 Guo Tang1
Guo Tang1 Long Feng
Long Feng Zhaoyan Gu
Zhaoyan Gu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 23 October 2023
Sec. Endocrinology of Aging
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1154927
This article is part of the Research Topic Menopause: Mood Disorders and Obesity View all 7 articles
Aim: To explore the risk factors of osteoporosis in postmenopausal women in China.
Method: This study collected all patient data from January 2014 to December 2015. Basic information and questionnaires were collected from 524 postmenopausal women in Sanya and Hainan Province. The questionnaire was administered to the enrolled participants by endocrinologists. Biochemical parameters were measured using fasting blood samples, and bone density was measured by dual energy X-ray absorptiometry at the department of radiology of Hainan hospital, PLA General Hospital. Participants with an R-value of ≤-2.5 were diagnosed with osteoporosis. After deleting missing values for each factor, 334 participants were divided into the osteoporosis (n=35) and non-osteoporosis (n=299) groups according to the R-values.
Results: The participants had a median age of 60.8 years (range: 44–94 years). Among the 334 postmenopausal women included in this study, 35 (10.5%) were diagnosed with osteoporosis. Univariate analysis showed statistically significant differences in age, BMI, type of work, alkaline phosphatase, years of smoking, blood calcium levels, kyphosis, fracture, and asthma between the two groups (P<0.05). In addition, multivariate logistic analysis showed that age (odds ratio [OR]: 1.185, 95% confidence interval [CI]: 1.085–1.293, P<0.001) and kyphosis times (OR:1.468, 95% CI: 1.076–2.001, P=0.015) were positively correlated with postmenopausal osteoporosis, whereas BMI (OR: 0.717, 95% CI: 0.617–0.832, P<0.001), blood calcium levels (OR: 0.920, 95% CI: 0.854-0.991, P=0.027), vitamin D levels (OR: 0.787, 95% CI: 0.674–0.918, P=0.002), and outdoor activity time (OR: 0.556, 95% CI: 0.338-0.915, P=0.021) were negatively correlated with postmenopausal osteoporosis.
Conclusion: Low BMI, blood calcium and vitamin D levels, kyphosis time, and outdoor activity time are independent risk factors for osteoporosis in postmenopausal women.
Osteoporosis (OP) is a systemic skeletal disorder characterized by low bone mineral density (BMD), loss of bone mass, microarchitectural deterioration, and loss of bone quality. Up to 71% of osteoporotic fractures occur in women aged 50 years and older (1, 2). In the United States, half of the women older than 50 years have osteoporotic fractures (3). Older postmenopausal women are prone to OP, which increases the risk of fractures associated with reduced quality of life, disability, economic burden, morbidity, and mortality (4–6). It is associated with estrogen deficiency, advanced age, heredity, smoking, leanness, and several diseases and drugs that impair bone health (7). In the United States, the cost of OP-related fractures was $17 billion in 2005, and the cost is expected to increase to $25.3 billion by 2025 (8). OP is also a significant disease in China; OP fractures require long-term hospitalization, and Chinese patients have the highest cost of all fractures, with an estimated 2.33 million OP-related fractures occurring in 2010 and a treatment cost of $9.45 billion, which is expected to rise to 5.99 million fractures at a cost of $25.43 billion USD by 2050 in China (2).
Postmenopausal osteoporosis (PMOP) is an asymptomatic skeletal disease that is often underdiagnosed and undertreated. Furthermore, the increasing burden of socioeconomic medical care and families with OP fractures worldwide highlights the needs to continue to improve the diagnosis of OP and to identify the risk factors for OP (7, 9). This was a cross-sectional study conducted in Hainan Province, Sanya City, China, to explore the risk factors for developing osteoporosis in postmenopausal women.
This study collected all data from January 2014 to December 2015. Basic information and questionnaires were collected from 524 postmenopausal women in Sanya and Hainan provinces. After deleting the missing values for each factor, 334 participants were divided into osteoporosis (n=35) and non-osteoporosis (n=299) groups according to the R-values (Figure 1). The questionnaire was administered to the enrolled participants by endocrinologists. In addition, the same caregiver was assigned to collect the biochemical parameters of each participant by going to the patient’s home to draw fasting blood, which was then sent to the Department of Biochemistry, Hainan hospital, PLA General Hospital for examination. Bone density was measured at the department of radiology of our hospital.
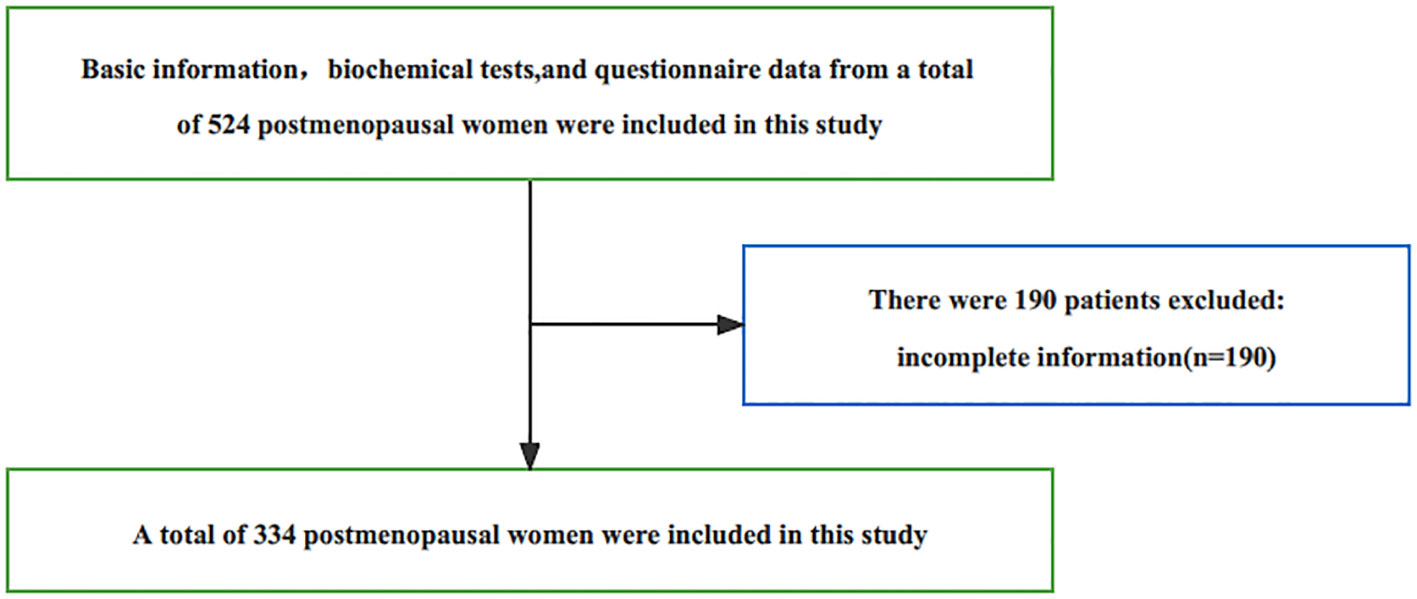
Figure 1 Numbers of centenarians included and excluded in this study.
To evaluate whether postmenopausal OP was present, this study used the R-value determined by dual-energy X-ray absorptiometry (DXA) in all postmenopausal women. BMD measured using DXA is currently considered the gold standard for diagnosing OP (10). According to the World Health Organization (WHO) criteria, OP is defined as a low BMD (> 2.5 SD below the mean) at any site in the lumbar spine (L1-L4), femoral neck, or total hip. It has been suggested that the diagnosis of OP can be based on fractures without significant trauma or low BMD, as measured using DXA. Furthermore, an R-value of ≤ -2.5 is sufficient for the diagnosis of OP (11). The exclusion criteria for this study included the use of OP drugs (such as bisphosphonates and teriparatide), corticosteroid drugs, anorexia nervosa, Cushing’s syndrome, hyperparathyroidism, and kidney disease. In addition, possible causes of secondary OP, such as osteogenesis imperfecta, rheumatism, multiple myeloma, leukemia, lymphoma, systemic mast cell hyperplasia, prior-related osteoporosis, gastrointestinal or biliary diseases, and adverse reactions to drug treatment (anticonvulsants), were excluded (12, 13).
The demographic characteristics and indicators of this study included age, BMI, education level, type of work, race, menarche, menopause, glutamic oxaloacetic transaminase, alkaline phosphatase, creatinine, blood calcium, blood phosphorus, blood vitamin D, urinary calcium, urinary creatinine, outdoor activity time, daily household chores, low back pain time, leg pain duration, leg cramp time, kyphosis, fracture, hypertension, coronary artery disease, diabetes, rheumatoid arthritis, hyperthyroidism, and asthma.
All data were processed using the Statistical Package for the Social Sciences software, version 17 (SPSS Inc., Chicago, IL, USA). Continuous variables with normal distribution were presented as mean and standard deviation and compared using the Student’s t-test. Skewed distributed continuous variables were presented as medians and interquartile ranges and compared using the Mann–Whitney U test. Categorical variables, presented as numbers and percentages of the total, were compared using the Chi-square test. Multivariate logistic analysis was performed for all relevant factors mentioned above to evaluate the risk factors for PMOP. A two-tailed P-value < 0.05 was considered statistically significant.
The participants had a median age of 60.8 years (range: 44–94 years). Among the 334 postmenopausal women in the study, 35 (10.5%) were diagnosed with osteoporosis. The baseline characteristics of the patients in the OP and non-OP groups are shown in Table 1. Univariate analysis of basic data showed that there were statistically significant differences in age, BMI, type of work, alkaline phosphatase, blood calcium, blood calcium, kyphosis, years of smoking, fracture, and asthma between the two groups (P<0.05).
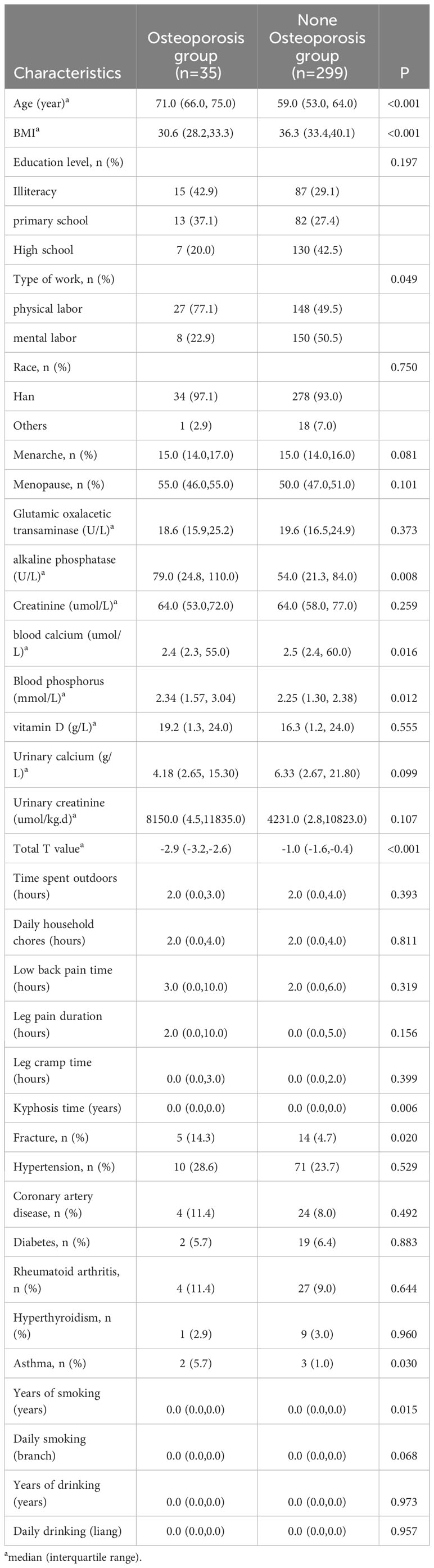
Table 1 Characteristic comparison between osteoporosis group and none osteoporosis group females.
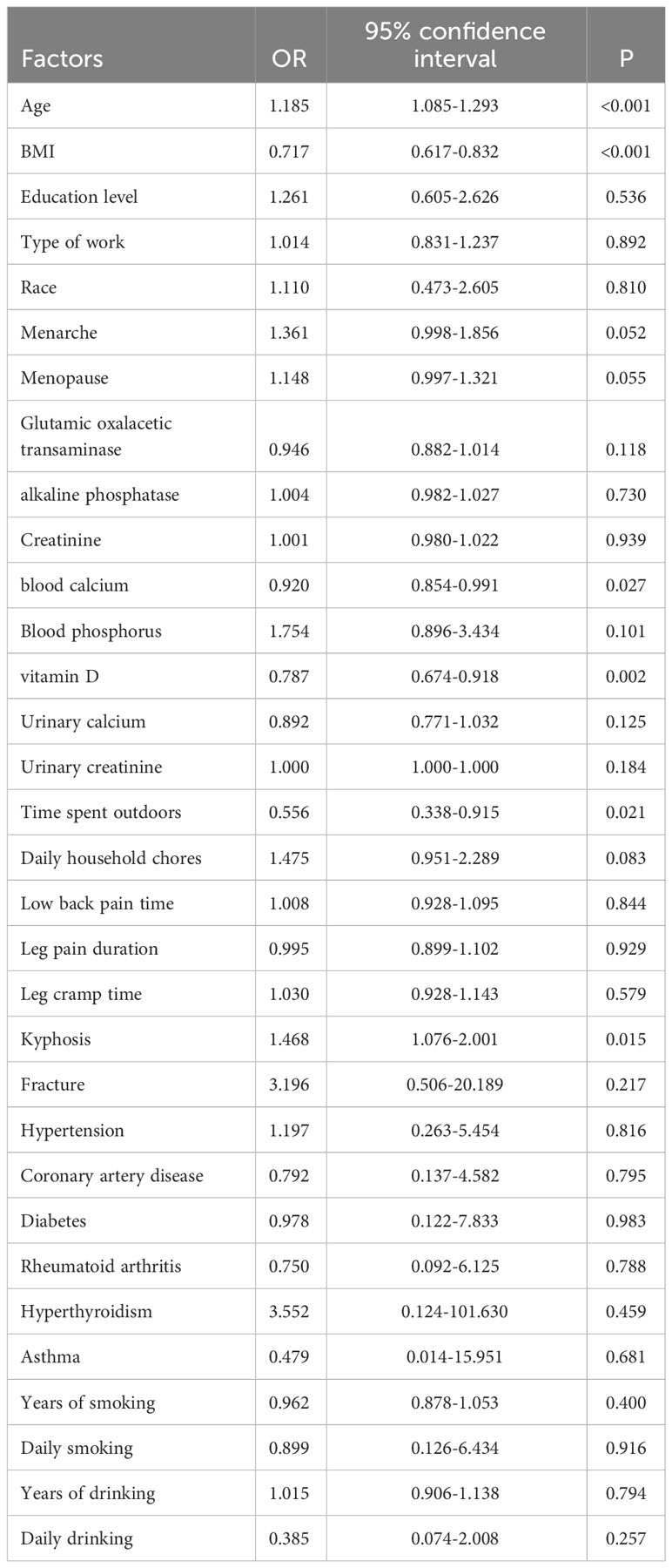
Table 2 Logistic multivariate analysis of different factors and postmenopausal osteoporosis.
In addition, logistic multivariate analysis showed that age (odds ratio [OR]: 1.185, 95% confidence interval [CI]: 1.085–1.293, P<0.001) and kyphosis times (OR: 1.468, 95% CI: 1.076–2.001, P=0.015) was positively correlated with postmenopausal osteoporosis, whereas BMI (OR: 0.717, 95% CI: 0.617–0.832, P<0.001), blood calcium (OR: 0.920, 95% CI: 0.854–0.991, P=0.027), vitamin D (OR: 0.787, 95% CI: 0.674–0.918, P=0.002), and outdoor activity time (OR: 0.556, 95% CI: 0.338–0.915, P=0.021) were negatively correlated with postmenopausal OP (Table 2).
OP and its associated increased risk of fragility fractures are the most disabling consequences of aging in women. Obesity, older age, lower bone density, and 25(OH)D are the main risk factors for hip fractures in postmenopausal women (14, 15); age and fracture history can also predict the risk factors. Moreover, low vitamin D levels also predicted the risk of hip fractures independent of clinical risk factors. The postmenopausal age and fracture incidence are increasing owing to aging populations (16). Hence, interventions to attenuate OP progression and prevent fractures should focus on the older adult population. The present study similarly found a positive association between age (OR: 1.185; 95% CI: 1.085-1.293, P<0.001) and PMOP. In addition, there was a close link between BMI and BMD, confirming the negative relationship between BMD and BMI values; the smaller the BMI, the greater the loss of BMD (15, 17). Another study reported an inverted U-shaped relationship between BMI and lumbar BMD in women and neonates. This finding suggests that increasing BMI may be beneficial for promoting BMD, while an excessively high BMI may be harmful to bone health among women (18). Moreover, BMD values were also associated with BMI in postmenopausal women (19).
The current study found that OP was negatively associated with blood calcium (OR: 0.920, 95% CI: 0.854–0.991, P=0.027) and vitamin D (OR: 0.787, 95% CI: 0.674–0.918, P=0.002) levels in postmenopausal women in Sanya. Dairy products with calcium and vitamin D have a positive effect on bone density in postmenopausal women, and combined supplementation with calcium and vitamin D can prevent osteoporotic hip fractures (20). Plasma calcium plays an important role in the bone remodeling process and can alter the bone structure to meet changing mechanical demands while maintaining bone cell viability and repairing microdamage in the bone matrix (21). Estrogen deficiency leads to many deleterious effects on the bone, including inhibition of osteocyte survival, impairment of osteoblast responses to mechanical stimuli, and repair of aging bone. Reyes-Garcia et al. showed that the daily intake of calcium- and vitamin D-rich milk in healthy postmenopausal women significantly improved vitamin D status, increased femoral neck BMD, and had favorable effects on glucose and lipid profiles (22). Studies have also confirmed that increased serum 25 (OH) D and calcium levels in postmenopausal women can increase skeletal muscle size, strength, balance, and functional task performance while reducing muscle fatigue (23). Furthermore, collagen peptide supplementation enhances the positive effect of calcium and vitamin D supplementation on bone metabolism in postmenopausal women (24).
Menopause is defined as the cessation of menstruation in women, and is associated with ovulatory failure due to oocyte depletion. Menopause is a physiological event that occurs simultaneously with a variety of diseases such as coronary heart disease, stroke, cancer, changes in neuropsychological status and immune function, and bone diseases such as osteopenia and OP. The possible mechanisms underlying the negative association of blood calcium and serum vitamin D levels with OP in postmenopausal women are as follows. First, postmenopausal bone loss may be related to estrogen deficiency and changes in immune status. Postmenopausal OP is a systemic disease characterized by decreased bone mass and increased risk of fractures, mainly due to the significant decrease in estrogen levels after menopause. In addition, the indirect impact of postmenopausal changes in immune status may lead to sustained bone damage, as postmenopausal women typically exhibit a chronic low-grade inflammatory phenotype with changes in both cytokine expression and the immune cell spectrum (25, 26). The second possible mechanism is related to aging. Aging is associated with increased serum parathyroid hormone and alkaline phosphatase levels and decreased serum calcium, phosphorus, and vitamin D metabolites (27). Vitamin D supplementation may improve metabolism in young, postmenopausal, and older adult women. Third, calcium absorption efficiency is an important factor for maintaining calcium balance, which may be related to many cytokines, hormones, growth factors, and reactive oxygen species (24). Fourth, it may be relevant to bone remodeling because of the interference with multiple mechanisms during bone remodeling in the osteoblast and osteoclast lineages. In addition, women with normal bone density and brittle fractures after menopause have lower cortical thickness, and the characteristics of several bone materials in cortical and trabecular mineralized bone tissue are uneven (28).
Patients with postmenopausal OP are prone to serious adverse consequences, such as vertebral compression fractures and thoracolumbar kyphosis (TLK). TLK can cause serious physical, emotional, and economic consequences (29–31). This study found a positive correlation between kyphosis time (OR: 1.468, 95% CI: 1.076–2.001, P=0.015) and postmenopausal OP. A prospective radiological evaluation of the kyphosis index confirmed that high kyphosis is a risk factor for spinal fractures in postmenopausal patients with OP (32). Bernardo et al. also found that older adult women with high kyphosis had a 1.7-fold increased risk of future fractures (33). As the curvature of the chest or waist increases, the local bone density in pre- and postmenopausal women decreases (34). Guo et al. also found that in postmenopausal patients with OP, TLK can occur even without compression fractures and that postmenopausal women are more likely to develop TLK in the future (35).
In addition, outdoor activity duration (OR: 0.556; 95% CI: 0.338–0.915, P=0.021) was associated with PMOP in this study. Age-related bone and muscle losses is associated with physical inactivity and dietary calcium deficiency (36). Studies have suggested that physical activity and muscle strength play a critical role in quality of life, and that physical activity may also reduce the occurrence of sarcopenia (37). Targeted exercise training is the only strategy that can simultaneously improve multiple bone-related and fall-related risk factors. Multiple exercises have a positive impact on bone mass, structure, and strength, and reduce the risk of fractures in postmenopausal women (38). The results of recent studies have emphasized that regular exercise may alleviate postmenopausal symptoms and that even short-term moderate exercise training may significantly reduce these positive effects. Not participating in a supervised high-intensity group exercise program for three months, even with a significant increase in outdoor sports activities, can impact postmenopausal symptoms (39). In addition, research on the influence of high-intensity resistance and impact training (HiRIT) and low-intensity Pilates-based exercise (LiPBE) on the geometric shape of the proximal femur in postmenopausal women has shown that HiRIT can improve the geometric parameters of proximal femoral strength and reduce the risk of hip fracture, whereas LiPBE exercise is largely ineffective (40). Therefore, this implies that the female population with PMOP, particularly the older adults and/or those with severe OP, should be careful when choosing appropriate exercise methods and intensity.
This study is the first to identify risk factors related to fractures and OP in postmenopausal women in Hainan Province, China. As Hainan Province is located in a subtropical region of China, postmenopausal women should make appropriate adjustments based on the strong local sunlight, outdoor work hours, and dietary habits to prevent OP. Epidemiological studies on postmenopausal centenarians and older adult females in Hainan Province have suggested that estrogen is associated with bone resorption and formation (41). Notably, the European postmenopausal guidelines, which state that postmenopausal women should consume 800–1200 mg of calcium and sufficient dietary protein per day. For postmenopausal women with an increased risk of fractures, a daily intake of 800 IU of cholecalciferol is recommended. We further considered supplementing patients with a risk or evidence of vitamin D deficiency, with vitamin D. Regular engagement in weight-bearing exercises based on individual needs and abilities is also recommended (42).
This study has the following limitations. First, it was a cross-sectional study with a limited sample size, and only included participants from a single region. Second, we did not examine the effects of estrogen on postmenopausal OP. Third, a large-sample, multicenter, randomized controlled study is required to confirm the results of this study.
In conclusion, this study found that low BMI, blood calcium and vitamin D levels, kyphosis time, and outdoor activity time were independent risk factors for OP in postmenopausal women. Based on the results of this study, the recommendations for preventing PMOP are as follows. Postmenopausal Chinese women, especially those in Hainan Province, should actively correct hypocalcemia, supplement with vitamin D, and increase their outdoor activity time.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by PLA General Hospital of Hainan Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
GT, TC, and ZF contributed to the design of the study and the review of the literature. LF, YP, and ZG participated in data collection, analysis and drifting of the manuscript. GT and LF are contribute equally to this work. All authors contributed to the article and approved the submitted version.
We thank Professors JM Ba and LL Ye for their hard work during the study. In addition, I would like to express my gratitude to the staff of the Radiology Department of Hainan Hospital of the People’s Liberation Army General Hospital for their support of this project.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Fink HA, MacDonald R, Forte ML, Rosebush CE, Ensrud KE, Schousboe JT, et al. Long-term drug therapy and drug discontinuations and holidays for osteoporosis fracture prevention: a systematic review. Ann Intern Med (2019) 171:37–50. doi: 10.7326/M19-0533
2. Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res (2007) 22:465–75. doi: 10.1359/jbmr.061113
3. US Department of Health and Human Services. Bone Health and Osteoporosis: a Report of the Surgeon General. Available at: https://www.ncbi.nlm.nih.gov/books/NBK45513 (Accessed December 7, 2021).
4. Adachi JD, Loannidis G, Berger C, Joseph L, Papaioannou A, Pickard L, et al. The influence of osteoporotic fractures on health-related quality of life in community-dwelling men and women across Canada. Osteoporos Int (2001) 12:903–8. doi: 10.1007/s001980170017
5. Brown JP, Adachi JD, Schemitsch E, Tarride JE, Brown V, Bell A, et al. Mortality in older adults following a fragility fracture: real-world retrospective matched-cohort study in Ontario. BMC Musculoskelet Disord (2021) 22:105. doi: 10.1186/s12891-021-03960-z
6. Tarride JÉ, Adachi JD, Brown JP, Schemitsch E, Slatkovska L, Burke N. Incremental costs of fragility fractures: a population-based matched -cohort study from Ontario, Canada. Osteoporos Int (2021) 32:1753–61. doi: 10.1007/s00198-021-05877-8
7. Si L, Winzenberg TM, Jiang Q, Chen M, Palmer AJ. Projection of osteoporosis-related fractures and costs in China: 2010–2050. Osteoporos Int (2015) 26:1929–37. doi: 10.1007/s00198-015-3093-2
8. Management of osteoporosis in postmenopausal women: the 2021 position statement of The North American Menopause Society. Menopause (2021) 28(9):973–97. doi: 10.1097/GME.0000000000001831
9. Lewiecki EM. Current and emerging pharmacologic therapies for the management of postmenopausal osteoporosis. J Womens Health (Larchmt) (2009) 18:1615–26. doi: 10.1089/jwh.2008.1086
10. Kanis JA, Cooper C, Rizzoli R, Reginster JY. Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int (2019) 30:3–44. doi: 10.1007/s00198-018-4704-5
11. Kanis JA. Assessing fracture risk and its use in screening for postmenopausal osteoporosis: WHO report. WHO study group. Osteoporos Int (1994) 4:368–81. doi: 10.1007/BF01622200
12. Fitzpatrick LA. Secondary causes of osteoporosis. Mayo Clin Proc (2002) 77:453–68. doi: 10.4065/77.5.453
13. Stein E, Shane E. Secondary osteoporosis. Endocrinol Metab Clin North Am (2003) 32:115–34. doi: 10.1016/s0889-8529(02)00062-2
14. Zhuang HF, Wang PW, Li YZ, Lin JK, Yao XD, Xu H. Analysis of related factors of brittle hip fracture in postmenopausal women with osteoporosis. Orthop Surg (2020) 12:194–8. doi: 10.1111/os.12605
15. Rikkonen T, Sund R, Sirola J, Honkanen R, Poole KES, Kröger H. Obesity is associated with early hip fracture risk in postmenopausal women: a 25-year follow-up. Osteoporos Int (2021) 32:769–77. doi: 10.1007/s00198-020-05665-w
16. Aspray TJ, Hill TR. Osteoporosis and the ageing skeleton. Subcell Biochem (2019) 91:453–76. doi: 10.1007/978-981-13-3681-2_16
17. Jia L, Cheng M. Correlation analysis between risk factors, BMD and serum osteocalcin, CatheK, PINP, β-crosslaps, TRAP, lipid metabolism and BMI in 128 patients with postmenopausal osteoporotic fractures. Eur Rev Med Pharmacol Sci (2022) 26:7955–9. doi: 10.26355/eurrev_202211_30147
18. Li Y. Association between obesity and bone mineral density in middle-aged adults. J Orthop Surg Res (2022) 17:268. doi: 10.1186/s13018-022-03161-x
19. Banack HR, Chang J, Stefanick ML, Arnold M, Anton-Culver H, Jiang L. Relationship between BMI trajectories and cardiometabolic outcomes in postmenopausal women: a growth mixture modeling approach. Ann Epidemiol (2022) 72:9–17. doi: 10.1016/j.annepidem.2022.04.004
20. Liu C, Kuang X, Li K, Guo X, Deng Q, Li D. Effects of combined calcium and vitamin D supplementation on osteoporosis in postmenopausal women: a systematic review and meta-analysis of randomized controlled trials. Food Funct (2020) 11:10817–27. doi: 10.1039/d0fo00787k
21. Hassanein MM, Huri HZ, Baig K, Abduelkarem AR. Determinants and effects of vitamin D supplementation in postmenopausal women: A systematic review. Nutrients (2023) 15:685. doi: 10.3390/nu15030685
22. Reyes-Garcia R, Mendoza N, Palacios S, Salas N, Quesada-Charneco M, Garcia-Martin A, et al. Effects of daily intake of calcium and vitamin D-enriched milk in healthy postmenopausal women: A randomized, controlled, double-blind nutritional study. J Womens Health (Larchmt) (2018) 27:561–8. doi: 10.1089/jwh.2017.6655
23. Hillstrom HJ, Soeters R, Miranda M, Backus SI, Hafer J, Gibbons M, et al. Effect of increased serum 25(OH)D and calcium on structure and function of post-menopausal women: a pilot study. Arch Osteoporos (2020) 15:154. doi: 10.1007/s11657-020-00814-4
24. Argyrou C, Karlafti E, Lampropoulou-Adamidou K, Tournis S, Makris K, Trovas G, et al. Effect of calcium and vitamin D supplementation with and without collagen peptides on bone turnover in postmenopausal women with osteopenia. J Musculoskelet Neuronal Interact (2020) 20:12–7.
25. Ko SH, Kim HS. Menopause-associated lipid metabolic disorders and foods beneficial for postmenopausal women. Nutrients (2020) 12:202. doi: 10.3390/nu12010202
26. Fischer V, Haffner-Luntzer M. Interaction between bone and immune cells: implications for postmenopausal osteoporosis. Semin Cell Dev Biol (2022) 123:14–21. doi: 10.1016/j.semcdb.2021.05.014
27. López-Baena MT, Pérez-Roncero GR, Pérez-López FR, Mezones-Holguín E, Chedraui P. Vitamin D, menopause, and aging: quo vadis? Climacteric (2020) 23:123–9. doi: 10.1080/13697137.2019.1682543
28. Kimmel DB, Vennin S, Desyatova A, Turner JA, Akhter MP, Lappe JM, et al. Bone architecture, bone material properties, and bone turnover in non-osteoporotic post-menopausal women with fragility fracture. Osteoporos Int (2022) 33:1125–36. doi: 10.1007/s00198-022-06308-y
29. Marcus R, Drinkwater B, Dalsky G, Dufek J, Raab D, Slemenda C, et al. Osteoporosis and exercise in women. Med Sci Sports Exerc (1992) 24 Supplement:S301–7. doi: 10.1249/00005768-199206001-00013
30. Hoyt D, Urits I, Orhurhu V, Orhurhu MS, Callan J, Powell J, et al. Current concepts in the management of vertebral compression fractures. Curr Pain Headache Rep (2020) 24:16. doi: 10.1007/s11916-020-00849-9
31. Marchenkova LA, Makarova EV. Exercise therapy and bracing in patients with osteoporotic compression vertebral fractures. Vopr Kurortol Fizioter Lech Fiz Kult (2019) 96:69–75. doi: 10.17116/kurort20199604169
32. Roux C, Fechtenbaum J, Kolta S, Said-Nahal R, Briot K, Benhamou CL. Prospective assessment of thoracic kyphosis in postmenopausal women with osteoporosis. J Bone Miner Res (2010) 25:362–8. doi: 10.1359/jbmr.090727
33. Huang MH, Barrett-Connor E, Greendale GA, Kado DM. Hyperkyphotic posture and risk of future osteoporotic fractures: the Rancho Bernardo Study. J Bone Miner Res (2006) 21:419–23. doi: 10.1359/JBMR.051201
34. Pavlovic A, Nichols DL, Sanborn CF, Dimarco NM. Relationship of thoracic kyphosis and lumbar lordosis to bone mineral density in women. Osteoporos Int (2013) 24:2269–73. doi: 10.1007/s00198-013-2296-7
35. Guo R, Li B, Zeng Z, Jiang X, Zhang D, Xie T, et al. Thoracolumbar kyphosis in postmenopausal osteoporosis patients without vertebral compression fractures. Ann Transl Med (2022) 10:52. doi: 10.21037/atm-21-6285
36. Laudisio A, Giovannini S, Finamore P, Loreti C, Vannetti F, Coraci D, et al. Muscle strength is related to mental and physical quality of life in the oldest old. Arch Gerontol Geriatr (2020) 89:104109. doi: 10.1016/j.archger.2020.104109
37. Giovannini S, Brau F, Forino R, Berti A, D’Ignazio F, Loreti C, et al. Sarcopenia: diagnosis and management, state of the art and contribution of ultrasound. J Clin Med (2021) 10(23):5552. doi: 10.3390/jcm10235552
38. Daly RM, Dalla Via J, Duckham RL, Fraser SF, Helge EW. Exercise for the prevention of osteoporosis in postmenopausal women: an evidence-based guide to the optimal prescription. Braz J Phys Ther (2019) 23:170–80. doi: 10.1016/j.bjpt.2018.11.011
39. Jungmann S, Hettchen M, Kohl M, Kemmler W. Impact of 3 months of detraining after high intensity exercise on menopause-related symptoms in early postmenopausal women – results of the randomized controlled actlife project. Front Sports Act Living (2022) 4:1039754. doi: 10.3389/fspor.2022.1039754
40. Kistler-Fischbacher M, Yong JS, Weeks BK, Beck BR. High-intensity exercise and geometric indices of hip bone strength in postmenopausal women on or off bone medication: the MEDEX-OP randomised controlled trial. Calcif Tissue Int (2022) 111:256–66. doi: 10.1007/s00223-022-00991-z
41. Liu Z, Li Y, Li X, Cheng F, Zhao Y, Hu H. Cross-sectional analysis of gonadal hormone expression and relevant factors in female centenarians in Hainan, China. Zhong Nan Da Xue Xue Bao Yi Xue Ban (2022) 47:45–51. doi: 10.11817/j.issn.1672-7347.2022.210079
42. Kanis JA, Cooper C, Rizzoli R, Reginster JY. Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF). Executive summary of the European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Calcif Tissue Int (2019) 104:235–8. doi: 10.1007/s00223-018-00512-x
Keywords: blood calcium, blood vitamin D, females, kyphosis, outdoor activity time, postmenopausal osteoporosis, osteoporosis
Citation: Tang G, Feng L, Pei Y, Gu Z, Chen T and Feng Z (2023) Low BMI, blood calcium and vitamin D, kyphosis time, and outdoor activity time are independent risk factors for osteoporosis in postmenopausal women. Front. Endocrinol. 14:1154927. doi: 10.3389/fendo.2023.1154927
Received: 31 January 2023; Accepted: 10 October 2023;
Published: 23 October 2023.
Edited by:
Monica Marques Telles, Federal University of São Paulo, BrazilReviewed by:
Kazuhiko Arima, Nagasaki University, JapanCopyright © 2023 Tang, Feng, Pei, Gu, Chen and Feng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tingting Chen, dHQxMzI2NDIyNDgyMkAxNjMuY29t; Zeguo Feng, QmVpamluZ18zMDFAc2luYS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.