
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 09 March 2023
Sec. Thyroid Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1058695
 Chun-Jui Huang1,2,3
Chun-Jui Huang1,2,3 Lin-Hsuan Lee1,4Cheng-Pin Cheng1Shan-Fan Yao5
Lin-Hsuan Lee1,4Cheng-Pin Cheng1Shan-Fan Yao5 Harn-Shen Chen1,2
Harn-Shen Chen1,2 Chii-Min Hwu1,2Kam-Tsun Tang1,2Fan-Fen Wang1,6Chiao-Wei Shih1Chen-Chang Yang2,3,7,8*†Wen-Sheng Huang5,9*†
Chii-Min Hwu1,2Kam-Tsun Tang1,2Fan-Fen Wang1,6Chiao-Wei Shih1Chen-Chang Yang2,3,7,8*†Wen-Sheng Huang5,9*†Background: Soy sauce is widely used in a variety of Asian dishes to enhance flavor. Soybean and most soybean products, including soy sauces, are listed as prohibited foods in a low iodine diet. However, the iodine content in soy sauces is largely unknown. The aim of this study was to determine the iodine content in domestic soy sauces in Taiwan.
Methods: Twenty-five different kinds of soy sauces were diluted with distilled water and with a dilution factor of fifty or above. Iodine concentrations of the diluted samples were measured colourimetrically based on the Sandell-Kolthoff reaction by a modified microplate method. All the measurements were repeated twelve times on three different days for determination of mean and standard deviation (SD), and coefficients of variance (CV). Serial dilution and recovery tests were also performed for validation. The results were confirmed by an inductively coupled plasma mass spectrometry (ICP-MS) method.
Results: Among the twenty-five surveyed soy sauces, most of them (n=22) were iodine-free (<16 ug/L, and thus un-detectable). The iodine concentrations (mean ± SD) of the three iodine-containing soy sauces were 2.7 ± 0.1, 5.1 ± 0.2, and 10.8 ± 0.6 mg/L, respectively. The inter-assay, intra-assay and total CVs were all <5.3% for the modified microplate method. The results obtained by ICP-MS were consistent with those of the modified microplate method. The recovery rates in the serial dilution test and recovery test ranged from 94.7% to 118.6%. Two of the three iodine-containing soy sauces were supplemented with kelp extract, while the other one without kelp extract had the highest amount of salt among the three iodine-containing soy sauces. Therefore, we postulate that iodized salt instead of kelp extract is the source of higher iodine content in that sauce.
Conclusion: The results suggest that most soy sauces are iodine-free and may be allowed during low iodine diets.
A low iodine diet (LID) has been suggested 2 weeks prior to radioiodine administration for patients with differentiated thyroid carcinoma after thyroidectomy to enhance radioiodine uptake in remnants or residual tumor to ensure effective ablation or treatment (1, 2). Available data indicate that the alcohol soluble component in soybeans inhibits thyroid absorption of iodine and thus interferes with radioiodine thyroid uptake, leading to reduced efficacy of radioiodine therapy (3). Soy sauces are made from soybeans and are not recommended during a LID (2, 4–6). Soybeans per se do not contain iodine, but soy sauces may contain iodine if iodized salts are added during the fermentation process or if food additives such as seaweeds or yeasts are added during processing to enhance the flavor of soy sauces (3, 7).
To carry out the LID appropriately, it is important to determine the iodine contents in local foods. With the same food type, the iodine content may vary greatly in different regions due to differences in soil conditions, animals’ diet and iodine contents of ingredients in processed foods (8). For instance, the milk iodine content is 343 μg/kg in the United States, 220 μg/kg in Israel and 160 μg/kg in Norway (9–11). Even within the same country, the milk iodine content also varies in different regions (12). A survey of food composition in Japan had determined iodine content in 8 types of soy sauces and found 4 of them containing iodine (10 μg/kg in 3 types and the other one was 7,500 μg/kg), while the other 4 were iodine-free (13). However, in a very detailed food database in the United States, iodine content (10 μg/kg) was detected in only one type of soy sauce (9). There are more than 20 types of soy sauces in Taiwan but none of them has been tested for iodine contents. Some regional databases for iodine contents in foods and dietary supplements were established, but this is not the case in Taiwan (9, 10, 14); this is confusing for patients because they cannot know whether soy sauces, an important condiment in Taiwan, can be consumed during a LID or not.
Measuring iodine contents in foods is more complex than determining urinary iodine concentrations (UIC). In Taiwan, measurements of UIC in iodine nutritional studies have been carried out by a modified microplate method based on the Sandell–Kolthoff (S-K) reaction during the past 10 years (15, 16). While highly accurate in measuring UIC, one of the drawbacks of the S-K method is its limitation in determining iodine content in complex matrixes such as breast milk and foods. Therefore, we recently validated an inductively coupled plasma mass spectrometry (ICP-MS) method using alkali dilution to measure UIC (17–19). Others have previously reported on ICP-MS method for the measurement of iodine in breast milk and foods (20–22). Whether iodine content in soy sauces could be determined by the S-K method or ICP-MS method needs to be clarified.
The aim of the study was to determine the iodine contents of Taiwanese marketing soy sauces and to compare the performance of the S-K reaction and the ICP-MS method.
A total of 25 soy sauces including some imported and exported brands were collected from supermarkets in Taiwan. The salt content of each brand of soy sauces was converted to the same units according to their labeling. Iodine concentrations were determined colourimetrically by a modified microplate method based on the Sandell-Kolthoff reaction (15, 16). Samples were also measured by an ICP-MS method as previously described (17–19).
The protocol of determining iodine content in soy sauces was similar to what had been previously used to measure UIC except for those needed to be diluted by distilled water to allow measurable light transmission of absorbance at the final step. In brief, the digestion step was performed by pipetting 23 μL of standard iodine solutions and sampling into a 96-well reaction plate (Applied Biosystems, Foster City, CA, USA), followed by addition of 46 μL of ammonium persulfate solution (freshly prepared, 1.35 mol/L; Sigma-Aldrich, St. Louis, MO, USA) to each well. The microplate was covered with a 96-well full plate cover, and the contents were digested in the GeneAmp® PCR System 9700 Fast Thermal Cycler (Applied Biosystems) with a program of 95°C for 30 min and 4°C for 5 min. After digestion, the microplate was centrifuged at 1000 rpm for 3 min. The S-K reaction step was then performed. From the resulting digests, 50 µL of aliquots were transferred to the corresponding wells of a 96-well reading plate (MicroWell®; Nalge Nunc International, Rochester, NY, USA), in which 100 μL of arsenious acid solution (0.05 mol/L; Sigma-Aldrich) had been preloaded. After mixing the solution by shaking the plate in the microplate reader (Tecan Infinite® F50; Tecan Group Ltd., Männedorf, Switzerland), 50 μL of ceric ammonium sulfate solution (0.019 mol/L; Wako Pure Chemical Industries Ltd, Osaka, Japan) was added into each well using a multichannel pipette as quickly as possible. The absorbance of the reaction mixture was read at 405 nm after incubating at room temperature (~25°C) for 30 min. The calibration curve was plotted for each plate by plotting the optical density values versus the concentration of standards. Sample concentrations were interpolated from the calibration curve (range: 0-400 ug/L). The detection limit is 1.6 ug/L. Quality control samples provided by the Ensuring the Quality of Urinary Iodine Procedures (EQUIP) program were tested in each run to verify the accuracy and the success of the digestion.
The tested samples were duplicated 12 times on 3 different days to determine the mean and standard deviation (SD), intra-assay, inter-assay and total coefficients of variance (CV). To validate the microplate method in determining iodine content in soy sauces, further experiments including the serial dilution and recovery tests were performed. The previously 100-fold or 50-fold diluted samples were further serially diluted (1, 0.8, 0.6, 0.4, and 0.2) to determine the recovery rate and linearity. The recovery test was performed twice on 2 different days and the soy sauces were measured twice to evaluate the iodine concentration before adding additional iodine. The potassium iodate solution was prepared by mixing 0.843 g of potassium iodate with water and diluting to solutions with iodine concentrations of 5 μg/L, 10 μg/L, and 15 μg/L (Table S1). One volume of each iodate solution (5 μg/L, 10 μg/L, or 15 μg/L) was added to 9 volumes of sample after being appropriately diluted 100-fold or 50-fold.
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) software, version 24.0 (IBM Corp., Armonk, NY, USA). Mann-Whitney U test was performed for comparison of salt content between the iodine-containing and iodine-free soy sauces. P <0.05 was served as statistically significant.
Samples with different dilution factors were measured by the S-K method to determine the most appropriate dilution factor to yield consistent results. While the samples were diluted with a dilution factor of 10 or less, some of the samples still appeared blackish and the absorbance was severely disturbed by the pigmentation. As diluted 50 times above the original samples, the light could be transmitted through the samples and the absorbance could be obtained accurately as shown in Figure 1.
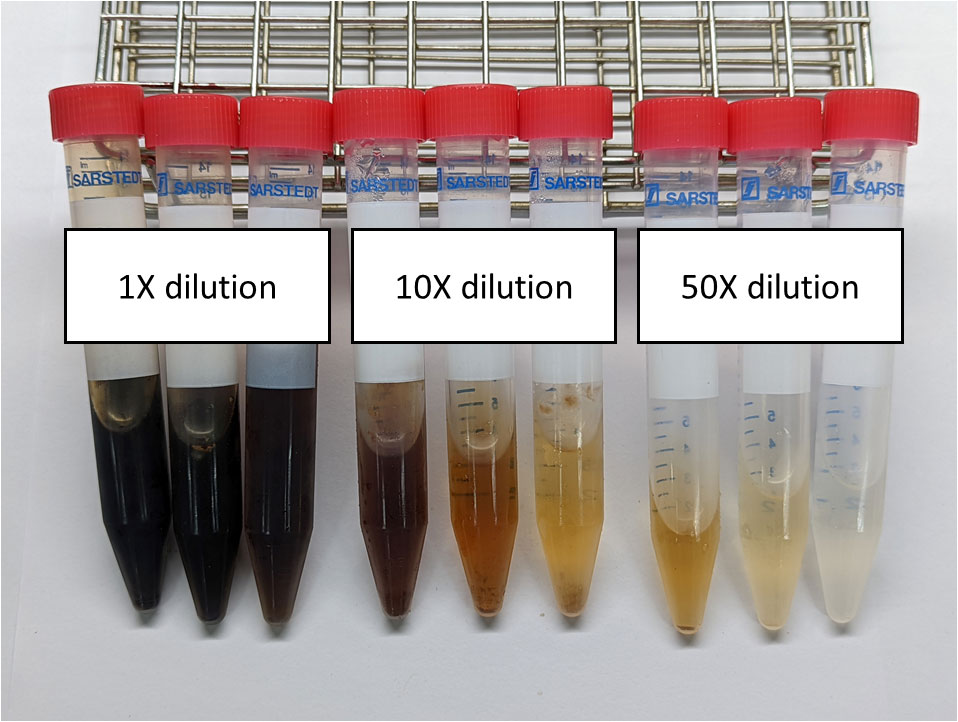
Figure 1 The appearance of the three iodine-containing soy sauces when diluted with different dilution factors.
The iodine contents in 25 different domestic soy sauces are summarized in Table 1. Only 3 of them contained iodine, while the other 22 were iodine-free. The lowest detectable iodine concentration in the soy sauces was 16 μg/L (Table S1). Of the 3 iodine-containing soy sauces, iodine concentrations were determined by a dilution factor of 100 or 50 and the results were 2.7 ± 0.1, 5.1 ± 0.2, and 10.8 ± 0.6 mg/L, respectively (Tables 2; S1). The inter-assay, intra-assay and total CVs were all <5.3%. The CVs using S-K and ICP-MS methods were 4.7%, 2.9%, and 2.7%, respectively. The mean recovery rate of the 3 iodine-containing soy sauces at serial dilution were 103.4%, 95.1%, and 99.1%, respectively (Table 3). The coefficients of linearity were >0.999, 0.987, and 0.996, respectively (Figure 2). The iodine recovery rates of the 3 iodate-added samples were 118.6%, 94.7% and 99.4%, respectively (Table 4).
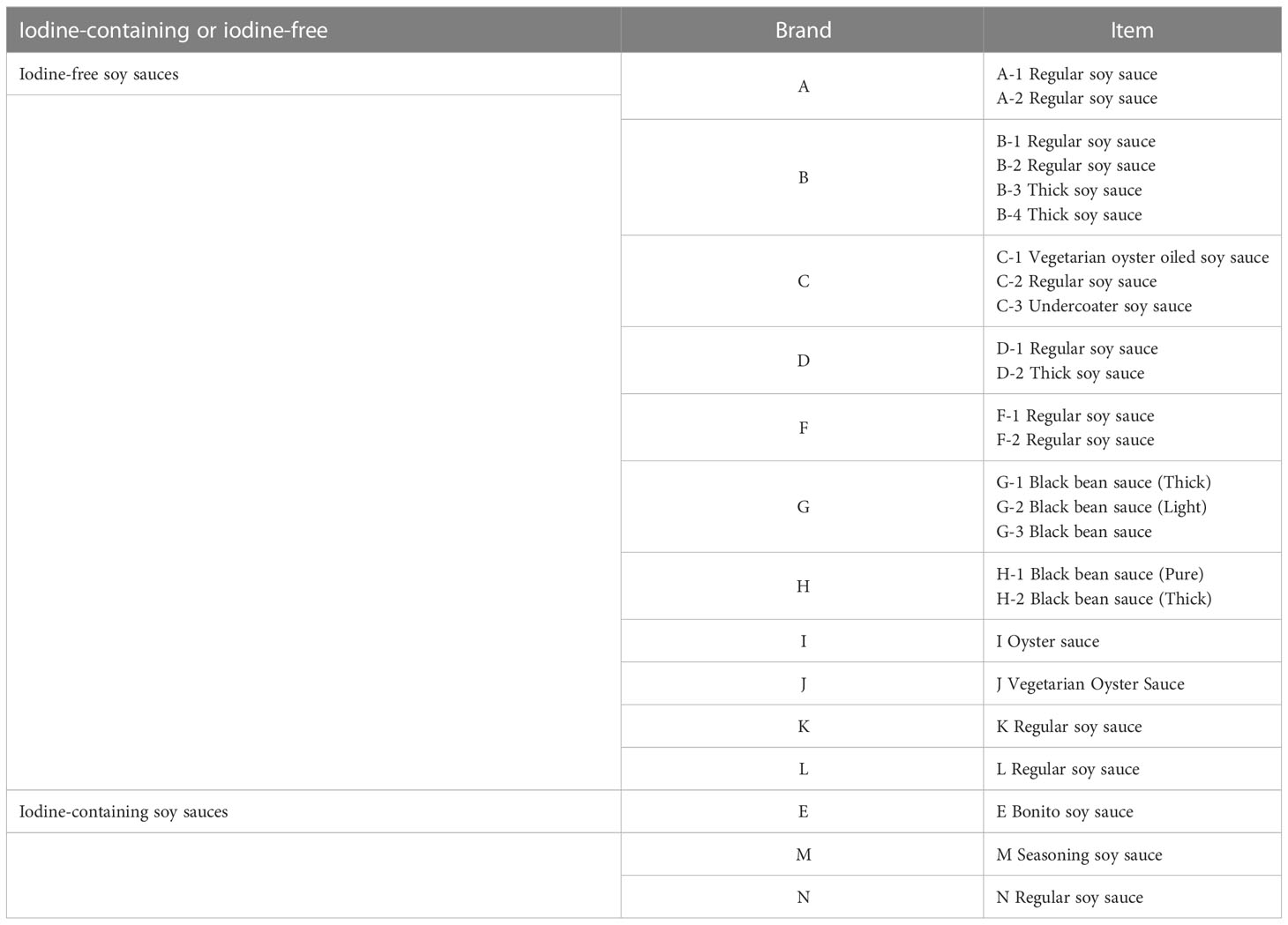
Table 1 Iodine-containing soy sauces and iodine-free soy sauces.
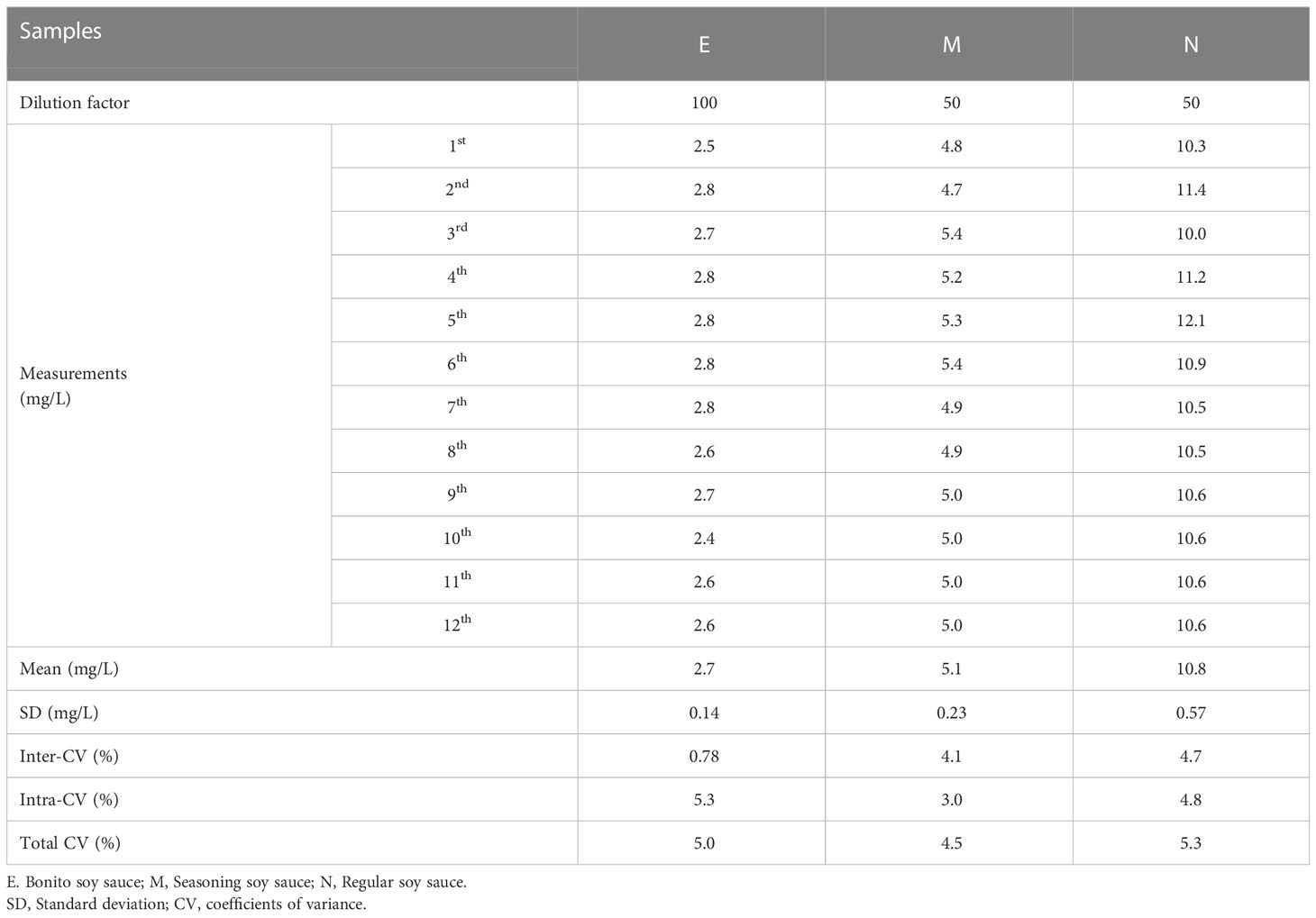
Table 2 Iodine concentration of the three iodine-containing soy sauces.
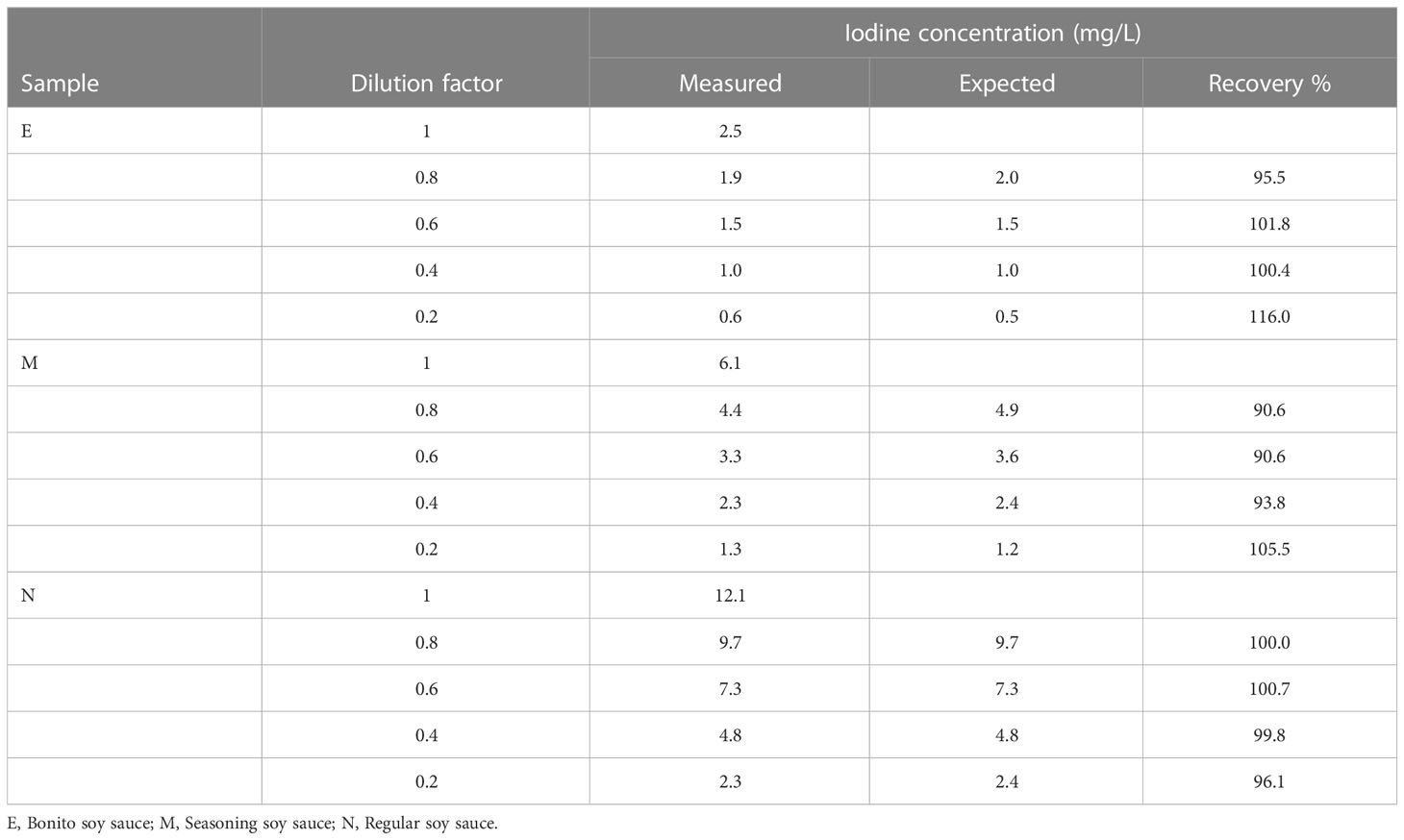
Table 3 Serial dilution of soy sauce samples within water.
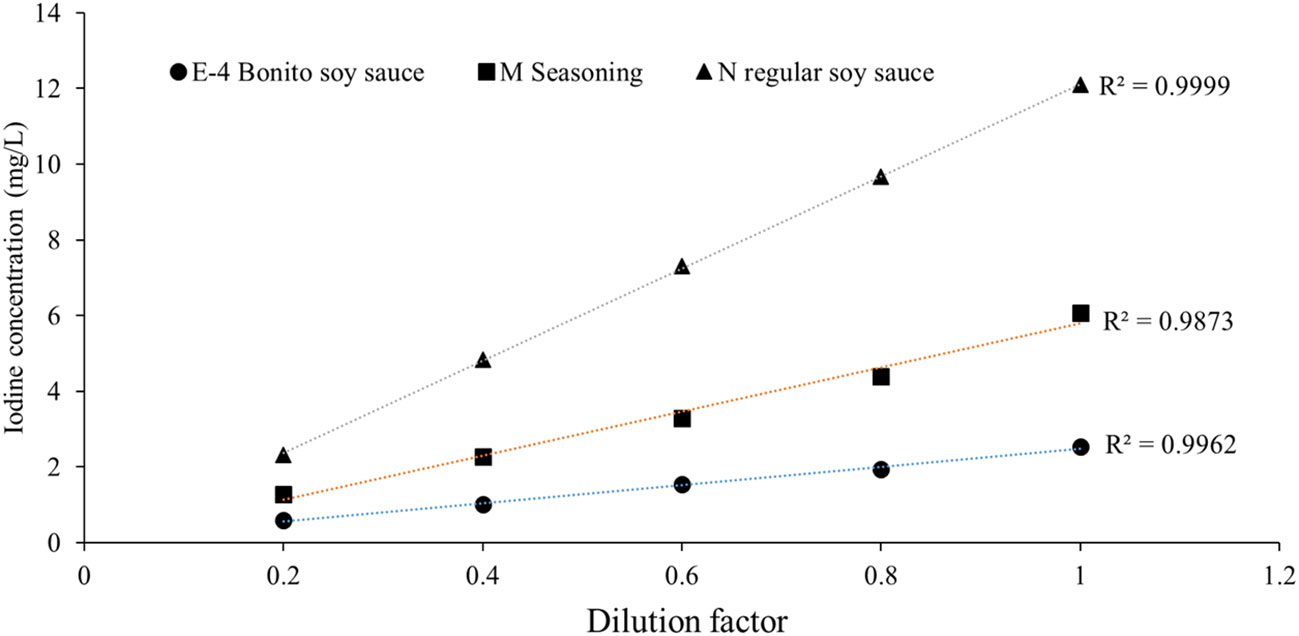
Figure 2 The linearity of iodine concentrations by serial dilution of three soy sauces.

Table 4 Recovery of iodine added to soy sauces.
Among the 3 iodine-containing soy sauces, 2 of them contained kelp extract. The salt (NaCl) contents of the 3 iodine-containing soy sauces were 5120, 9255, and 1340 mg per 100 mL, while the average salt content of the other iodine-free soy sauces was 4252 ± 1217.7 mg per 100 mL (Tables 5; S1).
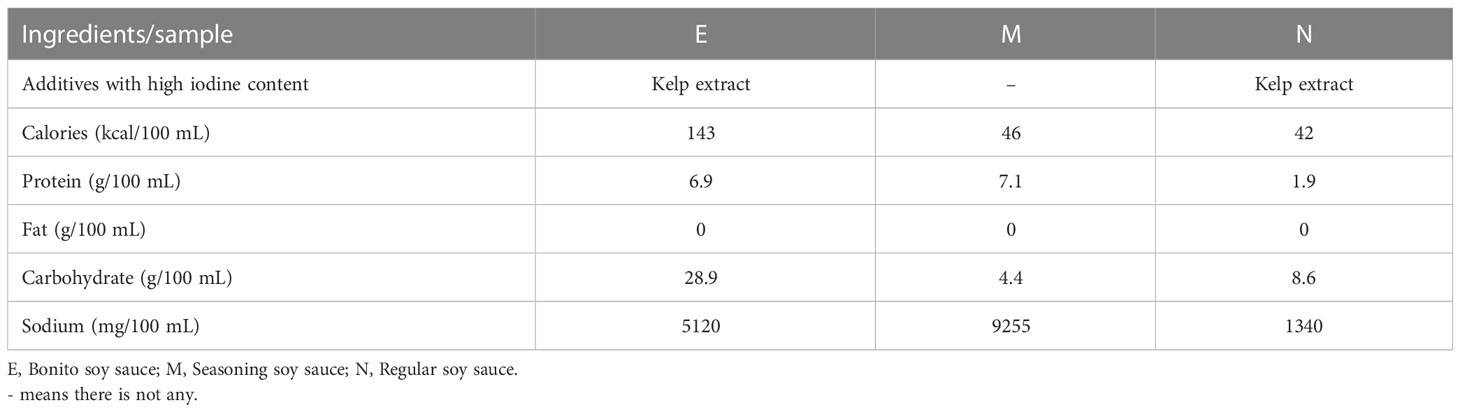
Table 5 Labeling of the three iodine-containing soy sauces.
The iodine content in soy sauces has not been reported thoroughly in the literature. The current observation, to our knowledge, appears to be the first study to comprehensively clarify the iodine contents in several soy sauces marketed in Taiwan. Information regarding iodine content in foods is very limited in Taiwan. As of yet, the iodine content has only been reported for the herbal cuisine soup (median iodine concentration 23.1 μg/L), post-partum teas (<10 μg/L), dairy products and milk-alternative drinks (mean iodine concentration of whole milk, low-fat milk, flavored milk and milk drinks, milk alternative drinks:210.4 μg/L, 263.2 μg/L, 100.0 μg/L, 65.6 μg/L, and <1 μg/L, respectively) (23, 24) (Table S1). This study provides additional data on iodine nutrition of local foods in Taiwan, which provides useful information for patients scheduled for a LID diet.
The current study shows that ingestion of 4~20 mL of the 3 iodine-containing soy sauces (iodine content 2.7, 5.1, and 10.8 mg/L, respectively) could exceed the LID recommended criteria, i.e., an iodine intake <50 µg/day (1, 2). It is thus reasonable to recommend against their use during the preparation of LID. Notably, LID does not mean “no” iodine diet. Patient’s convenience, diet habit and well-being are also of major importance in addition to therapeutic efficacy when setting up dietary guidelines. From the clinical point of view, iodine-free soy sauces can be permitted for LID preparation. First, radioiodine uptake would not be impaired by pre-administration of such soybean products per se (25). Second, soy sauces used as seasonings in Asian food are not ingested in large amounts. Lastly, the flavor of soy sauces is so popular in the general population that their use cannot be readily avoided. Therefore, we recommend to allow the consumption of iodine-free soy sauces identified in the current study during the 2 weeks’ LID period.
The source of iodine content in iodine-containing soy sauces might come from food additives, as found in the 2 brands of soy sauces that contain kelp extracts. Kelp is rich in elemental iodine and is often used to provide additional umami in soy sauces (13). Based on the findings presented here, most soy sauces do not contain iodine and can be consumed during a LID. The other iodine-containing soy sauce that did not contain kelp extract had a much higher salt content as compared to iodine-free soy sauces (9,255 mg/100 mL vs. 4,252 mg/100 mL). Therefore, the source of elemental iodine might have originated from the added iodized salt. According to the Taiwan Food and Drug Administration, the iodine in salt fortified with potassium iodide or potassium iodate was 12–20 mg/kg before June, 2017 (26). However, around two thirds of the salts available in the domestic markets are non-iodized based on a salt survey in 2012 (27). This might be the reason that most of the salts added in soy sauces are iodine-free. While we do not have information on the manufacturing processes of the soy sauces, we assume that iodized salt rather than kelp extract has been used during processing and was thus responsible for the high iodine-content in the soy sauce. We strongly recommend that soy sauce manufacturers should be required to indicate the iodine content on the product label.
Measurements of iodine content in soy sauces poses certain difficulties compared to UIC measurements because soy sauces have a blackish color due to the fermentation processes of soy beans or the additives such as caramel color. When absorbance was measured at the final step of the S-K reaction, light needs to be transmittable and thus a high dilution factor is compulsory. Typically, when UIC is measured by the S-K method, urine samples do not need to be diluted unless the concentration is outside the range of the calibration curve. Even if dilution is needed, the dilution factor of UIC measurements is usually below 10. In this study, we found that a dilution factor of 50 or above enabled us to achieve a highly accurate result using the S-K method. To our knowledge, this is the first time that iodine content of soy sauces was determined by the S-K reaction. Being prudent, we performed tests including the precision test, serial dilution test, and recovery tests and then obtained the CVs, recovery rates and linearity to validate the results. In addition, we also measured iodine content in soy sauces using ICP-MS and the obtained results were highly consistent with those of the S-K method. Notably, the pipeline and cone orifice of ICP-MS would clog easily after measurements, probably due to the metal ions and volatile compounds in the soy sauces. The ICP-MS method used in the present study employed triton X-100 and 0.5% ammonia solution to prepare the samples into aqueous solution with a final volume 100 times of the original sample (17–19). Tellurium (128Te) was the internal standard. Microwave digestion was not needed when UIC was measured by ICP-MS but this needed to be modified when iodine contents were measured in complex matrixes such as soy sauces (22, 28). Furthermore, microwave digestion is time-consuming and is not routinely applicable in ICP-MS measurements. The ammonium persulfate used in the S-K method is able to digest the interfering substances in soy sauces. Based on these considerations and the results presented here, the S-K method can be used to measure the iodine content in soy sauces after appropriate dilution.
There are some limitations in this study. First, not all soy sauces marketed in Taiwan were tested in this study. Second, neither the manufacturing process of soy sauces nor the types of salt (iodized or non-iodized) added during fermentationis known. We postulate that kelp extract and iodized salt at least in part contribute to the iodine content in iodine-containing soy sauces. We suggest that the S-K method can be used to measure the iodine content in soy sauces after appropriate dilution. Finally, further modifications of the analytical procedures may permit ICP-MS to be used to measure the iodine content in complex matrixes such as soy sauces in the future.
In conclusion, except for certain special additives such as kelp extracts or iodized salts, most domestic soy sauces in Taiwan are iodine-free.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
C-JH and W-SH designed the study. L-HL, C-PC, C-WS performed the iodine measurements. L-HL, C-PC, S-FW, H-SC, C-MH, K-TT, F-FW, C-WS, C-CY analyzed and interpreted the data. C-JH, L-HL, C-PC prepared the manuscript. C-CY and W-SH critically revised the manuscript. All authors contributed to the article and approved the submitted version.
This research was partially supported by the Ministry of Science and Technology, Taiwan (grant number: MOST 109-2314-B-075-068, MOST 110-2314-B-075-007, MOST 111-2314- B-350-004 & B-075-071), 104-CCH-IRP-085 and the Taipei Veterans General Hospital (grant number: V110B-003, V111B-001, V112B-003, VN110-13, VN111-03, VN112-09).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1058695/full#supplementary-material
1. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid (2016) 26:1–133. doi: 10.1089/thy.2015.0020
2. Morsch EP, Vanacor R, Furlanetto TW, Schmid H. Two weeks of a low-iodine diet are equivalent to 3 weeks for lowering urinary iodine and increasing thyroid radioactive iodine uptake. Thyroid (2011) 21:61–7. doi: 10.1089/thy.2010.0232
3. Tran L, Hammuda M, Wood C, Xiao CW. Soy extracts suppressed iodine uptake and stimulated the production of autoimmunogen in rat thyrocytes. Exp Biol Med (2013) 238:623–30. doi: 10.1177/1535370213489488
4. JTP II, Hennessey JV. Two-week low iodine diet is necessary for adequate outpatient preparation for radioiodine rhTSH scanning in patients taking levothyroxine. Thyroid (2004) 14:57–63. doi: 10.1089/105072504322783858
5. Moon JA, Yoo CH, Kim MH, Lee SM, Oh YJ, Ryu YH, et al. Knowledge, self-efficacy, and perceived barriers on the low-iodine diet among thyroid cancer patients preparing for radioactive iodine therapy. Clin Nutr Res (2012) 1:13–22. doi: 10.7762/cnr.2012.1.1.13
6. Ju DL, Park YJ, Paik HY, Song Y. The impact of low adherence to the low-iodine diet on the efficacy of the radioactive iodine ablation therapy. Clin Nutr Res (2015) 4:267–71. doi: 10.7762/cnr.2015.4.4.267
7. Song DH, Chun BH, Lee S, Son SY, Reddy CK, Mun HI, et al. Comprehensive metabolite profiling and microbial communities of doenjang (Fermented soy paste) and ganjang (Fermented soy sauce): A comparative study. Foods (2021) 10:641. doi: 10.3390/foods10030641
8. Ershow AG, Skeaff SA, Merkel JM, Pehrsson PR. Development of databases on iodine in foods and dietary supplements. Nutrients (2018) 10:100. doi: 10.3390/nu10010100
9. Patterson KY, Spungen JH, Roseland JM, Pehrsson PR, Ershow AG, Gahche JJ. USDA, FDA And ODS-NIH database for the iodine content of common foods. U.S. Depart Agric (2020) 1:11. Available at: https://www.ars.usda.gov/ARSUSERFILES/80400535/DATA/IODINE/IODINE%20DATABASE_DOCUMENTATION_.PDF.
10. Carlsen MH, Andersen LF, Dahl L, Norberg N, Hjartaker A. New iodine food composition database and updated calculations of iodine intake among norwegians. Nutrients (2018) 10:930. doi: 10.3390/nu10070930
11. Ovadia YS, Gefel D, Weizmann N, Raizman M, Goldsmith R, Mabjeesh SJ, et al. Low iodine intake from dairy foods despite high milk iodine content in Israel. Thyroid (2018) 28:1042–51. doi: 10.1089/thy.2017.0654
12. Coneyworth LJ, Coulthard L, Bailey EH, Young SD, Stubberfield J, Parsons L, et al. Geographical and seasonal variation in iodine content of cow's milk in the UK and consequences for the consumer s supply. J Trace Elem Med Biol (2020) 59:126453. doi: 10.1016/j.jtemb.2020.126453
13. Watanabe T. Food composition tables of Japan and the nutrient. J Nutr Sci Vitaminol (Tokyo) (2015) 61 Suppl:S25–7. doi: 10.3177/jnsv.61.S25
14. Katagiri R, Asakura K, Sasaki S, Hirota N, Notsu A, Miura A, et al. Estimation of habitual iodine intake in Japanese adults using 16 d diet records over four seasons with a newly developed food composition database for iodine. Br J Nutr (2015) 114:624–34. doi: 10.1017/S0007114515002019
15. Tang KT, Wang FF, Fu SS, Braverman LE, Lin JD, Won GS. A simple microplate method with improved low iodine concentration sensitivity in urinary iodine measurement. Thyroid (2015) 25:1173–4. doi: 10.1089/thy.2015.0184
16. Huang CJ, Tseng CL, Chen HS, Garabwan C, Korovo S, Tang KT, et al. Iodine nutritional status of school children in Nauru 2015. Nutrients (2016) 8:520. doi: 10.3390/nu8090520
17. Huang CJ, Lee LH, Cheng CP, Chen HS, Hwu CM, Tang KT, et al. (2021). Analytical validation of an inductively coupled plasma mass spectrometry method for urinary iodine concentration measurements in Taiwan. J Formos Med Assoc (2023). doi: 10.1016/j.jfma.2023.02.010
18. Huang CJ, Cheng CP, Lee LH, Chen HS, Hwu CM, Tang KT, et al. Iodine nutritional status of lactating women in northern Taiwan in 2019. J Chin Med Assoc (2021) 84:400–4. doi: 10.1097/JCMA.0000000000000505
19. Huang CJ, Tseng CL, Chen HS, Hwu CM, Tang KT, Won JG, et al. Iodine nutritional status of pregnant women in an urban area of northern Taiwan in 2018. PloS One (2020) 15:e0233162. doi: 10.1371/journal.pone.0233162
20. Dold S, Baumgartner J, Zeder C, Krzystek A, Osei J, Haldimann M, et al. Optimization of a new mass spectrometry method for measurement of breast milk iodine concentrations and an assessment of the effect of analytic method and timing of within-feed sample collection on breast milk iodine concentrations. Thyroid (2016) 26:287–95. doi: 10.1089/thy.2015.0317
21. Flores EMM, Mello PA, Krzyzaniak SR, Cauduro VH, Picoloto RS. Challenges and trends for halogen determination by inductively coupled plasma mass spectrometry: A review. Rapid Commun Mass Spectrom (2020) 34 Suppl 3:e8727. doi: 10.1002/rcm.8727
22. Huynh D, Zhou SJ, Gibson R, Palmer L, Muhlhausler B. Validation of an optimized method for the determination of iodine in human breast milk by inductively coupled plasma mass spectrometry (ICPMS) after tetramethylammonium hydroxide extraction. J Trace Elem Med Biol (2015) 29:75–82. doi: 10.1016/j.jtemb.2014.07.005
23. Chang TY, Wang FF, Yang CC, Liu YL, Huang CJ. (2022). Iodine concentration determination in commercial dairy milk and plant-based substitutes in northern Taiwan, in: Abstract 11 at poster presentation. The Annual meeting of the Endocrine Society, Taipei, Taiwan, 2022 March 19-20. ROC.
24. Wang FF. (2020). Dietary iodine intake and iodine content in breast milk in lactating mothers in a regional teaching hospital in Taiwan, in: Poster presentation. The 17th Asia-Oceania Congress of Endocrine and the 8th Seoul International Congress of Endocrinology and Metabolism, Seoul, Korea, 2020 October 28-31.
25. Messina M, Redmond G. Effects of soy protein and soybean isoflavones on thyroid function in healthy adults and hypothyroid patients: A review of the relevant literature. Thyroid (2006) 16:249–58. doi: 10.1089/thy.2006.16.249
26. Iodine Global Network. Taiwan To raise iodine levels in salt (2015). Available at: https://www.ign.org/taiwan-to-raise-iodine-levels-in-salt.htm (Accessed September 21, 2022).
27. Shaw N. Monitoring iodine contents of salt products and related health risk. Taipei: Project of Food and Drug Administration, Ministry of Health and Welfare in Taiwan (2012).
Keywords: iodine, low iodine diet, soybean, soy sauce, Taiwan
Citation: Huang C-J, Lee L-H, Cheng C-P, Yao S-F, Chen H-S, Hwu C-M, Tang K-T, Wang F-F, Shih C-W, Yang C-C and Huang W-S (2023) Measurements of elemental iodine in soy sauces in Taiwan using a modified microplate method. Front. Endocrinol. 14:1058695. doi: 10.3389/fendo.2023.1058695
Received: 30 September 2022; Accepted: 28 February 2023;
Published: 09 March 2023.
Edited by:
Terry Francis Davies, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Peter Kopp, Centre Hospitalier Universitaire Vaudois (CHUV), SwitzerlandCopyright © 2023 Huang, Lee, Cheng, Yao, Chen, Hwu, Tang, Wang, Shih, Yang and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wen-Sheng Huang, d3NodWFuZzAxQGdtYWlsLmNvbQ==; Chen-Chang Yang, Y2N5YW5nQHZnaHRwZS5nb3YudHc=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.