
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Endocrinol. , 02 June 2023
Sec. Obesity
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1167119
This article is part of the Research Topic Obesogens in the XXI century: emerging health challenges Volume II View all 6 articles
 Beatriz Rodrigues Risuenho Peinado1
Beatriz Rodrigues Risuenho Peinado1 Deborah Ribeiro Frazão1
Deborah Ribeiro Frazão1 Leonardo Oliveira Bittencourt1
Leonardo Oliveira Bittencourt1 Renata Duarte de Souza-Rodrigues1
Renata Duarte de Souza-Rodrigues1 Maria Tereza Campos Vidigal2Douglas Teixeira da Silva2
Maria Tereza Campos Vidigal2Douglas Teixeira da Silva2 Luiz Renato Paranhos2
Luiz Renato Paranhos2 Marcela Baraúna Magno3
Marcela Baraúna Magno3 Nathalia Carolina Fernandes Fagundes4
Nathalia Carolina Fernandes Fagundes4 Lucianne Cople Maia3
Lucianne Cople Maia3 Rafael Rodrigues Lima1*
Rafael Rodrigues Lima1*Background: Obesity is a growing chronic public health problem. The causes of obesity are varied, but food consumption decisions play an important role, especially decisions about what foods to eat and how much to consume. Food consumption decisions are driven, in part, by individual taste perceptions, a fact that can influence eating behavior and, therefore, body mass.
Methodology: The searches were conducted in the electronic databases PubMed, Web of Science, Scopus, Lilacs, and the grey literature (Google Scholar and Open Grey). The acronym PECO will be used, covering studies with adult humans (P) who have obesity (E) compared to adult humans without obesity (C), having as an outcome the presence of taste alterations (O). After searching, duplicates were removed. The articles were first evaluated by title and abstract, following the inclusion and exclusion criteria; then, the papers were read in full. After the studies were selected, two reviewers extracted the data and assessed the individual risk of bias and control statements for possible confounders and bias consideration. The narrative GRADE system performed the methodological quality assessment using the New Castle Ottawa qualifier and analysis of certainty of evidence.
Results: A total of 3782 records were identified from the database search, of these 19 were considered eligible. Forty percent of the eligible studies show that there was an association between obesity and different taste alterations for different flavors comparing with normal weights adults. In the methodological quality analysis of the nineteen studies, which assesses the risk of bias in the results, fifteen showed good methodological reliability, three showed fair methodological reliability, and one showed low methodological reliability.
Conclusion: Despite methodological limitations, the results of the studies suggest the existence of a association between obesity and taste alterations, but further investigations with more sensitive methodologies are necessary to confirm this hypothesis.
Systematic review registration: https://osf.io/9vg4h/, identifier 9vg4h.
Obesity is a growing public health problem (1), since according to the World Obesity Atlas 2022 estimate published by the World Obesity Federation, the world will have, on average, one billion obese people in 2030. According to the latest global estimation from the World Health Organization (WHO), worldwide, obesity cases have more than doubled since 1980 (2).
An excessive increase in body fat characterizes this disease. It is associated with several deleterious aspects, such as lack of physical activity, poor eating habits, genetic conditions (e.g., mutations in the leptin gene or receptor), central nervous system abnormalities (e.g., hypothalamic alterations), hormonal factors (e.g., resistance to insulin action), psychological disorders (e.g., depression and anxiety), and socioeconomic factors (e.g., purchasing power) and obesity at levels directly proportional (3–9).
According to the WHO, the diagnosis of obesity based on is the parameter stipulated by the World Health Organization - the body mass index (BMI), obtained from the relationship between body weight (kg) and height (m)² of individuals. An individual is classified as obese when your BMI (Body Mass Index) exceeds 30kg/m². In addition, obesity has three levels of classification: Obesity Grade I with a BMI between 30 and 34.9 kg/m², Grade II obesity with a BMI between 35 and 39.9 kg/m² and Grade III obesity from 40 kg/m², also known as obesity morbid (2).
Much of the investigation on obesity is focused on individuals’ eating behavior or food reward response rather than the sensory aspects of eating, so the complex link between taste perception and BMI is unclear (10). The decisions of which and how much food to consume have significant relevance in the issue of body weight gain and these decisions are promoted, in part, by the taste perceptions of each individual (1).
Taste perception, provided mainly by the taste buds present at the beginning of the digestive tract, is directly associated with food intake. Therefore, alterations in this perception can interfere with a healthy eating routine and lead to problems such as ingesting toxic products (for example, spoiled or poisoned foods) or the overconsumption of certain foods (11). Two-thirds of the taste buds are located on the tongue and the rest are in the epiglottic vallecula and soft palate (12).
A critical hypothesis was formulated by Cabanac, theorizing the existence of a homeostatic set point of body weight inherent and individualized to each individual. This theory is defended through the principle of alaesthesia, characterized as a phenomenon in which, the first amount of food or substance causes a palatable pleasant sensation, however, as the consumption of the same food or substance continues and increases, an unpleasant sensation begins to be felt, which resembles the conception of specific sensory satiety. The authors say that alaesthesia depends on as yet unknown internal signals and suggest that this signal may be the variation in systemic glucose concentration (13, 14).
Altered taste perception can also lead to unbalanced eating routines, leading to over-nutrition or malnutrition resulting in disease conditions such as cognitive deficits, sensory deficits, immunity problems, malnutrition, cardiovascular problems, and neurodegeneration caused by a chronic high-fat diet. Therefore, investigations must be carried out on the sensory aspects of food intake, that is, sensitivity, preference, intensity of perception and specific sensory sensitivity, to understand the link between taste perception and obesity (2, 15–18).
The role of taste factors in obesity is a clinically important issue, as dietary non-compliance is a major issue in managing obesity and associated diseases such as diabetes. Therefore, quantifying the differences in taste perception may represent a new risk factor for obesity or obesity phenotype and inform future weight loss interventions. So far, no records in the literature of any previous systematic review on this subject exist. Thus, this systematic review aims to assess the association between obesity and taste alterations in adults.
The protocol was reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) (19) and is available in the Open Science Framework (OSF) database at the following link: (osf.io/9vg4h). This systematic review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (20).
The review was designed to answer whether there is an association between obesity and taste alterations in adult patients. The PECO strategy was used to define the eligibility criteria, where “P” represents the population (adult patients), “E” the exposure (obesity), “C” the comparison (subjects without obesity) and “O” the outcome (taste alteration).
The inclusion criteria for selection of articles were as follows (1): prospective or retrospective observational studies as cross-sectional, case-control, or cohort studies being conducted in adult humans with no others systemic diseases, and (2) studies whose focus was the comparison of taste sensitivity in average weight and obese subjects. There were no restrictions on the language or year of publication.
We excluded studies with sample overlapping (in this case, considering the most recent study that best described the methodology and results); Studies being conducted in animal, children or teenagers and in vitro studies; Case reports, reviews, descriptive studies, opinion articles, technical articles, editorials, letters to the editor, personal opinions, books, and book chapters.
Two authors (BRRP and DRF) used a search strategy consisting of MeSH and free terms to systematically search the online databases: PubMed, Scopus, Web of Science, Lilacs, and the grey literature (Google Scholar and Open Grey). The primary descriptors used to compose the search strategies were: “Obesity”; “Taste”; “Adult”. Several combinations among the descriptors were performed with the Boolean operators AND and OR, respecting the syntax rules of each database. The search strategy containing the keywords used in the search bases are included in the Table 1. These procedures were taken to reduce selection bias. Until December 2022, all databases’ searches were regularly updated.
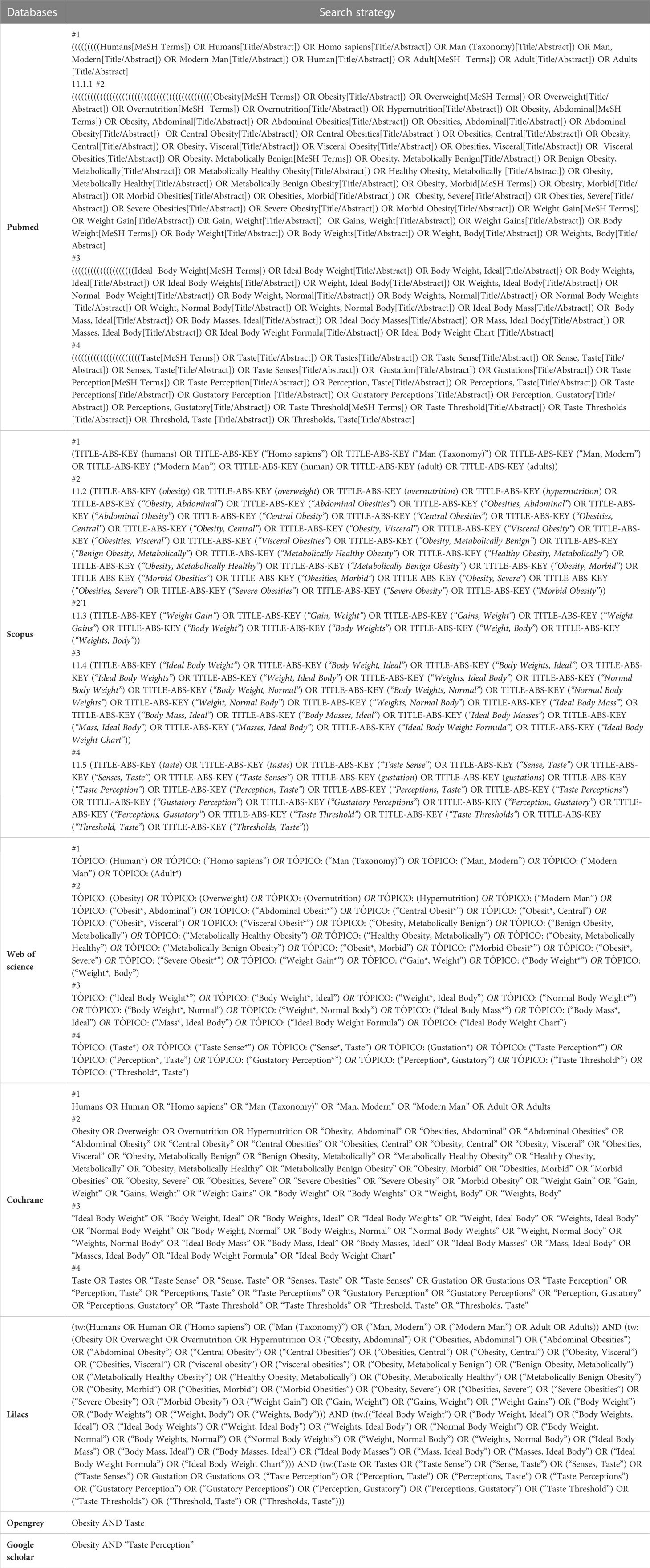
Table 1 Terms used on databases searches.
The recovered findings were transferred to the EndNote X9™ software (Clarivate™ Analytics, Philadelphia, USA), where duplicates were automatically deleted, and the remaining duplicates were manually removed. The gray literature was manually evaluated with Microsoft Word™ 2010 (Microsoft™ Ltd., Washington, USA) simultaneously and thoroughly.
Prior to selecting the studies, two reviewers conducted a calibration exercise in which they reviewed the eligibility criteria and applied them to a sample of 20% of the retrieved studies to determine inter-examiner agreement. The selection process began once an appropriate degree of agreement (Kappa ≥ 0.81) was reached.
Two reviewers (BRRP and DRF) chose the studies after reading the titles and abstracts. A third examiner (LOB) interpreted and defined disagreements between the examiners. Subsequently, the preliminary eligible studies’ full texts were obtained and evaluated. If the full texts could not be located, a bibliographic request was made to the library database (COMUT), and an e-mail was sent to the corresponding authors to obtain the texts.
After a complete reading of all studies included, two reviewers (BRRP and DRF) independently and blindly extracted data from the eligible studies. When there was disagreement about data extraction, a third reviewer (LOB) looked into the issues. The following data were extracted: country, year, study design, main characteristics of the participants (origin, sample size and age), diagnosis of obesity, diagnosis of taste alterations, statistical analysis and results. For situations where relevant information was not available for data extraction and/or risk of bias analysis, the authors were contacted by email.
Two reviewers (BRRP and DRF) independently assessed the methodological quality/risk of bias of the studies included. In case of disagreement, a third reviewer (RRL) was consulted to make a final decision. The Newcastle-Ottawa Scale (NOS) (21) for assessing the quality of studies (Ottawa quality assessment scale case-control studies) was used. This scale consists of questions with predefined domains divided into selection, comparability, and exposure. The first section evaluates the study based on the case definition, the representativeness of the cases, and the selection and definition of the controls. The second domain assesses the comparability of cases and controls based on the design or analysis related to confounding factor control. The exposure section examines the method of determining exposure, the non-response rate, and whether the study used the same exposure assessment method for cases and controls. Thus, studies can get a maximum of nine “stars,” four “stars” for selection, two for comparability, and three for the outcome. These processes were repeated for each type of study included (cross-sectional, case-control, and cohort).
Data extracted from articles fitting the inclusion criteria were analyzed using a narrative synthesis approach in systematic reviews consistent with best practices (22). Data as sample size and age were subgrouped into obese or normal weight. The way of diagnosing obesity was subgrouped into overweight or body mass index percentages. The perception threshold was tested with different flavors such as sweet, bitter, sour, salty and foods with a high-fat content to assess the taste alterations, so this could represent pleasant taste stimuli, sensitivity and preference. Ideally, a formal meta-analysis should be conducted to provide quantitative estimates of differences in taste perception between obese and normal-weight adults, but due to the heterogeneity in exposure metrics and methodologies used across eligible studies, a meta-analysis was not possible.
The GRADE system (Grades of Recommendation, Assessment, Development and Evaluation) was used to assess the certainty of evidence. Four levels of reliability were assigned to the studies included: high, moderate, low, and very low. The highest level indicates strong confidence that the actual effect is close to that estimated, and the lowest level demonstrates that confidence in the effect estimate is very limited, with a significant degree of uncertainty in the findings.
Initially, 3793 records were found from the electronic databases, including the “grey literature.” Then, 106 duplicates were excluded, leaving 3687 articles. A careful reading of the titles and abstracts excluded 3645 studies, leaving 42 for full-text reading. However, 10 of them were not retrieved. In this way, the 32 articles retrieved were read in full. Finally, seven studies were excluded due to the absence of an exposed group, one for not specifying the method of analysis of the taste alteration, one for evaluating taste alterations only after sucrose ingestion, one for associating obesity with alterations in the oral microbiota, and two for the absence of separation between the obese and overweight groups. Thus, 19 articles were included in this review. Figure 1 demonstrates the study selection process in detail.
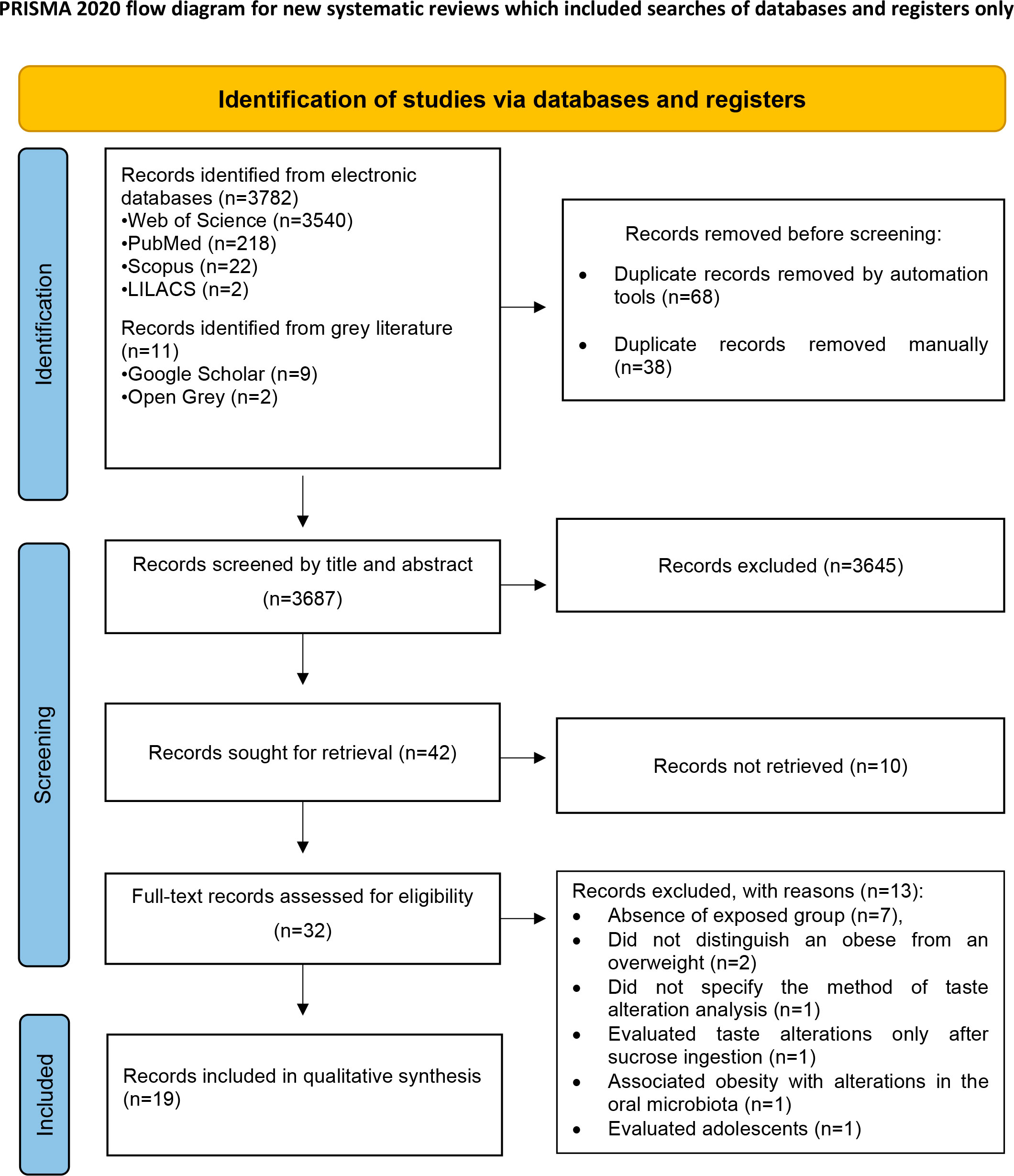
Figure 1 Flow diagram of databases searched according to PRISMA guidelines (Preferred Reporting Items for Systematic Review and Meta-Analysis).
According to the study design, twelve are case-control studies, seven are cross-sectional studies, and one is a cohort study. The studies varied in different outcomes related to taste alterations and in various flavors analyzed: sweet, bitter, sour, salty, and foods with high-fat content.
Eight studies (12, 17, 18, 23–28) evaluated the perception threshold of the groups, that is, the smallest stimulus capable of provoking the least possible sensation of taste. Among the results obtained, six (12, 18, 24, 25, 27, 28) showed no difference between the groups for some flavors, and two (25, 26) concluded that people without obesity had a higher threshold of perception for sweet, salt, bitter and sour taste, and three (17, 18, 23, 24) studies showed that participants with obesity had a higher threshold compared to participants without obesity for same flavors, thus needing higher concentrations to taste any flavor.
Eight studies (11, 12, 14, 15, 24, 25, 29, 30) evaluated whether people with obesity had a reduced intensity of taste perception; that is, for the same supra-threshold concentration, a flavor can be felt less intensely by participants with obesity. Among these, no one obtained results that agreed with this hypothesis; seven results (11, 12, 14, 15, 24, 29, 30) did not identify this taste alteration in either of the two groups, one analysis (25) recognized that aspect in participants without obesity for sweet, salty and sour tastes. However, a specific article (5) investigated initial levels of perception between groups and the speed of decline of this perception with consumption. The result found was that individuals with obesity felt higher initial levels of taste perception than participants without obesity but experienced a slower rate of decline in this perception; that is, the exposed group felt the taste with the same intensity for a more extended period.
Regarding the outcome related to preference for higher concentrations, four results (3, 14, 15, 24) did not identify any difference between the groups evaluated regarding the concentration of sweetness and fat. In contrast, one result (14) found that the control group preferred lower concentrations of sweet fat, and two (25, 29) studies observed that the group with obesity preferred higher concentrations of sweet and one (24) for salty.
In the evaluations of the hedonic response presented by the participants, two (4, 11) studies found that both groups obtained the same level of hedonic response for sweet, salty, and bitter tastes, and one (2) study observed a more significant response of participants with obesity in relation to salty, sweet and fatty tastes.
Among the chosen articles, only two (7, 30) evaluated the outcome related to specific sensory satiety, which is basically defined as a decrease in pleasure and perception when food is consumed until satiety. Thus, one study (7) had similar results for both groups, and the other (30) observed that people with obesity take longer to feel this satiety.
The last analyzed outcome was the brain activation of the groups regarding food consumption, and the results of this study (13) showed that for sweet stimuli, participants with obesity showed greater brain activation in several areas related to gustatory perception. Table 2 summarizes and presents more details of the included studies’ characteristics.
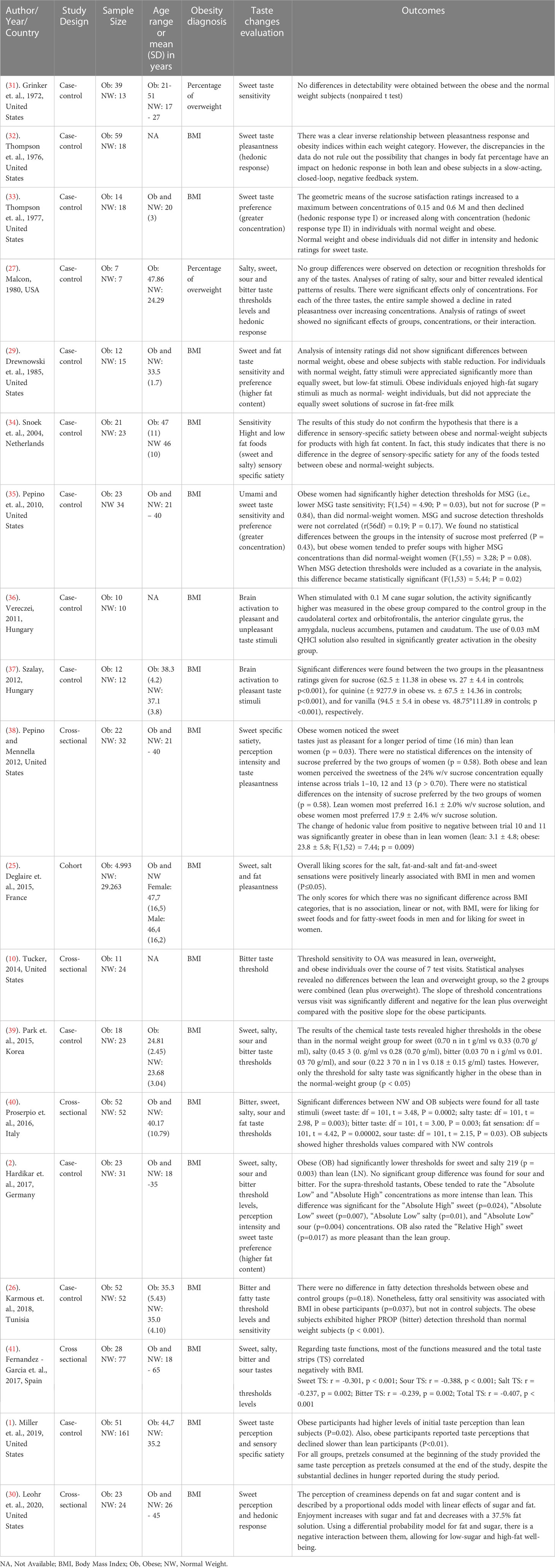
Table 2 Characteristics of included studies.
The main problems among the articles were related to the lack of definition of the controls and the non-response rate (Table 3). All case-control studies scored well on the following items: “Is the case definition adequate?”, “Determination of exposure” and “Same verification method for cases and controls.” Regarding the “representativeness of the cases,” 4 articles (3, 15, 24, 25) did not describe the origin of the sample used. In the item “controls selection,” 5 studies (3, 15, 24) did not score because the origin of the control group is not mentioned. Major problems were identified in the “defining controls” domain, and only seven studies investigated the participants’ history of obesity. Most studies (3–5, 7, 12, 13, 18, 24, 25, 28, 29) used one or more parameters to compare groups; however, three studies (14, 15, 23) did not score in this regard. The Quality Assessment of studies included according to New Castle Ottawa protocol is exposed in Tables 3–5.
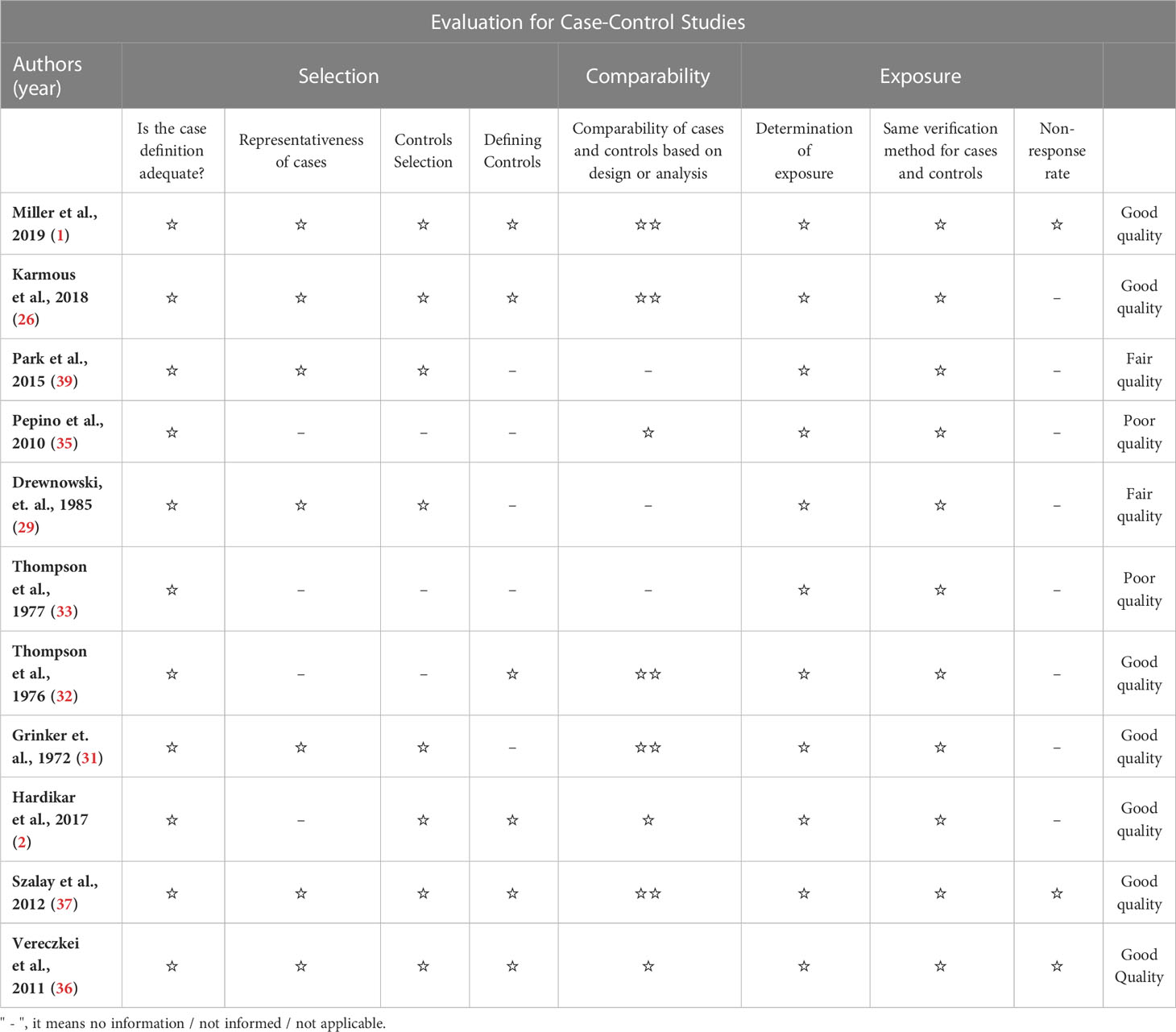
Table 3 Quality Assessment of Case-control studies included, according to New Castle Otawa protocol.
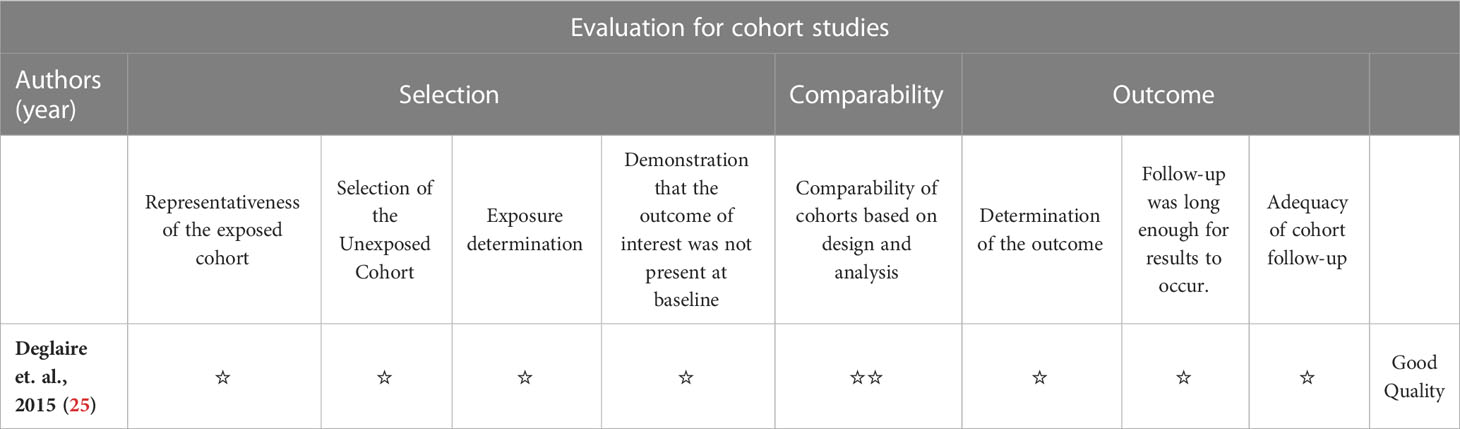
Table 4 Quality Assessment of cohort study included, according to New Castle Otawa protocol.
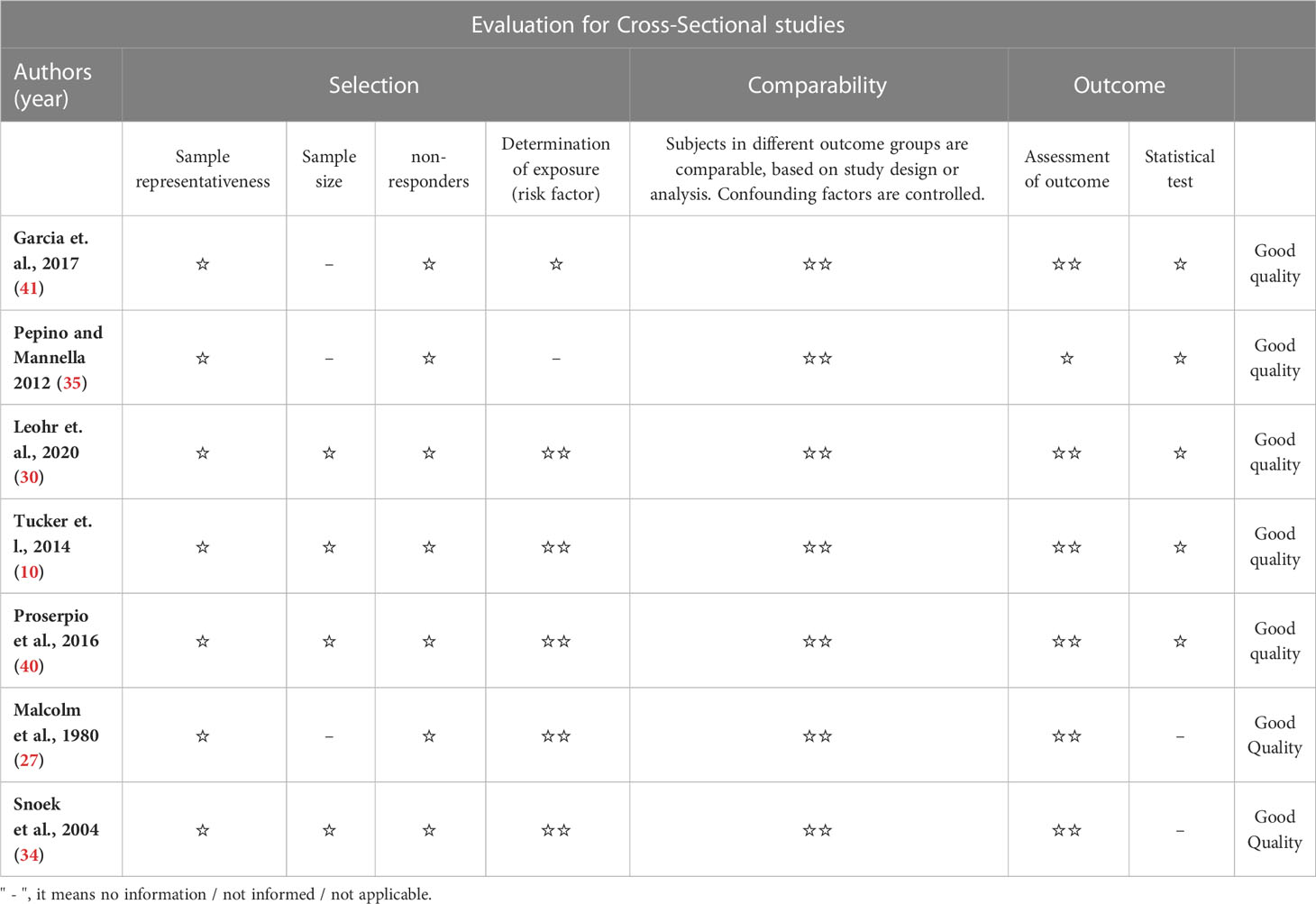
Table 5 Quality Assessment of Cross-Sectional studies included, according to New Castle Otawa protocol.
Regarding the outcome on sweet tastes, 14 observational studies showed low certainty of evidence, indicating that the true effect may be substantially different from the estimated one. As for salty, bitter, and fatty flavors, the 13 observational studies showed moderate certainty of evidence. Regarding sour flavors, five observational studies showed high certainty of evidence, denoting high reliability that the actual effect is close to the effect estimate. Table 6 summarizes these assessments.
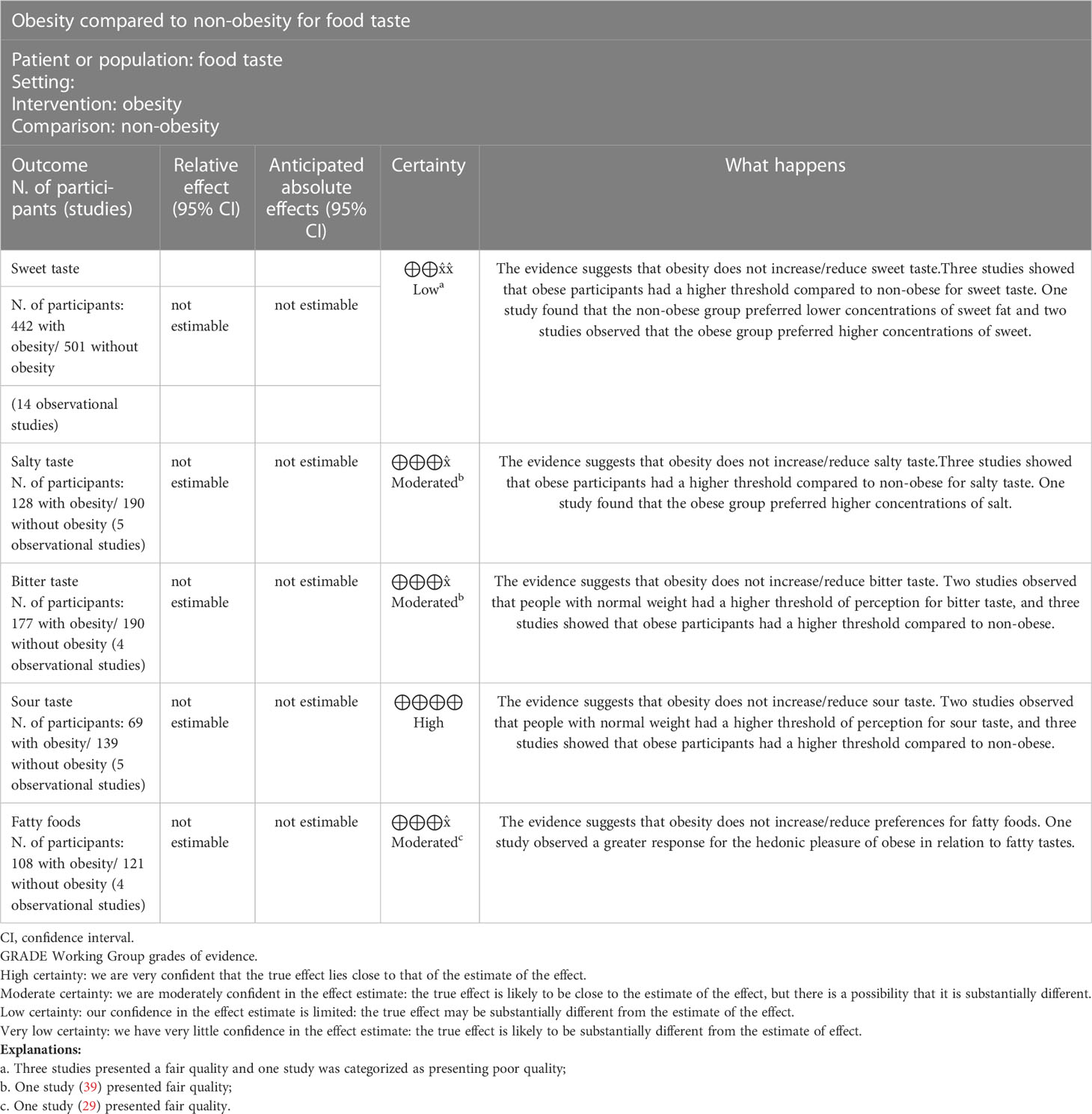
Table 6 Summary of GRADE assessment of each outcome.
This review aimed to gather evidence that would contribute to the scientific community’s understanding possible factors associated with obesity and new possible ways to aid in treating and diagnosing this pathology. Thus, we sought to assess the existence of an association between obesity and taste alterations, finding twenty articles, fifteen of them with good methodological quality and low risk of bias, four with medium risk, and three with low quality and high risk of bias. Among the selected studies, most test results supported the hypothesis of this association’s existence.
The human gustatory system allows the assessment of nutrition and toxicity during food consumption, which assists in the decision of what to eat (10). However, taste acts as an essential checkpoint and plays the most crucial role in the process of acceptance or rejection of food, preferences, and food options and, consequently, influences nutritional status and health (10). Although this association between taste acceptability and food choice has been determined, the extent of individual taste perception in relation to body weight is not well understood (36). Olfactory and gustatory sensations can induce pleasure, commonly associated with excessive food consumption, one of the leading causes of obesity (12). Greater intensities of sweet taste perception may induce stronger hedonic sensations, which may modulate eating behavior, leading to a preference for very sweet and energy-rich foods, indicating a possible etiological factor of obesity (29).
In this systematic review, four articles (26, 35, 39, 40) observed that participants with obesity had a higher threshold of gustatory perception; that is, people with obesity take longer to be able to recognize the taste of food, denoting that they are less sensitive in terms of taste. Studies show that obese or overweight people have a greater preference for sweeter and fatty foods (42, 43), which could be explained by the theory that obese people need higher concentrations of compounds responsible for flavoring food, thus justifying a greater consumption of salt and sugar, for example.
On the other hand, some studies (2, 10, 29–31, 35, 38) reported that participants with obesity felt the flavors at suprathreshold concentrations, that is, above the threshold of gustatory perception, equally intense to the control groups. That is, the ability to discriminate the presence of sweet and/or salty flavors in isomolar concentrations of salt and sugar was similar in both groups. Only one study (25) identified that people with obesity had a high intensity of gustatory perception, that is, the sweet and salty flavors were more intensely experienced, showing a greater gustatory sensitivity for this group. However, all of them had limitations since they used a model of sucrose, monosodium glutamate (MSG), or sodium chloride (NaCl) solution diluted in water at increasing concentrations, which may not be applicable to real life.
Brondel (24) cites the existence of sensory phenomena known to modulate the inhibition of food intake by reducing the pleasure derived from olfactory and gustatory stimuli in humans. These phenomena are directly associated with the feeling of satiety. They are divided into three mechanisms: conditioned satiety, alimentary alliesthesia, and sensory-specific satiety, the latter being investigated by several articles included in this review. According to their study (24), “sensory-specific satiety” is defined as “a relative decrease in the pleasure aroused by a food that has been consumed until satiety, in contrast to uneaten food.” Miller (1) states that the decrease in taste perception is not just a result of satiety and that marginal perceptions of taste seem to decrease due to sensory boredom resulting from repeated consumption of the same item. Thus, the continuous consumption of a type of food creates specific satiety and induces reduced consumption. In individuals without obesity, these sensory phenomena act as negative and final feedback mechanisms for food intake. Therefore, the dysfunction of these mechanisms can be one of the causes of excessive mass gain.
Regarding the outcome of specific sensory satiety, presented in two articles, one result (38) showed that, when consuming food repeatedly, the obese group took longer to experience sensory satiety specific to the food in question. This delay could justify a longer time of food consumption for people with obesity compared to people without obesity. However, another study (34) that evaluated this parameter did not identify differences between the groups. A specific article (1) observed that, in addition to the obesity group having presented higher initial levels of perception intensity than the control group, it also showed a lower perception decline speed than the control group, that is, the specific sensory satiety of the group with obesity manifested itself more slowly, which corroborates other results found (38). Therefore, to help create more effective and specific interventions in treating obesity, understanding the particularities of taste perception plays a vital role in elucidating new risk factors for obesity or obesity phenotype (1). However, the literature is still quite controversial regarding the influence of these phenomena on obesity.
Two studies (36, 37) evaluated the group’s brain activation concerning food consumption in a condition of the intrinsic physiological state of hunger and satiety maintained at a constant level. The neurophysiological investigation of the neural factors that may lead to obesity is an innovative and promising form of research since taste perception is microscopically initiated when food molecules interact with taste receptors existing on the surface of the cells that make up the taste buds, thus generating impulses to the central nervous system related to taste and promoting behavioral responses to different food stimuli in different aspects such as preference, threshold and supra-threshold sensitivity, hedonism, among others. Thus, the authors of both studies reported that, for the analyzes using the compounds: sucrose, vanilla, and quinine, participants with obesity showed greater brain activation in several areas related to taste perception, with emphasis on the hedonically positive stimulation of sucrose in the secondary gustatory cortex (COF) and in the cingulate cortex, both responsible for encoding the reward value of a particular flavor, showing that this may be a more accurate method in helping to understand the neural factors that can lead to obesity.
A case-control study (23) evaluated the association of the composition of the oral microbiota around contoured papillae and salivary parameters involved in sensitivity to oral fat with the threshold of detection of linoleic acid (fatty acid widely found in foods). This research was based on data that indicate that obesity seems to be associated with alterations in taste detection parameters, such as the flow of salivary activity or lipase activity. However, its results did not show differences between the groups with and without obesity.
Some articles included in this review have observed a greater sensitivity of the group with obesity to the salty and bitter taste in threshold concentrations (26, 35, 39, 40). Moreover, there was a preference for higher concentrations and higher hedonic responses (2, 25, 29, 35), especially for the sweet taste. However, the combined results of many studies have obtained inconclusive results, which have found no apparent difference in threshold and suprathreshold sensitivity and hedonic response between individuals with and without obesity (10, 10, 26, 27, 29–31, 35, 37, 38).
An additional interesting information is that Cabanac (13) theorized that food intake is physiologically monitored and regulated according to the needs of each individual, associating pleasure and body mass, thus as long as food contributes to the maintenance of predefined body weight by an individual set point inherent (“ponderostat”), the taste of that food will be perceived pleasantly, inducing a greater consumption, on the other hand, the additional ingestion of food beyond the necessity would make the taste of the food become unpleasant, avoiding the excess of food consumption (32). However, this theory has not been fully confirmed.
To qualify the methods used in the studies, the Newcastle-Otawa Scale was adopted. This protocol helped to assess the consistency and validity of the results generated by the observational studies included in this review. One study (33) presented more significant methodological problems (definition and selection of controls, representativeness of cases, comparability between them, and non-response rate), thus presenting a high risk of bias and low methodological quality. To make a more reliable analysis of the association between the multifactorial pathology in question and taste alterations, there should be a more significant control of confounding factors, using one or more comparability parameters between the groups, which was not done in the methodology of this study, in addition, the obesity history of the participants was also not investigated, as well as the origin of both the groups and the non-response rate, thus this study obtained the worst methodological rating among the others.
On the other hand, another case-control study (37) obtained the maximum score for methodological quality by investigating the groups’ brain activity in the face of gustatory stimulation. Three other cross-sectional studies also receive the maximum qualitative score, with five stars in the selection criterion, two in the comparability criterion, and three in the outcome, demonstrating excellent reliability in the results presented.
Most of the results expressed an association between obesity and taste alterations. On the other hand, the selected articles have some methodological limitations that directly affect the analyses presented here. One of the major limitation observed was the way obesity is diagnosed through BMI, which was used by most studies. More recent researches and guidelines indicate that this parameter, despite being frequently used in nutritional assessments, is very imprecise, since it doesn’t consider body composition, i.e., it doesn’t distinguish fat mass from muscle mass. Therefore, people with a lot of muscle mass can have a high BMI, even though they have a low percentage of body fat. Similarly, people with low muscle mass may have a BMI within the healthy range, but a high body fat percentage. Thus, more current and accurate methods of diagnosis is through analysis of body fat measurement, such as electoral bioimpedance or Dual-energy X-ray absorptiometry, which is not performed by most studies and would decrease the risk of methodological bias for that matter (44).
Another methodological deficiency is about the method for evaluating taste alterations, since many studies use only sucrose or sodium chloride solutions diluted in water at different concentrations to analyze hedonic response, preference and intensity (2, 27, 31–33, 38, 40) which is not representative of a normal daily diet, and therefore does not indicate results compatible with reality. In addition, all the studies are punctual evaluations, clippings of a continuous panorama that does not provide information on how long the patient has had an obesity condition and how the time factor may have influenced this scenario and consequently this association.
Futhermore, studies that despite presenting a well-designed, ethical, and thorough methodology, express some possible limitations that could interfere with the absence of statistical difference. To illustrate, the study from Leohr et al., 2020 (30) conducted a sugar/fat preference test (SFPT) after a standardized lunch meal to avoid any influence of hunger on the scoring of the solutions. However, it is possible that the meal itself could have affected the SFPT results. In addition, studies using only female participants (34, 35, 38) have obtained no statistical difference in some analyses, which could be explained by the fact that the study may be more susceptible to confounding variables that are related to gender, as hormonal differences and menstrual cycle phases can have a direct influence on women’s eating behavior, potentially impacting the results (44).
The heterogeneity and lack of standardization of methods among the included studies was a limiting factor regarding the possibility of making direct comparisons and making more accurate and safe inferences. Therefore, the lack of homogeneity prevented the performance of a meta-analysis in order to evaluate the real difference in perception, sensitivity, and taste pleasure between obese adults and people with average weight.
The studies found in this review aimed to elucidate possible physiological factors associated with the development of this complex pathology, such as behavioral phenotypes, unique brain activations, and distinct sensory responses. Nevertheless, due to the subjectivity of most analysis methods and the great variety of factors that could influence the results, many of the data obtained were inconclusive. Therefore, there is a need for more research on the possible factors associated with obesity and the necessity to create more accurate assessment methods.
Even though 40% of the included studies (2, 29–31, 33, 35, 38) reported that participants with obesity perceived flavors at suprathreshold concentrations (i.e. above the threshold of gustatory perception, with the same intensity as the control groups), methodological tests could be developed and applied in future studies to simulate conditions closer to reality and standardize the methods of measuring the perception of sensitivity to flavors.
According to the articles included, there is a possible association between obesity and taste alterations since most of them report some association between different taste alterations and this pathology. However, further longitudinal investigations using more sensitive methodologies are needed to describe the establishment of these alterations and their interactions with other factors.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
BP, and RL: study concept and design. LB, BP, DF, MM, NF, LM, and RL: analysis and interpretation of data. BP, DF, MM, NF, MV, DS, LP, LM, and RL: preparation of the manuscript. LM, NF, MM, MV, LP, DS, and RL: critical revision of the manuscript. All authors contributed to the article and approved the submitted version.
This research was funded by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior-Brazil (CAPES)-Finance Code 001.
We thanks to Pró-Reitoria de Pesquisa e Pós-Graduação of Federal University of Pará (PROPESP, UFPA, Brazil).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Miller AC, Polgreen LA, Segre EM, Polgreen PM. Variations in marginal taste perception by body mass index classification: a randomized controlled trial. J Acad Nutr Dietetics (2020) 120(1):45–52. doi: 10.1016/j.jand.2019.05.018
2. Hardikar S, Höchenberger R, Villringer A, Ohla K. Higher sensitivity to sweet and salty taste in obese compared to lean individuals. Appetite (2017) 111:158–65. doi: 10.1016/j.appet.2016.12.017
3. Clement K, Vaisse C, Lahlou N, Cabrol S, Pelloux V, Cassuto D, et al. A mutation in the human leptin receptor gene causes obesity and pituitary dysfunction. Nature (1998) 392(6674):398–401. doi: 10.1038/32911
4. Farooqi S, Rau H, Whitehead J, O'Rahilly S. Ob gene mutations and human obesity. Proc Nutr Soc (1998) 57(3):471–5. doi: 10.1079/PNS19980067
5. De Azevedo MASB, Spadotto C. Estudo psicológico da obesidade: dois casos clínicos. Temas em Psicologia (2004) 12(2):127–44.
6. Da Silva GAP, Balaban G, De Motta MEFA. Prevalência de sobrepeso e obesidade em crianças e adolescentes de diferentes condições socioeconômicas. Rev Bras Saúde Materno Infantil (2005) 5:53–9. doi: 10.1590/S1519-38292005000100007
7. Miller GD. Appetite Regulation: Hormones, Peptides, and Neurotransmitters and Their Role in Obesity. Am J Lifestyle Med (2017) 13(6):586–601. doi: 10.1177/1559827617716376
8. Guimarães AC, Feijó I, Soares A, Fernandes S, Machado Z, Parcias SR. Excesso de peso e obesidade em escolares: associação com fatores biopsicológicos, socioeconômicos e comportamentais [Overweight and obesity in school children: association between biopsychological, socioeconomic and behavioral factors]. Arq Bras Endocrinol Metabol (2012) 56(2):142–8. doi: 10.1590/s0004-27302012000200008
9. Dimitri P. Treatment of acquired hypothalamic obesity: now and the future. Front Endocrinol (Lausanne) (2022) 13:846880. doi: 10.3389/fendo.2022.846880
10. Tucker RM, Edlinger C, Craig BA, Mattes RD. Associations between BMI and fat taste sensitivity in humans. Chem senses (2014) 39(4):349–57. doi: 10.1093/chemse/bju006
11. Spence C. Multisensory flavor perception. Cell (2015) 61(1):24–35. doi: 10.1016/j.cell.2015.03.007
12. Alves LMT, Dantas RO. Percepção de sabores em pessoas normais. GED Gastroenterol Endosc Dig (2014) 33(3):102–5.
13. Cabanac M, Duclaux R. Specificity of internal signals in producing satiety for taste stimuli. Nature (1970) 227(5261):966–7. doi: 10.1038/227966a0
14. Cabanac M, Duclaux R, Spector NH. Sensory feedback in regulation of body weight: is there a ponderostat? Nature (1971) 229(5280):125–7. doi: 10.1038/229125a0
15. De Arruda IK, De Arruda BK. Nutrição e desenvolvimento. Cadernos Saúde Pública (1994) 10:392–7. doi: 10.1590/S0102-311X1994000300019
16. Sawaya AL. Desnutrição: conseqüências em longo prazo e efeitos da recuperação nutricional. Estudos avançados (2006) 20:147–58. doi: 10.1590/S0103-40142006000300016
17. Mandavia CH, Pulakat L, DeMarco V, Sowers JR. Over-nutrition and metabolic cardiomyopathy. Metabolism (2012) 61(9):1205–10. doi: 10.1016/j.metabol.2012.02.013
18. Cai D. Neuroinflammation and neurodegeneration in overnutrition-induced diseases. Trends Endocrinol Metab (2013) 24(1):40–7. doi: 10.1016/j.tem.2012.11.003
19. Moher D, Shamseer L., Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev (2015) 4:1. doi: 10.1186/2046-4053-4-1
20. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (2021) 372:n71. doi: 10.1136/bmj.n71
21. de Sousa Né YG, Frazão DR, Bittencourt LO, Fagundes NCF, Marañón-Vásquez G, Crespo-Lopez ME, et al. Are dental caries associated with oxidative stress in saliva in children and adolescents? a systematic review. Metabolites (2022) 12(9):858. doi: 10.3390/metabo12090858
22. Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan S E, Ellis S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ (2020) 368:l6890. doi: 10.1136/bmj.l6890
23. Besnard P, Christensen JE, Brignot H, Besnard A, Passilly-Degrace P, Nicklaus S, et al. Obese subjects with specific gustatory papillae microbiota and salivary cues display an impairment to sense lipids. Sci Rep (2018) 8:6742. doi: 10.1038/s41598-018-24619-1
24. Brondel L, Romer M, Van Wymelbeke V, Walla P, Jiang T, Deecke L, et al. Sensory-specific satiety with simple foods in humans: no influence of BMI? Int J Obes (2007) 31(6):987–95. doi: 10.1038/sj.ijo.0803504
25. Deglaire A, Méjean C, Castetbon K, Kesse-Guyot E, Hercberg S, Schlich P. Associations between weight status and liking scores for sweet, salt and fat according to the gender in adults (The nutrinet-sante study). Eur J Clin Nutr (2015) 69(1):40–6. doi: 10.1038/ejcn.2014.139
26. Karmous I, Plesník J, Khan AS, Šerý O, Abid A, Mankai A, et al. Orosensory detection of bitter in fat-taster healthy and obese participants: genetic polymorphism of CD36 and TAS2R38. Clin Nutr (2018) 37(1):313–20. doi: 10.1016/j.clnu.2017.06.004
27. Malcolm R, O'Neil PM, Hirsch AA, Currey HS, Moskowitz G. Taste hedonics and thresholds in obesity. Int J Obes (1980) 4(3):203–12.
28. Melis M, Mastinu M, Pintus S, Cabras T, Crnjar R, Tomassini Barbarossa I. Differences in salivary proteins as a function of PROP taster status and gender in normal weight and obese subjects. Molecules (2021) 26(8):2244. doi: 10.3390/molecules26082244
29. Drewnowski A, Brunzell JD, Sande K, Iverius PH, Greenwood MR. Sweet tooth reconsidered: taste responsiveness in human obesity. Physiol Behav (1985) 35(4):617–22. doi: 10.1016/0031-9384(85)90150-7
30. Leohr J, Kjellsson MC. Sweet/fat preference taste in subjects who are lean, obese and very obese. Pharm Res (2020) 37(12):1–11. doi: 10.1007/s11095-020-02968-9
31. Grinker J, Hirsch J, Smith D. Taste sensitivity and susceptibility to external influence in obese and normal weight subjects. J Pers Soc Psychol (1972) 22(3):320. doi: 10.1037/h0032924
32. Thompson DA, Moskowitz HR, Campbell RG. Effects of body weight and food intake on pleasantness ratings for a sweet stimulus. J Appl Physiol (1976) 41(1):77–83. doi: 10.1152/jappl.1976.41.1.77
33. Thompson DA, Moskowitz HR, Campbell RG. Taste and olfaction in human obesity. Physiol Behav (1977) 19(2):335–7. doi: 10.1016/0031-9384(77)90348-1
34. Snoek HM, Huntjens L, Van Gemert LJ, De Graaf C, Weenen H. Sensory-specific satiety in obese and normal-weight women. Am J Clin Nutr (2004) 80(4):823–31. doi: 10.1093/ajcn/80.4.823
35. Pepino MY, Finkbeiner S, Beauchamp GK, Mennella JA. Obese women have lower monosodium glutamate taste sensitivity and prefer higher concentrations than do normal‐weight women. Obesity (2010) 18(5):959–65. doi: 10.1038/oby.2009.493
36. Vereczkei A, Szalay C, Aradi M, Schwarcz A, Orsi G, Perlaki G, et al. Ízstimulációval kiváltott agyi tevékenység funkcionális MR-vizsgálata elhízásban. Magyar Sebészet (2011) 64(6):289–93. doi: 10.1556/maseb.64.2011.6.4
37. Szalay C, Aradi M, Schwarcz A, Orsi G, Perlaki G, Németh L, et al. Gustatory perception alterations in obesity: an fMRI study. Brain Res (2012) 1473:131–40. doi: 10.1016/j.brainres.2012.07.051
38. Pepino MY, Mennella JA. Habituation to the pleasure elicited by sweetness in lean and obese women. Appetite (2012) 58(3):800–5. doi: 10.1016/j.appet.2012.01.026
39. Park DC, Yeo JH, Ryu IY, Kim SH, Jung J, Yeo SG. Differences in taste detection thresholds between normal-weight and obese young adults. Acta oto-laryngologica (2015) 135(5):478–83. doi: 10.3109/00016489.2014.975370
40. Proserpio C, Laureati M, Bertoli S, Battezzati A, Pagliarini E. (2016) Determinants of obesity in Italian adults: the role of taste sensitivity, food liking, and food neophobia. Chem Senses 41(2):169–176, 2016. doi: 10.1093/chemse/bjv072
41. Fernandez-Garcia JC, Alcaide J, Santiago-Fernandez C, Roca-Rodriguez MM, Aguera Z, Baños R, et al. An increase in visceral fat is associated with a decrease in the taste and olfactory capacity. PloS One (2017) 12(2):e0171204. doi: 10.1371/journal.pone.0171204
42. Spinelli S, Monteleone E. Food preferences and obesity. Endocrinol Metab (2021) 36(2):209–19. doi: 10.3803/EnM.2021.105
43. Mela DJ, Sacchetti DA. Sensory preferences for fats: relationships with diet and body composition. Am J Clin Nutr (1991) 53(4):908–15. doi: 10.1093/ajcn/53.4.908
Keywords: humans, obesity, overweight, taste, taste perception
Citation: Peinado BRR, Frazão DR, Bittencourt LO, Souza-Rodrigues RDd, Vidigal MTC, da Silva DT, Paranhos LR, Magno MB, Fagundes NCF, Maia LC and Lima RR (2023) Is obesity associated with taste alterations? a systematic review. Front. Endocrinol. 14:1167119. doi: 10.3389/fendo.2023.1167119
Received: 01 March 2023; Accepted: 03 May 2023;
Published: 02 June 2023.
Edited by:
Tomohiko Isobe, National Institute for Environmental Studies (NIES), JapanReviewed by:
Silvia Salvatore, University of Insubria, ItalyCopyright © 2023 Peinado, Frazão, Bittencourt, Souza-Rodrigues, Vidigal, da Silva, Paranhos, Magno, Fagundes, Maia and Lima. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rafael Rodrigues Lima, cmFmYWxpbWFAdWZwYS5icg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.