risk factors for LEAs, similarly to non-Indigenous peoples, were male sex, living in low-income area, living with comorbidities, and being older. A protective factor was to see the same physician for at least one half of their visit over the two-year period (49, 75). Among those aged 44 years or younger, the frequency of LEA was six times higher and living in a remote community was a high-risk factor for LEA (44). The first major LEA on Indigenous peoples occurred at a younger age (65), Indigenous peoples had a shorter average time from initial clinic visits to major LEA compared to non-Indigenous population which also correlated with living on rural or on reserve (61). When controlling the effect of the place of residence (i.e., rurality and on reserve), Indigenous identity was not associated with poorer outcomes such as LEA and death, but early LEA was associated with non-urban residence, identity and arterial insufficiency (61). Indigenous patients with DFU are at-risk of LEA approximately 12 weeks earlier than non-Indigenous patients (61). A study has reported that on average, Indigenous peoples had less phantom limb pain (65). A study related to diabetes has observed seven hospitalizations, totalizing 81 days of hospitalization over a 5-year period related to five cases of amputations (68). Finally, LEA trends (i.e., overall LEA rate, primary LEA, subsequent LEA) increased over a 13-year period by about 5% over this period compared to the trend in the non-Indigenous population which was more stable or declining (75).
Eighteen studies provided data about neuropathy (13, 47, 48, 50, 51, 56, 58, 63, 64, 69, 70, 72–74, 80, 81). The prevalence of neuropathy ranged from 5% to 94% (47, 56, 58, 60, 63, 64, 72–74). Prevalence of neuropathy was reported higher in Indigenous peoples in Canada compared to the one from Australia (48). Among Indigenous peoples, the likelihood of developing neuropathy was 2.7 times higher for women than for men and 3 times higher for those who had completed less education than for those who had completed grade 9 or higher. The risk of neuropathy was twice as high for a person with a glycated hemoglobin level of 9% compared to 6%, and 3 times higher for heavy smokers (56).
Eighteen studies provided data about PAD (44, 45, 47, 48, 50, 51, 54, 57, 58, 60, 62–64, 66, 69, 72, 73, 75). PAD prevalence was estimated between 0.2% to 23.0% (47, 48, 51, 57, 64, 69, 75). A genetic mutation that may be present particularly in Indigenous peoples is significantly associated with an increased risk of PAD (66). It was found that 92% of Indigenous peoples with diabetes and PAD required more bypass revascularization compared with 42% in the non-Indigenous population (62). Indigenous peoples also had a greater burden of PAD symptoms (i.e., claudication, rest pain, gangrene and acute ischemia) than the non-Indigenous (62).
Four studies provided data related to foot deformities and Charcot neuroarthropathy (50, 58, 60, 63). Foot deformities were estimated to be between 16% and 51% in Indigenous peoples and included hallux valgus, claw toes, hallux rigidus, flat feet, cavus feet, long second toe, ankle deformity, heel pad atrophy, dorsal exostosis (58, 63). There was more Charcot neuroarthropathy in the Indigenous group with end-stage renal disease than in a similar non-Indigenous group (60). In a study, Charcot neuroarthropathy was a very rare condition estimated at less than 1% of the population (63).
Three studies provided data related to mortality and DRFC (44, 60, 71). Mortality (age- and sex- adjusted) after LEAs was 15% higher in Indigenous peoples than in non-Indigenous peoples, with a median survival of 3.5 years compared to 4.1 (44). First Nations people with diabetes were very concerned about the loss of freedom, mortality and LEA (71). Risk factors for mortality were the same for the Indigenous and comparative populations i.e. mean number of prior DFU, the proportion of patients with either an absent dorsalis pedis pulse, prior myocardial infarction, LEA, prior angiogram, not performing a daily foot inspection, occluded vessels detected by angiography (60).
Two studies provided data related diabetic foot infections (47, 60). In patients with diabetes and end-stage renal disease, DFUs had significantly greater prior osteomyelitis amongst Indigenous peoples compared to their non-Indigenous counterparts (60).
Three studies provided data related to diabetic foot disease and quality of life (58, 65, 67). Indigenous peoples reported having suffered from LEA for the rest of their life and living in fear of the future (for themselves and their families). They realized that they have to live with these DRFC on a daily basis and were stressed about living another 20 years because they realized that it may get worse (67). There was no difference between Indigenous and non-Indigenous peoples in their feelings of distress related to DRFC. They expressed feelings of regret, self-blame, and guilt about their general health, diabetes, and LEA (65). Many Indigenous peoples reported chronic and persistent foot pain, which affected their quality of life. LEA has changed their lives as it restricted their ability to participate meaningfully in their community (58).
There were 11 studies that provided insights about other relevant data detailed in Supplemental Material 2. Over a 7-year period, for 169 people with 498 DRFC, this resulted in 18% emergency room visits, 16% hospitalizations, 11% elective transfers and 6% emergency transfers (63). Progression of poor clinical outcomes in this population is associated with referral with a lesion, age greater than 60 years, prior LEA or vascularization, PAD, more than one lesion at presentation, longer duration of diabetes, higher grade of DFU on the Wagner classification (61). The reasons for inadequate foot care are associated with financial cost, lack of family support, and language barriers (60). Despite interventions to achieve the recommended practice guidelines and recommendations, there is still limited foot screening in this population (76, 81). Foot abnormalities are more common in Indigenous men (52), and unspecified diabetic foot disease was estimated to 35% of the population from 19 different Indigenous communities (51). The revascularization rate (age and sex adjusted) is equivalent to the non-Indigenous and Indigenous populations with diabetes (82), and the Indigenous population presented worsen symptoms before revascularization (62). Health disparity related to DRFC in Indigenous population may be driven in part by poor access to health care, particularly specialized services for wound care and rehabilitation and especially because of their residency in remote communities (82). Indigenous identity is associated with prolonged postoperative acute care length of stay after a LEA (79).
We have listed the different factors of the PROGRESS-Plus framework in Table 3 for the included studies. The most frequently included factors in ascending order were place of residence, sex, race and age. One study included all factors (58). Education, income, and social per capita were minimally included in the included studies. There was little data on the occupation of the Indigenous population. Religion and spirituality were not discussed in any study. Patient-oriented research has been clearly mentioned in six studies representing 17% of included studies (49, 51, 58, 75, 77–79, 81), and it was particularly favored in the last decade. Details about the integration of patient-oriented research are also displayed in Table 3. None of those studies has used the GRIPP-2 tool to reported patient and public involvement in research (83).
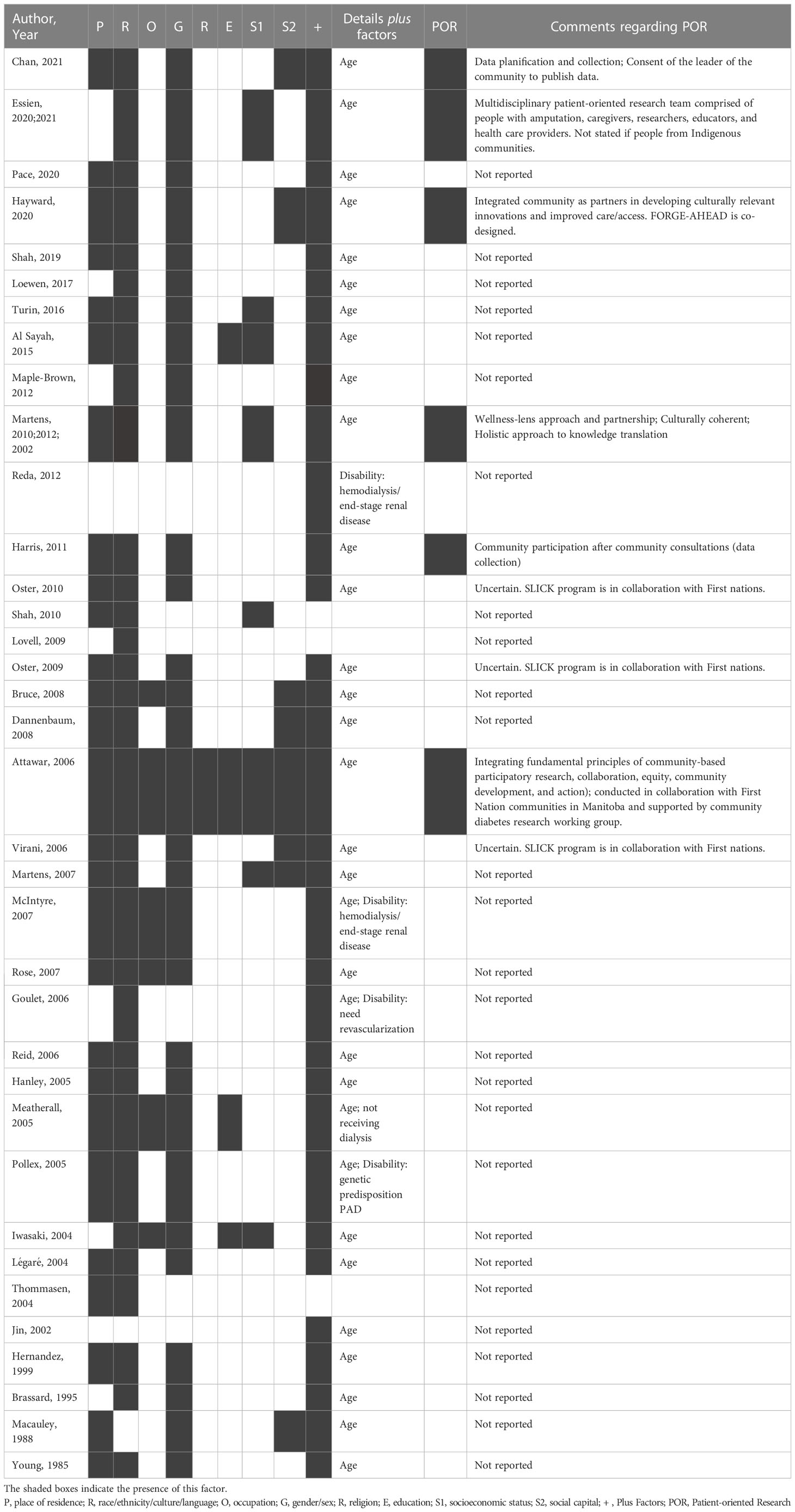
Table 3 PROGRESS-Plus Factors and Patient-Oriented Research Data in the Included Studies.
We conducted a critical quality appraisal of the included studies, and the results are presented in Figure 2. All three qualitative studies were of good quality. One of the mixed-method studies was good (81). The quality of the non-randomized qualitative and descriptive studies was variable but mostly of average quality. It was highlighted by the consultation that there is substantial bias in that the bulk, if not all, studies included were led by non-Indigenous people using non-Indigenous methodology.
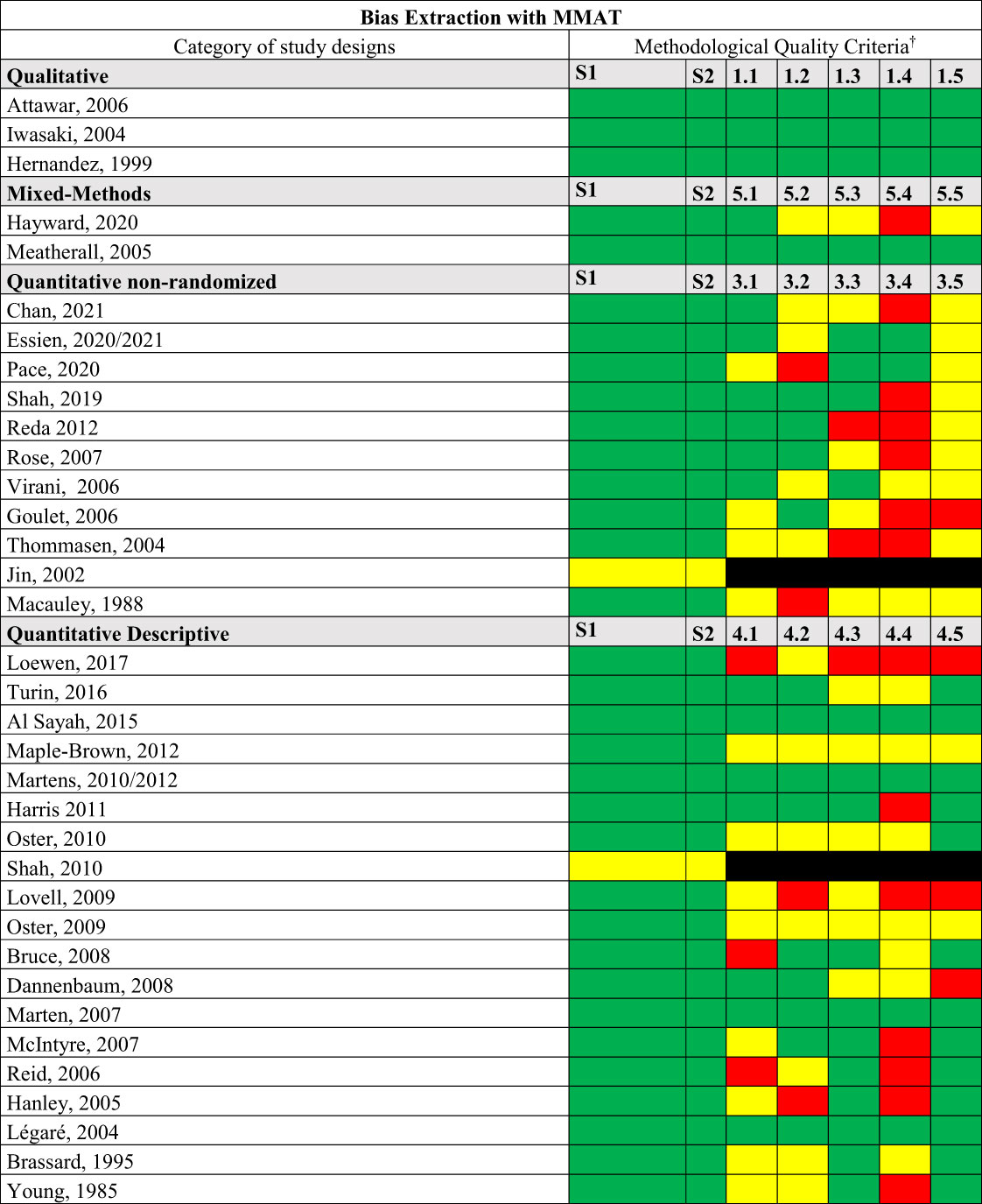
Figure 2 Quality Appraisal of included studies. MMAT, Mixed Methods Appraisal Tool. †Are criteria are available in MMAT (84).
Six stakeholders from the Indigenous peoples and/or working very closely with them were consulted about this review: a citizen, a patient with DRFC, a caregiver, a clinician, a decision-maker and a researcher. These people chosen from our networks are from different communities and representing three different provinces. Their feedback was incorporated into this review.
Our objective was to map the existing literature published in database related to diabetic foot disease among Indigenous peoples in Canada based on a systematic methodology and incorporating an equity lens. Thus, Indigenous peoples experience a heavy burden of diabetic foot disease compared to the non-Indigenous population. LEA, the most reported complications, are higher in Indigenous peoples. Very little is reported on patient-reported experience and outcomes related to DRFC. Besides, studies mainly report on First Nations and Métis data, with very little representation for Inuit people. Data on Inuit living with diabetes in Northern communities in Canada is limited, as they represent the least populated group in the Indigenous population (3). Their voices are still less represented in diabetes research which is coherent with our results (85). We examined our results from three perspectives: trends in DRFC, the equity lens, and POR.
The trends identified in this study confirm a high level of DRFC in this population, but it may be only the tips of the iceberg. DRFCs affect more Indigenous men than Indigenous women and both sexes are at higher risk for LEA at a younger age than non-Indigenous people. In addition, there is a significant effect of the place of residence where rural and remote communities are associated with increased numbers of LEA. These trends are consistent with those demonstrated previously (10, 86, 87). Indigenous identity is associated with LEA in Indigenous peoples of Australia (88). Recent studies in the United States on race and rurality have identified their association resulting in more LEA events, both major and minor (24, 89). Indeed, deficiencies of specialized care and the effect of rurality on LEA was also demonstrated similarly as highlighted in our review (24). LEAs are amplified by race, particularly in ethnic minorities groups of a population (24). In general, LEAs are also more prevalent among men (90), and this trend was also identified amongst the Indigenous population in Canada. Similarly, the same trend was identified with respect to age, with the mean age of first LEA being younger among Indigenous peoples, approximately 14 years younger than in the non-Indigenous population, and LEA being more common among those under 50 years of age (10, 86). PAD appears to be underdiagnosed in Indigenous peoples, whereas revascularization procedures may be overdone compared with non-Indigenous peoples. Those trends have also been identified among marginalized groups (87, 91). There is very little Canadian data on diabetic foot infection which has been documented to be very prevalent in the Indigenous peoples of Australia (86). Indigenous identity has been associated with an increased risk of neuropathy and DFU, with a 3- to 6-fold increase in the likelihood of experiencing LEA, but our data do not permit such a precise estimate in comparison (86).
Our results support that, although this research topic is receiving more recent attention in Canada, knowledge remains limited. In fact, most of the DFRC identified seem to be underestimated including neuropathy, PAD, diabetic foot infection, when compared to those of the Indigenous population in Australia (86). Moreover, we did not identify any study reporting on mental health (e.g., depression, anxiety) and DRFC. Yet the association with DFU and LEA is well demonstrated (92, 93). This result is consistent with the fact that these data are often missing for this population related to mental health studies (94). Nevertheless, this is a difficult topic for this population given the intergenerational effects of colonization, residential schools and other trauma (95), in addition to competing health priorities.
The overall results are consistent with those of a previous study conducted 10 years ago, which identified increased biomedical risk factors for all Indigenous populations with diabetes related to LEA, neuropathy and PAD, and highlighted that complex political and social factors are also barriers to optimal health care for Indigenous peoples (10). Therefore, Indigenous identity alone does not explain all the outcomes, it is mainly the synergy of socio-historical-political conditions (and colonization) faced by Indigenous peoples that predispose them to diabetes and its complications in Canada (8). Hence the importance of considering factors related to the inequity.
This review suggests that the magnitude of the problems associated with diabetic foot disease and its complications in this population is identified but underestimated, particularly with respect to equity as their influence on DRFC remains unclear. That this review did not identify the real inequity experienced by Indigenous people regarding DRFC only highlights how problematic western methodologies are. Only minimal robust data was available, and few studies have incorporated PROGRESS-Plus factor perspective. When equity factors are less accounted for in research, this inevitably impacts the results. Yet the effect of equity factors is well known in the Indigenous population with diabetes (12). Strategies were suggested to address social barriers and to improve outcomes, equity and cultural safety approach in Indigenous population in Canada (96). However, it takes time to set up at all levels i.e., individual, organizational, system and in research.
Social determinants of health, identified with PROGRESS-Plus factors may not be enough and appropriate. This must be grounded in decolonization and increasingly centering on Indigenous ways of knowing, being and doing and Indigenous health determinants (97). While our project has shown that even Western factors have been given little consideration, it is essential to also include determinants of wellness that are much more aligned with the beliefs, values and preferences of Indigenous peoples, including elements such as self-determination, identity, language and land (98). Mental, physical, spiritual and social are holistic dimensions of health for this population and specific Indigenous frameworks may better support the equity lens (99). Foot health in Indigenous peoples should be no different from the non-Indigenous population and based on prevention and management that is proven to be effective (100). However, evidence-based, trauma-informed, and culturally safe care should be inseparable in order to decrease health disparities for this population. Poor outcomes included in this review may be consistent with the limitations of the Canadian health services/system, especially when actions are not relevant to the social and cultural contexts of Indigenous peoples (12). A focus on building relationships with an Indigenous person with diabetes is important rather than a singular emphasis on achieving management targets. This also needs to be considered in research. Previous studies have shown that there is little good quality evidence to assess diabetes health outcomes in primary care or system services for Indigenous peoples in Canada with type 2 diabetes (101). In addition, the limited success in achieving evidence-based targets (e.g., glycated hemoglobin, lipid levels, physical activity levels) in this population has highlighted the limitations of health services, as the targets are not necessarily relevant to Indigenous peoples and are not aligned with the equity factor (102, 103). The access to culturally safe health care, delivered by culturally competent (allied) health professionals were seen as a contributing factor to foot and lower extremity health (102). This is also aligned with a call to action as per the Truth and Reconciliation Committee of 2015, commissioned by the Government of Canada (104).
Our results highlighted the hypothesis of disparities regarding prevention, treatments, and quality of care, particularly in rural and remote communities, and may be the direct effect of colonization. Disparities have been well demonstrated for the management of diabetes and its complications in rurality (105). Deficiencies of specialized care and the effect of rurality on LEA was demonstrated on race and ethnicity in a previous study (24). Socio-economic conditions and risk factors for type 2 diabetes and its complication are important determinants of health and therefore culturally safe and appropriate policies, programs and services that address health equity have a preponderant role to play in preventing diabetes complications at different (from individuals to structural) levels of change (106, 107).. Appropriate screening and intervention programs and improved access to effective health care services are required to prevent a widening of the gap in DRFC between Indigenous and non-Indigenous in Canada (86), while advocating for systemic changes to address health inequities. Indigenous peoples living in Canada are among the highest-risk populations for DRFC and screening should be carried out earlier and at more frequent intervals (12). Currently, this is not the case (108), but some studies included in the review aimed to reach a better standard of care for foot health and reduce disparities (13, 50, 76, 80, 81). Thus, establishing more healthcare services that integrate Indigenous Peoples cultures and traditions could improve access to care and the course of treatment (109). Finally, engagement is a paramount component of care for DRFC. A recent study on engagement did not identify specific data on this population (110), but it is worth bearing in mind that Indigenous populations are not less “engaged” than non-Indigenous populations (111). This is also a Western perspective on their engagement. Some populations are not difficult to reach - to mobilize - but they may find it hard to trust clinicians, researchers and policymakers (27, 112). Effects of colonialism (e.g., traumatic historical relationship with the government, health care professional too prescriptive or authoritarian, racism, discrimination, stereotypes, and structural barriers to cares) may be at the root of the heavy burden of DRFC. However, our study did not set out to precisely explore this population’s engagement, and this is an important avenue to explore in diabetic foot care.
It is not surprising that POR was not particularly integrated before 2020 for research with this population because we are more likely to employ Indigenous health research methodologies. In fact, actions that develop cultural safety, integrate all care spectrum and stakeholders, respect the values, customs, and traditions of Indigenous Peoples, and joint data collection to monitor progress and outcomes are a necessity in research to achieve health equity (101). There are specific methods for Indigenous population-centered research such as the use of Indigenous frameworks, western methods adapted to Indigenous context, community-based participatory research, storytelling and culture-specific methods (113). We have very little information about this in the literature reviewed, apart from community-based participatory research in recent years and the request for community permission in connection with ethical approval. Furthermore, based on our findings, it is also clear that this population needs to be more fully considered in research and health initiatives to promote culturally safe and quality health care. The predominantly western biomedical approach to health care in Canada has been identified as culturally insensitive and not inclusive of Indigenous perspectives and well-being (114). Currently, there is a lot of work being done in hospitals, but it’s a long-term effort. Patient interactions and engagement in diabetes care have been influenced by personal and collective historical experiences with health care providers and contemporary exposures to culturally inappropriate and potentially harmful healthcare (27). Moreover, social determinants of wellness are drivers of health equity and community research capacity (115).
Data regarding Indigenous people’s perspectives on foot health were scarce, yet critical. Thus, in order to develop culturally safe health care and promote positive change in foot health among First Nations people, it is imperative that stakeholders such as clinicians and researchers including Indigenous peoples perspectives (102). There is also a need to engage empowered Indigenous peoples in the foot health initiative. A recent call to action was issued to integrate traditional Indigenous and Western health models to improve outcomes as well as radical changes to reduce inequities and support the transformation of primary health care programs to empower Indigenous peoples and communities and improve chronic disease prevention and management (7, 116). As far as First Nations are concerned, they have the control and aim to achieve data sovereignty for data collection processes, and they want to own and control how that information can be used using the principles of ownership, control, access and possession, better known as OCAP® (117). Therefore, Indigenous peoples are empowered to act independently and address their own health issue with research including DRFC (118, 119). POR is aligned with this and the non-Indigenous and Indigenous research community can team up for the health of all Canadians. Taking over control of health, well-being and clinical care by Indigenous peoples is a desirable way forward such as in the NUKA health project (120, 121).
There are strengths and limitations to our scoping review. First, to our knowledge, this is the first comprehensive review of DRFC using a systematic method specifically targeting this Canadian population and including an equity lens and POR data. However, the high heterogeneity of the included studies makes it very difficult to obtain comprehensive results representing the situation. For this reason, we opted for a narrative synthesis and focused on studies including comparison/control to express broad trends. The chosen methodology is also Western and focuses on research done by predominantly non-Indigenous researchers, published in the Western evidence base and therefore Indigenous ways of knowing, being and acting based on their teachings and medicines are lacking. In addition, the overall quality of the evidence reported is dependent on the quality level of evidence of included studies. The use of the MMAT quality assessment tool (43) is a strength of our work as this is not mandatory with this research design but highlights the average quality of observational studies. Therefore, this is an area that needs improvement.
Second, although our database search strategy was robust and validated by an academic librarian, we may have missed data from the grey literature and specific communities. However, grey literature is rarely peer-reviewed and difficult to identify, but our attempt is a plus value to portray the overall situation. Otherwise, we minimized bias by testing our selection strategy with a two-arm independent reviewer pilot, and agreements were strong (Cohen’s kappa > 80%) (122). Due to a selection performed by two groups of reviewers, this may lead to differences in selection and extraction. We attempted to reduce this disparity by involving the lead reviewer in both arms.
Third, this review followed the recorded protocol, but was modified to improve the robustness of the methodology based on the progress of the study and evidence. This study was initiated in November 2020. The adjustment concerned the research questions on equity and POR, and the choice of the scoping design, being less restrictive, allowed this malleability. We wanted to provide a concrete analysis of the evidence regarding equity and POR to also contribute to the improvement of research in this area. Finally, although the initial research question emanated from a clinical setting dealing with Indigenous peoples and wanted to identify the overall burden of the diabetic foot disease, no patient or citizen were included in the research process as co-investigators. On the other hand, consultation with stakeholders was our way of involving them and was undoubtedly a great addition as we have conducted inclusive research, used culturally acceptable language, and discussed the results in concert with what is important for them.
With these strengths and limitations in mind, we emphasized the urgent need for robust research in Canada with Indigenous peoples, particularly integrating all factors related to equity and to consider specific socio-historical-political conditions and risk factors to worse outcomes identified in this review such as rurality/remote locations, age, sex, health care accessibility (123, 124). We highlight the catastrophic effects of limb loss on this growing population, without even considering what happens to young people (≤18 years old), but knowing that the youth is increasingly affected by diabetes (125). Indigenous peoples have different identities, cultures, and contexts in the society, but data on their specific characteristics are scarce in terms of their diversity and DRFCs. There are reportedly over 630 different First Nations communities in Canada, representing more than 50 Nations and speaking more than 50 Indigenous languages, in addition to Inuit and Métis (3). We have presented our results as one group, but each subgroup (i.e., First Nations, Métis and Inuit) need to be considered independently as they have a unique situation. Precise population definition can support a better portrayal of the situation, on the one hand, and the development of adapted interventions on the other. It is well known that user-based interventions in patient-centered research are developed and implemented more easily (126). We also strongly suggest that future studies apply national and international validated standards, recommendations and definitions for DRFC research on this population (39, 127). In addition, outcomes research needs to be more inclusive with nationally representative populations by including Indigenous peoples to better inform the national burden of this disease in Canada.
Finally, it appears from all the literature reviewed that less attention has been paid to diabetic foot disease from a preventive perspective and the major focus was related to LEAs. Although these results support previous findings (10, 86), more data are needed to better understand the burden of DFU, PAD, neuropathy, and foot deformities in Indigenous in Canada, particularly in those with additional vulnerability factors such as end-stage renal disease and/or frailty (128, 129). Researchers need to embrace Indigenous methods and co-research with two eyed seeing. The Inuit peoples of the provinces and territories, who are still poorly integrated in the knowledge of the burden of diabetic foot disease, deserves special attention in further research. While efforts have been made in recent years to identify and manage DFRCs, particularly in collaboration with the community, it is imperative that Indigenous communities and peoples be considered as partners in the promotion of quality and culturally safe health and social services for limb preservation within the research. Knowledge development with this population should move in this direction regardless of the type of study and resources and ensure adequate transfer.
Indigenous peoples in Canada experience a high burden of foot disease and DRFC, however since the data and high-quality studies are limited and heterogeneous, the extent of the situation may be underestimated. Even if Indigenous identity shows trends for worst health outcomes related to DRFC, it is also the synergy of socio-historical-political conditions (and colonialism) faced by Indigenous peoples that predispose them to diabetes and its complications. We have done a comprehensive review that specifically included an equity lens and POR, but this review highlights the problem of our western method. This knowledge is only the tip of the iceberg in terms of truly supporting this population through concrete and concerted action with, not for, Indigenous peoples. Social services and health care must be improved using Indigenous ways of knowing, being and acting to reach equity, especially for those living in rural and remote communities in Canada. Potential solutions lie with them. Although these results corroborate previous findings for other populations, additional data are needed to better understand the impacts of DRFC considering culture, beliefs, traditional medicine, and lifestyle of Indigenous peoples. The Indigenous peoples should be given further consideration in research and initiatives aimed at promoting culturally safe and quality health care and access. It is crucial to recognize the specific needs and prioritize prevention strategies to reduce the burden of diabetic foot disease among this at-risk population.
The project was conceptualized by VB, JP, and A-ML. Data acquisition, including selection, review, and extraction was performed by VB, ST, JP, MB-F, and SL. VB performed most of the analysis with JP and ST. VB conducted the consultation. VB drafted the manuscript and was mentored and advised by DA and M-CT. All authors contributed equally to the revision of the manuscript and its final approval. All authors take full responsibility for its content.
The study has no funding source. However, VB has received a leadership grant from Wounds Canada for this project and was also supported by Diabetes Action Canada and its networks during her postdoctoral fellowship. DA is partially supported by the National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases Award Number 1R01124789-01A1.
The authors would like to thank the UQTR’s librarian for the validation of the search strategy. The authors warmly thank the precious collaboration of stakeholders solicited in the consultation phase that have provided relevant input: a patient and two researchers who prefers to remain, Corinne Paul, Jeremy Caul, Isabel Desgagné-Penix and Nora Abibsi.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1177020/full#supplementary-material
2. LeBlanc AG, Gao YJ, McRae L, Pelletier C. At-a-glance-Twenty years of diabetes surveillance using the Canadian Chronic Disease Surveillance System. Health Promot chronic Dis Prev Canada: Res Policy practice. (2019) 39(11):306. doi: 10.24095/hpcdp.39.11.03
3. Statistic Canada. First nations people, Métis and Inuit in Canada: Diverse and growing populations. Ottawa, Ontario, Canada (2018).
5. Statistic Canada. La population autochtone continue de croître et est beaucoup plus jeune que la population non autochtone, malgré un ralentissement de son rythme de croissance Gouvernement du Canada. Ottawa, Ontario, Canada (2022).
6. Pelletier C, Dai S, Roberts K, Bienek A. Report summary Diabetes in Canada: facts and figures from a public health perspective. Chronic Dis injuries Canada (2012) 33(1):53–4. doi: 10.24095/hpcdp.33.1.07
7. Harris SB, Tompkins JW, TeHiwi B. Call to action: a new path for improving diabetes care for indigenous peoples, a global review. Diabetes Res Clin practice. (2017) 123:120–33. doi: 10.1016/j.diabres.2016.11.022
8. Dyck R, Osgood N, Lin TH, Gao A, Stang MR. Epidemiology of diabetes mellitus among First Nations and non-First Nations adults. Cmaj (2010) 182(3):249–56. doi: 10.1503/cmaj.090846
9. Adelson N. The embodiment of inequity: Health disparities in Aboriginal Canada. Can J Public Health (2005) 96(2):S45–61. doi: 10.1007/BF03403702
10. Schoen DE, Norman PE. Diabetic foot disease in Indigenous people. Diabetes Manag (2014) 4(6):489. doi: 10.2217/dmt.14.43
11. Halseth R, Greenwood M. Indigenous early childhood development in Canada: Current state of knowledge and future directions: National Collaborating Centre for Aboriginal Health Prince George. (2019), 1–68.
12. Crowshoe L, Dannenbaum D, Green M, Henderson R, Hayward MN, Toth E. Type 2 diabetes and Indigenous peoples. Can J diabetes. (2018) 42:S296–306. doi: 10.1016/j.jcjd.2017.10.022
13. Oster RT, Toth EL. Differences in the prevalence of diabetes risk-factors among First Nation, Metis and non-Aboriginal adults attending screening clinics in rural Alberta, Canada. Rural Remote Health (2009) 9(2):1. doi: 10.22605/RRH1170
14. Campbell DJT, Lacny SL, Weaver RG, Manns BJ, Tonelli M, Barnabe C, et al. Age modification of diabetes-related hospitalization among First Nations adults in Alberta, Canada. Diabetol Metab Syndrome (2014) 6(1):1–5. doi: 10.1186/1758-5996-6-108
15. Isa D, Pace D. Is ethnicity an appropriate measure of health care marginalization? A systematic review and meta-analysis of the outcomes of diabetic foot ulceration in Aboriginal populations. Can J Surg J canadien chirurgie. (2021) 64(5):E476–E83. doi: 10.1503/cjs.004619
16. Armstrong DG, Boulton AJ, Bus SA. Diabetic foot ulcers and their recurrence. New Engl J Med (2017) 376(24):2367–75. doi: 10.1056/NEJMra1615439
17. Rathnayake A, Saboo A, Malabu UH, Falhammar H. Lower extremity amputations and long-term outcomes in diabetic foot ulcers: A systematic review. World J Diabetes. (2020) 11(9):391. doi: 10.4239/wjd.v11.i9.391
18. Zamani N, Chung J, Evans-Hudnall G, Martin LA, Gilani R, Poythress EL, et al. Engaging patients and caregivers to establish priorities for the management of diabetic foot ulcers. J Vasc Surg (2020) 73(4):138–95.e4. doi: 10.1016/j.jvs.2020.08.127
19. Blanchette V, Brousseau-Foley M, Cloutier L. Effect of contact with podiatry in a team approach context on diabetic foot ulcer and lower extremity amputation: systematic review and meta-analysis. J foot ankle Res (2020) 13(1):1–12. doi: 10.1186/s13047-020-0380-8
20. Tan T-W, Armstrong DG, Concha-Moore KC, Marrero DG, Zhou W, Calhoun E, et al. Association between race/ethnicity and the risk of amputation of lower extremities among medicare beneficiaries with diabetic foot ulcers and diabetic foot infections. BMJ Open Diabetes Res Care (2020) 8(1):e001328. doi: 10.1136/bmjdrc-2020-001328
21. Rice K, Te Hiwi B, Zwarenstein M, Lavallee B, Barre DE, Harris SB. Best practices for the prevention and management of diabetes and obesity-related chronic disease among indigenous peoples in Canada: A review. Can J Diabetes. (2016) 40(3):216–25. doi: 10.1016/j.jcjd.2015.10.007
22. Fayed ST, King A, King M, Macklin C, Demeria J, Rabbitskin N, et al. In the eyes of Indigenous people in Canada: exposing the underlying colonial etiology of hepatitis C and the imperative for trauma-informed care. Can Liver J (2018) 1(3):115–29. doi: 10.3138/canlivj.2018-0009
23. Brennan MB, Powell WR, Kaiksow F, Kramer J, Liu Y, Kind AJ, et al. Association of race, ethnicity, and rurality with major leg amputation or death among medicare beneficiaries hospitalized with diabetic foot ulcers. JAMA network Open (2022) 5(4):e228399–e. doi: 10.1001/jamanetworkopen.2022.8399
24. Minc SD, Goodney PP, Misra R, Thibault D, Smith GS, Marone L. The effect of rurality on the risk of primary amputation is amplified by race. J Vasc surgery. (2020) 72(3):1011–7. doi: 10.1016/j.jvs.2019.10.090
25. Bonneau C, Caron NR, Hussain MA, Kayssi A, Verma S, Al-Omran M. Peripheral artery disease among Indigenous Canadians: What do we know? Can J Surg (2018) 61(5):305. doi: 10.1503/cjs.013917
26. Naqshbandi M, Harris SB, Esler JG, Antwi-Nsiah F. Global complication rates of type 2 diabetes in Indigenous peoples: A comprehensive review. Diabetes Res Clin practice. (2008) 82(1):1–17. doi: 10.1016/j.diabres.2008.07.017
27. Jacklin KM, Henderson RI, Green ME, Walker LM, Calam B, Crowshoe LJ. Health care experiences of Indigenous people living with type 2 diabetes in Canada. Cmaj (2017) 189(3):E106–E12. doi: 10.1503/cmaj.161098
28. Greenwood M, de Leeuw S, Lindsay N. Challenges in health equity for Indigenous peoples in Canada. Lancet (2018) 391(10131):1645–8. doi: 10.1016/S0140-6736(18)30177-6
29. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol (2005) 8(1):19–32. doi: 10.1080/1364557032000119616
30. Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implementat Sci (2010) 5(1):1–9. doi: 10.1186/1748-5908-5-69
31. Colquhoun HL, Levac D, O'Brien KK, Straus S, Tricco AC, Perrier L, et al. Scoping reviews: time for clarity in definition, methods, and reporting. J Clin Epidemiol (2014) 67(12):1291–4. doi: 10.1016/j.jclinepi.2014.03.013
32. Peters MD, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis. (2020) 18(10):2119–26. doi: 10.11124/JBIES-20-00167
33. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Internal Med (2018) 169(7):467–73. doi: 10.7326/M18-0850
34. Eriksen MB, Frandsen TF. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Library Associat: JMLA. (2018) 106(4):420. doi: 10.5195/jmla.2018.345
35. O'Neill J, Tabish H, Welch V, Petticrew M, Pottie K, Clarke M, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol (2014) 67(1):56–64. doi: 10.1016/j.jclinepi.2013.08.005
36. Canadian Institutes of Health Research. Strategy for patient-oriented research—patient engagement framework : Government of Canada. Canada (2014).
37. Kavanaugh J, Oliver S, Lorenc T. Reflections on developing and using PROGRESS-Plus Equity Update. Cochrane Health Equity Field Campbell Equity Methods Group (2008) 2:1–3.
38. Browne AJ, Varcoe C, Lavoie J, Smye V, Wong ST, Krause M, et al. Enhancing health care equity with Indigenous populations: evidence-based strategies from an ethnographic study. BMC Health Serv Res (2016) 16(1):1–17. doi: 10.1186/s12913-016-1707-9
39. van Netten JJ, Bus SA, Apelqvist J, Lipsky BA, Hinchliffe RJ, Game F, et al. Definitions and criteria for diabetic foot disease. Diabetes/metab Res Rev (2020) 36:e3268. doi: 10.1002/dmrr.3268
40. Allan J, Munro W, Figgins E. Foot deformities within the diabetic foot and their influence on biomechanics: a review of the literature. Prosthetics orthotics Int (2016) 40(2):182–92. doi: 10.1177/0309364615592705
41. Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Internal Med (1993) 118(8):622–9. doi: 10.7326/0003-4819-118-8-199304150-00009
42. Sim J, Wright CC. The kappa statistic in reliability studies: use, interpretation, and sample size requirements. Phys Ther (2005) 85(3):257–68. doi: 10.1093/ptj/85.3.257
43. Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed methods appraisal tool (MMAT), version 2018. Registrat copyright. (2018) 1148552:10.
44. Shah BR, Slater M, Frymire E, Jacklin K, Sutherland R, Khan S, et al. Use of the health care system by Ontario First Nations people with diabetes: a population-based study. CMAJ Open (2020) 8(2):E313–E8. doi: 10.9778/cmajo.20200043
45. Turin TC, Saad N, Jun M, Tonelli M, Ma Z, Barnabe CCM, et al. Lifetime risk of diabetes among First Nations and non–First Nations people. CMAJ (2016) 188(16):1147–53. doi: 10.1503/cmaj.150787
46. Loewen K, Jordan Vigliarolo CPAC, Lance B, Rockley M, Yoko Schreiber M, Catherine Kivi R, et al. Rates of diabetes-related lower-limb amputation in northwestern Ontario: an incidence study and introduction of a standardized diabetic foot ulcer management protocol. Can J Rural Med (2017) 22(3):100.
47. Al Sayah F, Soprovich A, Qiu W, Edwards AL, Johnson JA. Diabetic foot disease, self-care and clinical monitoring in adults with type 2 diabetes: the Alberta’s Caring for Diabetes (ABCD) cohort study. Can J diabetes. (2015) 39:S120–S6. doi: 10.1016/j.jcjd.2015.05.006
48. Maple-Brown LJ, Cunningham J, Zinman B, Mamakeesick M, Harris SB, Connelly PW, et al. Cardiovascular disease risk profile and microvascular complications of diabetes: comparison of Indigenous cohorts with diabetes in Australia and Canada. Cardiovasc Diabetol (2012) 11:30. doi: 10.1186/1475-2840-11-30
49. Martens P, Bartlett J, Burland E, Prior H, Burchill C, Huq S, et al. Profile of Metis health status and healthcare utilization in Manitoba: a population-based study. Winnipeg, MB: Manitoba Centre for Health Policy (2010) p. 1–652.
50. Reda A, Hurton S, Embil JM, Smallwood S, Thomson L, Zacharias J, et al. Effect of a preventive foot care program on lower extremity complications in diabetic patients with end-stage renal disease. Foot Ankle Surgery. (2012) 18(4):283–6. doi: 10.1016/j.fas.2012.05.002
51. Harris SB, Naqshbandi M, Bhattacharyya O, Hanley AJ, Esler JG, Zinman B, et al. Major gaps in diabetes clinical care among Canada's First Nations: results of the CIRCLE study. Diabetes Res Clin Practice. (2011) 92(2):272–9. doi: 10.1016/j.diabres.2011.02.006
52. Oster RT, Shade S, Strong D, Toth EL, Oster RT, Shade S, et al. Improvements in indicators of diabetes-related health status among first nations individuals enrolled in a community-driven diabetes complications mobile screening program in Alberta, Canada. Can J Public Health (2010) 101(5):410–4. doi: 10.1007/BF03404863
53. Shah BR, Cauch-Dudek K, Pigeau L. Diabetes prevalence and care in the Metis population of Ontario, Canada. Diabetes Care (2011) 34(12):2555–6. doi: 10.2337/dc11-0945
54. Lovell M, Harris K, Forbes T, Twillman G, Abramson B, Criqui MH, et al. Peripheral arterial disease: lack of awareness in Canada. Can J Cardiol (2009) 25(1):39–45. doi: 10.1016/S0828-282X(09)70021-2
55. Oster RT, VIrani S, Strong D, Shade S, Toth EL. Diabetes care and health status of First Nations individuals with type 2 diabetes in Alberta. Can Family Physician. (2009) 55(4):386–93.
56. Bruce SG, Young TK. Prevalence and risk factors for neuropathy in a Canadian First Nation community. Diabetes Care (2008) 31(9):1837–41. doi: 10.2337/dc08-0278
57. Dannenbaum D, Kuzmina E, Lejeune P, Torrie J, Gangbe M. Prevalence of diabetes and diabetes-related complications in First Nations communities in northern Quebec (Eeyou Istchee), Canada. Can J Diabetes. (2008) 32(1):46–52. doi: 10.1016/S1499-2671(08)21010-5
58. Attawar DS. Diabetes-related foot complications and amputations in a Manitoba First Nation community: a systems approach to prevention. Winnipeg, Manitoba, Canada (2008).
59. Martens PJ, Martin BD, O'Neil JD, MacKinnon M. Diabetes and adverse outcomes in a First Nations population: associations with healthcare access, and socioeconomic and geographical factors. Can J Diabetes. (2007) 31(3):223–32. doi: 10.1016/S1499-2671(07)13009-4
60. McIntyre I, Boughen C, Trepman E, Embil JM. Foot and ankle problems of Aboriginal and non-Aboriginal diabetic patients with end-stage renal disease. Foot ankle Int (2007) 28(6):674–86. doi: 10.3113/FAI.2007.0674
61. Rose G, Duerksen F, Trepman E, Cheang M, Simonsen JN, Koulack J, et al. Multidisciplinary treatment of diabetic foot ulcers in Canadian Aboriginal and non-Aboriginal people. Foot Ankle Surgery. (2008) 14(2):74–81. doi: 10.1016/j.fas.2007.10.006
62. Goulet S, Trepman E, Koulack J, Fong H, Duerksen F, Martin B, et al. Revascularization for peripheral vascular disease in Aboriginal and non-Aboriginal patients. J Vasc surgery. (2006) 43(4):735–41. doi: 10.1016/j.jvs.2005.11.058
63. Reid KS, Martin BD, Duerksen F, Nicolle LE, Garrett M, Simonsen JN, et al. Diabetic foot complications in a northern Canadian Aboriginal community. Foot ankle Int (2006) 27(12):1065–73. doi: 10.1177/107110070602701212
64. Hanley AJ, Harris SB, Mamakeesick M, Goodwin K, Fiddler E, Hegele RA, et al. Complications of type 2 diabetes among Aboriginal Canadians: prevalence and associated risk factors. Diabetes Care (2005) 28(8):2054–7. doi: 10.2337/diacare.28.8.2054
65. Meatherall BL, Garrett MR, Kaufert J, Martin BD, Fricke MW, Arneja AS, et al. Disability and quality of life in Canadian aboriginal and non-aboriginal diabetic lower-extremity amputees. Arch Phys Med rehabilit (2005) 86(8):1594–602. doi: 10.1016/j.apmr.2004.11.026
66. Pollex RL, Mamakeesick M, Zinman B, Harris SB, Hanley AJ, Hegele RA. Methylenetetrahydrofolate reductase polymorphism 677C> T is associated with peripheral arterial disease in type 2 diabetes. Cardiovasc diabetol (2005) 4(1):1–7. doi: 10.1186/1475-2840-4-17
67. Iwasaki Y, Bartlett J, O'neil J. An examination of stress among Aboriginal women and men with diabetes in Manitoba, Canada. Ethnicity Health (2004) 9(2):189–212. doi: 10.1080/1355785042000222888
68. Légaré G. Project of diabetes surveillance among the cree of eeyou istchee. Cree Health Publicat (2010), 84.
69. Thommasen H, Patenaude J, Anderson N, McArthur A, Tildesley H. Differences in diabetic co-morbidity between Aboriginal and non-Aboriginal people living in Bella Coola, Canada. Rural Remote Health (2004) 4(4):1. doi: 10.22605/RRH319
70. Jin A, Martin JD, Sarin C. Diabetes mellitus in the First Nations population of British Columbia, Canada. Part 2. Hosp morbidity. Int J circumpolar Health (2002) 61(3):254–9. doi: 10.3402/ijch.v61i3.17459
71. Hernandez CA, Antone I, Cornelius I. A grounded theory study of the experience of type 2 diabetes mellitus in First Nations adults in Canada. J Transcultural Nursing. (1999) 10(3):220–8. doi: 10.1177/104365969901000313
72. Brassard P, Robinson E, Dumont C. Descriptive epidemiology of non-insulin-dependent diabetes mellitus in the James Bay Cree population of Quebec, Canada. Arctic Med Res (1993) 52(2):47–54.
73. Macaulay AC, Montour LT, Adelson N. Prevalence of diabetic and atherosclerotic complications among Mohawk Indians of Kahnawake, PQ. CMAJ: Can Med Assoc J (1988) 139(3):221.
74. Young TK, McIntyre LL, Dooley J, Rodriguez J. Epidemiologic features of diabetes mellitus among Indians in northwestern Ontario and northeastern Manitoba. Can Med Assoc J (1985) 132(7):793.
75. Essien SK, Linassi G, Larocque M, Zucker-Levin A. Incidence and trends of limb amputation in first nations and general population in Saskatchewan 2006-2019. PloS One (2021) 16(7):e0254543. doi: 10.1371/journal.pone.0254543
76. VIrani S, Strong D, Tennant M, Greve M, Young H, Shade S, et al. Rationale and implementation of the SLICK project. Can J Public Health (2006) 97(3):241–7. doi: 10.1007/BF03405595
77. Chan BTB, Sodhi SK, Mecredy GC, Farrell T, Gordon J. Diabetes prevalence and complication rates: In individual First Nations communities in the Sioux Lookout region of Ontario. Can Family physician Medecin famille canadien. (2021) 67(8):601–7. doi: 10.46747/cfp.6708601
78. Martens PJ, Bond R, Jebamani L, Burchill C, Roos NP, Derksen S, et al. Martens patricia ea. The health and health care use of registered first nations people living in manitoba: A population-based study. Manitoba, Canada: Manitoba Centre for Health Policy, Department of Community Health Sciences, Faculty of Medicine, University of Manitoba (2002).
79. Essien SK, Zucker-Levin A. Factors associated with prolonged post-operative acute care length of stay in limb amputation patients in Saskatchewan, Canada. BMC Health Serv Res (2021) 21(1):1–9. doi: 10.1186/s12913-021-07163-z
80. Pace R, Harris S, Parry M, Zaran H. Primary and secondary cardiovascular prevention among first nations peoples with type 2 diabetes in Canada: findings from the FORGE AHEAD program. CJC Open (2020) 2(6):547–54. doi: 10.1016/j.cjco.2020.07.004
81. Hayward MN, Pace R, Zaran H, Dyck R, Hanley AJ, Green ME, et al. Closing the indigenous health gap in Canada: Results from the TransFORmation of IndiGEnous PrimAry HEAlthcare delivery (FORGE AHEAD) program. Diabetes Res Clin Practice. (2020) 162:108066. doi: 10.1016/j.diabres.2020.108066
82. Shah BR, Cauch-Dudek K, Pigeau L. Diabetes prevalence and care in the Métis population of Ontario, Canada. Diabetes Care (2011) 34(12):2555–6. doi: 10.2337/dc11-0945
83. Staniszewska S, Brett J, Simera I, Seers K, Mockford C, Goodlad S, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. Res involvement engagement. (2017) 3(1):13. doi: 10.1186/s40900-017-0062-2
84. Hong QN, Fábregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ Inf (2018) 34(4):285–91.
85. Bird SM, Wiles JL, Okalik L, Kilabuk J, Egeland GM. Living with diabetes on Baffin Island: Inuit storytellers share their experiences. Can J Public Health (2008) 99:17–21. doi: 10.1007/BF03403734
86. West M, Chuter V, Munteanu S, Hawke F. Defining the gap: a systematic review of the difference in rates of diabetes-related foot complications in Aboriginal and Torres Strait Islander Australians and non-Indigenous Australians. J Foot Ankle Res (2017) 10(1):1–10. doi: 10.1186/s13047-017-0230-5
87. Isa D, Pace D. Is ethnicity an appropriate measure of health care marginalization? A systematic review and meta-analysis of the outcomes of diabetic foot ulceration in Aboriginal populations. Can J Surg (2021) 64(5):E476. doi: 10.1503/cjs.004619
88. Rodrigues BT, Vangaveti VN, Malabu UH. Prevalence and risk factors for diabetic lower limb amputation: a clinic-based case control study. J Diabetes Res (2016) 2016:1–7. doi: 10.1155/2016/5941957
89. Akinlotan MA, Primm K, Bolin JN, Ferdinand Cheres AL, Lee J, Callaghan T, et al. Racial, rural, and regional disparities in diabetes-related lower-extremity amputation rates 2009–2017. Diabetes Care (2021) 44(9):2053–60. doi: 10.2337/dc20-3135
90. Fan L, Wu X-J. Sex difference for the risk of amputation in diabetic patients: A systematic review and meta-analysis. PloS One (2021) 16(3):e0243797. doi: 10.1371/journal.pone.0243797
91. Hackler EL III, Hamburg NM, White Solaru KT. Racial and ethnic disparities in peripheral artery disease. Circ Res (2021) 128(12):1913–26. doi: 10.1161/CIRCRESAHA.121.318243
92. Jiang F-H, Liu X-M, Yu H-R, Qian Y, Chen H-L. The incidence of depression in patients with diabetic foot ulcers: a systematic review and meta-analysis. Int J Lower Extremity Wounds. (2022) 21(2):161–73. doi: 10.1177/1534734620929892
93. O’Neill SM, Kabir Z, McNamara G, Buckley CM. Comorbid depression and risk of lower extremity amputation in people with diabetes: systematic review and meta-analysis. BMJ Open Diabetes Res Care (2017) 5(1):e000366. doi: 10.1136/bmjdrc-2016-000366
94. Goins RT, Noonan C, Winchester B, Brock D. Depressive symptoms and all-cause mortality in older American Indians with type 2 diabetes mellitus. J Am Geriatrics Society. (2019) 67(9):1940–5. doi: 10.1111/jgs.16108
95. O’Neill L, Fraser T, Kitchenham A, McDonald V. Hidden burdens: A review of intergenerational, historical and complex trauma, implications for indigenous families. J Child Adolesc Trauma. (2018) 11:173–86. doi: 10.1007/s40653-016-0117-9
96. Crowshoe LL, Henderson R, Jacklin K, Calam B, Walker L, Green ME. Educating for Equity Care Framework: Addressing social barriers of Indigenous patients with type 2 diabetes. Can Family Physician. (2019) 65(1):25–33.
97. King M, Smith A, Gracey M. Indigenous health part 2: the underlying causes of the health gap. Lancet (2009) 374(9683):76–85. doi: 10.1016/S0140-6736(09)60827-8
98. Morriseau TS. Determinants of wellness: A perspective on diabetes and indigenous health. Can J Diabetes. (2022) 46(6):551–2. doi: 10.1016/j.jcjd.2022.06.008
99. Murdoch-Flowers J, Tremblay M-C, Hovey R, Delormier T, Gray-Donald K, Delaronde E, et al. Understanding how Indigenous culturally-based interventions can improve participants’ health in Canada. Health Promot Int (2019) 34(1):154–65. doi: 10.1093/heapro/dax059
100. Monteiro-Soares M, Vale-Lima J, Martiniano J, Pinheiro-Torres S, Dias V, Boyko EJ. A systematic review with meta-analysis of the impact of access and quality of diabetic foot care delivery in preventing lower extremity amputation. Diabetes its Complicat (2020) 107837:1–21. doi: 10.1016/j.jdiacomp.2020.107837
101. Liu PP, King M, King A. Achieving health equities in indigenous peoples in Canada: learnings adaptable for diverse populations. Circulation (2022) 146(3):153–5. doi: 10.1161/CIRCULATIONAHA.122.060773
102. Sadler S, Gerrard J, West M, Lanting S, Charles J, Searle A, et al. Aboriginal and Torres Strait Islander Peoples’ perceptions of foot and lower limb health: a systematic review. J Foot Ankle Res (2022) 15(1):1–11. doi: 10.1186/s13047-022-00557-0
103. Leclerc A-M, Busque A, Miquelon P, Rivard M-C. cardiovascular Disease Prevention: A scoping review of Healthy eating and Physical Activity Among indigenous Peoples in Canada. Can J Cardiovasc Nursing. (2019) 29(3):26–37.
104. Truth and Reconciliation Commission of Canada. Calls to action. In: Canada, governement of Canada. Winnipeg, Manitoba (2015).
105. Ricci-Cabello I, Ruiz-Perez I, Rojas-Garcia A, Pastor G, Goncalves DC. Improving diabetes care in rural areas: a systematic review and meta-analysis of quality improvement interventions in OECD countries. PloS One (2013) 8(12):e84464. doi: 10.1371/journal.pone.0084464
106. Rosella LC, Kornas K, Green ME, Shah BR, Walker JD, Frymire E, et al. Characterizing risk of type 2 diabetes in First Nations people living in First Nations communities in Ontario: a population-based analysis using cross-sectional survey data. Can Med Assoc Open Access J (2020) 8(1):E178–E83. doi: 10.9778/cmajo.20190210
107. Tremblay MC, Bradette-Laplante M, Witteman HO, Dogba MJ, Breault P, Paquette JS, et al. Providing culturally safe care to Indigenous people living with diabetes: Identifying barriers and enablers from different perspectives. Health Expectations. (2021) 24(2):296–306. doi: 10.1111/hex.13168
108. Patel J, Zamzam A, Syed M, Blanchette V, Cross K, Albalawi Z, et al. A scoping review of foot screening in adults with diabetes mellitus across Canada. Can J Diabetes (2022) 46(5):435–40.e2. doi: 10.1016/j.jcjd.2021.09.018
109. Beckett M, Firestone MA, McKnight CD, Smylie J, Rotondi MA. A cross-sectional analysis of the relationship between diabetes and health access barriers in an urban First Nations population in Canada. BMJ Open (2018) 8(1):e018272. doi: 10.1136/bmjopen-2017-018272
110. Blanchette V, Todkar S, Brousseau-Foley M, Rheault N, Weisz T, Poitras M-E, et al. Collaboration and partnership in a five-level engagement framework for diabetic foot ulcer management: a patient-oriented scoping review. Can J Diabetes (2023), S1499-2671(23)00163-6. doi: 10.1016/j.jcjd.2023.07.002
111. Turpel-Lafond ME, Johnson H. In plain sight: Addressing Indigenous-specific racism and discrimination in BC health care. BC Studies: Br Columbian Q (2021) 209):7–17.
112. Bonevski B, Randell M, Paul C, Chapman K, Twyman L, Bryant J, et al. Reaching the hard-to-reach: a systematic review of strategies for improving health and medical research with socially disadvantaged groups. BMC Med Res Methodol (2014) 14:1–29. doi: 10.1186/1471-2288-14-42
113. Drawson AS, Toombs E, Mushquash CJ. Indigenous research methods: A systematic review. Int Indigenous Policy J (2017) 8(2):1–27. doi: 10.18584/iipj.2017.8.2.5
114. Adelson N. The embodiment of inequity: health disparities in aboriginal Canada. Can J Public Health. (2005) 96(Suppl 2):S45–61. doi: 10.1007/BF03403702
115. Pearson O, Schwartzkopff K, Dawson A, Hagger C, Karagi A, Davy C, et al. Aboriginal community controlled health organisations address health equity through action on the social determinants of health of Aboriginal and Torres Strait Islander peoples in Australia. BMC Public Health (2020) 20:1–13. doi: 10.1186/s12889-020-09943-4
116. Asiniwasis R, Stonechild AB, Queen D, Sibbald RG. Indigenous diabetic foot-related lower extremity amputations: integrating traditional indigenous and western health models for improved outcomes. LWW; (2023) p:63. doi: 10.1097/01.ASW.0000905664.97542.fd
118. Allan B, Smylie J. First Peoples, second class treatment: The role of racism in the health and well-being of Indigenous peoples in Canada. Toronto, Canada: Wellesley Institute (2015).
119. Loppie C, Wien F. Understanding Indigenous health inequalities through a social determinants model. National Collaborating Centre for Indigenous Health: Prince George, BC, Canada (2022).
120. Gottlieb K. The Nuka System of Care: improving health through ownership and relationships. Int J circumpolar Health (2013) 72(1):21118. doi: 10.3402/ijch.v72i0.21118
121. Allen L, Hatala A, Ijaz S, Courchene ED, Bushie EB. Indigenous-led health care partnerships in Canada. Cmaj (2020) 192(9):E208–E16. doi: 10.1503/cmaj.190728
122. McHugh ML. Interrater reliability: the kappa statistic. Biochemia medica. (2012) 22(3):276–82. doi: 10.11613/BM.2012.031
123. Blanchette V, Kayssi A. Sex, gender, race and ethnicity matter in limb preservation in north america. Wound Care Canada. (2022) 3(3):30–6.
124. Hussain MA, Al-Omran M, Salata K, Sivaswamy A, Verma S, Forbes TL, et al. A call for integrated foot care and amputation prevention pathways for patients with diabetes and peripheral arterial disease across Canada. Can J Public Health (2019) 110(2):1–3. doi: 10.17269/s41997-018-0166-y
125. Bjornstad P, Chao LC, Cree-Green M, Dart AB, King M, Looker HC, et al. Youth-onset type 2 diabetes mellitus: an urgent challenge. Nat Rev Nephrol (2022) 19(3):1–17. doi: 10.1038/s41581-022-00645-1
126. Sacristán JA. Patient-centered medicine and patient-oriented research: improving health outcomes for individual patients. BMC Med Inf decision making. (2013) 13(1):1–8. doi: 10.1186/1472-6947-13-6
127. Blanchette V, Patry J, Brousseau-Foley M. Adequacy between canadian clinical guidelines and recommendations compared with international guidelines for the management of diabetic foot ulcers. Can J Diabetes. (2021) 45(8):761–7. e12. doi: 10.1016/j.jcjd.2021.03.004
128. Fernando ME, Blanchette V, Mishra R, Zulbaran-Rojas A, Rowe V, Mills JL, et al. Frailty in people with chronic limb threatening ischemia and diabetes-related foot ulcers: A systematic review. Ann Vasc Surg (2022) 89:322–37. doi: 10.1016/j.avsg.2022.09.057
Keywords: diabetes, foot ulcer, lower extremity amputation, indigenous peoples, diabetic neuropathy, peripheral arterial disease, health equity
Citation: Blanchette V, Patry J, Brousseau-Foley M, Todkar S, Libier S, Leclerc A-M, Armstrong DG and Tremblay M-C (2023) Diabetic foot complications among Indigenous peoples in Canada: a scoping review through the PROGRESS-PLUS equity lens. Front. Endocrinol. 14:1177020. doi: 10.3389/fendo.2023.1177020
Received: 01 March 2023; Accepted: 18 July 2023;
Published: 14 August 2023.
Edited by:
Richard Paisey, South Devon Healthcare NHS Foundation Trust, United KingdomReviewed by:
Angie Abbott, South Devon Healthcare NHS Foundation Trust, United KingdomCopyright © 2023 Blanchette, Patry, Brousseau-Foley, Todkar, Libier, Leclerc, Armstrong and Tremblay. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Virginie Blanchette, VmlyZ2luaWUuQmxhbmNoZXR0ZUB1cXRyLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.