 Dorota Filipowicz1*
Dorota Filipowicz1* Ewelina Szczepanek-Parulska1
Ewelina Szczepanek-Parulska1 Aniceta A. Mikulska-Sauermann2
Aniceta A. Mikulska-Sauermann2 Marta Karaźniewicz-Łada2Franciszek K. Główka2Krzysztof Szymanowski3
Marta Karaźniewicz-Łada2Franciszek K. Główka2Krzysztof Szymanowski3 Mariusz Ołtarzewski4
Mariusz Ołtarzewski4 Lutz Schomburg5
Lutz Schomburg5 Marek Ruchała1
Marek Ruchała1- 1Department of Endocrinology, Metabolism and Internal Medicine, Poznan University of Medical Sciences, Poznan, Poland
- 2Department of Physical Pharmacy and Pharmacokinetics, Poznan University of Medical Sciences, Poznan, Poland
- 3Department of Perinatology and Gynaecology, Poznan University of Medical Sciences, Poznan, Poland
- 4Institute of Mother and Child, Warsaw, Poland
- 5Institute of Experimental Endocrinology, Charité - Universitätsmedizin Berlin, Berlin, Germany
Introduction: Iodine is a pivotal component of thyroid hormones, and its deficiency leads to negative pregnancy outcomes. Therefore, during gestation, additional iodine supplementation is recommended.
Objectives: By evaluating a group of women from western Poland, the study updated on iodine status during pregnancy and the effectiveness of iodine supplementation in relation to the maternal and neonatal thyroid function.
Patients and methods: A total of 91 women were recruited before the delivery between 2019 and 2021. During the medical interview, the patients declared their dietary supplements intake. Thyroid parameters (TSH, ft3, ft4, a-TPO, a-Tg, and TRAb) were measured in the serum of mothers and in the cord blood of newborns after birth. Urinary iodine concentration (UIC) and urine/creatinine (UIC/crea) ratio were assessed in single urine samples using a validated high-performance liquid chromatography with ultraviolet detection (HPLC-UV). Neonatal TSH screening from dried blood spot was analyzed.
Results: Pregnant women showed a median (interquartile range) UIC of 106 (69–156) µg/liter and UIC/crea ratio of 104 (62–221) µg/g, whereas approximately 20% had UIC/crea below 50 µg/g, indicating iodine deficiency. The iodine supplementation ratio was 68%. No significant differences in UIC, UIC/crea and thyroid parameters were found between iodine supplemented and non-supplemented groups; however, the highest ioduria was detected when iodine was supplemented in addition to levothyroxine in comparison with both substances administered separately. Patients with UIC/crea within 150–249 µg/g demonstrated the lowest TSH and a-TPO levels. Screening TSH was above 5 mIU/liter in 6% of children.
Conclusions: Despite the national salt iodization and the recommendation to supplement iodine during gestation, the status of the abovementioned microelement and real-life intake revealed the ineffectiveness of the current iodine-deficiency prophylaxis model in pregnancy.
1 Introduction
Thyroid dysregulation is a prevalent clinical issue, particularly relevant during pregnancy, affecting almost one-fifth of women. In the course of gestation, the requirement for thyroid hormones (THs) increases by 25–50%, due to the elevation in thyroid-binding globulin production, placental transfer of iodine and thyroxine (T4) to the fetus, TH degradation in the placenta and the enhanced renal microelement clearance (1). Moreover, THs are involved in the neuronal migration and myelination during fetal nervous system development (2). Notably, iodine represents a fundamental component of THs. Pregnant women with iodine deficiency frequently suffer from hypothyroidism (HT) as well as goiter and present an increased risk of developing thyroid autoimmunity (3). Moreover, TH deficiency results in poorer obstetric outcomes, such as higher prevalence of miscarriages, stillbirths, growth retardation, and congenital abnormalities (4). Significant iodine deficiency in prenatal life leads to the most severe form of HT, whereas mild or moderate maternal lack of iodine may cause intellectual disability, disturbed psychomotor function, poorer socialization, and a decreased IQ score in school-aged children (5, 6). In 1997 in Poland, the iodine deficiency prophylaxis program was introduced, involving mandatory iodization of household salt [20–40 mg potassium iodide (KI) per kg of salt] or neonate formulas (10 μg/100 ml of milk), and recommending additional supplementation of 100–150 μg KI per day for pregnant and breastfeeding women, which subsequently restored the optimal iodine status in the general population (7). In terms of epidemiology, it eradicated the endemic goiter in children and reduced its prevalence in pregnant women (from 80 to 19%), decreased neonatal transient HT (from 2 to 0.16%), as well as limited the thyroid cancer incidence in women over 40 years of age (8, 9). According to the latest WHO report, Poland fulfilled the requirement of > 90% of households with iodinated salt (7).
However, salt consumption may currently decrease due to the high incidence of hypertension in the population and the recommendations of the Polish Society of Hypertension, which aim to decrease the daily salt intake to 5 g/day or due to a higher proportion of imported food in the local diet (10, 11). Nevertheless, in terms of the optimal ioduria, following a 10- and almost 20-year follow-up after the introduction of the prophylaxis, the program has undoubtedly failed with regard to pregnant and lactating women (12, 13). Therefore, the necessity of additional iodine supplementation in the dose of 150–200 µg daily during pregnancy and the lactation period was particularly emphasized in the latest guidelines of the Polish Society of Endocrinology (14).
In contrast, according to the consensus of the World Health Organization (WHO), the United Nations Children’s Fund (UNICEF) and the International Council for Control of Iodine Deficiency Disorders (ICCIDD), currently renamed as the Iodine Global Network (IGN), iodine supplementation is not recommended when the general population has been iodine-sufficient over the previous 2 years, as expressed by urinary iodine concentration (UIC) >/= 100 µg/liter, whereas the UIC value of < 150 µg has been defined as a deficiency in the course of pregnancy (15). The abovementioned recommendations are ambiguous, although they remain unanimous regarding the benefits of continuous monitoring and updating iodine status in pregnancy worldwide. The available national data evaluating iodine deficiency prophylaxis effectiveness were obtained from central, northern, and southern regions of Poland, in which all experts concur regarding the ineffectiveness of this model among pregnant women. However, to date, no studies have been conducted on residents of the western part of the country (12, 16–18).
The objective of the study was to evaluate iodine status in pregnant women and assess the supplementation rate, effects, and guidelines adherence in a real-life setting among pregnant women from western Poland, with a particular emphasis on maternal and neonatal thyroid function.
2 Patients and methods
The study comprised 91 Caucasian women from the area of Greater Poland (western region of Poland) who were enrolled on admission to the obstetric ward prior to their term delivery. They were randomly recruited in a public hospital, which is the leading obstetrics center in the western Poland—Gynecological and Obstetric Clinical Hospital at Poznan University of Medical Sciences (tertiary referral center) within the period between 2019 and 2021. The group consisted of women, who were healthy, euthyroid, or hypothyroid in the range adjusted to the pregnancy status, with or without antithyroid antibodies [anti-thyroid peroxidase (a-TPO), anti-thyroglobulin (a-Tg), anti–TSH-receptor (TRAb)], and either treated or not with levothyroxine (LT4). They were divided into subgroups receiving supplementation or not, treated with LT4 or not, as well as into a subgroup with or without antithyroid antibodies. Patients were in good general condition, with a negative history of any serious chronic diseases, malignancies, or renal/liver disease (except for benign cysts). None of the patients declared a specific type of diet, including a fish-rich, vegan, or vegetarian diet, and the patients denied foreign trips lasting more than 1 month.
Patients were screened and interviewed by instructed midwives in terms of inclusion/exclusion criteria and the intake of dietary supplements during pregnancy, including product brand name, dose, frequency, and duration. A random single spot urine sample was collected before the delivery and stored in a freezer at −20°C in the amount of approximately 10 ml. Additionally, a maternal non-fasting venous blood sample was taken by venipuncture prior to the delivery. Up to 2 ml of cord blood from the neonatal part of the placenta was collected during the third phase of labor after cessation of umbilical cord pulsation. Both serum samples were stored frozen in −20°C. Ioduria, as UIC, was measured using a validated ion-pair high-performance liquid chromatography with ultraviolet detection (HPLC–UV), as described (19). Creatinine was determined in the same urine sample by a colorimetric enzyme-linked immunosorbent assay (ELISA) detection kit (ThermoFisher, EIACUN, Frederick, USA). In order to objectify the results, the urinary iodine/creatinine ratio (UIC/crea) was calculated. UIC and UIC/crea results were analyzed according to the latest WHO criteria for iodine status assessment in pregnant women (20). Concentrations of serum TSH, ft3, ft4, and antithyroid antibodies (a-TPO, a-Tg) were measured by means of electrochemiluminescence (ECLIA, Hitachi and Roche Diagnostics kits) using Cobas e601 analyzer (Indianapolis, IN, USA) and TRAb by radioimmunoassay (RIA, BRAHMS Diagnostics, Berlin, Germany). Neonatal TSH was verified on the 3rd–4th day of life (TSHs) as part of national screening for congenital HT. The measurement was performed in dried blood spots from the heel puncture by an immunoluminometric (LIA) assay.
The study was performed in accordance with the Declaration of Helsinki (21) and was approved by The Local Bioethics Committee of Poznan University of Medical Sciences (protocol no. 104/19, date of approval: 10 January 2019, annexed 4 February 2021, protocol no. 132/21).
2.1 Statistical analysis
Statistica, version 13.3 (TIBCO Software Inc., California, USA), GraphPad Prism, version 9.5.1. (GraphPad Software, LCC, Boston, USA) and Microsoft Excel (2019) from Microsoft Office (Adobe Inc., California, USA) were used for statistical calculations. The data were not normally distributed, according to Shapiro–Wilk’s test, thus non-parametric statistical tests were applied. The groups were compared using the Mann–Whitney U or the paired Wilcoxon test (when parameters were analyzed within the mother–child pairs), as well as the analysis of variance (ANOVA)/Kruskal–Wallis tests with post-hoc analysis. The Spearman R test was performed to analyze correlations between the parameters. The results are presented mainly as the median and interquartile range (IQR, Q1–Q3), 95% confidence intervals (95% CIs), or mean with standard deviation (± SD). A p-value < 0.05 was considered significant.
3 Results
The patients’ characteristics are presented in Table 1.
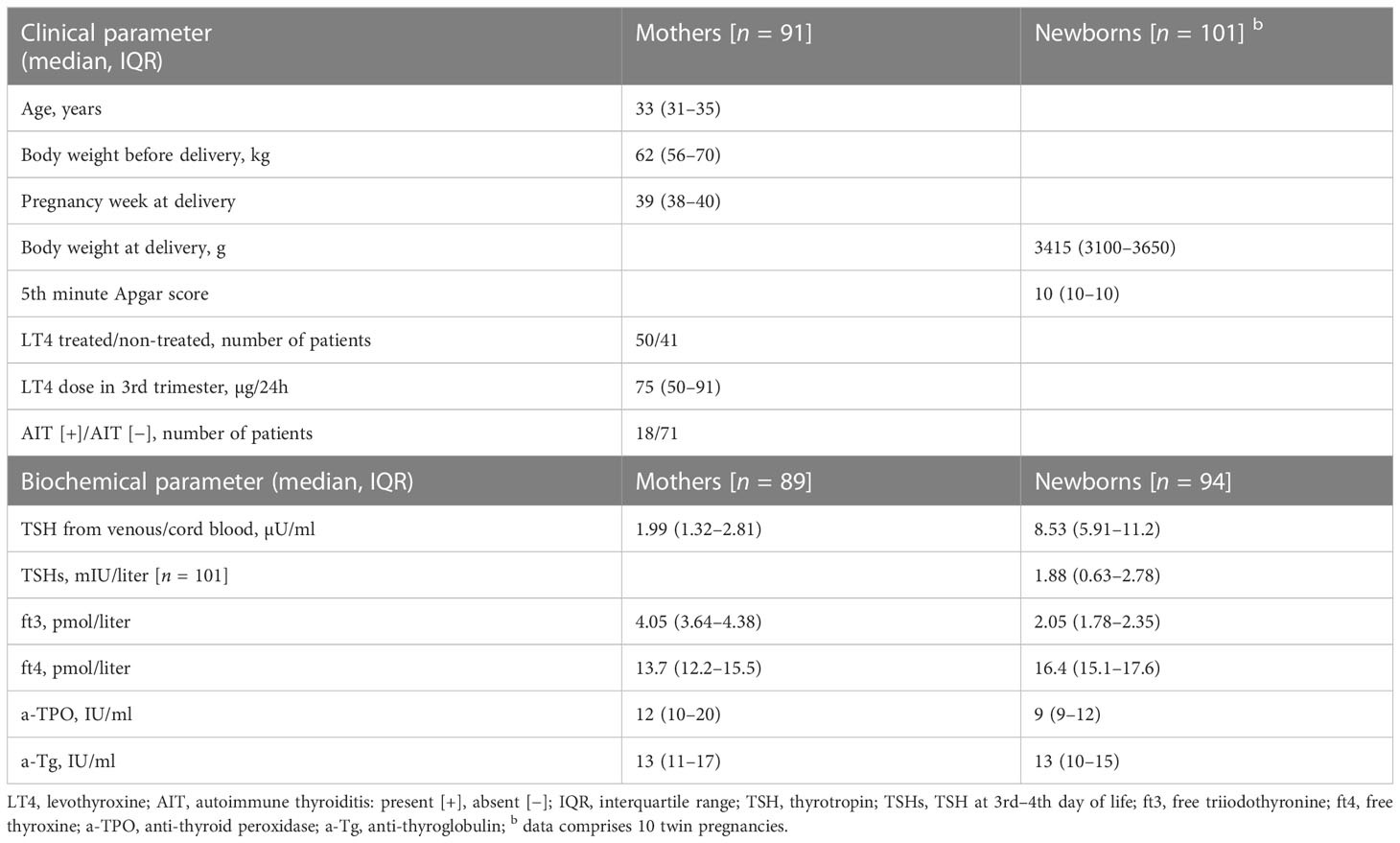
Table 1 Clinical and biochemical characteristics of the recruited women and newborns.
Pregnant women from the western Poland showed a median (IQR) UIC 106 (69–156) µg/liter and UIC/crea ratio equal to 104 (62–221) µg/g, which is defined as iodine deficiency (UIC or UIC/crea < 150 µg/liter or µg/g) for this particular group, according to the WHO ranges (15); see Table 2. Approximately 20% had UIC/crea below 50 µg/g, which is a borderline value for another indicator of iodine deficits. The correlation was observed between both indicators of ioduria used in the study, that is, UIC and UIC/crea (R = 0.63, p < 0.001).
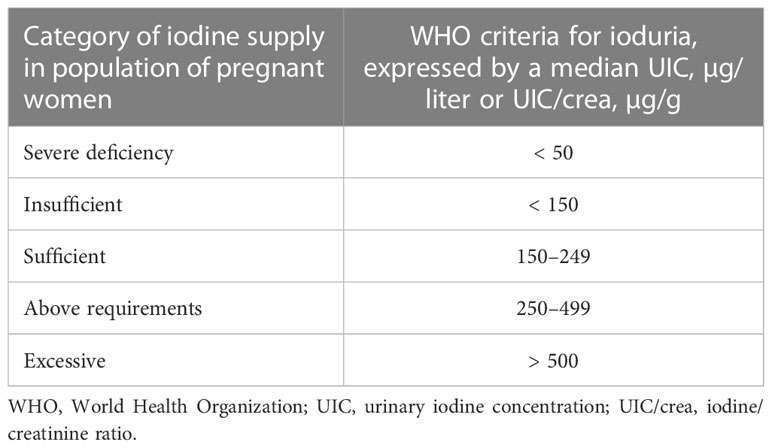
Table 2 Median ioduria of pregnant women according to the WHO classification.
Supplementation of iodine during pregnancy was declared by 62/91 pregnant women (68%). In the majority of cases, iodine was ingested as a part of multivitamin diet supplements in a median dose (IQR) of 200 (150–200) per day, with a range extending from 100–300 µg/day. In 13 out of 62 (21%) cases, iodine was not supplemented throughout the entire pregnancy, 4/62 (6.5%) of patients administered it only in the 1st and 2nd trimester, and 9/62 (14.5%) only in the 3rd trimester of pregnancy. The dose and formula of the dietary supplements are presented in Table 3.
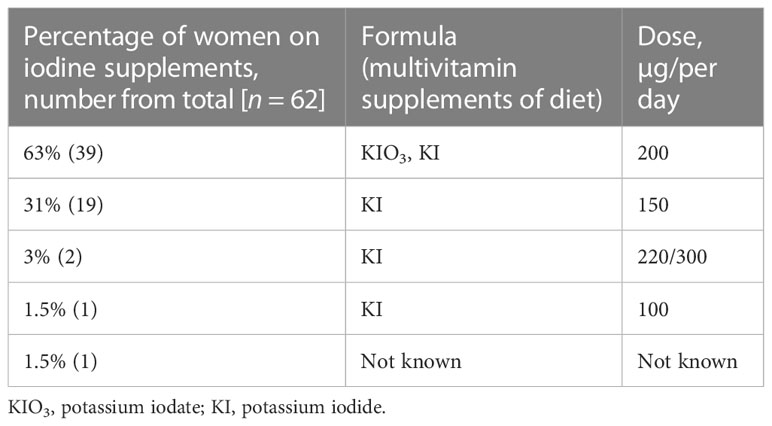
Table 3 Iodine supplements, doses, and formulas declared by pregnant women.
In the subsequent stages of the analysis, women who did not supplement iodine in the 3rd trimester and patients who presented abnormal TSH for this period of pregnancy were excluded.
No significant differences in UIC (median, Q1–Q3) were found in the group which declared iodine supplementation (105 µg/liter, 69–170, n = 50) in comparison with the women who denied iodine supplementation (99 µg/liter, 84–130, n = 27) during pregnancy (p = 0.55); see Figure 1.
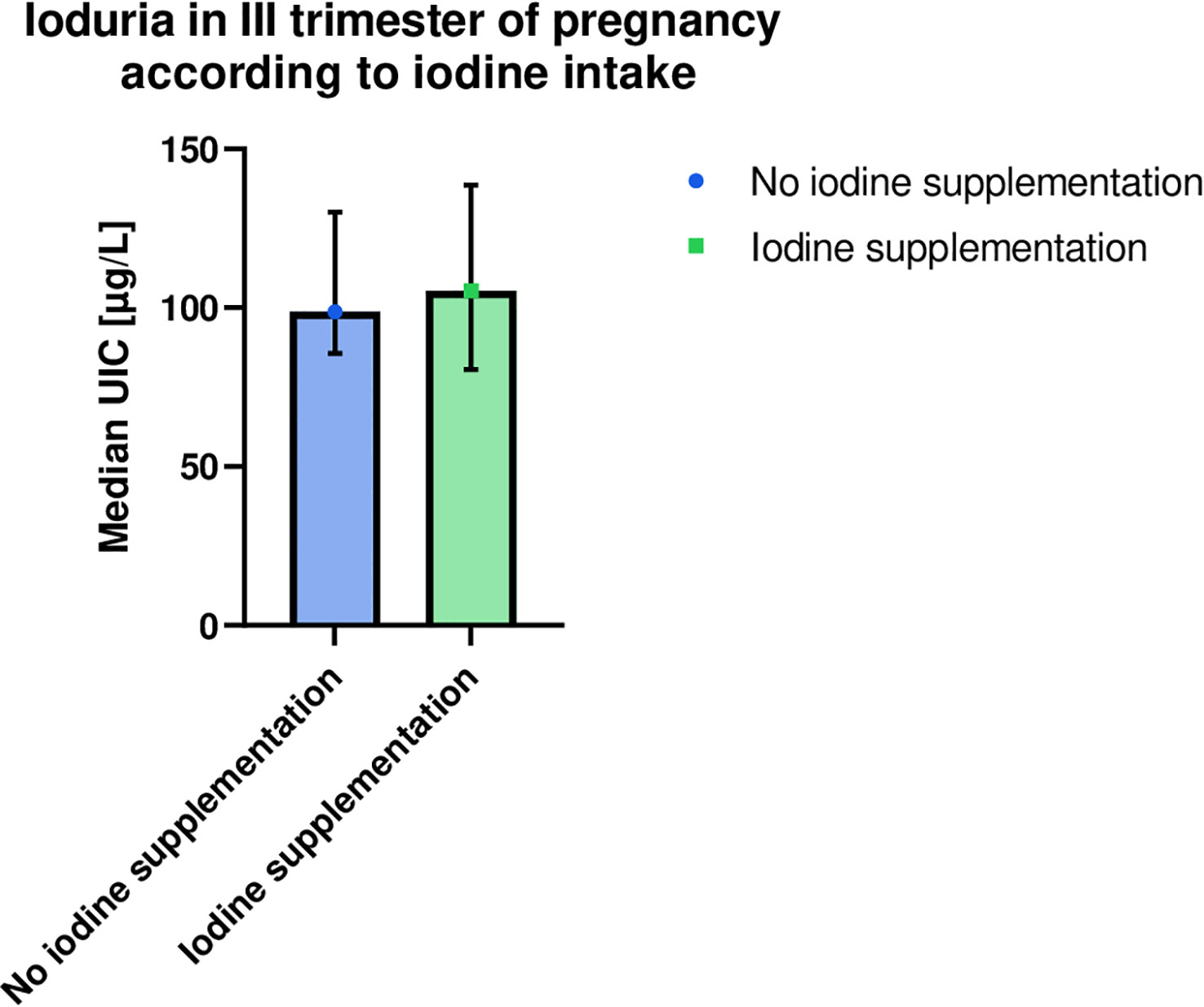
Figure 1 Comparison of ioduria in the last trimester of pregnancy in women who confirmed or denied iodine supplementation. Higher median UIC and wider confidence interval (95% CI) were observed in the iodine supplementing group, although the result was not significant (p = 0.55). Both intervals are below the normal range established by the World Health Organization (< 150 μg/liter). Medians (symbols), 95% CI (error bars). UIC, urinary iodine concentration.
There was no significant difference in UIC between the iodine-supplemented and non-supplemented groups, also in the subgroups of patients not treated with LT4 (p = 0.47) as well as those receiving the medication (p = 0.15).
No difference was found between the group of iodine-supplementing and non-supplementing mothers and those showing UIC below and above 150 µg/liter in maternal and neonatal thyroid hormone indices (TSH, ft3, ft4, and TSHs), even after excluding patients receiving LT4. There were also no differences in maternal and child antibodies (a-TPO, a-Tg, and TRAb) with regards to iodine supplementation, tested in both AIT(+) and AIT (−) subgroups.
All thyroid antibodies of mothers and their children correlated positively (a-TPO with p < 0.001, R = 0.59; a-Tg with p < 0.001, R = 0.52; TRAb with p < 0.001, R = 0.49). Additionally, the children’s ft4 correlated with maternal TRAb level (p = 0.03, R = −0.26), and cord blood TSH correlated with the mothers’ UIC (p = 0.03, R = 0.25).
A comparison of the three groups of women receiving external iodine source, that is, iodine without LT4, LT4 without iodine and the combined iodine and LT4 intake, revealed no significant differences regarding UIC (p = 0.18) or UIC/crea (p = 0.09). However, the highest ioduria was reported in the group with the combined LT4 and iodine intake; see Figure 2.
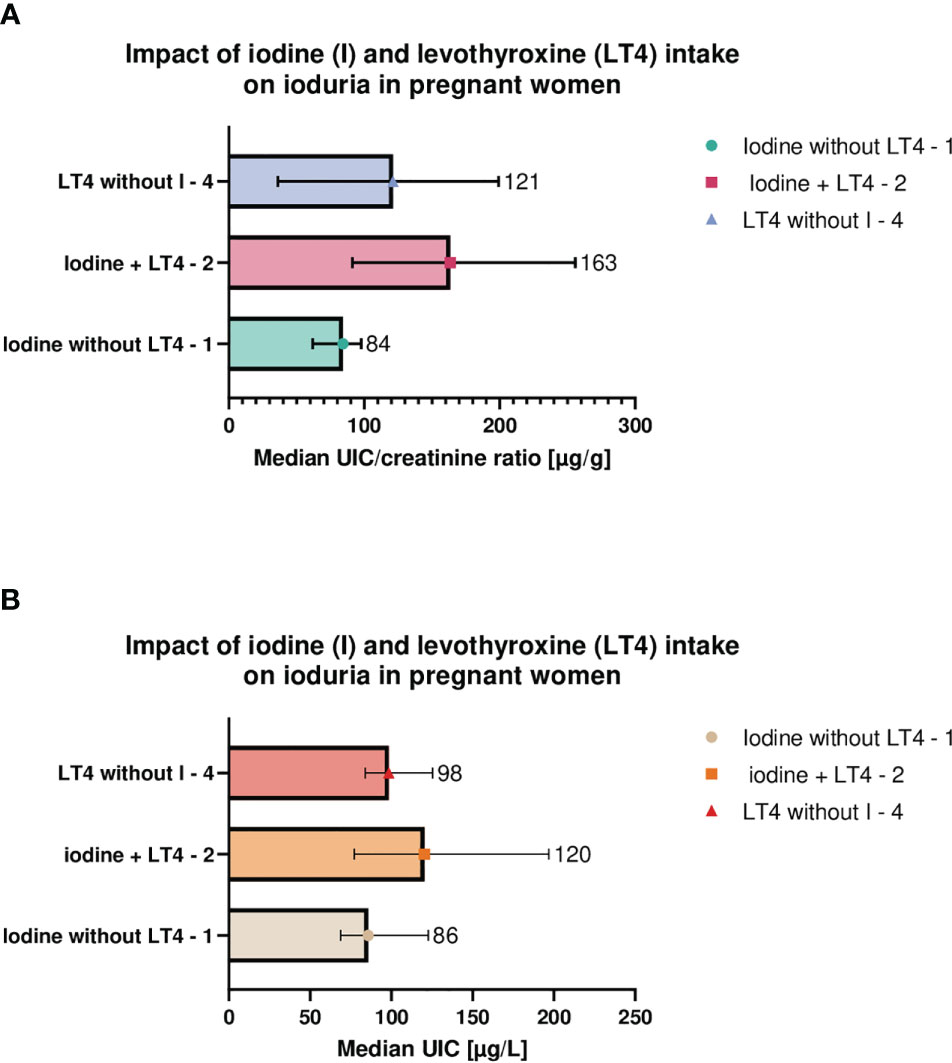
Figure 2 Maternal urinary iodine concentration (A) and iodine/creatinine ratio (B) in relation to levothyroxine and/or iodine supplements intake. Pregnant women differed with respect to iodine (I) and levothyroxine (LT4) intake and were divided into three groups; I only (group 1), LT4 only (group 2), or the combined I and LT4 intake (group 3). No significant differences in urinary iodine concentration (UIC, p = 0.18, KW-H = 3.46) and iodine/creatinine ratio (UIC/crea, p = 0.09, KW-H = 5.84) between the groups were observed. However, the highest UIC or UIC/crea were observed in the group with the combined LT4 therapy and I supplementation. Medians (symbols and numbers), 95% CI (error bars) are shown. UIC/crea, urine/creatinine ratio; LT4, levothyroxine; I, iodine; KW-H, the result of Kruskal–Wallis test.
Women with UIC/crea within 150–249 µg/g presented the lowest values of TSH (in the subgroup after excluding LT4-treated patients) and a-TPO (in the subgroup with the negative antithyroid antibodies) in comparison with those with a lower or higher ioduria (Table 4).
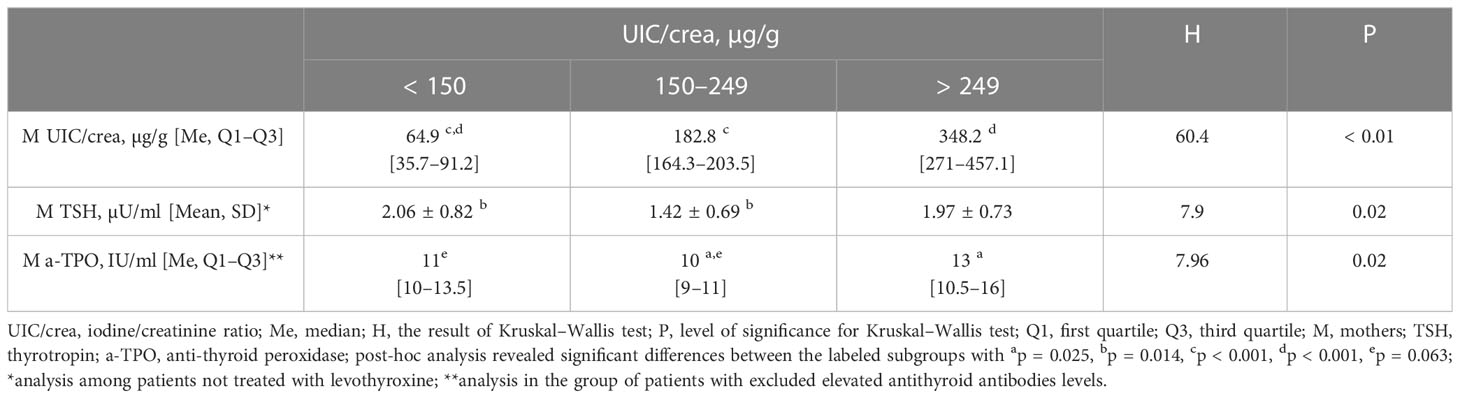
Table 4 The impact of maternal ioduria (according to the WHO criteria) on thyroid parameters.
Additionally, TSHs was above 5 mIU/liter in 6% of newborns. All newborns showed TSH < 12 mIU/liter (one had > 10 mIU/liter); thus, none of the children required further investigation for congenital HT.
4 Discussion
Our study aimed to characterize the iodine status of pregnant women in the leading obstetric center in western Poland, as well as to analyze whether supplementation involving regular nutritional supplement preparations was effective in correcting iodine deficiency. The data indicate that the presented group of pregnant women residing in the area of western Poland is iodine deficient, despite the fact that the entire country is considered to be optimally iodine-supplied at the population level. Approximately one-third of pregnant women denied supplementing iodine in the course of pregnancy, and many supplemented the microelement inappropriately with regard to the onset and duration of the supplementation, disregarding both Polish and international guidelines.
Despite the differences in UIC among the supplemented and non-supplemented subgroups of women found in the literature, no study has shown sufficient iodine concentrations in pregnant Polish women with regard to the UIC reference ranges established by the WHO (see Table 5), with the exception of the data provided in one interventional study by Jastrzębska et al. (22). In the presented study, the supplemented group did not show a significantly higher UIC, although the subjects declared taking a proper iodine dose. The abovementioned notion is in line with the observation that the supplementation rate was one of the highest in comparison with the previous Polish reports, yet it still did not significantly affect the overall ioduria. This may be attributed to inappropriate formulas used by the patients, whereby in our study only one participant received KI in the form of the prescription drug, and the rest used a multi-nutrient over-the-counter pregnancy dietary supplements. In addition, iodine supplementation was frequently initiated too late or discontinued too early (21% of subjects in our cohort received iodine only through a short period). This unfortunate inconsequence of supplementation, was already observed in the previous analyses (23). The only report where borderline sufficient ioduria was achieved, was an interventional study involving the administration of 150 μg of KI per day in a separate tablet (22). In terms of dietary supplements, KI is the most recommended form, whereas Kelp should be avoided, due to high-dose variation (24). Interestingly, the U.S. market analysis revealed that 24% of prenatal multivitamin supplements did not contain iodine at all, and in those containing iodine, the doses varied considerably (25–290 μg), with still others contained Kelp (25).
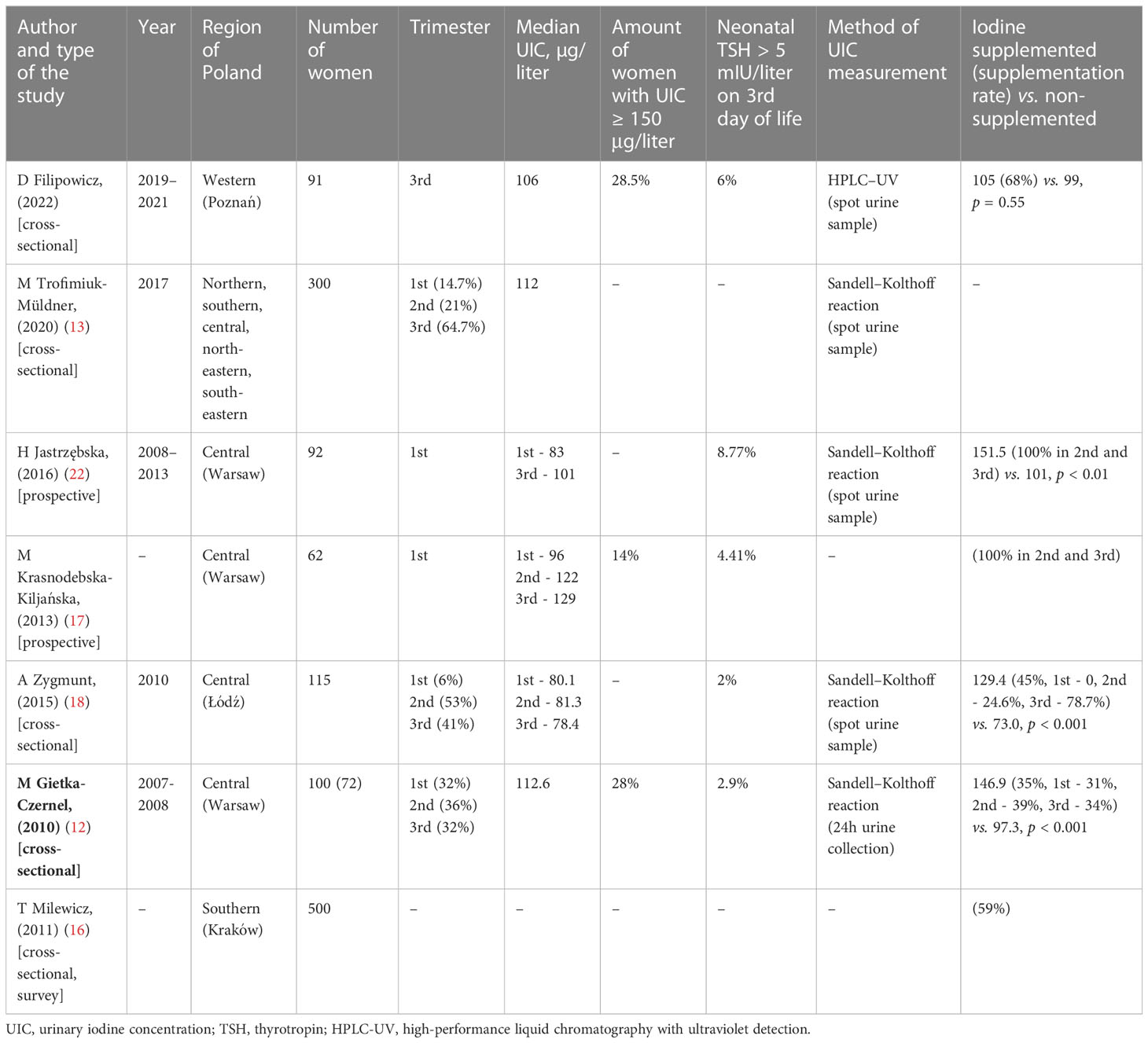
Table 5 A comparison of the Polish studies with regard to pregnancy ioduria in the past 14 years.
Furthermore, the study group had already been evaluated with regard to the selenium intake, where the authors found both poor selenium status and a similar ineffectiveness of self-administered micronutrient supplementation (26). A similar observation was made in Latvia where, despite a wide supplement usage (70%), pregnant women failed to achieve optimal selenium and iodine status. However, the baseline concentrations of both trace elements were higher than in Poland (26). Therefore, local guidelines concerning microelement and vitamin supplementation are necessary to provide the evidence-based medicine background for physicians and self-reported users, with particular emphasis on the most beneficial groups, such as pregnant women and autoimmune thyroiditis patients (27, 28). In other European countries, where salt iodization had been introduced, the optimal ioduria was achieved in school-aged children, although not in pregnant women (29, 30). Similar results were obtained in Portuguese pregnant women in the 1st trimester, where median UIC was 104 μg/liter, 19% had UIC < 50 μg/liter, and the supplementation rate was 57%, despite a decade long official recommendations regarding iodine supplementation during pregnancy, thus, showing poor adherence to the guidelines (31). The low iodine status was associated with poorer knowledge in terms of iodine significance and its sources (32). This may also potentially account for the results obtained in the presented study.
Notably, our cohort included also hypothyroid patients, some of whom were treated with LT4, which releases 64% of iodine itself. Possibly, the local population, or individuals with a disturbed thyroid function, experienced excessive local tissue iodine deficits in the thyroid gland, or the need for this micronutrient is too great to be effectively supplemented with the recommended dose. Nevertheless, in our further calculations, we excluded the hypothyroid patients with abnormal TSH, based on the population-adjusted referenced values, established by the Polish Society of Endocrinology for the 3rd trimester of pregnancy (TSH 0.11–3.53). Additionally, bearing in mind the effect of iodine supplementation on thyroid function, in calculations comprising thyroid parameters, only women not receiving LT4 therapy were included, and accounted for the presence or absence of AIT.
Only women in the 3rd trimester of pregnancy were enrolled in this study (at one time point—a few days before the delivery, following hospital admission) in order to avoid inconsistency due to changes in UIC during pregnancy, where increased urine volume may lead to a decrease in iodine concentration in comparison with the 1st trimester (33). This may account for the lower value of UIC in this study in comparison with research including also the 1st and 2nd trimesters of pregnancy. Nevertheless, it should be emphasized that the second half of the 1st trimester is the most crucial time for the newborn’s maternal iodine intake, as the placenta is the only source of supplying a sufficient amount of T3 for the development of the fetal central nervous system until midgestation (2).
Conversely, elevated population ioduria may be harmful when median UIC exceeds 500 µg/liter, or the daily intake increases above 500 µg (twofolds higher than recommended). Elevated iodine may serve as an endocrine disruptor, causing oxidative damage to lipid membranes, disturbing thyroid hormones metabolism, or enhancing autoimmune processes, particularly in vulnerable individuals with preexisting iodine deficiencies (34). It is vital to note that, according to one report, iodine and selenium content in multivitamin supplements exceeds the amount stated on the label by the manufacturer, by up to 25% (35). Therefore, it is essential to avoid overdosing, or ingesting unknown microelements dosages, as well as poorly characterized supplement mixtures.
According to the WHO, iodine sufficiency at pregnancy, expressed by ioduria, can be estimated only on the population level (due to the significant intra- and interindividual differences). It reflects the total iodine consumption within the past few days. The median UIC values between 150 and 249 µg/liter are considered an optimal supply. As iodine is excreted in > 90% by kidneys, UIC in a spot urine sample is a biomarker of iodine status during gestation in epidemiological studies, recommended by the WHO (36). Nonetheless, in the course of pregnancy, physiological increase in renal filtration and urine iodine dilution may result in underestimating iodine concentration level. Moreover, hydration status and day-to-day iodine concentration differences may also impact the results. Hence, a reasonable additional indicator seems to be UIC/crea ratio, which reduces the impact of changes in urine volume. In pregnant women, this biomarker correlates with 24h urine iodine collection, and is consistent with serum concentration during pregnancy (33). Bearing in mind the aforementioned, in this study, both biomarkers were assessed. Additionally, for the purpose of the presented study, a new inexpensive and selective ion-pair HPLC-UV technique for iodine assessment in human urine was developed and validated. In comparison with the former method, inductively coupled plasma mass spectrometry (ICP–MS), HPLC-UV is less complicated and does not require any advanced equipment. Compared with the spectrophotometric method, using the Sandell–Kolthoff reaction (S–K), HPLC-UV does not involve the ingestion of the initial material, or the use of noxious substances (arsenic and cerium) (19, 37). Moreover, HPLC-UV provides better selectivity of the analytes to be determined in such a complex biological matrix as urine.
The impact of iodine intake on the thyroid may be reflected by the lowest TSH and a-TPO of mothers in the subgroup where ioduria was within the recommended ranges. Analogously, the Chinese cohort of more than a thousand pregnant women revealed lower TSH in the group with UIC 150–249 μg/liter, than in those with UIC 250 μg/liter or above, and estimated the 2.5 higher risk for developing subclinical HT in late pregnancy for women with UIC lower than 100 μg/liter in the 1st trimester (38). Two randomized controlled trials demonstrated a lower increase in TSH throughout pregnancy when supplemented with 200–225 µg iodine/day and in one study, and a lower maternal TSH was found at the 1st trimester in the supplemented group (39, 40). Additionally, in our study, a weak-positive correlation was observed between maternal UIC and neonatal TSH from the cord blood. However, according to meta-analyses, in the majority of studies, iodine supplementation itself did not impact maternal TSH, ft4, a-TPO and neonatal TSH (41). Low UIC (< 100 μg/liter) was found as an independent risk factor for positive a-Tg among iodine-sufficient population (42). Our research indicated that the lowest a-TPO was seen in the subgroup with the optimal ioduria. In terms of the reluctance to supplement iodine in pregnant women suffering from AIT, due to the fact that excessive iodine is considered a trigger of antithyroid autoimmunity, no significant increase in a-TPO was found after administrating a dose of 100 or 150 μg daily (43), and the prevalence of a-TPO positivity among Iranian pregnant women did not increase 2 years following introduction of a national iodine supplementation (44). Notably, in our study, a positive correlation was found between all maternal and newborns’ thyroid autoantibodies, which proved maternofetal transplacental transfer of IgG antibodies, since a neonate is unable to produce antibodies during the first months of life. Moreover, higher maternal TRAb concentration was related to a lower fetal ft4 level, which may be attributed to the presence of TSH receptor blocking autoantibodies fraction, detected by TRAb assessment, which reduce fetal thyroid hormones production.
Neonatal TSHs evaluated in a dried whole blood sample (heel prick) 3 to 4 days after birth may serve as a sensitive indicator of population iodine deficiency. The latter is recognized when TSH is above 5 mlU/liter in more than 3% of neonates, as presented in this study (20, 45). Newborns poorly supplied in iodine showed an elevated thyroidal iodine turnover. As a consequence, TSH increases in the first weeks of life, causing neonatal transient hyperthyrotropinemia. This condition resolves spontaneously after 2 weeks and should be distinguished from the physiological TSH elevation in the first 36h of life due to perinatal stress. Nevertheless, neonatal transient hyperthyrotropinemia increases the risk of developing persistent hyperthyrotropinemia in childhood (46). In the presented study, TSH elevation in the first minutes of life was verified after 3 days, and achieved physiological concentrations in all newborns, showing no correlations with former TSH results. Therefore, it should be emphasized that only a delayed TSH assessment should be taken into account.
The American Thyroid Association guidelines recommend supplementation of 150-µg iodine daily during pregnancy and lactation, although the optimal ioduria was demonstrated in this geographical area (47). In contrast to the Polish guidelines in hypothyroid women treated with LT4, they discourage additional supplementation of iodine. In the present study, among patients treated with LT4, supplementing only iodine or receiving both LT4 and iodine, no significant difference was found. However, it is worth bearing in mind that the addition of iodine to LT4 in hypothyroid patients may improve the iodine status to a greater extent than iodine or LT4 alone, which would favor local recommendations (see Table 6). This is supported by another Polish study, where optimal UIC was achieved after the addition of 150 μg of KI to the standard LT4 dose (22). Nevertheless, more studies are necessary to prove the currently observed tendency.
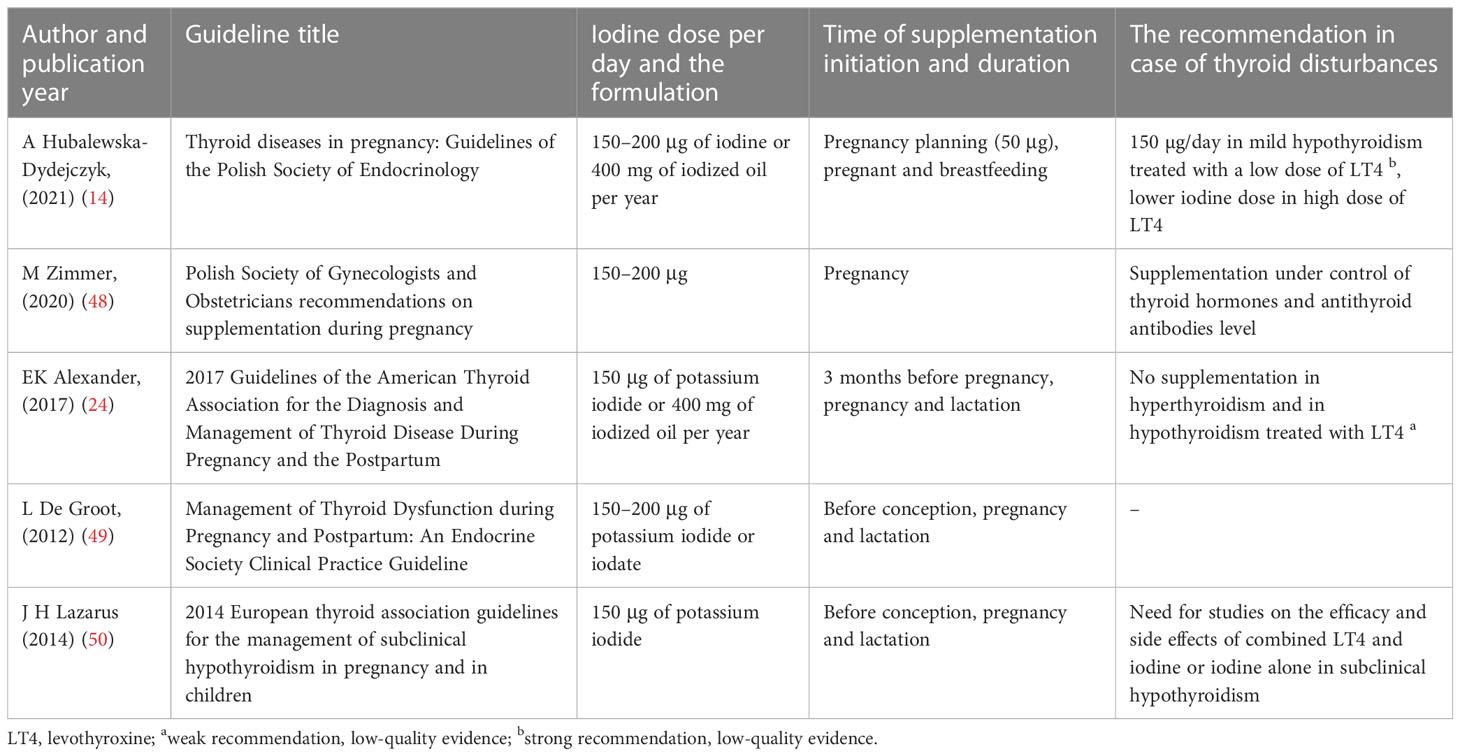
Table 6 Summary of the recommendations for iodine supplementation in pre-conception, pregnancy and the lactation period.
The conducted study also has a few limitations. Median ioduria was assessed in the heterogenous group in terms of the thyroid status (including euthyroid, hypothyroid women, with and without AIT, patients receiving LT4). The data concerning supplement intake were interview-based; thus, it is impossible to exclude the bias of underreporting. Additionally, no detailed daily food questionnaire was performed; hence, the impact of individual diets, possibly rich in iodine, was also not addressed. However, any specific diet followers and individuals residing abroad for longer periods were excluded, and due to obligatory salt iodization, the population baseline iodine status was assumed to be nearly equal. Iodine was assessed only in the 3rd trimester of pregnancy, where the most complete iodine status would have been documented, with the assessments performed at least once per trimester, including the most crucial for the neonatal development—the 1st trimester.
In most countries, universal salt iodization programs are ineffective in restoring adequate maternal ioduria with regard to the ranges established by the WHO. Despite the recommendation to additionally supplement iodine during pregnancy, the real-life assessment of this trace element supplementation revealed the ineffectiveness of the current model. An interventional study would presumably need to be conducted in order to verify the effectiveness of the dose and avoid a possible bias due to self-reporting supplementation, irregularity in the supplement intake (particularly in the end of pregnancy), HT, or LT4 impact, as well as diversity of the preparations declared. Physicians should consider prescribing KI as a medication (verified composition), and it should possibly come as a separate formulation. It is essential to increase the awareness of endocrinologists, gynecologists, general practitioners, and the society, especially pregnant women, regarding the significance and the benefits of a proper iodine supplementation during pregnancy for mothers and their newborns to restore appropriate levels of this element.
In conclusion, despite the relevant guidelines, the analyzed group of pregnant women from the western Poland demonstrated an insufficient iodine status, which may present potential negative implications for pregnancy and child development. Considering that this issue is preventable, additional measures are essential in order to provide a more comprehensive information to attending physicians and medical caregivers, as well as to the general public, including young women, and to improve the iodine intake in pregnancy to the level which safely allows to avoid iodine deficiency.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by The Local Bioethics Committee of Poznan University of Medical Sciences (protocol no. 104/19, date of approval: 10 January 2019, annexed 4 February 2021, protocol no. 132/21). The patients/participants provided their written informed consent to participate in this study.
Author contributions
Conceptualization, MR, DF, ES-P. Methodology, DF, FG, MK-Ł, AM-S, KS. Statistical analysis, DF. Investigation, DF, MR, ES-P. Data collection, DF, KS, MO. Writing - original draft preparation, DF. Writing - review and editing, MR, ES-P, LS, KS, FG, MK-Ł, AM-S, MO. Supervision, MR, ES-P. Funding acquisition, DF, MR. All authors contributed to the article and approved the submitted version.
Funding
The research was funded by National Science Centre in Poland (grant number 2019/33/N/NZ5/02303) - a PRELUDIUM-17 grant.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zimmermann MB. The importance of adequate iodine during pregnancy and infancy. World Rev Nutr Diet (2016) 115:118–24. doi: 10.1159/000442078
2. Puig-Domingo M, Vila L. The implications of iodine and its supplementation during pregnancy in fetal brain development. Curr Clin Pharmacol (2013) 8(2):97–109. doi: 10.2174/1574884711308020002
3. Chen X, Wu C, Wang Z, Wu C, Guo Y, Zhu X, et al. Iodine nutrition status and thyroid autoimmunity during pregnancy: a cross-sectional study of 4635 pregnant women. Nutr J (2022) 21(1):7. doi: 10.1186/s12937-022-00760-6
5. Levie D, Korevaar TIM, Bath SC, Murcia M, Dineva M, Llop S, et al. Association of maternal iodine status with child IQ: a meta-analysis of individual participant data. J Clin Endocrinol Metab (2019) 104(12):5957–67. doi: 10.1210/jc.2018-02559
6. Bath SC, Steer CD, Golding J, Emmett P, Rayman MP. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: results from the Avon longitudinal study of parents and children (ALSPAC). Lancet Lond Engl (2013) 382(9889):331–7. doi: 10.1016/S0140-6736(13)60436-5
7. World Health Organization. Iodine deficiency in Europe: a continuing public health problem. World Health Organization (Switzerland: WHO Press) (2007). Available at: https://apps.who.int/iris/handle/10665/43398.
8. Szybiński Z. Work of the polish council for control of iodine deficiency disorders, and the model of iodine prophylaxis in Poland. Endokrynol Pol (2012) 63(2):156–60.
9. Szybinski Z, Delange F, Lewinski A, Podoba J, Rybakowa M, Wasik R, et al. A programme of iodine supplementation using only iodised household salt is efficient - the case of Poland. Eur J Endocrinol (2001) 144(4):331–7. doi: 10.1530/eje.0.1440331
10. Tykarski A, Narkiewicz K, Gaciong Z, Januszewicz A, Litwin M, Kostka-Jeziorny K, et al. 2015 Guidelines for the management of hypertension. recommendations of the polish society of hypertension - short version. Kardiol Pol (2015) 73(8):676–700. doi: 10.5603/KP.2015.0157
11. Lewiński A, Zygmunt A. Iodine prophylaxis in Poland - new, old challenges. Ann Agric Environ Med (2014) 21(1):1–4.
12. Gietka-Czernel M, Dębska M, Kretowicz P, Jastrzębska H, Kondracka A, Snochowska H, et al. Iodine status of pregnant women from central Poland ten years after introduction of iodine prophylaxis programme. Endokrynol Pol (2010) 61(6):646–51.
13. Trofimiuk-Müldner M, Konopka J, Sokołowski G, Dubiel A, Kieć-Klimczak M, Kluczyński Ł, et al. Current iodine nutrition status in Poland (2017): is the polish model of obligatory iodine prophylaxis able to eliminate iodine deficiency in the population? Public Health Nutr (2020) 23(14):2467–77. doi: 10.1017/S1368980020000403
14. Hubalewska-Dydejczyk A, Trofimiuk-Müldner M, Ruchala M, Lewiński A, Bednarczuk T, Zgliczyński W, et al. Thyroid diseases in pregnancy: guidelines of the polish society of endocrinology. Endokrynol Pol (2021) 72(5):425–88. doi: 10.5603/EP.a2021.0089
15. WHO Secretariat, Andersson M, de Benoist B, Delange F, Zupan J. Prevention and control of iodine deficiency in pregnant and lactating women and in children less than 2-years-old: conclusions and recommendations of the technical consultation. Public Health Nutr (2007) 10(12A):1606–11. doi: 10.1017/S1368980007361004
16. Milewicz T, Czyżewicz M, Stochmal E, Galicka-Latała D, Hubalewska-Dydejczyk A, Krzysiek J. Intake of iodine-containing multivitamin preparations by pregnant women from the Krakow region of Poland. Endokrynol Pol (2011) 62(4):309–15.
17. Krasnodebska-Kiljańska M, Kondracka A, Bartoszewicz Z, Niedźwiedzka B, Ołtarzewski M, Grzesiuk W, et al. Iodine supply and thyroid function in the group of healthy pregnant women living in Warsaw. Pol Merkur Lek Organ Pol Tow Lek (2013) 34(202):200–4.
18. Zygmunt A, Adamczewski Z, Zygmunt A, Adamczewska K, Trofimiuk-Muldner M, Hubalewska-Dydejczyk A, et al. An assessment of the effectiveness of iodine prophylaxis in pregnant women - analysis in one of reference gynaecological-obstetric centres in Poland. Endokrynol Pol (2015) 66(5):404–11. doi: 10.5603/EP.2015.0050
19. Mikulska AA, Filipowicz D, Główka FK, Szczepanek-Parulska E, Ruchała M, Bartecki M, et al. HPLC analysis of the urinary iodine concentration in pregnant women. Molecules (2021) 26(22):6797. doi: 10.3390/molecules26226797
20. World Health Organization. Assessment of iodine deficiency disorders and monitoring their elimination: a guide for programme managers, 3rd Edn. Switzerland: WHO Press (2007). Available at: https://apps.who.int/iris/handle/10665/43781.
21. Sawicka-Gutaj N, Gruszczyński D, Guzik P, Mostowska A, Walkowiak J. Publication ethics of human studies in the light of the declaration of Helsinki – a mini-review. J Med Sci (2022) 91(2):e700. doi: 10.20883/medical.e700
22. Jastrzębska H, Kochman M, Bartoszewicz Z, Ołtarzewski M, Dębski R, Zgliczyńskiz W. Iodine supplementation during pregnancy of hypothyroid women treated with l-thyroxine neither influences neonatal TSH nor prevents decrease in maternal free thyroid hormone concentrations in second and third trimesters. Endokrynol Pol (2016) 67(4):367–74. doi: 10.5603/EP.a2016.0049
23. Zygmunt A, Lewinski A. Iodine prophylaxis in pregnant women in Poland - where we are? (update 2015). Thyroid Res (2015) 8:17. doi: 10.1186/s13044-015-0029-z
24. Alexander EK, Pearce EN, Brent GA, Brown RS, Chen H, Dosiou C, et al. 2017 Guidelines of the American thyroid association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid Off J Am Thyroid Assoc (2017) 27(3):315–89. doi: 10.1089/thy.2016.0457
25. Patel A, Lee SY, Stagnaro-Green A, MacKay D, Wong AW, Pearce EN. Iodine content of the best-selling united states adult and prenatal multivitamin preparations. Thyroid Off J Am Thyroid Assoc (2019) 29(1):124–7. doi: 10.1089/thy.2018.0386
26. Filipowicz D, Szczepanek-Parulska E, Kłobus M, Szymanowski K, Chillo TS, Asaad S, et al. Selenium status and supplementation effects in pregnancy-a study on mother-child pairs from a single-center cohort. Nutrients (2022) 14(15):3082. doi: 10.3390/nu14153082
27. Mikulska AA, Karaźniewicz-Łada M, Filipowicz D, Ruchała M, Główka FK. Metabolic characteristics of hashimoto’s thyroiditis patients and the role of microelements and diet in the disease management-an overview. Int J Mol Sci (2022) 23(12):6580. doi: 10.3390/ijms23126580
28. Filipowicz D, Majewska K, Kalantarova A, Szczepanek-Parulska E, Ruchała M. The rationale for selenium supplementation in patients with autoimmune thyroiditis, according to the current state of knowledge. Endokrynol Pol (2021) 72(2):153–62. doi: 10.5603/EP.a2021.0017
29. Manousou S, Andersson M, Eggertsen R, Hunziker S, Hulthén L, Nyström HF. Iodine deficiency in pregnant women in Sweden: a national cross-sectional study. Eur J Nutr (2020) 59(6):2535–45. doi: 10.1007/s00394-019-02102-5
30. Andersson M, Hunziker S, Fingerhut R, Zimmerman MB, Herter-Aeberli I. Effectiveness of increased salt iodine concentration on iodine status: trend analysis of cross-sectional national studies in Switzerland. Eur J Nutr (2020) 59(2):581–93. doi: 10.1007/s00394-019-01927-4
31. Matta Coelho C, Guimarães J, Bracchi I, Xavier Moreira N, Pinheiro C, Ferreira P, et al. Noncompliance to iodine supplementation recommendation is a risk factor for iodine insufficiency in Portuguese pregnant women: results from the IoMum cohort. J Endocrinol Invest (2022) 45(10):1865–74. doi: 10.1007/s40618-022-01813-7
32. Pinheiro C, Xavier Moreira N, Ferreira P, Matta Coelho C, Guimarães J, Pereira G, et al. Iodine knowledge is associated with iodine status in Portuguese pregnant women: results from the IoMum cohort study. Br J Nutr (2021) 126(9):1331–9. doi: 10.1017/S0007114521000155
33. Li C, Peng S, Zhang X, Xie X, Wang D, Mao J, et al. The urine iodine to creatinine as an optimal index of iodine during pregnancy in an iodine adequate area in China. J Clin Endocrinol Metab (2016) 101(3):1290–8. doi: 10.1210/jc.2015-3519
34. Karbownik-Lewińska M, Stępniak J, Iwan P, Lewiński A. Iodine as a potential endocrine disruptor-a role of oxidative stress. Endocrine (2022) 78(2):219–40. doi: 10.1007/s12020-022-03107-7
35. Andrews KW, Roseland JM, Gusev PA, Palachuvattil J, Dang PT, Savarala S, et al. Analytical ingredient content and variability of adult multivitamin/mineral products: national estimates for the dietary supplement ingredient database. Am J Clin Nutr (2017) 105(2):526–39. doi: 10.3945/ajcn.116.134544
36. Wainwright P, Cook P. The assessment of iodine status - populations, individuals and limitations. Ann Clin Biochem (2019) 56(1):7–14. doi: 10.1177/0004563218774816
37. Cui L, Wen J, Zhou T, Wang S, Fan G. Optimization and validation of an ion-pair RP-HPLC-UV method for the determination of total free iodine in rabbit plasma: application to a pharmacokinetic study. BioMed Chromatogr BMC (2009) 23(11):1151–9. doi: 10.1002/bmc.1237
38. Wang T, Liu Y, Kong Q, Cao X, Liu Y, Xia S, et al. Effect of moderate-to-Severe iodine deficiency in early pregnancy on subclinical hypothyroidism: a longitudinal study in an iodine-sufficient region in China. Front Nutr (2022) 9:839651. doi: 10.3389/fnut.2022.839651
39. Gowachirapant S, Jaiswal N, Melse-Boonstra A, Galetti V, Stincaa S, Mackenzie I, et al. Effect of iodine supplementation in pregnant women on child neurodevelopment: a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol (2017) 5(11):853–63. doi: 10.1016/S2213-8587(17)30332-7
40. Censi S, Watutantrige-Fernando S, Groccia G, Manso J, Plebani M, Faggian D, et al. The effects of iodine supplementation in pregnancy on iodine status, thyroglobulin levels and thyroid function parameters: results from a randomized controlled clinical trial in a mild-to-Moderate iodine deficiency area. Nutrients (2019) 11(11):E2639. doi: 10.3390/nu11112639
41. Dineva M, Fishpool H, Rayman MP, Mendis J, Bath SC. Systematic review and meta-analysis of the effects of iodine supplementation on thyroid function and child neurodevelopment in mildly-to-moderately iodine-deficient pregnant women. Am J Clin Nutr (2020) 112(2):389–412. doi: 10.1093/ajcn/nqaa071
42. Chen X, Chen L, Lian X, Liu X, Shan Z, Shi B, et al. URINARY IODINE CONCENTRATION IS INVERSELY ASSOCIATED WITH THYROGLOBULIN ANTIBODIES. Endocr Pract (2019) 25(5):454–60. doi: 10.4158/EP-2018-0252
43. van Heek L, Staudacher C, Faust M, Chiapponi C, Mettler J, Schmidt M, et al. Avoidance of iodine deficiency/excess during pregnancy in hashimoto’s thyroiditis. Nukl Nucl Med (2021) 60(4):266–71. doi: 10.1055/a-1400-3522
44. Delshad H, Raeisi A, Abdollahi Z, Tohidi M, Hedayati M, Mirmiran P, et al. Iodine supplementation for pregnant women: a cross-sectional national interventional study. J Endocrinol Invest (2021) 44(10):2307–14. doi: 10.1007/s40618-021-01538-z
45. Zimmermann MB, Aeberli I, Torresani T, Bürgi H. Increasing the iodine concentration in the Swiss iodized salt program markedly improved iodine status in pregnant women and children: a 5-y prospective national study. Am J Clin Nutr (2005) 82(2):388–92. doi: 10.1093/ajcn.82.2.388
46. Cuestas E, Gaido MI, Capra RH. Transient neonatal hyperthyrotropinemia is a risk factor for developing persistent hyperthyrotropinemia in childhood with repercussion on developmental status. Eur J Endocrinol (2015) 172(4):483–90. doi: 10.1530/EJE-13-0907
47. Sullivan KM. Iodine supplementation for pregnancy and lactation: united states and Canada: recommendations of the American thyroid association. Thyroid Off J Am Thyroid Assoc (2007) 17(5):483–4. doi: 10.1089/thy.2007.0073
48. Zimmer M, Sieroszewski P, Oszukowski P, Huras H, Fuchs T, Pawlosek A, et al. Polish society of gynecologists and obstetricians recommendations on supplementation during pregnancy. Ginekol Pol (2020) 91(10):644–53. doi: 10.5603/GP.2020.0159
49. De Groot L, Abalovich M, Alexander EK, Amino N, Barbou L, Cobin RH, et al. Management of thyroid dysfunction during pregnancy and postpartum: an endocrine society clinical practice guideline. J Clin Endocrinol Metab (2012) 97(8):2543–65. doi: 10.1210/jc.2011-2803
Keywords: urinary iodine concentration (UIC), micronutrients at pregnancy, iodine, selenium, hypothyroidism, thyroiditis, neonatal cord blood, pregnancy supplementation guidelines
Citation: Filipowicz D, Szczepanek-Parulska E, Mikulska-Sauermann AA, Karaźniewicz-Łada M, Główka FK, Szymanowski K, Ołtarzewski M, Schomburg L and Ruchała M (2023) Iodine deficiency and real-life supplementation ineffectiveness in Polish pregnant women and its impact on thyroid metabolism. Front. Endocrinol. 14:1068418. doi: 10.3389/fendo.2023.1068418
Received: 12 October 2022; Accepted: 23 May 2023;
Published: 16 June 2023.
Edited by:
Jie Yan, Peking University, ChinaReviewed by:
Malgorzata Trofimiuk-Muldner, Jagiellonian University Medical College, PolandCharles Bitamazire Businge, Walter Sisulu University, South Africa
Copyright © 2023 Filipowicz, Szczepanek-Parulska, Mikulska-Sauermann, Karaźniewicz-Łada, Główka, Szymanowski, Ołtarzewski, Schomburg and Ruchała. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dorota Filipowicz, ZG9yb3RhLmZpbGlwb3dpY3oxMjNAZ21haWwuY29t