 Ze Yang
Ze Yang Kai Huang2†
Kai Huang2†
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Endocrinol. , 01 March 2023
Sec. Obesity
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1028708
This article is part of the Research Topic Advances in Obesity Prevention, Treatment and Management: Lifecycle and Complex System Approaches View all 19 articles
Background: Obesity is considered one of the biggest public health problems, especially in the background of the coronavirus disease 2019 (COVID-19) lockdown. It is urgent to find interventions to control and improve it. We performed this systematic review and meta-analysis to summarize the effect of traditional Chinese exercise on obesity.
Methods: We searched PubMed, Embase, Cochrane Library, the China National Knowledge Infrastructure (CNKI), the Chinese Scientific Journal Database (VIP), the Chinese Biomedical Literature Database (CBM), and WanFang database for updated articles published from the inception of each database to June 2022. Randomized controlled trials (RCTs) on traditional Chinese exercise in weight reduction were included, and related data were extracted. The random-effects model was used to adjust for the heterogeneity of the included studies, and funnel plots were used to examine publication bias.
Results: A total of 701 participants were included in the 10 studies. Compared with the control group, the outcome of body weight [mean difference (MD) = −6.10; 95% CI = -8.79, -3.42], body mass index (MD = −2.03; 95% CI = -2.66, -1.41), body fat mass (MD = −3.12; 95% CI = -4.49, -1.75), waist circumference (MD = −3.46; 95% CI = -4.67, -2.24), hip circumference (MD = −2.94; 95% CI = -4.75, -1.30), and waist-to-hip ratio (MD = −0.04; 95% CI = -0.06, -0.03) in the intervention group had significant differences. Egger’s test and funnel plots showed that the potential publication bias of the included studies was slight (p = 0.249).
Conclusion: Traditional Chinese exercise is an effective treatment for obesity; people under the COVID-19 lockdown could do these exercises to control weight. However, a precise and comprehensive conclusion calls for RCTs on a larger scale with more rigorous designs considering the inferior methodological quality and limited retrieved articles.
Systematic review registration: www.crd.york.ac.uk/PROSPERO/, identifier CRD42021270015.
In the past 50 years or so, the prevalence of obesity has increased worldwide, reaching an epidemic level (1). The prevalence of obesity has doubled worldwide since 1980 (2). Nearly a third of the global population has been determined to be obese or overweight (3). Since December 2019, when the coronavirus infection first emerged (4), this challenge faced by individuals has been more outstanding, with more than 50% of individuals with obesity reporting increased weight during the lockdown (5). The health problem of obesity ranges from psychological consequences to physical consequences, such as obstructive sleep apnea and arthritis, which severely affect the quality of life; the condition becomes even worse if other diseases occur together with it (6, 7). These diseases include hypertension (8), dyslipidemia, cardiovascular disease, type 2 diabetes mellitus, and dementia (9, 10). Therefore, weight reduction and weight loss maintenance are particularly important.
Studies have manifested that physical exercise is an effective way to achieve weight loss whether in women or in children (11–14). However, many kinds of physical exercise are intense or monotonous, making it difficult for people to maintain exercising. Moreover, patients with obesity cannot do too much intensive and strenuous exercise or it may induce severe exercise-induced muscle injury (15), thus the exercise intensity and duration for obese patients must be carefully selected (16). Traditional Chinese exercise (TCE), originating from traditional Chinese medicine tracing back to approximately 3,000 years ago, is used as a therapeutic and aerobic exercise, including tai chi, qigong, Baduanjin, Wuqinxi, Yijinjing, and other mind–body therapies (17, 18). This kind of exercise is part of low- to moderate-intensity aerobic exercises, which are different substantially from the high-intensity physical exercise (19).
Although meta-analyses have shown the effectiveness of TCE in knee osteoarthritis, stroke, and cognitive outcomes for older adults (20–22), whether TCE is more effective in weight reduction and weight loss maintenance than other exercise interventions or without treatment has not been reported yet. The main objective of this study was to identify whether TCE is effective in weight reduction and weight loss maintenance, to incorporate all available randomized controlled trials (RCTs), and to investigate relevant subgroups.
We searched PubMed, Embase, Cochrane Library, the China National Knowledge Infrastructure (CNKI), the Chinese Scientific Journal Database (VIP), the Chinese Biomedical Literature Database (CBM), and WanFang Database for updated articles published from the inception of each database to 1 June 2022. At the same time, we searched for gray literature that met the inclusion criteria in Open Grey, Clinical Trials.gov, and WHO Clinical Trial Registration Center. When duplicate publications were identified, we chose the most complete and recent trial. Two investigators (YY and ZY) independently retrieved all related studies in the database and excluded duplicate publications. The search strategy for PubMed is presented in Table 1.
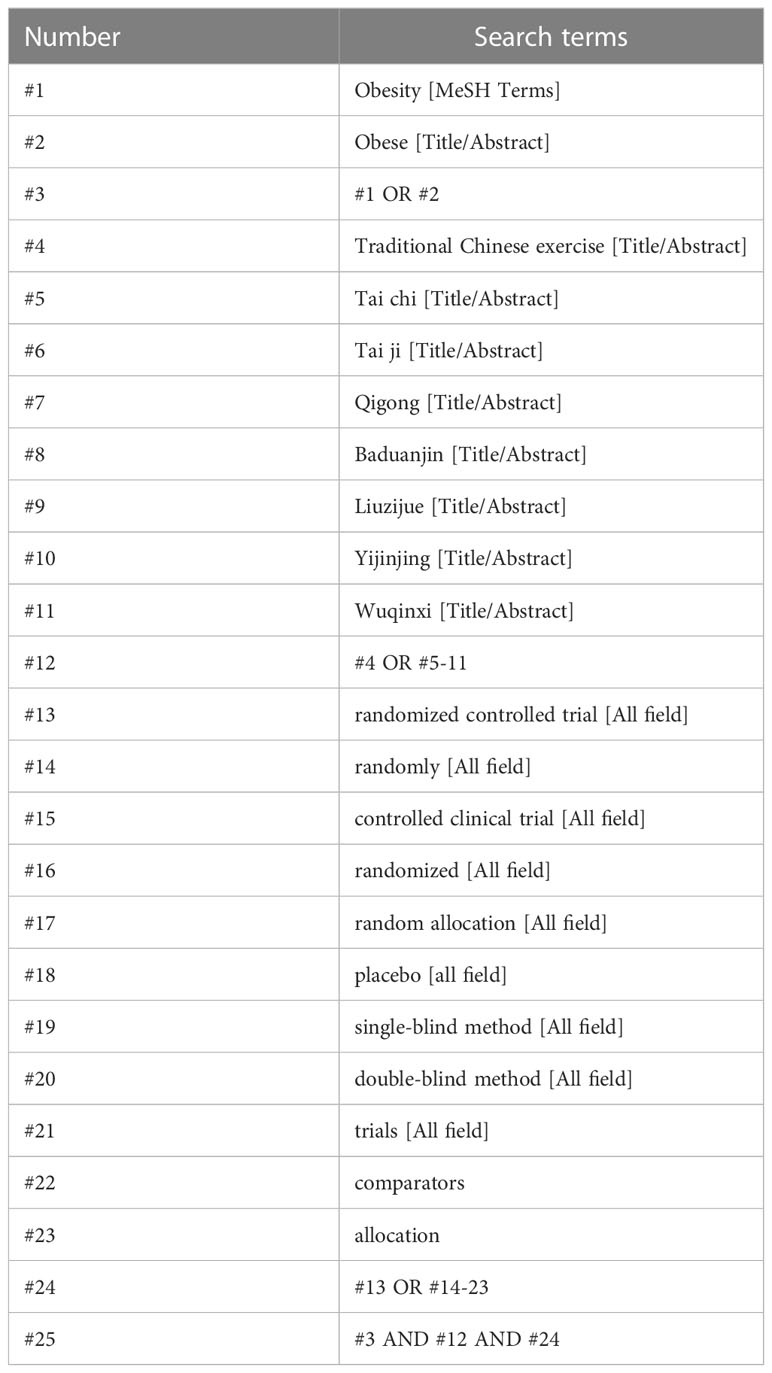
Table 1 Search strategy in PubMed database.
Our meta-analysis is reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (23) Statement and has been registered at the International Prospective Register of Systematic Reviews (number: CRD42021270015).
The inclusion criteria are as follows: 1) the studies must be RCTs; 2) age of participation >18 years; 3) diagnostic criteria for obesity in the study are employed according to the region and ethnic group (Asia-Pacific ≥25.0 kg/m2 and America ≥30.0 kg/m2 for adults); 4) the intervention group must do TCE, such as tai chi, qigong, Baduanjin, Yijinjing, or Wuqinxi, whether combined with other interventions like control group or not. The control group does casual exercise or only diet education, auricular plaster therapy, acupoint catgut-embedding therapy without exercise, etc.
Exclusion criteria are as follows: 1) the participation according to the region and ethnic group did not meet the body mass index (BMI) of obesity; 2) age of participation ≤18 years; 3) the intervention group did not do TCE or the control group also did TCE.
Two independent researchers (YY and ZY) read the title, abstract, and full text, screened the literature according to the inclusion and exclusion criteria, and cross-checked the results. If there is a disagreement, a third researcher (QX) will be consulted. Data extracted from the included literature included the following: first author, publication time, mean age or age range, sample size of the study, measures, intervention group and control group taken, duration time, and outcomes.
The quality of the included studies was assessed by the revised Cochrane risk of bias tool (ROB 2.0) in the Cochrane Handbook for Systematic Reviews of Interventions. The following parameters were evaluated: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each item was determined to be at high risk of bias, some concerns (unclear risk of bias), or low risk of bias. The combined evaluation of the above items resulted in overall bias.
Review Manager software (Revman 5.4 Cochrane Collaboration) was used to meta-analyze the selected studies. The odds ratio (OR) was used as the effect size index for dichotomous variables, and the mean difference (MD) was used as the effect size index for continuous variables, with 95% confidence intervals (CIs) in forest plots. Sensitivity analysis and subgroup analysis will be used to analyze the source of heterogeneity. For the sensitivity analysis, it can help find the source of heterogeneity by reestimating the combined effect using the one-by-one elimination method. For subgroup analysis, the studies may be divided into different subgroups according to the duration time, different types of TCE, etc., and whether it could be shown that the subgroup factors were the source of heterogeneity. When high heterogeneity exists (p < 0.1 or I2 > 50%), a random-effects model was used for meta-analysis. Publication bias of major outcome indicators was analyzed by funnel plot in RevMan 5.4 software. When the funnel plot was symmetrical on both sides, the possibility of publication bias between studies was considered low.
The quality of evidence was graded according to the GRADE method and was classified as high grade, moderate grade, low grade, and very low grade. The assessment criteria used in the GRADE method included risk of bias, inconsistency, indirectness, imprecision, and publication bias. A grade would be given for each outcome.
Our initial search yielded 196 articles in total, 28 of which were removed because of duplication. After screening the titles and abstracts, a further 38 items were taken away. A total of 130 articles were reviewed, among which 10 were included in this meta-analysis (24–33). No further study was identified by manual search. The flow diagram of study selection was shown in Figure 1 (guideline flow diagram).
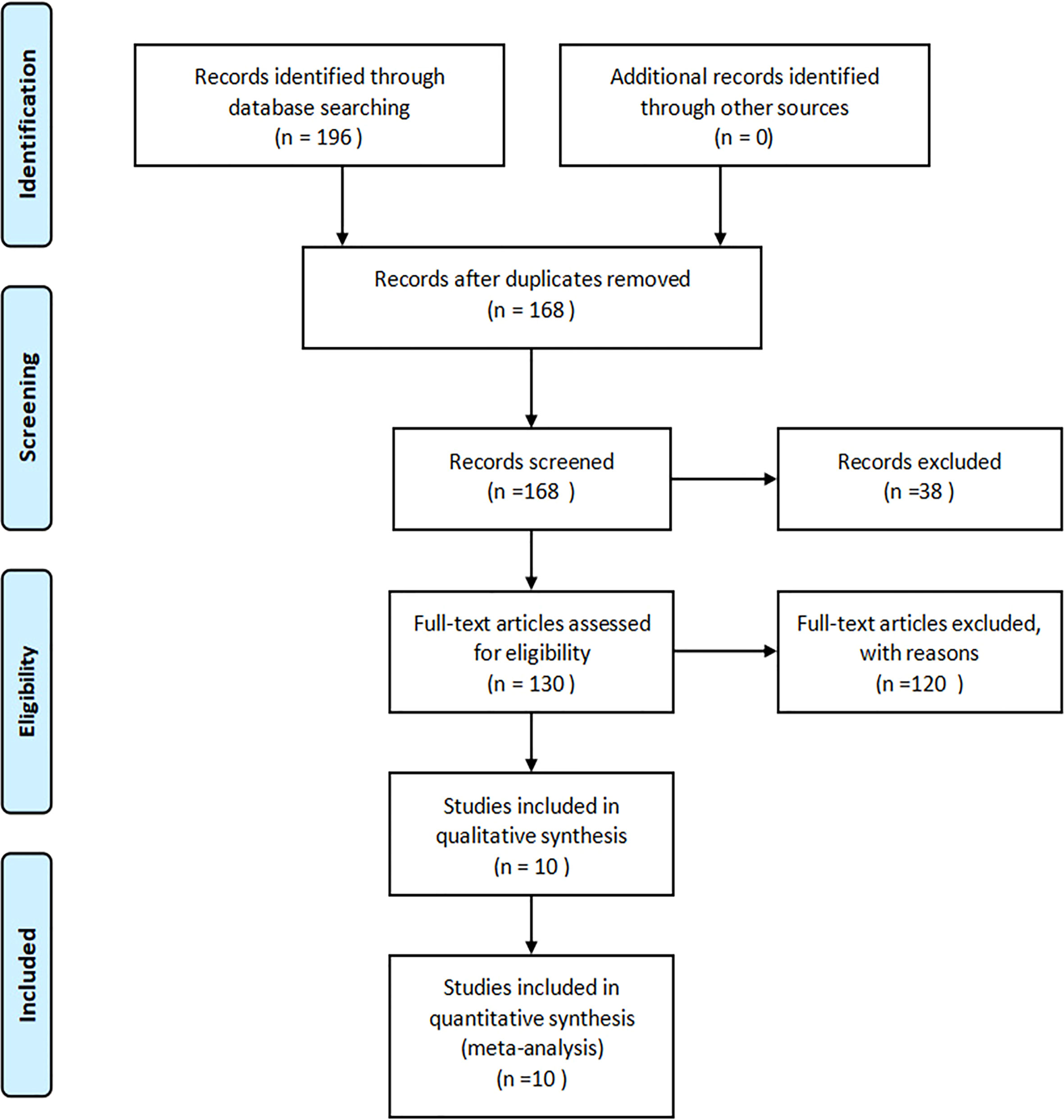
Figure 1 Flowchart of the study selection process.
Ten studies with 701 participants were included for the meta-analysis. Outcomes of the studies are as follows: body weight (BW), BMI, body fat mass (BFM), waist circumference (WC), hip circumference (HC), and waist-to-hip ratio (WHR). The main characteristics of the 10 articles were summarized in Table 2.
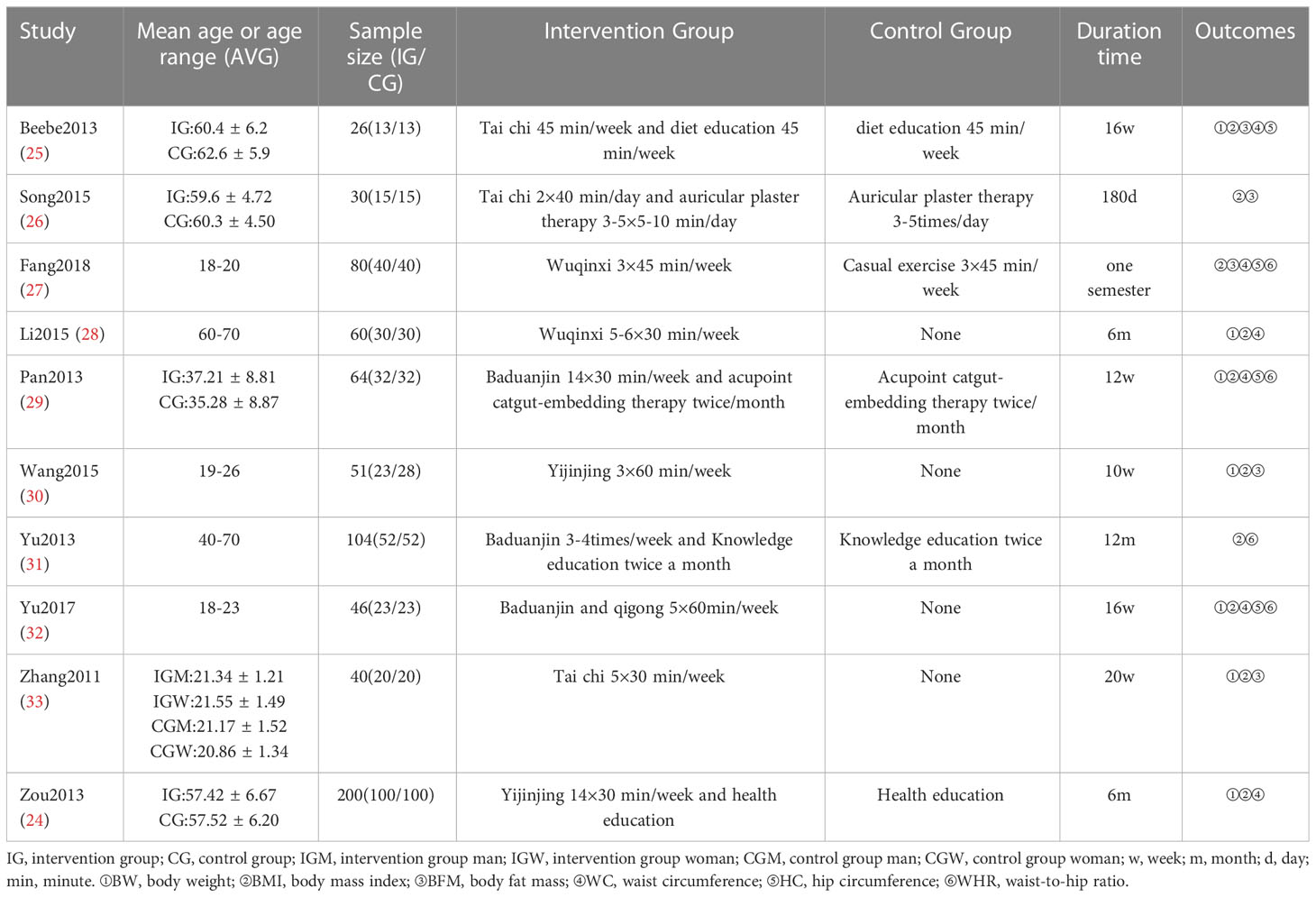
Table 2 Characteristics of the 10 studies included in the meta-analysis.
Results of risk of bias assessment for all included studies were summarized in Figure 2. For bias from the randomization process, eight RCTs were considered as low risk, one study as unclear risk, and one study as high risk. For bias from deviations from intended interventions, bias from missing outcome data, and bias from measurement of the outcome, all 10 RCTs were considered as low risk. For bias from selection of the reported result, six RCTs were rated as likely low risk, three studies were considered as unclear risk, and one study as high risk. For overall risk of bias, five RCTs were considered as low risk, four studies as unclear risk, and one study as high risk. The items that generated bias included the following: ① randomization was reported or but the process was not specifically described or the randomization method was incorrect; ② whether allocation concealment was implemented for the randomization protocol was not reported or unclear; ③ whether blinding was implemented was not clearly reported; ④ whether study protocol registration was not reported or the discussion of reported entries was unclear.
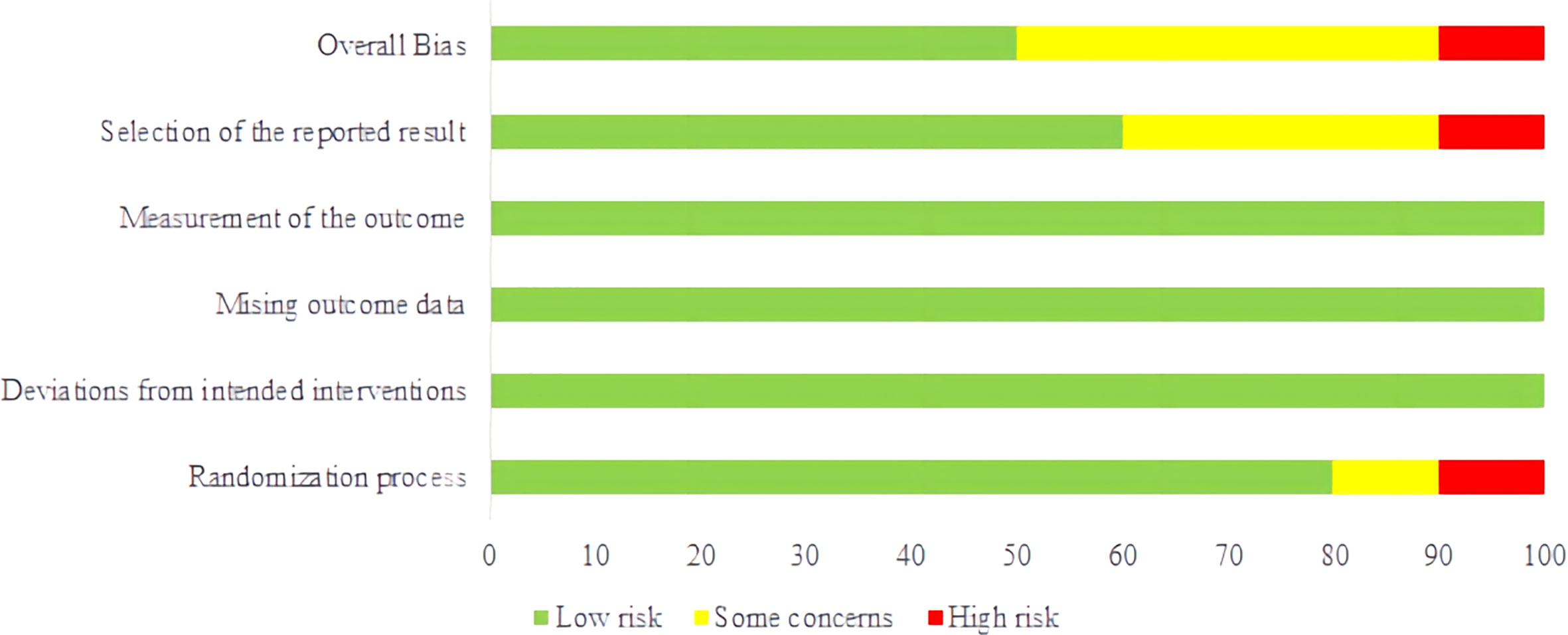
Figure 2 Risk of bias graph. (TCE) on body weight (BW).
Seven studies (24, 25, 28–30, 32, 33) involving 487 participants reported the outcome of BW. The synthesized data indicated that the TCE group had effectively decreased weight as compared with that of the control group (MD = −6.10; 95% CI = -8.79, -3.42), with a high heterogeneity (I2 = 70%, p = 0.0008).
Subgroup analysis showed that the heterogeneity in BW between the two groups disappeared when we excluded the studies whose duration time was less than 16 weeks [including three studies (24, 28, 33); MD = -3.95; 95% CI = -5.78, -2.13; I2 = 0%] (Figure 3). However, whether the duration time was less than 16 weeks or more, there was a significant difference between the two groups in BW.
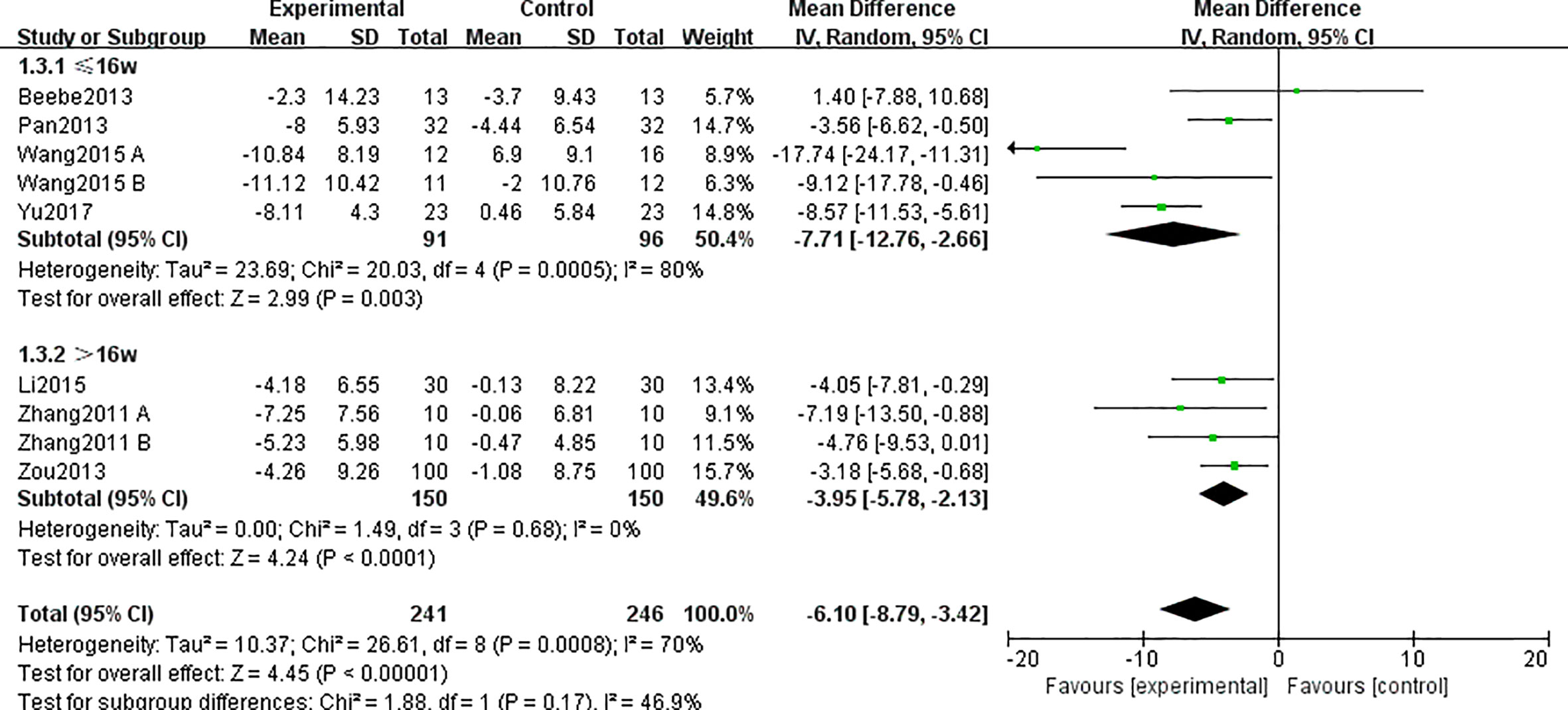
Figure 3 Forest plots and subgroup analysis of duration time for TCE on BW.
Subgroup analysis also showed that all kinds of TCE have a significant difference in BW (Figure 4), which was consistent with the results reported in every study. Heterogeneity analysis suggested that there was a high heterogeneity in the study of exercise styles of Baduanjin (I2 = 81%, p = 0.02) and Yijinjing (I2 = 89%, p = 0.0001) (Figure 4). It may be due to the existence of low-quality research or differences in the duration and time of the research.
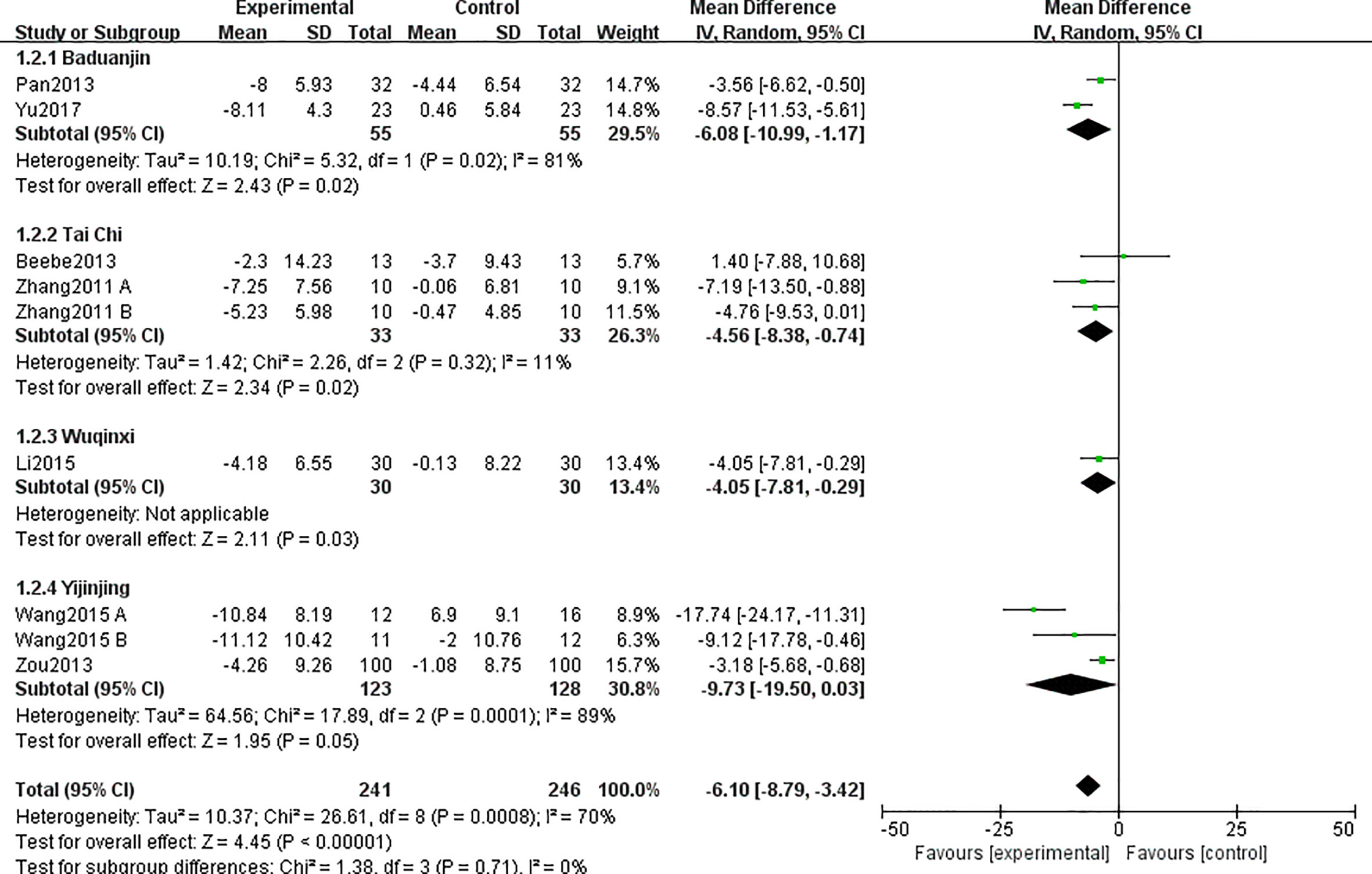
Figure 4 Forest plots and subgroup analysis of different exercise types for TCE on BW.
All 10 included studies (24–33) totaling 701 participants were included in this outcome. The synthesized data indicated that the TCE group had a significant impact on decreasing BMI as compared with the control group (MD = −2.03; 95% CI = -2.66, -1.41), and there was a substantial heterogeneity for this synthesized outcome (I2 = 64%, p = 0.0001). Therefore, these studies were combined using the random-effects model.
Subgroup analysis showed that when excluding the studies whose duration time was less than 16 weeks, the heterogeneity in BMI between intervention groups and control groups decreased [including six studies (24, 26–28, 31, 33); MD = -1.73; 95% CI = -2.33, -1.13; I2 = 40%; p = 0.12] (Figure 5).
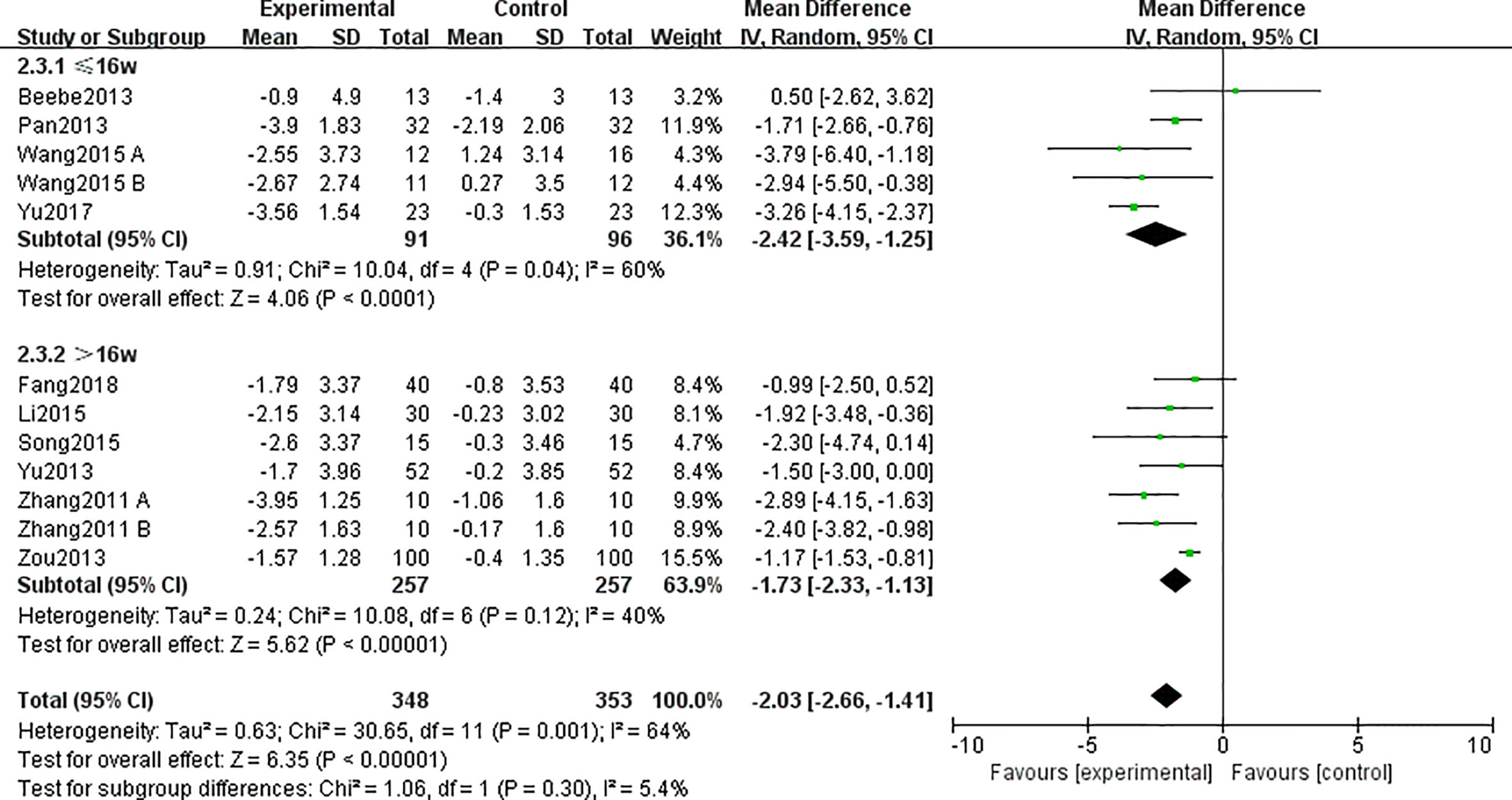
Figure 5 Forest plots and subgroup analysis for traditional Chinese exercise (TCE) on body mass index (BMI).
A total of five studies (25–27, 30, 33) involving 227 participants reported the effects of different interventions on the outcome of BFM. The TCE group had effectively decreased it as compared with that in the control group (MD = −3.12; 95% CI = -4.49, -1.75; I2 = 36%; p < 0.00001) (Figure 6), and there was a low heterogeneity.
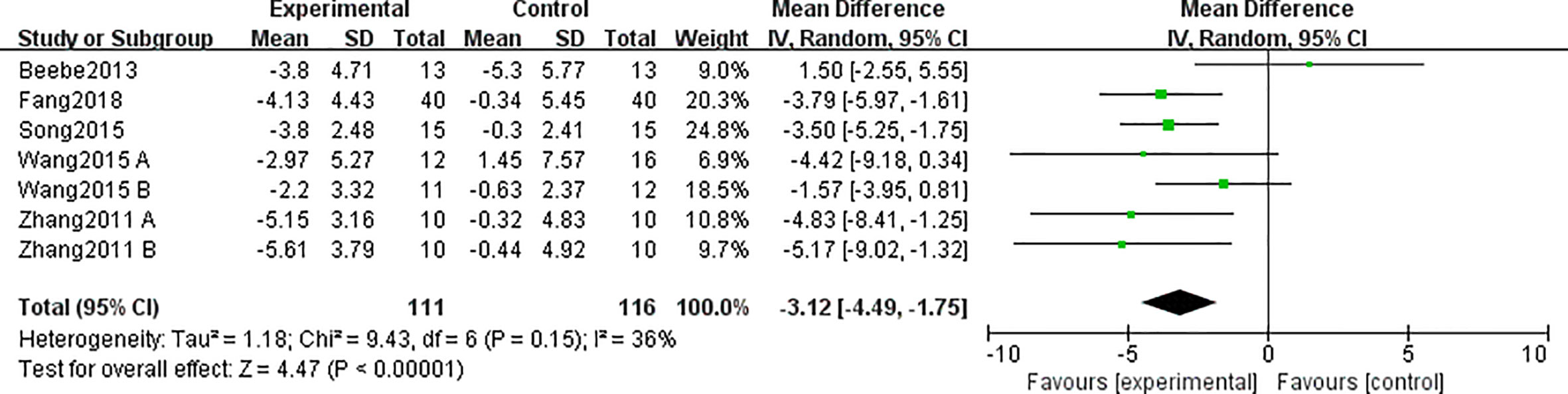
Figure 6 Forest plots for traditional Chinese exercise (TCE) on body fat mass (BFM).
A total of six studies (24, 25, 27–29, 32) reported this outcome. Heterogeneity analysis suggested that there was a high heterogeneity (I2 = 86%, p = 0.003). The sensitivity analysis was carried out one by one, and it was found that when the research by Yu (32) was removed, the heterogeneity between the studies disappeared (I2 = 0%, p = 0.52). The data analysis indicated that WC in the TCE group was lower than that in the control group (MD = −3.46; 95% CI = -4.67, -2.24) (Figure 7).
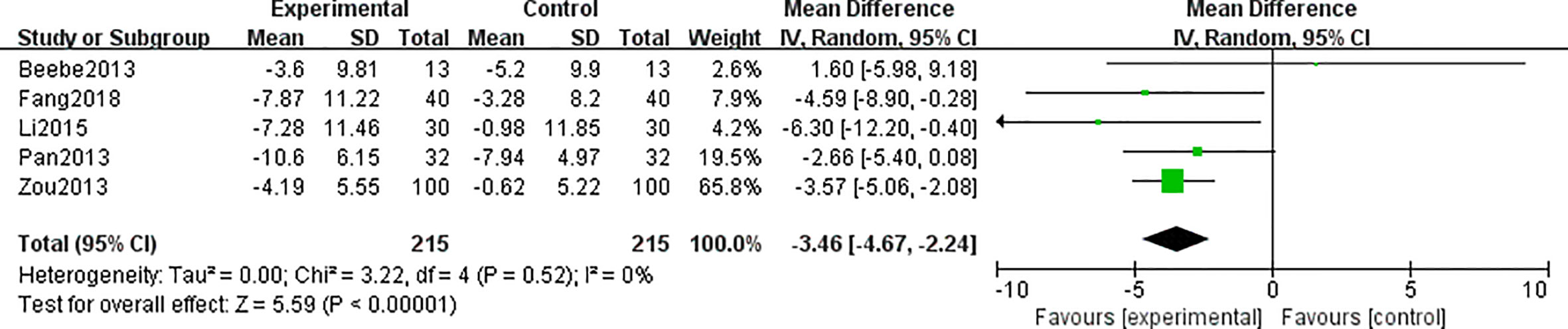
Figure 7 Forest plots for traditional Chinese exercise (TCE) on waist circumference (WC).
A total of four studies (25, 27, 29, 32) involving 216 participants reported the effects of different interventions on the outcome of HC. There was a high heterogeneity (I2 = 70%, p = 0.002). Sensitivity analysis suggested that after removing the research by Yu (32), the heterogeneity disappeared (I2 = 0%, p = 0.68). The data indicated that the TCE group had an effect in decreasing HC as compared with that in the control group (MD = −2.94; 95% CI = -4.75, -1.30) (Figure 8).

Figure 8 Forest plots for traditional Chinese exercise (TCE) on hip circumference (HC).
Four studies (27, 29, 31, 32) involving 240 participants were included in this outcome. Compared with that in the control group, the TCE group had effectively decreased WHR (MD = −0.04; 95% CI = -0.06, -0.03), with no heterogeneity among the studies (I2 = 0%, p < 0.00001) (Figure 9).

Figure 9 Forest plots for traditional Chinese exercise (TCE) on waist-to-hip ratio (WHR).
The publication bias of outcomes was evaluated using funnel plots based on the 10 studies. It can be seen that the funnel plot was not symmetrical, which indicated that no significant publication bias existed (Figure 10).
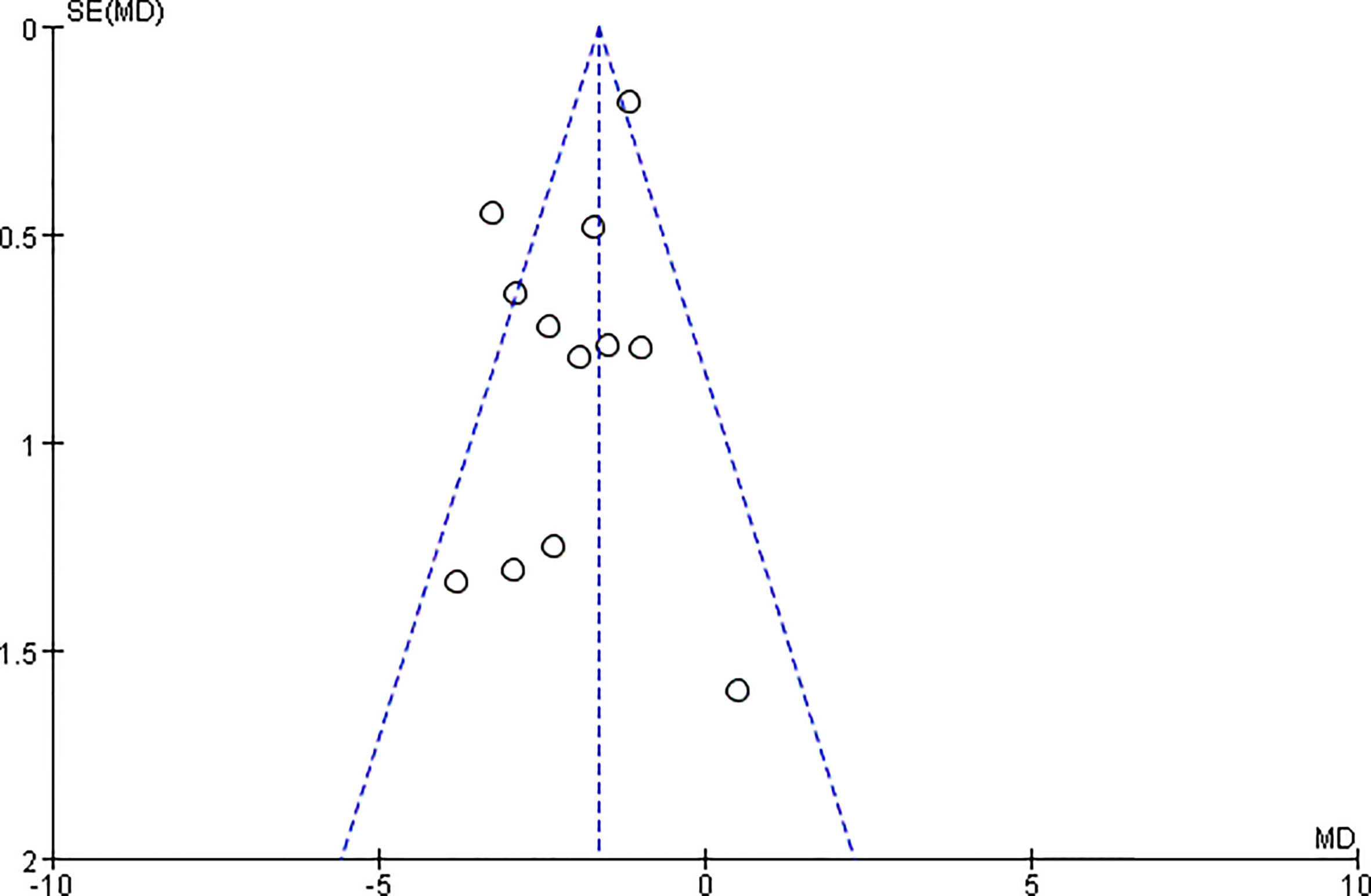
Figure 10 Funnel plots of the body mass index (BMI).
GRADE assessment was conducted for the main outcomes, and the results showed that the evidence quality of BW, BMI, HC, BFM and WHR was low; the evidence quality of WC was moderate (Table 3).
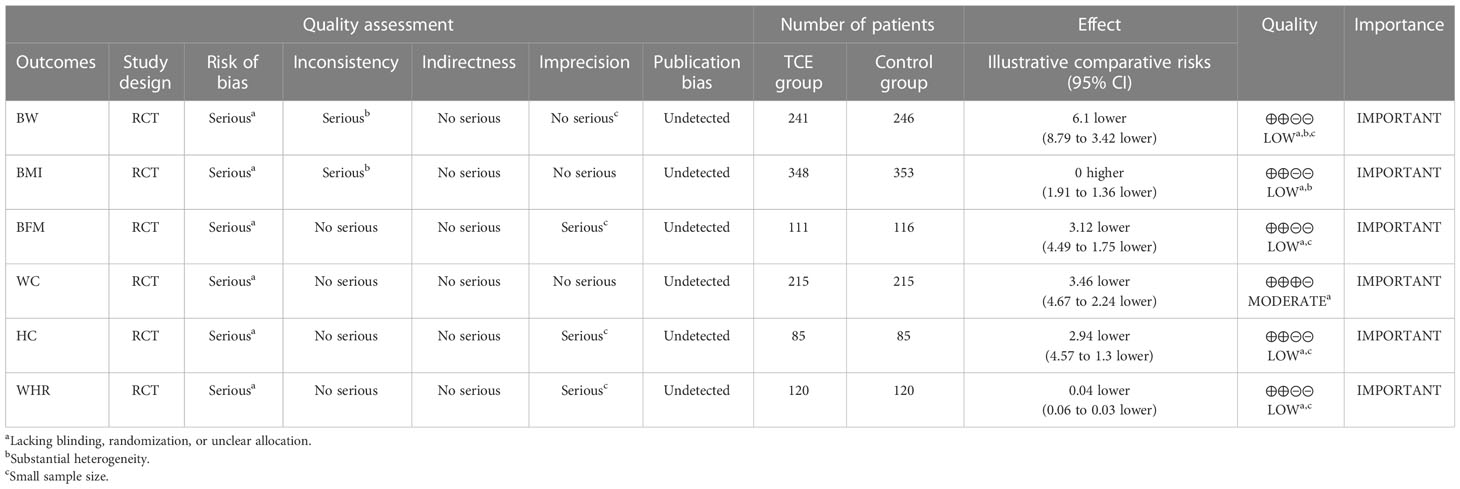
Table 3 Summary of GRADE.
Obesity has been a more outstanding issue during the coronavirus disease 2019 (COVID-19) lockdown, which should be paid more attention to and adopt measures to control. It is the cause of many cardiovascular and cerebrovascular diseases (34) and may be accompanied by an increase in the prevalence of diabetes, cancer, and other diseases (35). There is no doubt that patients with simple obesity can lose weight through exercise, thereby reducing diseases caused by obesity. However, studies reported that the excessive exercise load was not suitable for obese people. They cannot bear too much intensity training (11, 36). TCE is a therapeutic physical and mental aerobic exercise that has been used to improve physical and mental health in China for thousands of years (20, 37–39), which does not need too much space and could be taken even in the COVID-19 lockdown. This meta-analysis and systematic review provide a quantitative estimate of whether TCE is a significant effective strategy for obesity improvement.
We have shown that TCE works significantly in decreasing BW, BMI, BFM, WC, HC, and WHR, which means it plays a positive role in weight reduction and weight loss maintenance. These effects are consistent with the results of individually included RCTs. For different types of TCE, subgroup analyses indicated that there was no significant difference among tai chi, Baduanjin, Yijinjing, and Wuqinxi in BW and BMI. And there was no significant difference among duration time, whether the time is more than 16 weeks or less; they both work. Many studies reported other outcomes, such as triglycerides, serum total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and blood pressure (34, 40). Obesity is often accompanied by lipoprotein atherogenicity, diabetes, hypertension, and hyperlipidemia (41), thus when controlling and treating obesity, TCE can reduce these indicators at the same time. (25, 26). Safety was not reported as an outcome because this outcome was not discussed in these studies. It should be recorded as an outcome in future research.
Our study has several strengths. Firstly, a detailed search strategy is employed by searching different kinds of databases and trial registries. Moreover, no language limitation is set to ensure inclusion of as much data as possible from appropriate studies. Additionally, we try to find heterogeneity between the studies included in our study and to decrease it, which make the results more convincing. Furthermore, our study is the first systematic review and meta-analysis to evaluate the efficacy of TCE on obesity; it could provide evidence for clinical workers that would help them make better clinical decisions. Moreover, we offer ways to control weight at home for those with obesity, which is very necessary in the background of the lockdown.
Our review has several limitations as well. First, the sample size of this meta-analysis was relatively small. As a result, the unknown risk of bias caused by incomplete data could constrain our results. Second, the research results are not restricted by the language of the published articles. Moreover, the intervention of the intervention group of the study is TCE, which is from China, thus eight of the studies are Chinese, which may be of relatively low quality. Third, the intervention protocol varied significantly in the aspect of exercise type (tai chi, Baduanjin, qigong, Yijinjing, Wuqinxi), duration time (from 10 weeks to 12 months), frequency (1–14 times per week), continued time of each exercise (from 30 to 60 min), and at the same time, the control group received different interventions as well; this may be the reason for the heterogeneity of the article.
Despite these limitations, this meta-analysis provides information on the association between TCE and obesity.
In summary, the results of our meta-analysis indicated that TCE may have statistically significant effects on decreasing participants’ BW, BFM, BMI, HC, WC, and WHR, which indicated that it helps to control obesity. The findings presented in the meta-analysis may have important implications worldwide, especially in the COVID-19 lockdown. However, a precise and comprehensive conclusion calls for RCTs on a larger scale with more rigorous designs considering the inferior methodological quality and limited retrieved articles.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Data curation: ZY, YY, QX, and KH; Formal analysis: ZY and QG; Investigation: ZY and XW; Methodology: ZY, YY, and QX; Project administration: ZY; Resources: YY, ZY, and XW; Software: ZY and XW; Supervision: ZY, KH, and QG; Validation: YY and KH; Visualization: ZY and YY; Writing – original draft: ZY, KH, and YY; Writing – review and editing: ZY and XW. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol (2019) 15(5):288–98. doi: 10.1038/s41574-019-0176-8
2. Lin X, Li H. Obesity: Epidemiology, pathophysiology, and therapeutics. Front Endocrinol (Lausanne). (2021) 12:706978. doi: 10.3389/fendo.2021.706978
3. Ataey A, Jafarvand E, Adham D, Moradi-Asl E. The relationship between obesity, overweight, and the human development index in world health organization Eastern Mediterranean region countries. J Prev Med Public Health (2020) 53(2):98–105. doi: 10.3961/jpmph.19.100
4. Qiao C, Zhang H, He M, Ying G, Chen C, Song Y, et al. Symptomatic COVID-19 in eye professionals in wuhan, China. Ophthalmology. (2020) 127(9):1268–70. doi: 10.1016/j.ophtha.2020.04.026
5. Sideli L, Lo Coco G, Bonfanti RC, Borsarini B, Fortunato L, Sechi C, et al. Effects of COVID-19 lockdown on eating disorders and obesity: A systematic review and meta-analysis. Eur Eat Disord Rev (2021) 29(6):826–41. doi: 10.1002/erv.2861
6. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. (2004) 364(9438):937–52. doi: 10.1016/s0140-6736(04)17018-9
7. Anjana M, Sandeep S, Deepa R, Vimaleswaran KS, Farooq S, Mohan V. Visceral and central abdominal fat and anthropometry in relation to diabetes in Asian indians. Diabetes Care (2004) 27(12):2948–53. doi: 10.2337/diacare.27.12.2948
8. Seravalle G, Grassi G. Obesity and hypertension. Pharmacol Res (2017) 122:1–7. doi: 10.1016/j.phrs.2017.05.013
9. Piché ME, Tchernof A, Després JP. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ Res (2020) 126(11):1477–500. doi: 10.1161/circresaha.120.316101
10. Qiao Q, Grandy S, Hiller J, Kostev K. Clinical and patient-related variables associated with initiating GLP-1 receptor agonist therapy in type 2 diabetes patients in primary care in Germany. PloS One (2016) 11(3):e0152281. doi: 10.1371/journal.pone.0152281
11. Chin SH, Kahathuduwa CN, Binks M. Physical activity and obesity: what we know and what we need to know. Obes Rev (2016) 17(12):1226–44. doi: 10.1111/obr.12460
12. Marson EC, Delevatti RS, Prado AK, Netto N, Kruel LF. Effects of aerobic, resistance, and combined exercise training on insulin resistance markers in overweight or obese children and adolescents: A systematic review and meta-analysis. Prev Med (2016) 93:211–8. doi: 10.1016/j.ypmed.2016.10.020
13. Nascimento SL, Pudwell J, Surita FG, Adamo KB, Smith GN. The effect of physical exercise strategies on weight loss in postpartum women: a systematic review and meta-analysis. Int J Obes (Lond). (2014) 38(5):626–35. doi: 10.1038/ijo.2013.183
14. Sirico F, Bianco A, D'Alicandro G, Castaldo C, Montagnani S, Spera R, et al. Effects of physical exercise on adiponectin, leptin, and inflammatory markers in childhood obesity: Systematic review and meta-analysis. Child Obes (2018) 14(4):207–17. doi: 10.1089/chi.2017.0269.Cited in: Pubmed
15. Verheggen RJ, Maessen MF, Green DJ, Hermus AR, Hopman MT, Thijssen DH. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: distinct effects on body weight and visceral adipose tissue. Obes Rev (2016) 17(8):664–90. doi: 10.1111/obr.12406
16. Kim J, Yoon JH. Does obesity affect the severity of exercise-induced muscle injury? J Obes Metab Syndr (2021) 30(2):132–40. doi: 10.7570/jomes20100. Cited in: Pubmed
17. Bo A, Mao W, Lindsey MA. Effects of mind-body interventions on depressive symptoms among older Chinese adults: a systematic review and meta-analysis. Int J Geriatr Psychiatry (2017) 32(5):509–21. doi: 10.1002/gps.4688
18. Nedeljkovic M, Ausfeld-Hafter B, Streitberger K, Seiler R, Wirtz PH. Taiji practice attenuates psychobiological stress reactivity–a randomized controlled trial in healthy subjects. Psychoneuroendocrinology. (2012) 37(8):1171–80. doi: 10.1016/j.psyneuen.2011.12.007
19. Song J, Liu ZZ, Huang J, Wu JS, Tao J. Effects of aerobic exercise, traditional Chinese exercises, and meditation on depressive symptoms of college student: A meta-analysis of randomized controlled trials. Med (Baltimore). (2021) 100(1):e23819. doi: 10.1097/md.0000000000023819
20. Li R, Chen H, Feng J, Xiao Y, Zhang H, Lam CW, et al. Effectiveness of traditional Chinese exercise for symptoms of knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. Int J Environ Res Public Health (2020) 17(21):7873.
21. Chen BL, Guo JB, Liu MS, Li X, Zou J, Chen X, et al. Effect of traditional Chinese exercise on gait and balance for stroke: A systematic review and meta-analysis. PloS One (2015) 10(8):e0135932. doi: 10.1371/journal.pone.0135932
22. Zhang Q, Hu J, Wei L, Cao R, Ma R, Song H, et al. Effects of traditional Chinese exercise on cognitive and psychological outcomes in older adults with mild cognitive impairment: A systematic review and meta-analysis. Med (Baltimore). (2019) 98(7):e14581. doi: 10.1097/md.0000000000014581
23. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-p) 2015 statement. Syst Rev (2015) 4(1):1. doi: 10.1186/2046-4053-4-1
24. Zou Z, Shi X, Zhang H. Clinical study on 100 cases of metabolic syndrome intervened by yijinjing. J Changchun Univ Traditional Chin Med (2013) 29(3):398–9. doi: 10.3969/j.issn.1007-4813.2013.03.011
25. Beebe N, Magnanti S, Katkowski L, Benson M, Xu F, Delmonico MJ, et al. Effects of the addition of t'ai chi to a dietary weight loss program on lipoprotein atherogenicity in obese older women. J Altern Complement Med (2013) 19(9):759–66. doi: 10.1089/acm.2012.0531
26. Song Q, Yuan Y, Jiao C, Zhu X. Curative effect of tai chi exercise in combination with auricular plaster therapy on improving obesity patient with secondary hyperlipidemia [Article]. Int J Clin Exp Med (2015) 8(11):21386–92.
27. Fang R. Effect of wuqinxi traditional Chinese medicine teaching model on serum leptin and insulin R esistance of obese students in senior high school. J Jinzhou Med Univ (2018) 39(5):26–30. doi: 10.13847/j.cnki.lnmu.2018.05.008
28. Li W, Li H, Luan H. Study for the intervention effect of wuqinxi for elder hypertension patients with obesity. Med Inf (Xi'an) (2015) (9):48–9.
29. Pan B, Pan J. Clinical observation on acupoint catgut-embedding therapy combining with ba-duanjin exercise treating simple obesity. Massage Rehabil Med (2013) 4(7):4–5.
30. Wang H, Lv X. Influence of yijinjing practice on body composition of obesity university students. J Sports Adult Educ (2015) 31(6):6466. doi: 0.16419/j.cnki.42-1684/g8.2015.06.017
31. Yu H. Clinical observation on the intervention of baduanjin exercise therapy in 104 patients with hypertension and obesity. Chin clinician (2013) (8):47–48. doi: 10.3969/j.issn.1008-1089.2013.08.025
32. Yu Z. Effects of health Qigong·Ba duan jin on lipid metabolism of obese female college Students①. Contemp Sports Technol (2017) 7(4):25–26. doi: 10.16655/j.cnki.2095-2813.2017.04.025.
33. Zhang H, Zhang H. Effects of long-term taijiquan practice on lipid metabolism and related hormones in obese college students. J Shenyang Sport Univ (2011) 30(6):95–98.
34. Song Q, Yuan Y, Jiao C, Zhu X. Curative effect of tai chi exercise in combination with auricular plaster therapy on improving obesity patient with secondary hyperlipidemia. Int J Clin Exp Med (2015) 8(11):21386–92.
35. Fogarty S, Stojanovska L, Harris D, Zaslawski C, Mathai ML, McAinch AJ. A randomised cross-over pilot study investigating the use of acupuncture to promote weight loss and mental health in overweight and obese individuals participating in a weight loss program. Eat Weight Disord (2015) 20(3):379–87. doi: 10.1007/s40519-014-0175-7
36. Lau PW, Wong del P, Ngo JK, Liang Y, Kim CG, Kim HS. Effects of high-intensity intermittent running exercise in overweight children. Eur J Sport Sci (2015) 15(2):182–90. doi: 10.1080/17461391.2014.933880
37. Guo Y, Xu M, Wei Z, Hu Q, Chen Y, Yan J, et al. Beneficial effects of qigong wuqinxi in the improvement of health condition, prevention, and treatment of chronic diseases: Evidence from a systematic review. Evid Based Complement Alternat Med (2018) 2018:3235950. doi: 10.1155/2018/3235950
38. Yu F, Xin M, Liu N, Huang N, Lu J. The qigong wuqinxi for chronic obstructive pulmonary disease: Protocol for a systematic review and meta-analysis. Med (Baltimore). (2019) 98(30):e16633. doi: 10.1097/md.0000000000016633
39. Yao C, Li Z, Zhang S, Wu Z, Zhu Q, Fang L. Effects of wuqinxi in the patients with chronic low back pain: A randomized controlled trial. Evid Based Complement Alternat Med (2020) 2020:1428246. doi: 10.1155/2020/1428246
40. Li X, Si H, Chen Y, Li S, Yin N, Wang Z. Effects of fitness qigong and tai chi on middle-aged and elderly patients with type 2 diabetes mellitus. PloS One (2020) 15(12):e0243989. doi: 10.1371/journal.pone.0243989
Keywords: obesity, traditional Chinese exercise, Tai Chi, Qigong, Baduanjin, Wuqinxi, COVID-19 lockdown, systematic review and meta-analysis
Citation: Yang Z, Huang K, Yang Y, Xu Q, Guo Q and Wang X (2023) Efficacy of traditional Chinese exercise for obesity: A systematic review and meta-analysis. Front. Endocrinol. 14:1028708. doi: 10.3389/fendo.2023.1028708
Received: 30 August 2022; Accepted: 06 February 2023;
Published: 01 March 2023.
Edited by:
Mikiko Watanabe, Sapienza University of Rome, ItalyReviewed by:
Hailiang Huang, Shandong University of Traditional Chinese Medicine, ChinaCopyright © 2023 Yang, Huang, Yang, Xu, Guo and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiang Wang, d2FuZ3hpYW5nYTE5OTVAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.