
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 23 May 2023
Sec. Diabetes: Molecular Mechanisms
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1152444
This article is part of the Research Topic Organ Crosstalk In the Pathophysiology and Treatment of Type-2 Diabetes View all 6 articles
 Robin Schürfeld1*†‡
Robin Schürfeld1*†‡ Benjamin Sandner1†
Benjamin Sandner1† Annett Hoffmann1,2Nora Klöting3Ekaterine Baratashvili1,4
Annett Hoffmann1,2Nora Klöting3Ekaterine Baratashvili1,4 Marcin Nowicki5
Marcin Nowicki5 Sabine Paeschke5Joanna Kosacka6Susan Kralisch1Anette Bachmann1
Sabine Paeschke5Joanna Kosacka6Susan Kralisch1Anette Bachmann1 Armin Frille7Anja Dietel8Jens-Uwe Stolzenburg8
Armin Frille7Anja Dietel8Jens-Uwe Stolzenburg8 Matthias Blüher1,3
Matthias Blüher1,3 Ming-Zhi Zhang9,10Raymond C. Harris9,10
Ming-Zhi Zhang9,10Raymond C. Harris9,10 Berend Isermann11Michael Stumvoll1
Berend Isermann11Michael Stumvoll1 Anke Tönjes1†
Anke Tönjes1† Thomas Ebert1†‡
Thomas Ebert1†‡Objective: Acyl-CoA-binding protein (ACBP)/diazepam-binding inhibitor has lately been described as an endocrine factor affecting food intake and lipid metabolism. ACBP is dysregulated in catabolic/malnutrition states like sepsis or systemic inflammation. However, regulation of ACBP has not been investigated in conditions with impaired kidney function, so far.
Design/methods: Serum ACBP concentrations were investigated by enzyme-linked immunosorbent assay i) in a cohort of 60 individuals with kidney failure (KF) on chronic haemodialysis and compared to 60 individuals with a preserved kidney function; and ii) in a human model of acute kidney dysfunction (AKD). In addition, mACBP mRNA expression was assessed in two CKD mouse models and in two distinct groups of non-CKD mice. Further, mRNA expression of mACBP was measured in vitro in isolated, differentiated mouse adipocytes - brown and white - after exposure to the uremic agent indoxyl sulfate.
Results: Median [interquartile range] serum ACBP was almost 20-fold increased in KF (514.0 [339.3] µg/l) compared to subjects without KF (26.1 [39.1] µg/l) (p<0.001). eGFR was the most important, inverse predictor of circulating ACBP in multivariate analysis (standardized β=-0.839; p<0.001). Furthermore, AKD increased ACBP concentrations almost 3-fold (p<0.001). Increased ACBP levels were not caused by augmented mACBP mRNA expression in different tissues of CKD mice in vivo or in indoxyl sulfate-treated adipocytes in vitro.
Conclusions: Circulating ACBP inversely associates with renal function, most likely through renal retention of the cytokine. Future studies need to investigate ACBP physiology in malnutrition-related disease states, such as CKD, and to adjust for markers of renal function.
Chronic kidney disease (CKD) has a leading global health impact and is a multisystem disease state accounting for about 1.2 million deaths per year worldwide (1). Key pathomechanisms include a proinflammatory status, increased oxidative stress and cellular senescence (2, 3), thereby contributing to increased mortality with about 40-50% of deaths attributed to cardiovascular diseases (4). Cardiometabolic disease states frequently observed in patients with CKD and kidney failure (KF) include diabetes (5, 6), dyslipidemia (7) and a proinflammatory phenotype. Therefore, potential endocrine cytokines linking cardiometabolic diseases with impaired renal function need to be investigated.
Recently, acyl-CoA binding protein (ACBP), also called diazepam binding inhibitor, has been introduced as an endocrine factor affecting food intake and lipid metabolism (8). ACBP is ubiquitously expressed throughout the body with highest levels observed in human liver, brain, kidney and gut (9). Bravo-San Pedro and co-workers demonstrated that intravenous injection of recombinant ACBP in mice enhances food intake, while lowering glucose levels. Furthermore, it activates lateral hypothalamic orexigenic neurons and increases lipogenic gene expression, e.g. fatty acid synthase in hepatocytes and white adipocytes (8). Conversely, ACBP-neutralizing antibodies induced hyperglycemia, hypophagia, and weight loss in mice (8). In accordance, a systemic knockout of the ACBP gene results in less weight gain following a high-fat diet in adult mice (10) and are more sensitive to fasting-induced weight loss (8). ACBP has also been reported to positively correlate with BMI in human studies supporting its role as an obesogenic factor (8, 11, 12). Importantly, conditions of severe catabolic states like sepsis or systemic inflammation are correlated to increased plasma ACBP levels (13, 14). As malnutrition and sarcopenia frequently occur in patients with advanced CKD and KF (2), the regulation of circulating ACBP in patients with CKD and KF needs to be investigated in more detail. Therefore, we quantified plasma ACBP concentrations in 60 individuals with KF on maintenance haemodialysis (HD) treatment and compared it to 60 individuals with an estimated glomerular filtration rate (eGFR) > 50 ml/min/1.73m². In addition, we measured ACBP in 20 patients with acute kidney dysfunction (AKD) after unilateral nephrectomy. Furthermore, we examined mACBP mRNA expression in two CKD mouse models due to diabetic kidney disease (i.e. eNOS-/-;db/db mice and db/db mice on a C57BLKS/J background) in relation to two mouse models without CKD (i.e. heterozygous db/+ mice and eNOS-/- mice). Finally, we determined mRNA expression of mACBP in cultured, differentiated murine brown and white fat cells after exposure to the uremic toxin indoxyl sulfate versus control treatment. Our main hypothesis was that ACBP is eliminated by the kidneys and hence ACBP is increased in i) CKD patients with HD treatment and ii) in patients with AKD.
For the investigation of ACBP regulation in human CKD, a cross-sectional study previously described in (15, 16) was used. The following inclusion criteria were required to participate in the study: age >18 years, non-pregnant, provided written informed consent. Patients were excluded if they had end-stage malignancy, acute generalized inflammation, acute infectious disease or a history of drug abuse. For the current analysis, 120 Caucasian participants (women: N = 58; men: N = 62) were available. Of the total cohort (N=120), about 60 (50%) patients had a kidney failure (KF) and were on maintenance HD. In study population 1, blood samples were obtained after an overnight fast of at least 8 hours. In all KF patients, blood draw was executed immediately before the start of HD. In a subgroup of 10 patients with KF (5 with type 2 diabetes (T2D) and 5 without T2D), serum ACBP concentrations were measured before and immediately after HD. Study participants with a preserved eGFR > 50 ml/min/1.73m² (N = 60) defined by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula (17) were used as control subjects. In all women and men, fasting glucose (FG) ≥ 7.0 mmol/l or use of insulin or other glucose-lowering medication was classified as type 2 diabetes (T2D) (18). Based on these criteria, 32 of the 60 patients with KF on maintenance HD and 30 out of 60 control patients were classified as T2D. The study was approved by the Ethics Committee of the University of Leipzig (Reg. No: 180-13-15072013), and written informed consent was obtained from all volunteers prior to their participation in the study.
To investigate ACBP in a human model of AKD, a second study population of patients undergoing elective partial or total unilateral nephrectomy was used, as previously described (19, 20). Former studies already established that these patients serve as a reliable model for AKD (21, 22). Inclusion criteria were an age between 18 and 80 years and provided written informed consent, whereas patients were excluded for the following criteria: presence of hemodialysis therapy, hereditary renal cysts, glomerulonephritis, and generalized inflammation. In brief, 61 consecutively recruited patients (17 women, 44 men) received elective partial or total unilateral nephrectomy at the Department of Urology of Leipzig University Hospital. In all patients, fasting blood samples were drawn before, as well as within 30 hours after, renal surgery. For the present analysis, 20 subjects were available. The study was approved by the Ethics Committee of the University of Leipzig (Reg. No: 029-12-23012012), and written informed consent was obtained from all volunteers prior to their participation in the study.
Serum levels of ACBP (DBI Human enzyme-linked immunosorbent assay (ELISA) Kit, #KA0532, Abnova, Taipeh, Taiwan) as well as high sensitivity interleukin 6 (hsIL6, #HS600B, R&D Systems, Wiesbaden, Germany) were measured using an ELISA according to the manufacturers’ instructions. Routine serum parameters, including creatinine, FG, fasting insulin (FI), triglycerides (TG), high density lipoprotein (HDL), low density lipoprotein (LDL) cholesterol, and C-reactive protein (CRP) were measured in a certified laboratory by standard methods. Using FG and FI, homeostasis model assessment of insulin resistance (HOMA2-IR) was determined as previously described (23).
To investigate tissue-specific ACBP regulation in CKD, two mice models of CKD caused by diabetic kidney disease (DKD) (eNOS-/-;db/db mice (i.e. mice with severe DKD (24) and db/db mice (i.e. mice with mild DKD (25)) were compared to two non-diabetic control groups (non-diabetic eNOS-/-mice, as well as db/+ mice (26)). All stated mice were on a C57BLKS/J background. All mice were kept under pathogen-free conditions at 21 ± 1°C on a 12-hour light/dark cycle (6 AM to 6 PM) and received free access to water and a normal chow pellet diet. At 24 weeks of age, mice were sacrificed by exsanguination while maintainingdeep anesthesia with intravenous ketamine (WDT, Garbsen, Germany) and xylazine (Bayer Health Care, Wuppertal, Germany). For later RNA isolation, biopsies of liver, kidney, visceral (VAT), subcutaneous (SAT), and brown (BAT) adipose tissue, as well as hypothalamus, were shock frozen in liquid nitrogen. Location of all animal experiments was the Medical Experimental Center at the University of Leipzig with previously described methods (26–28). The local ethics committee of the state of Saxony (Landesdirektion Leipzig) permitted all animal experiments (approval nos. TVV 12/14 and TVV 65/15).
Immortalized murine brown preadipocytes were cultured according to (29) In brief, selected preadipocytes were grown to confluence in culture medium supplemented with differentiation medium. After confluence, cells were incubated in differentiation medium supplemented with induction medium. Subsequently, the cells were maintained only in differentiation medium for 4–5 days until exhibiting a fully differentiated phenotype. Murine 3T3-L1 white preadipocytes (American Type Culture Collection, Rockville, MD) were also grown to confluence in culture medium. Confluent cells were then differentiated to adipocytes by supplementation of culture medium with insulin, isobutylmethylxanthine, and dexamethasone as outlined in (30). Using the methods of Stockler-Pinto et al. (31), as well as Gondouin et al. (32), after starvation for a period of 24 hours, brown and white adipocytes were incubated with 1 mM indoxyl sulfate for 24 hours. For controls, cells were also exposed for 24 hours to 1 mM potassium sulfate (Sigma, Darmstadt, Germany) according to the recommendations of the European Uremic Toxin Work Group (EUTox) (33). Both, indoxyl sulfate and potassium sulfate, were diluted in NaCl 0.9%.
mACBP mRNA expression was determined relative to acidic ribosomal phosphoprotein P0 (m36B4) using quantitative real-time RT-PCR. This includes all animal and in vitro-experiments. In more detail, 1 µg total RNA was obtained from each sample and reverse transcribed in a 20 µl reverse transcription reaction. 1 µl of each reverse transcription reaction, producing cDNA, was used on a LightCycler 480 real-time PCR 96 well thermocycler using LightCycler 480 Probes Master Mix (Roche Diagnostics GmbH, Mannheim, Germany) essentially as described in (26, 34). Primer pairs with the following sequence were used: mACBP, TTTCGGCATCCGTATCACCT (sense) and TTTGTCAAATTCAGCCTGAGACA (antisense); m36B4, AAGCGCGTCCTGGCATTGTCT (sense) and CCGCAGGGGCAGCAGTGGT (antisense).
SPSS software version 27.0 (IBM, Armonk, NY) and GraphPad Prism 9 (GraphPad Software Inc., La Jolla, CA) were used for all statistical analyses. In study population 1, overall group differences between the four subgroups were assessed by non-parametric Kruskal-Wallis test with Bonferroni post hoc analysis for continuous parameters, whereas χ²-test was used for categorical parameters. To conduct univariate correlation analyses, we used Spearman’s rank correlation methods. To identify independent associations between ACBP and cardiometabolic and anthropometric markers, linear regression analysis was calculated. For this purpose, parameters that correlated significantly with ACBP in univariate analysis (except for covariates) were included in the multivariate model with further adjustment for sex. Prior to carrying out multivariate linear regression analysis, all non-normally distributed parameters were logarithmically transformed.
For analysis of paired samples in study population 1 (i.e. before vs. after hemodialysis in a subset) and in study population 2 (i.e. before vs. after unilateral nephrectomy), Wilcoxon signed-rank test was used.
In the animal and in vitro experiments, relative mACBP mRNA expression in different mouse tissues and adipocytes were analyzed by one-way ANOVA with Bonferroni post hoc tests, as well as by Student’s t test, after logarithmical transformation prior the analyses.
A p-value of <0.05 was considered as statistically significant in all analyses.
Study population 1 was subdivided into the four described subgroups (i.e. Control/nonT2D; Control/T2D; HD/nonT2D; HD/T2D). Basic clinical characteristics of each group are displayed in Table 1. Median [interquartile range] serum ACBP levels were 109.7 [488.6] µg/l in the total sample and did not depend on sex (p = 0.472) and T2D (p = 0.610). In contrast, patients with KF (514.0 [339.3] µg/l) had significantly, almost 20-fold, higher serum concentrations of ACBP as compared to subjects with a preserved renal function (26.1 [39.1] µg/l) (p < 0.001). In the subgroup of 10 patients with ACBP levels before and after HD, serum ACBP level were decreased from 772.7 [297.1] (before HD) to 581.4 [205.6] µg/l (after HD) (Figure 1A, p < 0.01).
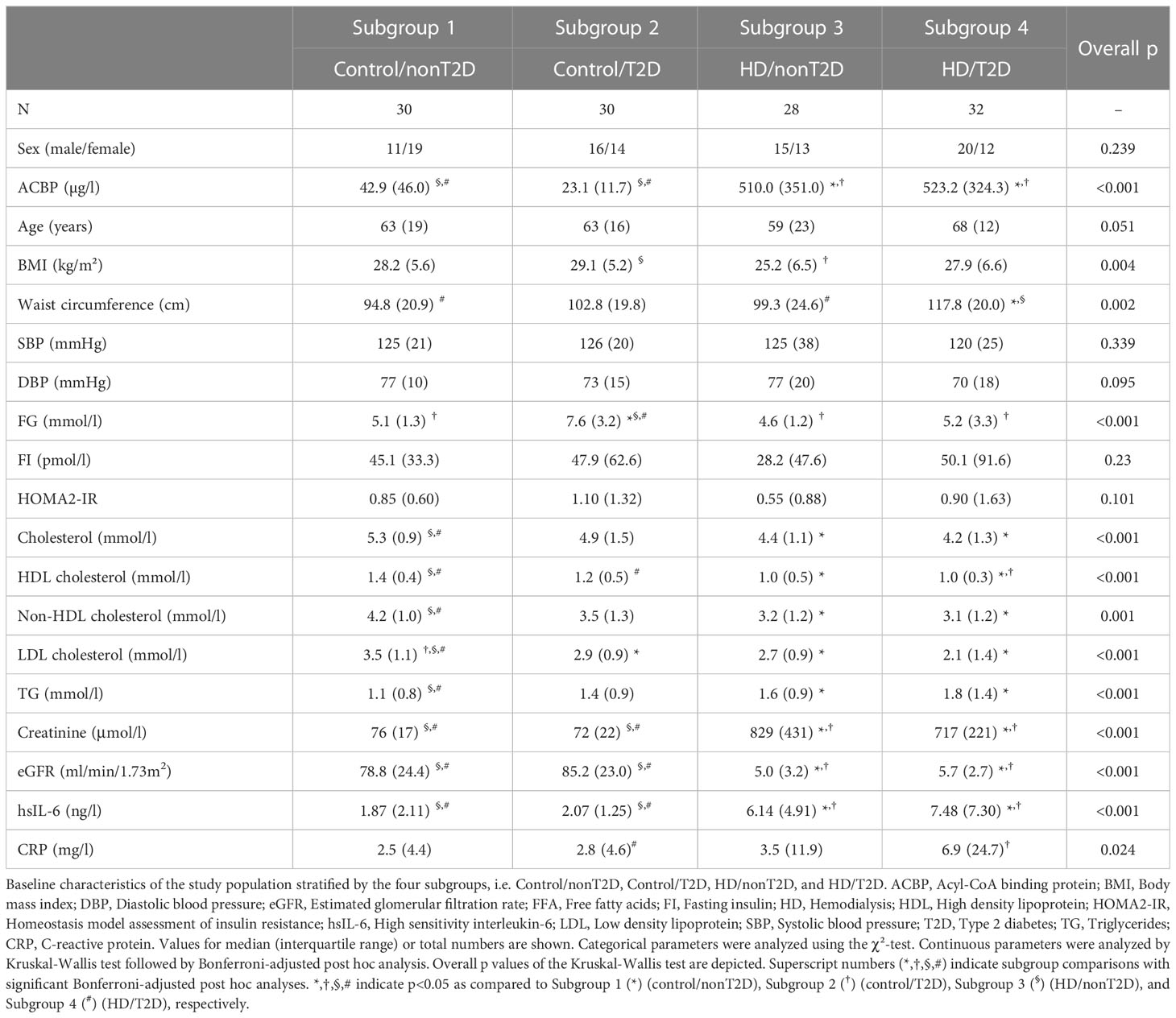
Table 1 Baseline characteristics of the study population.
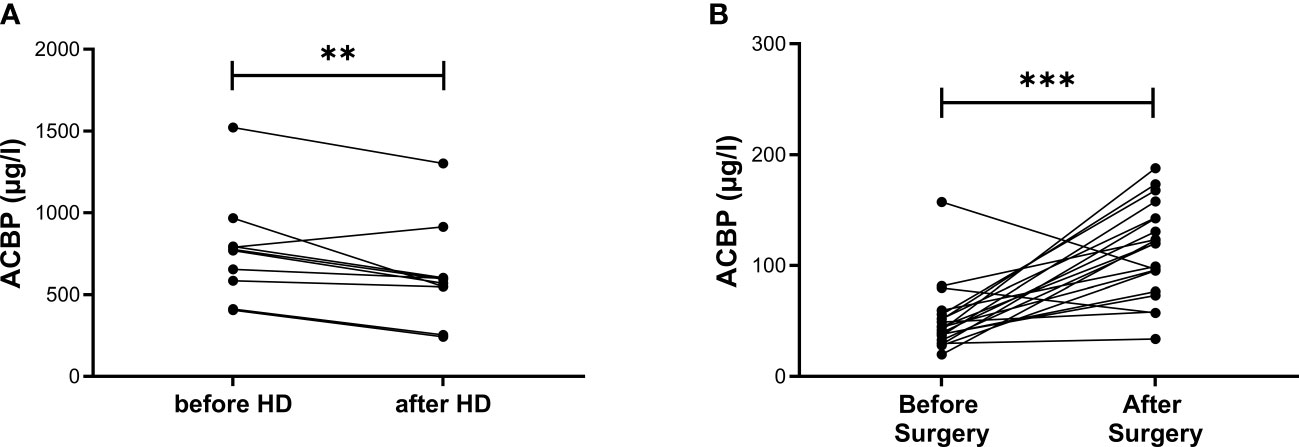
Figure 1 ACBP serum concentrations before and after HD as well as before and after unilateral nephrectomy in matched samples of patients. ACBP serum concentrations were measured before and immediately after hemodialysis (HD) in 10 subjects from study population 1 in (A) and before, as well as within 30 hours after, partial or total unilateral nephrectomy in 20 subjects from study population 2 in (B). Each data point refers to one patient. P-values were calculated by Wilcoxon signed-rank test. ** indicates p < 0.01, ***p < 0.001.
When patients were stratified by the four subgroups, i.e. Control/nonT2D; Control/T2D; HD/nonT2D; HD/T2D, circulating ACBP differed significantly between the four subgroups (p < 0.001) and the HD subgroups had significantly higher ACBP concentrations compared to both non-HD subgroups (Table 1).
Analysing all 120 individuals, ACBP serum levels were positively correlated to age, WHR, TG, creatinine, hsIL-6, and CRP (all p < 0.05; Table 2). Furthermore, ACBP was negatively related to BMI, FG, cholesterol, HDL cholesterol, non-HDL cholesterol, LDL cholesterol, and eGFR (all p < 0.05; Table 2).
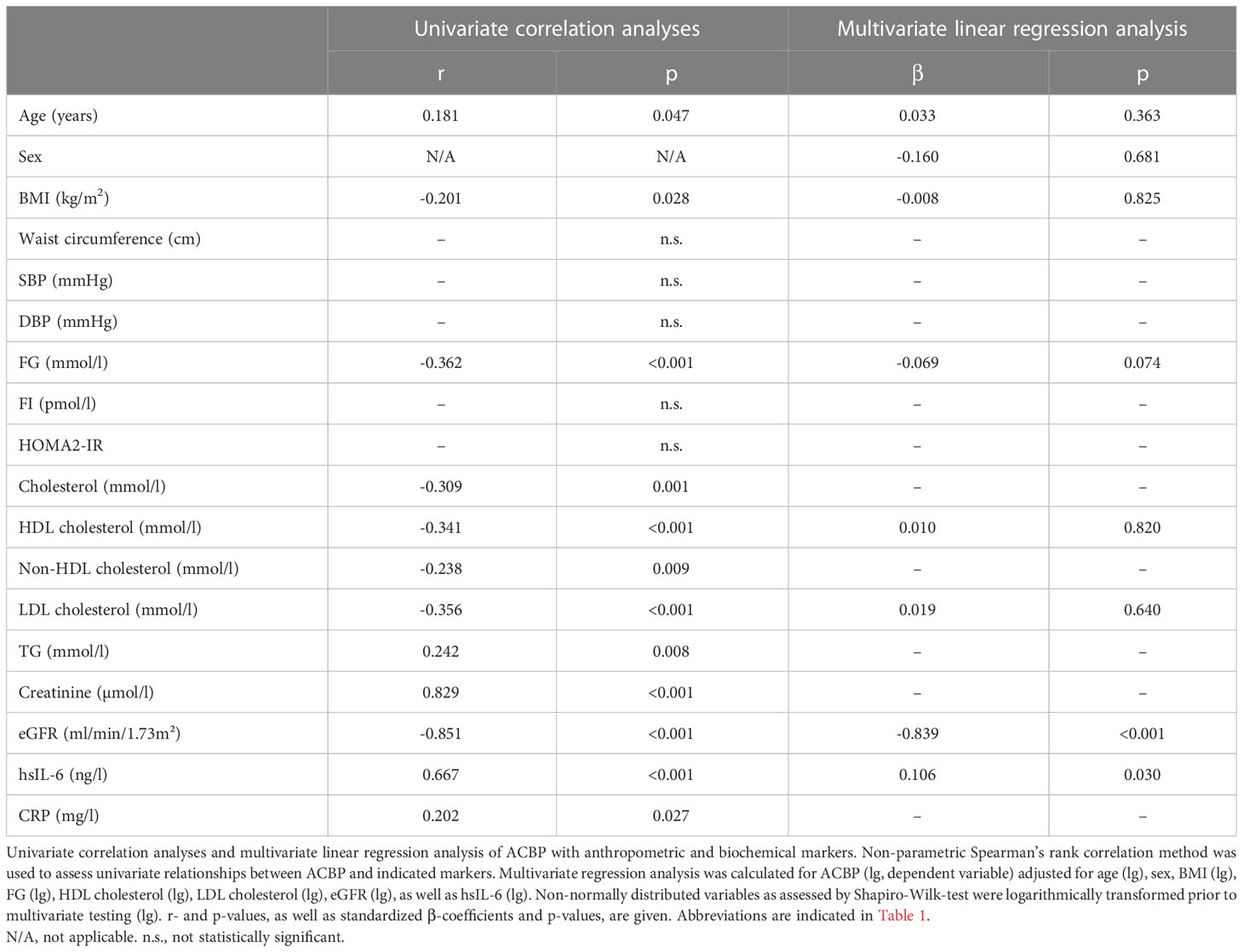
Table 2 Univariate correlation analyses and multivariate linear regression analysis of serum ACBP with anthropometric parameters and markers of glucose metabolism, serum lipids, inflammation, and renal function.
Again, analysing all 120 individuals, eGFR was the most relevant, significant, and negative predictor of ACBP levels (p < 0.001; Table 2) after adjustment for age, sex, and cardiometabolic markers in linear regression analysis. Furthermore, hsIL-6 positively associated with circulating ACBP (p = 0.030; Table 2). On the other hand, ACBP was not independently associated with markers of obesity, glucose homeostasis, and dyslipidemia in multivariate linear regression analysis in the entire cohort (Table 2) nor with CRP when included instead of hsIL-6 (Supplementary Table S1, Model 2).
Baseline characteristics, as well as pre- and postsurgery biochemical parameters, have already been described elsewhere (28). Median serum concentrations of ACBP were significantly, almost 3-fold, higher after surgery (120.0 [52.1] µg/l) compared to before surgery (43.2 [17.1] µg/l) (Figure 1B, p < 0.001).
Figure 2 depicts tissue-specific mACBP mRNA expression in insulin-sensitive tissues (i.e. liver and adipose tissue depots), as well as kidney and hypothalamus, in four groups of mice with different renal function, i.e. healthy, lean db/+ mice vs. endothelial dysfunctional eNOS-/- mice vs. obese, diabetic db/db mice with mild DKD vs. obese, diabetic eNOS-/-;db/db mice with severe DKD.

Figure 2 mACBP mRNA expression in a mouse model of diabetic kidney disease compared to control mice. In all experiments, mice with 24 weeks of age with severe diabetic kidney disease (DKD) (eNOS-/-; db/db; black bars) were compared to obese, diabetic (db/db; dark grey bars), lean, endothelial dysfunctional (eNOS-/- mice; light grey bars), as well as healthy, lean control mice (db/+ mice; white bars). (A–F) mACBP mRNA expression normalized to m36B4 in (A) brown adipose tissue (BAT), (B) subcutaneous adipose tissue (SAT), (C) visceral adipose tissue (VAT), (D) kidney, (E) liver, and (F) hypothalamus. Results are displayed as means ± standard deviation. p-values were calculated by one-way ANOVA including Bonferroni adjustment for post-hoc tests. N ≥ 5 per group. *indicates p < 0.05, **p < 0.01, ****p<0.0001 for subgroup comparisons.
In BAT, mACBP mRNA expression was significantly decreased in 24-week-old CKD mice. We detected thelowest mACBP expression in mice with severe DKD, i.e. eNOS-/-;db/db (Figure 2A, overall p < 0.001). In contrast, mACBP mRNA expression did not differ between the animal groups in SAT, VAT, kidney, liver, and hypothalamus (Figures 2B–F, all p > 0.05).
To investigate whether uremic toxins contribute to an altered mACBP mRNA expression in adipocytes in vitro, murine 3T3-L1 white adipocytes, as well as brown adipocytes, were treated with the major uremic toxin indoxyl sulfate for 24 hours compared to potassium sulfate. Mean mACBP mRNA expression was non-significantly altered after indoxyl sulfate treatment compared to control cells in 3T3-L1 white adipocytes (Figure 3A, p = 0.667) and brown adipocytes (Figure 3B, p = 0.111).
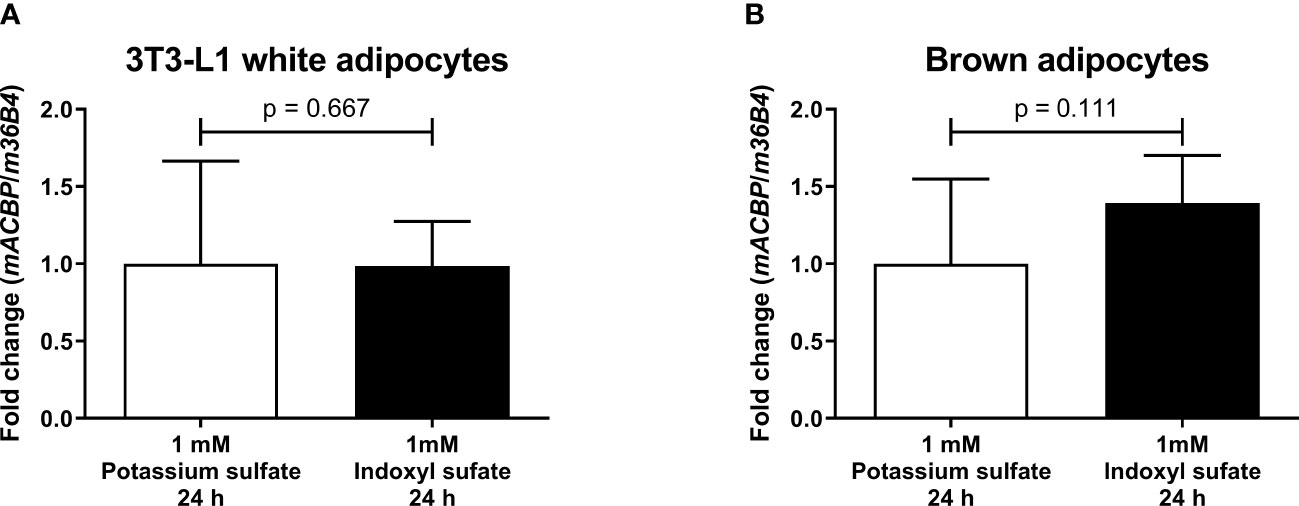
Figure 3 mACBP mRNA expression after treatment in 3T3-L1 white adipocytes and brown adipocytes with uremic toxin indoxyl sulfate. mACBP mRNA expression in (A) murine 3T3-L1 white adipocytes, and (B) differentiated, immortalized murine brown adipocytes after 24 hours-lasting incubation with 1 mM indoxyl sulfate and control cells exposed to 1 mM potassium sulfate for 24 hours. The mACBP mRNA expression is shown as normalized to m36B4. Results are displayed as means ± standard deviation. p-values were calculated by Student’s t test. N ≥ 5 per group.
Here we show, that ACBP is significantly, almost 20-fold, increased in patients with KF receiving HD treatment as compared to control subjects, and almost 3-fold increased in patients with AKD after unilateral nephrectomy compared to presurgical concentrations. Furthermore, eGFR, as well as hsIL-6, are independently associated with circulating ACBP concentrations in patients with KF.
Similar to ACBP, several other cytokines with cardiometabolic effects are also significantly elevated in KF, including leptin (35), adiponectin (36), adipocyte fatty acid-binding protein (19), and follistatin-like 3 (28). To investigate whether increased ACBP levels in CKD could be due to enhanced ACBP protein synthesis in various tissues, we analyzed mACBP mRNA expression in two CKD mouse models as compared to two distinct non-diabetic control mouse models. mACBP mRNA expression is downregulated in brown adipocytes in CKD mice, whereas gene expression of the cytokine in other tissues is not different between CKD and non-CKD mice. Furthermore, mRNA expression of mACBP is not modified by the uremic toxin indoxyl sulfate in adipocytes in vitro. Based on these results, increased ACBP serum levels in KF are not caused by augmented mRNA expression of the cytokine in the uremic milieu (i.e. similar to adiponectin (36)), but rather by decreased kidney function leading to subsequent retention of ACBP. In agreement with this rationale and with the findings in KF, ACBP levels are increased after unilateral nephrectomy in a human AKD model, as well. While HD treatment can partially remove ACBP from the circulation (Figure 1A), ACBP concentrations remain to be significantly elevated after HD treatment compared to controls indicating only a small effect of HD on ACBP levels. Our results appear to be independent of the cause of KF, and ACBP concentrations do not differ in KF due to DKD vs. other diseases. It should be noted that ACBP has been negatively related to eGFR in the French general population-based DESIR study, in a French advanced cancer cohort and in 63 randomly selected patients undergoing a short-term weight loss program (12, 37). Importantly, mean eGFR was 85.3 ml/min/1.73m² in the DESIR study (12), and therefore, these cohorts (12, 37), are not applicable to investigate ACBP regulation in patients with CKD in more detail.
Interestingly, ACBP is not independently associated with BMI in multivariate analysis in our cohort, while several other studies have shown a positive association of BMI and ACBP (8, 11, 12, 37, 38). However, patients from all of these studies have not been specifically selected for CKD, and in several cohorts even been excluded in the presence of advanced CKD/KF (8, 11, 12, 37, 38). Furthermore, the association of ACBP with BMI is lost in cancer patients and patients with cardiovascular diseases (12), and cancer patients with malnutrition even show an inverse correlation of ACBP with BMI (37). Malnutrition and sarcopenia are also common in CKD (2) and hence may contribute to increased ACBP levels, hypothetically partly through autophagy, which causes ACBP release to extracellular space (8, 39). It is, therefore tempting to speculate that in healthier conditions ACBP levels are positively related to BMI, whereas this relationship is lost or even reversed in individuals with CVD and malnutrition-related diseases, e.g. cancer and KF. Future studies, therefore, need to elucidate whether impaired ACBP regulation in these disease states is causally involved in malnutrition and impaired body composition status, thereby contributing to CVD.
Apart from markers of renal function, CRP and hsIL-6 are positively correlated with ACBP levels in the univariate analysis of study population 1, with hsIL-6 furthermore being independently correlated in the multivariate analysis. This is probably due to the higher sensitivity of IL-6 for chronic inflammation. Interestingly, ACBP’s cleavage peptide ODN enhances LPS-stimulated IL-6 secretion of human monocytes (40), as well as ROS production in human neutrophils (41), in vitro. Furthermore, ACBP levels are increased in a rat model of sepsis (13) and conversely, ACBP-neutralizing antibodies inhibit proinflammatory pathways and profibrotic genes, while upregulating antioxidant resources in mice (42, 43). This implicates that ACBP is involved in pro-inflammatory pathways, but future studies need to determine whether the cytokine contributes to systemic inflammation or is driven by it.
In the univariate correlation analyses, ACBP was associated with a dyslipidemic profile. These results are in line with a meta-analysis by Joseph et al. demonstrating a positive association of ACBP levels with TG (37). Furthermore, Montegut and co-workers have validated these findings observing not only a positive correlation between ACBP and TG, but also a negative correlation between HDL cholesterol and ACBP, independent of age and BMI (12), supporting our findings in patients with impaired renal function.
Some limitation of the current study need to be pointed out. First, ACBP is known to be associated with short- and long-term caloric ingestion (37), so correlation of caloric intake with ACBP levels would be informative, but was lacking in our cohort. Second, possible pre- to post surgery differences, for instance increased CRP after surgery and/or a prolonged fasting state (37) during the perioperative period, could have influenced ACBP levels in study population 2. Third, only mRNA expression levels for mACBP were used to account for possible changes in ACBP serum levels, while protein expression data either by western blot or by immunohistochemistry could reflect circulating ACBP more accurate. Last, the number of animals used in our experiments may have been too low to identify potential differences in mRNA expression of mACBP.
In conclusion, ACBP plasma concentrations are almost 20-fold higher in patients with KF on HD treatment as compared to control subjects and almost 3-fold higher in a human model of AKD. As mACBP mRNA expression is not increased in the uremic milieu, circulating ACBP is most likely increased in CKD due to retention. Therefore, markers of renal function need to be reported in future studies on ACBP. Future studies should focus on the interplay of malnutrition, inflammation and impaired renal function, which all influence ACBP concentrations and are to be encountered in CKD patients. Whether an anti-ACBP therapy may reduce inflammation, remains to be investigated.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the University of Leipzig. The patients/participants provided their written informed consent to participate in this study. The animal study was reviewed and approved by Local ethics committee of the state of Saxony (Landesdirektion Leipzig).
RS, BS, AT, and TE wrote the manuscript and researched data. AH, NK, EB, MN, SP, SK and AB researched data and reviewed/edited the manuscript. MB, M-ZZ, RCH, BI, AF, AD, J-US, and MS contributed to the discussion and reviewed/edited the manuscript. Guarantor: RS and TE are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors contributed to the article and approved the submitted version.
This work was funded by the German Research Foundation (Deutsche Forschungsgemeinschaft, DFG) – through SFB 1052, project number 209933838, CRC 1052/3, subprojects C6 (AT), B1 (MB), B4 (NK), and A1 (MS). RS was supported by a travel grant for the Diabetes congress 2023 by the German diabetes Association (DDG). TE was supported by a Novo Nordisk postdoctoral fellowship run in partnership with Karolinska Institutet, Stockholm, Sweden, a Karolinska Institutet Research Foundation grant, the Stiftelsen Stig och Gunborg Westman, the Swedish Kidney Foundation (Njurfonden), and the German Diabetes Association (DDG). TE was further funded through the EFSD Mentorship Programme supported by AstraZeneca. This work was additionally supported by a grant of the Deutsche Diabetes Gesellschaft to MB and MN (DDG 934300-002), as well as to AH (“Projektpreis der AG Diabetes und Niere 2020”). MB received honoraria as a consultant and speaker from Amgen, AstraZeneca, Bayer, Boehringer-Ingelheim, Lilly, Novo Nordisk, Novartis, Pfizer and Sanofi. AF was supported by the postdoctoral fellowship “MetaRot program” from the Federal Ministry of Education and Research (BMBF), Germany (FKZ 01EO1501, IFB Adiposity Diseases), a research grant from the Mitteldeutsche Gesellschaft für Pneumologie (MDGP) e.V. (2018-MDGP-PA-002), a junior research grant from the Medical Faculty, University of Leipzig (934100-012), and the PETictCAC” project (ERAPerMed_324), which was funded with tax funds on the basis of the budget passed by the Saxon State Parliament (Germany) under the frame of ERA PerMed (Horizon 2020). All mentioned funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
The authors acknowledge support from the Open Access Publishing Fund of Leipzig University supported by the German Research Foundation (DFG) within the program of Open Access Publication Funding.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1152444/full#supplementary-material
1. Bikbov B, Purcell C, Levey A, Smith M, Abdoli A, Abebe M, et al. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet (2020) 395(10225):709–33. doi: 10.1016/S0140-6736(20)30045-3
2. Ebert T, Neytchev O, Witasp A, Kublickiene K, Stenvinkel P, Shiels PG. Inflammation and oxidative stress in chronic kidney disease and dialysis patients. Antioxid Redox Signal (2021) 35(17):1426–48. doi: 10.1089/ars.2020.8184
3. Ebert T, Tran N, Schurgers L, Stenvinkel P, Shiels PG. Ageing - oxidative stress, ptms and disease. Mol Aspects Med (2022) 86:101099. doi: 10.1016/j.mam.2022.101099
4. Jankowski J, Floege J, Fliser D, Bohm M, Marx N. Cardiovascular disease in chronic kidney disease: pathophysiological insights and therapeutic options. Circulation (2021) 143(11):1157–72. doi: 10.1161/CIRCULATIONAHA.120.050686
5. Saran R, Robinson B, Abbott KC, Bragg-Gresham J, Chen X, Gipson D. US renal data system 2019 annual data report: epidemiology of kidney disease in the united states. Am J Kidney Dis (2019) 75(1). doi: 10.1053/j.ajkd.2019.09.002
6. Al-Ghamdi SMG, Bieber B, AlRukhaimi M, AlSahow A, Al Salmi I, Al Ali F, et al. Diabetes prevalence, treatment, control, and outcomes among hemodialysis patients in the gulf cooperation council countries. Kidney Int Rep (2022) 7(5):1093–102. doi: 10.1016/j.ekir.2022.02.012
7. Noels H, Lehrke M, Vanholder R, Jankowski J. Lipoproteins and fatty acids in chronic kidney disease: molecular and metabolic alterations. Nat Rev Nephrol (2021) 17(8):528–42. doi: 10.1038/s41581-021-00423-5
8. Bravo-San Pedro JM, Sica V, Martins I, Pol J, Loos F, Maiuri MC, et al. Acyl-Coa-Binding protein is a lipogenic factor that triggers food intake and obesity. Cell Metab (2019) 30(6):1171. doi: 10.1016/j.cmet.2019.10.011
9. Ball JA, Ghatei MA, Sekiya K, Krausz T, Bloom SR. Diazepam binding inhibitor-like Immunoreactivity(51-70): distribution in human brain, spinal cord and peripheral tissues. Brain Res (1989) 479(2):300–5. doi: 10.1016/0006-8993(89)91632-6
10. Neess D, Kruse V, Marcher AB, Waede MR, Vistisen J, Moller PM, et al. Epidermal acyl-Coa-Binding protein is indispensable for systemic energy homeostasis. Mol Metab (2021) 44:101144. doi: 10.1016/j.molmet.2020.101144
11. Joseph A, Moriceau S, Sica V, Anagnostopoulos G, Pol J, Martins I, et al. Metabolic and psychiatric effects of acyl coenzyme a binding protein (Acbp)/Diazepam binding inhibitor (Dbi). Cell Death Dis (2020) 11(7):502. doi: 10.1038/s41419-020-2716-5
12. Montegut L, Joseph A, Chen H, Abdellatif M, Ruckenstuhl C, Motino O, et al. High plasma concentrations of acyl-coenzyme a binding protein (Acbp) predispose to cardiovascular disease: evidence for a phylogenetically conserved proaging function of acbp. Aging Cell (2022) 22(1):e13751. doi: 10.1111/acel.13751
13. Clavier T, Besnier E, Lefevre-Scelles A, Lanfray D, Masmoudi O, Pelletier G, et al. Increased hypothalamic levels of endozepines, endogenous ligands of benzodiazepine receptors, in a rat model of sepsis. Shock (2016) 45(6):653–9. doi: 10.1097/SHK.0000000000000560
14. Clavier T, Tonon MC, Foutel A, Besnier E, Lefevre-Scelles A, Morin F, et al. Increased plasma levels of endozepines, endogenous ligands of benzodiazepine receptors, during systemic inflammation: a prospective observational study. Crit Care (2014) 18(6):633. doi: 10.1186/s13054-014-0633-7
15. Kralisch S, Hoffmann A, Kloting N, Bachmann A, Kratzsch J, Bluher M, et al. The novel Adipokine/Hepatokine fetuin b in severe human and murine diabetic kidney disease. Diabetes Metab (2017) 43(5):465–8. doi: 10.1016/j.diabet.2017.01.005
16. Kralisch S, Hoffmann A, Kloting N, Frille A, Kuhn H, Nowicki M, et al. The brown fat-secreted adipokine neuregulin 4 is decreased in human and murine chronic kidney disease. Eur J Endocrinol (2019) 181(2):151–9. doi: 10.1530/EJE-19-0017
17. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med (2009) 150(9):604–12. doi: 10.7326/0003-4819-150-9-200905050-00006
18. Draznin B, Aroda VR, Bakris G, Bakris G, Brown FM, Freeman R. American Diabetes association professional practice c. 2. classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes Care (2022) 45(Suppl 1):S17–38. doi: 10.2337/dc22-S002
19. Ebert T, Hopf LM, Wurst U, Bachmann A, Kralisch S, Lossner U, et al. Circulating adipocyte fatty acid binding protein is increased in chronic and acute renal dysfunction. Nutr Metab Cardiovasc Dis (2014) 24(9):1027–34. doi: 10.1016/j.numecd.2014.03.006
20. Richter J, Focke D, Ebert T, Kovacs P, Bachmann A, Lossner U, et al. Serum levels of the adipokine progranulin depend on renal function. Diabetes Care (2013) 36(2):410–4. doi: 10.2337/dc12-0220
21. Argiles A, Mourad G, Basset N, Axelrud-Cavadore C, Haiech J, Mion C, et al. Acute adaptative changes to unilateral nephrectomy in humans. Kidney Int (1987) 32(5):714–20. doi: 10.1038/ki.1987.265
22. Siebels M, Theodorakis J, Schmeller N, Corvin S, Mistry-Burchardi N, Hillebrand G, et al. Risks and complications in 160 living kidney donors who underwent nephroureterectomy. Nephrol Dial Transplant (2003) 18(12):2648–54. doi: 10.1093/ndt/gfg482
23. Holman R, Hines G, Kennedy I, Stevens RJ, Matthews D, Levy J. A calculator for homa. Diabetologia (2004) 47:222. doi: 10.1007/BF03375463
24. Zhao HJ, Wang S, Cheng H, Zhang MZ, Takahashi T, Fogo AB, et al. Endothelial nitric oxide synthase deficiency produces accelerated nephropathy in diabetic mice. J Am Soc Nephrol (2006) 17(10):2664–9. doi: 10.1681/ASN.2006070798
25. Sharma K, McCue P, Dunn SR. Diabetic kidney disease in the Db/Db mouse. Am J Physiol Renal Physiol (2003) 284(6):F1138–44. doi: 10.1152/ajprenal.00315.2002
26. Tonjes A, Hoffmann A, Kralisch S, Qureshi AR, Kloting N, Scholz M, et al. Pro-neurotensin depends on renal function and is related to all-cause mortality in chronic kidney disease. Eur J Endocrinol (2020) 183(3):233–44. doi: 10.1530/EJE-20-0087
27. Ebert T, Kralisch S, Kloting N, Hoffmann A, Bluher M, Zhang MZ, et al. Circulating progranulin but not renal progranulin expression is increased in renal dysfunction. Kidney Int (2015) 88(5):1197–8. doi: 10.1038/ki.2015.266
28. Kralisch S, Hoffmann A, Kloting N, Bachmann A, Kratzsch J, Stolzenburg JU, et al. Fstl3 is increased in renal dysfunction. Nephrol Dial Transplant (2017) 32(10):1637–44. doi: 10.1093/ndt/gfw472
29. Klein J, Fasshauer M, Ito M, Lowell BB, Benito M, Kahn CR. Beta(3)-adrenergic stimulation differentially inhibits insulin signaling and decreases insulin-induced glucose uptake in brown adipocytes. J Biol Chem (1999) 274(49):34795–802. doi: 10.1074/jbc.274.49.34795
30. Kralisch S, Klein J, Lossner U, Bluher M, Paschke R, Stumvoll M, et al. Interleukin-6 is a negative regulator of visfatin gene expression in 3t3-L1 adipocytes. Am J Physiol Endocrinol Metab (2005) 289(4):E586–90. doi: 10.1152/ajpendo.00090.2005
31. Stockler-Pinto MB, Saldanha JF, Yi D, Mafra D, Fouque D, Soulage CO. The uremic toxin indoxyl sulfate exacerbates reactive oxygen species production and inflammation in 3t3-L1 adipose cells. Free Radic Res (2016) 50(3):337–44. doi: 10.3109/10715762.2015.1125996
32. Gondouin B, Cerini C, Dou L, Sallee M, Duval-Sabatier A, Pletinck A, et al. Indolic uremic solutes increase tissue factor production in endothelial cells by the aryl hydrocarbon receptor pathway. Kidney Int (2013) 84(4):733–44. doi: 10.1038/ki.2013.133
33. Cohen G, Glorieux G, Thornalley P, Schepers E, Meert N, Jankowski J, et al. Review on uraemic toxins iii: recommendations for handling uraemic retention solutes in vitro–towards a standardized approach for research on uraemia. Nephrol Dial Transplant (2007) 22(12):3381–90. doi: 10.1093/ndt/gfm210
34. Ebert T, Kralisch S, Hoffmann A, Bachmann A, Lossner U, Kratzsch J, et al. Circulating angiopoietin-like protein 8 is independently associated with fasting plasma glucose and type 2 diabetes mellitus. J Clin Endocrinol Metab (2014) 99(12):E2510–7. doi: 10.1210/jc.2013-4349
35. Merabet E, Dagogo-Jack S, Coyne DW, Klein S, Santiago JV, Hmiel SP, et al. Increased plasma leptin concentration in end-stage renal disease. J Clin Endocrinol Metab (1997) 82(3):847–50. doi: 10.1210/jcem.82.3.3817
36. Martinez Cantarin MP, Waldman SA, Doria C, Frank AM, Maley WR, Ramirez CB, et al. The adipose tissue production of adiponectin is increased in end-stage renal disease. Kidney Int (2013) 83(3):487–94. doi: 10.1038/ki.2012.421
37. Joseph A, Chen H, Anagnostopoulos G, Montegut L, Lafarge A, Motino O, et al. Effects of acyl-coenzyme a binding protein (Acbp)/Diazepam-binding inhibitor (Dbi) on body mass index. Cell Death Dis (2021) 12(6):599. doi: 10.1038/s41419-021-03864-9
38. Conti E, Tremolizzo L, Bomba M, Uccellini O, Rossi MS, Raggi ME, et al. Reduced fasting plasma levels of diazepam-binding inhibitor in adolescents with anorexia nervosa. Int J Eat Disord (2013) 46(6):626–9. doi: 10.1002/eat.22129
39. Sica V, Martins I, Pietrocola F, Bravo-San Pedro JM. Quantification of intracellular Acbp/Dbi levels. Methods Cell Biol (2021) 165:111–22. doi: 10.1016/bs.mcb.2020.12.004
40. Stepien H, Agro A, Crossley J, Padol I, Richards C, Stanisz A. Immunomodulatory properties of diazepam-binding inhibitor: effect on human interleukin-6 secretion, lymphocyte proliferation and natural killer cell activity in vitro. Neuropeptides (1993) 25(3):207–11. doi: 10.1016/0143-4179(93)90104-i
41. Cosentino M, Marino F, Cattaneo S, Di Grazia L, Francioli C, Fietta AM, et al. Diazepam-binding inhibitor-derived peptides induce intracellular calcium changes and modulate human neutrophil function. J Leukoc Biol (2000) 67(5):637–43. doi: 10.1002/jlb.67.5.637
42. Motino O, Lambertucci F, Anagnostopoulos G, Li S, Martins I, Kroemer G. Cardio-, hepato- and pneumoprotective effects of autophagy checkpoint inhibition by targeting Dbi/Acbp. Autophagy (2022) 1–3. doi: 10.1080/15548627.2022.2131241
43. Motino O, Lambertucci F, Anagnostopoulos G, Li S, Nah J, Castoldi F, et al. Acbp/Dbi protein neutralization confers autophagy-dependent organ protection through inhibition of cell loss, inflammation, and fibrosis. Proc Natl Acad Sci U.S.A. (2022) 119(41):e2207344119. doi: 10.1073/pnas.2207344119
Keywords: Acyl-CoA-binding protein, adipokines, chronic kidney disease, diabetic kidney disease, diazepam binding inhibitor, hemodialysis, type 2 diabetes mellitus
Citation: Schürfeld R, Sandner B, Hoffmann A, Klöting N, Baratashvili E, Nowicki M, Paeschke S, Kosacka J, Kralisch S, Bachmann A, Frille A, Dietel A, Stolzenburg J-U, Blüher M, Zhang M-Z, Harris RC, Isermann B, Stumvoll M, Tönjes A and Ebert T (2023) Renal function is a major predictor of circulating acyl-CoA-binding protein/diazepam-binding inhibitor. Front. Endocrinol. 14:1152444. doi: 10.3389/fendo.2023.1152444
Received: 27 January 2023; Accepted: 09 May 2023;
Published: 23 May 2023.
Edited by:
Gencer Sancar, Universitätsklinikum Tübingen, GermanyReviewed by:
Siresha Bathina, Baylor College of Medicine, United StatesCopyright © 2023 Schürfeld, Sandner, Hoffmann, Klöting, Baratashvili, Nowicki, Paeschke, Kosacka, Kralisch, Bachmann, Frille, Dietel, Stolzenburg, Blüher, Zhang, Harris, Isermann, Stumvoll, Tönjes and Ebert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robin Schürfeld, Um9iaW4uU2NodWVyZmVsZEBtZWRpemluLnVuaS1sZWlwemlnLmRl
†ORCID: Robin Schürfeld, orcid.org/0000-0002-7488-916X
Thomas Ebert, orcid.org/0000-0003-1683-9276
†These authors have contributed equally to this work and share first and senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.