
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 24 August 2022
Sec. Translational and Clinical Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.945626
This article is part of the Research TopicMetabolic-Associated Fatty Liver Disease (MAFLD): Overcoming the Storm through Multidisciplinary CollaborationView all 5 articles
 Juan Bañares1†Ramiro Manzano-Nuñez1†Alba Prió1
Juan Bañares1†Ramiro Manzano-Nuñez1†Alba Prió1 Jesús Rivera-Esteban1,2Laura Camps-Relats1Ana Villarejo1Lourdes Ruiz-Ortega1Mònica Pons1,3
Jesús Rivera-Esteban1,2Laura Camps-Relats1Ana Villarejo1Lourdes Ruiz-Ortega1Mònica Pons1,3 Andreea Ciudin2,4,5*María Teresa Salcedo2,6
Andreea Ciudin2,4,5*María Teresa Salcedo2,6 Víctor Vargas1,2,3Joan Genescà1,2,3
Víctor Vargas1,2,3Joan Genescà1,2,3 Juan M. Pericàs1,3*
Juan M. Pericàs1,3*Introduction: Non-alcoholic fatty liver disease (NAFLD) is the most prevalent chronic liver disease in developed countries, with its incidence growing parallel to the epidemics of obesity and type 2 diabetes mellitus (T2DM). Sodium-glucose co-transporter-2 inhibitors (SGLT2i) are becoming a cornerstone in the management of cardiovascular health and some studies suggest the potential role in NAFLD. However, patients under treatment with SGLT2i are at risk of developing genitourinary fungal infections (GFIs). Moreover, both NAFLD and SGLT2i have a strong influence on the immune system, and therefore the risk of infections other than GFIs could be increased in NAFLD patients treated with SGLT2i. We aimed to examine the possible association of SGLT2i with infections and hepatic outcomes in NAFLD patients.
Methods: We conducted a case-control study including NAFLD patients with T2DM visited at the Liver Unit outpatient clinic from 2016 to 2021 with a minimum follow-up of 6 months by selecting 65 patients receiving SGLT2i and 130 matched patients with other types of antidiabetic treatment.
Results: During follow-up, GFIs were significantly higher in the SGLT2i group (15.4% vs. 3.8%; p=0.008), whereas there were no differences in the occurrence of overall infections (41.5% vs. 30%; p=0.1) nor in other types of specific infections. In the multivariable analysis, treatment with SGLT2i was not independently associated with higher odds of overall infection. On the other hand, SGLT2i patients showed a significantly lower incidence of hepatic events (1.5% vs. 10.7%; p=0.02). There were no significant different in all-cause mortality between cases and controls.
Conclusions: NAFLD patients with T2DM receiving SGLT2i more frequently presented GFIs, whereas the incidence of other types of infections was not found to be higher than in other patients with NAFLD and T2DM treated with other drugs. Moreover, SGLT2i-treated patients had a lower occurrence of hepatic events. Further studies are warranted to validate our data.
Non-alcoholic fatty liver disease (NAFLD) encompasses a progressive clinical spectrum: from simple steatosis, through inflammation [i.e., non-alcoholic steatohepatitis (NASH)] and fibrosis, to liver cirrhosis (1, 2). From an epidemiological standpoint, parallel to the growing epidemic of obesity and type 2 diabetes mellitus (T2DM), NAFLD has emerged as the most prevalent liver disease in the US and probably will become the leading cause of liver transplantation in the upcoming years (3). It is estimated that 25% of general population in Western countries to have NAFLD, but this prevalence increases up to 60-80% in patients with obesity or T2DM and can reach 80-100% when both risk factors are present (2, 3). In addition, it is estimated that 20-30% of patients with NAFLD will progress to liver inflammation and fibrosis (2–4).
NAFLD is considered the liver manifestation of metabolic syndrome, both sharing multiple pathophysiological mechanisms such as insulin resistance (1–3). Moreover, improvements in metabolic factors such as weight loss, are associated with amelioration in inflammation and liver fibrosis (1). Sodium-glucose co-transporter-2 inhibitors (SGLT2i) are now solidly established amongst the armamentarium to improve metabolic status and cardiovascular health in T2DM, chronic kidney disease and cardiovascular diseases (5, 6). Emerging data suggest that SGLT2i may play a role in treating NAFLD being associated with an impact in the metabolic status, including reduction in liver fat content and even histologic improvement in liver steatosis and fibrosis (7–10). Such effects could have a clinically relevant impact on the outcomes of patients with T2DM and NAFLD, making SGLT2i an attractive therapeutic alternative. Even though there are currently several clinical trials underway assessing their efficacy to treat NAFLD (11, 12), there is insufficient information regarding an impact in clinical practice.
SGLT2i inhibit glucose reabsorption in the kidney via inhibition of the SGLT channels primarily located in the proximal tubules, promoting glycosuria, which has been associated with a higher incidence of urinary and genital infections, mainly caused by fungi, with odds ratios ranging approximately from 3 to 5 (13–17). Moreover, patients with T2DM have increased susceptibility to a wide array of infections due to variable degrees of baseline immunosuppression caused by complex mechanisms that are tightly intertwined with pathways leading to the enhanced systemic inflammation and immune system dysfunction characteristic of advanced liver disease, while obesity and NAFLD may also increase infection susceptibility (1, 18, 19). However, no studies have investigated whether T2DM patients with NAFLD treated with SGLT2i present increased rates of infections and particularly genitourinary fungal infections (GFIs).
The present study aimed to examine the impact of SGLT2i treatment in the incidence of infections in patients with NAFLD and T2DM. In addition, we aimed to investigate whether NAFLD patients treated with SGLT2i presented significant differences in liver outcomes compared to those not receiving SGLT2i.
Case-control study conducted at the Vall d’Hebron University Hospital (VHUH), a tertiary care setting with 1,300 beds in Barcelona, Spain.
An ongoing prospective cohort study on NAFLD was used to identify patients considered eligible to be included in the present case-control study. The ongoing prospective cohort study includes consecutive patients from the VHUH NAFLD outpatient clinics diagnosed with NAFLD and T2DM from 2016 to 2021. Patients with a diagnosis of both NAFLD and T2DM were considered eligible for inclusion. Patients with NAFLD and T2DM receiving treatment with SGLT2i and with a minimum of 6 months of follow-up were identified and defined as cases. NAFLD and T2DM patients receiving other antidiabetic drug different than SGLT2i were considered as potential controls (see flowchart in Figure 1). Matching variables were sex and age (+/- 3 years).
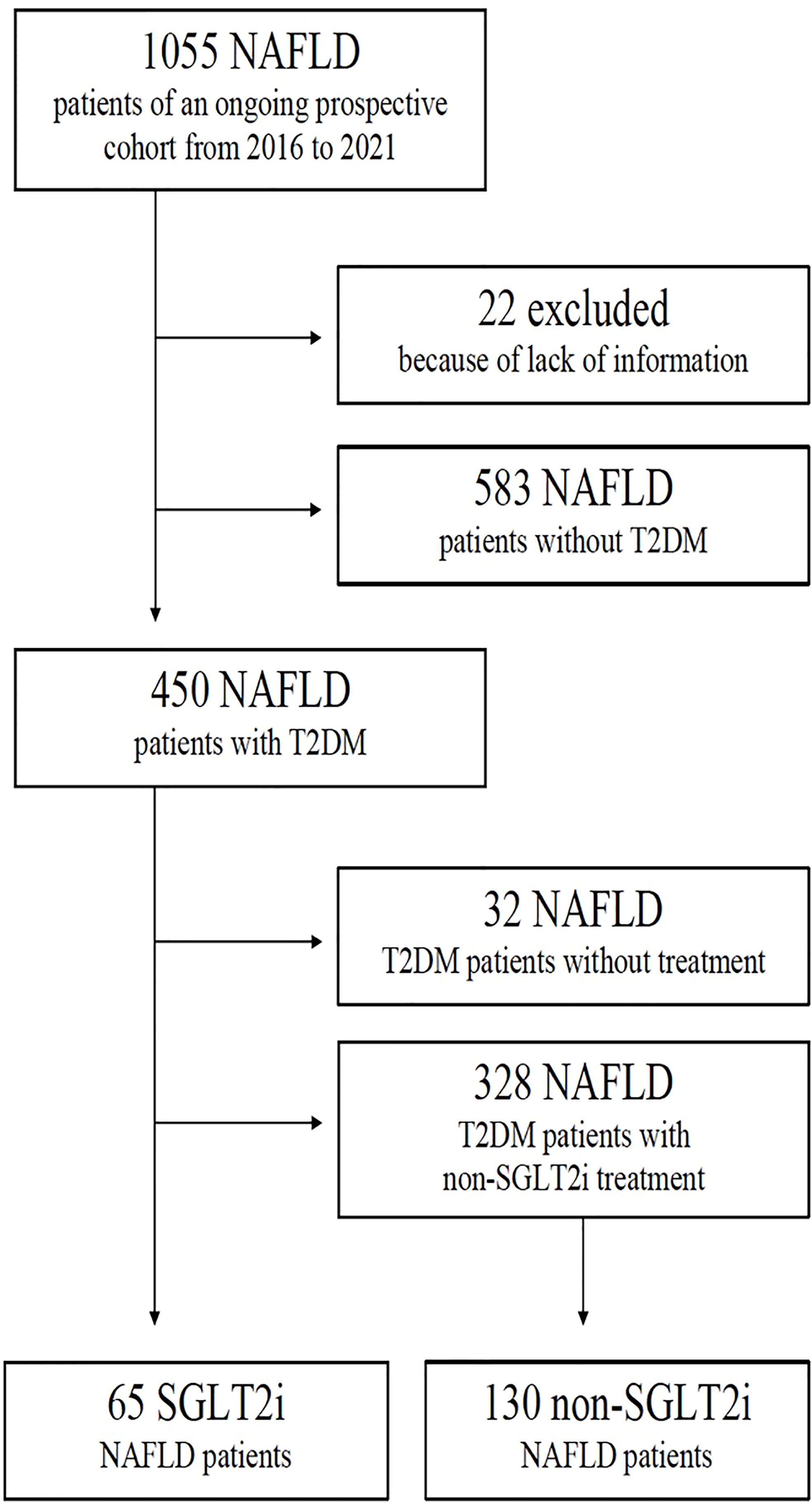
Figure 1 Patients’ disposition flowchart.
We excluded patients with Child B and C cirrhosis from the analysis to avoid bias in the allocation of SGLT2i treatment, as we considered that patients with more severe liver disease were less likely to receive treatment with SGLT2i because these are not widely recommended in patients with moderate-severe hepatic insufficiency, and also because patients with advanced chronic liver disease are at higher risk of infections and these might trigger hepatic events.
The occurrence of any type of infection was considered as the primary outcome of interest. Secondary outcomes included the occurrence of each type of infection separately, the occurrence of hepatic events (only the first episode accounted for each patient), and all-cause mortality.
The diagnostic criteria for NAFLD and T2DM are described elsewhere (1, 20). Briefly, NAFLD was diagnosed either based on steatosis in abdominal ultrasound or transient elastography and the presence of at least one feature of metabolic syndrome or by liver biopsy. T2DM was diagnosed following current clinical practice recommendations from the American Diabetes Association (20). Cirrhosis was defined by histological analysis when available and/or by a combination of clinical, analytical, liver stiffness measurement, endoscopic assessment and/or radiological evidence of advanced chronic liver disease. Hepatic events were defined as the presence of ascites, hepatic encephalopathy, and upper gastrointestinal bleeding. Infections were defined as urogenital fungal infections, urogenital bacterial infections, bacteremia, upper and lower respiratory tract infections, COVID-19, intra-abdominal, skin and soft tissues infections, and spontaneous bacterial peritonitis. Infections were diagnosed in a real clinical setting by means of clinical presentation and, when needed, radiological, laboratory and microbiological analysis.
The study protocol was approved by the VHUH Ethics Committee for Clinical Research (protocol code: PR(AG)222/2021) and conformed to the ethical guidelines of the 1975 Declaration of Helsinki.
Data were collected into a pre-specified and de-identified database in electronic format. Categorical variables were presented as frequencies and percentages. Continuous variables were expressed as means with standard deviation or medians with interquartile ranges as appropriate according to data distribution. Categorical variables were compared with Chi square test or Fisher exact test where appropriate. Continuous variables were compared using T test or nonparametric tests when necessary. A multivariate logistic regression analysis adjusted by relevant covariates was used to examine the association between SGLT2i use and the occurrence of infections. Findings were presented as odds ratios (OR) with 95% confidence intervals. Kaplan-Meier survival curves and long-rank test were calculated for the occurrence of overall infections and hepatic events along time. All analyses were performed in STATA statistical software.
The flowchart of patients’ disposition is shown in Figure 1.
After applying the inclusion and exclusion criteria, sixty-five patients with NAFLD and T2DM received SGLT2i and were considered as cases, whereas 130 diabetic patients with NAFLD not receiving SGLT2i were matched as controls. Characteristics of patients are shown in Table 1. Overall median follow-up was 34.4 months (IQR 17-48.3), with no significant differences found between cases and controls. There were neither differences regarding age, sex (matching variables), the prevalence of comorbidities, or the values of glycosylated hemoglobin, albumin, and liver enzymes between groups. Patients receiving SGLT2i had significantly higher BMI values and were more likely to present obesity.
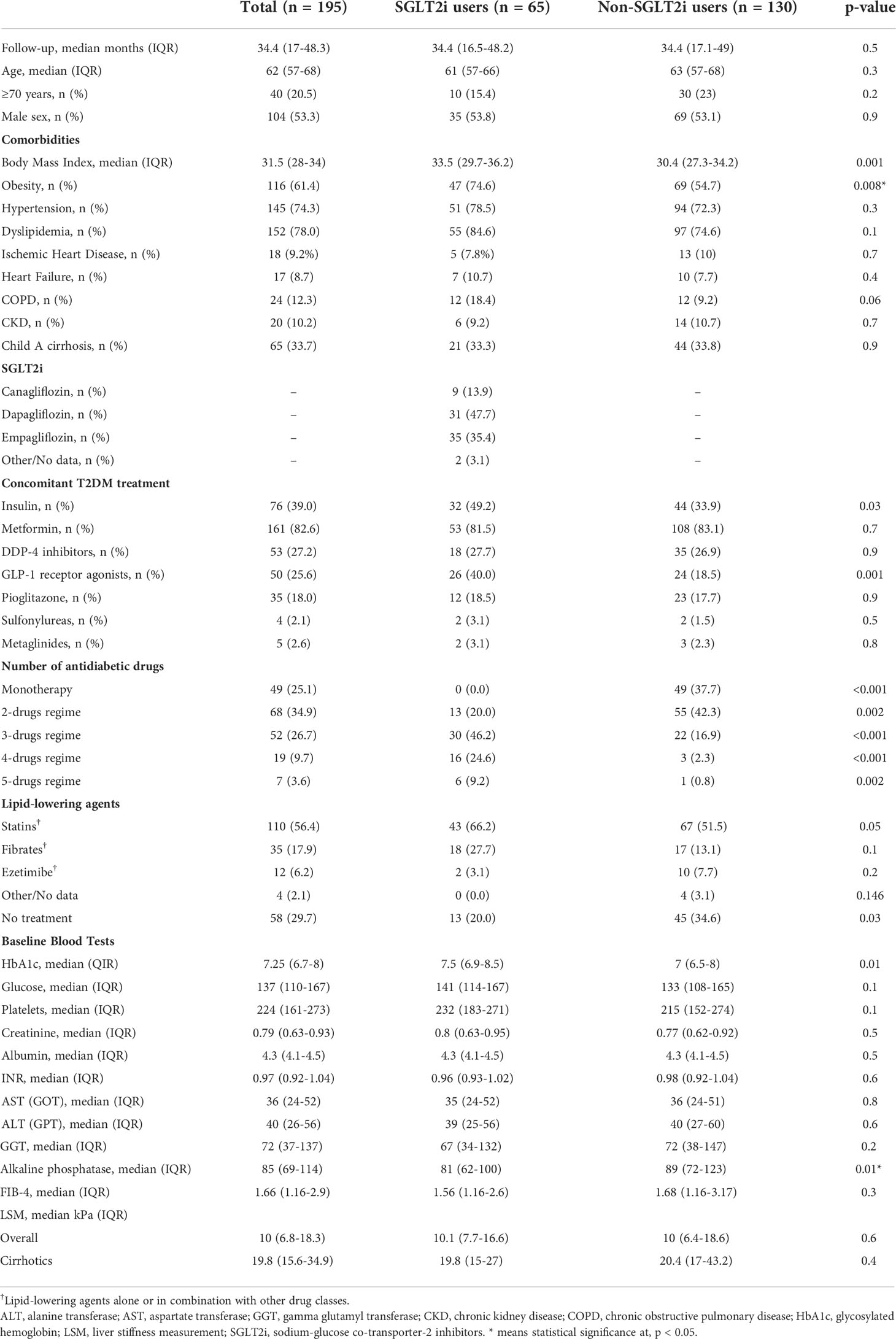
Table 1 Demographics and clinical characteristics of cases (SGLT2i users) and controls (non-SGLT2i users) in a cohort of patients with NAFLD and type 2 diabetes.
Outcomes’ information is outlined in Table 2. There were no significant differences in the occurrence of overall infections between groups (41.5% vs. 30%; p=0.1). With respect to the infection’s etiology, the proportion of patients presenting genital mycotic infections was significantly higher in patients receiving SGLT2i compared to those not receiving SGLT2i (15.4% vs. 3.8%; p=0.008), with incidence rates of 5.12 and 1.28 cases per 100 person-year in SGLT2i and non-SGLT2i groups, respectively (p<0.001). There were no significant differences in the proportion of the other types of infections between the two group of patients, including urinary tract infections of bacterial etiology (10.7% vs. 7.7%, p=0.4).
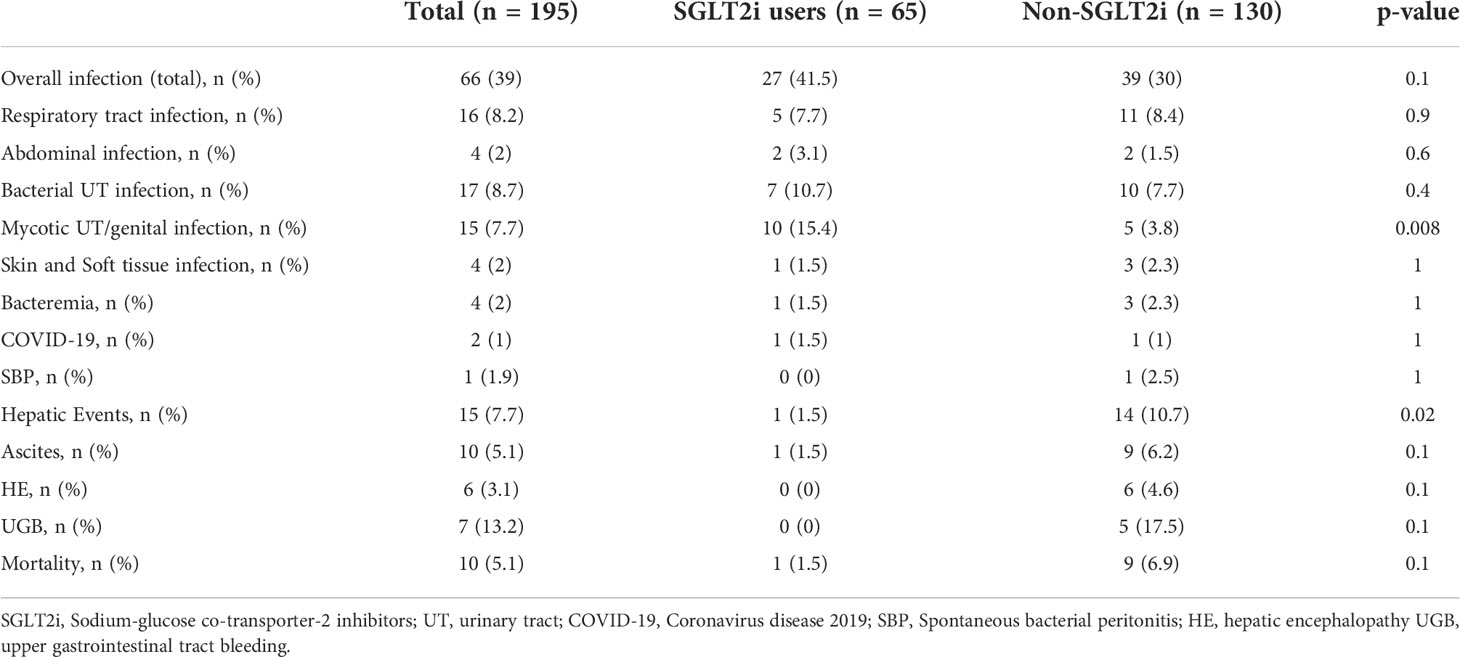
Table 2 Outcomes in cases (SGLT2i users) and controls (non- SGLT2i users) in a cohort of patients with NAFLD and type 2 diabetes.
As shown in Table 3, multivariate logistic regression analysis showed no significant risk-adjusted odds of infections with the use of SGLT2i (OR 1.68, 95% CI 0.93-3.05; p=0.084).
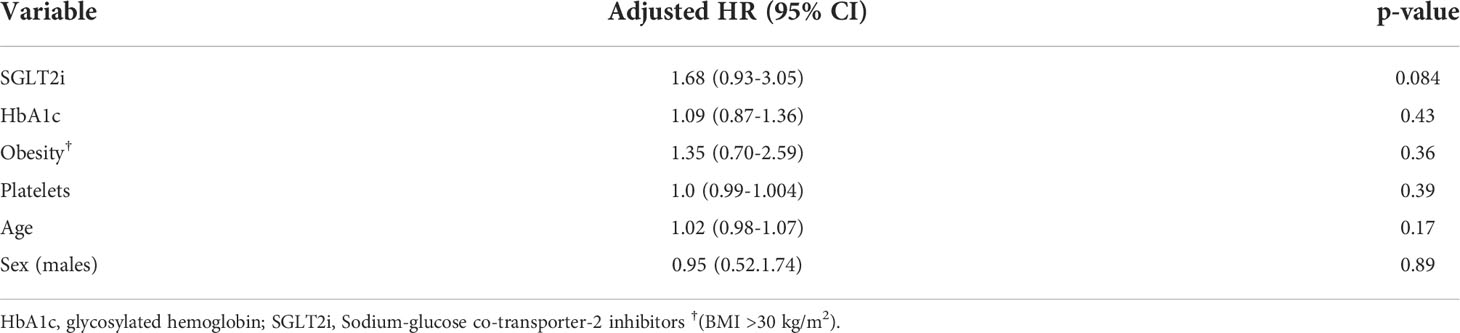
Table 3 Multivariate logistic regression analysis for risk of infection.
Kaplan-Meier survival curve on the occurrence of overall infections is shown in Figure 2A (log-rank test= 0.02).
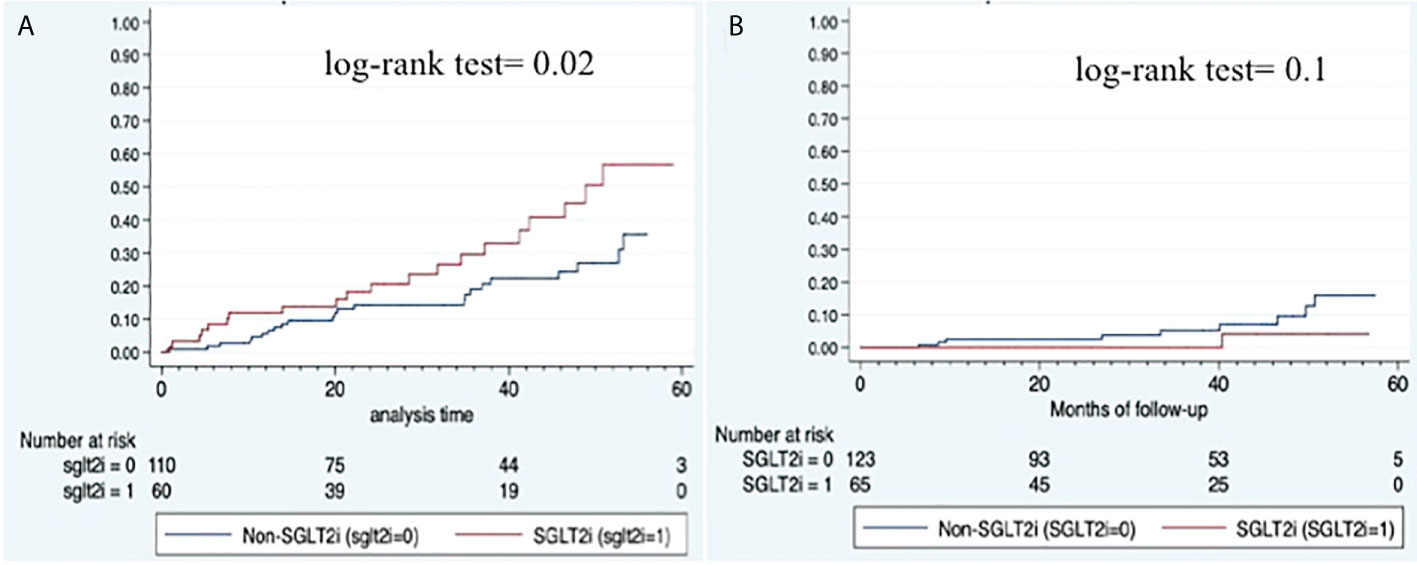
Figure 2 Kaplan-Meier survival curves. (A) Overall infections; (B) Hepatic events.
Overall, patient who received SGLT2i showed a significantly lower incidence of hepatic events (1.5% vs. 10.7%; p=0.02) although the proportion of cirrhosis was similar between groups. Each individual decompensating event was less frequent in SGLT2i treated patients (Table 2) although the difference did not reach statistical significance. Figure 2B shows the Kaplan-Meier curve for hepatic events (log-rank test= 0.1).
No significant differences in overall mortality [1.5% vs 6.9%; p=0.1] were observed between groups. Out-of-hospital cardiac arrest was the cause of death of the only patient who died in the SGLT2i group. In the non-SGLT2i group 5 patients died because of an infection (two of them of COVID-19) and one as a direct complication of hepatocellular carcinoma. The other three died of cardiac arrest, extrahepatic cancer and a motor vehicle collision.
In this study we aimed at examining the frequency of infections and hepatic events in patients with NAFLD and T2DM treated with SGLT2i as compared to patients treated with other antidiabetic agents. Although we did not find a significantly higher rate of overall infections in patients treated with SGLT2i, we described for the first time that genitourinary fungal infections are also more frequent in T2DM patients with NAFLD treated with SGLT2i. Moreover, we found that SGLT2i-treated patients had lower rates of hepatic events during the follow-up time included in the study.
Despite there were no significant differences in the occurrence of overall infectious episodes among SGLT2i patients, these were more likely to present genitourinary fungal infections (GFIs). In the general population, the incidence of GFIs has been estimated to be approximately 1-2% (13). As previously reported across a large body of literature, through their glycosuric effect there is a higher risk of these types on infections in SGLT2i users, with rates between 3 to 8% (13, 15, 16). Several randomized controlled trials revealed a 3- to 4-fold increase for SGLT2i compared with placebo (14, 17), which led manufacturers to include GFIs as common adverse reactions in the prescribing information of SGLT2i. Furthermore, observational real-world studies analyzing claims data revealed similar results. For example, a large population-based observational study, analyzing data of more than 40,000 patients, found a two-fold increase in the risk of GFIs with the use of SGLT2i in older diabetic patients (16). Our study is the first to corroborate these findings in a NAFLD cohort. Furthermore, the 15% rate of GFIs in NAFLD patients found in our cohort is higher than those previously reported in SGLT2i-treated diabetic patients without NAFLD (17), which could point to a synergistic effect of NAFLD-related underlying immune dysfunction (1) added to the SGLT2i intrinsic increased risk of these infections. NAFLD indeed has been linked to immune system malfunctioning (18), including microcirculation disarrangements leading to diminished microbial clearance, undermined function of neutrophils and natural killer cells, and deficiency of vitamin-D levels, which in turn further impair innate immunity (19).
Notwithstanding the increased risk of GFIs infection, treatment with SGLT2i was not associated with and overall increase of infections. In contrast, HbA1c levels were independently associated with the risk of infections. This has been previously described in patients with T2DM (21–23). To our knowledge, this is the first study that corroborates this finding in NAFLD patients. As infections can precipitate acute decompensation and acute-on-chronic liver failure in cirrhotic patients (24), improving glycemic control could reduce the risk of infection. Further studies are required to better understand the pathologic pathways and clinical implications of these findings.
We found that patients with T2DM and comorbid NAFLD receiving treatment with SGLT2i were less likely to present hepatic events. Though preliminary, these data suggest the potential beneficial effects of SGLT2i in avoiding liver disease-related complications amongst patients with T2DM and NAFLD. Translational research in animal models and clinical studies has shown that SLGT2i use is related to improved hepatic metabolism (9). Its use has been associated with reductions in hepatic steatosis measured by controlled attenuation parameter, MRI-proton density fat fraction or magnetic resonance spectroscopy (7), as well as liver stiffness ameliorations in patients with previous significant fibrosis (8). In a single-arm pilot study with paired biopsies demonstrated that SGLT2i might induce histological improvements in NASH features without a worsening of fibrosis (10, 25). Moreover, a small randomized controlled trial found that SGLT2i treatment resulted in reduced liver fat content by MRI-derived proton density fat fraction and improvements in liver enzymes, compared to placebo (12). Several ongoing clinical trials are currently assessing the effects of SGLT2i in patients with NAFLD and NASH, which may provide more definitive answers. Parallel to their well-known beneficial cardiovascular and renal effects (5), SLGT2i may exert additional hepatic protection, which could be a cornerstone in the treatment of T2DM patients with NAFLD. Moreover, while SLGT2i undoubtedly increase GFIs, by improving the metabolic control the overall risk of infection could decrease. This balancing situation presents a trade-off for physicians and patients between metabolic control and adverse effects. Cirrhotic patients, especially those that have already presented decompensations, are of special interest regarding the role of SGLT2i because their combined glycosuric and natriuric effects might be beneficial in patients with hypervolemia and renal dysfunction such as those with hepatorrenal syndrome (26). Nonetheless, SGLT2i are seldom prescribed in patients with advanced liver disease. Preliminary findings by Saffo, Garcia-Tsao and Tadei in a cohort of seventy-eight patients with cirrhosis treated with SGLT2i, including 39 (50%) with non-alcoholic steatohepatitis and 63 (81%) with compensated disease, rates of hepatic decompensation and mortality were not increased compared to most published cohorts of cirrhotics, and SGLT2i use was not identified as a cause of decompensation (27). Whether administering SGLT2i before first decompensation or as earlier as possible in both diabetic and non-diabetic patients might be not only safe but beneficial as suggested by our findings warrants further investigation.
This study is not without limitations and results should be interpreted in the context of the study design. First, we performed a case-control study, which is prone to selection bias thereby limiting the validity of the results presented. In the case of our study, cases had higher rates of obesity, were using more drugs for T2DM, had more insulin use and also statin, and had also higher glycated hemoglobin, which might contribute to both infections and hepatic events. Second, the collection of relevant data was retrospective. Third, the relatively small sample size constrains the robustness of multivariate analyses. Fourth, the potential effects of medications other than SGLT2i (e.g., GLP1 receptor agonists) were not addressed in our analysis. Despite our limitations, we provide data about infectious and metabolic outcomes that are relevant to clinical practice. Nevertheless, these results should be interpreted in the context of hypothesis generating research and should be tested in subsequent, larger, studies.
When compared with patients with NAFLD and T2DM without SGLT2i treatment, patients receiving SGLT2i were more likely to present genitourinary fungal infections but not other types of infections. In addition, patients receiving SGLT2i had a lower occurrence of hepatic events. Further studies are required to confirm these results.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Vall d’Hebron University Hospital Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
Conceptualization and design: JB, JP; Data collection: JB, AP, JR-E, LC-R, AV, LR-O, MS; Data analysis: RM-N, MP; Interpretation: JR-E, AC, MS, VV, JG, JP; First manuscript drafting: JB, RM-N; Revision and acceptance of last version: All authors; Supervision: JP. All authors contributed to the article and approved the submitted version.
Preliminary analyses related to the present study were presented during the 46th Spanish Conference of the Association for the Study of the Liver (AEEH, Abstract 01213, June 14-16, 2021, Madrid, Spain).
JP reports having received consulting fees from Boehringer Ingelheim and Novo Nordisk. He has received speaking fees from Gilead, and travel expenses from Gilead, Rubió, Pfizer, Astellas, MSD, CUBICIN, and Novo Nordisk. He has received educational and research support from Gilead, Pfizer, Astellas, Accelerate, Novartis, Abbvie, ViiV, and MSD. Funds from European Commission/EFPIA IMI2 853966-2, IMI2 777377, H2020 847989, and ISCIII PI19/01898.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.945626/full#supplementary-material
NAFLD, Non-alcoholic fatty liver disease; T2DM, type 2 diabetes mellitus; SGLT2i, Sodium-glucose co-transporter-2 inhibitors; GFIs, genitourinary fungal infections; NASH, non-alcoholic steatohepatitis; VHUH, Vall d’Hebron University Hospital; HE, hepatic encephalopathy; COVID-19, Coronavirus disease 2019; IQR, interquartile range; BMI, body mass index; OR, odds ratio; CI, confidence of interval; MRI, magnetic resonance imaging.
1. Eslam M, Sanyal AJ, George J, International Consensus Panel. MAFLD: A consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology (2020) 158(7):1999–2014. doi: 10.1053/j.gastro.2019.11.312
2. Powell EE, Wong VW, Rinella M. Non-alcoholic fatty liver disease. Lancet. (2021) 397(10290):2212–24. doi: 10.1016/S0140-6736(20)32511-3
3. Younossi ZM. Non-alcoholic fatty liver disease - A global public health perspective. J Hepatol (2019) 70(3):531–44. doi: 10.1016/j.jhep.2018.10.033
4. Harrison SA, Gawrieh S, Roberts K, Lisanti CJ, Schwope RB, Cebe KM, et al. Prospective evaluation of the prevalence of non-alcoholic fatty liver disease and steatohepatitis in a large middle-aged US cohort. J Hepatol (2021) 75(2):284–91. doi: 10.1016/j.jhep.2021.02.034
5. Kalyani RR. Glucose-lowering drugs to reduce cardiovascular risk in type 2 diabetes. N Engl J Med (2021) 384(13):1248–60. doi: 10.1056/NEJMcp2000280
6. Storgaard H, Gluud LL, Bennett C, Grøndahl MF, Christensen MB, Knop K, et al. Benefits and harms of sodium-glucose Co-transporter 2 inhibitors in patients with type 2 diabetes: A systematic review and meta-analysis. PloS One (2016) 11(11):e0166125. doi: 10.1371/journal.pone.0166125
7. Dougherty JA, Guirguis E, Thornby KA. A systematic review of newer antidiabetic agents in the treatment of nonalcoholic fatty liver disease. Ann Pharmacother. (2021) 55(1):65–79. doi: 10.1177/1060028020935105
8. Shimizu M, Suzuki K, Kato K, Jojima T, Iijima T, Murohisa T, et al. Evaluation of the effects of dapagliflozin, a sodium-glucose co-transporter-2 inhibitor, on hepatic steatosis and fibrosis using transient elastography in patients with type 2 diabetes and non-alcoholic fatty liver disease. Diabetes Obes Metab (2019) 21(2):285–92. doi: 10.1111/dom.13520
9. Sumida Y, Yoneda M, Tokushige K, Kawanaka M, Fujii H, Yoneda M, et al. Antidiabetic therapy in the treatment of nonalcoholic steatohepatitis. Int J Mol Sci (2020) 21(6):1907. doi: 10.3390/ijms21061907
10. Lai LL, Vethakkan SR, Nik Mustapha NR, Mahadeva S, Chan WK. Empagliflozin for the treatment of nonalcoholic steatohepatitis in patients with type 2 diabetes mellitus. Dig Dis Sci (2020) 65(2):623–31. doi: 10.1007/s10620-019-5477-1
11. Mantovani A, Petracca G, Csermely A, Beatrice G, Targher G. Sodium-glucose cotransporter-2 inhibitors for treatment of nonalcoholic fatty liver disease: A meta-analysis of randomized controlled trials. Metabolites. (2020) 11(1):22. doi: 10.3390/metabo11010022
12. Kuchay MS, Krishan S, Mishra SK, Farooqui KJ, Singh MK, Wasir JS, et al. Effect of empagliflozin on liver fat in patients with type 2 diabetes and nonalcoholic fatty liver disease: A randomized controlled trial (E-LIFT trial). Diabetes Care (2018) 41(8):1801–8. doi: 10.2337/dc18-0165
13. Nichols GA, Brodovicz KG, Kimes TM, Déruaz-Luyet A, Bartels DB. Prevalence and incidence of urinary tract and genital infections among patients with and without type 2 diabetes. J Diabetes Complications. (2017) 31(11):1587–91. doi: 10.1016/j.jdiacomp.2017.07.018
14. Li D, Wang T, Shen S, Fang Z, Dong Y, Tang H. Urinary tract and genital infections in patients with type 2 diabetes treated with sodium-glucose co-transporter 2 inhibitors: A meta-analysis of randomized controlled trials. Diabetes Obes Metab (2017) 19(3):348–55. doi: 10.1111/dom.12825
15. McGovern AP, Hogg M, Shields BM, Sattar NA, Holman RR, Pearson ER, et al. Risk factors for genital infections in people initiating SGLT2 inhibitors and their impact on discontinuation. BMJ Open Diabetes Res Care (2020) 8(1):e001238. doi: 10.1136/bmjdrc-2020-001238
16. Lega IC, Bronskill SE, Campitelli MA, Guan J, Stall NM, Lam K, et al. Sodium glucose cotransporter 2 inhibitors and risk of genital mycotic and urinary tract infection: A population-based study of older women and men with diabetes. Diabetes Obes Metab (2019) 21(11):2394–404. doi: 10.1111/dom.13820
17. Engelhardt K, Ferguson M, Rosselli JL. Prevention and management of genital mycotic infections in the setting of sodium-glucose cotransporter 2 inhibitors. Ann Pharmacother. (2021) 55(4):543–8. doi: 10.1177/1060028020951928
18. Nseir W, Taha H, Khateeb J, Grosovski M, Assy N. Fatty liver is associated with recurrent bacterial infections independent of metabolic syndrome. Dig Dis Sci (2011) 56(11):3328–34. doi: 10.1007/s10620-011-1736-5
19. Adenote A, Dumic I, Madrid C, Barusya C, Nordstrom CW, Rueda Prada L. NAFLD and infection, a nuanced relationship. Can J Gastroenterol Hepatol (2021) 2021:5556354. doi: 10.1155/2021/5556354
20. Association AD. 2. classification and diagnosis of diabetes: Standards of medical care in diabetes–2021. Diabetes Care (2021) 44(Suppl 1):S15. doi: 10.2337/dc21-S002
21. Mor A, Dekkers OM, Nielsen JS, Beck-Nielsen H, Sørensen HT, Thomsen RW. Impact of glycemic control on risk of infections in patients with type 2 diabetes: A population-based cohort study. Am J Epidemiol. (2017) 186(2):227–36. doi: 10.1093/aje/kwx049
22. Critchley JA, Carey IM, Harris T, DeWilde S, Hosking FJ, Cook DG. Glycemic control and risk of infections among people with type 1 or type 2 diabetes in a Large primary care cohort study. Diabetes Care (2018) 41(10):2127–35. doi: 10.2337/dc18-0287
23. Carey IM, Critchley JA, DeWilde S, Harris T, Hosking FJ, Cook DG. Risk of infection in type 1 and type 2 diabetes compared with the general population: A matched cohort study. Diabetes Care (2018) 41(3):513–21. doi: 10.2337/dc17-2131
24. Villanueva C, Albillos A, Genescà J, Garcia-Pagan JC, Brujats A, Calleja JL, et al. Bacterial infections adversely influence the risk of decompensation and survival in compensated cirrhosis. J Hepatol (2021) 75(3):589–99. doi: 10.1016/j.jhep.2021.04.022
25. Akuta N, Kawamura Y, Watanabe C, Nishimura A, Okubo M, Mori Y, et al. Impact of sodium glucose cotransporter 2 inhibitor on histological features and glucose metabolism of non-alcoholic fatty liver disease complicated by diabetes mellitus. Hepatol Res (2019) 49:531–9. doi: 10.1111/hepr.13304
26. Saffo S, Taddei T. SGLT2 inhibitors and cirrhosis: A unique perspective on the comanagement of diabetes mellitus and ascites. Clin Liver Dis (Hoboken) (2018) 11(6):141–4. doi: 10.1002/cld.714
Keywords: NAFLD, type 2 diabetes mellitus, sodium-glucose co-transporter-2 inhibitors, infections, hepatic outcomes
Citation: Bañares J, Manzano-Nuñez R, Prió A, Rivera-Esteban J, Camps-Relats L, Villarejo A, Ruiz-Ortega L, Pons M, Ciudin A, Salcedo MT, Vargas V, Genescà J and Pericàs JM (2022) Risk of infections in patients with NAFLD and Type 2 Diabetes under treatment with SGLT2 inhibitors and relationship with liver outcomes: A retrospective case-control study. Front. Endocrinol. 13:945626. doi: 10.3389/fendo.2022.945626
Received: 16 May 2022; Accepted: 04 August 2022;
Published: 24 August 2022.
Edited by:
Cristiane Nogueira, Federal University of Rio de Janeiro, BrazilReviewed by:
Man-Fung Tsoi, The University of Manchester, United KingdomCopyright © 2022 Bañares, Manzano-Nuñez, Prió, Rivera-Esteban, Camps-Relats, Villarejo, Ruiz-Ortega, Pons, Ciudin, Salcedo, Vargas, Genescà and Pericàs. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan M. Pericàs, anVhbi5wZXJpY2FzQHZoaXIub3Jn; Andreea Ciudin, YW5kcmVlYS5jaXVkaW5AdmFsbGhlYnJvbi5jYXQ=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.