 Chang Min Kim1†
Chang Min Kim1† Kihun Kim
Kihun Kim Yun Hak Kim
Yun Hak Kim
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Endocrinol. , 24 October 2022
Sec. Obesity
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.999455
Background: A previous 2014 meta-analysis reported a positive association between obesity and periodontitis. It was considered necessary to update the recently published papers and to analyse subgroups on important clinical variables that could affect the association between obesity and periodontitis. Therefore, we updated the latest studies and attempted to derive more refined results.
Methods: All observational studies were eligible for inclusion. The Newcastle–Ottawa scale was used to qualitatively evaluate the risk of bias. Subgroup analyses were conducted for patients aged 18–34, 35–54, and 55+ years and the countries (European countries, USA, Brazil, Japan, Korea, and other Asian countries).
Results: Thirty-seven full-text articles were included. Obesity conferred increased odds of periodontal disease with an odds ratio (1.35, 95% CI: 1.05–1.75). In the subgroup analysis by age, the odds ratio was the highest in the 18–34 years group (2.21, 95% CI: 1.26–3.89). In the subgroup analysis by country, European countries had the highest odds ratio (2.46, 95% CI: 1.11–5.46).
Conclusion: Despite the differences in degree, a positive association between obesity and periodontitis was found regardless of country or age. Therefore, medical professionals should try to prevent periodontitis by controlling patient weights, and more studies should be conducted to determine the association between obesity and oral health.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42022301343.
Obesity has increased worldwide in the past 50 years and become a significant social problem (1). The prevalence of obesity is seen in one-third of the entire population, and it increases in all age groups of both sexes (2). According to the World Health Organization, which defines obesity as a body mass index (BMI) ≥ 30 kg/m2, obesity is a 21st-century epidemic and health risk factor with a prevalence that is rapidly increasing in children and adolescents (3, 4).
Obesity negatively impacts an individual’s physical and mental health, leading to poor quality of life (5). Obesity can aggravate chronic inflammatory diseases such as diabetes and coronary artery disease (6). Obesity also significantly affects cancer risk and prognosis in individuals (7). Adipokines, which are found in obesity, may induce inflammation, atherosclerosis, diabetes, and psoriasis (8). Patients with coronavirus disease 2019 and who are obese showed higher risks and had worse outcomes than those who were not obese (9). It has been reported that obesity has negative effects on health and systemic diseases (10).
Periodontitis is a very common disease with a high global prevalence as half of all adults worldwide have at least one tooth with apical periodontitis (11). According to the National Health and Nutrition Examination Survey of adults in the US (2009–2014), it is seen that periodontitis is highly prevalent in adults 30 years or older (12). Its social burden has been increasing globally, warranting global changes in public health policy (13). However, more studies related to its risk factors are needed to prevent it.
Several studies have reported an association between obesity and periodontitis. A previous meta-analysis conducted in 2014 reported a positive association between the two diseases (14). It was thought necessary to update the recently published papers and to analyze subgroups on clinical variables (e.g., age or country) that could affect the association between obesity and periodontitis. Therefore, the current study aimed to include newly published studies and to perform novel subgroup analyses.
This systematic review was conducted in accordance with the PRISMA guidelines (15). This guideline was designed to allow authors to report transparently why this review was done, what they did, and what they found. PRISMA checklist was presented in Supplementary materials. The study protocol was registered with PROSPERO (registration number: CRD42022301343). We searched the Embase and PubMed (Medline) databases for studies published between 2010 and January 3, 2022. Initially, the mesh term was considered when establishing a search strategy. However, it was not sufficient to search for relevant papers with only mesh terms. A search strategy was established by adding mesh terms as well as free words related to the topic through discussion between authors. The search strategy was presented in Supplementary Table 1. The search screened the titles and abstracts. Non-human studies, non-articles, and conference abstracts were excluded.
Studies investigating periodontitis in obese and normal-weight individuals of all ages were also included. A previous meta-analysis article that synthesised studies published through 2010 was included, and studies published after 2010 were searched and selected (14). Odds ratio (OR) was identified for studies that included four groups according to the state of periodontitis and obesity. All observational studies (cohort, case-control, and cross-sectional studies) were eligible for inclusion. Case reports, review articles, animal studies, and studies without a control group were excluded. In the case of duplicated studies, those with a larger range of patients were included, while those that did not were excluded. Among the studies in the previous meta-analysis, cases in which the data were incorrectly extracted were confirmed and excluded. Only cases in which periodontitis and obesity were classified according to clear criteria were included. We defined obesity is as a BMI ≥ 30kg/m2 or higher, but BMI ≥ 25 kg/m2 in Asians (16, 17). In addition, We additionally defined obesity based on waist circumference as ≥88 cm in women and ≥102 cm in men, but ≥ 90 cm for men and ≥ 80 cm for women in Asians (18, 19). Periodontal status was based on the periodontal pocket depth, clinical attachment loss, or community periodontal index. Periodontitis was defined as periodontal pocket depth (PPD) ≥ 4mm, clinical attachment level (CAL) ≥ 1mm, and community periodontal index (CPI) ≥ 3 (20, 21). We excluded papers that did not meet the obesity criteria (e.g., BMI mean) or periodontitis criteria.
The literature search was conducted independently by three authors (CK, SL, and WH) who thoroughly screened the titles and abstracts of each study. The full-text articles were reviewed by the same authors and evaluated for eligibility. Any disagreements were resolved through discussion. The extracted information included the number of patients, mean age and range, sex, country providing the sample, periodontal disease evaluation method, nutritional status evaluation method, and main confounding variables. We extracted the number of samples or ORs as effect measures according to all patient and age groups for the data synthesis and subgroup analysis.
We performed meta-analyses to calculate the pooled odds ratio and corresponding 95% confidence intervals (CIs) stratified according to obesity and periodontitis status. The classification of I2 statistics as presented by Higgins et al. was used to evaluate the heterogeneity of the effect measures (22). Heterogeneity was considered low, moderate, or high for I2 values of 25%, 50%, or 75%, respectively. An I² value > 50% indicated substantial heterogeneity. If the heterogeneity exceeded 50%, the random effects method was used; otherwise, the fixed effects method was used. We considered the results statistically significant at values of p < 0.05 or when the CI did not include 1. Review Manager 5.4 software was used to analyse the results. Forest plots were drawn to clearly visualise the synthesised risk. Subgroup analyses were conducted for patients aged 18–34 years, 35–54 years, and 55+ years as well as the countries providing the samples (European countries, USA, Brazil, Japan, Korea, and other Asian countries).
The Newcastle–Ottawa scale was used to qualitatively evaluate the risk of bias for cohort and case-control studies (23). The adapted version of the Newcastle–Ottawa scale presented by Herzog et al. (24) was used to evaluate cross-sectional studies (24). We evaluated the score for each category and classified it as good, fair, and poor according to the Agency for Healthcare Research and Quality (AHRQ) standard (25). We evaluated study quality by establishing a criterion similar to the AHRQ standard for cross-sectional studies.
A funnel plot was drawn to visually evaluate publication bias using Review Manager 5 (RevMan 5). Egger’s regression test was performed to statistically verify publication bias using Stata 13 software.
We used the GRADE approach, a tool for measuring the overall grade in risk estimates as high, moderate. low, or very based on 8 classifications; study limitation, directness, consistency, precision, reporting bias, dose-response association, plausible confounding that would decrease observed effect, and strength of association (26, 27). The assessment tools were shown in Supplementary Tables 2 and 3.
A total of 995 records, including 30 studies from the previous meta-analysis study and 965 studies, were initially found based on the search terms. We excluded 848 records based on the exclusion criteria, including animal studies, duplicated studies, irrelevant articles; therefore, we fully screened 147 records. Of those, 36 studies, which were unrelated to our study topic, were excluded. Thus, a full-text review of 111 papers was conducted. We excluded 74 papers according to the following criteria: inadequate measures of periodontitis or obesity classification or no control group. Ultimately, 37 full-text articles were assessed and finally included (Figure 1). The characteristics of the included studies are shown in Table 1.
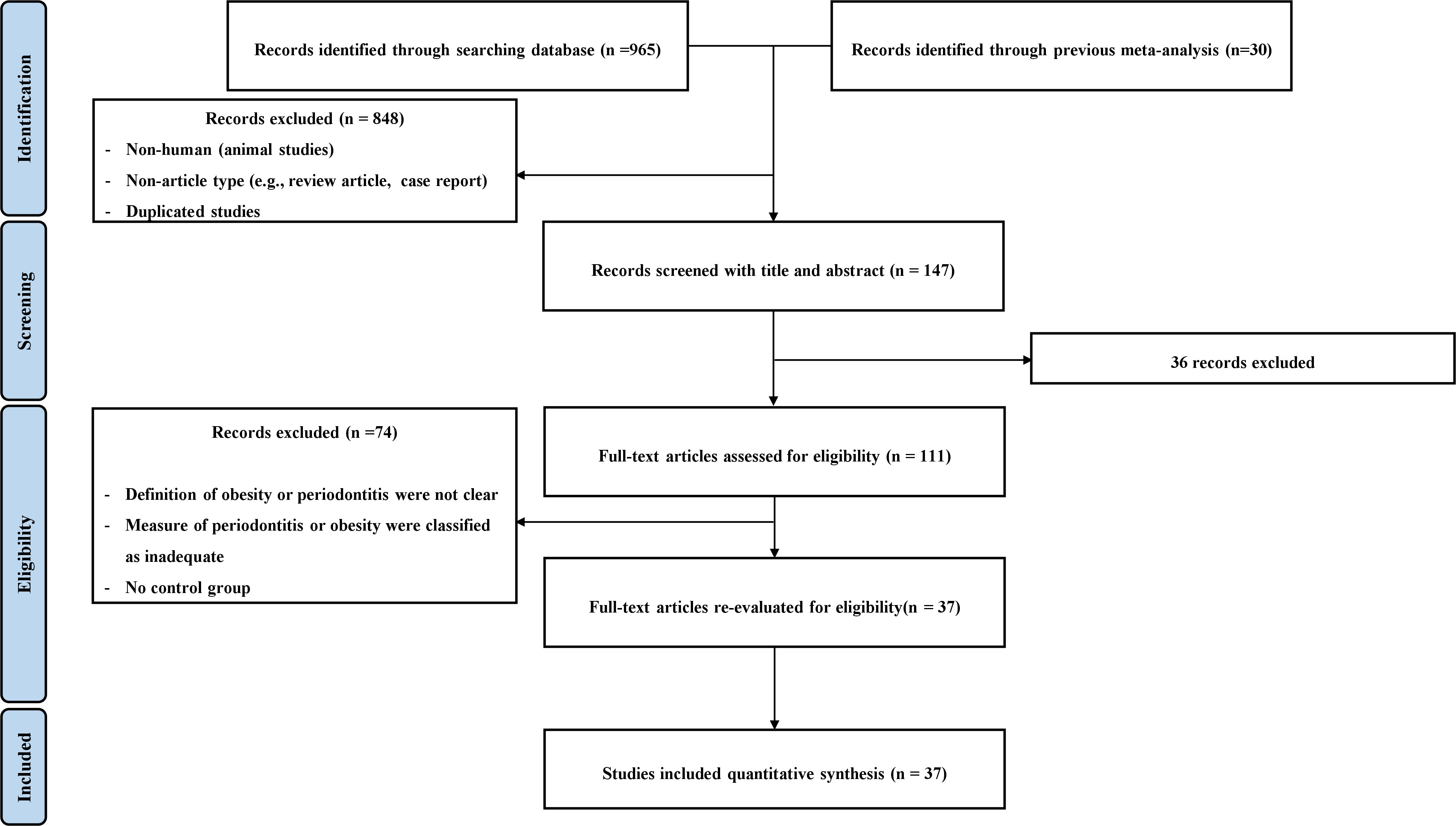
Figure 1 PRISMA flow diagram.
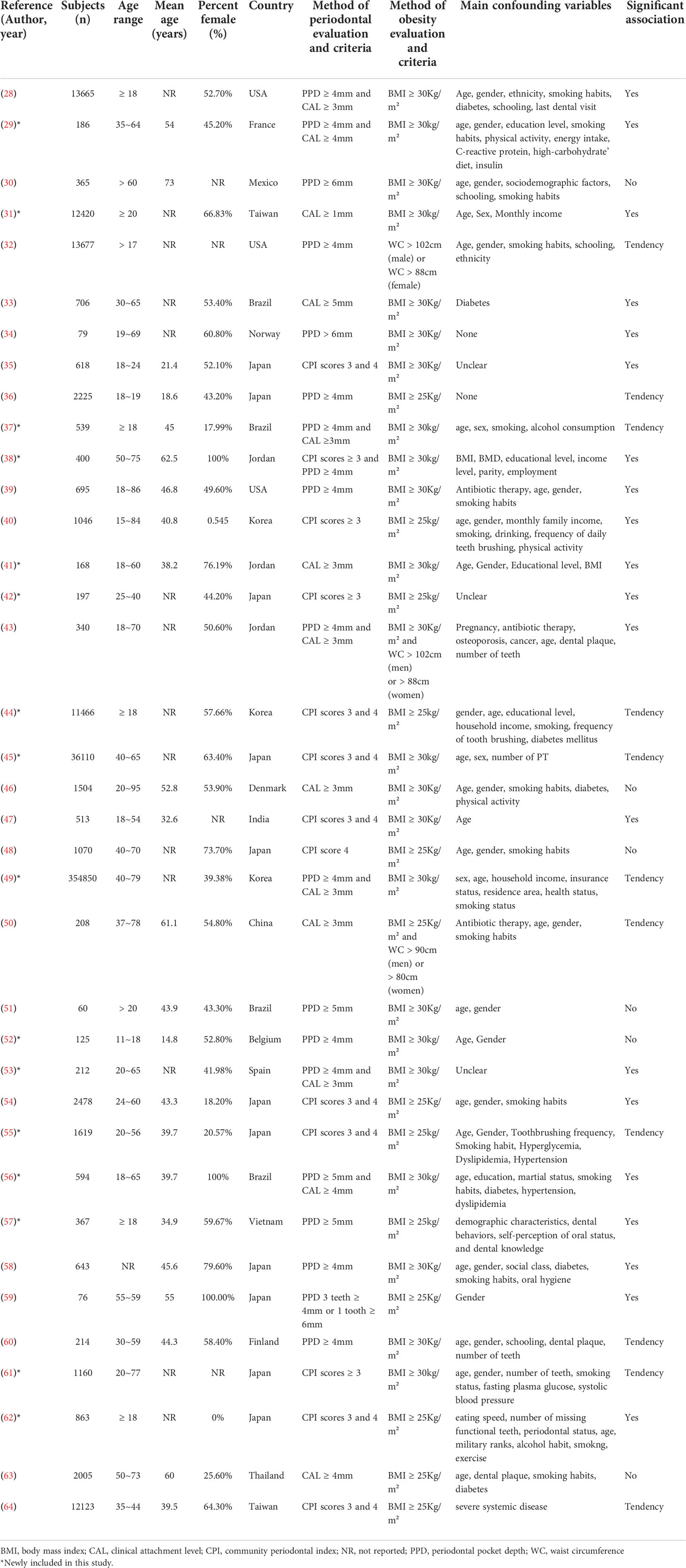
Table 1 Characteristics of the included studies.
We included 29 studies specifying the number of BMI–periodontitis cases or ORs. Among them, the risk of periodontitis was positively associated with obesity in 17 studies. Compared with non-obese group, obesity group conferred increased odds of periodontal disease with an OR of 1.35 (1.05-1.75) (Figure 2). The heterogeneity was 98%.
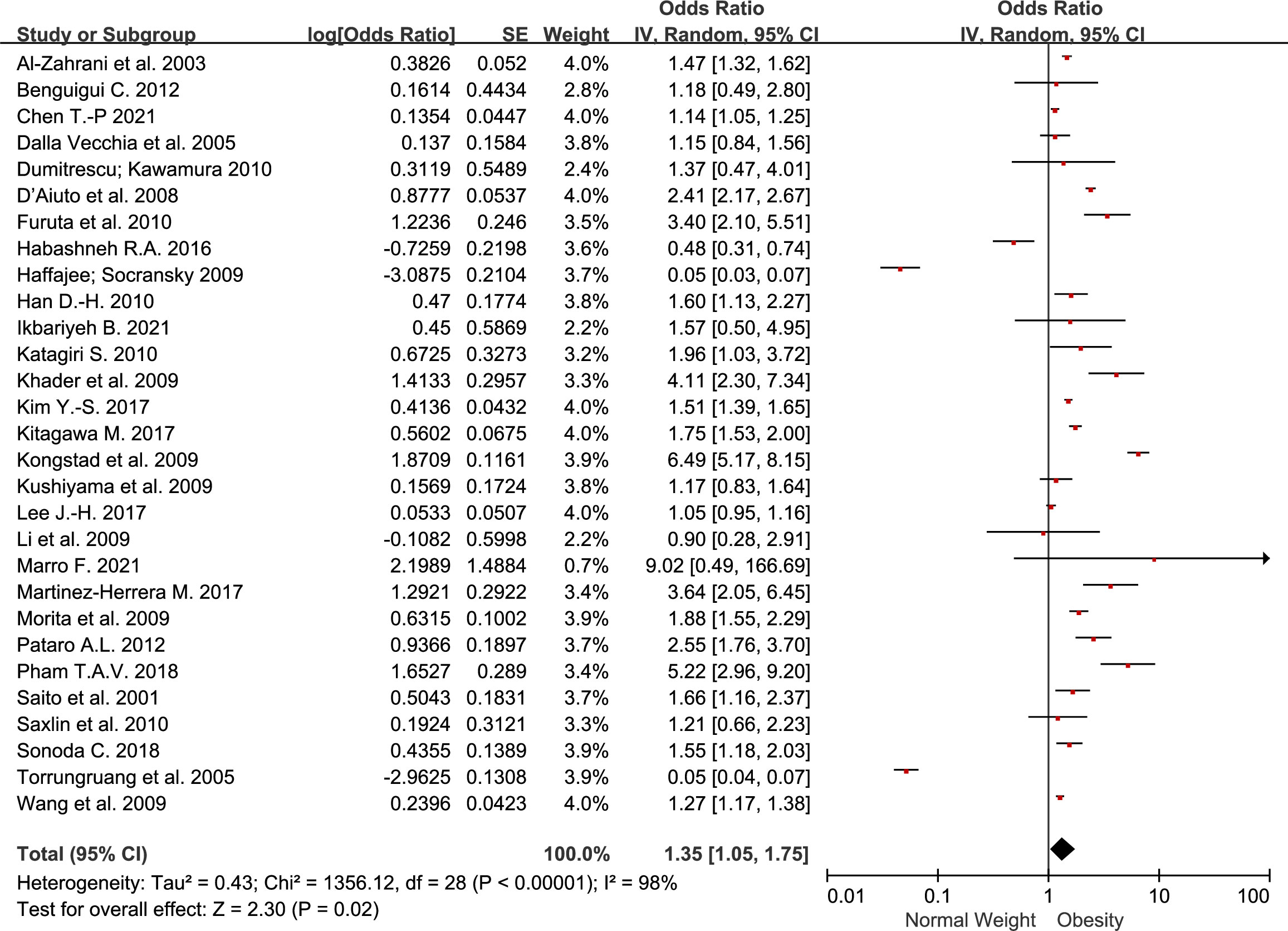
Figure 2 Forest plot of the risk of periodontitis for obesity group compared to non-obesity group.
To determine the effect of age on the obesity-periodontitis association, we classified patients into 18–34, 35–54, and 55+ years age groups. The OR was 2.21 (1.26–3.89) in 18–34 years group, 1.53 (1.17–2.00) in 35–54 years group, and 1.82 (1.16–2.83) in 55+ years group (Table 2).
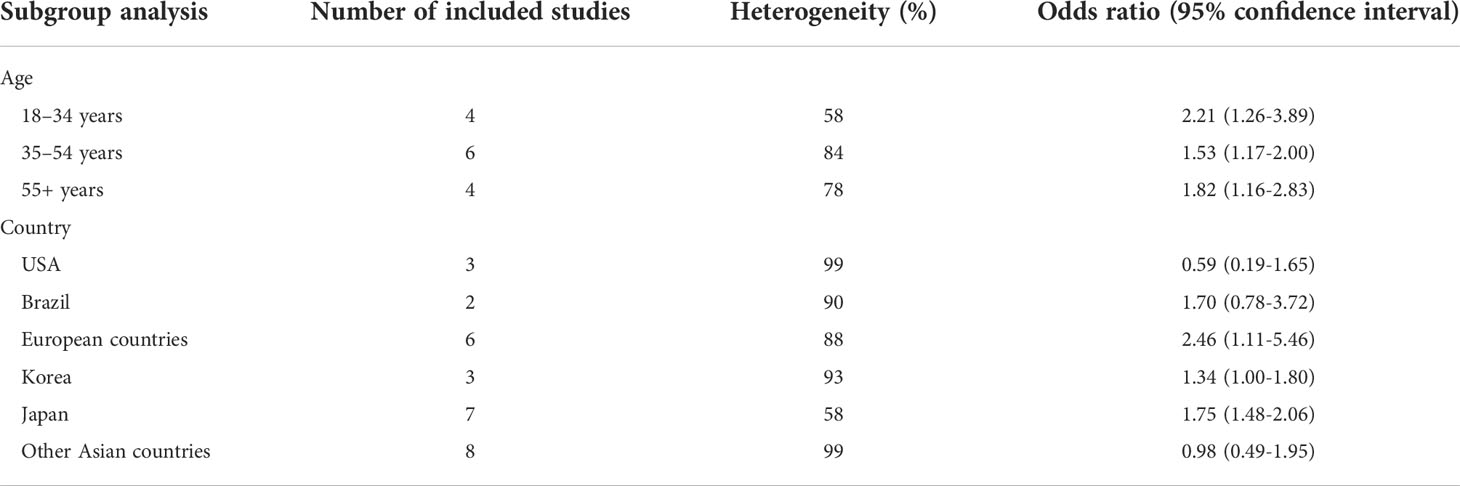
Table 2 Subgroup analysis stratified by age and country.
To evaluate the association by country, we classified the patients into country groups (European countries, USA, Brazil, Korea, Japan, and other Asian countries) and compared their results (Table 2). The largest OR was noted in European countries 2.46 (1.11-5.46). The OR was 0.59 (0.19-1.65) in the USA and 1.70 (0.78-3.72) in Brazil. The odds ratio was 1.34 (1.00-1.80) in Korea, 1.75 (1.48-2.06) in Japan, and 0.98 (0.49-1.95) in other Asian countries.
We assessed the quality of the included studies using the Newcastle–Ottawa scale. Of the 29 cross-sectional studies, 21 were evaluated as ‘very good’ and 8 were evaluated as ‘good’ (Supplementary Table 4). Of the 4 cohort studies, 3 were evaluated as ‘good’ and 1 as ‘fair’ (Supplementary Table 5). Of the 4 case-control studies, 3 were evaluated as ‘good’ and 1 as ‘fair’ (Supplementary Table 6).
A funnel plot for the overall obesity-periodontitis association is shown in Figure 3. Egger’s regression test revealed no significant publication bias (p = 0.871).
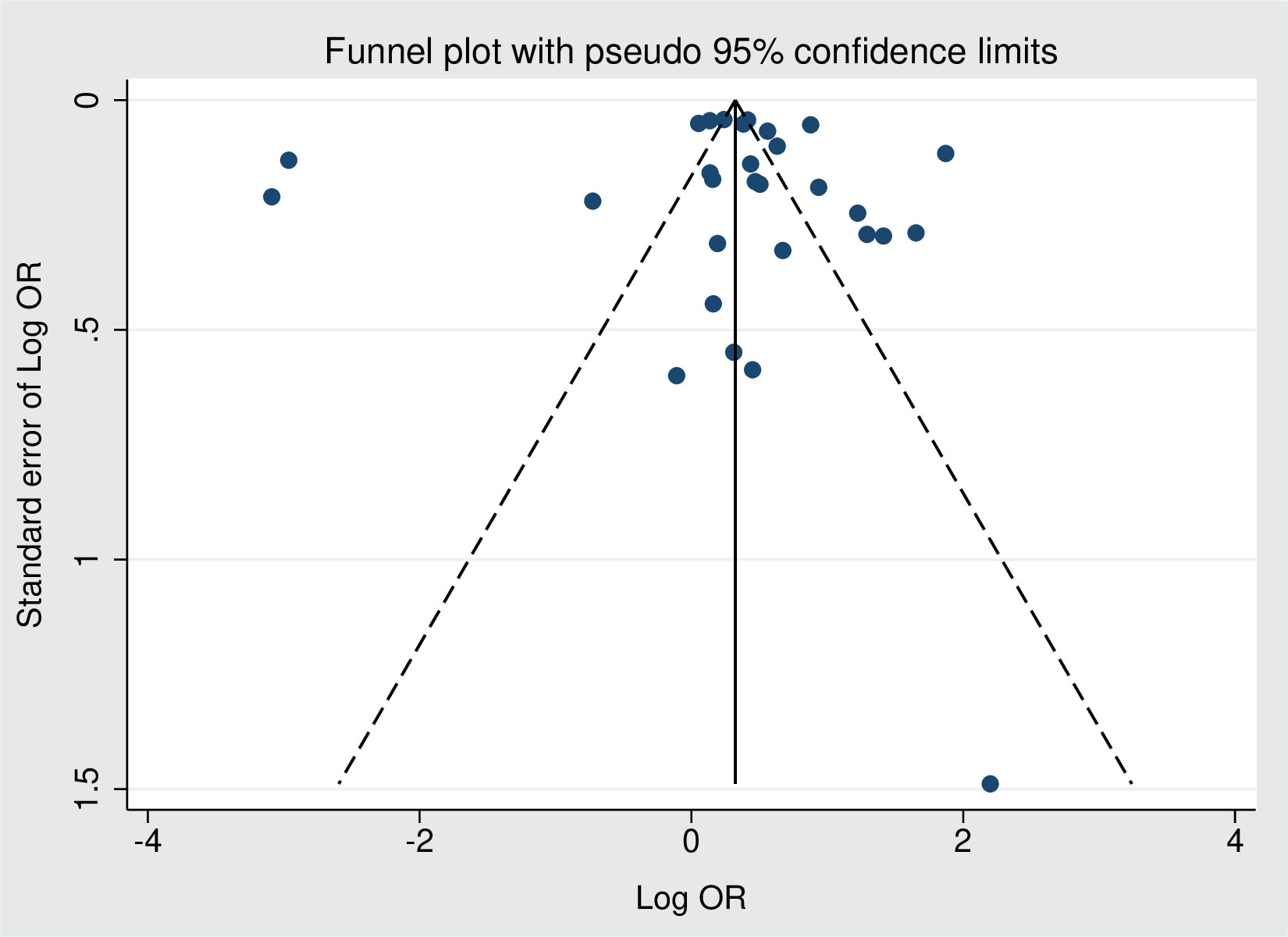
Figure 3 Funnel plot for the risk of periodontitis for obesity group compared to non-obesity group.
The strength of evidence for 8 domains was rated individually for the primary outcome. The quality of evidence was low according to the GRADE approach (Table 3).
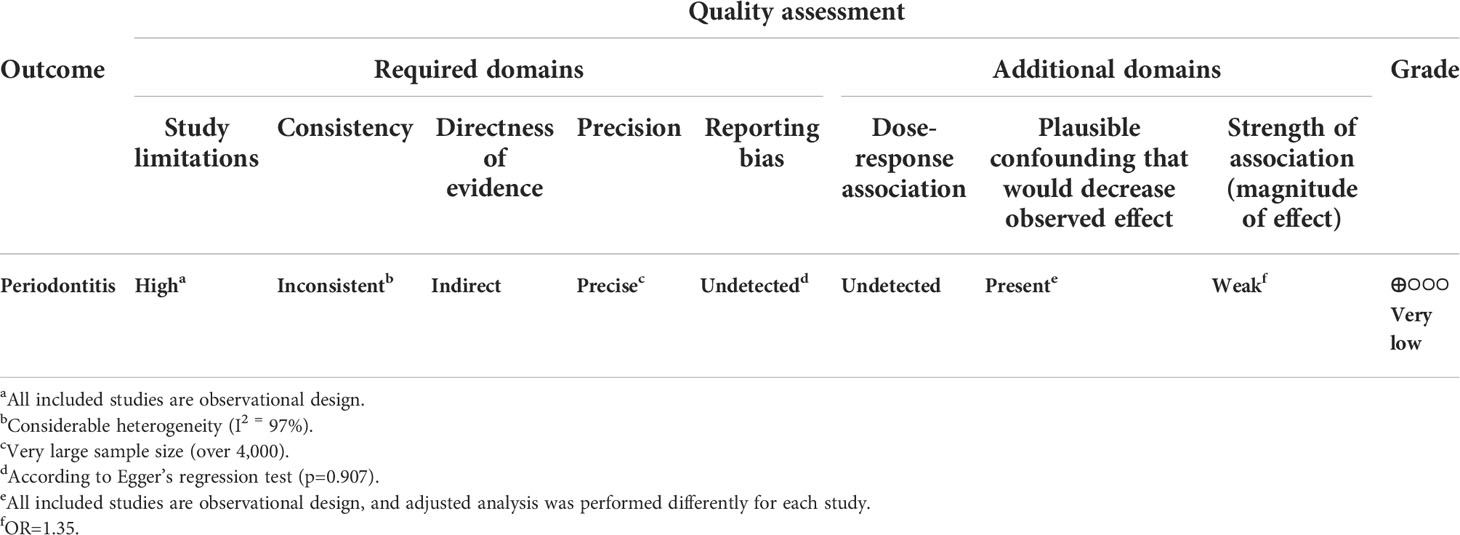
Table 3 GRADE approach for the primary outcome.
This systematic review and meta-analysis provided strong evidence to support the positive association between obesity and periodontitis. Among the 29 studies, 17 studies showed a significant increased odds ratio of periodontitis in the obesity group. Nine studies showed not statistically significant results, and 3 studies showed statistically decreased odds ratio.
As periodontitis progresses differently by age, it is necessary to focus on its association with age (65). The OR of the 18–34 years group was 2.21 (1.26–3.89), which showed the highest association between obesity and periodontitis. Young people have better oral health than other age groups (66). Thus, they have fewer risk factors for periodontitis, and the impact of each risk factor is higher. Therefore, periodontitis is greatly affected by obesity, a risk factor in a large proportion of young people. The OR of the 35–54 years group was 1.53 (1.17–2.00) and 55+ years group was 1.82 (1.16–2.83). This is an expected result indicating that elderly individuals are more vulnerable to periodontitis than middle-aged individuals. Therefore, they are vulnerable to the effects of obesity (67). In conclusion, both elderly and young people showed a significant correlation between obesity and periodontitis. Why is the OR value for young people noticeably high? Young people with few other periodontitis risk factors are largely affected by obesity. In addition, especially vulnerable groups (e.g., autism spectrum disorder) among young people may be more susceptible to oral pathogens due to poor oral hygiene management and preference for cariogenic foods (68, 69). Therefore, constant weight management and inspection are needed to maintain the periodontal health of young people.
Compared to the overall OR in the present study, European countries had highest OR among all countries. High odds ratio observed in European countries also could be explained by several factors. According to Nazir et al. (70), the high prevalence of periodontal disease in European countries may be attributed to the high proportion of older population and easy access to medical institutions (70). Japan had a high OR among Asian countries. This might be partially explained by the Japanese medical system. Because Japan has universal health insurance systems, the economic barrier to dental care would be low (71). In addition, the coverage and amount of cost are wider than Korea, which has similar universal health insurance systems (71). Therefore, it was thought that high odds ratio would be observed because the accessibility of dental care may be higher than other countries when periodontitis occurs.
Our study has several limitations. It is difficult to identify a causal relationship between obesity and periodontitis because all included study designs were observational. There were differences in the definition of obesity and periodontitis in each study, which may lead to selection bias. No adjustment was performed for potential confounders such as diabetes, diet, and smoking habit. The true value could be distorted by these confounding factors, and there is a possibility of toward null or away from null depending on the nature of the confounder (72). The search was performed using only the Embase and Medline databases. Nevertheless, it is thought that this meta-analysis has the advantage of updating the latest studies to increase external validity and drawing more precise conclusions through subgroup analysis.
European countries and Japan showed a significant positive association, and the USA, Brazil, and other Asian countries showed insignificant association. A positive association was found regardless of age. Therefore, medical professionals should try to prevent periodontitis by controlling patient weights, and more studies should be conducted to determine the association between obesity and oral health.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
CK: Methodology, Investigation, Formal analysis, Data curation, Writing – Original draft preparation. SL: Methodology, Investigation, Formal analysis, Data curation, Writing – Original draft preparation. WH: Methodology, Investigation, Formal analysis, Data curation, Writing – Original draft preparation. ES: Software, Visualization, Supervision. TK: Software, Visualization, Supervision. KK Conceptualization, Visualization, Project Administration, Writing – Reviewing and Editing, Supervision. YK: Conceptualization, Visualization, Project Administration, Funding acquisition, Writing – Reviewing and Editing, Supervision. All authors contributed to the article and approved the submitted version.
This work was supported by the Medical Research Center (MRC) program [grant number NRF-2018R1A5A2023879] and the Basic Science Research Program [grant number NRF-2020R1C1C1003741], and the Ministry of Health & Welfare, Republic of Korea (HI22C1377).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.999455/full#supplementary-material
AHRQ, Agency for Healthcare Research and Quality; BMI, body mass index; CIs, confidence intervals; OR, Odds ratio.
1. Bluher M. Obesity: Global epidemiology and pathogenesis. Nat Rev Endocrinol (2019) 15:288–98. doi: 10.1038/s41574-019-0176-8
2. Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism (2019) 92:6–10. doi: 10.1016/j.metabol.2018.09.005
4. Nicolucci A, Maffeis C. The adolescent with obesity: What perspectives for treatment? Ital J Of Pediatr (2022) 48:1–9. doi: 10.1186/s13052-022-01205-w
5. Dixon JB. The effect of obesity on health outcomes. Mol Cell Endocrinol (2010) 316:104–8. doi: 10.1016/j.mce.2009.07.008
6. Hlatky MA, Chung SC, Escobedo J, Hillegass WB, Melsop K, Rogers W, et al. The effect of obesity on quality of life in patients with diabetes and coronary artery disease. Am Heart J (2010) 159:292–300. doi: 10.1016/j.ahj.2009.11.004
7. Colditz GA, Peterson LL. Obesity and cancer: Evidence, impact, and future directions. Clin Chem (2018) 64:154–62. doi: 10.1373/clinchem.2017.277376
8. Zorena K, Jachimowicz-Duda O, Slezak D, Robakowska M, Mrugacz M. Adipokines and obesity. potential link to metabolic disorders and chronic complications. Int J Mol Sci (2020) 21. doi: 10.3390/ijms21103570
9. Yang J, Tian C, Chen Y, Zhu C, Chi H, Li J. Obesity aggravates covid-19: An updated systematic review and meta-analysis. J Med Virol (2021) 93:2662–74. doi: 10.1002/jmv.26677
10. Hamjane N, Benyahya F, Nourouti NG, Mechita MB, Barakat A. Cardiovascular diseases and metabolic abnormalities associated with obesity: What is the role of inflammatory responses? a systematic review. Microvascular Res (2020) 131:104023. doi: 10.1016/j.mvr.2020.104023
11. Tiburcio-Machado CS, Michelon C, Zanatta FB, Gomes MS, Marin JA, Bier CA. The global prevalence of apical periodontitis: A systematic review and meta-analysis. Int Endod J (2021) 54:712–35. doi: 10.1111/iej.13467
12. Eke PI, Thornton-Evans GO, Wei L, Borgnakke WS, Dye BA, Genco RJ. Periodontitis in us adults: National health and nutrition examination survey 2009-2014. J Am Dent Assoc (2018) 149:576–88.E6. doi: 10.1016/j.adaj.2018.04.023
13. Chen MX, Zhong YJ, Dong QQ, Wong HM, Wen YF. Global, regional, and national burden of severe periodontitis 1990-2019: An analysis of the global burden of disease study 2019. J Clin Periodontol (2021) 48:1165–88. doi: 10.1111/jcpe.13506
14. Moura-Grec PG, Marsicano JA, Carvalho CA, Sales-Peres SH. Obesity and periodontitis: Systematic review and meta-analysis. Cien Saude Colet (2014) 19:1763–72. doi: 10.1590/1413-81232014196.13482013
15. Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The prisma 2020 statement: An updated guideline for reporting systematic reviews. Int J Of Surg (2021) 88:105906. doi: 10.1016/j.ijsu.2021.105906
16. Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, et al. 2013 Aha/Acc/Tos guideline for the management of overweight and obesity in adults: A report of the American college of Cardiology/American heart association task force on practice guidelines and the obesity society. J Of Am Coll Of Cardiol (2014) 63:2985–3023. doi: 10.1016/j.jacc.2013.11.004
17. Goda A, Masuyama T. Obesity and overweight in Asian people. Circ J (2016) 80(12):2425–6. doi: 10.1253/circj.CJ-16-1087
18. Lean M, Han T, Morrison C. Waist circumference as a measure for indicating need for weight management. Bmj (1995) 311:158–61. doi: 10.1136/bmj.311.6998.158
19. Alberti KGM, Zimmet P, Shaw J. The metabolic syndrome–a new worldwide definition. Lancet (2005) 366:1059–62. doi: 10.1016/S0140-6736(05)67402-8
20. Maeng Y-J, Kim B-R, Jung H-I, Jung U-W, Kim HE, Kim B-I. Diagnostic accuracy of a combination of salivary hemoglobin levels, self-report questionnaires, and age in periodontitis screening. J Of Periodontal Implant Sci (2016) 46:10–21. doi: 10.5051/jpis.2016.46.1.10
21. Gomes-Filho I, Trindade S, Passos-Soares JDS, Figueiredo A, Vianna M, Hintz A, et al. Clinical diagnosis criteria for periodontal disease: An update. J Dent Health Oral Disord Ther (2018) 9:354–6. doi: 10.15406/jdhodt.2018.09.00408
22. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
23. Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa scale (Nos) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute (2011).
24. Herzog R, Álvarez-Pasquin MJ, Dïaz C, Del Barrio JL, Estrada JM, Gil Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? a systematic review. BMC Public Health (2013) 13:154. doi: 10.1186/1471-2458-13-154
25. Viswanathan M, Patnode CD, Berkman ND, Bass EB, Chang S, Hartling L, et al. Assessing the risk of bias in systematic reviews of health care interventions. methods guide for effectiveness and comparative effectiveness reviews. (2017). https://www.ncbi.nlm.nih.gov/books/NBK91433/pdf/Bookshelf_NBK91433.pdf
26. Berkman ND, Lohr KN, Ansari M, Mcdonagh M, Balk E, Whitlock E, et al. Grading the strength of a body of evidence when assessing health care interventions: An EPC update. J Clin Epidemiol (2014) 68(11):1312–24. doi: 10.1016/j.jclinepi.2014.11.023
27. Schþnemann H, Brożek J, Guyatt G, Oxman A eds. Handbook for grading the quality of evidence and the strength of recommendations using the grade approach. updated octobe (2013). https://gdt.gradepro.org/app/handbook/handbook.html
28. Al-Zahrani MS, Bissada NF, Borawskit EA. Obesity and periodontal disease in young, middle-aged, and older adults. J Periodontol (2003) 74:610–5. doi: 10.1902/jop.2003.74.5.610
29. Benguigui C, Bongard V, Ruidavets JB, Sixou M, Chamontin B, Ferrieres J, et al. Evaluation of oral health related to body mass index. Oral Dis (2012) 18:748–55. doi: 10.1111/j.1601-0825.2012.01940.x
30. Borges-Yanez SA, Irigoyen-Camacho ME, Maupome G. Risk factors and prevalence of periodontitis in community-dwelling elders in Mexico. J Clin Periodontol (2006) 33:184–94. doi: 10.1111/j.1600-051X.2006.00897.x
31. Chen TP, Yu HC, Lin TH, Wang YH, Chang YC. Association between obesity and chronic periodontitis: A nationwide population-based cohort study in Taiwan. Medicine (2021) 100:E27506. doi: 10.1097/MD.0000000000027506
32. D'aiuto F, Sabbah W, Netuveli G, Donos N, Hingorani AD, Deanfield J, et al. Association of the metabolic syndrome with severe periodontitis in a Large U.S. population-based survey. J Clin Endocrinol Metab (2008) 93:3989–94. doi: 10.1210/jc.2007-2522
33. Dalla Vecchia CF, Susin C, Rosing CK, Oppermann RV, Albandar JM. Overweight and obesity as risk indicators for periodontitis in adults. J Periodontol (2005) 76:1721–8. doi: 10.1902/jop.2005.76.10.1721
34. Dumitrescu AL, Kawamura M. Involvement of psychosocial factors in the association of obesity with periodontitis. J Oral Sci (2010) 52:115–24. doi: 10.2334/josnusd.52.115
35. Ekuni D, Yamamoto T, Koyama R, Tsuneishi M, Naito K, Tobe K. Relationship between body mass index and periodontitis in young Japanese adults. J Periodontal Res (2008) 43:417–21. doi: 10.1111/j.1600-0765.2007.01063.x
36. Furuta M, Ekuni D, Yamamoto T, Irie K, Koyama R, Sanbe T, et al. Relationship between periodontitis and hepatic abnormalities in young adults. Acta Odontol Scand (2010) 68:27–33. doi: 10.3109/00016350903291913
37. Goulart AC, Armani F, Arap AM, Nejm T, Andrade JB, Bufarah HB, et al. Relationship between periodontal disease and cardiovascular risk factors among young and middle-aged brazilians. cross-sectional study. Sao Paulo Med J (2017) 135:226–33. doi: 10.1590/1516-3180.2016.0357300117
38. Al Habashneh R, Azar W, Shaweesh A, Khader Y. The relationship between body mass index and periodontitis among postmenopausal women. Obes Res Clin Pract (2016) 10:15–23. doi: 10.1016/j.orcp.2015.03.010
39. Haffajee AD, Socransky SS. Relation of body mass index, periodontitis and tannerella forsythia. J Clin Periodontol (2009) 36:89–99. doi: 10.1111/j.1600-051X.2008.01356.x
40. Han DH, Lim SY, Sun BC, Paek DM, Kim HD. Visceral fat area-defined obesity and periodontitis among koreans. J Clin Periodontol (2010) 37:172–9. doi: 10.1111/j.1600-051X.2009.01515.x
41. Ikbariyeh B, Al Habashneh R, Khassawneh B, Alrawashdeh M, Elsalem L, Al-Nusair J. Clinical and biological indicators of periodontal disease in obese and non-obese adults with and without bronchial asthma. J Asthma (2021) 59(9):1–9. doi: 10.1080/02770903.2021
42. Katagiri S, Nitta H, Nagasawa T, Izumi Y, Kanazawa M, Matsuo A, et al. High prevalence of periodontitis in non-elderly obese Japanese adults. Obes Res Clin Pract (2010) 4:E247–342. doi: 10.1016/j.orcp.2010.08.005
43. Khader YS, Bawadi HA, Haroun TF, Alomari M, Tayyem RF. The association between periodontal disease and obesity among adults in Jordan. J Clin Periodontol (2009) 36:18–24. doi: 10.1111/j.1600-051X.2008.01345.x
44. Kim YS, Kim JH. Body mass index and oral health status in Korean adults: The fifth Korea national health and nutrition examination survey. Int J Dent Hyg (2017) 15:172–8. doi: 10.1111/idh.12207
45. Kitagawa M, Kurahashi T, Matsukubo T. Relationship between general health, lifestyle, oral health, and periodontal disease in adults: A Large cross-sectional study in Japan. Bull Tokyo Dent Coll (2017) 58:1–8. doi: 10.2209/tdcpublication.2016-2100
46. Kongstad J, Hvidtfeldt UA, Gronbaek M, Stoltze K, Holmstrup P. The relationship between body mass index and periodontitis in the Copenhagen city heart study. J Periodontol (2009) 80:1246–53. doi: 10.1902/jop.2009.080559
47. Kumar S, Dagli RJ, Dhanni C, Duraiswamy P. Relationship of body mass index with periodontal health status of green marble mine laborers in kesariyaji, India. Braz Oral Res (2009) 23:365–9. doi: 10.1590/S1806-83242009000400003
48. Kushiyama M, Shimazaki Y, Yamashita Y. Relationship between metabolic syndrome and periodontal disease in Japanese adults. J Periodontol (2009) 80:1610–5. doi: 10.1902/jop.2009.090218
49. Lee JH, Oh JY, Youk TM, Jeong SN, Kim YT, Choi SH. Association between periodontal disease and non-communicable diseases: A 12-year longitudinal health-examinee cohort study in south Korea. Medicine (2017) 96:E7398. doi: 10.1097/MD.0000000000007398
50. Li P, He L, Sha YQ, Luan QX. Relationship of metabolic syndrome to chronic periodontitis. J Periodontol (2009) 80:541–9. doi: 10.1902/jop.2009.080387
51. Machado AC, Quirino MR, Nascimento LF. Relation between chronic periodontal disease and plasmatic levels of triglycerides, total cholesterol and fractions. Braz Oral Res (2005) 19:284–9. doi: 10.1590/S1806-83242005000400009
52. Marro F, De Smedt S, Rajasekharan S, Martens L, Bottenberg P, Jacquet W. Associations between obesity, dental caries, erosive tooth Wear and periodontal disease in adolescents: A case-control study. Eur Arch Paediatr Dent (2021) 22:99–108. doi: 10.1007/s40368-020-00534-w
53. Martinez-Herrera M, Silvestre FJ, Silvestre-Rangil J, Banuls C, Rocha M, Hernandez-Mijares A. Involvement of insulin resistance in normoglycaemic obese patients with periodontitis: A cross-sectional study. J Clin Periodontol (2017) 44:981–8. doi: 10.1111/jcpe.12773
54. Morita T, Ogawa Y, Takada K, Nishinoue N, Sasaki Y, Motohashi M, et al. Association between periodontal disease and metabolic syndrome. J Public Health Dent (2009) 69:248–53. doi: 10.1111/j.1752-7325.2009.00130.x
55. Morita T, Yamazaki Y, Seto M, Yamamoto T, Nakai K, Tanaka H, et al. Effect of periodontitis and toothbrushing frequency on obesity onset: A cohort study. Med Sci Monit (2019) 25:9712–20. doi: 10.12659/MSM.917356
56. Pataro AL, Costa FO, Cortelli SC, Cortelli JR, Abreu MH, Costa JE. Association between severity of body mass index and periodontal condition in women. Clin Oral Investig (2012) 16:727–34. doi: 10.1007/s00784-011-0554-7
57. Pham TAV, Kieu TQ, Ngo LTQ. Risk factors of periodontal disease in Vietnamese patients. J Investig Clin Dent (2018) 9:1631–6. doi: 10.1111/jicd.12272
58. Saito T, Shimazaki Y, Koga T, Tsuzuki M, Ohshima A. Relationship between upper body obesity and periodontitis. J Dent Res (2001) 80:1631–6. doi: 10.1177/00220345010800070701
59. Saito T. Obesity may be associated with periodontitis in elderly men. J Evid Based Dent Pract (2008) 8:97–8. doi: 10.1016/j.jebdp.2008.03.015
60. Saxlin T, Ylostalo P, Suominen-Taipale L, Aromaa A, Knuuttila M. Overweight and obesity weakly predict the development of periodontal infection. J Clin Periodontol (2010) 37:1059–67. doi: 10.1111/j.1600-051X.2010.01633.x
61. Shimazaki Y, Egami Y, Matsubara T, Koike G, Akifusa S, Jingu S, et al. Relationship between obesity and physical fitness and periodontitis. J Periodontol (2010) 81:1124–31. doi: 10.1902/jop.2010.100017
62. Sonoda C, Fukuda H, Kitamura M, Hayashida H, Kawashita Y, Furugen R, et al. Associations among obesity, eating speed, and oral health. Obes Facts (2018) 11:165–75. doi: 10.1159/000488533
63. Torrungruang K, Tamsailom S, Rojanasomsith K, Sutdhibhisal S, Nisapakultorn K, Vanichjakvong O, et al. Risk indicators of periodontal disease in older Thai adults. J Periodontol (2005) 76:558–65. doi: 10.1902/jop.2005.76.4.558
64. Wang TT, Chen TH, Wang PE, Lai H, Lo MT, Chen PY, et al. A population-based study on the association between type 2 diabetes and periodontal disease in 12,123 middle-aged Taiwanese (Kcis no. 21). J Clin Periodontol (2009) 36:372–9. doi: 10.1111/j.1600-051X.2009.01386.x
65. Burt BA. Periodontitis and aging: Reviewing recent evidence. J Am Dent Assoc (1994) 125:273–9. doi: 10.14219/jada.archive.1994.0034
66. Oh TJ, Eber R, Wang HL. Periodontal diseases in the child and adolescent. J Clin Periodontol (2002) 29:400–10. doi: 10.1034/j.1600-051X.2002.290504.x
67. Clark D, Kotronia E, Ramsay SE. Frailty, aging, and periodontal disease: Basic biologic considerations. Periodontol 2000 (2021) 87:143–56. doi: 10.1111/prd.12380
68. Pagano S, Lombardo G, Coniglio M, Donnari S, Canonico V, Antonini C, et al. Autism spectrum disorder and paediatric dentistry: A narrative overview of intervention strategy and introduction of an innovative technological intervention method. Eur J Of Paediatric Dentistry (2022) 23:54–60. doi: 10.23804/ejpd.2022.23.01.10
69. Carli E, Pasini M, Pardossi F, Capotosti I, Narzisi A, Lardani L. Oral health preventive program in patients with autism spectrum disorder. Children (2022) 9:535. doi: 10.3390/children9040535
70. Nazir M, Al-Ansari A, Al-Khalifa K, Alhareky M, Gaffar B, Almas K. Global prevalence of periodontal disease and lack of its surveillance. Sci World J (2020) 2020. doi: 10.1155/2020/2146160
71. Furuta M, Takeuchi K, Shimazaki Y, Takeshita T, Shibata Y, Hata J, et al. Comparison of the periodontal condition in Korean and Japanese adults: A cross-sectional study. BMJ Open (2018) 8:Bmjopen–2018-024332. doi: 10.1136/bmjopen-2018-024332
Keywords: obesity, periodontitis, observational study, systematic review, meta-analysis
Citation: Kim CM, Lee S, Hwang W, Son E, Kim TW, Kim K and Kim YH (2022) Obesity and periodontitis: A systematic review and updated meta-analysis. Front. Endocrinol. 13:999455. doi: 10.3389/fendo.2022.999455
Received: 21 July 2022; Accepted: 10 October 2022;
Published: 24 October 2022.
Edited by:
Bert B. Little, University of Louisville, United StatesReviewed by:
Stefano Pagano, University of Perugia, ItalyCopyright © 2022 Kim, Lee, Hwang, Son, Kim, Kim and Kim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kihun Kim, a2lodW43NjAzQG5hdmVyLmNvbQ==; Yun Hak Kim, eXVuaGFrMTA1MTBAcHVzYW4uYWMua3I=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.