 Jie Jiang1†Xiaoxia Tang2†Yongzhu Pu1†Yong Yang3†Conghui Yang1Fake Yang1Yadong Tian1
Jie Jiang1†Xiaoxia Tang2†Yongzhu Pu1†Yong Yang3†Conghui Yang1Fake Yang1Yadong Tian1 Jindan Li1Hua Sun1*Sheng Zhao1*
Jindan Li1Hua Sun1*Sheng Zhao1* Long Chen1*
Long Chen1*- 1Department of PET/CT Center, Yunnan Cancer Hospital, The Third Affiliated Hospital of Kunming Medical University, Yunnan, China
- 2Department of Pharmacy, The Second Affiliated Hospital of Kunming Medical University, Yunnan, China
- 3Department of Urology, Yunnan Cancer Hospital, The Third Affiliated Hospital of Kunming Medical University, Yunnan, China
Prostate cancer (PCa) induced death is the predominant cause of cancer-related death among men in 48 countries. After radical treatment, biochemical recurrence has become an important factor for prognosis. The early detection and diagnosis of recurrent lesions are very helpful in guiding treatment and improving the prognosis. PET/CT is a promising method for early detection of lesions in patients with biochemical recurrence of prostate cancer. This article reviews the progress of the research on PET/CT in the PCa biochemical recurrence and aims to introduce new technologies and provide more direction for future research.
Background
Prostate cancer (PCa), the fifth reason of cancer-related death among male, is also the second most commonly diagnosed cancer (1). In 2020 1.4 million cases were newly diagnosed and 375,000 deaths were identified around the world (2). With the general promotion of prostate-specific antigen (PSA) screening, the improvement of biopsy technology, as well as the optimization of treatment methods, both of the incidence and mortality rates of PCa have declined or stabilized in most countries in recent years. However, the incidence of advanced PCa has increased (2, 3). Prostate cancer is a malignant tumor with extremely heterogeneous clinical behavior and has biological behaviors ranging from inertia and organ limitation to rapid invasion and easy metastasis (4). It is diagnosed mainly through digital rectal examination (DRE) and PSA testing. Once a preliminary diagnosis is made, a needle biopsy guided by a rectal ultrasound (TRUS) is performed (5). After an initial treatment via radical prostatectomy (RP) or local radiotherapy (RT), almost half of patients develop biochemical recurrence (BCR) and an increase in PSA. After a potential remedial treatment option, androgen deprivation therapy (ADT) is usually used for the patient. After the ADT, prostate-specific antigens begin to rise again in 2-8 years, and metastatic castration-resistant PCa can develop (6). Studies have shown that salvage RT (SRT) after early RP provides a cure for increased PSA in patients after RP (7–9), and therefore, early detection of BCR and lesion metastasis and accurate restaging guidance for the treatment of recurrent PCa is very important. Both of CT and MRI are structural imaging techniques and are of limited sensitivity and specificity for detecting a minimal metastatic lesion, which leads to a lower diagnostic rate for common imaging techniques in asymptomatic patients (10). The molecular imaging PET/CT is believed to be superior to BCR detection.
PET/CT Imaging Agent for BCR PCa
BCR is generally defined by elevated PSA values (more than 0.2 ng/ml) in consecutively two tests after RP (11, 12). For patients receiving radiation therapy, biochemical failure is defined as the end of radiotherapy with the lowest PSA increase in the last 6 weeks being ≥ 2 ng/mL (13). Over the past decade, a variety of PET probes have achieved good results in detecting recurrent lesions and disease staging in PCa patients. PET radiotracers that are used have developed rapidly and mainly include radiolabeled choline, prostate specific membrane antigen (PSMA) ligands,18F-fluciclovine, gastrin-releasing peptide receptor(GRPR), fibroblast activation protein inhibitors(FAPI) and so on (14–22) (Table 1)
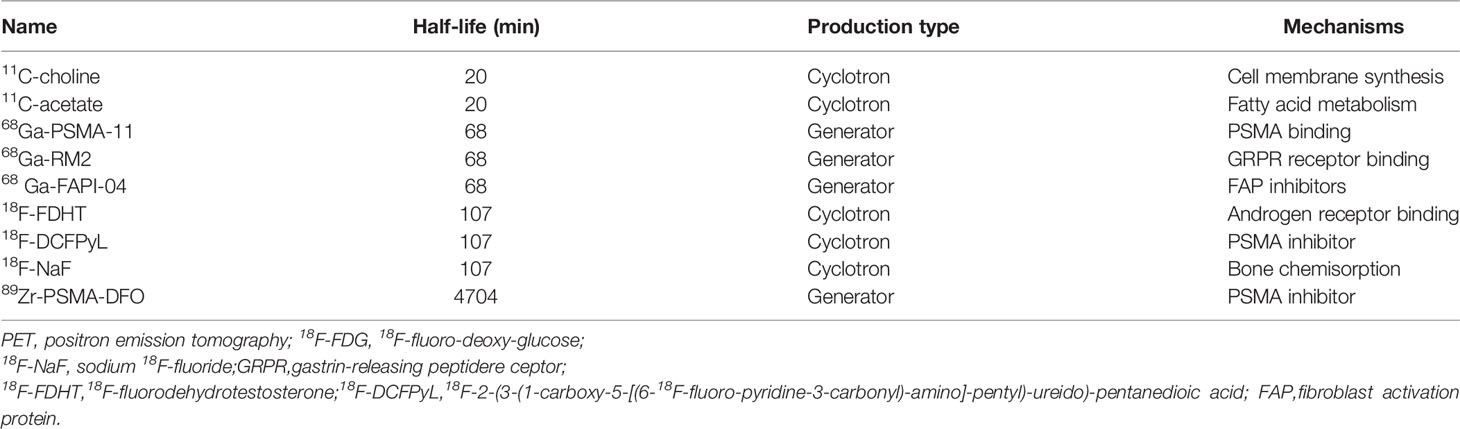
Table 1 Common PET-CT imaging agents to detect biochemical recurrence of prostate cancer.
PSMA is a highly overexpressed transmembrane glycoprotein detected in the majority of prostate cancer cells (23) and is located in the apical region of prostate cells (i.e., the prostate tube) (Figure 1). PSMA is expressed in peripheral epithelial cells (24), and high-grade PCa have higher PSMA expression, and PSMA expression in late and castration-resistant PCa is further increased (25). PSMA binds with high affinity to the folate hydrolase of the PC cells, allowing the PSMA to show its potential to recognize BCR sites (26), and becomes the target of PCa imaging and therapy. PSMA-PET exhibits good early detection and localization of PCa recurrence lesions and identification of BCR lymph node metastasis after RP (27, 28). (Table 2) And 68Ga-PSMA-11 is the first FDA-approved radiotracer for PCa-specific PET/CT imaging (29, 30) (Table 2)
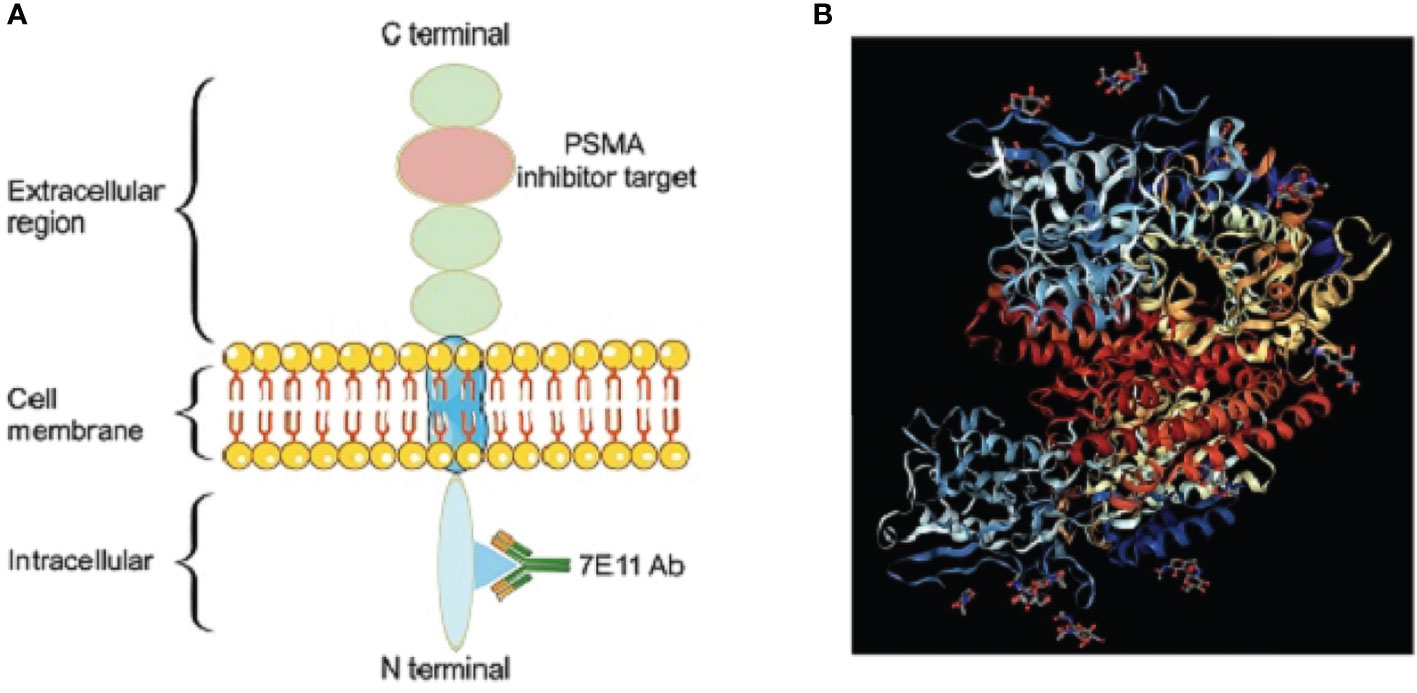
Figure 1 PSMA structure diagram. (A) Schematic illustration of PSMA. (B) Cyrstal structure of PSMA.
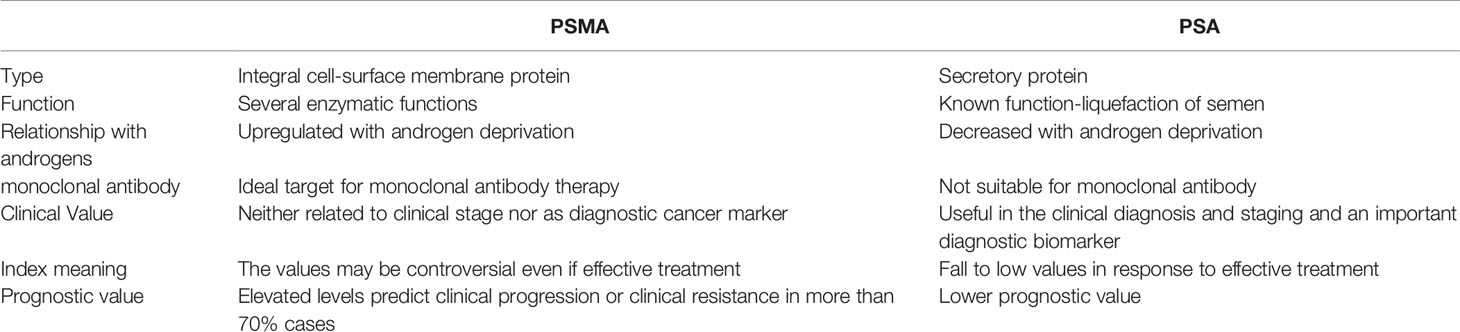
Table 2 The difference between PSMA and PSA.
Choline radiopharmaceuticals were used for prostate cancer earlier, and often labeled with 11C and 18F, which can be used for the detection of recurrent lesions and the detection of early recurrence in patients with a history of BCR PCa (31, 32). 18F-fluciclovine is a synthetic amino acid with good biodistribution and little urinary disturbance, is often used for restaging of BCR patients (33). Gastrin-releasing peptide receptor antagonist (RM2) binds to GRPR on PCa cells, complementary to PSMA-targeted imaging (15, 34). Fibroblast activation protein (FAP) is highly expressed in a variety of epithelial cancers, and FAP inhibitor (FAPI) PET/CT has been used for various tumor imaging. Research has confirmed the uptake of 68Ga-FAPI-04 in PCa tissue was higher than that in normal prostate tissue, and FAP expression was increased after ADT, which has potential when the detection of lesions is limited after ADT (16, 21, 35).
Recurrent Lesions Detection and Localization
Patients with a large number of RPs have an elevated PSA, and early detection and localization of anatomical sites of recurrence are critical to guide subsequent treatment. PET/CT was believed to be better than a morphological-based standard imaging mode (CWU) (36). An analysis of prostate cancer in Asian populations showed that standard imaging was not sensitive to recurrent PCa, and none of the bone lesions detected by PET was detected by CWU (37). Choline-PET is the most widely studied method, and although it has excellent specificity (38), its sensitivity is low, especially when PSA levels are low (39). A prospective study showed a PSMA-PET/CT detection rate of 66%, which is remarkably higher than the 18F-choline PET/CT detection rate of 32% (40). 68Ga-PSMA PET showed an obviously higher detection rate and a higher general impact on the clinical management than 18F-fluoromethylcholine (41, 42). 18F-fluciclovine has excellent detection rates for low, medium and high PSA levels (43, 44), and the test results are significantly better than those obtained with 11C-choline (38, 45). A meta-analysis showed that in BCR patients, the combined detection rates of 18F-labeled choline, fluciclovir, and PSMA were 66%, 74%, and 83%, respectively (38). The study by Hoffmann et al. compared the detection rates of 18F-PSMA and 68Ga-PSMA PET, and the results showed that the detection rates of the two tracers were similar, 87.5% (112/128) and 88.9% (121/136), respectively (46). A recent study showed, 68Ga-P16-093, a small molecule PSMA ligand, detected 71% of lesions in BCR patients (47) (Table 3)
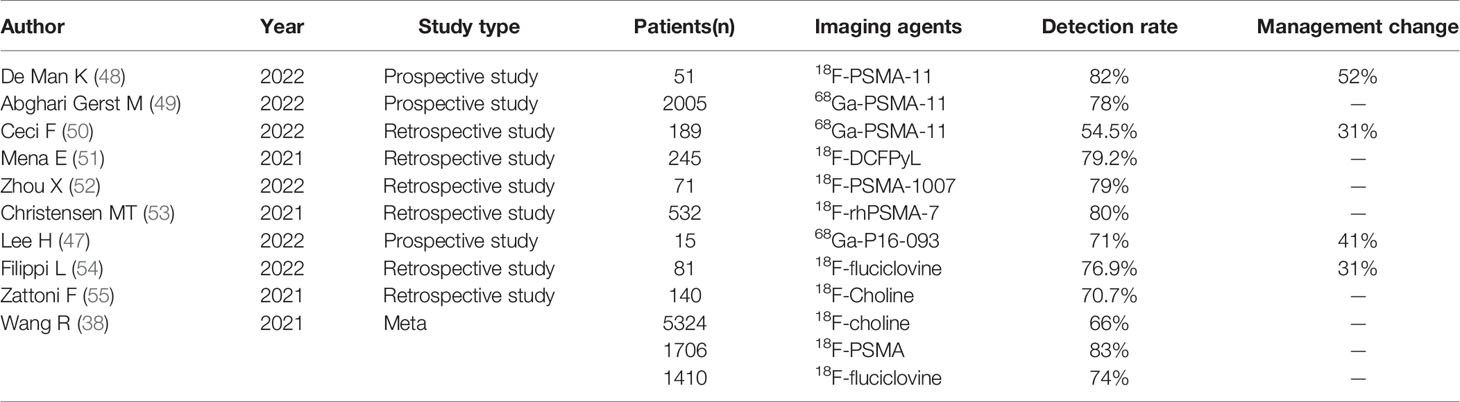
Table 3 Detection rate of different imaging agents for BCR PCa.
Previous studies have shown that PSMA PET has a higher detection rate than other tracers, and some researchers have found that when PSMA expression is low or PSMA negative tumor area ≥ 50%, PSMA-PET results are negative, although PSA levels are very high (56). When PSMA expression is low, Dietlein et al. found 5 89Zr-PSMA-DFO PET-positive lesions in 14 PSMA-PET-negative patients.89Zr-PSMA-DFO PET becomes a good supplement because its half-life is long enough to allow the process of ligand internalization to proceed sufficiently to make the lesions visible (22, 56, 57). Targeting gastrin-releasing peptide receptor (GRPR) is thought to complement PSMA-negative prostate cancer (PCa) patients (58), and it is helpful for the localization of recurrent lesions in 18FECH PET/CT-negative patients (59).Another study showed that the detection rate of 18F-FDG PET/CT in PSMA-PET negative patients was 16.7%, and patients with PSA ≥2.3 ng/mL and high Gleason score were more likely to benefit from FDG PET (60).
Factors Affecting the Detection Rate
Many studies (41, 61–65) have indicated that PSMA, choline, fluciclovine PET/CT positive results possibly are significantly correlated with increased PSA levels (37). For patients with BCR, the positive rate of the PET/CT scan varies based on the clinical stage of the BCR, PSA levels as well as PSA doubling time during the scan are correlated with positive results (27, 66). A study showed that the detection rates of 18F-labeled choline, fluciclovine, and PSMA were 35, 23, and 58% for a PSA level less than 0.5 ng/ml;80, 92, and 94% for a PSA level more than 2.0 ng/ml (38). The rate of increase grows with a rise in the serum PSA levels before the PET (27, 67, 68). There are studies that shown that when the PSA levels higher than 0.2 ng/ml while the PSA velocity ≥ 1 ng/ml/year, there will be a positive PSMA scan (69), and with higher PSA levels, the PSMA-PET shows better diagnostic performance (28).
It has been documented that androgen deprivation therapy experience in BCR patients is correlated with the positive rate of PSMA-PET scans (69), and there is evidence that PSMA is induced with low doses of ADT at lower PSA levels (≤0.3 ng/mL). Imaging may enhance the positive scan rate (70), but further research is needed. In addition, the time to inject the imaging agent is related to the contrast of the image. For BCR with low PSA levels, imaging 3 hours after injection is more advantageous in terms of lesion contrast (71), which may also have an effect on the positive scan rate. Scanning technology and timing also have an impact on the positive rate. Morawitz et al. (72) found that 68Ga-PSMA-11 PET/CT scanning in the late abdominal and pelvic stage after emptying the bladder was helpful to detect missed local recurrence lesions. Uprimny et al. (73) improved the detection rate of lesions by using furosemide before scanning.
PET Imaging for BCR of Low PSA Levels
Currently, salvage RT (SRT) is one valuable treatments for patients with PSA elevation after RP. Early diagnosis of BCR at low PSA levels has a major impact on patients’ follow-up treatment. EVU guidelines recommend that PSA levels greater than 0.2 ng/mL and results influence subsequent treatment decisions, imaging of biochemically recurrent PCa with PSMA-labeled PET/CT (74). A study in 2005 patients with BCR found that the detection rate of 68Ga-PSMA-11 was 44.8% when the PSA was less than 0.25 ng/mL (49). A meta-analysis showed that the detection rates of 18F-Choline, 18F-Fluciclovine and 18F-PSMA PET/CT at PSA levels less than 0.5 ng/ml were 35%, 23%, and 58%, respectively (38). PEMA-PET is superior to other imaging methods at low PSA levels, as recommended by guidelines (Figure 2). 18F-fluciclovine PET is feasible for patients with PSA <1.0ng/ml. Filippi et al (54) found that the detection rate in 81 Italian patients was 66.7% when the PSA level was 0.2-0.57 ng/ml, and Wang et al. (75) in 46 patients with PSA level of 0.3-1.0ng/ml found the positive rate was about 33%, but it was not found positive cases in very low PSA (less than 0.3ng/ml) BCR patients. The value of 18F-fluciclovine PET in detecting lesions in BCR patients with very low PSA levels remains to be explored. A recent study found that at very low PSA (≤0.1ng/ml) levels, dynamic detection of 11C-choline PET was helpful in detecting early recurrence in BCR PCa patients (32). This could be a valuable new direction.
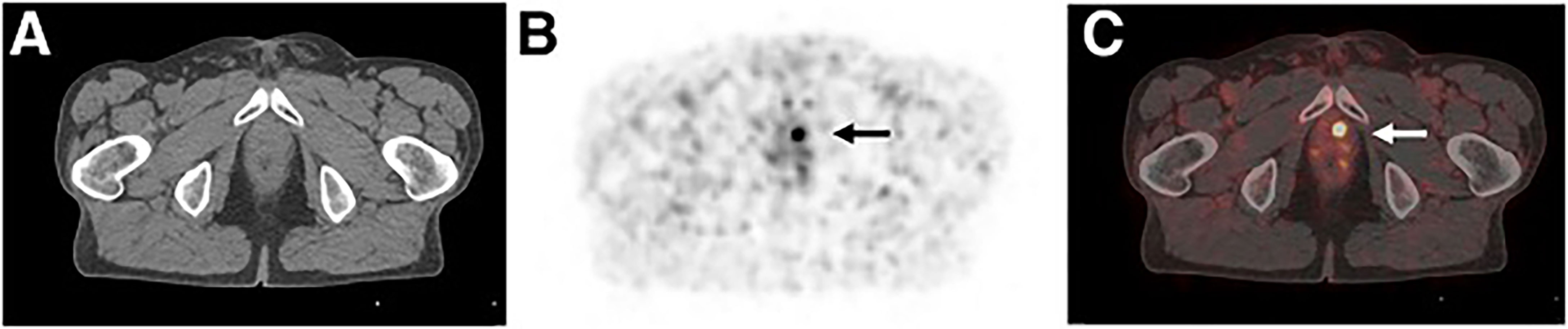
Figure 2 A 78-year-old patient with biochemical recurrence (PSA of 0.54 ng/mL) after radical prostatectomy (initially pT3b N0 M0 R0 G2). 68Ga-PSMA ligand PET/CT reveals focal uptake in left paramedian prostatic fossa, indicating local recurrence. The picture below shows transaxial CT (A), PET (B), and fused PET/CT (C) images respectively. Patient was referred for salvage radiation treatment. This research was originally published in JNM. Author(Schwarzenboeck SM, Rauscher I, Bluemel C, Fendler WP, Rowe SP, Pomper MG, Afshar-Oromieh A, Herrmann K, Eiber M). PSMA Ligands for PET Imaging of Prostate Cancer. J Nucl Med. 2017 Oct;58(10):1545-1552.© SNMMI.
Detection of Metastases in BCR Patients
Increased serum PSA levels are sensitive to in vitro markers of recurrent prostate cancer; however, it is still hard to differentiate local recurrence and regional or distant metastasis. Identifying metastatic disease can impact therapeutic schedule options and contributes to prognosis assessment (27). PSMA PET/CT is most commonly used to detect LN metastases and staging in BCR patients after RP, and its performance depends on the PSA levels as well as the volume of debris from metastatic cells (28). However, in small lymph nodes, this method performs well (76). Rauscher showed that 68Ga-PSMA PET detected LNM (77.9%) in 68 histopathologically confirmed metastatic LN regions, whereas conventional imaging modality only detected 18 of 67 regions (26.9%) (77). Studies have shown that 18F-rhPSMA-7 and 18F-rhPSMA-7.3 PET have a detection rate of 81.3% for lymph node metastasis in BCR patients after RP, and their accuracy in evaluating lymph node metastasis is comparable to that of 18F-PSMA-11 (78).PSMA-PET/CT has higher diagnostic accuracy for lymph node recurrence after RP, especially for small-volume metastases, 18 F-PSMA-1007 PET/CT can reliably detect malignant lymph nodes larger than 3 mm with a specificity of over 99% (79–81) (Figure 3)
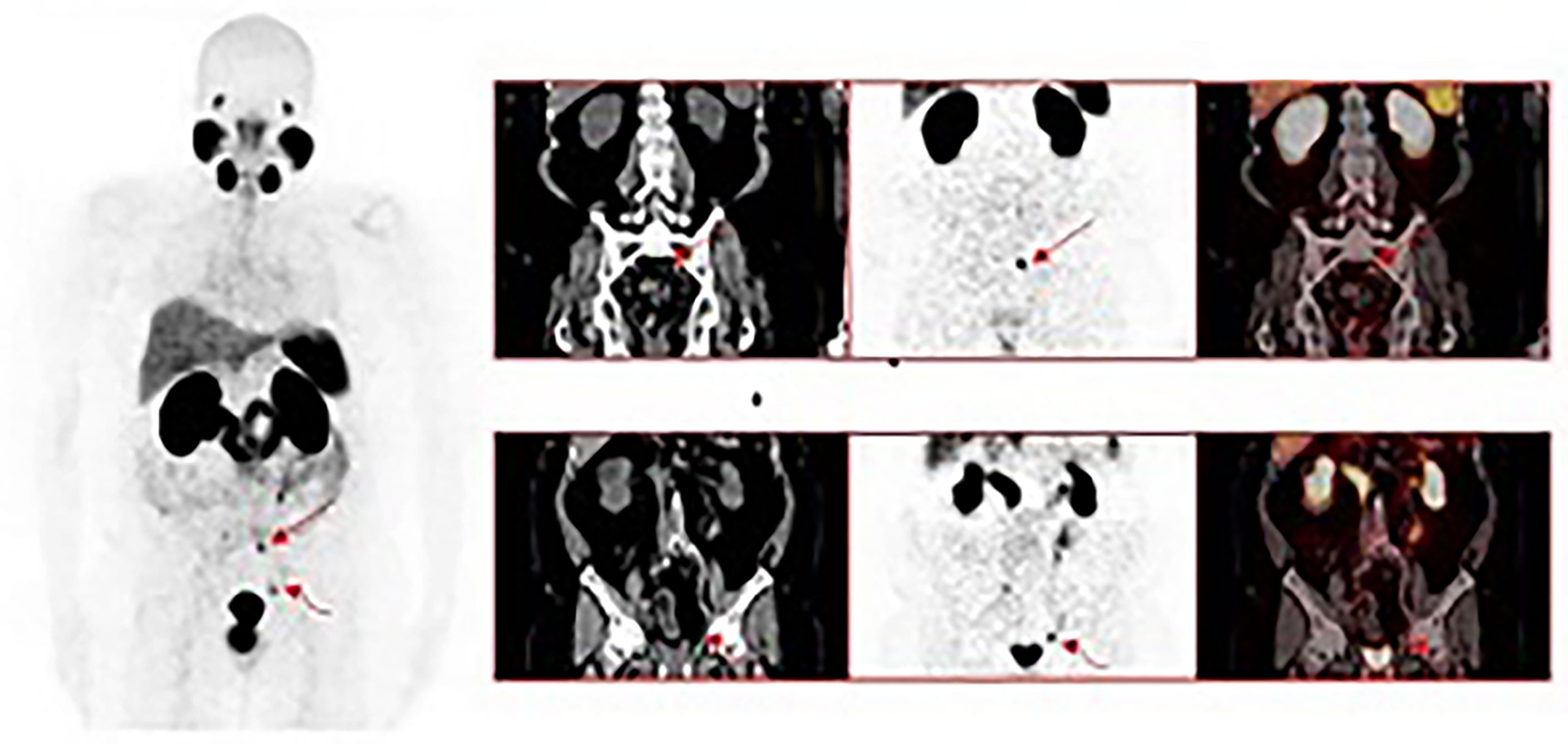
Figure 3 A 63-year-old male with a history of radical prostatectomy for adenocarcinoma of the prostate, Gleason 4 + 4. 68Ga-PSMA-11 PET/CT was requested for localization of disease recurrence at a serum PSA of 0.54 ng/mL. Images show intense tracer uptake in a subcentimeter left presacral node (straight arrows) and a subcentimeter left external iliac node consistent with the sites of prostate cancer recurrence. This research was originally published in JCM.Lawal IO, Lengana T, Popoola GO, Orunmuyi AT, Kgatle MM, Mokoala KMG, Sathekge MM. Pattern of Prostate Cancer Recurrence Assessed by 68Ga-PSMA-11 PET/CT in Men Treated with Primary Local Therapy. J Clin Med. 2021 Aug 29;10(17):3883.
Bone metastasis is one of the common metastasis methods of prostate cancer, and it is difficult to differentiate diagnosis by traditional imaging due to degenerative changes. Mingels et al. found in 177 BCR patients that the PPV of 18F-PSMA-1007 PET to identify bone lesions was 79%, which was lower than the positive rate of the overall and LN (82). A meta-analysis showed that the highest sensitivity of NaF-PET/CT in identifying bone metastases was 0.97, followed by PSMA PET, higher than choline, MRI and bone scintigraphy (83). A recent study found that 18F-NaF PET/CT detected 93.6% of bone metastases, and the interobserver agreement was very high, with stable and reproducible results (18).
PET/CT False Negatives and False Positives
For PSMA-PET, a small fraction (<10%) of PCa expressed low PSMA, which results in little or no uptake on PSMA-PET (79, 84). In these PSMA-negative patients, PSMA-PET is ineffective (36). In addition, metal artifacts low levels of PSMA uptake and bladder overflow are also possible elements of false negatives (85).Positive images need to be differentiated from normal tissue, benign lesions, and other non-PCa malignant lesions (25, 86–88). Reports have shown that in normal tissues, high or mild 68 Ga-PSMA-11 uptake was observed in the renal cortex, duodenum, parotid gland, and submandibular salivary glands, spleen, lacrimal gland, and liver (89–92). In some benign tissues with high proliferation rate, just like heart valves, pleura, endometrial scars, and granulation tissue, endothelial cells also express PSMA (25, 93, 94). Abnormal accumulation of PSMA-PET were detected in lots of benign lesions, including sarcoidosis (86, 95), Paget’s disease (96), healing fractures (97, 98), hemangioma (99), schwannomas (100), adenoma (101), and so on. Malignant tumors other than PCa, such as renal cell carcinoma (102, 103) and hepatocellular carcinoma (104), also have high expression. In addition, 18F-fluorocholine imaging usually shows abnormal uptake in lymph nodes due to inflammatory changes (105).All of the above cause false positive results, so it is necessary to learn about the physiological uptake and normal distribution in order to reduce the false positive results in the diagnosis.
Conclusions
PSMA-PET has high accuracy in the detection of PCa BCR and the identification of metastasis, especially at low PSA levels. Its diagnostic potential is significantly better than that of choline and amino acid analogues, and this has a remarkable influence on managing patients in clinical. However, due to the expression and distribution characteristics of PSMA, it is unable to reliably recognize the PSMA-negative lesions, and other imaging methods need to be selected as supplements. According to the actual situation of patients, the combined use of complementary imaging agents to detect and locate BCR lesions is helpful for the early and effective detection and localization of recurrent lesions in BCR PCa patients, and is conducive to the selection of treatment options and the improvement of prognosis. Radiocomposites (such as 18F-NOTA-GRPR-PSMA, etc.) with the advantages of two or more imaging agents at the same time may become a research hotspot in the future.
Author Contributions
HS conducted project management, writing review and editing. LC and SZ conducted method guidance, writing review and editing. JJ, XXT, YZP and YY conducted data collection, writing-draft preparation. CHY and FKY carried out illustration drawing and software support. YDT and JDL supervised the process. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
This work was supported by the National Natural Science Foundation of China (grant number 81960496), Yunnan Fundamental Research Projects (grant number 202101AT070050), the Project funded by China Postdoctoral Science Foundation (grant number 2019M653501), Scientific Research Fund of Yunnan Province Educational Department (grant number K13219357), Yunnan Provincial Science and Technology Agency/Kunming Medical University Joint Project [grant number #2019FE001(-087)], Kunming Medical University Graduate Innovation Fund (grant number 2021S070), and the Xingdianyingcai support plan.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. Ca-a Cancer J Clin (2021) 71(1):7–33. doi: 10.3322/caac.21654
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
3. Culp MB, Soerjomataram I, Efstathiou JA, Bray F, Jemal A. Recent Global Patterns in Prostate Cancer Incidence and Mortality Rates. Eur Urol (2020) 77(1):38–52. doi: 10.1016/j.eururo.2019.08.005
4. Rodrigues DN, Butler LM, Estelles DL, de Bono JS. Molecular Pathology and Prostate Cancer Therapeutics: From Biology to Bedside. J Pathol (2014) 232(2):178–84. doi: 10.1002/path.4272
5. Mohler JL, Antonarakis ES, Armstrong AJ, D’Amico AV, Davis BJ, Dorff T, et al. Prostate Cancer, Version 2.2019, Nccn Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw (2019) 17(5):479–505. doi: 10.6004/jnccn.2019.0023
6. Schwarzenboeck SM, Rauscher I, Bluemel C, Fendler WP, Rowe SP, Pomper MG, et al. Psma Ligands for Pet Imaging of Prostate Cancer. J Nucl Med Off Publ Soc Nucl Med (2017) 58(10):1545–52. doi: 10.2967/jnumed.117.191031
7. Pfister D, Bolla M, Briganti A, Carroll P, Cozzarini C, Joniau S, et al. Early Salvage Radiotherapy Following Radical Prostatectomy. Eur Urol (2014) 65(6):1034–43. doi: 10.1016/j.eururo.2013.08.013
8. Wiegel T, Lohm G, Bottke D, Hocht S, Miller K, Siegmann A, et al. Achieving an Undetectable Psa After Radiotherapy for Biochemical Progression After Radical Prostatectomy Is an Independent Predictor of Biochemical Outcome–Results of a Retrospective Study. Int J Radiat Oncol Biol Phys (2009) 73(4):1009–16. doi: 10.1016/j.ijrobp.2008.06.1922
9. Soto DE, Passarelli MN, Daignault S, Sandler HM. Concurrent Androgen Deprivation Therapy During Salvage Prostate Radiotherapy Improves Treatment Outcomes in High-Risk Patients. Int J Radiat Oncol Biol Phys (2012) 82(3):1227–32. doi: 10.1016/j.ijrobp.2010.08.030
10. Rouviere O, Vitry T, Lyonnet D. Imaging of Prostate Cancer Local Recurrences: Why and How? Eur Radiol (2010) 20(5):1254–66. doi: 10.1007/s00330-009-1647-4
11. Cookson MS, Aus G, Burnett AL, Canby-Hagino ED, D’Amico AV, Dmochowski RR, et al. Variation in the Definition of Biochemical Recurrence in Patients Treated for Localized Prostate Cancer: The American Urological Association Prostate Guidelines for Localized Prostate Cancer Update Panel Report and Recommendations for a Standard in the Reporting of Surgical Outcomes. J Urol (2007) 177(2):540–5. doi: 10.1016/j.juro.2006.10.097
12. Cornford P, Bellmunt J, Bolla M, Briers E, De Santis M, Gross T, et al. Eau-Estro-Siog Guidelines on Prostate Cancer. Part Ii: Treatment of Relapsing, Metastatic, and Castration-Resistant Prostate Cancer. Eur Urol (2017) 71(4):630–42. doi: 10.1016/j.eururo.2016.08.002
13. Hofman MS, Murphy DG, Williams SG, Nzenza T, Herschtal A, Lourenco RA, et al. A Prospective Randomized Multicentre Study of the Impact of Gallium-68 Prostate-Specific Membrane Antigen (Psma) Pet/Ct Imaging for Staging High-Risk Prostate Cancer Prior to Curative-Intent Surgery or Radiotherapy (Propsma Study): Clinical Trial Protocol. BJU Int (2018) 122(5):783–93. doi: 10.1111/bju.14374
14. Boustani AM, Pucar D, Saperstein L. Molecular Imaging of Prostate Cancer. Br J Radiol (2018) 91(1084):20170736. doi: 10.1259/bjr.20170736
15. Baratto L, Song H, Duan H, Hatami N, Bagshaw HP, Buyyounouski M, et al. Psma- and Grpr-Targeted Pet: Results From 50 Patients With Biochemically Recurrent Prostate Cancer. J Nucl Med (2021) 62(11):1545–9. doi: 10.2967/jnumed.120.259630
16. Kratochwil C, Flechsig P, Lindner T, Abderrahim L, Altmann A, Mier W, et al. (68)Ga-Fapi Pet/Ct: Tracer Uptake in 28 Different Kinds of Cancer. J Nucl Med (2019) 60(6):801–5. doi: 10.2967/jnumed.119.227967
17. Mohsen B, Giorgio T, Rasoul ZS, Werner L, Ali GR, Reza DK, et al. Application of C-11-Acetate Positron-Emission Tomography (Pet) Imaging in Prostate Cancer: Systematic Review and Meta-Analysis of the Literature. BJU Int (2013) 112(8):1062–72. doi: 10.1111/bju.12279
18. Zacho HD, Fonager RF, Nielsen JB, Haarmark C, Hendel HW, Johansen MB, et al. Observer Agreement and Accuracy of (18)F-Sodium Fluoride Pet/Ct in the Diagnosis of Bone Metastases in Prostate Cancer. J Nucl Med (2020) 61(3):344–9. doi: 10.2967/jnumed.119.232686
19. Beattie BJ, Smith-Jones PM, Jhanwar YS, Schöder H, Schmidtlein CR, Morris MJ, et al. Pharmacokinetic Assessment of the Uptake of 16beta-18f-Fluoro-5alpha-Dihydrotestosterone (Fdht) in Prostate Tumors as Measured by Pet. J Nucl Med (2010) 51(2):183–92. doi: 10.2967/jnumed.109.066159
20. Müller PJ, Dietlein M, Kobe C, Heidenreich A, Drzezga A. Oligometastatic Disease in Biochemical Recurrence of Prostate Cancer: Prevalence on Psma Pet/Ct and Consecutive Metastasis-Directed Therapy - Experience at a Tertiary Referral Center. Nuklearmedizin (2022). doi: 10.1055/a-1697-8111
21. Kesch C, Yirga L, Dendl K, Handke A, Darr C, Krafft U, et al. High Fibroblast-Activation-Protein Expression in Castration-Resistant Prostate Cancer Supports the Use of Fapi-Molecular Theranostics. Eur J Nucl Med Mol Imaging (2021) 49(1):385–9. doi: 10.1007/s00259-021-05423-y
22. Vázquez SM, Endepols H, Fischer T, Tawadros SG, Hohberg M, Zimmermanns B, et al. Translational Development of a Zr-89-Labeled Inhibitor of Prostate-Specific Membrane Antigen for Pet Imaging in Prostate Cancer. Mol Imaging Biol (2022) 24(1):115–25. doi: 10.1007/s11307-021-01632-x
23. Mannweiler S, Amersdorfer P, Trajanoski S, Terrett JA, King D, Mehes G. Heterogeneity of Prostate-Specific Membrane Antigen (Psma) Expression in Prostate Carcinoma With Distant Metastasis. Pathol Oncol Res: POR (2009) 15(2):167–72. doi: 10.1007/s12253-008-9104-2
24. DeMarzo AM, Nelson WG, Isaacs WB, Epstein JI. Pathological and Molecular Aspects of Prostate Cancer. Lancet (London England) (2003) 361(9361):955–64. doi: 10.1016/s0140-6736(03)12779-1
25. Bostwick DG, Pacelli A, Blute M, Roche P, Murphy GP. Prostate Specific Membrane Antigen Expression in Prostatic Intraepithelial Neoplasia and Adenocarcinoma: A Study of 184 Cases. Cancer (1998) 82(11):2256–61. doi: 10.1002/(sici)1097-0142(19980601)82:11<2256::aid-cncr22>3.0.co;2-s
26. Kaittanis C, Andreou C, Hieronymus H, Mao N, Foss CA, Eiber M, et al. Prostate-Specific Membrane Antigen Cleavage of Vitamin B9 Stimulates Oncogenic Signaling Through Metabotropic Glutamate Receptors. J Exp Med (2018) 215(1):159–75. doi: 10.1084/jem.20171052
27. Perera M, Papa N, Christidis D, Wetherell D, Hofman MS, Murphy DG, et al. Sensitivity, Specificity, and Predictors of Positive (68)Ga-Prostate-Specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer: A Systematic Review and Meta-Analysis. Eur Urol (2016) 70(6):926–37. doi: 10.1016/j.eururo.2016.06.021
28. Abufaraj M, Grubmuller B, Zeitlinger M, Kramer G, Seitz C, Haitel A, et al. Prospective Evaluation of the Performance of [(68)Ga]Ga-Psma-11 Pet/Ct(Mri) for Lymph Node Staging in Patients Undergoing Superextended Salvage Lymph Node Dissection After Radical Prostatectomy. Eur J Nucl Med Mol Imaging (2019) 46(10):2169–77. doi: 10.1007/s00259-019-04361-0
29. Mena E, Lindenberg LM, Choyke PL. New Targets for Pet Molecular Imaging of Prostate Cancer. Semin Nucl Med (2019) 49(4):326–36. doi: 10.1053/j.semnuclmed.2019.02.001
31. Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, et al. Eau Guidelines on Prostate Cancer. Part Ii: Treatment of Advanced, Relapsing, and Castration-Resistant Prostate Cancer. Eur Urol (2014) 65(2):467–79. doi: 10.1016/j.eururo.2013.11.002
32. Garg I, Nathan MA, Packard AT, Kwon ED, Larson NB, Lowe V, et al. (11)C-Choline Positron Emission Tomography/Computed Tomography for Detection of Disease Relapse in Patients With History of Biochemically Recurrent Prostate Cancer and Prostate-Specific Antigen ≤0.1 Ng/Ml. J Cancer Res Ther (2021) 17(2):358–65. doi: 10.4103/jcrt.JCRT_373_19
33. Nappi AG, Ferrari C, Mammucci P, Rubini D, Lavelli V, Sardaro A, et al. [(18)F]Fluciclovine Pet/Ct Improves the Clinical Management of Early Recurrence Prostate Cancer Patients. Cancers (2022) 14(6):1461. doi: 10.3390/cancers14061461
34. Touijer KA, Michaud L, Alvarez HAV, Gopalan A, Kossatz S, Gonen M, et al. Prospective Study of the Radiolabeled Grpr Antagonist Bay86-7548 for Positron Emission Tomography/Computed Tomography Imaging of Newly Diagnosed Prostate Cancer. Eur Urol Oncol (2019) 2(2):166–73. doi: 10.1016/j.euo.2018.08.011
35. Gündoğan C, Güzel Y, Can C, Kaplan İ, Kömek H. Fapi-04 Uptake in Healthy Tissues of Cancer Patients in (68)Ga-Fapi-04 Pet/Ct Imaging. Contrast Media Mol Imaging (2021) 2021:9750080. doi: 10.1155/2021/9750080
36. Rayn KN, Elnabawi YA, Sheth N. Clinical Implications of Pet/Ct in Prostate Cancer Management. Trans Androl Urol (2018) 7(5):844–54. doi: 10.21037/tau.2018.08.26
37. Tan JSH, Goh CXY, Koh YS, Li Y, Tuan JKL, Chua ET, et al. (68)Gallium-Labelled Psma-Pet/Ct as a Diagnostic and Clinical Decision-Making Tool in Asian Prostate Cancer Patients Following Prostatectomy. Cancer Biol Med (2019) 16(1):157–66. doi: 10.20892/j.issn.2095-3941.2018.0288
38. Wang R, Shen G, Huang M, Tian R. The Diagnostic Role of (18)F-Choline, (18)F-Fluciclovine and (18)F-Psma Pet/Ct in the Detection of Prostate Cancer With Biochemical Recurrence: A Meta-Analysis. Front Oncol (2021) 11:684629. doi: 10.3389/fonc.2021.684629
39. Li R, Ravizzini GC, Gorin MA, Maurer T, Eiber M, Cooperberg MR, et al. The Use of Pet/Ct in Prostate Cancer. Prostate Cancer Prostatic Dis (2018) 21(1):4–21. doi: 10.1038/s41391-017-0007-8
40. Afshar-Oromieh A, Zechmann CM, Malcher A, Eder M, Eisenhut M, Linhart HG, et al. Comparison of Pet Imaging With a (68)Ga-Labelled Psma Ligand and (18)F-Choline-Based Pet/Ct for the Diagnosis of Recurrent Prostate Cancer. Eur J Nucl Med Mol Imaging (2014) 41(1):11–20. doi: 10.1007/s00259-013-2525-5
41. Morigi JJ, Stricker PD, van Leeuwen PJ, Tang R, Ho B, Nguyen Q, et al. Prospective Comparison of 18f-Fluoromethylcholine Versus 68ga-Psma Pet/Ct in Prostate Cancer Patients Who Have Rising Psa After Curative Treatment and Are Being Considered for Targeted Therapy. J Nucl Med (2015) 56(8):1185–90. doi: 10.2967/jnumed.115.160382
42. von Eyben FE, Picchio M, von Eyben R, Rhee H, Bauman G. (68)Ga-Labeled Prostate-Specific Membrane Antigen Ligand Positron Emission Tomography/Computed Tomography for Prostate Cancer: A Systematic Review and Meta-Analysis. Eur Urol Focus (2018) 4(5):686–93. doi: 10.1016/j.euf.2016.11.002
43. Bulbul JE, Grybowski D, Lovrec P, Solanki AA, Gabriel MS, Wagner RH, et al. Positivity Rate of [(18)F]Fluciclovine Pet/Ct in Patients With Suspected Prostate Cancer Recurrence at Psa Levels Below 1 Ng/Ml. Mol Imaging Biol (2022) 24(1):42–9. doi: 10.1007/s11307-021-01644-7
44. Garza D, Kandathil A, Xi Y, Subramaniam RM. 18f-Fluciclovine Pet/Ct Detection of Biochemical Recurrent Prostate Cancer in Patients With Psa Levels <2.00 Ng/Ml. Nucl Med Commun (2021) 42(8):907–13. doi: 10.1097/mnm.0000000000001412
45. Nanni C, Schiavina R, Brunocilla E, Boschi S, Borghesi M, Zanoni L, et al. 18f-Fluciclovine Pet/Ct for the Detection of Prostate Cancer Relapse: A Comparison to 11c-Choline Pet/Ct. Clin Nucl Med (2015) 40(8):e386–91. doi: 10.1097/rlu.0000000000000849
46. Hoffmann MA, von Eyben FE, Fischer N, Rosar F, Müller-Hübenthal J, Buchholz HG, et al. Comparison of [(18)F]Psma-1007 With [(68)Ga]Ga-Psma-11 Pet/Ct in Restaging of Prostate Cancer Patients With Psa Relapse. Cancers (2022) 14(6):1479. doi: 10.3390/cancers14061479
47. Lee H, Scheuermann JS, Young AJ, Doot RK, Daube-Witherspoon ME, Schubert EK, et al. Preliminary Evaluation of (68)Ga-P16-093, A Pet Radiotracer Targeting Prostate-Specific Membrane Antigen in Prostate Cancer. Mol Imaging Biol (2022). doi: 10.1007/s11307-022-01720-6
48. De Man K, Piron S, Van Laeken N, Delrue L, Fonteyne V, Lumen N, et al. Impact of 18F-PSMA-11 PET/CT on Management of Biochemical Recurrence and High-Risk Prostate Cancer Staging: 18F-PSMA-11 PET/CT and Impact on Prostate Cancer Management. Mol Imaging Biol. (2022). doi: 10.1007/s11307-022-01724-2
49. Abghari-Gerst M, Armstrong WR, Nguyen K, Calais J, Czernin J, Lin D, et al. A Comprehensive Assessment of (68)Ga-Psma-11 Pet in Biochemically Recurrent Prostate Cancer: Results From a Prospective Multicenter Study on 2,005 Patients. J Nucl Med (2022) 63(4):567–72. doi: 10.2967/jnumed.121.262412
50. Ceci F, Rovera G, Iorio GC, Guarneri A, Chiofalo V, et al. Event-Free Survival After 68 Ga-PSMA-11 PET/CT in Recurrent Hormone-Sensitive Prostate Cancer (HSPC) Patients Eligible for Salvage Therapy. Eur J Nucl Med Mol Imaging (2022). doi: 10.1007/s00259-022-05741-9
51. Mena E, Rowe SP, Shih JH, Lindenberg L, Turkbey B, Fourquet A, et al. Predictors of 18F-DCFPyL-PET/CT Positivity in Patients With Biochemical Recurrence of Prostate Cancer After Local Therapy. J Nucl Med. (2021). doi: 10.2967/jnumed.121.262347
52. Zhou X, Jiang X, Liu L, Wang X, Li C, Yao Y, et al. Evaluation of 18F-PSMA-1007 PET/CT in Prostate Cancer Patients With Biochemical Recurrence After Radical Prostatectomy. Transl Oncol (2022) 15(1):101292. doi: 10.1016/j.tranon.2021.101292
53. Christensen MT, Jochumsen MR, Klingenberg S, Sørensen KD, Borre M, Bouchelouche K, et al. Evaluation of Predictors of Biochemical Recurrence in Prostate Cancer Patients, as Detected by 68Ga-PSMA PET/CT. Diagnostics (Basel) (2022) 12(1):195. doi: 10.3390/diagnostics12010195
54. Filippi L, Bagni O, Crisafulli C, Cerio I, Brunotti G, Chiaravalloti A, et al. Detection Rate and Clinical Impact of Pet/Ct With (18)F-Facbc in Patients With Biochemical Recurrence of Prostate Cancer: A Retrospective Bicentric Study. Biomedicines (2022) 10(1):177. doi: 10.3390/biomedicines10010177
55. Zattoni F, Artioli P, Burei M, Chiaravalloti A, Chierichetti F, Donner D, et al. Detection Rate of 18F-Choline Positron Emission Tomography/computed Tomography in Patients With Non-Metastatic Hormone Sensitive and Castrate Resistant Prostate Cancer. Q J Nucl Med Mol Imaging (2021). doi: 10.23736/S1824-4785.21.03366-5
56. Ferraro DA, Rüschoff JH, Muehlematter UJ, Kranzbühler B, Müller J, Messerli M, et al. Immunohistochemical Psma Expression Patterns of Primary Prostate Cancer Tissue Are Associated With the Detection Rate of Biochemical Recurrence With (68)Ga-Psma-11-Pet. Theranostics (2020) 10(14):6082–94. doi: 10.7150/thno.44584
57. Dietlein F, Kobe C, Vázquez SM, Fischer T, Endepols H, Hohberg M, et al. An (89)Zr-Labeled Psma Tracer for Pet/Ct Imaging of Prostate Cancer Patients. J Nucl Med (2022) 63(4):573–83. doi: 10.2967/jnumed.121.262290
58. Ye S, Li H, Hu K, Li L, Zhong J, Yan Q, et al. Radiosynthesis and Biological Evaluation of 18f-Labeled Bispecific Heterodimer Targeted Dual Gastrin-Releasing Peptide Receptor and Prostate-Specific Membrane Antigen for Prostate Cancer Imaging. Nucl Med Commun (2022) 43(3):323–31. doi: 10.1097/mnm.0000000000001520
59. Wieser G, Popp I, Christian Rischke H, Drendel V, Grosu AL, Bartholomä M, et al. Diagnosis of Recurrent Prostate Cancer With Pet/Ct Imaging Using the Gastrin-Releasing Peptide Receptor Antagonist (68)Ga-Rm2: Preliminary Results in Patients With Negative or Inconclusive [(18)F]Fluoroethylcholine-Pet/Ct. Eur J Nucl Med Mol Imaging (2017) 44(9):1463–72. doi: 10.1007/s00259-017-3702-8
60. Chen R, Wang Y, Shi Y, Zhu Y, Xu L, Huang G, et al. Diagnostic Value of (18)F-Fdg Pet/Ct in Patients With Biochemical Recurrent Prostate Cancer and Negative (68)Ga-Psma Pet/Ct. Eur J Nucl Med Mol Imaging (2021) 48(9):2970–7. doi: 10.1007/s00259-021-05221-6
61. Eiber M, Maurer T, Souvatzoglou M, Beer AJ, Ruffani A, Haller B, et al. Evaluation of Hybrid (6)(8)Ga-Psma Ligand Pet/Ct in 248 Patients With Biochemical Recurrence After Radical Prostatectomy. J Nucl Med (2015) 56(5):668–74. doi: 10.2967/jnumed.115.154153
62. Afshar-Oromieh A, Avtzi E, Giesel FL, Holland-Letz T, Linhart HG, Eder M, et al. The Diagnostic Value of Pet/Ct Imaging With the (68)Ga-Labelled Psma Ligand Hbed-Cc in the Diagnosis of Recurrent Prostate Cancer. Eur J Nucl Med Mol Imaging (2015) 42(2):197–209. doi: 10.1007/s00259-014-2949-6
63. Hofman MS, Hicks RJ, Maurer T, Eiber M. Prostate-Specific Membrane Antigen Pet: Clinical Utility in Prostate Cancer, Normal Patterns, Pearls, and Pitfalls. Radiographics Rev Publ Radiol Soc North Am Inc (2018) 38(1):200–17. doi: 10.1148/rg.2018170108
64. Verburg FA, Pfister D, Heidenreich A, Vogg A, Drude NI, Voo S, et al. Extent of Disease in Recurrent Prostate Cancer Determined by [(68)Ga]Psma-Hbed-Cc Pet/Ct in Relation to Psa Levels, Psa Doubling Time and Gleason Score. Eur J Nucl Med Mol Imaging (2016) 43(3):397–403. doi: 10.1007/s00259-015-3240-1
65. Ceci F, Uprimny C, Nilica B, Geraldo L, Kendler D, Kroiss A, et al. (68)Ga-Psma Pet/Ct for Restaging Recurrent Prostate Cancer: Which Factors Are Associated With Pet/Ct Detection Rate? Eur J Nucl Med Mol Imaging (2015) 42(8):1284–94. doi: 10.1007/s00259-015-3078-6
66. Ceci F, Castellucci P, Graziani T, Farolfi A, Fonti C, Lodi F, et al. (68)Ga-Psma-11 Pet/Ct in Recurrent Prostate Cancer: Efficacy in Different Clinical Stages of Psa Failure After Radical Therapy. Eur J Nucl Med Mol Imaging (2019) 46(1):31–9. doi: 10.1007/s00259-018-4189-7
67. Eissa A, Elsherbiny A, Coelho RF, Rassweiler J, Davis JW, Porpiglia F, et al. The Role of 68ga-Psma Pet/Ct Scan in Biochemical Recurrence After Primary Treatment for Prostate Cancer: A Systematic Review of the Literature. Minerva Urol Nefrol J Urol Nephrol (2018) 70(5):462–78. doi: 10.23736/s0393-2249.18.03081-3
68. Yilmaz U, Komek H, Can C, Altindag S. The Role of [(68)Ga]Psma I&T in Biochemical Recurrence After Radical Prostatectomy: Detection Rate and the Correlation Between the Level of Psa, Gleason Score, and the Suvmax. Ann Nucl Med (2019) 33(8):545–53. doi: 10.1007/s12149-019-01360-x
69. Aydin AM, Haberal B, Artykov M, Bilen CY, Yazici S. Clinicopathological Predictors of Positive (68)Ga-Psma-11 Pet/Ct in Psa-Only Recurrence of Localized Prostate Cancer Following Definitive Therapy. Ann Nucl Med (2019) 33(5):326–32. doi: 10.1007/s12149-019-01340-1
70. Leitsmann C, Thelen P, Schmid M, Meller J, Sahlmann CO, Meller B, et al. Enhancing Psma-Uptake With Androgen Deprivation Therapy - a New Way to Detect Prostate Cancer Metastases? Int Braz J Urol (2019) 45(3):459–67. doi: 10.1590/s1677-5538.Ibju.2018.0305
71. Hohberg M, Kobe C, Tager P, Hammes J, Schmidt M, Dietlein F, et al. Combined Early and Late [(68)Ga]Psma-Hbed-Cc Pet Scans Improve Lesion Detectability in Biochemical Recurrence of Prostate Cancer With Low Psa Levels. Mol Imaging Biol :MIB (2019) 21(3):558–66. doi: 10.1007/s11307-018-1263-2
72. Morawitz J, Kirchner J, Hertelendy J, Loberg C, Schimmöller L, Dabir M, et al. Is There a Diagnostic Benefit of Late-Phase Abdomino-Pelvic Pet/Ct After Urination as Part of Whole-Body (68) Ga-Psma-11 Pet/Ct for Restaging Patients With Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy? EJNMMI Res (2022) 12(1):12. doi: 10.1186/s13550-022-00885-z
73. Uprimny C, Bayerschmidt S, Kroiss AS, Fritz J, Nilica B, Svirydenka H, et al. Early Injection of Furosemide Increases Detection Rate of Local Recurrence in Prostate Cancer Patients With Biochemical Recurrence Referred for (68)Ga-Psma-11 Pet/Ct. J Nucl Med (2021) 62(11):1550–7. doi: 10.2967/jnumed.120.261866
74. Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. Eau-Eanm-Estro-Esur-Siog Guidelines on Prostate Cancer. Part Ii-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur Urol (2021) 79(2):263–82. doi: 10.1016/j.eururo.2020.09.046
75. Wang Y, Chow DZ, Ebert E, Tajmir S, Scott JA, Palmer EL. Utility of (18)F-Fluciclovine Pet/Ct for Detecting Prostate Cancer Recurrence in Patients With Low (< 1 Ng/Ml) or Very Low (< 0.3 Ng/Ml) Prostate-Specific Antigen Levels. AJR Am J Roentgenol (2020) 215(4):997–1001. doi: 10.2214/ajr.19.22180
76. Giesel FL, Fiedler H, Stefanova M, Sterzing F, Rius M, Kopka K, et al. Psma Pet/Ct With Glu-Urea-Lys-(Ahx)-[(6)(8)Ga(Hbed-Cc)] Versus 3d Ct Volumetric Lymph Node Assessment in Recurrent Prostate Cancer. Eur J Nucl Med Mol Imaging (2015) 42(12):1794–800. doi: 10.1007/s00259-015-3106-6
77. Rauscher I, Maurer T, Beer AJ, Graner FP, Haller B, Weirich G, et al. Value of 68ga-Psma Hbed-Cc Pet for the Assessment of Lymph Node Metastases in Prostate Cancer Patients With Biochemical Recurrence: Comparison With Histopathology After Salvage Lymphadenectomy. J Nucl Med (2016) 57(11):1713–9. doi: 10.2967/jnumed.116.173492
78. Kroenke M, Schweiger L, Horn T, Haller B, Schwamborn K, Wurzer A, et al. Validation of (18)F-Rhpsma-7 and (18)F-Rhpsma-7.3 Pet Imaging Results With Histopathology From Salvage Surgery in Patients With Biochemical Recurrence of Prostate Cancer. J Nucl Med (2022). doi: 10.2967/jnumed.121.263707
79. Maurer T, Gschwend JE, Rauscher I, Souvatzoglou M, Haller B, Weirich G, et al. Diagnostic Efficacy of (68)Gallium-Psma Positron Emission Tomography Compared to Conventional Imaging for Lymph Node Staging of 130 Consecutive Patients With Intermediate to High Risk Prostate Cancer. J Urol (2016) 195(5):1436–43. doi: 10.1016/j.juro.2015.12.025
80. Maurer T, Eiber M, Schwaiger M, Gschwend JE. Current Use of Psma-Pet in Prostate Cancer Management. Nat Rev Urol (2016) 13(4):226–35. doi: 10.1038/nrurol.2016.26
81. Sprute K, Kramer V, Koerber SA, Meneses M, Fernandez R, Soza-Ried C, et al. Diagnostic Accuracy of (18)F-Psma-1007 Pet/Ct Imaging for Lymph Node Staging of Prostate Carcinoma in Primary and Biochemical Recurrence. J Nucl Med (2021) 62(2):208–13. doi: 10.2967/jnumed.120.246363
82. Mingels C, Bohn KP, Rominger A, Afshar-Oromieh A, Alberts I. Diagnostic Accuracy of [(18)F]Psma-1007 Pet/Ct in Biochemical Recurrence of Prostate Cancer. Eur J Nucl Med Mol Imaging (2022) 49:2436–44. doi: 10.1007/s00259-022-05693-0
83. Zhou J, Gou Z, Wu R, Yuan Y, Yu G, Zhao Y. Comparison of Psma-Pet/Ct, Choline-Pet/Ct, Naf-Pet/Ct, Mri, and Bone Scintigraphy in the Diagnosis of Bone Metastases in Patients With Prostate Cancer: A Systematic Review and Meta-Analysis. Skeletal Radiol (2019) 48(12):1915–24. doi: 10.1007/s00256-019-03230-z
84. Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA. The 2014 International Society of Urological Pathology (Isup) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am J Surg Pathol (2016) 40(2):244–52. doi: 10.1097/pas.0000000000000530
85. Yakar D, Noordzij W, Kwee TC. Potential Causes of False-Negative Interpretations in 68ga-Psma Pet/Ct for the Detection of Local and Recurrent Prostate Cancer: An Underexposed Issue. Clin Nucl Med (2019) 45(1):e32-5. doi: 10.1097/rlu.0000000000002750
86. Prasad V, Steffen IG, Diederichs G, Makowski MR, Wust P, Brenner W. Biodistribution of [(68)Ga]Psma-Hbed-Cc in Patients With Prostate Cancer: Characterization of Uptake in Normal Organs and Tumour Lesions. Mol Imaging Biol MIB (2016) 18(3):428–36. doi: 10.1007/s11307-016-0945-x
87. Ristau BT, O’Keefe DS, Bacich DJ. The Prostate-Specific Membrane Antigen: Lessons and Current Clinical Implications From 20 Years of Research. Urol Oncol (2014) 32(3):272–9. doi: 10.1016/j.urolonc.2013.09.003
88. Perry E, Talwar A, Sharma S, O’Connor D, Wong LM, Taubman K, et al. Non-Prostate Cancer Tumours: Incidence on (18)F-Dcfpyl Psma Pet/Ct and Uptake Characteristics in 1445 Patients. Eur J Nucl Med Mol Imaging (2022). doi: 10.1007/s00259-022-05721-z
89. Afshar-Oromieh A, Malcher A, Eder M, Eisenhut M, Linhart HG, Hadaschik BA, et al. Pet Imaging With a [68ga]Gallium-Labelled Psma Ligand for the Diagnosis of Prostate Cancer: Biodistribution in Humans and First Evaluation of Tumour Lesions. Eur J Nucl Med Mol Imaging (2013) 40(4):486–95. doi: 10.1007/s00259-012-2298-2
90. Pfob CH, Ziegler S, Graner FP, Kohner M, Schachoff S, Blechert B, et al. Biodistribution and Radiation Dosimetry of (68)Ga-Psma Hbed Cc-a Psma Specific Probe for Pet Imaging of Prostate Cancer. Eur J Nucl Med Mol Imaging (2016) 43(11):1962–70. doi: 10.1007/s00259-016-3424-3
91. Afshar-Oromieh A, Hetzheim H, Kubler W, Kratochwil C, Giesel FL, Hope TA, et al. Radiation Dosimetry of (68)Ga-Psma-11 (Hbed-Cc) and Preliminary Evaluation of Optimal Imaging Timing. Eur J Nucl Med Mol Imaging (2016) 43(9):1611–20. doi: 10.1007/s00259-016-3419-0
92. Krohn T, Verburg FA, Pufe T, Neuhuber W, Vogg A, Heinzel A, et al. [(68)Ga]Psma-Hbed Uptake Mimicking Lymph Node Metastasis in Coeliac Ganglia: An Important Pitfall in Clinical Practice. Eur J Nucl Med Mol Imaging (2015) 42(2):210–4. doi: 10.1007/s00259-014-2915-3
93. Kinoshita Y, Kuratsukuri K, Landas S, Imaida K, Rovito PM Jr., Wang CY, et al. Expression of Prostate-Specific Membrane Antigen in Normal and Malignant Human Tissues. World J Surg (2006) 30(4):628–36. doi: 10.1007/s00268-005-0544-5
94. Gordon IO, Tretiakova MS, Noffsinger AE, Hart J, Reuter VE, Al-Ahmadie HA. Prostate-Specific Membrane Antigen Expression in Regeneration and Repair. Mod Pathol Off J United States Can Acad Pathol Inc (2008) 21(12):1421–7. doi: 10.1038/modpathol.2008.143
95. Ardies PJ, Gykiere P, Goethals L, De Mey J, De Geeter F, Everaert H. Psma Uptake in Mediastinal Sarcoidosis. Clin Nucl Med (2017) 42(4):303–5. doi: 10.1097/rlu.0000000000001543
96. Froehner M, Toma M, Zophel K, Novotny V, Laniado M, Wirth MP. Psma-Pet/Ct-Positive Paget Disease in a Patient With Newly Diagnosed Prostate Cancer: Imaging and Bone Biopsy Findings. Case Rep Urol (2017) 2017:1654231. doi: 10.1155/2017/1654231
97. Gykiere P, Goethals L, Everaert H. Healing Sacral Fracture Masquerading as Metastatic Bone Disease on a 68ga-Psma Pet/Ct. Clin Nucl Med (2016) 41(7):e346–7. doi: 10.1097/rlu.0000000000001222
98. Vamadevan S, Le K, Bui C, Mansberg R. Incidental Psma Uptake in an Undisplaced Fracture of a Vertebral Body. Clin Nucl Med (2017) 42(6):465–6. doi: 10.1097/rlu.0000000000001599
99. Artigas C, Otte FX, Lemort M, van Velthoven R, Flamen P. Vertebral Hemangioma Mimicking Bone Metastasis in 68ga-Psma Ligand Pet/Ct. Clin Nucl Med (2017) 42(5):368–70. doi: 10.1097/rlu.0000000000001631
100. Kanthan GL, Izard MA, Emmett L, Hsiao E, Schembri GP. Schwannoma Showing Avid Uptake on 68ga-Psma-Hbed-Cc Pet/Ct. Clin Nucl Med (2016) 41(9):703–4. doi: 10.1097/rlu.0000000000001281
101. Derlin T, Kreipe HH, Schumacher U, Soudah B. Psma Expression in Tumor Neovasculature Endothelial Cells of Follicular Thyroid Adenoma as Identified by Molecular Imaging Using 68ga-Psma Ligand Pet/Ct. Clin Nucl Med (2017) 42(3):e173–e4. doi: 10.1097/rlu.0000000000001487
102. Rowe SP, Gorin MA, Hammers HJ, Som Javadi M, Hawasli H, Szabo Z, et al. Imaging of Metastatic Clear Cell Renal Cell Carcinoma With Psma-Targeted (1)(8)F-Dcfpyl Pet/Ct. Ann Nucl Med (2015) 29(10):877–82. doi: 10.1007/s12149-015-1017-z
103. Rhee H, Blazak J, Tham CM, Ng KL, Shepherd B, Lawson M, et al. Pilot Study: Use of Gallium-68 Psma Pet for Detection of Metastatic Lesions in Patients With Renal Tumour. EJNMMI Res (2016) 6(1):76. doi: 10.1186/s13550-016-0231-6
104. Perez PM, Flavell RR, Kelley RK, Umetsu S, Behr SC. Heterogeneous Uptake of 18f-Fdg and 68ga-Psma-11 in Hepatocellular Carcinoma. Clin Nucl Med (2019) 44(3):e133–e5. doi: 10.1097/rlu.0000000000002452
105. Roland A, Drouet C, Boulahdour H, Cochet A, De Bari B. Unusual Uptakes on (18)F-Fluorocholine Positron Emission Tomography/Computed Tomography (Pet/Ct): A Retrospective Study of 368 Prostate Cancer Patients Referred for a Biochemical Recurrence or an Initial Staging. Quant Imaging Med Surg (2021) 11(1):172–82. doi: 10.21037/qims-19-981
Keywords: prostate cancer, biochemical recurrence, PET/CT- Positron Emission Tomography Computed Tomography, imaging
Citation: Jiang J, Tang X, Pu Y, Yang Y, Yang C, Yang F, Tian Y, Li J, Sun H, Zhao S and Chen L (2022) The Value of Multimodality PET/CT Imaging in Detecting Prostate Cancer Biochemical Recurrence. Front. Endocrinol. 13:897513. doi: 10.3389/fendo.2022.897513
Received: 16 March 2022; Accepted: 26 April 2022;
Published: 27 May 2022.
Edited by:
Ihtisham Bukhari, Fifth Affiliated Hospital of Zhengzhou University, ChinaReviewed by:
Chunlei Han, Turku PET Centre, FinlandXilin Sun, The Fourth Hospital of Harbin Medical University, China
Copyright © 2022 Jiang, Tang, Pu, Yang, Yang, Yang, Tian, Li, Sun, Zhao and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Long Chen, bG9uZWNoZW4xOTgzQGhvdG1haWwuY29t; Hua Sun, NjQ5NzkwODI3QHFxLmNvbQ==; Sheng Zhao, ODM5MDY4MUBxcS5jb20=
†These authors have contributed equally to this work