
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Endocrinol. , 16 February 2023
Sec. Clinical Diabetes
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1079009
This article is part of the Research Topic Frontiers in Diagnostic and Therapeutic approaches in Diabetic Sensorimotor Neuropathy View all 6 articles
 Orsolya E. Vági1*†
Orsolya E. Vági1*† Márk M. Svébis1,2†Beatrix A. Domján1
Márk M. Svébis1,2†Beatrix A. Domján1 Anna E. Körei1
Anna E. Körei1 Solomon Tesfaye4
Solomon Tesfaye4 Viktor J. Horváth1‡
Viktor J. Horváth1‡ Péter Kempler1‡Ádám Gy. Tabák1,3,5*‡
Péter Kempler1‡Ádám Gy. Tabák1,3,5*‡Background: Distal symmetric polyneuropathy (DSPN) is a common microvascular complication of both type 1 and 2 diabetes with substantial morbidity burden and reduced quality of life. Its association with mortality is equivocal.
Purpose: To describe the association between DSPN and all-cause mortality in people with diabetes and further stratify by the type of diabetes based on a meta-analysis of published observational studies.
Data Sources: We searched Medline from inception to May 2021.
Study Selection: Original data were collected from case-control and cohort studies that reported on diabetes and DSPN status at baseline and all-cause mortality during follow-up.
Data Extraction: was completed by diabetes specialists with clinical experience in neuropathy assessment.
Data Synthesis: Data was synthesized using random-effects meta-analysis. The difference between type 1 and 2 diabetes was investigated using meta-regression.
Results: A total of 31 cohorts (n=155,934 participants, median 27.4% with DSPN at baseline, all-cause mortality 12.3%) were included. Diabetes patients with DSPN had an almost twofold mortality (HR: 1.96, 95%CI: 1.68-2.27, I2 = 91.7%), I2 = 91.7%) compared to those without DSPN that was partly explained by baseline risk factors (adjusted HR: 1.60, 95%CI: 1.37-1.87, I2 = 78.86%). The association was stronger in type 1 compared to type 2 diabetes (HR: 2.22, 95%CI: 1.43-3.45). Findings were robust in sensitivity analyses without significant publication bias.
Limitations: Not all papers reported multiple adjusted estimates. The definition of DSPN was heterogeneous.
Conclusions: DSPN is associated with an almost twofold risk of death. If this association is causal, targeted therapy for DSPN could improve life expectancy of diabetic patients.
The prevalence of diabetes mellitus is increasing rapidly worldwide: it is expected to reach 578 million in 2030 (1). Meta-analyses of prospective studies (mostly from high-income countries) have found that diabetes is associated with an almost two-fold risk of a wide range of vascular diseases. This increase was clearly present in both men and women and was independent of other major conventional vascular risk factors (2). In addition to the values of individual risk factors, the overall burden (estimated as the number of abnormal values) of risk factors showed a dose-response relationship with cardiovascular risk (3). Although diabetes patients with well-controlled conventional vascular risk factors have a comparable mortality risk to that of the background population (4), not all excess vascular and mortality risk can be explained by conventional vascular risk factors (such as smoking, hyperlipidemia, hypertension, etc.) (2).
Diabetic microvascular complications could be partially responsible for this unexplained vascular and mortality burden. Indeed, there is strong evidence from a meta-analysis of observational studies that decreased estimated glomerular filtration rate and urinary albumin to creatinine ratio are both associated with an up to 2 times increased mortality (5). Furthermore, a former meta-analysis of observational studies of diabetes patients reported a substantially increased risk of mortality among diabetic patients with cardiovascular autonomic neuropathy (CAN) (6, 7). In addition to CAN, distal symmetric polyneuropathy (DSPN) is also a prevalent chronic microvascular complication of both type 1 and type 2 diabetes (8). Although DSPN is most prevalent in diabetic persons, it was found in people with normoglycemia or prediabetes (9–12). As DSPN may start early in the course of metabolic alteration, it could be a burden throughout the whole spectrum of impaired glucose metabolism leaving these patients prone to its potential effects on mortality and morbidity.
Given the equivocal data on the association of DSPN with all-cause mortality, we aimed to conduct a systematic review and meta-analysis on the impact of DSPN on all-cause mortality. Our hypotheses were that (1) DSPN is related to all-cause mortality in both types of diabetes. Furthermore, we thought that (2) this relationship would be stronger in type 1 diabetes given the younger age at the diagnosis of these patients.
The search strategy was designed by a diabetes specialist with experience in diabetes epidemiology (AGT) with input from all other investigators in accordance with the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guideline (13). MEDLINE databases from their inception until 31/MAY/2021 were searched. Controlled vocabulary supplemented with keywords was used to search for studies fulfilling the criteria of reporting on both sensory diabetic neuropathy and mortality. We imposed no limitation on regional origin or language of any findings. We used the following search phrase: ((senso* OR DSPN OR neuropat* OR “diabetic foot” OR (foot AND ulcer*) OR Charcot) AND (diabete* OR diabeti*) AND (mortality OR death)). We aimed to collect case-control and cohort studies of diabetic people where baseline DSPN status was reported and follow-up mortality by DSPN status could be retrieved. All studies had to be of original data. We did not impose restriction on the length of follow-up.
Several approaches (including questionnaires, symptoms, physical examination, and equipment-based techniques) were accepted for the diagnosis of DSPN (Table 1) as long as the same validated approach was used consistently within a report. Quality assessment of the papers was completed by the Newcastle-Ottawa Scale (NOS). We translated the NOS scores into the following strata using the Agency for Healthcare Research and Quality (AHQR) standards (1): good quality: 3 or 4 stars in selection domain AND 1 or 2 stars in comparability domain AND 2 or 3 stars in outcome/exposure domain (2); fair quality: 2 stars in selection domain AND 1 or 2 stars in comparability domain AND 2 or 3 stars in outcome/exposure domain (3); poor quality: 0 or 1 star in selection domain OR 0 stars in comparability domain OR 0 or 1 stars in outcome/exposure domain (41). The corresponding authors of potentially eligible primary studies without the required information within their publication were not invited to contribute with their raw data.
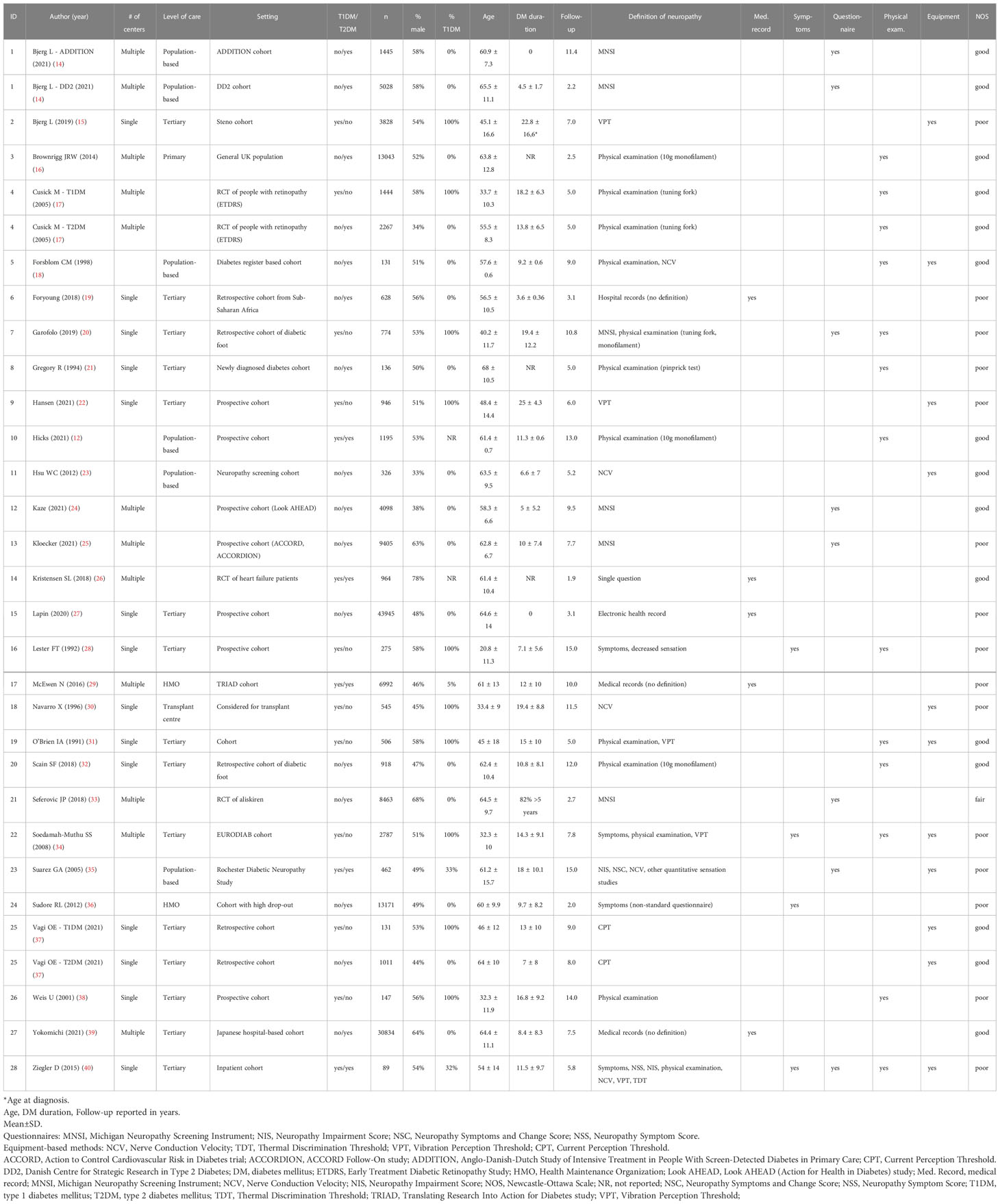
Table 1 Baseline characteristics of observational studies included in the meta-analysis on the association between DSPN and all-cause mortality.
Reviewers worked independently and checked all abstracts and selected full-text manuscripts for eligibility. Preselected manuscripts were evaluated by 2 independent reviewers for eligibility. The total number of included and excluded articles was documented by the reviewers, including reasons for exclusion or non-eligibility. Any disagreements were discussed with the study designer (AGT). Whenever reviewers disagreed and no consensus was found, the article was included into the full-text phase. Disagreements at full-text screening were resolved by consensus of all authors.
For all studies, we extracted information on study design, number and characteristics of participants (i.e. age, sex, type of diabetes), prevalence of DSPN, method of DSPN assessment, duration of follow-up, all-cause mortality, matching, and confounding factors. Additionally, in the case of multiple publications, we included the most up-to-date or comprehensive information.
From the given publications, we sought data on the association between DSPN and all-cause mortality with their respective 95% confidence intervals (CI) based on unadjusted (minimally adjusted) and fully adjusted models. For the unadjusted models, we collected raw numbers, odds ratios (OR), hazard ratios (HR), or incidence rate ratios (IRR) that were either unadjusted or adjusted for only age and sex. If any other variable (i.e. diabetes type, BMI, and diabetes duration, co-morbidities) was taken into account, the estimate was considered to be fully adjusted. If more than one model was reported, the one with the most co-variables was selected. At this stage, we excluded unadjusted estimates from those studies, where the population was referred specifically for the examination of sensory or autonomic neuropathy, given the high risk of collider bias in this setting. If a given paper reported adjusted estimates, those were used in the analysis.
The outcome measure of this meta-analysis was pooled all-cause mortality among individuals with DSPN compared to those without DSPN. We pooled estimates with their 95% confidence intervals (CIs) using random effect meta-analysis, as this methodology works well even when heterogeneity between studies is substantial (42). We also pre-planned to run analyses stratified by the type of diabetes (type 1 diabetes, type 2 diabetes, or undefined/mixture of type 1 and type 2 diabetes). We also tested formally for a difference between the estimates for type 1 and type 2 diabetes using meta-regression. For the main analysis, we included all cohorts that provided either unadjusted or adjusted estimates (using the unadjusted estimates if available).
To assess statistical heterogeneity, visual inspection of the forest plots was used, followed by formal testing using the I2-statistic. This provides an estimate of the percentage of variability across studies due to heterogeneity rather than chance: I2 < 40% may represent low heterogeneity; 30-60% may represent moderate heterogeneity; 50-90% represent substantial heterogeneity; and 75-100% represent considerable heterogeneity (43). Publication bias was evaluated by visual inspection of the funnel plots and formally by Egger’s tests. Additionally, we tested for influence of individual studies using a meta-analysis influence test that eliminated included studies one by one.
Given the expected heterogeneity of the eligible studies, pre-planned sensitivity analyses (stratified by type of diabetes) were also carried out by restricting the analysis to (1) studies that adjusted for potential predictors of mortality (other than age and sex) (2), population-based investigations (3), studies that used semi-quantitative (physical examination including monofilament or tuning fork or pinprick tests) or quantitative (vibration or current perception threshold or nerve conduction test) methods for DSPN assessment, and to studies that were deemed to be of good quality according to the Newcastle-Ottawa Scale (41). A further sensitivity analysis was done using meta-regression with adjustment for diabetes duration to investigate whether a risk difference between type 1 and type 2 diabetes would be explained by different length of diabetes duration.
All statistical tests were two sided and used a significance level of p<0.05. We used STATA 15.1 (StataCorp, CollegeStation, TX) for all statistical analyses.
The flow chart of the search strategy is presented in Figure 1. An initial search produced 4904 articles (Figure 1). Based on titles and abstracts, we excluded 4844 articles that reported no original data that didn’t investigate DSPN or didn’t report mortality data, or had no control population (without DSPN), leaving 60 papers for full text retrieval. All these papers were written in English. We excluded a further 31 papers due to different reasons leaving 29 papers that could be included in the meta-analysis. Of the 29, two studies (17, 37) reported estimates separately for type 1 and type 2 diabetes and one (14) reported estimates separately for two population-based cohorts (ADDITION and DD2) that allowed us to use them as altogether six separate cohorts. In contrast, we excluded 2 studies from the unadjusted analysis (37, 44), due to the potential of collider bias. Our final sample for the main analysis thus included 31 cohorts and for the fully adjusted analysis 17 cohorts (12, 14–40).
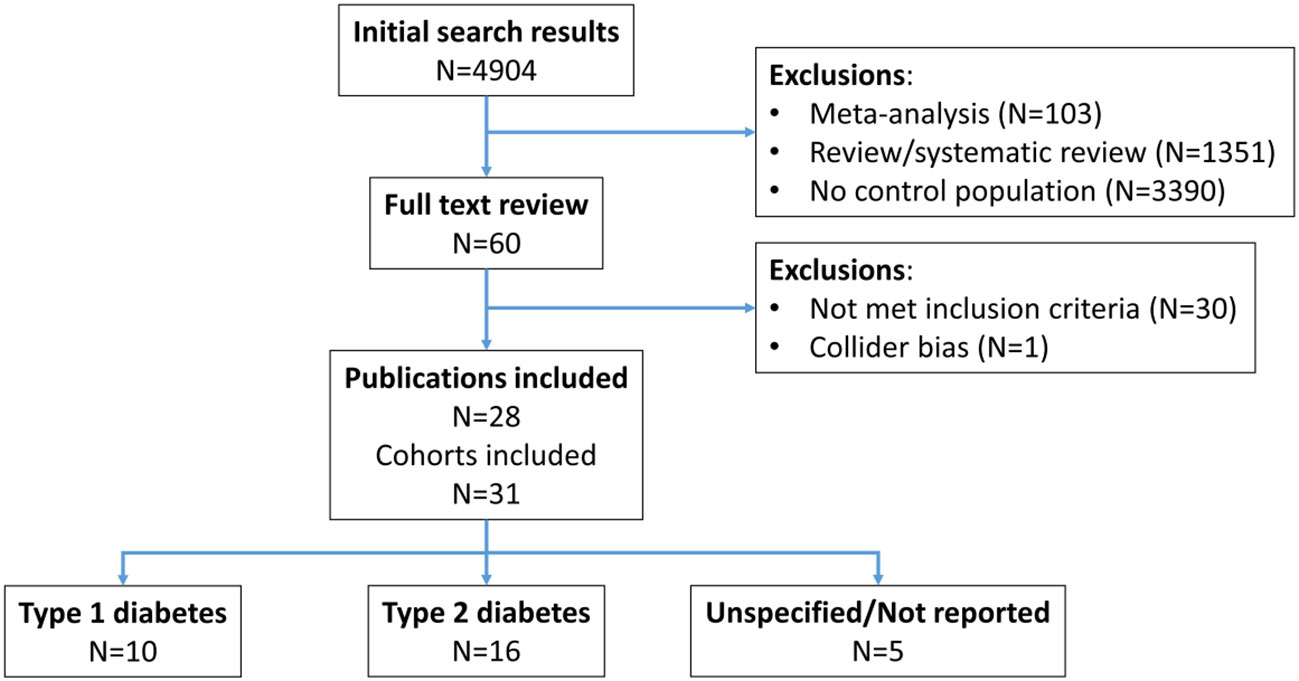
Figure 1 Flow chart of the selection of included studies.
Detailed characteristics of the included cohorts are summarized in Table 1. Out of the included 31 cohorts, 10 reported on type 1 diabetic patients, 16 on type 2 diabetic patients. In the remaining 6 papers, type of diabetes was either not reported, or estimates could not be separated for patients with type 1 and type 2 diabetes.
Nine of the cohorts included population-based samples, while most were performed in tertiary care (14 in single, 2 in multiple centers). Six cohorts used data from randomized trials or their follow-up cohorts (Table 1).
Diagnosis of DSPN varied widely between the different cohorts. Five cohorts used medical records as the source of data, leading to potential bias related to the non-standardized ways of examination. 3 cohorts used non-standardized symptom-checks only for diagnosis, 6 cohorts standardized questionnaires, 8 physical examination, and 7 studies used different equipments that provide quantitative measures of neuronal function. Only 5 studies used a combination of the above methods to provide the diagnosis of DSPN. When quantitative or semi-quantitative methods were considered as more reliable tools for the diagnosis of DSPN, 18 studies fulfilled this requirement (Table 1).
Altogether over 150 thousand diabetes patients (54% male) were included in the main analysis of whom 12.3% died during the median 7.5 (range 1.9-15.0) years of follow-up. The median proportion of participants with DSPN was 27.4% (range 8.8%-73.6%).The median age of participants was 60 years (range 20.8-68.0 years), diabetes duration ranged 0 to 25 years (median 11.1 years) in the different cohorts (Table 1).
While all studies provided some estimates of mortality, unadjusted (including those only adjusted for age and sex) estimates were available for 29 cohorts, while multiple adjusted estimates were reported in 17 cohorts (Table 1).
According to the NOS classification, 18 studies had good, 1 study had fair, and 9 poor quality (Supplementary Table S1).
In the pooled primary analysis, the presence of DSPN at baseline was significantly associated with an almost doubled risk of mortality (pooled HR 1.96, 95%CI 1.68-2.27). While the point estimates in the individual studies were over one for all but one studies, the heterogeneity between studies was large (I2 = 91.7%, p<0.001) (Figure 2).

Figure 2 Forest plot and pooled estimates of the association between DSPN and all-cause mortality stratified by type of diabetes. Error bars show 95% confidence intervals. Abbreviations: ADDITION: Anglo-Danish-Dutch Study of Intensive Treatment in People With Screen-Detected Diabetes in Primary Care; CI: confidence interval; DD2: Danish Centre for Strategic Research in Type 2 Diabetes; ES: effect size;.
According to our primary hypothesis we stratified the analysis between DSPN and mortality by the type of diabetes. Among patients with type 1 diabetes, the mortality was 3.64 (95%CI 2.55-5.20) times higher in the presence of DSPN compared to those without DSPN. While the I2 value (75.4%, p<0.0001) was somewhat lower in these studies compared to the overall value, heterogeneity remained large (Figure 2).
The pooled association between DSPN and mortality was weaker in patients with type 2 diabetes (pooled HR 1.63, 95%CI 1.37-1.93), although DSPN still was a strong predictor of all-cause mortality. There was large heterogeneity in the estimates between studies reflected by the high I2 value (91.8%, p<0.0001), partly related to the study by Foryoung et al. that reported a decreased risk of mortality in patients with DSPN (Figure 2).
In cohorts where it was impossible to assess the risks by diabetes type, we found a similar association between DPSN and mortality as in type 2 diabetes (pooled HR 1.49, 95% CI 1.35-1.64). There was a low heterogeneity between the individual risk estimates (I2 0%, p=0.48), suggesting that these estimates may have come from a common background population (probably mostly type 2 diabetes patients) (Figure 2).
When we formally tested for a difference in the estimates between type 1 and type 2 diabetes by meta-regression, we found that the risk associated with DSPN was more than 2 times higher in type 1 compared to type 2 diabetes (HR 2.22, 95%CI 1.43-3.45, p=0.001).
We also investigated the potential for publication bias in our estimates. Given the large difference in risks between diabetes types, we drew funnel plots separately for each type of diabetes. These funnel plots confirmed the large difference between type 1 and type 2 (and also undefined diabetes) groups but were incompatible with the presence of strong publication bias. The Egger tests were all non-significant (all p>0.8) further confirming the visual interpretation (Supplementary Figure 2).
We also tested for influential studies by eliminating individual studies from the meta-analysis run for each type of diabetes. All these analyses showed overlapping confidence intervals with the overall (diabetes type specific) estimates arguing against the role of some influential studies in the findings. (Figures are available on request.)
Our pre-planned sensitivity analyses restricted included cohorts by level of covariate adjustment, type of study setting, diagnostic test used to define DSPN, and overall quality of studies.
First, we run separate analyses including 29 studies that reported unadjusted, and 17 studies that reported adjusted estimates. The overall risk associated with DSPN was smaller according to the adjusted estimates (pooled HR 2.0 vs. 1.6) suggesting that the included covariates explained some of the increased mortality in DSPN. In contrast, the difference between type 1 and type 2 diabetes remained statistically significant showing stronger associations between DSPN and mortality in type 1 compared to type 2 diabetes (Table 2).
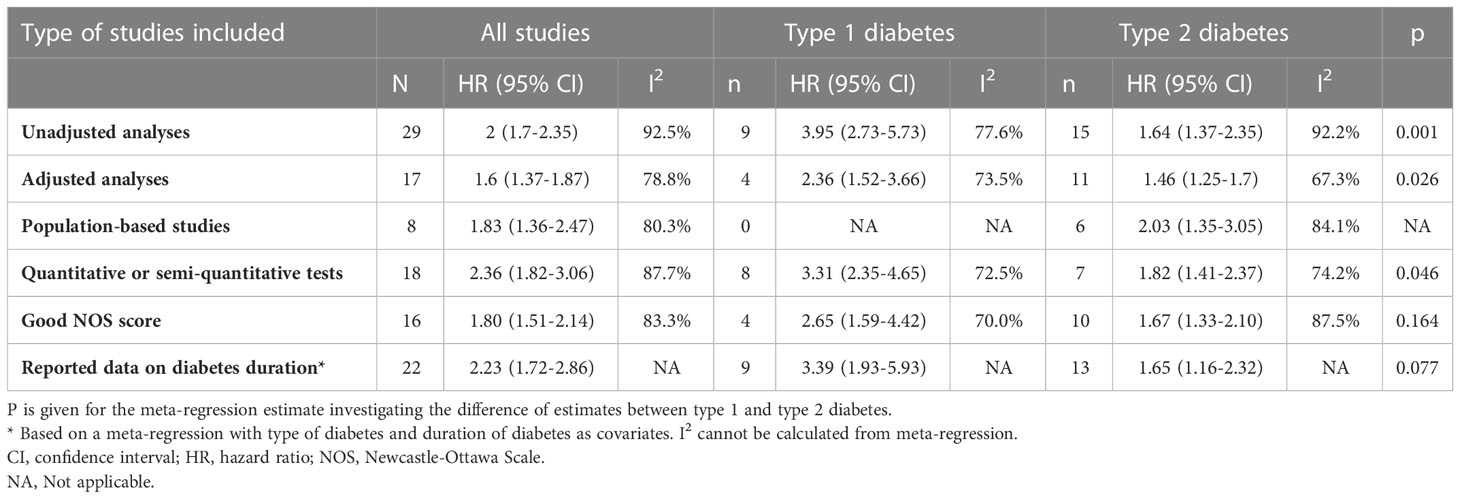
Table 2 Association between DSPN and all-cause mortality in sensitivity analyses restricted to cohorts based on adjustment of estimates, study setting, measurement methods, NOS score, and those that reported diabetes duration.
When we restricted the analysis to population-based studies, no cohort performed on type 1 diabetes patients remained. The overall risk estimates however confirmed the association between DSPN and mortality with an almost 2 times higher risk in patients with DSPN (Table 2).
When we restricted the analysis to cohorts that used quantitative or semi-quantitative methods to define DSPN, the overall association between DSPN and mortality remained and the point estimate was similar to those of the other analyses. Furthermore, heterogeneity was somewhat smaller for both types of diabetes (<75%), suggesting that the use of different methods could increase heterogeneity in the mortality estimates. Although the absolute difference in hazard ratios between type 1 and type 2 diabetes was smaller in this analysis, the estimates remained statistically significantly different further supporting our hypothesis that a stronger association exists between DSPN and mortality in type 1 diabetes (Table 2).
When we restricted our analysis to cohorts that deemed to be of good quality according to the NOS scale, we found point estimates similar to those from the main analysis, confirming the association between DSPN and mortality. Although the difference between type 1 and type 2 diabetes pointed to the same direction as in the main analysis, the difference between hazard ratios was statistically not different probably due to the limited number of studies included in this analysis (Table 2).
Finally, in a meta-regression adjusted for diabetes duration, we found a similarly increased mortality in type 1 diabetes compared to type 2 diabetes as in the main analysis, although due to the wide confidence intervals, it lost its statistical significance.
Based on a meta-analysis of 31 cohorts comprising over 150 thousand diabetic patients, we found an almost doubling (HR 1.96, 95%CI 1.68-2.27) of all-cause mortality among diabetes patients with distal symmetric polyneuropathy compared to those without DSPN. The association was somewhat attenuated but still statistically and clinically significant (HR 1.60, 95%CI 1.37-1.87) in those studies that take into account multiple risk factors of vascular disease and all-cause mortality. The observed association was more than two times stronger in type 1 compared to type 2 diabetes (HR 2.22, 95%CI 1.43-3.45), most likely reflecting the much smaller background mortality of younger patients without DSPN. The observed findings were robust in several sensitivity analyses that aimed to remove bias related to different study designs, methods for DSPN definitions, and overall study quality. Furthermore, we found no sign of publication bias, or any individual study with a major influence on the estimates.
Our overall finding of a statistically significantly increased mortality among people with diabetes is not very surprising given the fact that more than two third (22/31) of the included cohorts found a significantly increased risk of mortality and a further 8 studies had point estimates above one. It should be noted however, that only 4 cohorts aimed at specifically investigating the association between DSPN and all-cause mortality (12, 23, 37). While two of these showed similarly increased mortality to the overall estimate (12, 37), the other two showed substantially higher risks (although one cohort included only type 1 diabetes patients) (23, 37).
Most of the other cohorts that reported adjusted estimates for the DSPN — all-cause mortality association, aimed to investigate either microvascular complications (or just risk factors) as predictors or cardiovascular outcomes according to their primary hypothesis. Some of the cohorts reported only unadjusted estimates that is related to the fact that these cohorts were aiming at investigating completely different questions, although reported on crude frequencies of DSPN and mortality.
The fact that the association between CAN and all-cause mortality was found to be substantially attenuated and even became non-significant after adjustment for known hypertension or nephropathy in the Pittsburgh Epidemiology of Diabetes Complications (EDC) Study (45) highlights the importance of taking into account estimated risk of mortality of the participants.
Given the above reasoning, we preplanned to analyze cohorts separately that reported estimates on the DSPN-mortality association using multiple adjustments for risk factors in addition to age and sex. The role of these confounders is obvious, given that in addition to glycemic control, other cardiovascular risk factors (for example, hyperlipidemia, hypertension, abdominal obesity, smoking, alcohol use) and micro- and macrovascular complications of diabetes are strong predictors of DSPN (8, 46, 47).
Altogether 55% (17/31) cohorts reported adjusted estimates that confirmed our hypothesis that the association would be attenuated compared to findings of the main analysis. It should be noted however that the association still remained strong with a 60% increased point estimate (HR 1.6, 95%CI 1.37-1.87) and a confidence interval that also suggests an important effect size.
Although 7 studies included both type 1 and type 2 diabetes patients, only 2 of these (17, 37) reported estimates separately for type 1 and type 2 diabetes reporting equivocal findings. Vági et al. showed increased risk in type 1 diabetes, while Cusick reported similar risks in type 1 and type 2 diabetes. Our meta-analysis strongly supports the hypothesis that the mortality risk is much stronger in type 1 than in type 2 diabetes with a more than 2 times increased risk in type 1 vs type 2 diabetes (HR 2.22, 95%CI 1.43-3.45). An indirect support of the validity for the risk difference between type 1 and type 2 diabetes comes from a meta-analysis that reported similar observation between CAN and all-cause mortality (7).
We suspect that this observation is mostly related to the huge age difference between type 1 and type 2 diabetes patients. Younger diabetes patients without DSPN are likely to be free of diabetes complications (given the strong grouping of these complications) and have a good general health, while those with DSPN are likely to have other complications, hence a hugely increased mortality. In contrast older patients with type 2 diabetes have several vascular risk factors (such as obesity, hypertension, hyperlipidemia) and an elevated mortality already independent of DSPN status leading to a smaller relative mortality increase. However it is important to note here that given the much lower absolute risk in younger people, the absolute risks still remain much higher in type 2 compared to type 1 diabetes (15, 48). It is also possible that DSPN has different etiologies in type 1 and 2 diabetes with mostly related to hyperglycemia in type 1 diabetes vs a multifactorial (partly non-glycemia related) origin in type 2 diabetes (12). A potential further explanation could be related to the fact that adults with type 1 diabetes usually have more severe disease related to longer diabetes duration and worse glycemic control. While our sensitivity analysis adjusted for diabetes duration argues against the role of diabetes duration, we could not test the role of long-term glycemia due to poor quality data on glycemic control.
It should be noted that the relative mortality difference between type 1 and type 2 diabetes became non-significant in some of the sensitivity analyses. Given that the point estimates even in those models remained well above unity (1.6-2.0), we suspect that this is most likely a power issue.
In contrast to our hypothesis, study design had no strong effect on the association of DSPN with all-cause mortality supported by the similar overall estimates in our main analysis and in a sensitivity analysis restricted to population-based studies. Furthermore, we found no influential study that would significantly alter the findings. We excluded one study at the selection phase based on the possibility of referral bias (44). This study reported unadjusted association of DSPN with mortality in a population that was referred with symptoms to a neuropathy center. For the same reason, we excluded unadjusted estimates from the study of Vági et al., however this study also reported multiple adjusted estimates that seemed to control for the imbalance in mortality risk factors between patients with or without DSPN (37).
The meta-analyses that evaluated the effect of diabetes related CAN with all-cause mortality suggested that the method used for the assessment of neuropathy has a strong effect on the association with larger estimates if more than one modality was taken into account (6, 7). Based on this observation, we preplanned a sensitivity analysis restricted to those studies that used quantitative or semiquantitative tests for diagnosis.
The definition of DSPN in the different studies varied widely. Some of the cohorts used administrative data for the definition of DSPN that is prone to (for example) indication bias, we defined these measures as high risk of bias. Another, unstandardized way for the definition is the use of simple questions on the symptoms of DSPN. Given that their wording is different between studies, these could introduce variability when meta-analyzed. Simple physical examination of absent reflexes by themselves are weak instruments for the diagnosis of DSPN and they are becoming less frequently used in research partly due to their subjectivity.
A potential way to improve the symptom-based definition of DSPN is the use of standardized questionnaires. Several studies used the validated Michigan Neuropathy Screening Instrument (MNSI) for the screening of DSPN (49). It should be mentioned however that it has a low sensitivity (26-40%) with potential differences between type 1 and type 2 diabetes patients (50, 51). Beside MNSI, other, less validated questionnaires were also used in some studies. The low sensitivity of the questionnaire methods could underestimate the association of DSPN with all-cause mortality.
We selected studies that used different instruments for the definition of DSPN as the most reliable tests. While the used tests are heterogeneous, given their quantitative nature and the use of equipment, they are in general less subjective. Furthermore, a skilled assistant could complete the investigation, making them suitable for the testing of large populations. These methods are also advocated in clinical guidelines for the screening of DSPN. However, it should be noted that these tests measure different modalities of sensation (i.e. pain, touch, vibration, electric current) (52, 53).
A potential way to improve the definition of DSPN would be the use of a combination of a standardized questionnaire and equipment-based methods. However the number of studies that used both of these are so limited that we were unable to perform a meta-analysis with this definition (Table 1).
Our finding that the association was stronger in studies that used semiquantitative methods for the definition of DSPN suggests that the risk associated with DSPN is probably underestimated in our main analysis. Furthermore, this sensitivity analysis is also compatible with a higher relative mortality in type 1 vs type 2 diabetes with DSPN.
We used the Newcastle-Ottawa scale to measure the overall quality of studies that includes all the above detailed aspects of study design.(NOS) The findings of the analysis restricted to good quality studies confirmed our findings in the main analysis with mostly overlapping confidence intervals (5, 41).
The mechanism responsible for the association between DSPN and mortality is not well investigated. In general, DSPN is thought to be a determinant of reduced quality of life through disturbed sleep, physical functioning, recreation, and diminished physical and emotional well-being (54). However, the neuroendocrine, proinflammatory, and neurodegenerative underpinnings of DSPN could also lead to cardiovascular disease through increased oxidative stress and levels of advanced glycation end products (55, 56). DSPN is also associated with balance impairment that could lead to falls and injuries (56). DSPN is a leading factor of diabetic foot ulcers and amputations, both associated with increased mortality through infection and chronic inflammation (57).
Furthermore, diabetic pain per se (through similar mechanisms as DSPN itself) could be associated with an even further increased risk of mortality, as suggested by the observation of Lapin et al. on increased mortality only in those patients with painful DSPN but not in those with DSPN without pain compared to DSPN free controls (27). This hypothesis seems to be further strengthened by a meta-analysis that suggests an increased risk of mortality in people with widespread body pain irrespective of its origin even after adjustment for some mortality risk factors (58).
Alternatively, it is also possible that DSPN is a marker of other diseases that increase mortality. Indeed, microvascular diabetes complications (especially DSPN and CAN) show remarkable clustering (59). Thus, it is possible that the association between DSPN and mortality could be mediated through CAN.
Our meta-analysis was based on a predefined protocol standardizing the inclusion of studies and also the testing of our hypotheses. Overall, our current analysis is based on a sample with over 150 thousand participants with sufficiently high rates of mortality and DSPN to provide stable estimates. The main outcome (all-cause mortality) is a hard outcome that is unlikely to be imprecisely reported. The observed effect size is clinically relevant and statistically significant. The similar results in our main and sensitivity analyses further confirm the observed strong associations. Furthermore, our tests for influential studies and publication bias argues against major effects of individual studies or selective publication.
As the quality of any meta-analysis is mostly determined by the quality of the included studies, the main limitations of our report are mostly related to the quality of the included studies. First, a large proportion of the included studies include patients from tertiary care centers, from high-income countries with Caucasian origin. All of these factors limit the external validity of our findings. Furthermore, although some of the studies reported on multiple adjusted associations between DSPN and all-cause mortality, the role of unmeasured confounding cannot be excluded. The included studies had limited data on important mortality risk factors, such as different medications, laboratory parameters, proportion of participants with risk factors at target, or other comorbidities with increased mortality. Furthermore, the differences in the definition of DSPN could have biased our results. Given that we included only cohort studies, bias related to lost to follow-up cannot be excluded. While all-cause mortality is an easily obtainable outcome, it would be of interest to see the associations of DSPN with different causes of death.
Our meta-analysis strongly suggests that distal symmetric neuropathy in diabetes patients is associated with a substantially increased all-cause mortality in both type 1 and type 2 diabetes. Even if this finding is not causal, this observation should have an effect on clinical practice: the known modifiable risk factors of mortality should be treated more stringently in the presence of DSPN similarly to people with type 2 diabetes and chronic kidney disease (60). If this finding is causal, the lack of an etiological treatment of DSPN becomes even more important. The finding of a stronger association between DSPN and mortality in type 1 diabetes highlights the fact that the deleterious effect of DSPN is not limited to older people with type 2 diabetes.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
AT and MS contributed to the study conception and design. Analysis and interpretation were handled by all authors. Drafting of the article was handled by OV, MS, BD, VH, and AT. Critical revision for intellectual content was handled by all authors. All authors contributed to the article and approved the submitted version.
AT was supported by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund (2021 Thematic Excellence Programme funding scheme, TKP2021-NKTA-47). Open access funding was partly provided by Semmelweis University. The funders had no influence on study design, data collection, analysis, or interpretation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer VS declared a past co-authorship with the authors ST, PK to the handling editor.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1079009/full#supplementary-material
1. Huang Y, Karuranga S, Malanda B, Williams DRR. Call for data contribution to the IDF diabetes atlas 9th edition 2019. Diabetes Res Clin Pract (2018) 140:351–2. doi: 10.1016/j.diabres.2018.05.033
2. Emerging Risk Factors C, Sarwar N, Gao P, Seshasai SR, Gobin R, Kaptoge S, et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. (2010) 375(9733):2215–22. doi: 10.1016/S0140-6736(10)60484-9
3. Sasso FC, Simeon V, Galiero R, Caturano A, De Nicola L, Chiodini P, et al. The number of risk factors not at target is associated with cardiovascular risk in a type 2 diabetic population with albuminuria in primary cardiovascular prevention. Post-hoc Anal NID-2 trial. Cardiovasc Diabetol (2022) 21(1):235. doi: 10.1186/s12933-022-01674-7
4. Rawshani A, Rawshani A, Franzen S, Sattar N, Eliasson B, Svensson AM, et al. Risk factors, mortality, and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med (2018) 379(7):633–44. doi: 10.1056/NEJMoa1800256
5. Fox CS, Matsushita K, Woodward M, Bilo HJ, Chalmers J, Heerspink HJ, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis. Lancet (2012) 380(9854):1662–73. doi: 10.1016/S0140-6736(12)61350-6
6. Maser RE, Mitchell BD, Vinik AI, Freeman R. The association between cardiovascular autonomic neuropathy and mortality in individuals with diabetes: A meta-analysis. Diabetes Care (2003) 26(6):1895–901. doi: 10.2337/diacare.26.6.1895
7. Chowdhury M, Nevitt S, Eleftheriadou A, Kanagala P, Esa H, Cuthbertson DJ, et al. Cardiac autonomic neuropathy and risk of cardiovascular disease and mortality in type 1 and type 2 diabetes: A meta-analysis. BMJ Open Diabetes Res Care (2021) 9(2):e002480. doi: 10.1136/bmjdrc-2021-002480
8. Pop-Busui R, Boulton AJ, Feldman EL, Bril V, Freeman R, Malik RA, et al. Diabetic neuropathy: A position statement by the American diabetes association. Diabetes Care (2017) 40(1):136–54. doi: 10.2337/dc16-2042
9. Putz Z, Tabak AG, Toth N, Istenes I, Nemeth N, Gandhi RA, et al. Noninvasive evaluation of neural impairment in subjects with impaired glucose tolerance. Diabetes Care (2009) 32(1):181–3. doi: 10.2337/dc08-1406
10. Singleton JR, Smith AG, Bromberg MB. Increased prevalence of impaired glucose tolerance in patients with painful sensory neuropathy. Diabetes Care (2001) 24(8):1448–53. doi: 10.2337/diacare.24.8.1448
11. Ziegler D, Rathmann W, Dickhaus T, Meisinger C, Mielck A, Group KS. Neuropathic pain in diabetes, prediabetes and normal glucose tolerance: the MONICA/KORA augsburg surveys S2 and S3. Pain Med (2009) 10(2):393–400. doi: 10.1111/j.1526-4637.2008.00555.x
12. Hicks CW, Wang D, Matsushita K, Windham BG, Selvin E. Peripheral neuropathy and all-cause and cardiovascular mortality in U.S. adults: A prospective cohort study. Ann Intern Med (2021) 174(2):167–74. doi: 10.7326/M20-1340
13. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: A proposal for reporting. meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. (2000) 283(15):2008–12. doi: 10.1001/jama.283.15.2008
14. Bjerg L, Nicolaisen SK, Christensen DH, Nielsen JS, Andersen ST, Jorgensen ME, et al. Diabetic polyneuropathy early in type 2 diabetes is associated with higher incidence rate of cardiovascular disease: Results from two Danish cohort studies. Diabetes Care (2021) 44(7):1714–21. doi: 10.2337/dc21-0010
15. Bjerg L, Hulman A, Carstensen B, Charles M, Witte DR, Jorgensen ME. Effect of duration and burden of microvascular complications on mortality rate in type 1 diabetes: An observational clinical cohort study. Diabetologia. (2019) 62(4):633–43. doi: 10.1007/s00125-019-4812-6
16. Brownrigg JR, de Lusignan S, McGovern A, Hughes C, Thompson MM, Ray KK, et al. Peripheral neuropathy and the risk of cardiovascular events in type 2 diabetes mellitus. Heart. (2014) 100(23):1837–43. doi: 10.1136/heartjnl-2014-305657
17. Cusick M, Meleth AD, Agron E, Fisher MR, Reed GF, Knatterud GL, et al. Associations of mortality and diabetes complications in patients with type 1 and type 2 diabetes: early treatment diabetic retinopathy study report no. 27. Diabetes Care (2005) 28(3):617–25. doi: 10.2337/diacare.28.3.617
18. Forsblom CM, Sane T, Groop PH, Totterman KJ, Kallio M, Saloranta C, et al. (non-insulin-dependent) diabetes: Evidence of a role for neuropathy and a protective effect of HLA-DR4. Diabetologia. (1998) 41(11):1253–62. doi: 10.1007/s001250051062
19. Foryoung JB, Ditah C, Nde Fon P, Mboue-Djieka Y, Nebongo DN, Mbango ND, et al. Long-term mortality in outpatients with type 2 diabetes in a reference hospital in Cameroon: A retrospective cohort study. BMJ Open (2018) 8(2):e019086. doi: 10.1136/bmjopen-2017-019086
20. Garofolo M, Gualdani E, Giannarelli R, Aragona M, Campi F, Lucchesi D, et al. Microvascular complications burden (nephropathy, retinopathy and peripheral polyneuropathy) affects risk of major vascular events and all-cause mortality in type 1 diabetes: A 10-year follow-up study. Cardiovasc Diabetol (2019) 18(1):159. doi: 10.1186/s12933-019-0961-7
21. Gregory R, Tattersall RB, Allison SP. Peripheral neuropathy as a presenting feature of type 2 diabetes: a case-controlled study. Diabetes Med (1994) 11(4):407–9. doi: 10.1111/j.1464-5491.1994.tb00294.x
22. Hansen GM, Jorgensen PG, Andersen HU, Rossing P, Jensen MT. Relationship between peripheral neuropathy, diastolic function and adverse cardiovascular outcome in individuals with type 1 diabetes mellitus without known cardiovascular disease: Results from the thousand & 1 study. Diabetes Obes Metab (2021) 23(1):158–65. doi: 10.1111/dom.14209
23. Hsu WC, Chiu SY, Yen AM, Chen LS, Fann CY, Liao CS, et al. Somatic neuropathy is an independent predictor of all- and diabetes-related mortality in type 2 diabetic patients: A population-based 5-year follow-up study (KCIS no. 29). Eur J Neurol (2012) 19(9):1192–8. doi: 10.1111/j.1468-1331.2011.03659.x
24. Kaze AD, Santhanam P, Erqou S, Bertoni AG, Ahima RS, Echouffo-Tcheugui JB. Microvascular disease and cardiovascular outcomes among individuals with type 2 diabetes. Diabetes Res Clin Pract (2021) 176:108859. doi: 10.1016/j.diabres.2021.108859
25. Kloecker DE, Khunti K, Davies MJ, Pitocco D, Zaccardi F. Microvascular disease and risk of cardiovascular events and death from intensive treatment in type 2 diabetes: The ACCORDION study. Mayo Clin Proc (2021) 96(6):1458–69. doi: 10.1016/j.mayocp.2020.08.047
26. Kristensen SL, Rorth R, Jhund PS, Shen L, Lee MMY, Petrie MC, et al. Microvascular complications in diabetes patients with heart failure and reduced ejection fraction-insights from the beta-blocker evaluation of survival trial. Eur J Heart Fail (2018) 20(11):1549–56. doi: 10.1002/ejhf.1201
27. Lapin BR, Pantalone KM, Milinovich A, Morrison S, Schuster A, Boulos F, et al. Pain in patients with type 2 diabetes-related polyneuropathy is associated with vascular events and mortality. J Clin Endocrinol Metab (2020) 105(9):3005–14. doi: 10.1210/clinem/dgaa394
28. Lester FT. Clinical features, complications and mortality in type 1 (insulin-dependent) diabetic patients in Addis Ababa, Ethiopia, 1976-1990. Q J Med (1992) 83(301):389–99. doi: 10.1093/oxfordjournals.qjmed.a068677
29. McEwen LN, Ylitalo KR, Munson M, Herman WH, Wrobel JS. Foot complications and mortality: Results from translating research into action for diabetes (TRIAD). J Am Podiatr Med Assoc (2016) 106(1):7–14. doi: 10.7547/14-115
30. Navarro X, Kennedy WR, Aeppli D, Sutherland DE. Neuropathy and mortality in diabetes: influence of pancreas transplantation. Muscle Nerve. (1996) 19(8):1009–16. doi: 10.1002/(SICI)1097-4598(199608)19:8<1009::AID-MUS9>3.0.CO;2-4
31. O'Brien IA, McFadden JP, Corrall RJ. The influence of autonomic neuropathy on mortality in insulin-dependent diabetes. Q J Med (1991) 79(290):495–502. doi: 10.1093/oxfordjournals.qjmed.a068570
32. Scain SF, Franzen E, Hirakata VN. Effects of nursing care on patients in an educational program for prevention of diabetic foot. Rev Gaucha Enferm. (2018) 39:e20170230. doi: 10.1590/1983-1447.2018.20170230
33. Seferovic JP, Pfeffer MA, Claggett B, Desai AS, de Zeeuw D, Haffner SM, et al. Three-question set from Michigan neuropathy screening instrument adds independent prognostic information on cardiovascular outcomes: Analysis of ALTITUDE trial. Diabetologia. (2018) 61(3):581–8. doi: 10.1007/s00125-017-4485-y
34. Soedamah-Muthu SS, Chaturvedi N, Witte DR, Stevens LK, Porta M, Fuller JH, et al. Relationship between risk factors and mortality in type 1 diabetic patients in Europe: The EURODIAB prospective complications study (PCS). Diabetes Care (2008) 31(7):1360–6. doi: 10.2337/dc08-0107
35. Suarez GA, Clark VM, Norell JE, Kottke TE, Callahan MJ, O'Brien PC, et al. Sudden cardiac death in diabetes mellitus: Risk factors in the Rochester diabetic neuropathy study. J Neurol Neurosurg Psychiatry (2005) 76(2):240–5. doi: 10.1136/jnnp.2004.039339
36. Sudore RL, Karter AJ, Huang ES, Moffet HH, Laiteerapong N, Schenker Y, et al. Symptom burden of adults with type 2 diabetes across the disease course: Diabetes & aging study. J Gen Intern Med (2012) 27(12):1674–81. doi: 10.1007/s11606-012-2132-3
37. Vagi OE, Svebis MM, Domjan BA, Korei AE, Istenes I, Putz Z, et al. Association of cardiovascular autonomic neuropathy and distal symmetric polyneuropathy with all-cause mortality: A retrospective cohort study. J Diabetes Res (2021) 2021:6662159. doi: 10.1155/2021/6662159
38. Weis U, Turner B, Gibney J, Watts GF, Burke V, Shaw KM, et al. Long-term predictors of coronary artery disease and mortality in type 1 diabetes. QJM. (2001) 94(11):623–30. doi: 10.1093/qjmed/94.11.623
39. Yokomichi H, Nagai A, Hirata M, Mochizuki M, Kojima R, Yamagata Z, et al. Cause-specific mortality rates in patients with diabetes according to comorbid macro- and microvascular complications: BioBank Japan cohort. Endocrinol Diabetes Metab (2021) 4(1):e00181. doi: 10.1002/edm2.181
40. Ziegler D, Buchholz S, Sohr C, Nourooz-Zadeh J, Roden M. Oxidative stress predicts progression of peripheral and cardiac autonomic nerve dysfunction over 6 years in diabetic patients. Acta Diabetol (2015) 52(1):65–72. doi: 10.1007/s00592-014-0601-3
41. Wells BS GA, O'Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (2011). Available at: https://www.ohri.ca//programs/clinical_epidemiology/oxford.asp.
42. Riley RD, Higgins JP, Deeks JJ. Interpretation of random effects meta-analyses. BMJ. (2011) 342:d549. doi: 10.1136/bmj.d549
43. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: A new edition of the cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev (2019) 10:ED000142. doi: 10.1002/14651858.ED000142
44. Ewing DJ, Campbell IW, Clarke BF. The natural history of diabetic autonomic neuropathy. Q J Med (1980) 49(193):95–108. doi: 10.1093/oxfordjournals.qjmed.a067610
45. Orchard TJ, LL CE, Maser RE, Kuller LH. Why does diabetic autonomic neuropathy predict IDDM mortality? an analysis from the Pittsburgh epidemiology of diabetes complications study. Diabetes Res Clin Pract (1996) 34 Suppl:S165–71. doi: 10.1016/S0168-8227(96)90025-X
46. Tesfaye S, Chaturvedi N, Eaton SE, Ward JD, Manes C, Ionescu-Tirgoviste C, et al. Vascular risk factors and diabetic neuropathy. N Engl J Med (2005) 352(4):341–50. doi: 10.1056/NEJMoa032782
47. Feldman EL, Callaghan BC, Pop-Busui R, Zochodne DW, Wright DE, Bennett DL, et al. Diabetic neuropathy. Nat Rev Dis Primers. (2019) 5(1):41. doi: 10.1038/s41572-019-0092-1
48. Hulman A, Simmons RK, Brunner EJ, Witte DR, Faerch K, Vistisen D, et al. Trajectories of glycaemia, insulin sensitivity and insulin secretion in south Asian and white individuals before diagnosis of type 2 diabetes: A longitudinal analysis from the Whitehall II cohort study. Diabetologia. (2017) 60(7):1252–60. doi: 10.1007/s00125-017-4275-6
49. Feldman EL, Stevens MJ, Thomas PK, Brown MB, Canal N, Greene DA. A practical two-step quantitative clinical and electrophysiological assessment for the diagnosis and staging of diabetic neuropathy. Diabetes Care (1994) 17(11):1281–9. doi: 10.2337/diacare.17.11.1281
50. Herman WH, Pop-Busui R, Braffett BH, Martin CL, Cleary PA, Albers JW, et al. Use of the Michigan neuropathy screening instrument as a measure of distal symmetrical peripheral neuropathy in type 1 diabetes: Results from the diabetes control and complications Trial/Epidemiology of diabetes interventions and complications. Diabetes Med (2012) 29(7):937–44. doi: 10.1111/j.1464-5491.2012.03644.x
51. Gylfadottir SS, Itani M, Kroigard T, Kristensen AG, Christensen DH, Nicolaisen SK, et al. Diagnosis and prevalence of diabetic polyneuropathy: A cross-sectional study of Danish patients with type 2 diabetes. Eur J Neurol (2020) 27(12):2575–85. doi: 10.1111/ene.14469
52. Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care (2010) 33(10):2285–93. doi: 10.2337/dc10-1303
53. American Diabetes Association Professional Practice C, Draznin B, Aroda VR, Bakris G, Benson G, Brown FM, et al. 12. retinopathy, neuropathy, and foot care: Standards of medical care in diabetes-2022. Diabetes Care (2022) 45(Suppl 1):S185–S94. doi: 10.2337/dc22-S012
54. Jensen MP, Chodroff MJ, Dworkin RH. The impact of neuropathic pain on health-related quality of life: Review and implications. Neurology. (2007) 68(15):1178–82. doi: 10.1212/01.wnl.0000259085.61898.9e
55. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: The role of cytokines in the pathophysiology of major depression. Biol Psychiatry (2009) 65(9):732–41. doi: 10.1016/j.biopsych.2008.11.029
56. Hewston P, Deshpande N. Falls and balance impairments in older adults with type 2 diabetes: Thinking beyond diabetic peripheral neuropathy. Can J Diabetes. (2016) 40(1):6–9. doi: 10.1016/j.jcjd.2015.08.005
57. Saluja S, Anderson SG, Hambleton I, Shoo H, Livingston M, Jude EB, et al. Foot ulceration and its association with mortality in diabetes mellitus: A meta-analysis. Diabetes Med (2020) 37(2):211–8. doi: 10.1111/dme.14151
58. Macfarlane GJ, Barnish MS, Jones GT. Persons with chronic widespread pain experience excess mortality: Longitudinal results from UK biobank and meta-analysis. Ann Rheum Dis (2017) 76(11):1815–22. doi: 10.1136/annrheumdis-2017-211476
59. Bjerg L, Hulman A, Charles M, Jorgensen ME, Witte DR. Clustering of microvascular complications in type 1 diabetes mellitus. J Diabetes Complications. (2018) 32(4):393–9. doi: 10.1016/j.jdiacomp.2018.01.011
Keywords: meta-analysis, cohort studies, all-cause mortality, diabetes mellitus, type 1 diabetes, type 2 diabetes, distal symmetric polyneuropathy
Citation: Vági OE, Svébis MM, Domján BA, Körei AE, Tesfaye S, Horváth VJ, Kempler P and Tabák ÁG (2023) The association between distal symmetric polyneuropathy in diabetes with all-cause mortality – a meta-analysis. Front. Endocrinol. 14:1079009. doi: 10.3389/fendo.2023.1079009
Received: 14 November 2022; Accepted: 30 January 2023;
Published: 16 February 2023.
Edited by:
Ferdinando Carlo Sasso, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Alfredo Caturano, University of Campania Luigi Vanvitelli, ItalyCopyright © 2023 Vági, Svébis, Domján, Körei, Tesfaye, Horváth, Kempler and Tabák. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Orsolya E. Vági, dmFnaW9yc2lAZ21haWwuY29t; Ádám Gy. Tabák, YS50YWJha0B1Y2wuYWMudWs=
†These authors share first authorship
‡These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.