
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 02 May 2022
Sec. Pediatric Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.868944
This article is part of the Research TopicExploring Obesity Risk, Prevention, and Research Innovation in the First 2000 Days of LifeView all 8 articles
 Mahalakshmi Ekambareshwar1,2*
Mahalakshmi Ekambareshwar1,2* Huilan Xu3
Huilan Xu3 Chris Rissel1,2Louise Baur1,2,4,5
Chris Rissel1,2Louise Baur1,2,4,5 Sarah Taki1,3Seema Mihrshahi1,6
Sarah Taki1,3Seema Mihrshahi1,6 Li Ming Wen1,2,3
Li Ming Wen1,2,3Background: Participant engagement with program interventions is vital to support intended behaviour changes and outcomes. The aim of this research was to investigate participant engagement with the Communicating Healthy Beginnings Advice by Telephone (CHAT) program, an early childhood obesity prevention program that included interventions for promoting healthy infant feeding practices and obesity-protective behaviours via telephone, and whether engagement with the telephone support program varied by participants’ sociodemographic characteristics.
Methods: This study used de-identified CHAT program data of participants who received the interventions via telephone. Data analysed included 1) participant engagement in telephone support from late pregnancy to 12 months of child's age, 2) demographic characteristics collected at late pregnancy and 3) intervention providers’ observations and notes (qualitative data) for 10 participants from each engagement group (low, medium, high) to explore issues discussed during telephone support.
Results: Call completion rate by participants was above sixty percent for all six stages of the telephone support program with more than half of the participants (57%) demonstrating high level of engagement. We found that participants’ country of birth, employment status and annual household income were predictors of engagement with the telephone support provided in the CHAT program. The odds of participants’ engagement with the telephone support program were 1.68 times higher for Australian born (95% CI 1.07 – 2.62), 1.63 times higher for participants who were employed (95% CI 1.01 – 2.66) and 1.63 times higher for participants with annual household income ≥AUD$80,000 (95% CI 1.02 – 2.60).
Conclusions: Participant engagement with the program interventions was good. Participants’ engagement with the telephone support program was significantly associated with certain socio-demographic characteristics. Australian born participants, and participants associated with higher household income and employment engaged significantly more with the telephone support provided in the CHAT program. Additionally, the program engaged more participants older than 30 years of age and those who spoke English at home. The program provided unintended personal benefits to some participants with high engagement level due to their various psychosocial needs such as domestic violence, mental health and sleep related issues. Although not an intended benefit of the intervention, psychosocial needs of participants were met which was a likely factor for mothers’ engagement with the program. This is an important factor that needs to be considered while implementing future programs or scale up of this program.
Obesity is recognised as a global health problem and prevention of obesity is a public health priority. In general, prevention research has received increased attention. For over a decade, in the case of early childhood obesity prevention interventions, the focus has been to commence early from when women are pregnant (1, 2). However, recruitment of participants to a program and keeping mothers and caregivers of infants engaged at a busy time of their lives remains a challenge (3–5).
Although face-to-face delivery of child obesity prevention interventions has been widely accepted by participants, some barriers have been identified that may inhibit uptake and attendance. Barriers include lack of transportation and travel time (6); poor enrolment and attendance (7); feelings of stigmatisation, fear and guilt (4, 7); and fear of being judged in face-to-face sessions for not possessing the desired skills (8, 9). To overcome the challenge of requiring participants’ presence at designated locations for in-person participation, and to make it less onerous on participants, more recently, interventions have been delivered remotely via telephone calls or text messages (1, 2). Intervention delivery via telephone calls provides participants with an opportunity to receive personalised health advice and to resolve questions about the program content (10, 11). Intervention delivery via a combination of telephone calls and text messages has the advantage of reminding participants via text messages about the interventions delivered via telephone calls (10, 11).
The Communicating Healthy Beginnings Advice by Telephone trial (CHAT program) is a three-arm randomised controlled trial (RCT) that delivered stage-based health behaviour change messages to women via nurse-led telephone calls or text messages (2). Intervention delivery commenced from the third trimester of pregnancy to 12 months of child’s age and beyond. In behavioural intervention trials, it is important to evaluate the process that occurred during intervention delivery and the extent to which participants engaged with the interventions (12). This research was one of four studies solely conducted to evaluate the process of delivering the CHAT program. There were other studies that evaluated the clinical outcomes of the CHAT trial (13, 14). In brief, telephone support was effective in promoting the appropriate timing of the introduction of solid foods and early-start tummy time (at 6 months). Both the nurse-led telephone support and SMS interventions were effective in reducing screen time and bottle use at bedtime (at 12 months) (13). At two years of child's age, the telephone or SMS support intervention was effective in increasing ‘no bottle use’ at bedtime, telephone support showed more effects than SMS on reducing screen time and eating behaviours (14). Meticulously describing the actual exposure to the intervention, the engagement experience of those exposed to the intervention (participants) and the intervention itself forms part of process evaluation, all of which are crucial towards understanding the success of interventions (15).
Program engagement is crucial to any intervention delivery for participants to adapt and to practice the intended behaviours (3, 4). Participant engagement is pivotal to participants’ adherence to intended behaviour changes and outcomes. In fact, dose-response is often expressed as dose received, a characteristic of the target audience that assesses the engagement of participants with the intervention (16). Participant engagement has been investigated in community-based childhood obesity prevention or treatment programs (7, 8); in digital/online delivery (17, 18); via web where more intense engagement led to better outcomes (19); and via mobile phone app where engagement level positively correlated with the combined use of app, email and intervention exposure for a longer period (17, 18). Remote contact with a health professional via email, telephone or text messages positively influenced enrolment in program (20).
To our knowledge, engagement of participants in infant obesity prevention interventions delivered via telephone calls has not been investigated, and characteristics of those who were engaged remain unexplored. Although telephone calls and text messages were used to deliver interventions in the CHAT program, it is not possible to measure actual engagement with text messages since we cannot know if participants actually received, opened and read the text messages (21). The purpose of this research is to investigate engagement of participants with the telephone support provided in the CHAT program, to inform the development of future programs. We evaluated whether participants’ engagement with the program was associated with their sociodemographic characteristics.
The CHAT program was conducted across four Local Health Districts (LHDs) within New South Wales (NSW) in Australia. Three LHDs were located within metropolitan Sydney and one LHD was in regional NSW, where pregnant women were recruited at eight hospital sites between February and July 2017. The study protocol, eligibility criteria, recruitment process and outcomes are reported in detail elsewhere (2, 11, 13, 20). In brief, CHAT is a three-arm RCT that compares: mailed Healthy Beginnings booklets plus telephone support (telephone); to mailed Healthy Beginnings booklets plus text messages; to the control arm. Interventions were stage-based and provided at six time points following key developmental milestones from the antenatal period (third trimester) until the end of first year of the infant’s life. The control arm participants were mailed general infant safety promotion materials. Usual care on infant development and safety is delivered by local child and family health services that are not mandatory.
Briefly, the focus of the stage-based interventions that were delivered to participants via telephone calls from recruitment until six months of children’s age were on breastfeeding, introduction of “tummy” time (allowing babies time lying prone on their abdomen while they are awake) within four weeks, introduction of solid food at six months. In addition to the above, between six and twelve months of children’s age, the focus of the intervention was on drinking from a cup, no screen time for children, children’s activity time and not offering food for reward to children.
The key messages of the telephone interventions intended to influence target behaviours were: an increased breastfeeding rate, and duration at 6 months and at 12 months of children’s age; an appropriate timing of introduction of solids at 6 months; the commencement of “tummy time” within 4 weeks of birth and increased rate of practising “tummy time” at 6 months; an increased rate of using cup and drinking water at 12 months; nil or reduced child TV screen time at 12 months of children’s age. The outcomes of the CHAT program, including child BMI z score at 12 months, are reported elsewhere (13).
Participants’ socio-demographic characteristics were assessed at baseline. The demographic summary of all CHAT participants is published elsewhere (13). Questions from the NSW Adult Population Health Survey 2003 were used to measure participants’ sociodemographic characteristics (22), which included participants’ age, country of birth, language spoken at home, education level, annual household income, employment and marital status, and parity of participants. Participants’ demographic and socioeconomic information were categorised into groups based on their engagement level.
We measured participants’ engagement as the number of completed telephone support calls recorded on the project implementation database using Research Electronic Data Capture (REDCap) (23). Telephone calls were considered completed (and included in our assessment of engagement) where participants answered the calls, and the intervention components were delivered as intended and recorded by the intervention providers. Where calls were directed to voicemail messages or were interrupted, these were not included in the number of completed calls. We did not include the amount of time spent on calls in our assessment of engagement since in some instances the intervention providers spent time on participants’ contextual/psychosocial issues (11, 24). Four staged telephone calls were delivered to participants until six months of child’s age, and two more between 6 and 12 months of child’s age.
We assessed engagement level of participants with the telephone intervention based on the number of telephone calls answered in the first six stages of the intervention i.e., from antenatal stage to 12 months of child’s age. We categorised engagement into three levels based on the number of calls answered - participants who answered less than three calls (lowest third) were regarded as ‘low engagement’, those who answered three to four calls (middle third) as ‘medium engagement’ and greater than four calls (upper third) as ‘high engagement’.
Statistical analyses were carried out using Stata 13 (25). All P-values are two sided and statistical significance was set at the 5% level. To examine the associations between participants’ baseline socio-demographic characteristics and their engagement in telephone support, Pearson’s Chi-squared tests were conducted using data from the telephone support group. Number and percentage were reported. Ordinal logistic regression models (Proportional odds model) were built to determine whether participants’ socio-demographic characteristics were associated with their level of engagement in telephone support intervention at 12 months of child's age. Participants’ socio-demographic variables that were significant on bivariate analyses using Pearson’s chi-squared tests with P<0.25 were entered in the ordinal logistic regression models. The least significant variables were progressively dropped until only those with P<0.05 remained. Variables dropped from the model were then entered into the model individually to assess for confounding factors. The Brant test of proportionality of odds showed that parallel regression assumption was not violated and indicated the proportional odds mode was appropriate. Adjusted odds ratio (AOR) with 95% confidence interval (CI) were calculated.
We randomly selected 10 participants from each engagement group (low, medium, high) to further explore intervention providers’ notes on these participants, and to see whether the issues raised and discussed during the telephone calls varied with participants’ engagement levels. Participants’ notes were recorded by intervention providers on REDCap. These data were extracted and transferred to NVivo for analysis (26).
Table 1 provides the number of staged telephone calls completed by participants in the telephone support program. There were a total of 1630 telephone calls answered by 386 participants in the telephone support group for the first six interventions delivered from the third trimester of pregnancy to 12 months’ of child’s age. An average of four calls were completed by each participant. The completion rate was above 60% for all 6 stages of telephone support, the highest completion (87%) at stage 2 (one month of child’s age) and the lowest completion (61%) at stage 1 (late pregnancy).
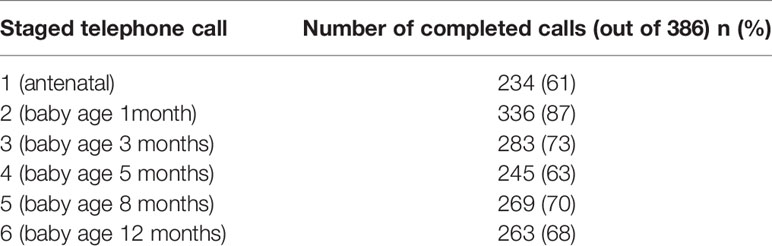
Table 1 Number of completed telephone calls for each stage of intervention.
Figure 1 represents the engagement level of participants based on the number of staged calls answered. Of the 386 participants in the telephone support group, 219 women answered more than four of the six calls and demonstrated high level of engagement with the telephone support program. 95 participants had mid-level of engagement and 72 had low level of engagement with the program.
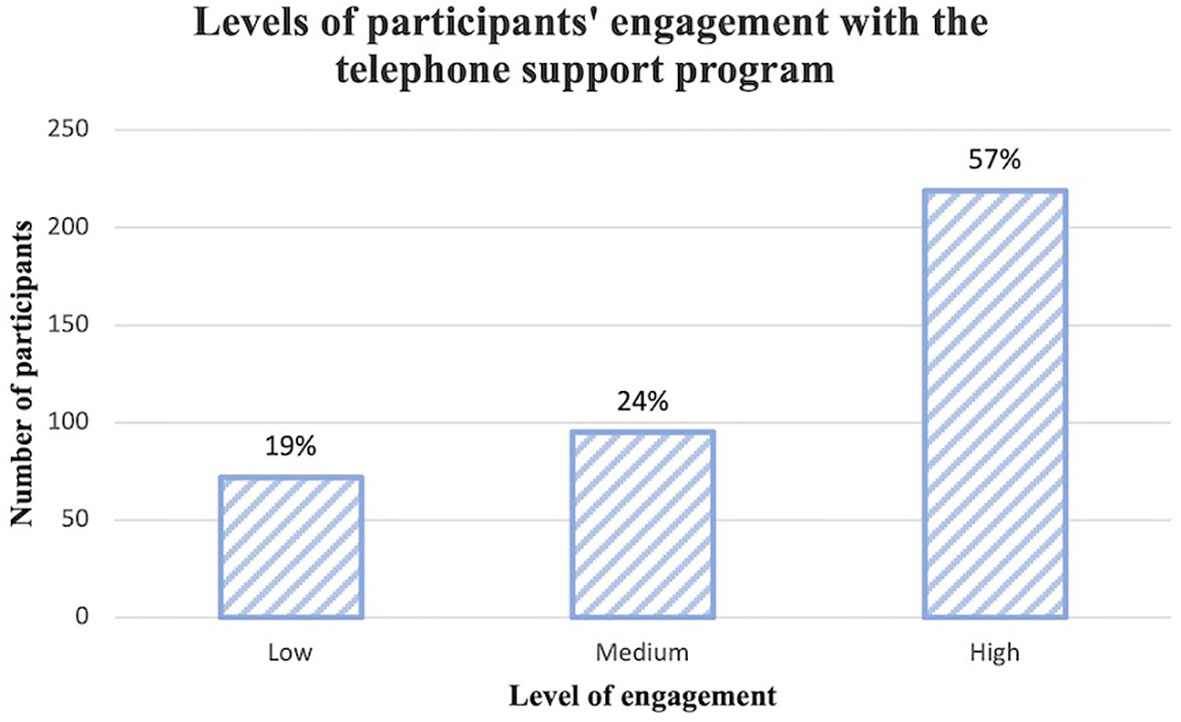
Figure 1 Levels of participants’ engagement with the telephone support program.
Table 2 shows that, using bivariate analyses, mothers’ age, country of birth, language spoken at home, educational level, employment status and annual household income were significantly associated with their level of engagement with the telephone support program at 12 months of child's age. Marital status and parity of mother were not significantly associated with their level of engagement with the program.
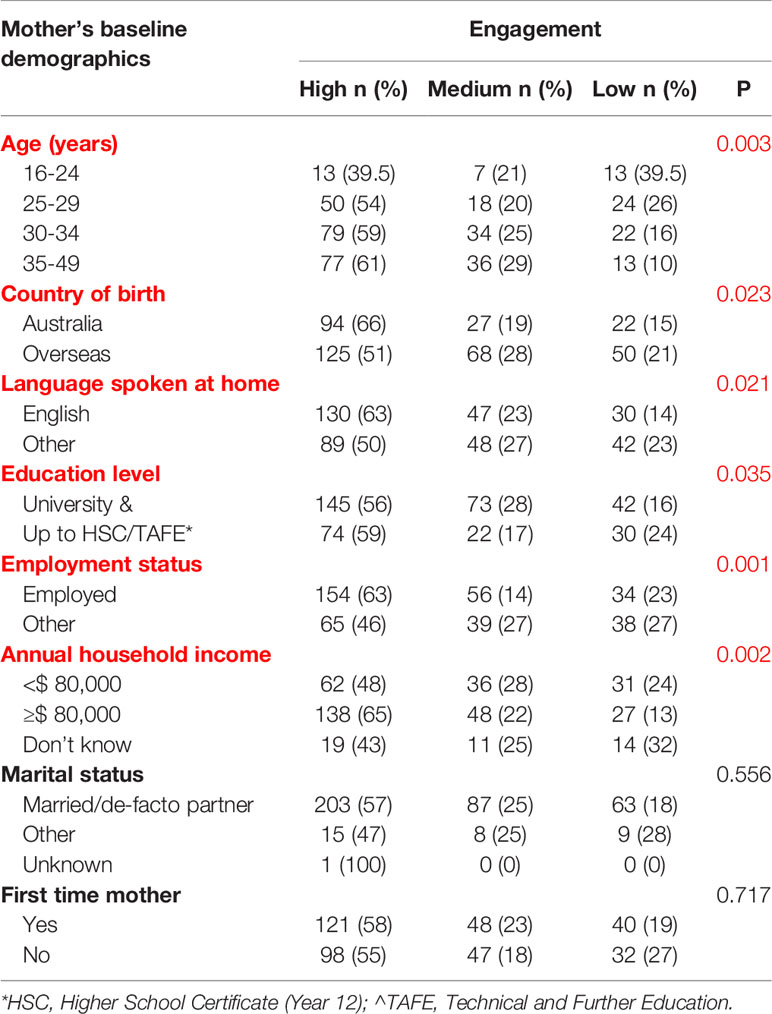
Table 2 Comparisons of the socio-demographic characteristics between those who had high, medium and low levels of engagement.
In a multivariable model the odds of participants’ engagement with the telephone support program were 1.68 times higher for Australian born (95% CI 1.07 – 2.62), 1.63 times higher for participants who were employed (95% CI 1.01 – 2.66) and 1.63 times higher for participants with higher annual household income (95% CI 1.02 – 2.60) (Table 3).
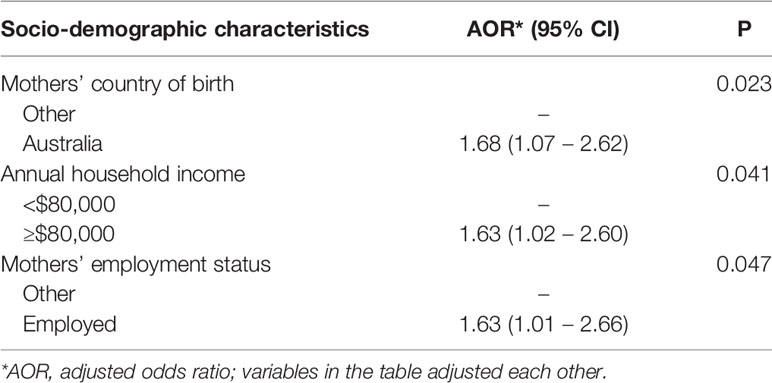
Table 3 Associations of participant socio-demographic characteristics with engagement in telephone support program using ordinal logistic regression.
For the sample of 30 participants from the three engagement level groups (low, medium, high), intervention providers’ notes demonstrated that a range of issues, including psychosocial concerns, were discussed at the time of intervention delivery. Concerns that were raised and recorded by the intervention providers included: medical issues (12); mental health issues (1); baby’s sleep and settling (11); return to work (8); referral to other services (8); and lack of support (8) (Table 4). Figure 2 represents concerns that were raised by participants based on the three levels of engagement: participants in the high engagement category discussed various issues outside of the intervention content than those in the lower engagement categories.
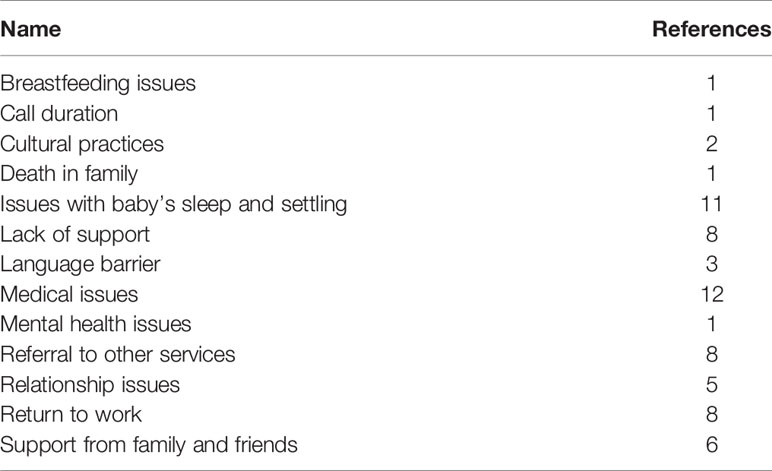
Table 4 Representation of themes discussed during intervention provision from intervention providers’ notes on a sample of participants (N=30) using NVivo.
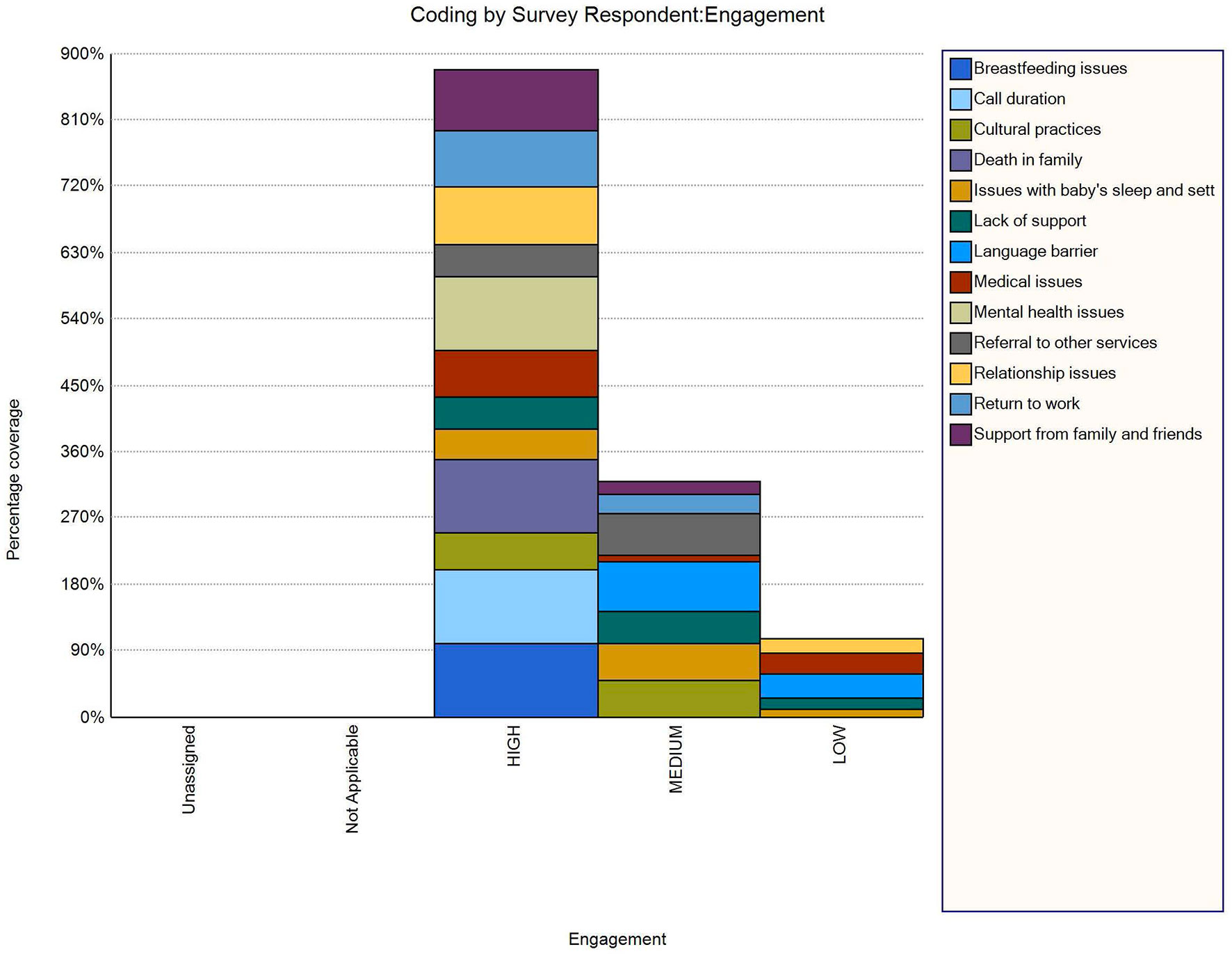
Figure 2 Representation of issues discussed during intervention provision by participants’ engagement level and as recorded by intervention providers who delivered telephone support.
To our knowledge, engagement of participants in infant obesity prevention interventions delivered via telephone calls was not previously investigated, and sociodemographic characteristics of those who engaged were not previously reported. We set out to explore participants’ engagement with infant feeding interventions delivered via telephone and whether engagement was related to participants’ sociodemographic characteristics. Overall, participant engagement with the program interventions was good with more than half of the participants (57%) demonstrating high level of engagement by answering more than four of the six calls; and only less than one-fifth of participants (19%) answering less than 3 calls. We found that participants born in Australia, who were employed, and had a higher annual household income were significantly more likely to engage with telephone calls in the CHAT program. To our knowledge, this is the first study to measure the relationship between engagement and participants’ characteristics in a trial that delivered infant feeding practices via telephone calls.
Participants in the 30-49 years age group were more likely to engage with the CHAT program. We were not able to locate a similar finding regarding participants’ engagement in the childhood obesity prevention literature. However, the positive association of participant engagement with increasing age is consistent with studies in the general population showing that interventions delivered digitally (27) or via eHealth (28) demonstrated increased uptake of and satisfaction with interventions with increasing age.
Employment and household income of participants were positively associated with engagement in the CHAT program, with higher level of engagement by participants with annual income ≥AUD$80,000. Previous studies have attributed higher eHealth service attendance to higher socioeconomic status and educational attainment (28), and families with lower socioeconomic status attended treatment infrequently in an infant obesity management intervention (6). Low socioeconomic status has been a strong predictor of program non-completion in paediatric and youth weight management programs (29–31). However, in a community-based weight management study, families with lower education levels achieved better outcomes with a greater number of sessions (32). Consistent with previous literature participants from higher socio-economic background appeared to seek out ‘reliable’ information (8).
Participants who spoke English at home were more likely to engage with the CHAT program in comparison to those participants who spoke other languages. Previous research has shown that ethnicity (Anglo-ethnic and largely identified by language spoken) was positively associated with access and uptake of eHealth services (28). Engagement and access to mainstream services and interventions have been particularly challenging for participants from other cultural backgrounds who speak a language other than English as their main language (9) and have been associated with inconsistent program attendance (29, 33–35). Consequently, there has been a need for cultural adaptation and translation of interventions to reach broader populations (36).
It is evident from our analyses of the intervention providers’ notes that demographic characteristics were not the only indicators of engagement with the CHAT program. Participants with high engagement level had various psychosocial needs such as addressing domestic violence, mental health, sleep related and other issues. Psychosocial characteristics are of great interest for subsequent studies to predict engagement. During the later stages, mainly participants with health and personal concerns sought help and found value in telephone calls and these calls were quite lengthy (24). Although most calls were under 30 minutes, participant-driven telephone conversations with personal concerns led to longer call duration which in some instances were more than an hour (24). Psychosocial concerns that participants were most concerned about, included medical issues; mental health issues; baby’s sleep and settling; participants’ return to work; referral to other services; and general lack of support available to them. Addressing the psychosocial needs of participants was not the primary focus of the CHAT program but clearly there is a need.
Recruitment of participants to an obesity prevention program and keeping mothers and caregivers of infants engaged at a busy time of their lives remains a challenge that could be overcome by telephone calls. The findings of this study indicate that without addressing the challenges that participants may experience at the time of intervention delivery, it is highly unlikely to engage participants to address factors related to their child’s health such as desirable behaviours around nutrition, physical activity and sleep. This evaluation of engagement with the telephone support, as part of the broader process evaluation of the CHAT program, has shown that there were unintended personal benefits that participants gained from the program. Despite the efforts of intervention providers to contact participants at a time nominated by participants that was convenient to them, intervention providers were unable to reach participants and sometimes up to 10 telephone calls were made before a successful attempt to reach a participant (24). To increase engagement, the program provided participants with the opportunity to nominate their preferred times to receive telephone calls.
Participant engagement has been investigated in child obesity prevention or treatment programs that were community-based (7, 8) or delivered digitally or on-line (17, 18), via the internet (19); via mobile phone app and email (17) or via email, telephone or text messages (27). Engagement with child obesity prevention interventions has been facilitated when the frequency of and access to intervention delivery was more intense via the web (19, 32), and a combination of app and email were employed for intervention delivery enabling regular push notifications for intervention exposure (17). Development of programs delivered remotely and flexibly via mobile or web has the potential to minimise participant burden and increase program scalability (3). A web-based behaviour change program delivered to adults for healthy body weight and lifestyle established a strong dose-response relationship between the number and intensity of counselling sessions and behaviour change outcomes (19).
Service engagement and program utilisation involves a degree of initiative on the part of parents as well as attempts by service providers to engage with them (9). With regards to successful approaches to engaging parents, the existing research base is far from robust. Parents want services that are reliable, accessible, sensitive to individual needs and well-co-ordinated (9). More research needs to be done on parents’ own help-seeking behaviours and attitudes (9, 37). Despite current availability of mainstream services for psychosocial support, this research has highlighted the need for additional support to meet the psychosocial needs of mothers with infants, for programs such as the CHAT to achieve the intended outcomes. It is important to recognise this for future programs or for scale up of the CHAT program.
The main limitation of this study is that we have used secondary data to measure engagement of participants’ engagement with the CHAT program. However, to overcome this limitation we have incorporated analysis of notes taken by intervention providers at the time of intervention delivery. To our knowledge, there is scant published literature on engagement with interventions delivered for obesity prevention practices to draw comparisons, we have attempted to draw comparisons with the limited literature available. Families with scarce resources and without access to telephone were not provided with an opportunity to engage in this program. Providing participants with a range of options to access the program could be considered in future programs.
Participants’ engagement with the telephone support provided in the CHAT program was good. Engagement with the program interventions and the anticipated behaviour changes were positively associated with certain socio-demographic characteristics. Australian born participants, and participants from a higher socio-economic background associated with household income and employment engaged significantly more with the telephone support provided in the CHAT program. Additionally, the program engaged more participants older than 30 years of age and those who spoke English at home. The program provided unintended personal benefits to some participants with high engagement level due to their various psychosocial needs such as domestic violence, mental health, sleep related issues, which was revealed as part of this evaluation of engagement with the telephone support of the CHAT program. There is limited research on participant engagement and on how to maintain engagement especially in behaviour change programs delivered for infant obesity prevention.
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Sydney Local Health District Ethics Committee (approval number X16-0360). The patients/participants provided their written informed consent to participate in this study.
LW, CR, and LB conceived and designed the original Healthy Beginnings and CHAT RCT project. ME and HX conducted the data analysis with input from LW and CR. ME received doctoral supervision from CR, LB, LW, SM, and ST. ME drafted the manuscript and all authors critically edited and approved the final version.
The CHAT RCT is a partnership project funded by the New South Wales Health Translational Research Grant Scheme 2016(TRGS 200) and Sydney Local Health District (SLHD). ME is a PhD scholar funded by the University of Sydney Postgraduate Award scheme.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CHAT, Communicating Healthy Beginnings Advice by Telephone; RCT, randomised controlled trial; NSW, New South Wales; LHD, Local Health District; AOR, Adjusted Odds Ratio; CI, Confidence Interval; REDCap, Research Electronic Data Capture.
1. Wen LM, Rissel C, Xu H, Taki S, Smith W, Bedford K, et al. Linking Two Randomised Controlled Trials for Healthy Beginnings©: Optimising Early Obesity Prevention Programs for Children Under 3 Years. BMC Public Health (2019) 19(1):1–10. doi: 10.1186/s12889-019-7058-9
2. Wen LM, Rissel C, Baur LA, Hayes AJ, Xu H, Whelan A, et al. A 3-Arm Randomised Controlled Trial of Communicating Healthy Beginnings Advice by Telephone (CHAT) to Mothers With Infants to Prevent Childhood Obesity. BMC Public Health (2017) 17(1):79. doi: 10.1186/s12889-016-4005-x
3. Morgan P, Jones R, Collins C, Hesketh K, Young M, Burrows T, et al. Practicalities and Research Considerations for Conducting Childhood Obesity Prevention Interventions With Families. Children (2016) 3(4):24. doi: 10.3390/children3040024
4. Mytton J, Ingram J, Manns S, Thomas J. Facilitators and Barriers to Engagement in Parenting Programs. Health Educ Behav (2014) 41(2):127–37. doi: 10.1177/1090198113485755
5. Bennett P, Gladman J. The Inclusion of Parents or Carers in the Consultation Process of Developing Health-Promotion Activities in the Australian Context. Health Educ J (2013) 72(1):70–85. doi: 10.1177/0017896911430561
6. Jensen CD, Aylward BS, Steele RG. Predictors of Attendance in a Practical Clinical Trial of Two Pediatric Weight Management Interventions. Pediatric Obesity (2012) 20(11):2250–6. doi: 10.1038/oby.2012.96
7. Burton W, Twiddy M, Sahota P, Brown J, Bryant M. Participant Engagement With a UK Community-Based Preschool Childhood Obesity Prevention Programme: A Focused Ethnography Study. BMC Public Health (2019) 19(1):1–14. doi: 10.1186/s12889-019-7410-0
8. Love P, Laws R, Litterbach E, Campbell KJ. Factors Influencing Parental Engagement in an Early Childhood Obesity Prevention Program Implemented at Scale: The Infant Program. Nutrients (2018) 10(4):509. doi: 10.3390/nu10040509
9. La Placa V, Corlyon J. Barriers to Inclusion and Successful Engagement of Parents in Mainstream Services: Evidence and Research. J Children’s Serv (2014) 9(3):220–34. doi: 10.1108/JCS-05-2014-0027
10. Kozica SL, Lombard CB, Ilic D, Ng S, Harrison CL, Teede HJ. Acceptability of Delivery Modes for Lifestyle Advice in a Large Scale Randomised Controlled Obesity Prevention Trial. BMC Public Health (2015) 15(1):1–13. doi: 10.1186/s12889-015-1995-8
11. Ekambareshwar M, Taki S, Mihrshahi S, Baur LA, Rissel C, Wen LM. Participant Experiences of an Infant Obesity Prevention Program Delivered via Telephone Calls or Text Messages. Healthcare (2020) 8(1):60. doi: 10.3390/healthcare8010060
12. Ekambareshwar M, Ekambareshwar S, Mihrshahi S, Wen LM, Baur LA, Laws R, et al. Process Evaluations of Early Childhood Obesity Prevention Interventions Delivered via Telephone or Text Messages: A Systematic Review. Int J Behav Nutr Phys Activity (2021) 18(1):1–25. doi: 10.1186/s12966-020-01074-8
13. Wen LM, Rissel C, Xu H, Taki S, Buchanan L, Bedford K, et al. Effects of Telephone and Short Message Service Support on Infant Feeding Practices, “Tummy Time,” and Screen Time at 6 and 12 Months of Child Age. Jama Pediatr (2020) 174(7):657–64. doi: 10.1001/jamapediatrics.2020.0215
14. Wen LM, Xu H, Taki S, Buchanan L, Rissel C, Phongsavan P, et al. Effects of Telephone Support or Short Message Service on Body Mass Index, Eating and Screen Time Behaviours of Children Age 2 Years: A 3-Arm Randomized Controlled Trial. Pediatr Obes (2021) e12875. doi: 10.1111/ijpo.12875
15. Hulscher MEJL. Process Evaluation on Quality Improvement Interventions. Qual Saf Health Care (2003) 12(1):40–6. doi: 10.1136/qhc.12.1.40
16. Steckler AB, Linnan L. Process Evaluation for Public Health Interventions and Research. San Francisco;Great Britain: Jossey-Bass (2002).
17. Taki S, Russell CG, Lymer S, Laws R, Campbell K, Appleton J, et al. A Mixed Methods Study to Explore the Effects of Program Design Elements and Participant Characteristics on Parents’ Engagement With an Mhealth Program to Promote Healthy Infant Feeding: The Growing Healthy Program. Front Endocrinol (2019) 10(397). doi: 10.3389/fendo.2019.00397
18. Litterbach EK, Russell CG, Taki S, Denney-Wilson E, Campbell KJ, Laws RA. Factors Influencing Engagement and Behavioral Determinants of Infant Feeding in an Mhealth Program: Qualitative Evaluation of the Growing Healthy Program. JMIR MHealth UHealth (2017) 5(12):e196. doi: 10.2196/mhealth.8515
19. Verheijden MW, Jans MP, Hildebrandt VH, Hopman-Rock M. Rates and Determinants of Repeated Participation in a Web-Based Behavior Change Program for Healthy Body Weight and Healthy Lifestyle. J Med Internet Res (2007) 9(1):e1. doi: 10.2196/jmir.9.1.e1
20. Ekambareshwar M, Mihrshahi S, Wen LM, Taki S, Bennett G, Baur LA, et al. Facilitators and Challenges in Recruiting Pregnant Women to an Infant Obesity Prevention Programme Delivered via Telephone Calls or Text Messages. Trials (2018) 19(494):1–9. doi: 10.1186/s13063-018-2871-5
21. Bala N, Price SN, Horan CM, Gerber MW, Taveras EM. Use of Telehealth to Enhance Care in a Family-Centered Childhood Obesity Intervention. Clin Pediatr (2019) 58(7):789–97. doi: 10.1177/0009922819837371
22. Centre for Epidemiology and Research. Report on Adult Health by Country of Birth From the New South Wales Population Health Survey. Sydney: NSW Department of Health (2006–2009).
23. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research Electronic Data Capture (Redcap) – A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J BioMed Inform 2009 (2009) 42(2):377–81. doi: 10.1016/j.jbi.2008.08.010
24. Ekambareshwar M, Taki S, Mihrshahi S, Baur L, Wen LM, Rissel C. Trial Collaborators’ Perceptions of the Process of Delivering Healthy Beginnings Advice via Telephone Calls or Text Messages. Health Promotion J Aust (2021) 00:1–19. doi: 10.1002/hpja.562
27. Perski O, Blandford A, West R, Michie S. Conceptualising Engagement With Digital Behaviour Change Interventions: A Systematic Review Using Principles From Critical Interpretive Synthesis. Trans Behav Med (2017) 7(2):254–67. doi: 10.1007/s13142-016-0453-1
28. Hardiker NR, Grant MJ. Factors That Influence Public Engagement With Ehealth: A Literature Review. Int J Med Inf (2011) 80(1):1–12. doi: 10.1016/j.ijmedinf.2010.10.017
29. Nobles J, Griffiths C, Pringle A, Gately P. Design Programmes to Maximise Participant Engagement: A Predictive Study of Programme and Participant Characteristics Associated With Engagement in Paediatric Weight Management. Int J Behav Nutr Phys Activity (2016) 13(1):1–10. doi: 10.1186/s12966-016-0399-1
30. Dolinsky DH, Armstrong SC, Østbye T. Predictors of Attrition From a Clinical Pediatric Obesity Treatment Program. Clin Pediatr (2012) 51(12):1168–74. doi: 10.1177/0009922812458355
31. Walker SE, Smolkin ME, O’Leary MLL, Cluett SB, Norwood VF, Deboer MD, et al. Predictors of Retention and BMI Loss or Stabilization in Obese Youth Enrolled in a Weight Loss Intervention. Obes Res Clin Pract (2012) 6(4):e330–9. doi: 10.1016/j.orcp.2011.08.157
32. Khanal S, Choi L, Innes-Hughes C, Rissel C. Dose Response Relationship Between Program Attendance and Children’s Outcomes in a Community Based Weight Management Program for Children and Their Families. BMC Public Health (2019) 19(1):1–18. doi: 10.1186/s12889-019-7094-5
33. Hampl S, Demeule M, Eneli I, Frank M, Hawkins MJ, Kirk S, et al. Parent Perspectives on Attrition From Tertiary Care Pediatric Weight Management Programs. Clin Pediatr (2013) 52(6):513–9. doi: 10.1177/0009922813482515
34. Braet C, Jeannin R, Mels S, Moens E, Van Winckel M. Ending Prematurely a Weight Loss Programme: The Impact of Child and Family Characteristics. Clin Psychol Psychother (2010) 17(5):406–17. doi: 10.1002/cpp.663
35. Cote MP. Service Quality and Attrition: An Examination of a Pediatric Obesity Program. Int J Qual Health Care (2004) 16(2):165–73. doi: 10.1093/intqhc/mzh015
36. Marshall S, Taki S, Love P, Laird Y, Kearney M, Tam N, et al. The Process of Culturally Adapting the Healthy Beginnings Early Obesity Prevention Program for Arabic and Chinese Mothers in Australia. BMC Public Health (2021) 21(1):1–16. doi: 10.1186/s12889-021-10270-5
Keywords: mobile telephone interventions, engagement, mHealth, childhood obesity prevention, process evaluation
Citation: Ekambareshwar M, Xu H, Rissel C, Baur L, Taki S, Mihrshahi S and Wen LM (2022) Participants’ Engagement With Telephone Support Interventions to Promote Healthy Feeding Practices and Obesity-Protective Behaviours for Infant Obesity Prevention. Front. Endocrinol. 13:868944. doi: 10.3389/fendo.2022.868944
Received: 03 February 2022; Accepted: 21 March 2022;
Published: 02 May 2022.
Edited by:
Andrea Enzo Scaramuzza, Istituti Ospitalieri di Cremona, ItalyReviewed by:
Hong Jiang, Fudan University, ChinaCopyright © 2022 Ekambareshwar, Xu, Rissel, Baur, Taki, Mihrshahi and Wen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mahalakshmi Ekambareshwar, bWFoYWxha3NobWkuZWthbWJhcmVzaHdhckBzeWRuZXkuZWR1LmF1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.