 Hiroshi Kataoka
Hiroshi Kataoka Kosaku Nitta
Kosaku Nitta
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Endocrinol., 09 February 2023
Sec. Obesity
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1097596
This article is part of the Research TopicAdvances in Obesity Prevention, Treatment and Management: Lifecycle and Complex System ApproachesView all 19 articles
Visceral adipose tissue plays a central role in obesity and metabolic syndrome and is an independent risk factor for both cardiovascular and metabolic disorders. Increased visceral adipose tissue promotes adipokine dysregulation and insulin resistance, leading to several health issues, including systemic inflammation, oxidative stress, and activation of the renin-angiotensin-aldosterone system. Moreover, an increase in adipose tissue directly and indirectly affects the kidneys by increasing renal sodium reabsorption, causing glomerular hyperfiltration and hypertrophy, which leads to increased proteinuria and kidney fibrosis/dysfunction. Although the interest in the adverse effects of obesity on renal diseases has grown exponentially in recent years, the relationship between obesity and renal prognosis remains controversial. This may be attributed to the long clinical course of obesity, numerous obesity-related metabolic complications, and patients’ attributes. Multiple individual attributes influencing the pathophysiology of fat accumulation make it difficult to understand obesity. In such cases, it may be effective to elucidate the pathophysiology by conducting research tailored to individual attributes from the perspective of attribute-based medicine/personalized medicine. We consider the appropriate use of clinical indicators necessary, according to attributes such as chronic kidney disease stage, level of visceral adipose tissue accumulation, age, and sex. Selecting treatments and clinical indicators based on individual attributes will allow for advancements in the clinical management of patients with obesity and chronic kidney disease. In the clinical setting of obesity-related nephropathy, it is first necessary to accumulate attribute-based studies resulting from the accurate evaluation of visceral fat accumulation to establish evidence for promoting personalized medicine.
Accumulated epidemiologic evidence indicates that being overweight and obese are risk factors for chronic kidney disease (CKD) (1–4) and end-stage kidney disease (ESKD) (5–8); additionally, the causal link between obesity and CKD has been extensively reviewed (9–11). Visceral fat accumulation is the central pathological condition in obesity/metabolic syndrome (12–15) and is significantly associated with atherosclerosis (14), hypertension (16, 17), and metabolic impairments, including hyperglycemia/diabetes mellitus (17–19), hypertriglyceridemia (17), low high-density lipoprotein (HDL) cholesterol (17, 20), hyperuricemia (21, 22), high C-reactive protein concentration (14, 17), fatty liver (14), cardiovascular disease (CVD) (23), and kidney disease (24, 25). Nevertheless, at present, no clinical practice guidelines for obesity-related glomerulopathy (ORG) have been established. This narrative review provides an overview of visceral fat and obesity-related kidney disease and its clinical indicators, aiming to generate novel ideas for future studies and clinical applications focusing on attribute-based medicine/personalized medicine.
The pathophysiology of obesity/visceral fat accumulation is complex, with numerous interrelated aspects, including a sedentary lifestyle, individual dietary habits, genetic predisposition, and environmental factors (26–29). Visceral adipose tissue (VAT) plays a central role in being overweight and obese (30–34), whereas subcutaneous fat tissue is considered benign or protective (35, 36). Increased visceral fat accumulation causes adipose tissue inflammation and adipokine dysregulation (30–34), which can lead to dyslipidemia, insulin resistance (32, 37), chronic systemic inflammation (32, 38, 39), oxidative stress (30), brain melanocortin system stimulation (38, 40), sympathetic nervous system overactivation (40–42), renin-angiotensin-aldosterone system (RAAS) overactivation (43–47), mineralocorticoid receptor activation (48), sodium retention (49, 50), and extracellular fluid volume expansion (50–52). Increased visceral fat accumulation is also accompanied with perirenal and renal sinus fat accumulation, which causes high intrarenal pressure, which leads to compression of the vasa recta capillaries and thin loops of Henle, reduced blood flow in the renal medulla, increased sodium reabsorption in the loop of Henle, RAAS activation, and increased sodium reabsorption (50, 53, 54). These pathological conditions interact in a complex manner, ultimately damaging the kidneys by causing glomerular hyperfiltration (55, 56) and inflammation (57, 58), both of which are characteristics of obesity-related kidney disease (50, 53, 54, 59–61).
Numerous studies in the last 20 years have investigated obesity, significantly elucidating the systemic pathology associated with visceral adiposity/obesity and the mechanism of kidney injury in patients with obesity (2, 62). However, while the number of patients with obesity and patients with ORG has continued to increase, treatment strategies for ORG generally have remained ineffective in clinical practice (63, 64). Although patients and medical staff understand that weight loss is a simple solution to obesity-related diseases, the clinical prognostic indicators for ORG are poorly established, as is the optimal treatment for individual patients, with no clinical practice guidelines for ORG (63, 65, 66).
The following issues may have led to some confusion in studies and the creation of a knowledge gap regarding obesity-related neuropathy (1): the concept of the “obesity paradox,” in which protective effects of obesity have been observed in certain patient populations [e.g., ESKD patients (67, 68)] (2); the idea of a “metabolically healthy obesity phenotype” (69, 70) (3); the biphasic clinical change in the estimated glomerular filtration rate (eGFR) based on hyperfiltration during CKD progression in patients with obesity (56, 71) (4); the biphasic course of glomerular size during glomerular damage (72, 73) (5); the presence of many obesity-related complications and the long clinical course of obesity; and (6) the lack of evidence based on the precise measurement of visceral fat. Among these, though the concept of the “obesity paradox” remains controversial (67, 74–76), its existence has recently been questioned owing to concerns about the limitation of epidemiological studies (i.e., selection biases, confounding factors, influence of malnutrition), the inherent limitations of anthropometric measures, such as the body mass index (BMI), and the limitations of studies with short periods of observation (74, 77–82). As Kramer et al. (83) reported, multiple residual confounders and biases strongly affect the “obesity paradox.” Indeed, bariatric surgery, effective for multiple residual confounders, such as obesity-related complications, solves the “obesity paradox” by decreasing visceral fat accumulation and glomerular hyperfiltration, which are essential pathophysiological conditions of obesity (84, 85). Furthermore, the concept of a “metabolically healthy obesity phenotype” is also questioned by an accumulation of results considering the long clinical course of obesity. The “metabolically healthy obesity phenotype” is reportedly associated with low levels of VAT/ectopic fat, high levels of lower body subcutaneous fat storage, younger age, insulin sensitivity, increased adiponectin, a favorable lipoprotein profile, and non-Hispanic black race/ethnicity (18, 86). Meta-analyses of studies with a follow-up duration >10 years reported that individuals with “metabolically healthy obesity phenotype” are at an increased risk for CVD events (87, 88), with this risk increasing with a longer follow-up duration (89). The accumulation of studies that precisely evaluates visceral fat is an issue that remains to be addressed by researchers and clinicians worldwide.
Although there are various anthropometric and imaging measurement methods clinically available to assess adiposity (51, 80, 90), to fully clarify the pathophysiological condition in obesity, it is important to determine whether volumetric fat measurements can accurately characterize the heterogeneity of abdominal fat distribution between individuals (91). BMI and waist circumference are easy to examine and have been widely used to define obesity and abdominal obesity. Waist circumference has been used as an indicator closely associated with visceral fat (92). However, theoretically, both BMI and waist circumference cannot be used to distinguish between visceral and subcutaneous fat mass. Since VAT and SAT differ greatly in their functional significance and response to weight gain, anthropometric data alone is not sufficient for an accurate risk assessment of adiposity (80). Therefore, imaging methods need to be developed to identify individuals with excessive visceral adiposity (51). Imaging measurement of adiposity can be performed by various methods, including computed tomography (CT), magnetic resonance imaging (MRI), dual-energy X-ray absorptiometry, and electrical bioimpedance (93). Among these, only CT accurately measures visceral fat area (VFA) (94). CT can be performed rapidly and interpreted to segment adipose tissue deposits and measure their area or volume (80). CT produces high-resolution images conveniently and with high repeatability (94), providing accurate localization data (95). Although CT is expensive and exposes the patient to radiation, quantitative CT is currently the technology of choice for the measurement and analysis of VFA (96). At present, though CT and MRI are ideal methods to assess adiposity in clinical research (51, 93, 97), studies using visceral fat assessment evaluated by these techniques are still lacking.
In recent years, the concept of personalized medicine/precision medicine/tailored medicine has been developed alongside the concepts of patient-centered medicine (98, 99). In a clinical setting, personalized medicine can provide access to knowledge that either validates or alters a medical decision from one that is based on the evidence for the average patient to one that is based on the individual’s unique characteristics/attributes (100). In personalized medicine, patients are treated individually according to their individual heterogeneous characteristics (101, 102), with the advantages of the disaggregation of data and analyses of differences within sub-cohorts having been reported (102, 103). Recently developed artificial intelligence/machine learning has the potential to bring about the ideal personalized medicine (100, 104, 105). However, there are still issues that need to be resolved to establish personalized medicine for patients with CKD (100, 104). Fröhlich et al. identified the following challenges in data science (artificial intelligence [AI]/machine learning) for personalized medicine (1): insufficient prediction performance for clinical practice (2), difficulties in interpretation, and (3) insufficient validation for clinical practice (105). Indeed, unlike in genetic diseases (106) where personalized medicine can be applied according only to genetic mutations (107–110), most patients with CKD are affected by multiple risk factors for disease progression (111, 112). In patients with CKD, the risk factors and pathophysiological conditions generally differ regarding patient attributes (113). In patients with obesity and CKD, multiple attributes, including age (114, 115), sex (116–119), race/ethnicity (17, 120), fat distribution (119, 121), the amount of VAT (119, 121, 122), and CKD stage (115), are known to more intricately influence the pathophysiology of fat accumulation and cardiorenal metabolic disease (51, 80). Such complex interactions of chronic diseases with obesity raise the difficulty of interpretation of pathophysiology, prognosis prediction, and validation in a clinical setting.
In such a multifactorial disease like CKD, we consider that attribute-based medicine (113, 123), supported by attributes/characteristics (100, 105) such as sex and age, is useful for the establishment of personalized medicine. That is, instead of jumping from traditional medicine in an entire cohort to personalized medicine in individuals, we interpose a step (attribute-based medicine) to bridge both approaches. Attribute-based medicine can help solve the challenges enumerated by Fröhlich et al. (105) by increasing the future accuracy of machine learning predictions, enabling patients and clinicians to interpret machine learning-generated predictions, and making it easier to validate in the clinical setting. Attribute-based medicine may provide a bridge between traditional statistical research and personalized medicine.
Before devising personalized medicine approaches in patients with CKD, high-quality databases must be created and risk factors for the acceleration of the CKD progression must be identified (113, 115, 118, 119, 124–129), paying attention to attributes such as sex differences or ages (130, 131). Indeed, it has been reported that even data used in AI should be divided according to sex and attribute, which makes collecting data disaggregated by age and sex essential if AI is to fulfill its promise of improving outcomes for everyone (132–135). Therefore, from the standpoint of patient-centered medicine, women and the elderly should be treated based on research evidence from female (131, 136–139) and geriatric cohorts (140–142), respectively. In chronic diseases, sex and age are important modifiers of pathophysiology and disease development. However, data disaggregated by age, sex, or obesity are still scarcely available from prospective studies (132, 137). To establish research supporting precision/personalized medicine, it is necessary to conduct further large-scale studies which include the analyses of disaggregated data (143).
In cardiology, sex-specific CVD risk assessment using CT or MRI-based fat measures has already been validated (144, 145). In nephrology, human studies on visceral fat and kidney prognosis have established clear evidence for kidney prognosis, especially regarding sex-specific differences (51, 144, 146). Several indicators that reflect obesity, such as BMI, waist circumference, VFA, and the visceral-to-subcutaneous fat ratio (V/S ratio), seem to explain CKD progression. However, the rationale and merits of various indicators likely vary and are insufficient to establish strong evidence (119, 147–152). Therefore, to address the gaps in knowledge regarding the pathophysiology of obesity and its impact on kidney disease, it will be important to accurately assess volumetric fat measurements to clearly characterize the heterogeneity of abdominal fat distribution between individuals and the differences in fat distribution between sexes (91). In this regard, CT- or MRI-based measures should be more indicated to study the effect of VAT on kidney disease.
Among the multiple attributes influencing the pathophysiology of fat accumulation, sex differences in visceral adiposity and CKD progression are particularly important. Firstly, sex hormones have important roles in the accumulation and distribution of body fat (153). As a result, fat distribution significantly differs between the sexes, as men have relatively more visceral fat and women have relatively more subcutaneous fat (36, 154). Furthermore, men have higher levels of visceral fat (155) than premenopausal women, with the decline in estrogen levels upon menopause being associated with an increase in visceral fat in women (156). Post-menopause, the amount of estrogen secreted from the ovaries dramatically diminishes, resulting in a decrease in brain anorexigenic signaling through estrogen, evoking the storage of lipids in visceral fat, a major source of estrogen in postmenopausal women (157, 158).
Secondly, premenopausal women are generally protected from CVDs due to the activation of RAAS, with a previously established involvement of estrogen in this mechanism (159, 160). Although the angiotensin-converting enzyme/angiotensin II/angiotensin receptor 1 (ACE/Ang II/AT1R) axis plays a major role in the classic renin-angiotensin signaling pathway, namely in water and salt retention, vasoconstriction, and in proliferative, proinflammatory, and profibrotic processes (161), estrogen has been reported to reduce the activation of that axis (162, 163). Estrogen reduces ACE activity (164), AT1R expression (165, 166), and aldosterone production in animal models (167). Men and postmenopausal women have higher renin activity and levels (168, 169), as well as increased plasma aldosterone levels (170), than premenopausal women. These increases in RAAS activation and visceral fat in postmenopausal women can be avoided by estrogen replacement therapy (169, 171–173). Furthermore, estrogen shifts the balance toward the AT2R/ACE2/Ang- (1–7)/mitochondrial assembly receptor (MasR) axis [the protective/depressor renin-angiotensin signaling pathways (174)], which opposes the pressor actions of AT1R (160). Obesity is associated with the activation of the ACE/Ang II/AT1R axis (175, 176), with the overactivation of Ang II in obesity stimulating AT1R to promote hypertension, insulin resistance, and energy imbalance (176). However, the protective estrogen-RAAS interactions via AT2R/ACE2/Ang- (1–7)/MasR appear to be diminished by obesity (177) and aging (177), suggesting that the protective effect against CVD in women may be attenuated by an increase in visceral fat. Indeed, in human studies, the various vasoprotective effects of estrogen, including vasodilation, anti-inflammatory properties, and lipid profile decline, are nonexistent in hyperglycemic states and obesity (178–180). Features associated with obesity or metabolic syndrome in women generally emerge after menopause (181, 182), which may induce a concurrent progression of CKD (183–186).
Men with CKD generally have a worse prognosis than women, which leads to a substantially higher proportion of men with ESKD (187–189). Women seem to be protected against the development and progression of CKD (183, 190, 191), and the presence of estrogen further protects against kidney injury (192). Although the pathological mechanism underlying the sex-specific differences in CKD has not yet been completely elucidated, sex-specific differences in visceral fat accumulation (157, 158) are associated with sex-specific differences in CKD progression (20, 115, 119, 193, 194). For example, in a representative multicenter CKD study in Japan, using a ≥50% eGFR decline or ESKD as the endpoints, the sex-based Kaplan–Meier survival curves revealed that the kidney survival rate was significantly lower in men than in women among nonelderly patients (age <65 years) (113).
In Japan, the clustered number of metabolic syndrome components is greater than 1.0 for individuals with a VFA ≥100 cm2 (13), with the best combination of sensitivity and specificity for determining patients with multiple risk factors identified for a VFA cutoff of 100 cm2 (13). Furthermore, VFA ≥100 cm2 is used as a diagnostic criterion for metabolic syndrome in Japan (12), with patients having VFA ≥100 cm2 being at risk for cardiovascular (195, 196), coronary artery (197), and cerebral small vessel (198) diseases. Although, generally, there are sex differences in waist circumference criteria for metabolic syndrome (199), it has been reported that there is no sex difference in the metabolic significance of the amount of visceral fat (196, 200). The mean number of obesity-related cardiovascular risk factors exceeded 1.0 at 100 cm2 of VFA both in men and women (196). These results indicate the significance of differentiating patients according to a 100 cm2 VFA threshold (201), regardless of sex, as well as highlight the need for studies based on the 100 cm2 threshold VFA value.
In kidney disease, the presence of metabolic syndrome (202) and a VFA ≥100 cm2 (115) are associated with CKD progression. Interestingly, a VFA ≥100 cm2 significantly interacted with the V/S ratio in terms of the renal prognosis (119). As metabolic complications are increased with a VFA ≥100 cm2 (115), the significance of VFA or V/S ratio in patients with a VFA ≥100 cm2 seems to become relatively less important. However, considering that many metabolic complications develop based on obesity, patients with a VFA ≥100 cm2 need not only medical intervention for each metabolic disease but also a reduction of excessive visceral fat itself (200).
As menopause influences obesity among women, it is clinically important to consider the influence of aging itself. Indeed, for women aged <55 years, which includes both pre- and menopausal statuses, VFA is markedly lower (median value, 59.8 cm2), with considerably fewer obesity-related cardiovascular risk factors, than for women ≥55 years of age or men (196). The average VFA increased with age in both men and women, above the 100 cm2 threshold after the age of 40 years in men, and close to the 100 cm2 threshold after the age of 60 years in women (196), with the mean number of obesity-related cardiovascular risk factors being >1.0 at ages 40 years in men and 60 years in women (196). Therefore, prevention of obesity-related diseases is required at an earlier stage for men than for women (200). On the other hand, though the incidence of CVDs in women lags behind men by 10 to 20 years (203), women generally live longer than men (160). Therefore, obesity management in postmenopausal women should not also be neglected.
Systemic renin and aldosterone levels decrease with age due to decreased renin production and release (204). It has been reported that older individuals have lower plasma renin and aldosterone levels compared with younger controls (205, 206), with impaired responses to RAAS stimuli, such as sodium depletion, hyperkalemia, and upright posture (207, 208), in older individuals (especially in late-elderly individuals). Generally, the rate of CKD progression is slow in elderly individuals (209–212). Although the reason for this has not been elucidated in human clinical studies, we consider that decreased systemic RAAS activation/glomerular hyperfiltration/glomerular hypertrophy axis (73, 129, 204) may be a factor. Although, the presence of diabetes mellitus (DM) (209, 213) and an increased BMI (213) are associated with kidney disease progression in elderly individuals, when patients with CKD are analyzed using cross-classification approach in detail (113), interestingly, DM alone was not an aggravating factor for renal prognosis in non-obese patients with CKD aged ≥65 years. In patients with CKD aged ≥65 years, poor kidney prognosis was observed only when both DM and obesity were present (113). This implies a decrease in RAAS activation in patients with CKD aged ≥65 years, and simultaneouslysuggests that attention should be paid to the overlapping of obesity and DM even in the elderly. The age-based Kaplan–Meier survival curves revealed that the kidney survival rate was significantly lower in obese patients with DM and a BMI ≥25 kg/m2 (4 years survival, 57.8%) than in non-obese patients with DM and a BMI <25 kg/m2 (4 years survival, 70.7%) (113). As RAAS overactivation (43–47) is one of the important pathologies contributing to obesity/metabolic syndrome and DM, the effects of RAAS activation among elderly individuals with obesity should be examined more specifically in future studies.
Currently, the biggest challenge in promoting attribute-based medicine for patients with CKD is the lack of evidence regarding visceral fat and kidney disease progression. We conducted a literature search in the PubMed database in December 2022 using the keywords “visceral fat,” “kidney,” and “outcome,” which yielded 130 relevant articles. Among these, only three studies from two cohorts reported statistically significant associations between obesity evaluated by visceral fat measured using CT or MRI and CKD progression (kidney function decline) over a >2-year longitudinal observation period (Table 1). One of these studies, from the cohort reported by Madero et al. (148), confirmed the association between VFA measured on CT and kidney function decline, defined as a decrease in eGFR of >30% during a median follow-up of 8.9 years; their recruited patients were limited to individuals aged 70–79 years (Table 1, upper line). The other two reports were from our cohort (115, 119). Manabe et al. (115) found that VFA was significantly associated with CKD progression in a cohort with a wide age range (mean age, 59.2 years). The hazard ratios of VFA regarding CKD progression were higher in patients with VFA <100 cm2 than in patients with VFA ≥100 cm2 but did not differ between sexes (Table 1, middle line). The study by Kataoka et al. (119) was the first to show that the V/S ratio was significantly associated with CKD progression, particularly in the sub-cohort of VFA <100 cm2 compared with that of VFA ≥100 cm2 (P-value for interaction <0.01). Additionally, the hazard ratios of the V/S ratio regarding CKD progression were higher in women than in men (Table 1, lower line). Therefore, in women and patients with low visceral adiposity, the V/S ratio appears to be an early indicator of CKD progression. In this manner, the studies on visceral fat measured by CT are suggestive of an association between visceral fat accumulation and CKD progression. However, sufficient evidence is not present to guide clinical decision-making; further studies with longer observation periods are necessary to detect unhealthy obesity. Furthermore, as patients with obesity or advanced CKD generally have many complications and risk factors (113), we expect that large-scale studies that appropriately manage confounding factors will be reported in the future.
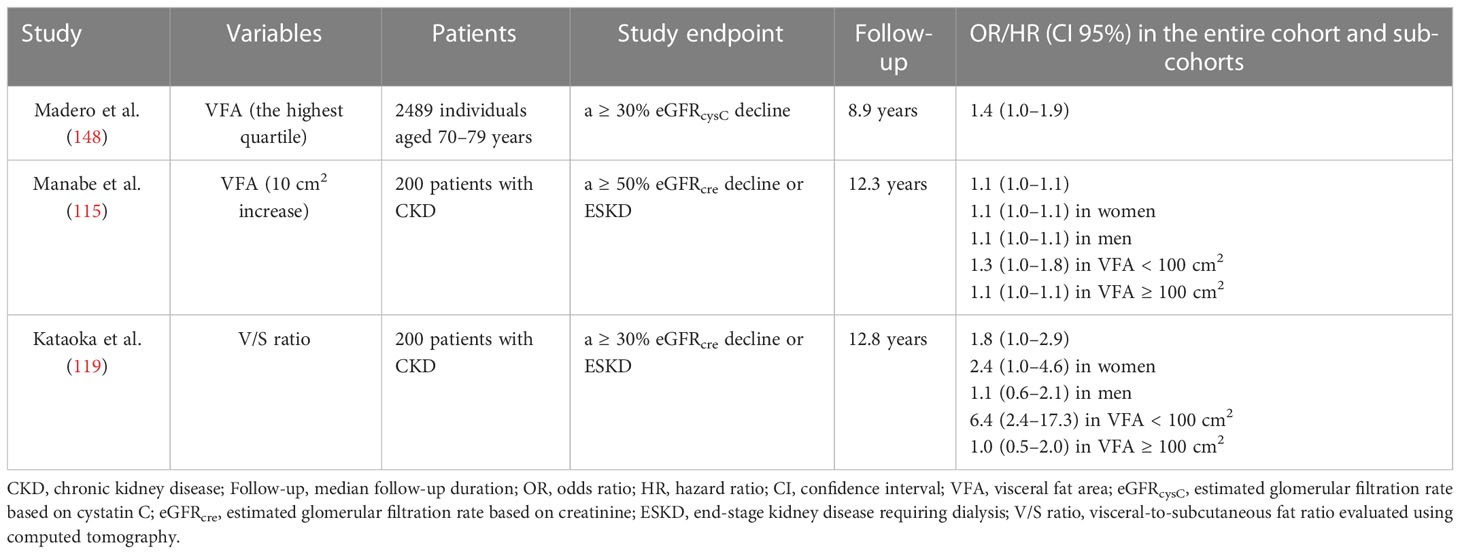
Table 1 Risks of visceral fat indicators for CKD progression.
Attribute-based medical care and research are the first steps to developing personalized medicine. However, at present, attribute-based medical care is not widespread enough to provide individual medical care in a clinical setting. Although much has been elucidated about the pathophysiology of kidney injury in patients with obesity, data from human studies on visceral fat and kidney prognosis are insufficient to establish the necessary evidence for attribute-based medicine in obesity-related renal pathologies. The accumulation of larger and longer-term studies focusing on specific attributes is necessary to resolve the existing controversy, especially concerning sex-specific kidney disease prognosis.
HK performed the literature search and wrote the manuscript. KN and JH were involved in planning and supervising the work. All authors contributed to the article and approved the submitted version.
This study was partly supported by a Grant-in-Aid for Intractable Renal Diseases Research and Research on Rare and Intractable Diseases, as well as by Health and Labor Sciences Research Grants from the Ministry of Health, Labor and Welfare of Japan.
The authors appreciate the advice on the cross-classification approach by Dr. Takahiro Mochizuki (deceased June 25, 2017) and his contribution to medical care and medical research in Japan.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wang Y, Chen X, Song Y, Caballero B, Cheskin LJ. Association between obesity and kidney disease: A systematic review and meta-analysis. Kidney Int (2008) 73(1):19–33. doi: 10.1038/sj.ki.5002586
2. Hsu C-y, McCulloch C, Iribarren C, Darbinian J, Go A. Body mass index and risk for end-stage renal disease. Ann Internal Med (2006) 144(1):21–8. doi: 10.7326/0003-4819-144-1-200601030-00006
3. Serra A, Romero R, Lopez D, Navarro M, Esteve A, Perez N, et al. Renal injury in the extremely obese patients with normal renal function. Kidney Int (2008) 73(8):947–55. doi: 10.1038/sj.ki.5002796
4. Yamagata K, Ishida K, Sairenchi T, Takahashi H, Ohba S, Shiigai T, et al. Risk factors for chronic kidney disease in a community-based population: A 10-year follow-up study. Kidney Int (2007) 71(2):159–66. doi: 10.1038/sj.ki.5002017
5. Zoccali C. The obesity epidemics in ESRD: from wasting to waist? Nephrol Dialysis Transplant (2009) 24(2):376–80. doi: 10.1093/ndt/gfn589
6. Iseki K, Ikemiya Y, Kinjo K, Inoue T, Iseki C, Takishita S. Body mass index and the risk of development of end-stage renal disease in a screened cohort. Kidney Int (2004) 65(5):1870–6. doi: 10.1111/j.1523-1755.2004.00582.x
7. Vivante A, Golan E, Tzur D, Leiba A, Tirosh A, Skorecki K, et al. Body mass index in 1.2 million adolescents and risk for end-stage renal disease. Arch Internal Med (1960) (2012) 172(21):1644–50. doi: 10.1001/2013.jamainternmed.85
8. Chang A, Grams M, Ballew S, Bilo H, Correa A, Evans M, et al. Adiposity and risk of decline in glomerular filtration rate: Meta-analysis of individual participant data in a global consortium. BMJ: Br Med J (2019) 364:k5301–1. doi: 10.1136/bmj.k5301
9. Docherty N, le Roux C. Bariatric surgery for the treatment of chronic kidney disease in obesity and type 2 diabetes mellitus. Nat Rev Nephrology. (2020) 16(12):709–20. doi: 10.1038/s41581-020-0323-4
10. Garofalo C, Borrelli S, Minutolo R, Chiodini P, De Nicola L, Conte G. A systematic review and meta-analysis suggests obesity predicts onset of chronic kidney disease in the general population. Kidney Int (2017) 91(5):1224–35. doi: 10.1016/j.kint.2016.12.013
11. Xu H, Kuja Halkola R, Chen X, Magnusson PKE, Svensson P, Carrero J-J. Higher body mass index is associated with incident diabetes and chronic kidney disease independent of genetic confounding. Kidney Int (2019) 95(5):1225–33. doi: 10.1016/j.kint.2018.12.019
12. Committee to Evaluate Diagnostic Standards for Metabolic Syndrome. Nihon Naika Gakkai Zasshi (2005) 94(4):794–809.
13. The Examination Committee of Criteria for 'Obesity Disease' in Japan, Japan Society for the Study of Obesity. New criteria for 'obesity disease' in Japan. Circ J Off J Japanese Circ Soc (2002) 66(11):987–92. doi: 10.1253/circj.66.987
14. Neeland I, Ayers C, Rohatgi A, Turer A, Berry J, Das S, et al. Associations of visceral and abdominal subcutaneous adipose tissue with markers of cardiac and metabolic risk in obese adults. Obesity. (2013) 21(9):E439–47. doi: 10.1002/oby.20135
15. Matsuzawa Y, Funahashi T, Nakamura T. The concept of metabolic syndrome: Contribution of visceral fat accumulation and its molecular mechanism. J Atheroscl Thrombosis. (2011) 18(8):629–39. doi: 10.5551/jat.7922
16. Chandra A, Neeland I, Berry J, Ayers C, Rohatgi A, Das S, et al. The relationship of body mass and fat distribution with incident hypertension: Observations from the Dallas heart study. J Am Coll Cardiol (2014) 64(10):997–1002. doi: 10.1016/j.jacc.2014.05.057
17. Nazare J-A, Smith J, Borel A-L, Haffner S, Balkau B, Ross R, et al. Ethnic influences on the relations between abdominal subcutaneous and visceral adiposity, liver fat, and cardiometabolic risk profile: The international study of prediction of intra-abdominal adiposity and its relationship with cardiometabolic Risk/Intra-abdominal adiposity. Am J Clin Nutr (2012) 96(4):714–26. doi: 10.3945/ajcn.112.035758
18. Neeland I, Turer A, Ayers C, Powell Wiley T, Vega G, Farzaneh Far R, et al. Dysfunctional adiposity and the risk of prediabetes and type 2 diabetes in obese adults. JAMA: J Am Med Assoc (2012) 308(11):1150–9. doi: 10.1001/2012.jama.11132
19. Boyko EJ, Fujimoto WY, Leonetti DL, Newell Morris L. Visceral adiposity and risk of type 2 diabetes: A prospective study among Japanese americans. Diabetes Care (2000) 23(4):465–71. doi: 10.2337/diacare.23.4.465
20. Kawachi K, Kataoka H, Manabe S, Mochizuki T, Nitta K. Low HDL cholesterol as a predictor of chronic kidney disease progression: A cross-classification approach and matched cohort analysis. Heart Vessels. (2019) 34(9):1440–55. doi: 10.1007/s00380-019-01375-4
21. Tamba S, Nishizawa H, Funahashi T, Okauchi Y, Ogawa T, Noguchi M, et al. Relationship between the serum uric acid level, visceral fat accumulation and serum adiponectin concentration in Japanese men. Internal Med (2008) 47(13):1175–80. doi: 10.2169/internalmedicine.47.0603
22. Yamada A, Sato KK, Kinuhata S, Uehara S, Endo G, Hikita Y, et al. Association of visceral fat and liver fat with hyperuricemia. Arthritis Care Res (2016) 68(4):553–61. doi: 10.1002/acr.22729
23. Neeland I, Turer A, Ayers C, Berry J, Rohatgi A, Das S, et al. Body fat distribution and incident cardiovascular disease in obese adults. J Am Coll Cardiol (2015) 65(19):2150–1. doi: 10.1016/j.jacc.2015.01.061
24. Hayashi T, Boyko EJ, Leonetti DL, McNeely MJ, Newell-Morris L, Kahn SE, et al. Visceral adiposity and the prevalence of hypertension in Japanese americans. Circulation (2003) 108(14):1718–23. doi: 10.1161/01.CIR.0000087597.59169.8D
25. Tamba S, Nakatsuji H, Kishida K, Noguchi M, Ogawa T, Okauchi Y, et al. Relationship between visceral fat accumulation and urinary albumin-creatinine ratio in middle-aged Japanese men. Atheroscl (Amsterdam). (2010) 211(2):601–5. doi: 10.1016/j.atherosclerosis.2010.02.037
26. Johnson RJ, Segal MS, Sautin Y, Nakagawa T, Feig DI, Kang DH, et al. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease. Am J Clin Nutr (2007) 86(4):899–906. doi: 10.1093/ajcn/86.4.899
27. Kataoka H, Ariyama Y, Deushi M, Osaka M, Nitta K, Yoshida M. Inhibitory effect of serotonin antagonist on leukocyte-endothelial interactions In vivo and in vitro. PloS One (2016) 11(1):e0147929. doi: 10.1371/journal.pone.0147929
28. Tchernof A, Despres JP. Pathophysiology of human visceral obesity: An update. Physiol Rev (2013) 93(1):359–404. doi: 10.1152/physrev.00033.2011
29. Sharma I, Liao Y, Zheng X, Kanwar Y. New pandemic: Obesity and associated nephropathy. Front Med (2021) 8:673556–6. doi: 10.3389/fmed.2021.673556
30. Hosogai N, Fukuhara A, Oshima K, Miyata Y, Tanaka S, Segawa K, et al. Adipose tissue hypoxia in obesity and its impact on adipocytokine dysregulation. Diabetes. (2007) 56(4):901–11. doi: 10.2337/db06-0911
31. Hall JE, da Silva AA, do Carmo JM, Dubinion J, Hamza S, Munusamy S, et al. Obesity-induced hypertension: Role of sympathetic nervous system, leptin, and melanocortins. J Biol Chem (2010) 285(23):17271–6. doi: 10.1074/jbc.R110.113175
32. Gregor M, Hotamisligil G. Inflammatory mechanisms in obesity. Annu Rev Immunol (2011) 29:415–45. doi: 10.1146/annurev-immunol-031210-101322
33. Ouchi N, Parker J, Lugus J, Walsh K. Adipokines in inflammation and metabolic disease. Nat Rev Immunol (2011) 11(2):85–97. doi: 10.1038/nri2921
34. Sharma K, Ramachandrarao S, Qiu G, Usui HK, Zhu Y, Dunn SR, et al. Adiponectin regulates albuminuria and podocyte function in mice. J Clin Invest (2008) 118(5):1645–56. doi: 10.1172/jci32691
35. Veilleux A, Caron Jobin M, Noël S, Laberge P, Tchernof A. Visceral adipocyte hypertrophy is associated with dyslipidemia independent of body composition and fat distribution in women. Diabetes. (2011) 60(5):1504–11. doi: 10.2337/db10-1039
36. Shi H, Strader A, Woods S, Seeley R. The effect of fat removal on glucose tolerance is depot specific in male and female mice. AJP-Endocrinology Metab (2007) 293(4):E1012–20. doi: 10.1152/ajpendo.00649.2006
37. Spoto B, Pisano A, Zoccali C. Insulin resistance in chronic kidney disease: A systematic review. Am J Physiol Renal Physiol (2016) 1;311(6):F1087–108. doi: 10.1152/ajprenal.00340.2016
38. Jais A, Brüning J. Hypothalamic inflammation in obesity and metabolic disease. J Clin Invest (2017) 127(1):24–32. doi: 10.1172/JCI88878
39. Hotamisligil G. Inflammation and metabolic disorders. Nature. (2006) 444(7121):860–7. doi: 10.1038/nature05485
40. Shi Z, Wong J, Brooks V. Obesity: Sex and sympathetics. Biol Sex Differences. (2020) 11(1):10–0. doi: 10.1186/s13293-020-00286-8
41. Alvarez G, Beske S, Ballard T, Davy K. Sympathetic neural activation in visceral obesity. Circulation. (2002) 106(20):2533–6. doi: 10.1161/01.CIR.0000041244.79165.25
42. Brooks V, Shi Z, Holwerda S, Fadel P. Obesity-induced increases in sympathetic nerve activity: Sex matters. Autonomic Neurosci (2015) 187:18–26. doi: 10.1016/j.autneu.2014.11.006
43. Gupte M, Thatcher S, Boustany Kari C, Shoemaker R, Yiannikouris F, Zhang X, et al. Angiotensin converting enzyme 2 contributes to sex differences in the development of obesity hypertension in C57BL/6 mice. Arteriosclerosis Thromb Vasc Biol (2012) 32(6):1392–9. doi: 10.1161/ATVBAHA.112.248559
44. Xue B, Yu Y, Zhang Z, Guo F, Beltz T, Thunhorst R, et al. Leptin mediates high-fat diet sensitization of angiotensin II-elicited hypertension by upregulating the brain renin-angiotensin system and inflammation. Hypertension. (2016) 67(5):970–6. doi: 10.1161/HYPERTENSIONAHA.115.06736
45. Engeli S, Böhnke J, Gorzelniak K, Janke J, Schling P, Bader M, et al. Weight loss and the renin-angiotensin-aldosterone system. Hypertension. (2005) 45(3):356–62. doi: 10.1161/01.HYP.0000154361.47683.d3
46. Tuck ML, Sowers J, Dornfeld L, Kledzik G, Maxwell M. The effect of weight reduction on blood pressure, plasma renin activity, and plasma aldosterone levels in obese patients. New Engl J Med (1981) 304(16):930–3. doi: 10.1056/NEJM198104163041602
47. Achard V, Boullu Ciocca S, Desbriere R, Nguyen G, Grino M. Renin receptor expression in human adipose tissue. AJP-Regulatory Integr Comp Physiol (2007) 292(1):R274–82. doi: 10.1152/ajpregu.00439.2005
48. de Paula R, da Silva A, Hall J. Aldosterone antagonism attenuates obesity-induced hypertension and glomerular hyperfiltration. Hypertension. (2004) 43(1):41–7. doi: 10.1161/01.HYP.0000105624.68174.00
49. Hall J. The kidney, hypertension, and obesity. Hypertension. (2003) 41(3):625–33. doi: 10.1161/01.HYP.0000052314.95497.78
50. Hall J, do Carmo J, da Silva A, Wang Z, Hall M. Obesity, kidney dysfunction and hypertension: Mechanistic links. Nat Rev Nephrology. (2019) 15(6):367–85. doi: 10.1038/s41581-019-0145-4
51. Neeland I, Ross R, Després J-P, Matsuzawa Y, Yamashita S, Shai I, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. Lancet Diabetes Endocrinology. (2019) 7(9):715–25. doi: 10.1016/S2213-8587(19)30084-1
52. da Silva A, do Carmo J, Li X, Wang Z, Mouton A, Hall J. Role of hyperinsulinemia and insulin resistance in hypertension: Metabolic syndrome revisited. Can J Cardiol (2020) 36(5):671–82. doi: 10.1016/j.cjca.2020.02.066
53. Kotsis V, Martinez F, Trakatelli C, Redon J. Impact of obesity in kidney diseases. Nutrients. (2021) 13(12):4482. doi: 10.3390/nu13124482
54. Praga M, Morales E. The fatty kidney: Obesity and renal disease. Nephron. (2017) 136(4):273–6. doi: 10.1159/000447674
55. Chagnac A, Herman M, Zingerman B, Erman A, Rozen-Zvi B, Hirsh J, et al. Obesity-induced glomerular hyperfiltration: Its involvement in the pathogenesis of tubular sodium reabsorption. Nephrology dialysis Transplant Off Publ Eur Dialysis Transplant Assoc - Eur Renal Assoc (2008) 23(12):3946–52. doi: 10.1093/ndt/gfn379
56. Chagnac A, Zingerman B, Rozen Zvi B, Herman Edelstein M. Consequences of glomerular hyperfiltration: The role of physical forces in the pathogenesis of chronic kidney disease in diabetes and obesity. Nephron journals. (2019) 143(1):38–42. doi: 10.1159/000499486
57. Wu Y, Liu Z, Xiang Z, Zeng C, Chen Z, Ma X, et al. Obesity-related glomerulopathy: Insights from gene expression profiles of the glomeruli derived from renal biopsy samples. Endocrinology. (2006) 147(1):44–50. doi: 10.1210/en.2005-0641
58. Liu Y, Wang L, Luo M, Chen N, Deng X, He J, et al. Inhibition of PAI-1 attenuates perirenal fat inflammation and the associated nephropathy in high-fat diet-induced obese mice. AJP-Endocrinology Metab (2019) 316(2):E260–7. doi: 10.1152/ajpendo.00387.2018
59. Martínez Montoro J, Morales E, Cornejo Pareja I, Tinahones F, Fernández García J. Obesity-related glomerulopathy: Current approaches and future perspectives. Obes Rev (2022) 23(7):e13450–0. doi: 10.1111/obr.13450
60. D'Agati VD, Chagnac A, de Vries AP, Levi M, Porrini E, Herman-Edelstein M, et al. Obesity-related glomerulopathy: Clinical and pathologic characteristics and pathogenesis. Nat Rev Nephrology. (2016) 12(8):453–71. doi: 10.1038/nrneph.2016.75
61. Wang M, Wang Z, Chen Y, Dong Y. Kidney damage caused by obesity and its feasible treatment drugs. Int J Mol Sci (2022) 23(2):747. doi: 10.3390/ijms23020747
62. Kambham N, Markowitz GS, Valeri AM, Lin J, D'Agati VD. Obesity-related glomerulopathy: An emerging epidemic. Kidney Int (2001) 59(4):1498–509. doi: 10.1046/j.1523-1755.2001.0590041498.x
63. Friedman A, Kaplan L, le Roux C, Schauer P. Management of obesity in adults with CKD. J Am Soc Nephrol (2021) 32(4):777–90. doi: 10.1681/ASN.2020101472
64. Kovesdy C, Furth S, Zoccali C. Obesity and kidney disease: Hidden consequences of the epidemic. Kidney Int (2017) 91(2):260–2. doi: 10.1016/j.kint.2016.10.019
65. Ikizler TA, Burrowes J, Byham Gray L, Campbell K, Carrero J-J, Chan W, et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am J Kidney diseases. (2020) 76(3 Suppl 1):S1–S107. doi: 10.1053/j.ajkd.2020.05.006
66. Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. 2020 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int (2020) 98(4S):S1–S115. doi: 10.1016/j.kint.2020.06.019
67. Tobias D, Manson J. The obesity paradox in type 2 diabetes and mortality. Am J Lifestyle Med (2018) 12(3):244–51. doi: 10.1177/1559827616650415
68. Donini L, Pinto A, Giusti A, Lenzi A, Poggiogalle E. Obesity or BMI paradox? beneath the tip of the iceberg. Front Nutr (2020) 7:53–3. doi: 10.3389/fnut.2020.00053
69. Bluher M. The distinction of metabolically 'healthy' from 'unhealthy' obese individuals. Curr Opin lipidology. (2010) 21(1):38–43. doi: 10.1097/MOL.0b013e3283346ccc
70. Bluher M. Are metabolically healthy obese individuals really healthy? Eur J Endocrinol (2014) 171(6):R209–19. doi: 10.1530/eje-14-0540
71. Melsom T, Nair V, Schei J, Mariani L, Stefansson VTN, Harder J, et al. Correlation between baseline GFR and subsequent change in GFR in Norwegian adults without diabetes and in pima indians. Am J Kidney diseases. (2019) 73(6):777–85. doi: 10.1053/j.ajkd.2018.11.011
72. Kataoka H, Ohara M, Honda K, Mochizuki T, Nitta K. Maximal glomerular diameter as a 10-year prognostic indicator for IgA nephropathy. Nephrology dialysis Transplant Off Publ Eur Dialysis Transplant Assoc - Eur Renal Assoc (2011) 26(12):3937–43. doi: 10.1093/ndt/gfr139
73. Kataoka H, Mochizuki T, Nitta K. Large Renal corpuscle: Clinical significance of evaluation of the largest renal corpuscle in kidney biopsy specimens. Contrib Nephrol. (2018) 195:20–30. doi: 10.1159/000486931
74. Han S, Boyko E. The evidence for an obesity paradox in type 2 diabetes mellitus. Diabetes Metab J (2018) 42(3):179–87. doi: 10.4093/dmj.2018.0055
75. Gravina G, Ferrari F, Nebbiai G. The obesity paradox and diabetes. Eating Weight Disord - Stud Anorexia Bulimia Obes (2021) 26(4):1057–68. doi: 10.1007/s40519-020-01015-1
76. Kalantar Zadeh K, Rhee C, Chou J, Ahmadi SF, Park J, Chen J, et al. The obesity paradox in kidney disease: How to reconcile it with obesity management. Kidney Int Rep (2017) 2(2):271–81. doi: 10.1016/j.ekir.2017.01.009
77. Banack H, Kaufman J. Does selection bias explain the obesity paradox among individuals with cardiovascular disease? Ann Epidemiol (2015) 25(5):342–9. doi: 10.1016/j.annepidem.2015.02.008
78. Lajous M, Banack H, Kaufman J, Hernán M. Should patients with chronic disease be told to gain weight? The obesity paradox and selection bias. Am J Med (2015) 128(4):334–6. doi: 10.1016/j.amjmed.2014.10.043
79. Loprinzi P. Application of the "Fat-but-Fit" paradigm in predicting 10-yr risk for an atherosclerotic cardiovascular disease (ASCVD) event using the pooled cohort risk equations among US adults. Int J Cardiol (2016) 202:297–9. doi: 10.1016/j.ijcard.2015.09.057
80. Neeland I, Poirier P, Després J-P. Cardiovascular and metabolic heterogeneity of obesity: Clinical challenges and implications for management. Circulation. (2018) 137(13):1391–406. doi: 10.1161/CIRCULATIONAHA.117.029617
81. Prado C, Gonzalez MC, Heymsfield S. Body composition phenotypes and obesity paradox. Curr Opin Clin Nutr Metab Care (2015) 18(6):535–51. doi: 10.1097/MCO.0000000000000216
82. Hällberg V, Kataja M, Lahtela J, Tarkka M, Inamaa T, Palomäki A. Obesity paradox disappears in coronary artery bypass graft patients during 20-year follow-up. Eur Heart J - Acute Cardiovasc Care (2017) 6(8):771–7. doi: 10.1177/2048872616633844
83. Kramer H, Dugas L, Shoham D. Obesity as an effect modifier of the risk of death in chronic kidney disease. Nephrology dialysis Transplant (2013) 28 Suppl 4:iv65–72. doi: 10.1093/ndt/gft242
84. Sheetz K, Gerhardinger L, Dimick J, Waits S. Bariatric surgery and long-term survival in patients with obesity and end-stage kidney disease. JAMA surgery. (2020) 155(7):581–8. doi: 10.1001/jamasurg.2020.0829
85. Sheetz K, Waits S. Unravelling the obesity paradox through bariatric surgery-reply. JAMA surgery. (2020) 155(12):1174–5. doi: 10.1001/jamasurg.2020.3793
86. Després J-P. Body fat distribution and risk of cardiovascular disease: An update. Circulation. (2012) 126(10):1301–13. doi: 10.1161/CIRCULATIONAHA.111.067264
87. Kramer CK, Zinman B, Retnakaran R. Are metabolically healthy overweight and obesity benign conditions? A systematic review and meta-analysis. Ann Internal Med (2013) 159(11):758–69. doi: 10.7326/0003-4819-159-11-201312030-00008
88. Zheng R, Zhou D, Zhu Y. The long-term prognosis of cardiovascular disease and all-cause mortality for metabolically healthy obesity: A systematic review and meta-analysis. J Epidemiol Community Health (1979-). (2016) 70(10):1024–31. doi: 10.1136/jech-2015-206948
89. Eckel N, Meidtner K, Kalle Uhlmann T, Stefan N, Schulze M. Metabolically healthy obesity and cardiovascular events: A systematic review and meta-analysis. Eur J Prev Cardiol (2016) 23(9):956–66. doi: 10.1177/2047487315623884
90. Cornier M-A, Després J-P, Davis N, Grossniklaus D, Klein S, Lamarche B, et al. Assessing adiposity: A scientific statement from the American heart association. Circulation. (2011) 124(18):1996–2019. doi: 10.1161/CIR.0b013e318233bc6a
91. Fox CS, Massaro JM, Hoffmann U, Pou KM, Maurovich-Horvat P, Liu CY, et al. Abdominal visceral and subcutaneous adipose tissue compartments: Association with metabolic risk factors in the framingham heart study. Circulation. (2007) 116(1):39–48. doi: 10.1161/CIRCULATIONAHA.106.675355
92. Noori N, Hosseinpanah F, Nasiri AA, Azizi F. Comparison of overall obesity and abdominal adiposity in predicting chronic kidney disease incidence among adults. J Renal Nutr Off J Council Renal Nutr Natl Kidney Foundation. (2009) 19(3):228–37. doi: 10.1053/j.jrn.2008.11.005
93. Pluta W, Dudzińska W, Lubkowska A. Metabolic obesity in people with normal body weight (MONW)-review of diagnostic criteria. Int J Environ Res Public Health (2022) 19(2):624. doi: 10.3390/ijerph19020624
94. Zang W, Zhu F, Yu Y. Computed tomography image analysis of body fat based on multi-image information. BioMed Res Int (2022) 2022:8265211–8265211. doi: 10.1155/2022/8265211
95. Berker D, Koparal S, Işik S, Paşaoğlu L, Aydin Y, Erol K, et al. Compatibility of different methods for the measurement of visceral fat in different body mass index strata. Diagn interventional radiology. (2010) 16(2):99–105. doi: 10.4261/1305-3825.DIR.2749-09.1
96. Cerit M, Şendur HN, Cindil E, Erbaş G, Yalçın MM, Cerit ET, et al. Quantification of liver fat content with ultrasonographic attenuation measurement function: Correlation with unenhanced multidimensional computerized tomography. Clin imaging. (2020) 65:85–93. doi: 10.1016/j.clinimag.2020.04.028
97. Jensen MD, Kanaley JA, Reed JE, Sheedy PF. Measurement of abdominal and visceral fat with computed tomography and dual-energy x-ray absorptiometry. Am J Clin Nutr (1995) 61(2):274–8. doi: 10.1093/ajcn/61.2.274
98. Sacristan JA. Patient-centered medicine and patient-oriented research: Improving health outcomes for individual patients. BMC Med Inf decision making. (2013) 13:6. doi: 10.1186/1472-6947-13-6
99. Bardes CL. Defining "patient-centered medicine. New Engl J Med (2012) 366(9):782–3. doi: 10.1056/NEJMp1200070
100. Johnson K, Wei W-Q, Weeraratne D, Frisse M, Misulis K, Rhee K, et al. Precision medicine, AI, and the future of personalized health care. Clin Trans Science. (2021) 14(1):86–93. doi: 10.1111/cts.12884
101. Kravitz RL, Duan N, Braslow J. Evidence-based medicine, heterogeneity of treatment effects, and the trouble with averages. Milbank quarterly. (2004) 82(4):661–87. doi: 10.1111/j.0887-378X.2004.00327.x
102. Sacristan JA. Exploratory trials, confirmatory observations: A new reasoning model in the era of patient-centered medicine. BMC Med Res methodology. (2011) 11:57. doi: 10.1186/1471-2288-11-57
103. Sacristan JA. Clinical research and medical care: Towards effective and complete integration. BMC Med Res methodology. (2015) 15:4. doi: 10.1186/1471-2288-15-4
104. Ushio Y, Kataoka H, Iwadoh K, Ohara M, Suzuki T, Hirata M, et al. Machine learning for morbid glomerular hypertrophy. Sci Rep (2022) 12(1):19155–5. doi: 10.1038/s41598-022-23882-7
105. Fröhlich H, Balling R, Beerenwinkel N, Kohlbacher O, Kumar S, Lengauer T, et al. From hype to reality: Data science enabling personalized medicine. BMC Med (2018) 16(1):150–0. doi: 10.1186/s12916-018-1122-7
106. Lan A, Corces MR. Deep learning approaches for noncoding variant prioritization in neurodegenerative diseases. Front Aging Neurosci (2022) 14:1027224–1027224. doi: 10.3389/fnagi.2022.1027224
107. Kataoka H, Yoshida R, Iwasa N, Sato M, Manabe S, Kawachi K, et al. Germline mutations for kidney volume in ADPKD. Kidney Int Rep (2022) 7(3):537–46. doi: 10.1016/j.ekir.2021.12.012
108. Kataoka H, Akagawa H, Ushio Y, Sato M, Manabe S, Makabe S, et al. Mutation type and intracranial aneurysm formation in autosomal dominant polycystic kidney disease. Stroke: Vasc Interventional Neurology. (2022) 2(5):e000203. doi: 10.1161/SVIN.121.000203
109. Kataoka H, Watanabe S, Sato M, Manabe S, Makabe S, Akihisa T, et al. Predicting liver cyst severity by mutations in patients with autosomal-dominant polycystic kidney disease. Hepatol Int (2021) 15(3):791–803. doi: 10.1007/s12072-021-10176-9
110. Kataoka H, Fukuoka H, Makabe S, Yoshida R, Teraoka A, Ushio Y, et al. Prediction of renal prognosis in patients with autosomal dominant polycystic kidney disease using PKD1/PKD2 mutations. J Clin Med (2020) 9(1):146. doi: 10.3390/jcm9010146
111. Nenov VD, Taal MW, Sakharova OV, Brenner BM. Multi-hit nature of chronic renal disease. Curr Opin Nephrol hypertension. (2000) 9(2):85–97. doi: 10.1097/00041552-200003000-00001
112. Taal MW, Brenner BM. Predicting initiation and progression of chronic kidney disease: Developing renal risk scores. Kidney Int (2006) 70(10):1694–705. doi: 10.1038/sj.ji.5001794
113. Kataoka H, Ono K, Mochizuki T, Hanafusa N, Imai E, Hishida A, et al. A body mass index-based cross-classification approach for the assessment of prognostic factors in chronic kidney disease progression. Kidney Blood Pressure Res (2019) 44(3):362–83. doi: 10.1159/000501021
114. Matsushita Y, Nakagawa T, Yamamoto S, Takahashi Y, Yokoyama T, Mizoue T, et al. Visceral fat area cutoff for the detection of multiple risk factors of metabolic syndrome in Japanese: The Hitachi health study. Obesity. (2012) 20(8):1744–9. doi: 10.1038/oby.2011.285
115. Manabe S, Kataoka H, Mochizuki T, Iwadoh K, Ushio Y, Kawachi K, et al. Impact of visceral fat area in patients with chronic kidney disease. Clin Exp nephrology. (2021) 25(6):608–20. doi: 10.1007/s10157-021-02029-4
116. Ju S, Yi H-S. Implication of sex differences in visceral fat for the assessment of incidence risk of type 2 diabetes mellitus. Diabetes Metab J (2022) 46(3):414–6. doi: 10.4093/dmj.2022.0089
117. Liu J, Fox C, Hickson D, May W, Hairston K, Carr JJ, et al. Impact of abdominal visceral and subcutaneous adipose tissue on cardiometabolic risk factors: the Jackson heart study. J Clin Endocrinol Metab (2010) 95(12):5419–26. doi: 10.1210/jc.2010-1378
118. Kataoka H, Ohara M, Mochizuki T, Iwadoh K, Ushio Y, Kawachi K, et al. Sex differences in time-series changes in pseudo-R(2) values regarding hyperuricemia in relation to the kidney prognosis. J Pers Med (2020) 26;10(4):248. doi: 10.3390/jpm10040248
119. Kataoka H, Mochizuki T, Iwadoh K, Ushio Y, Kawachi K, Watanabe S, et al. Visceral to subcutaneous fat ratio as an indicator of a >/=30% eGFR decline in chronic kidney disease. PloS One (2020) 15(11):e0241626. doi: 10.1371/journal.pone.0241626
120. Shah AD, Kandula NR, Lin F, Allison MA, Carr J, Herrington D, et al. Less favorable body composition and adipokines in south asians compared with other US ethnic groups: Results from the MASALA and MESA studies. Int J Obes (2016) 40(4):639–45. doi: 10.1038/ijo.2015.219
121. Yano Y, Vongpatanasin W, Ayers C, Turer A, Chandra A, Carnethon M, et al. Regional fat distribution and blood pressure level and variability: The Dallas heart study. Hypertension. (2016) 68(3):576–83. doi: 10.1161/HYPERTENSIONAHA.116.07876
122. Okauchi Y, Iwahashi H, Okita K, Funahashi T, Kishida K, Noguchi M, et al. Weight reduction is associated with improvement of glycemic control in Japanese men, whose hemoglobin A1C is 5.6-6.4%, with visceral fat accumulation, but not without visceral fat accumulation. J Diabetes Invest (2013) 4(5):454–9. doi: 10.1111/jdi.12084
123. Kataoka H, Mochizuki T, Ohara M, Tsuruta Y, Iwasa N, Yoshida R, et al. Urate-lowering therapy for CKD patients with asymptomatic hyperuricemia without proteinuria elucidated by attribute-based research in the FEATHER study. Sci Rep (2022)12(1):3784. doi: 10.1038/s41598-022-07737-9
124. Manabe S, Kataoka H, Mochizuki T, Iwadoh K, Ushio Y, Kawachi K, et al. Maximum carotid intima-media thickness in association with renal outcomes. J Atheroscler Thromb (2021) 28(5):491–505. doi: 10.5551/jat.57752
125. Kataoka H, Ohara M, Suzuki T, Inoue T, Akanuma T, Kawachi K, et al. Time series changes in pseudo-R2 values regarding maximum glomerular diameter and the Oxford MEST-c score in patients with IgA nephropathy: A long-term follow-up study. PloS One (2020) 15(5):e0232885. doi: 10.1371/journal.pone.0232885
126. Ushio Y, Kataoka H, Sato M, Manabe S, Watanabe S, Akihisa T, et al. Association between anemia and renal prognosis in autosomal dominant polycystic kidney disease: A retrospective study. Clin Exp nephrology. (2020) 24(6):500–8. doi: 10.1007/s10157-020-01856-1
127. Sato M, Kataoka H, Ushio Y, Manabe S, Watanabe S, Akihisa T, et al. High serum phosphate level as a risk factor to determine renal prognosis in autosomal dominant polycystic kidney disease: A retrospective study. Medicines (Basel) (2020) 12;7(3):13. doi: 10.3390/medicines7030013
128. Kataoka H, Tsuchiya K, Naganuma T, Okazaki M, Komatsu M, Kimura T, et al. Relationship between anaemia management at haemodialysis initiation and patient prognosis. Nephrol (Carlton Vic). (2015) 20 Suppl 4:14–21. doi: 10.1111/nep.12639
129. Kataoka H, Ohara M, Shibui K, Sato M, Suzuki T, Amemiya N, et al. Overweight and obesity accelerate the progression of IgA nephropathy: Prognostic utility of a combination of BMI and histopathological parameters. Clin Exp nephrology. (2012) 16(5):706–12. doi: 10.1007/s10157-012-0613-7
130. Bellary S, Kyrou I, Brown J, Bailey C. Type 2 diabetes mellitus in older adults: Clinical considerations and management. Nat Rev Endocrinology. (2021) 17(9):534–48. doi: 10.1038/s41574-021-00512-2
131. Heidari S, Babor T, De Castro P, Tort S, Curno M. Sex and gender equity in research: Rationale for the SAGER guidelines and recommended use. Res Integrity Peer Review. (2016) 1:2–2. doi: 10.1186/s41073-016-0007-6
132. Seeland U, Nemcsik J, Lønnebakken M, Kublickiene K, Schluchter H, Park C, et al. Sex and gender aspects in vascular ageing - focus on epidemiology, pathophysiology, and outcomes. Heart Lung circulation. (2021) 30(11):1637–46. doi: 10.1016/j.hlc.2021.07.006
133. Norori N, Hu Q, Aellen F, Faraci F, Tzovara A. Addressing bias in big data and AI for health care: A call for open science. Patterns. (2021) 2(10):100347–7. doi: 10.1016/j.patter.2021.100347
134. Cirillo D, Catuara Solarz S, Morey C, Guney E, Subirats L, Mellino S, et al. Sex and gender differences and biases in artificial intelligence for biomedicine and healthcare. NPJ Digital Med (2020) 3:81–1. doi: 10.1038/s41746-020-0288-5
135. Lee M, Guo L, Nambudiri V. Towards gender equity in artificial intelligence and machine learning applications in dermatology. J Am Med Inf Assoc (2022) 29(2):400–3. doi: 10.1093/jamia/ocab113
136. White J, Tannenbaum C, Klinge I, Schiebinger L, Clayton J. The integration of sex and gender considerations into biomedical research: Lessons from international funding agencies. J Clin Endocrinol Metab (2021) 106(10):3034–48. doi: 10.1210/clinem/dgab434
137. Rechlin R, Splinter TFL, Hodges T, Albert A, Galea LAM. An analysis of neuroscience and psychiatry papers published from 2009 and 2019 outlines opportunities for increasing discovery of sex differences. Nat Commun (2022) 13(1):2137–7. doi: 10.1038/s41467-022-29903-3
138. Woodward M. Rationale and tutorial for analysing and reporting sex differences in cardiovascular associations. Heart (British Cardiac Society). (2019) 105(22):1701–8. doi: 10.1136/heartjnl-2019-315299
139. Shansky R. Are hormones a "female problem" for animal research? Sci (New York NY) (2019) 364(6443):825–6. doi: 10.1126/science.aaw7570
140. Brinkley T, Stites S, Hunsberger H, Karvonen Gutierrez C, Li M, Shaaban CE, et al. Research centers collaborative network workshop on sex and gender differences in aging. Innovation Aging (2022) 6(7):igac055–igac055. doi: 10.1093/geroni/igac055
141. Matthias K, Honekamp I, De Santis K. The influence of sex, gender, or age on outcomes of digital technologies for treatment and monitoring of chronic obstructive pulmonary disease: Protocol for an overview of systematic reviews. JMIR Res Protoc (2022) 11(10):e40538–8. doi: 10.2196/40538
142. Diaz T, Strong K, Cao B, Guthold R, Moran A, Moller A-B, et al. A call for standardised age-disaggregated health data. Lancet Healthy Longevity. (2021) 2(7):e436–43. doi: 10.1016/S2666-7568(21)00115-X
143. Hulsen T, Jamuar S, Moody A, Karnes J, Varga O, Hedensted S, et al. From big data to precision medicine. Front Med (2019) 6:34–4. doi: 10.3389/fmed.2019.00034
144. Kammerlander A, Lyass A, Mahoney T, Massaro J, Long M, Vasan R, et al. Sex differences in the associations of visceral adipose tissue and cardiometabolic and cardiovascular disease risk: The framingham heart study. J Am Heart Assoc Cardiovasc Cerebrovascular Disease. (2021) 10(11):e019968–e019968. doi: 10.1161/JAHA.120.019968
145. Abraham T, Pedley A, Massaro J, Hoffmann U, Fox C. Association between visceral and subcutaneous adipose depots and incident cardiovascular disease risk factors. Circulation. (2015) 132(17):1639–47. doi: 10.1161/CIRCULATIONAHA.114.015000
146. Dekkers I, de Vries APJ, Smit RAJ, Rosendaal F, Rabelink T, Lamb H, et al. The separate contributions of visceral fat and liver fat to chronic kidney disease-related renal outcomes. J Renal Nutr (2020) 30(4):286–95. doi: 10.1053/j.jrn.2019.09.002
147. Kuma A, Uchino B, Ochiai Y, Kawashima M, Enta K, Tamura M, et al. Relationship between abdominal adiposity and incident chronic kidney disease in young- to middle-aged working men: A retrospective cohort study. Clin Exp nephrology. (2019) 23(1):76–84. doi: 10.1007/s10157-018-1606-y
148. Madero M, Katz R, Murphy R, Newman A, Patel K, Ix J, et al. Comparison between different measures of body fat with kidney function decline and incident CKD. Clin J Am Soc Nephrol CJASN. (2017) 12(6):893–903. doi: 10.2215/CJN.07010716
149. Grubbs V, Lin F, Vittinghoff E, Shlipak MG, Peralta CA, Bansal N, et al. Body mass index and early kidney function decline in young adults: A longitudinal analysis of the CARDIA (Coronary artery risk development in young adults) study. Am J Kidney Dis Off J Natl Kidney Foundation. (2014) 63(4):590–7. doi: 10.1053/j.ajkd.2013.10.055
150. Esmeijer K, Geleijnse JM, Giltay EJ, Stijnen T, Dekker FW, de Fijter JW, et al. Body-fat indicators and kidney function decline in older post-myocardial infarction patients: The alpha omega cohort study. Eur J Prev Cardiol (2018) 25(1):90–9. doi: 10.1177/2047487317739986
151. Oh H, Quan SA, Jeong JY, Jang SN, Lee JE, Kim DH. Waist circumference, not body mass index, is associated with renal function decline in korean population: Hallym aging study. PloS One (2013) 8(3):e59071. doi: 10.1371/journal.pone.0059071
152. Kim SR, Yoo JH, Song HC, Lee SS, Yoo SJ, Kim YD, et al. Relationship of visceral and subcutaneous adiposity with renal function in people with type 2 diabetes mellitus. Nephrology dialysis Transplant Off Publ Eur Dialysis Transplant Assoc - Eur Renal Assoc (2011) 26(11):3550–5. doi: 10.1093/ndt/gfq634
153. Klaver M, de Blok CJM, Wiepjes CM, Nota NM, Dekker MJHJ, de Mutsert R, et al. Changes in regional body fat, lean body mass and body shape in trans persons using cross-sex hormonal therapy: Results from a multicenter prospective study. Eur J endocrinology. (2018) 178(2):163–71. doi: 10.1530/EJE-17-0496
154. Demerath E, Sun S, Rogers N, Lee M, Reed D, Choh A, et al. Anatomical patterning of visceral adipose tissue: Race, sex, and age variation. Obesity. (2007) 15(12):2984–93. doi: 10.1038/oby.2007.356
155. Kvist H, Chowdhury B, Grangard U, Tylen U, Sjostrom L. Total and visceral adipose-tissue volumes derived from measurements with computed tomography in adult men and women: Predictive equations. Am J Clin Nutr (1988) 48(6):1351–61. doi: 10.1093/ajcn/48.6.1351
156. Lovejoy JC, Champagne CM, de Jonge L, Xie H, Smith SR. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int J Obes (2005) (2008) 32(6):949–58. doi: 10.1038/ijo.2008.25
157. Steiner B, Berry D. The regulation of adipose tissue health by estrogens. Front Endocrinology. (2022) 13:889923–3. doi: 10.3389/fendo.2022.889923
158. Bracht J, Vieira Potter V, De Souza Santos R, Öz O, Palmer B, Clegg D. The role of estrogens in the adipose tissue milieu. Ann New York Acad Sci (2020) 1461(1):127–43. doi: 10.1111/nyas.14281
159. Medina D, Mehay D, Arnold A. Sex differences in cardiovascular actions of the renin-angiotensin system. Clin Autonomic Res (2020) 30(5):393–408. doi: 10.1007/s10286-020-00720-2
160. Colafella KMM, Denton K. Sex-specific differences in hypertension and associated cardiovascular disease. Nat Rev Nephrology. (2018) 14(3):185–201. doi: 10.1038/nrneph.2017.189
161. White M, Fleeman R, Arnold A. Sex differences in the metabolic effects of the renin-angiotensin system. Biol Sex Differences. (2019) 10(1):31–1. doi: 10.1186/s13293-019-0247-5
162. Komukai K, Mochizuki S, Yoshimura M. Gender and the renin-angiotensin-aldosterone system. Fundam Clin Pharmacol (2010) 24(6):687–98. doi: 10.1111/j.1472-8206.2010.00854.x
163. Fischer M, Baessler A, Schunkert H. Renin angiotensin system and gender differences in the cardiovascular system. Cardiovasc Res (2002) 53(3):672–7. doi: 10.1016/S0008-6363(01)00479-5
164. Brosnihan KB, Li P, Ganten D, Ferrario CM. Estrogen protects transgenic hypertensive rats by shifting the vasoconstrictor-vasodilator balance of RAS. Am J Physiol (1997) 273(6):R1908–15. doi: 10.1152/ajpregu.1997.273.6.R1908
165. Wu Z, Maric C, Roesch D, Zheng W, Verbalis J, Sandberg K. Estrogen regulates adrenal angiotensin AT1 receptors by modulating AT1 receptor translation. Endocrinology. (2003) 144(7):3251–61. doi: 10.1210/en.2003-0015
166. Ichiki T, Usui M, Kato M, Funakoshi Y, Ito K, Egashira K, et al. Downregulation of angiotensin II type 1 receptor gene transcription by nitric oxide. Hypertension. (1998) 31(1):342–8. doi: 10.1161/01.HYP.31.1.342
167. Roesch DM, Tian Y, Zheng W, Shi M, Verbalis JG, Sandberg K. Estradiol attenuates angiotensin-induced aldosterone secretion in ovariectomized rats. Endocrinology. (2000) 141(12):4629–36. doi: 10.1210/endo.141.12.7822
168. Reckelhoff JF. Gender differences in the regulation of blood pressure. Hypertension. (2001) 37(5):1199–208. doi: 10.1161/01.HYP.37.5.1199
169. Schunkert H, Danser AH, Hense HW, Derkx FH, Kürzinger S, Riegger GA. Effects of estrogen replacement therapy on the renin-angiotensin system in postmenopausal women. Circulation. (1997) 95(1):39–45. doi: 10.1161/01.CIR.95.1.39
170. Toering T, Gant C, Visser F, van der Graaf AM, Laverman G, Danser AHJ, et al. Sex differences in renin-angiotensin-aldosterone system affect extracellular volume in healthy subjects. AJP-Renal Physiol (2018) 314(5):F873–8. doi: 10.1152/ajprenal.00109.2017
171. Gambacciani M, Ciaponi M, Cappagli B, Piaggesi L, De Simone L, Orlandi R, et al. Body weight, body fat distribution, and hormonal replacement therapy in early postmenopausal women. J Clin Endocrinol Metab (1997) 82(2):414–7. doi: 10.1210/jcem.82.2.3735
172. Haarbo J, Marslew U, Gotfredsen A, Christiansen C. Postmenopausal hormone replacement therapy prevents central distribution of body fat after menopause. Metabolism Clin experimental. (1991) 40(12):1323–6. doi: 10.1016/0026-0495(91)90037-W
173. Papadakis G, Hans D, Gonzalez Rodriguez E, Vollenweider P, Waeber G, Marques Vidal P, et al. Menopausal hormone therapy is associated with reduced total and visceral adiposity: The OsteoLaus cohort. J Clin Endocrinol Metab (2018) 103(5):1948–57. doi: 10.1210/jc.2017-02449
174. Medina D, Arnold A. Angiotensin-(1-7): Translational avenues in cardiovascular control. Am J hypertension. (2019) 32(12):1133–42. doi: 10.1093/ajh/hpz146
175. Saiki A, Ohira M, Endo K, Koide N, Oyama T, Murano T, et al. Circulating angiotensin II is associated with body fat accumulation and insulin resistance in obese subjects with type 2 diabetes mellitus. Metabolism Clin experimental. (2009) 58(5):708–13. doi: 10.1016/j.metabol.2009.01.013
176. Luther J, Brown N. The renin-angiotensin-aldosterone system and glucose homeostasis. Trends Pharmacol Sci (Regular ed Print). (2011) 32(12):734–9. doi: 10.1016/j.tips.2011.07.006
177. Vargas Castillo A, Tobon Cornejo S, Del Valle-Mondragon L, Torre Villalvazo I, Schcolnik Cabrera A, Guevara Cruz M, et al. Angiotensin-(1-7) induces beige fat thermogenesis through the mas receptor. Metabolism Clin experimental. (2020) 103:154048–8. doi: 10.1016/j.metabol.2019.154048
178. Wannamethee SG, Papacosta O, Lawlor DA, Whincup PH, Lowe GD, Ebrahim S, et al. Do women exhibit greater differences in established and novel risk factors between diabetes and non-diabetes than men? The British regional heart study and British women's heart health study. Diabetologia. (2012) 55(1):80–7. doi: 10.1007/s00125-011-2284-4
179. Peters SA, Huxley RR, Woodward M. Diabetes as a risk factor for stroke in women compared with men: A systematic review and meta-analysis of 64 cohorts, including 775,385 individuals and 12,539 strokes. Lancet. (2014) 383(9933):1973–80. doi: 10.1016/S0140-6736(14)60040-4
180. Koh KK, Kang MH, Jin DK, Lee SK, Ahn JY, Hwang HY, et al. Vascular effects of estrogen in type II diabetic postmenopausal women. J Am Coll Cardiol (2001) 38(5):1409–15. doi: 10.1016/S0735-1097(01)01566-2
181. Carr MC. The emergence of the metabolic syndrome with menopause. J Clin Endocrinol Metab (2003) 88(6):2404–11. doi: 10.1210/jc.2003-030242
182. Ozbey N, Sencer E, Molvalilar S, Orhan Y. Body fat distribution and cardiovascular disease risk factors in pre- and postmenopausal obese women with similar BMI. Endocr J (2002) 49(4):503–9. doi: 10.1507/endocrj.49.503
183. Eriksen BO, Ingebretsen OC. The progression of chronic kidney disease: A 10-year population-based study of the effects of gender and age. Kidney Int (2006) 69(2):375–82. doi: 10.1038/sj.ki.5000058
184. Suzuki H, Kondo K. Chronic kidney disease in postmenopausal women. Hypertension Res (2012) 35(2):142–7. doi: 10.1038/hr.2011.155
185. Jafar TH, Schmid CH, Stark PC, Toto R, Remuzzi G, Ruggenenti P, et al. The rate of progression of renal disease may not be slower in women compared with men: a patient-level meta-analysis. Nephrology dialysis Transplant Off Publ Eur Dialysis Transplant Assoc - Eur Renal Assoc (2003) 18(10):2047–53. doi: 10.1093/ndt/gfg317
186. Ahmed S, Ramesh S. Sex hormones in women with kidney disease. Nephrology dialysis transplantation. (2016) 31(11):1787–95. doi: 10.1093/ndt/gfw084
187. de Hauteclocque A, Ragot S, Slaoui Y, Gand E, Miot A, Sosner P, et al. The influence of sex on renal function decline in people with type 2 diabetes. Diabetic Med J Br Diabetic Assoc (2014) 31(9):1121–8. doi: 10.1111/dme.12478
188. Fernandez-Prado R, Fernandez-Fernandez B, Ortiz A. Women and renal replacement therapy in Europe: Lower incidence, equal access to transplantation, longer survival than men. Clin Kidney J (2018) 11(1):1–6. doi: 10.1093/ckj/sfx154
189. Iseki K, Nakai S, Shinzato T, Nagura Y, Akiba T. Increasing gender difference in the incidence of chronic dialysis therapy in Japan. Ther Apher Dial. (2005) 9(5):407–11. doi: 10.1111/j.1744-9987.2005.00318.x
190. Coggins CH, Breyer Lewis J, Caggiula AW, Castaldo LS, Klahr S, Wang SR. Differences between women and men with chronic renal disease. Nephrology dialysis Transplant Off Publ Eur Dialysis Transplant Assoc - Eur Renal Assoc (1998) 13(6):1430–7. doi: 10.1093/ndt/13.6.1430
191. Tsai WC, Wu HY, Peng YS, Ko MJ, Wu MS, Hung KY, et al. Risk factors for development and progression of chronic kidney disease: A systematic review and exploratory meta-analysis. Medicine. (2016) 95(11):e3013. doi: 10.1097/md.0000000000003013
192. Doublier S, Lupia E, Catanuto P, Elliot SJ. Estrogens and progression of diabetic kidney damage. Curr Diabetes Rev (2011) 7(1):28–34. doi: 10.2174/157339911794273982
193. Kataoka H, Sawara Y, Kawachi K, Manabe S, Mochizuki T, Nitta K. Impacts of sex differences in pulse pressure among patients with chronic kidney disease. J Pers Med (2019) 9(4):52. doi: 10.3390/jpm9040052
194. Seong J, Lee J, Gi M, Son Y, Moon A, Park C, et al. Gender difference in the association of chronic kidney disease with visceral adiposity index and lipid accumulation product index in Korean adults: Korean national health and nutrition examination survey. Int Urol nephrology. (2021) 53(7):1417–25. doi: 10.1007/s11255-020-02735-0
195. Ryo M, Kishida K, Nakamura T, Yoshizumi T, Funahashi T, Shimomura I. Clinical significance of visceral adiposity assessed by computed tomography: A Japanese perspective. World J Radiol (2014) 6(7):409–16. doi: 10.4329/wjr.v6.i7.409
196. Hiuge-Shimizu A, Kishida K, Funahashi T, Ishizaka Y, Oka R, Okada M, et al. Absolute value of visceral fat area measured on computed tomography scans and obesity-related cardiovascular risk factors in large-scale Japanese general population (the VACATION-J study). Ann Med (2012) 44(1):82–92. doi: 10.3109/07853890.2010.526138
197. Hiuge-Shimizu A, Kishida K, Funahashi T, Okutsu M, Kametani R, Kobayashi H, et al. Coexistence of visceral fat and multiple risk factor accumulations is strongly associated with coronary artery disease in Japanese (the VACATION-J study). J Atheroscler Thromb (2012) 19(7):657–63. doi: 10.5551/jat.13037
198. Yamashiro K, Tanaka R, Tanaka Y, Miyamoto N, Shimada Y, Ueno Y, et al. Visceral fat accumulation is associated with cerebral small vessel disease. Eur J Neurol (2014) 21(4):667–73. doi: 10.1111/ene.12374
199. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. (2009) 120(16):1640–5. doi: 10.1161/circulationaha.109.192644
200. Nishizawa H, Shimomura I. Population approaches targeting metabolic syndrome focusing on Japanese trials. Nutrients. (2019) 11(6):1430. doi: 10.3390/nu11061430
201. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults–the Evidence Report. National Institutes of Health (NIH). . Obes Res (1998) 6 Suppl 2:51S–209S.
202. Navaneethan SD, Schold JD, Kirwan JP, Arrigain S, Jolly SE, Poggio ED, et al. Metabolic syndrome, ESRD, and death in CKD. Clin J Am Soc Nephrol CJASN. (2013) 8(6):945–52. doi: 10.2215/cjn.09870912
203. Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, et al. American Heart association statistics c, stroke statistics s. heart disease and stroke statistics-2017 update: A report from the American heart association. Circulation. (2017) 135(10):e146–603. doi: 10.1161/CIR.0000000000000485
204. Weinstein J, Anderson S. The aging kidney: physiological changes. Adv chronic Kidney disease. (2010) 17(4):302–7. doi: 10.1053/j.ackd.2010.05.002
205. Noth RH, Lassman MN, Tan SY, Fernandez Cruz A, Mulrow PJ. Age and the renin-aldosterone system. Arch Internal Med (1960). (1977) 137(10):1414–7. doi: 10.1001/archinte.1977.03630220056014
206. Yoon H, Choi B. The renin-angiotensin system and aging in the kidney. Korean J Internal Med (2014) 29(3):291–5. doi: 10.3904/kjim.2014.29.3.291
207. Weidmann P, De Myttenaere-Bursztein S, Maxwell MH, de Lima J. Effect on aging on plasma renin and aldosterone in normal man. Kidney Int (1975) 8(5):325–33. doi: 10.1038/ki.1975.120
208. Mulkerrin E, Epstein FH, Clark BA. Aldosterone responses to hyperkalemia in healthy elderly humans. J Am Soc Nephrology. (1995) 6(5):1459–62. doi: 10.1681/ASN.V651459
209. Hemmelgarn BR, Zhang J, Manns BJ, Tonelli M, Larsen E, Ghali WA, et al. Progression of kidney dysfunction in the community-dwelling elderly. Kidney Int (2006) 69(12):2155–61. doi: 10.1038/sj.ki.5000270
210. Hsu CY, Iribarren C, McCulloch CE, Darbinian J, Go AS. Risk factors for end-stage renal disease: 25-year follow-up. Arch Internal Med (2009) 169(4):342–50. doi: 10.1001/archinternmed.2008.605
211. O'Hare AM, Choi AI, Bertenthal D, Bacchetti P, Garg AX, Kaufman JS, et al. Age affects outcomes in chronic kidney disease. J Am Soc Nephrol JASN. (2007) 18(10):2758–65. doi: 10.1681/asn.2007040422
212. Schaeffner E, Ebert N, Kuhlmann M, Martus P, Mielke N, Schneider A, et al. Age and the course of GFR in persons aged 70 and above. Clin J Am Soc Nephrology. (2022) 17(8):1119–28. doi: 10.2215/CJN.16631221
Keywords: visceral fat, patient-centered medicine, sex difference, personalized medicine, obesity, precision medicine, chronic kidney disease, attribute-based medicine
Citation: Kataoka H, Nitta K and Hoshino J (2023) Visceral fat and attribute-based medicine in chronic kidney disease. Front. Endocrinol. 14:1097596. doi: 10.3389/fendo.2023.1097596
Received: 14 November 2022; Accepted: 13 January 2023;
Published: 09 February 2023.
Edited by:
Shen Qu, Tongji University, ChinaReviewed by:
Jiahong Sun, Shandong University, ChinaCopyright © 2023 Kataoka, Nitta and Hoshino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hiroshi Kataoka, a2F0YW9rYUB0d211LmFjLmpw
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.