
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 20 February 2023
Sec. Bone Research
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1109322
 Xiao-jing Chen1,2Xiao-feng Wang3Zheng-can Pan1,2Deng Zhang1,2Ke-cheng Zhu1,2
Xiao-jing Chen1,2Xiao-feng Wang3Zheng-can Pan1,2Deng Zhang1,2Ke-cheng Zhu1,2 Tao Jiang1,2Xiao-ke Kong1,2Rui Xie1,2Li-hao Sun1,2Bei Tao1,2
Tao Jiang1,2Xiao-ke Kong1,2Rui Xie1,2Li-hao Sun1,2Bei Tao1,2 Jian-min Liu1,2*
Jian-min Liu1,2* Hong-yan Zhao1,2*
Hong-yan Zhao1,2*Aim: This study investigated the association between nerve conduction velocity (NCV) and bone mineral density (BMD) in patients with type 2 diabetes mellitus (T2DM).
Methods: This study retrospectively collected medical data of T2DM patients who underwent dual-energy X-ray absorptiometry and nerve conduction study at the Shanghai Ruijin Hospital, Shanghai, China. The primary outcome was the total hip BMD T-score. The main independent variables were motor nerve conduction velocities (MCVs), sensory nerve conduction velocities (SCVs), and composite Z-scores of MCV and SCV. T2DM patients were divided into total hip BMD T-scores < -1 and total hip BMD T-scores ≥ -1 groups. The association between the primary outcome and main independent variables was evaluated by Pearson bivariate correlation and multivariate linear regression.
Results: 195 female and 415 male patients with T2DM were identified. In male patients with T2DM, bilateral ulnar, median, and tibial MCVs and bilateral sural SCVs were lower in the total hip BMD T-score < -1 group than T-score ≥ -1 group (P < 0.05). Bilateral ulnar, median, and tibial MCVs, and bilateral sural SCVs showed positive correlations with total hip BMD T-score in male patients with T2DM (P < 0.05). Bilateral ulnar and tibial MCVs, bilateral sural SCVs, and composite MCV SCV and MSCV Z-scores were independently and positively associated with total hip BMD T-score in male patients with T2DM, respectively (P < 0.05). NCV did not show significant correlation with the total hip BMD T-score in female patients with T2DM.
Conclusion: NCV showed positive association with total hip BMD in male patients with T2DM. A decline in NCV indicates an elevated risk of low BMD (osteopenia/osteoporosis) in male patients with T2DM.
Diabetes mellitus (DM) has emerged as a major global epidemic in the 21st century. The prevalence of type 2 diabetes mellitus (T2DM) is constantly increasing worldwide and is a major healthcare concern. According to epidemiological statistics, 462 million individuals were affected with T2DM worldwide in 2017, accounting for 6.28% of the global population (1). Diabetes peripheral neuropathy (DPN) is a common complication of T2DM with prevalence rates of 35.34% in China (2), 39.3% in India (3), 42.2% in Germany (4), and 19.4% in America (5). DPN is the primary cause of foot ulceration and neuropathic pain in diabetic patients, thereby negatively impacting daily activities and adversely affecting the quality of life (6). Osteoporotic fracture is another major complication of T2D. The risk of osteoporotic fracture is significantly increased with decreased bone mineral density (BMD) (7), diabetes duration, age, previous history of fracture, and insulin use (8, 9). T2DM patients with vertebral fractures show significantly higher risk of mortality than those with T2DM alone (10).
Neurological diseases adversely affect the quality of life and alter bone metabolism (11). However, the association between DPN and bone disease in T2DM patients remains controversial. A retrospective analysis of a cohort comprising old male veterans found that DPN mediated 21.1% of the diabetes-associated increased fracture risk (12). Retrospective case-control studies demonstrated that DPN was an independent risk factor for osteoporosis and was independently associated with the risk of fracture and non-traumatic fractures in T2DM patients (13, 14). However, there were findings that foot bone density or fracture risk was similar in diabetic patients with and without diabetic neuropathies (15, 16). Another observational study reported bone material properties were poor in type 2 diabetes patients with DPN than those without DPN, but the association between DPN and bone health parameters were not statistically significant (17).
Two key limitations contribute to the inconsistent findings of studies on DPN: underdiagnosis of DPN in clinical settings and lack of comprehensiveness and consistency for neuropathy screening (18). Nerve conduction study (NCS) is a primary clinical screening method for DPN. Owing to its noninvasiveness, repeatability, high sensitivity, and high specificity, this method offers advantages for the assessment of neuropathic disorders (19). NCS parameters provide an objective and direct evaluation of DPN and can accurately predict disease severity (20). Myelin and axonal damages are two major lesions in DPN. In the NCS, nerve conduction velocity (NCV) mainly reflects the myelin sheath function, and action potential amplitude mainly indicates the axonal defect of nerve fibers and axon change (21). The mechanistic study revealed that myelin loss started at the prediabetic stage and preceding nerve fibers impairment (22). These results suggested that NCV is an early indicator of DPN and may be useful as an objective parameter in research studies.
It is well established that DPN and osteoporosis are two major complications of T2DM, but further investigation is warranted to determine their association. The aims of the present study were to investigate the association between NCV and BMD in T2DM patients and aimed to provide more clinical evidence concerning DPN and osteoporosis in T2DM.
This was a retrospective study that reviewed in-patient electronic medical records between January 2017 and December 2019 at the Department of Endocrine and Metabolic Diseases, Shanghai Ruijin Hospital, a tertiary medical hospital affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China. This study was approved by the Ethics committee of Shanghai Ruijin Hospital.
The subjects in this study were patients with T2DM that underwent dual-energy X-ray absorptiometry (DXA) and NCS. The diagnosis of T2DM was according to the World Health Organization 1999 criteria (23). Differential diagnosis of DPN included assessing the etiology of neuropathies that mimic clinical presentation of DPN, so the patients were excluded from this study if they had the following: alcohol abuse, vitamin B12 deficiency, neoplasia, HIV treatment, chemotherapy, amyloidosis, and genetic neuropathies (24).
Demographic information, clinical and laboratory data, and antidiabetic treatments on admission or during hospitalization were retrieved from the electronic medical records. The laboratory tests were done following standard procedures in the hospital. The laboratory variables included HbA1c concentration (%), bilirubin (μmol/L), albumin (g/L), creatinine (μmol/L), triglycerides (mmol/L), total cholesterol (mmol/L), high-density lipoprotein cholesterol (mmol/L), low-density lipoprotein cholesterol (mmol/L), apolipoprotein A1 (g/L), apolipoprotein B (g/L), apolipoprotein E (mg/dL), lipoprotein (a) (g/L), and 25(OH)D (nmol/L).
BMD was measured by DXA (Lunar Expert-1313; Lunar Corp, Madison, WI, USA), and BMD T-score was calculated as the difference between the BMD of an individual and that of the reference population divided by the standard deviation (SD) of the reference population. This study evaluated the total hip BMD T-score as the primary outcome because the risk of hip fracture increased significantly in T2DM (25–27), and T2DM patients with hip fracture suffered high post-hip fracture mortality (28). According to the WHO diagnostic criteria, osteoporosis is defined as a BMD T-score lower than or equal to -2.5 SD, low bone mass (osteopenia) as a BMD T-score between -2.5 and -1 SD, and normal BMD as T-score equal to or greater than -1 SD (29). Therefore, the subjects were divided into two groups: the normal BMD group with total hip BMD T-score ≥-1 and the low BMD group, including low bone mass (osteopenia) and osteoporosis, with total hip BMD T-Score < -1.
The NCV data, including motor nerve conduction velocities (MCVs) and sensory nerve conduction velocities (SCVs), were collected from the results of NCS by an electromyography machine (Dantec Keypoint 9033, USA) according to standard procedure. This study used the NCS values of healthy Chinese adults (18-30 years) as normal reference values: 58.8 ± 3.3 m/s for ulnar MCV, 57.8 ± 2.58 m/s for median MCV, 49.8 ± 4.39 m/s for tibial MCV, 47.44 ± 4.65 m/s for median SCV and 46.71 ± 4.17 m/s for sural SCV (30). A Z-score was developed from every NCV value based on the following formula: Z-score = (value of the individual – mean value of the normal reference)/standard deviation of the normal reference. A composite MCV Z-score was calculated as the following formula: [(bilateral ulnar MCV Z-scores) + (bilateral median MCV Z-scores) + (bilateral tibial MCV Z-scores)]/6, a composite SCV Z-score calculated as: [(bilateral median SCV Z-scores) + (bilateral sural MCV Z-scores)]/4, and a composite MSCV Z-score calculated as the composite MCV Z-score + SCV Z-score (31, 32). The main independent variables in this study were MCVs of the bilateral ulnar, median, and tibial nerves, SCVs of bilateral median and sural nerves, and composite Z-scores.
Categorical variables were displayed as numbers and percentages. Continuous variables were checked for normal distribution by the Kolmogorov–Smirnov test and were summarized as the arithmetic mean ± SD if with normal distribution and as the median and interquartile range (IQR) if with no normal distribution. The characteristics between T-score < -1 and T-score ≥ -1 groups were compared by chi-square test for categorical variables and by two-way ANOVA and t-test for continuous variables as appropriate.
This study hypothesized that NCV is associated with BMD in T2DM and applied a multi-step modeling process to identify the association between NCV and total hip BMD. Firstly, Pearson correlations were conducted to evaluate the bivariate relationship between total hip BMD T-score and each MCV, SCV, and composite Z-score. Subsequently, univariate linear regression was performed to assess the univariate association between total hip BMD T-score and age, BMI, laboratory variables, and each MCV, SCV, and composite Z-score, respectively. Finally, stepwise multivariate linear regression was performed to identify the independent association between NCV and total hip BMD T-score and adjust the effects of covariates. MCVs, SCVs, and composite Z-scores were independent variables and separately entered into multivariate linear regression models to avoid collinearity. Covariates in multivariate linear regression included smoke, alcohol, T2DM treatments, HbA1c, and variables that were significantly associated with total hip BMD T-score in univariate linear regression or possibly associated with BMD from scientific/clinical knowledge. The sample size of our study was large enough and already met the ten events per variable principle, which is a widely advocated minimal criterion of the sample size to avoid overfitting in regression analysis (33). No collinearity was observed among covariates (VIF < 3.0 and r < 0.7). Statistical analysis was performed with IBM SPSS Statistics 27.
This study identified 195 female and 415 male patients with T2DM. The prevalence of T-score < -1 was higher in females than males among T2DM patients (29.23% vs. 12.05%, P < 0.001). The clinical characteristics were compared between total hip BMD T-score < -1 and T-score ≥ -1 groups separately for male and female patients (Table 1). The age was older in the T-score < -1 group than in the T-score ≥ -1 group in female patients with T2DM (P < 0.001). The BMI was lower in T-score < -1 group than in the T-score ≥ -1 group in the female and male patients with T2DM (P < 0.001). The HbA1c level was lower in T-score < -1 group than in the T-score ≥ -1 group in the female patients with T2DM (P < 0.05). In male patients with T2DM, compared to the T-score ≥ -1 group, the T-score < -1 group had a lower level of left ulnar MCV, right ulnar MCV, left median MCV, right median MCV, left tibial MCV, right tibial MCV, left sural SCV, right sural SCV, composite MCV Z-score, composite SCV Z-score, and composite MSCV Z-score, respectively (P < 0.05). However, the two groups did not show significant differences in the MCVs and SCVs in female patients with T2DM.

Table 1 Clinical characteristics compared between total hip BMD T-score < -1 and ≥ -1 groups for female and male patients with T2DM.
In male patients with T2DM, a significant positive bivariate correlation existed between total hip BMD T-score and variables: left ulnar MCV, right ulnar MCV, left median MCV, right median MCV, left tibial MCV, right tibial MCV, left sural SCV, right sural SCV, composite MCV Z-score, composite SCV Z-score, and composite MSCV Z-score, respectively (P < 0.05) (Figure 1A). While in female patients with T2DM, there was no significant bivariate correlation between total hip BMD T-score and NCV (Figure 1B).
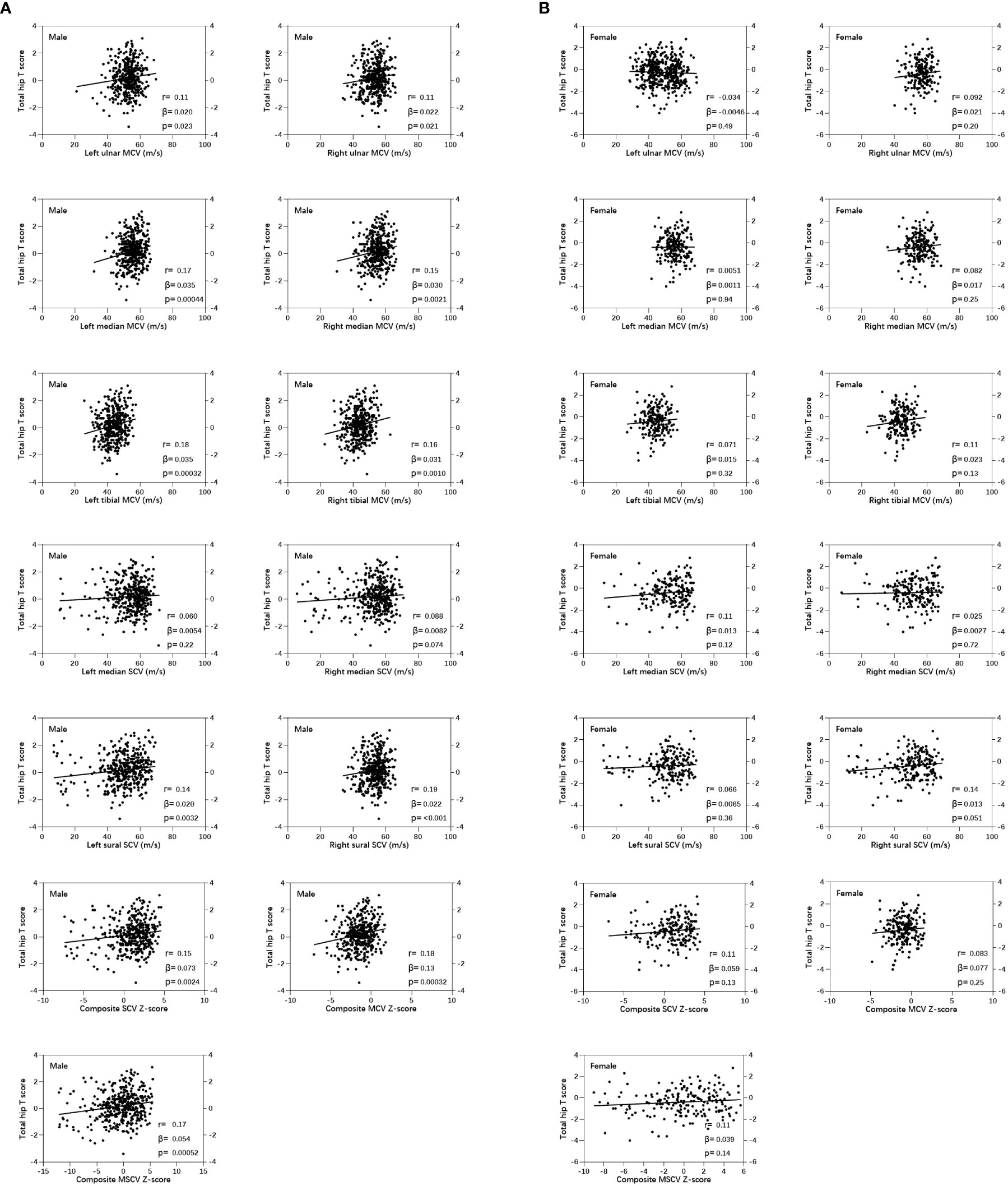
Figure 1 Pearson correlations showed the correlation between nerve conduction velocity and total hip bone mineral density (BMD) T-score in male (A) and female (B) patients with T2DM.
In male patients with T2DM, univariate linear regression analysis revealed that each of the following variables was significantly correlated with the total hip BMD T score: age, BMI, left ulnar MCV, right ulnar MCV, left median MCV, right median MCV, left tibial MCV, right tibial MCV, left sural SCV, right sural SCV, composite MCV Z-score, composite SCV Z-score and composite MSCV Z-score (P < 0.05) (Figure 2). While in female patients with T2DM, NCV was not significantly correlated with total hip BMD T score (Figure 3).
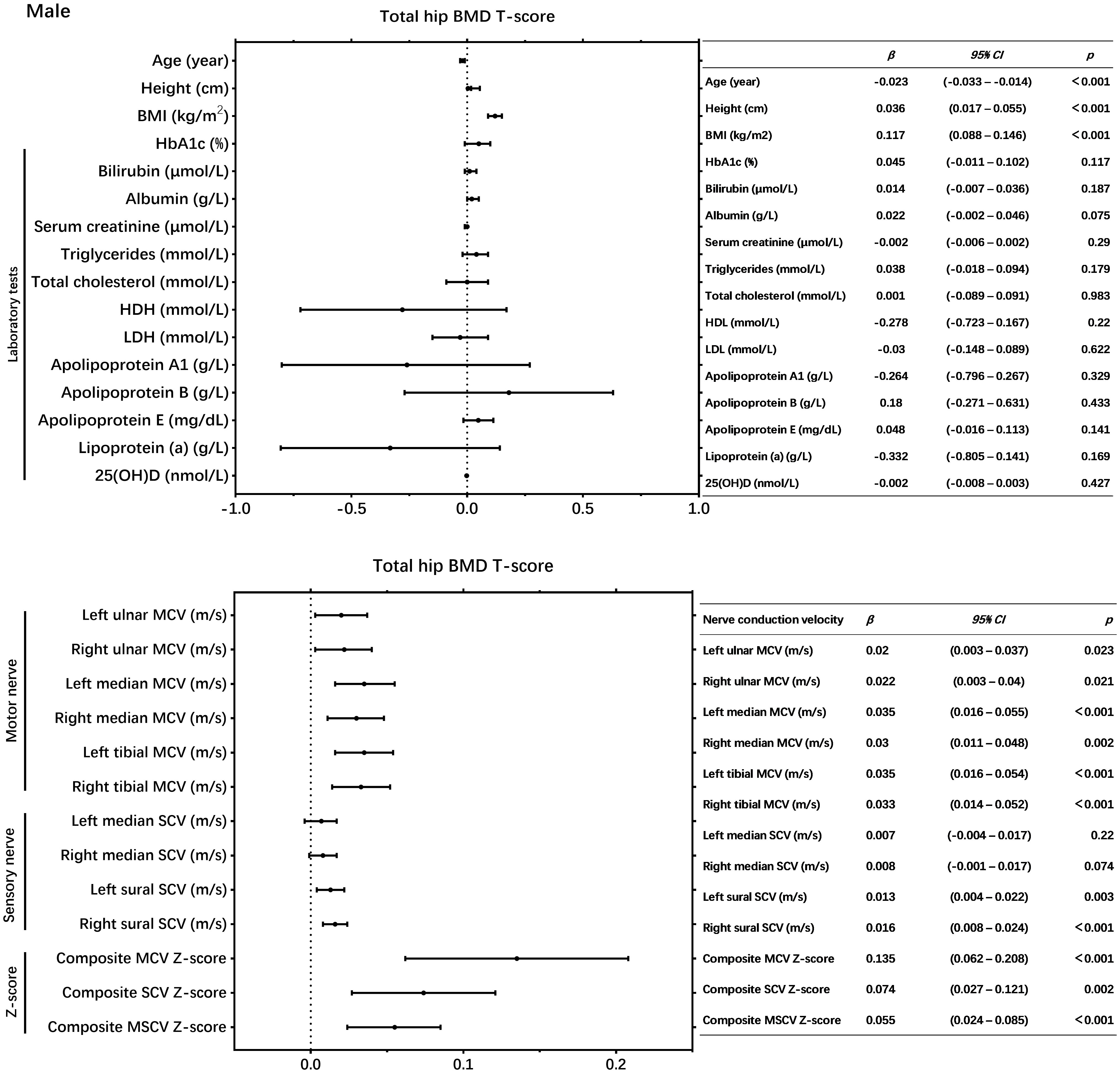
Figure 2 Univariate linear regression showed the association between nerve conduction velocity and total hip bone mineral density (BMD) T-score in male patients with T2DM.
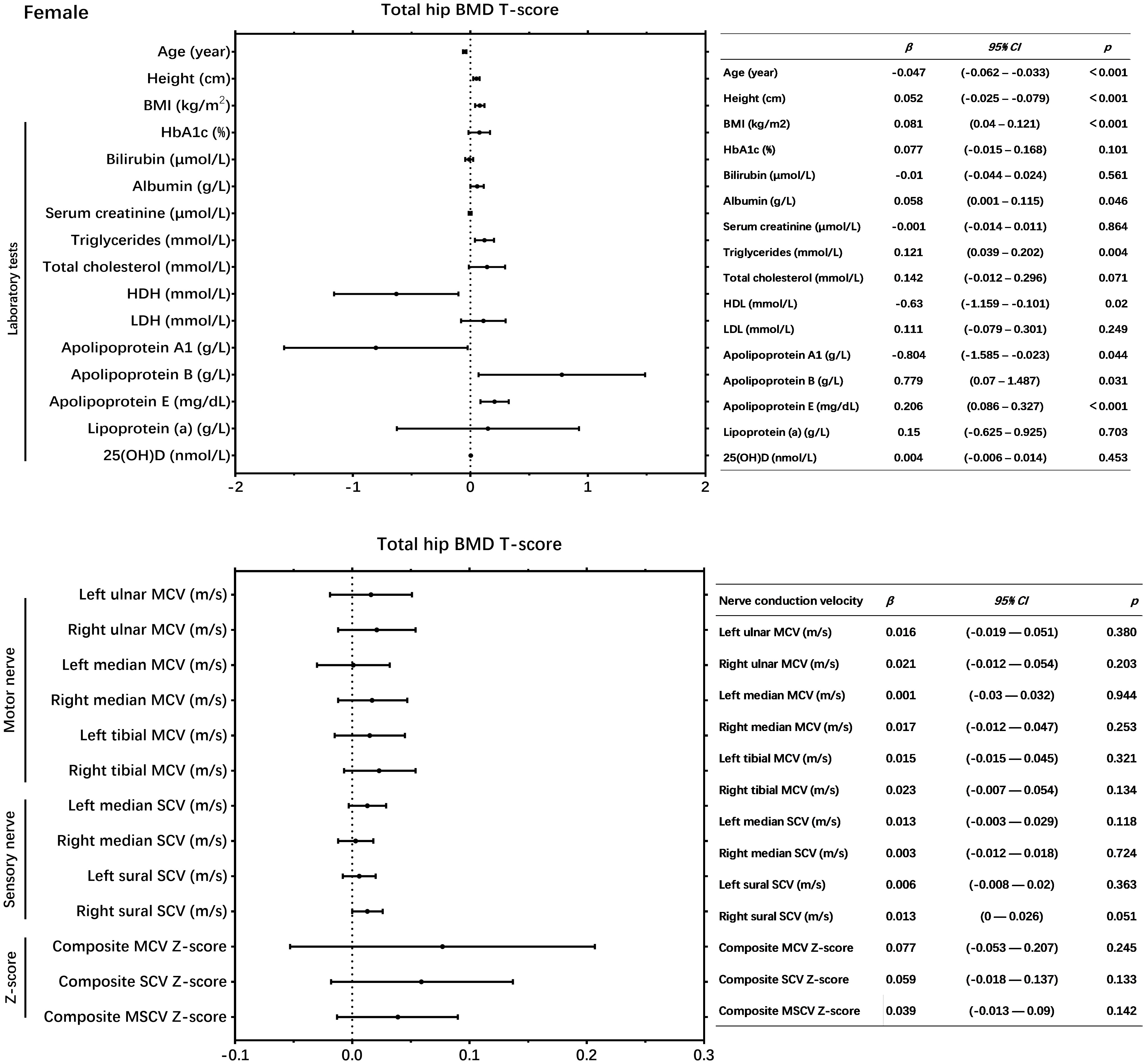
Figure 3 Univariate linear regression showed the association between neSrve conduction velocity and total hip bone mineral density (BMD) T-score in female patients with T2DM.
In male patients with T2DM, multivariable regression models, adjusting for age, BMI, and other confounding variables, revealed that each of the following NCVs was independently and positively associated with the total hip BMD T score: left median MCV, right median MCV, left tibial MCV, right tibial MCV, left sural SCV, right sural SCV, composite MCV Z-score, composite SCV Z-score, and composite MSCV Z-score (P < 0.05) (Table 2). Multivariable regression revealed no other covariables were significantly associated with the total hip BMD T score in male patients with T2DM.
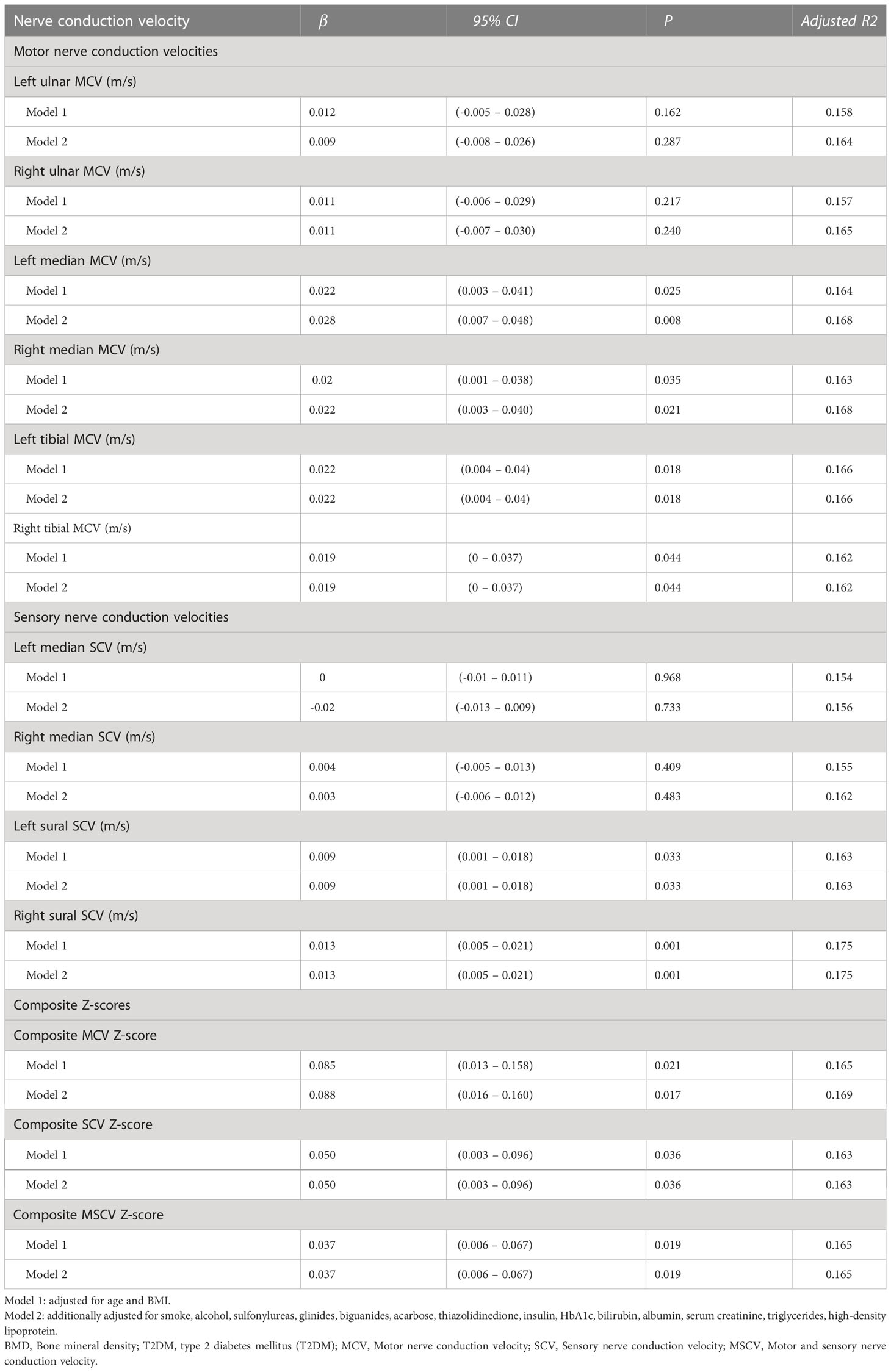
Table 2 Association of nerve conduction velocity and total hip BMD T-score in male patients with T2DM by multivariable linear regression.
Osteoporotic fracture is a critical survival factor for T2DM, but the risk of which is often underestimated. BMD decline increases osteoporotic fracture risk in T2DM (7). Thus, it is important to identify T2DM patients at high risk of osteoporosis and osteoporotic fractures and explore factors responsible for or associated with BMD changes. In the current study, we found that NCV is independently and positively associated with BMD in male patients with T2DM, which highlighted NCV decline as a high-risk factor for low BMD (osteopenia/osteoporosis).
The previous studies have yet to reach a consistent conclusion about the association between DPN and osteoporosis in DM. A meta-analysis included five studies investigating the association between DPN and BMD in T1DM or T2DM, 4 of which found no effect of DPN on BMD, and this study highlighted the major limitation for analysis is the different diagnostic criteria for DPN among five studies (34). DPN is a heterogeneous clinical condition and an exclusive diagnosis. It needs multistep screening processes to exclude other peripheral neuropathies, including alcoholism, vitamin B12 deficiency, autoimmune diseases, tumors, and infection. DPN varies considerably in the screening and diagnostic criteria, including questionnaires, electrophysiological methods, imaging diagnostic tools, and hierarchical classification schemes (35), leading to heterogeneity across studies. In addition, more than half of physicians did not adhere to standardized multistep screening and diagnosis of DPN (36). Nearly half of DPN cases may be asymptomatic (37, 38), thereby complicating the recognition by the patients (39) and their physicians (40). These facts lead to heterogeneity in the diagnostic rate of DPN in T2DM among different clinical settings and make it difficult to reach consistent and certain conclusions in DPN studies.
The NCS is a sensitive, specific, non-invasive, and quantitative screening tool for DPN, and it has been recommended as the gold diagnostic standard by expert consensus (41). The NCS result has been found to be associated with glycemic control (42), duration of diabetes (43), and cognitive dysfunction in T2DM (44). Therefore, this study used NCVs as important parameters and found their positive association with total hip BMD in male patients with T2DM. This finding supports the advantage of using NCS in DPN research.
In the present study, bilateral tibial MCV and sural SCV were independently associated with total hip BMD; however, such associations were not observed for ulnar MCV and median SCV. This finding is consistent with the phenomenon that the symptom of DPN starts at the toes, feet, and lower legs (45). In NCS, the tibial was the most sensitive nerve compared to the peroneal and sural for diagnosis of polyneuropathy (46). The composite Z-scores are a summary parameter that can quantify the overall abnormality of NCVs. It has been demonstrated to have higher specificity and sensitivity for evaluating polyneuropathies than individual nerve MCV or SCV results (47). Our study found that each of the composite MCV, SCV, and MSCV Z-scores was independently and positively associated with total hip BMD T-score in male patients with T2DM, which shows the association between overall abnormality of NCV and total hip BMD decline.
Sympathectomy in diabetic mice would induce the increased stromal cell-derived factor 1 level and decreased bone regeneration, but the specific molecular mechanism is unknown (48). Besides, no other study deeply evaluates the underlying mechanism of distal peripheral neuronal regulation on bone homeostasis and remodeling in diabetes. However, the regulation of neurotrophic and neurovascular bone metabolism suggests the contribution of neuropathy to decreased bone health in DM. Peripheral nerves promote bone remodeling and regeneration, which is mediated by osteogenesis induction of nerve growth factor and axon guidance molecule (49). The diabetes adults also have decreased levels of two sensory neuropeptides with bone anabolic activity, namely substance P and calcitonin gene-related peptide (CGRP) (50). In diabetes, peripheral neuropathy was associated with blood vessel damage (51) and abdominal obesity (52), which might mediate the interplay between DPN and bone disease. More clinical studies are needed to examine the association between DPN and bone disease in diabetes.
It is noteworthy that the association between NCV and total hip BMD was not observed in female type 2 diabetes in this study. Some studies provided clues to explain this phenomenon. Epidemiological studies showed that, in T2DM, the male was more susceptible to microvascular complications (53) and had an earlier onset of DPN than the female (54). In the diabetic model, male mice had a slower level of MCV than female mice at 16-weeks of diabetes (55). In addition, neuroactive steroids regulate the peripheral nervous system in a sex-dependent manner (56). In the male rat, short-term diabetic status affected the respiratory chain complex IV and ATP levels and decreased the axoplasm protein contents and mRNA levels of kinesin family member protein 1A, 5B, and 5A in axons of dorsal root ganglion neurons, which was mediated by decreased levels of neuroactive steroid, including testosterone, dihydrotestosterone, and allopregnanolone. Meanwhile, those changes were not observed in female rats (57). The above studies suggest the impact of gender or sex hormone on the development of DPN, and more mechanistic studies are needed to explain the gender-based difference in the association between DPN and osteoporosis in type 2 diabetes.
Undoubtedly, there were several limitations in the present study. Firstly, NCV normal values were referred from relatively young, healthy Chinese. However, a significant difference did not exist because the NCV reference was homogeneous to all the subjects. Secondly, fall is an important external factor responsible for fracture in T2DM, but fall data was unavailable for our database. Thirdly, this study did not include osteoporotic fracture and failed to evaluate bone disease in T2DM comprehensively. More large-scale cohort studies are required to yield more comprehensive clinical data and determine the cause-to-consequence effect between DPN and osteoporosis and osteoporotic fracture in type 2 diabetes.
In summary, this study revealed that NCV was independently and positively associated with total hip BMD in male patients with T2DM, however, this association was not observed in female patients with T2DM. Hence, NCV decline might be a high-risk indicator for low BMD (osteopenia/osteoporosis) in male patients with T2DM. Mechanistic and epidemiological studies are warranted to determine the causal effect between DPN and low BMD in T2DM.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by Ruijin Hospital Ethics Committee Shanghai JiaoTong University School of Medicine. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
H-yZ and J-mL were the guarantors of this work and, as such, had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis and was involved in the conception and design of the study. X-jC collected and analyzed the data. X-fW, Z-cP, DZ, K-cZ, TJ, X-kK, RX, L-hS, and BT were involved in the collection and interpretation of data. X-jC drafted the manuscript. J-mL modified the manuscript. H-yZ revised the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
This work was supported by the National Natural Science Foundation of China (NO.81970758, 82070865).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of type 2 diabetes – global burden of disease and forecasted trends. J Epidemiol Glob Health (2020) 10(1):107–11. doi: 10.2991/jegh.k.191028.001
2. Pan Q, Li Q, Deng W, Zhao D, Qi L, Huang W, et al. Prevalence of and risk factors for peripheral neuropathy in Chinese patients with diabetes: A multicenter cross–sectional study. Front Endocrinol (Lausanne) (2018) 9:617. doi: 10.3389/fendo.2018.00617
3. Darivemula S, Nagoor K, Patan SK, Reddy NB, Deepthi CS, Chittooru CS. Prevalence and its associated determinants of diabetic peripheral neuropathy (DPN) in individuals having type–2 diabetes mellitus in rural south India. Indian J Community Med (2019) 44(2):88–91. doi: 10.4103/ijcm.IJCM_207_18
4. Pfannkuche A, Alhajjar A, Ming A, Walter I, Piehler C, Mertens PR. Prevalence and risk factors of diabetic peripheral neuropathy in a diabetics cohort: Register initiative “diabetes and nerves”. Endocrine Metab Sci (2020) 1(1–2):100053. doi: 10.1016/j.endmts.2020.100053
5. Gregg EW, Gu Q, Williams D, de Rekeneire N, Cheng YJ, Geiss L, et al. Prevalence of lower extremity diseases associated with normal glucose levels, impaired fasting glucose, and diabetes among U.S. adults aged 40 or older. Diabetes Res Clin Pract (2007) 77(3):485–8. doi: 10.1016/j.diabres.2007.01.005
6. Dermanovic Dobrota V, Hrabac P, Skegro D, Smiljanic R, Dobrota S, Prkacin I, et al. The impact of neuropathic pain and other comorbidities on the quality of life in patients with diabetes. Health Qual Life Outcomes (2014) 12:171. doi: 10.1186/s12955-014-0171-7
7. Schwartz AV, Vittinghoff E, Bauer DC, Hillier TA, Strotmeyer ES, Ensrud KE, et al. Association of BMD and FRAX score with risk of fracture in older adults with type 2 diabetes. JAMA (2011) 305(21):2184–92. doi: 10.1001/jama.2011.715
8. Leslie WD, Johansson H, McCloskey EV, Harvey NC, Kanis JA, Hans D. Comparison of methods for improving fracture risk assessment in diabetes: The Manitoba BMD registry. J Bone Miner Res (2018) 33(11):1923–30. doi: 10.1002/jbmr.3538
9. Kong X–K, Zhao Z–Y, Zhang D, Xie R, Sun L–H, Zhao H–Y, et al. Major osteoporosis fracture prediction in type 2 diabetes: A derivation and comparison study. Osteoporos Int (2022) 33(9):1957–67. doi: 10.1007/s00198-022-06425-8
10. Koromani F, Oei L, Shevroja E, Trajanoska K, Schoufour J, Muka T, et al. Vertebral fractures in individuals with type 2 diabetes: More than skeletal complications alone. Diabetes Care (2020) 43(1):137–44. doi: 10.2337/dc19-0925
11. Beeve AT, Brazill JM, Scheller EL. Peripheral neuropathy as a component of skeletal disease in diabetes. Curr Osteoporos Rep (2019) 17(5):256–69. doi: 10.1007/s11914-019-00528-8
12. Lee RH, Sloane R, Pieper C, Lyles KW, Adler RA, van Houtven C, et al. Clinical fractures among older men with diabetes are mediated by diabetic complications. J Clin Endocrinol Metab (2018) 103(1):281–7. doi: 10.1210/jc.2017-01593
13. Li T, Hu L, Yin X–L, Zou Y, Fu H–Y, Li H–L. Prevalence and risk factors of osteoporosis in patients with type 2 diabetes mellitus in nanchang (China): A retrospective cohort study. Diabetes Metab Syndr Obes (2022) 15:3039–48. doi: 10.2147/DMSO.S372348
14. Kim J–H, Jung M–H, Lee J–M, Son H–S, Cha B–Y, Chang S–A. Diabetic peripheral neuropathy is highly associated with nontraumatic fractures in Korean patients with type 2 diabetes mellitus. Clin Endocrinol (Oxf) (2012) 77(1):51–5. doi: 10.1111/j.1365-2265.2011.04222.x
15. Barwick AL, Tessier JW, Janse de Jonge X, Chuter VH. Foot bone density in diabetes may be unaffected by the presence of neuropathy. J Diabetes Complications (2016) 30(6):1087–92. doi: 10.1016/j.jdiacomp.2016.04.013
16. Khan KS, Christensen DH, Nicolaisen SK, Gylfadottir SS, Jensen TS, Nielsen JS, et al. Falls and fractures associated with type 2 diabetic polyneuropathy: A cross–sectional nationwide questionnaire study. J Diabetes Investig (2021) 12(10):1827–34. doi: 10.1111/jdi.13542
17. Lasschuit JWJ, Greenfield JR, Tonks KTT. Contribution of peripheral neuropathy to poor bone health in the feet of people with type 2 diabetes mellitus. Acta Diabetol (2022) 59(2):217–24. doi: 10.1007/s00592-021-01803-w
18. Petropoulos IN, Ponirakis G, Khan A, Almuhannadi H, Gad H, Malik RA. Diagnosing diabetic neuropathy: Something old, something new. Diabetes Metab J (2018) 42(4):255–69. doi: 10.4093/dmj.2018.0056
19. Haque F, Reaz MBI, Ali SHM, Arsad N, Chowdhury MEH. Performance analysis of noninvasive electrophysiological methods for the assessment of diabetic sensorimotor polyneuropathy in clinical research: a systematic review and meta–analysis with trial sequential analysis. Sci Rep (2020) 10(1):21770. doi: 10.1038/s41598-020-78787-0
20. Kamiya H, Shibata Y, Himeno T, Tani H, Nakayama T, Murotani K, et al. Point–of–care nerve conduction device predicts the severity of diabetic polyneuropathy: A quantitative, but easy–to–use, prediction model. J Diabetes Investig (2021) 12(4):583–91. doi: 10.1111/jdi.13386
21. Chung T, Prasad K, Lloyd TE. Peripheral neuropathy: Clinical and electrophysiological considerations. Neuroimaging Clin N Am (2014) 24(1):49–65. doi: 10.1016/j.nic.2013.03.023
22. Palavicini JP, Chen J, Wang C, Wang J, Qin C, Baeuerle E, et al. Early disruption of nerve mitochondrial and myelin lipid homeostasis in obesity–induced diabetes. JCI Insight (2020) 5(21):e137286. doi: 10.1172/jci.insight.137286
23. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med (1998) 15(7):539–53.
24. Feldman EL, Callaghan BC, Pop–Busui R, Zochodne DW, Wright DE, Bennett DL, et al. Diabetic neuropathy. Nat Rev Dis Primers (2019) 5(1):41. doi: 10.1038/s41572-019-0092-1
25. Martinez–Laguna D, Tebe C, Javaid MK, Nogues X, Arden NK, Cooper C, et al. Incident type 2 diabetes and hip fracture risk: a population–based matched cohort study. Osteoporosis Int (2015) 26(2):827–33. doi: 10.1007/s00198-014-2986-9
26. Moayeri A, Mohamadpour M, Mousavi SF, Shirzadpour E, Mohamadpour S, Amraei M. Fracture risk in patients with type 2 diabetes mellitus and possible risk factors: a systematic review and meta–analysis. Ther Clin Risk Manag (2017) 13:455–68. doi: 10.2147/TCRM.S131945
27. Wang H, Ba Y, Xing Q, Du J–L. Diabetes mellitus and the risk of fractures at specific sites: a meta–analysis. BMJ Open (2019) 9(1):e024067. doi: 10.1136/bmjopen-2018-024067
28. Tebé C, Martínez–Laguna D, Carbonell–Abella C, Reyes C, Moreno V, Diez–Perez A, et al. The association between type 2 diabetes mellitus, hip fracture, and post–hip fracture mortality: a multi–state cohort analysis. Osteoporosis Int (2019) 30(12):2407–15. doi: 10.1007/s00198-019-05122-3
29. Kanis JA. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Synopsis of a WHO report. WHO study group. . Osteoporos Int (1994) 4(6):368–81. doi: 10.1007/BF01622200
30. Cai F, Zhang J. Study of nerve conduction and late responses in normal Chinese infants, children, and adults. J Child Neurol (1997) 12(1):13–8. doi: 10.1177/088307389701200102
31. Zhang Y, Shen X, He L, Zhao F, Yan S. Association of sarcopenia and muscle mass with both peripheral neuropathy and nerve function in patients with type 2 diabetes. Diabetes Res Clin Pract (2020) 162:108096. doi: 10.1016/j.diabres.2020.108096
32. Yu C, Zhuang L, Xu F, Zhao L–H, Wang X–H, Wang C–H, et al. Increased levels of serum adenosine deaminase and increased risk of diabetic peripheral neuropathy in type 2 diabetes. Front Endocrinol (Lausanne) (2022) 13:997672. doi: 10.3389/fendo.2022.997672
33. Riley RD, Ensor J, Snell KIE, Harrell FE, Martin GP, Reitsma JB, et al. Calculating the sample size required for developing a clinical prediction model. BMJ (2020), 368:m441. doi: 10.1136/bmj.m441
34. Mohseni M, Hosseinzadeh P, Civitelli R, Eisen S. Effect of peripheral neuropathy on bone mineral density in adults with diabetes: A systematic review of the literature and meta–analysis. Bone (2021) 147:115932. doi: 10.1016/j.bone.2021.115932
35. Jensen TS, Karlsson P, Gylfadottir SS, Andersen ST, Bennett DL, Tankisi H, et al. Painful and non–painful diabetic neuropathy, diagnostic challenges and implications for future management. Brain (2021) 144(6):1632–45. doi: 10.1093/brain/awab079
36. Ziegler D, Landgraf R, Lobmann R, Reiners K, Rett K, Schnell O, et al. Screening and diagnosis of diabetic polyneuropathy in clinical practice: A survey among German physicians (PROTECT study survey). Prim Care Diabetes (2022) 16(6):804–9. doi: 10.1016/j.pcd.2022.09.009
37. Pop–Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, et al. Diabetic neuropathy: A position statement by the American diabetes association. Diabetes Care (2017) 40(1):136–54. doi: 10.2337/dc16-2042
38. Kamalarathnam SR, Varadarajan S. Diabetic peripheral neuropathy in diabetic patients attending an urban health and training centre. J Family Med Prim Care (2022) 11(1):113–7. doi: 10.4103/jfmpc.jfmpc_470_21
39. Lee PY, Hani SS, Cheng YG, Zainuddin Z, Singh H, Loh KW. The proportion of undiagnosed diabetic peripheral neuropathy and its associated factors among patients with T2DM attending urban health clinics in selangor. Malays Fam Physician (2022) 17(1):36–43. doi: 10.51866/oa1297
40. Ziegler D, Landgraf R, Lobmann R, Reiners K, Rett K, Schnell O, et al. Polyneuropathy is inadequately treated despite increasing symptom intensity in individuals with and without diabetes (PROTECT follow–up study). J Diabetes Investig (2020) 11(5):1272–7. doi: 10.1111/jdi.13267
41. Tesfaye S, Boulton AJM, Dyck PJ, Freeman R, Horowitz M, Kempler P, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care (2010) 33(10):2285–93. doi: 10.2337/dc10-1303
42. Akaza M, Akaza I, Kanouchi T, Sasano T, Sumi Y, Yokota T. Nerve conduction study of the association between glycemic variability and diabetes neuropathy. Diabetol Metab Syndr (2018) 10:69. doi: 10.1186/s13098-018-0371-0
43. Hamid WS, Ahmed HS, Osman MA, Babiker R. Nerve conduction and its correlations with duration of diabetes mellitus and glycosylated haemoglobin in type 2 diabetes mellitus (T2DM). J Endocrinology Metab Diabetes South Afr (2021) 26(2):46–51. doi: 10.1080/16089677.2021.1877444
44. Ni W, Zhang Z, Zhang B, Zhang W, Cheng H, Miao Y, et al. Connecting peripheral to central neuropathy: Examination of nerve conduction combined with olfactory tests in patients with type 2 diabetes. Diabetes Metab Syndr Obes (2021) 14:3097–107. doi: 10.2147/DMSO.S312021
45. Said G. Diabetic neuropathy–a review. Nat Clin Pract Neurol (2007) 3(6):331–40. doi: 10.1038/ncpneuro0504
46. Tankisi H, Pugdahl K, Beniczky S, Andersen H, Fuglsang–Frederiksen A. Evidence–based recommendations for examination and diagnostic strategies of polyneuropathy electrodiagnosis. Clin Neurophysiol Pract (2019) 4:214–22. doi: 10.1016/j.cnp.2019.10.005
47. Heise CO, Machado FCN, de Amorim SC, de Toledo SM. Combined nerve conduction index in diabetic polyneuropathy. . Arq Neuropsiquiatr (2012) 70(5):330–4. doi: 10.1590/S0004-282X2012000500005
48. Wagner JM, Wallner C, Becerikli M, Reinkemeier F, Glinski von M, Sogorski A, et al. Role of autonomous neuropathy in diabetic bone regeneration. Cells (2022) 11(4):612. doi: 10.3390/cells11040612
49. Fukuda T, Takeda S, Xu R, Ochi H, Sunamura S, Sato T, et al. Sema3A regulates bone–mass accrual through sensory innervations. Nature (2013) 497(7450):490–3. doi: 10.1038/nature12115
50. Wang LH, Zhou SX, Li RC, Zheng LR, Zhu JH, Hu SJ, et al. Serum levels of calcitonin gene–related peptide and substance p are decreased in patients with diabetes mellitus and coronary artery disease. J Int Med Res (2012) 40(1):134–40. doi: 10.1177/147323001204000114
51. Li L, Yang Y, Bai J, Zhang Y, Yang H, Zhang Y, et al. Impaired vascular endothelial function is associated with peripheral neuropathy in patients with type 2 diabetes. Diabetes Metab Syndr Obes (2022) 15:1437–49. doi: 10.2147/DMSO.S352316
52. Zhou R, Li F, Chen G, Fu Q, Gu S, Wu X. Associations between general and abdominal obesity and incident diabetic neuropathy in participants with type 2 diabetes mellitus. J Diabetes (2021) 13(1):33–42. doi: 10.1111/1753-0407.13075
53. de Ritter R, Sep SJS, van der Kallen CJH, van Greevenbroek MMJ, de Jong M, Vos RC, et al. Sex differences in the association of prediabetes and type 2 diabetes with microvascular complications and function: The maastricht study. Cardiovasc Diabetol (2021) 20(1):102. doi: 10.1186/s12933-021-01290-x
54. Fan B, Liu XS, Szalad A, Wang L, Zhang R, Chopp M, et al. Influence of sex on cognition and peripheral neurovascular function in diabetic mice. Front Neurosci (2018) 12:795. doi: 10.3389/fnins.2018.00795
55. de La Hoz CL, Cheng C, Fernyhough P, Zochodne DW. A model of chronic diabetic polyneuropathy: Benefits from intranasal insulin are modified by sex and RAGE deletion. . Am J Physiol Endocrinol Metab (2017) 312(5):E407–19. doi: 10.1152/ajpendo.00444.2016
56. Melcangi RC, Giatti S, Garcia–Segura LM. Levels and actions of neuroactive steroids in the nervous system under physiological and pathological conditions: Sex–specific features. Neurosci Biobehav Rev (2016) 67:25–40. doi: 10.1016/j.neubiorev.2015.09.023
Keywords: bone mineral density, nerve conduction velocity, type 2 diabetes mellitus, diabetic peripheral neuropathy, osteoporosis
Citation: Chen X-j, Wang X-f, Pan Z-c, Zhang D, Zhu K-c, Jiang T, Kong X-k, Xie R, Sun L-h, Tao B, Liu J-m and Zhao H-y (2023) Nerve conduction velocity is independently associated with bone mineral density in type 2 diabetes mellitus. Front. Endocrinol. 14:1109322. doi: 10.3389/fendo.2023.1109322
Received: 27 November 2022; Accepted: 09 February 2023;
Published: 20 February 2023.
Edited by:
Zhongjian Xie, Second Xiangya Hospital, Central South University, ChinaReviewed by:
Jill Slade, Michigan State University, United StatesCopyright © 2023 Chen, Wang, Pan, Zhang, Zhu, Jiang, Kong, Xie, Sun, Tao, Liu and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong-yan Zhao, aHlhbnpoYW9AMTYzLmNvbQ==; Jian-min Liu, bGptMTA1ODZAcmpoLmNvbS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.