
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 19 May 2022
Sec. Obesity
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.807380
This article is part of the Research Topic Endocrine and Metabolic Consequences of Childhood Obesity View all 16 articles
 Jinling Wang1
Jinling Wang1 Hu Lin1
Hu Lin1 Valentina Chiavaroli2,3
Valentina Chiavaroli2,3 Binghan Jin1Jinna Yuan1
Binghan Jin1Jinna Yuan1 Ke Huang1Wei Wu1Guanping Dong1
Ke Huang1Wei Wu1Guanping Dong1 José G. B. Derraik1,3,4,5*
José G. B. Derraik1,3,4,5* Junfen Fu1*
Junfen Fu1*Objective: This study aimed to describe the clinical characteristics of children and adolescents with obesity, and the prevalence of cardiometabolic comorbidities over 10 years in this population from a large metropolitan centre in China.
Methods: This was a cross-sectional study (2008–2017) of patients aged <18 years with obesity [body mass index (BMI) ≥ 95th percentile for age and sex] enrolled at the Department of Endocrinology, Children’s Hospital of Zhejiang University School of Medicine (Hangzhou, Zhejiang Province). Clinical assessments included anthropometry, blood pressure, liver ultrasound, lipid profile, oral glucose tolerance test, and uric acid. For examination of outcomes, our study cohort was stratified by sex and age bands (<10 vs. ≥10 years), with the study period also split into two strata (2008–2012 and 2013–2017).
Results: A total of 2,916 patients (1,954 boys and 962 girls) were assessed at a mean age of 10.5 years. Patients almost invariably presented severe obesity (median BMI SDS = 2.98; Q1 = 2.60, Q3 = 3.39). Obesity-related comorbidities were common among boys and girls, including type 2 diabetes mellitus (2.6% and 3.6%, respectively), abnormal glycaemia (33.6% and 35.5%, respectively), hypertension (33.9% and 32.0%, respectively), dyslipidaemia (35.2% and 39.6%, respectively), hyperuricaemia (16.2% and 8.3%, respectively), acanthosis nigricans (71.9% and 64.0%, respectively), abnormal liver function (66.9% and 47.0%, respectively), and non-alcoholic fatty liver disease (NAFLD) (63.8% and 45.1%, respectively); 38.7% of boys and 44.4% of girls aged ≥10 years had metabolic syndrome. Notably, the incidence of many cardiometabolic comorbidities was in 2013–2017 compared to 2008–2012. For example, rates of hypertension among boys aged <10 years and aged ≥10 years rose from 28.4% and 26.5% to 48.0% and 35.8%, respectively, and in girls from 20.3% and 20.8% to 41.7% and 39.6%, respectively. In 2013–2017, 9.5% of girls in the older group had metabolic syndrome compared to 2.2% in 2008–2013.
Conclusions: We observed a high incidence of obesity-related cardiometabolic comorbidities among Chinese children and adolescents with severe obesity over 10 years. It was particularly concerning that rates of several comorbidities rose markedly over the study period, highlighting the need to address the obesity epidemic early in life (in China and elsewhere) to prevent the development of obesity-related comorbidities and, subsequently, of overt disease.
Worldwide, obesity is a major public health issue (1). The number of children and adolescents aged 5 to 19 years with obesity has risen 10-fold over the last four decades, reaching 124 million in 2016, with the global prevalence increasing from 0.7% to 5.6% in girls and from 0.9% to 7.8% in boys between 1975 and 2016, respectively (2). Notably, the mean body mass index (BMI) among children and adolescents has increased steadily, including in China (3). In 2015–2019, the prevalence of overweight and obesity in China was 6.8% and 3.6%, respectively, for children aged less than 6 years, and 11.1% and 7.9%, respectively, for those aged 6–17 years (4), with higher obesity rates reported in urban areas (5).
Children with obesity are at increased risk for cardiometabolic comorbidities, including hypertension, dyslipidaemia, hyperglycaemia, non-alcoholic fatty liver disease (NAFLD), and metabolic syndrome, which often track into adulthood with an increased risk of cardiovascular morbidity and mortality (6, 7). Of note, several paediatric definitions of metabolic syndrome agree on its components but differ in diagnostic criteria, and the International Diabetes Federation (IDF) definition seems to be more easily adopted in clinical practice (8). Moreover, the hazard ratio for type 2 diabetes mellitus is markedly elevated among adolescents with severe obesity (9). China is currently experiencing an accelerating diabetes epidemic as a result of a combination of factors (many of which interact), including increasing rates of obesity, changes in dietary habits (e.g., high in fat) and lifestyle (i.e., sedentary), ageing, and genetic and epigenetic factors (10). Of interest, a higher risk of diabetes at a lower BMI has been observed in the Chinese population compared to Europeans, likely resulting from the former’s greater visceral adiposity (11) and lower insulin response (12). Additionally, childhood obesity may favour early pubertal development or skeletal maturation and adverse psychosocial outcomes, including depression, anxiety, and eating disorder (13–15).
Therefore, childhood obesity and related cardiometabolic comorbidities are important issues that must be addressed. However, the incidence and severity of cardiometabolic comorbidities among Chinese children and adolescents with obesity have been overlooked in China over the last decades. Thus, our primary aim was to describe the clinical features of children and adolescents with obesity, particularly obesity-related cardiometabolic comorbidities. In addition, we also examined possible changes in the incidence of these comorbidities in boys and girls over the 10-year study period.
This was a cross-sectional study of children and adolescents voluntarily brought to our hospital by their parents who were concerned about excessive weight gain. These patients were then referred to the Department of Endocrinology at the Children’s Hospital of Zhejiang University School of Medicine, National Clinical Research Center for Child Health in Hangzhou, between January 1, 2008, and December 31, 2017. Hangzhou is the capital of Zhejiang Province, with a population of 6.77 million in 2008 and 7.53 million in 2017, including 1.05 million and 1.25 million children and adolescents aged ≤17 years, respectively (16, 17). The Children’s Hospital is one of only two National Clinical Research Centers for Child Health in China, recording approximately 81,000 inpatient and 3.5 million outpatient visits per year. Patients were only included once in this study, corresponding to their first visit to our clinic during the 10-year study period.
The main inclusion criterion was obesity at presentation, defined as a BMI SD score [SDS; derived as per the WHO standards (18) for age and sex] ≥1.645 (i.e., ≥95th percentile). At admission, none of our patients was on therapy with medications known to affect energy metabolism; had an overt chronic heart, lung, or kidney disease; or had been previously with diagnosed endocrine or metabolic dysfunction (e.g., Wilson’s disease), genetic disorders (e.g., Prader–Willi syndrome), or any severe chronic illness.
Participants were admitted to our inpatient clinic and underwent comprehensive clinical assessments over 24 h performed by nurses. Demographic characteristics were recorded or obtained from clinical records.
Standing height was measured to the nearest 0.1 cm using a wall-mounted Harpenden stadiometer while patients were barefoot. Weight was measured with the participant in light clothing using a digital scale to the nearest 0.1 kg; BMI was subsequently derived. Height, weight, and BMI were transformed into SDS (18). Waist circumference was measured to the nearest 1 mm with a tape measure around the participant’s body in the horizontal plane, at the midpoint level between the lowest rib and the iliac crest, on bare skin, and at the end of normal expiration. The waist-to-height ratio was then calculated. Maternal and paternal anthropometry data (i.e., height and weight) were obtained by self-report, and their BMI was calculated.
Systolic (SBP) and diastolic blood pressures (DBP) were measured using a sphygmomanometer on the right upper arm while patients seated and after a 5-min rest. Venous blood samples were taken on the morning of the assessment after an overnight fast. Parameters measured included glucose, insulin, glycated haemoglobin (HbA1c), triglycerides, low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), total cholesterol, aspartate transaminase (AST), alanine transaminase (ALT), and uric acid.
All participants underwent a 75-g oral glucose tolerance test (OGTT; 1.75 g per kg, maximum 75 g), with blood samples drawn at 0, 30, 60, 90, and 120 min for glucose, insulin, and C-peptide measurements. Insulin sensitivity was assessed using the Matsuda index, which is strongly correlated with the hyperinsulinaemic–euglycaemic clamp and has high reproducibility during multiple measures (19).
Cardiometabolic comorbidities assessed included the following: impaired fasting glucose, impaired glucose tolerance, type 2 diabetes, and abnormal glycaemia (20); hypertension (21); dyslipidaemia (22); metabolic syndrome (22); NAFLD (23); and hyperuricaemia (24) (Table 1). Acanthosis nigricans was also recorded, as it is a clinical sign of hyperinsulinaemia and insulin resistance (26, 27). Central obesity was defined as per Chinese criteria for children and adolescents based on the waist-to-height ratio (21) (Table 1).
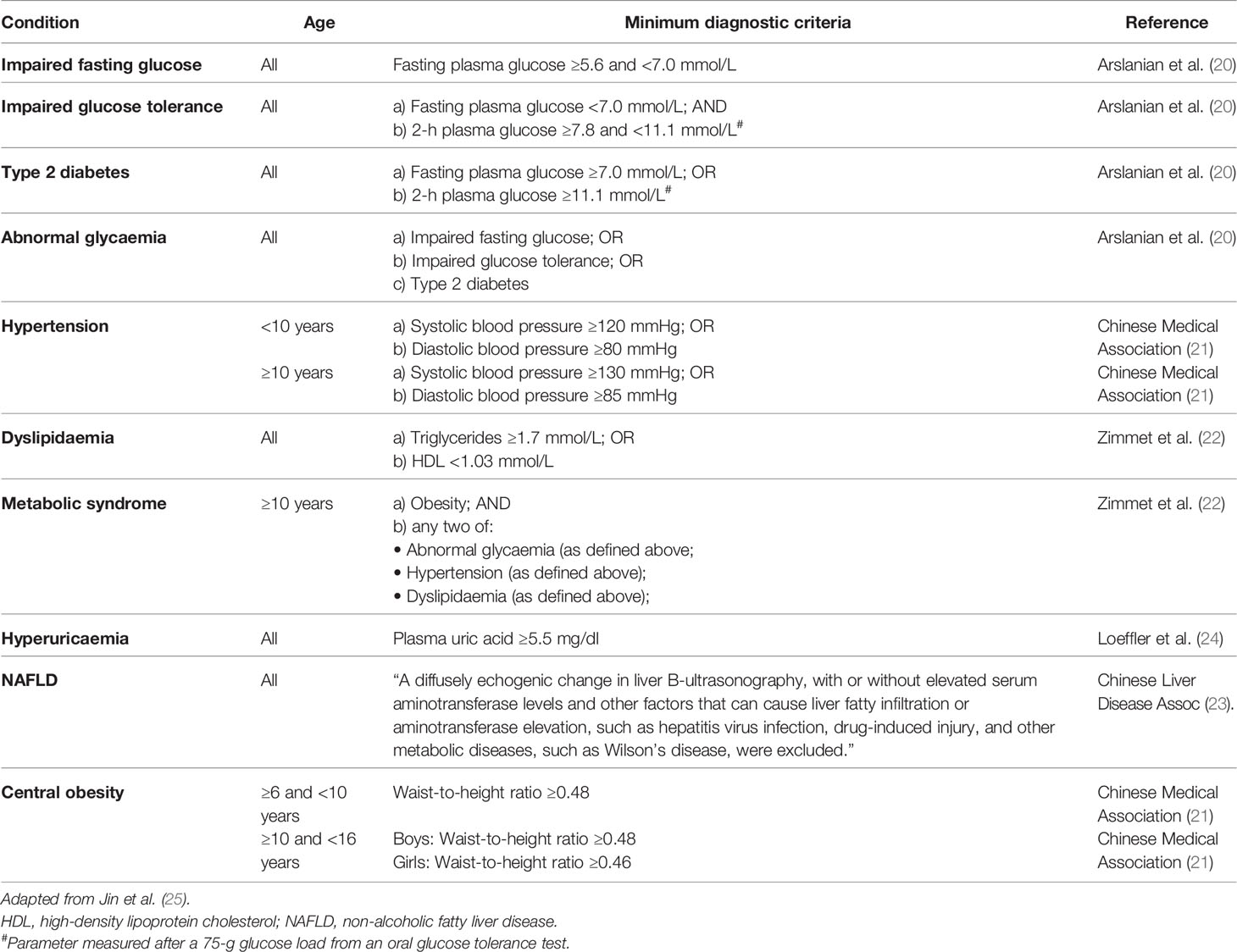
Table 1 Diagnostic criteria for central adiposity and obesity-related cardiometabolic comorbidities assessed.
Descriptive data for demographic and anthropometric characteristics of our overall study population are provided as means ± SDs or frequency (n) and percentages (%). The incidence of central obesity and obesity-related cardiometabolic comorbidities is provided as n (%).
Patients were then stratified according to the year of admission (into two 5-year study periods: 2008–2012 and 2013–2017), sex (male and female), and age (<10 and ≥10 years). Within each age group, the incidence of comorbidities was compared between sexes and between study periods using Fisher’s exact tests.
Continuous outcomes for anthropometry, blood pressure, glucose metabolism, and lipid profile were also compared between the groups mentioned above. Potential differences were assessed using general linear regression models adjusting for the participant’s age, with the latter replaced with height for blood pressure outcomes. The data distribution of each outcome was examined, and, where appropriate, data were log-transformed to approximate a normal distribution. For continuous variables, differences between sexes or study periods are reported in the text as the estimated marginal means (adjusted means) and 95% CIs.
Analyses were performed in SPSS v25 (IBM Corp., Armonk, NY, USA) and SAS v9.4 (SAS Institute, Cary, NC, USA). All tests were two-tailed, with statistical significance maintained at p < 0.05, and without adjustment for multiple comparisons as per Rothman (1990) (28).
Our study population consisted of 2,916 children and adolescents with obesity, assessed at a mean age of 10.5 ± 2.6 years, including 1,954 boys and 962 girls (Table 2). Participants had a median BMI SDS of 2.98 (Q1 = 2.60, Q3 = 3.39; range 1.65–9.51), and the vast majority had severe obesity (Figure 1). Among caregivers, 1 in 3 mothers (33.2%) and more than half of fathers (54.7%) had overweight or obesity (Table 2).
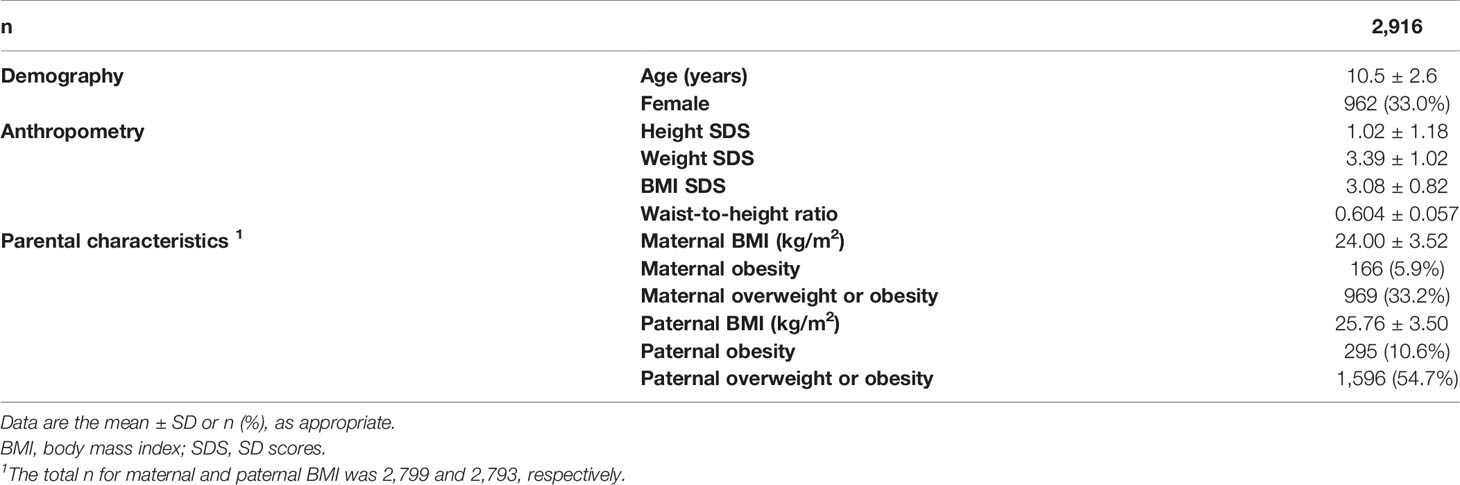
Table 2 Demographic, anthropometric, and clinical characteristics of our study population of children and adolescents with obesity from Hangzhou (Zhejiang Province, China) in 2008–2017.
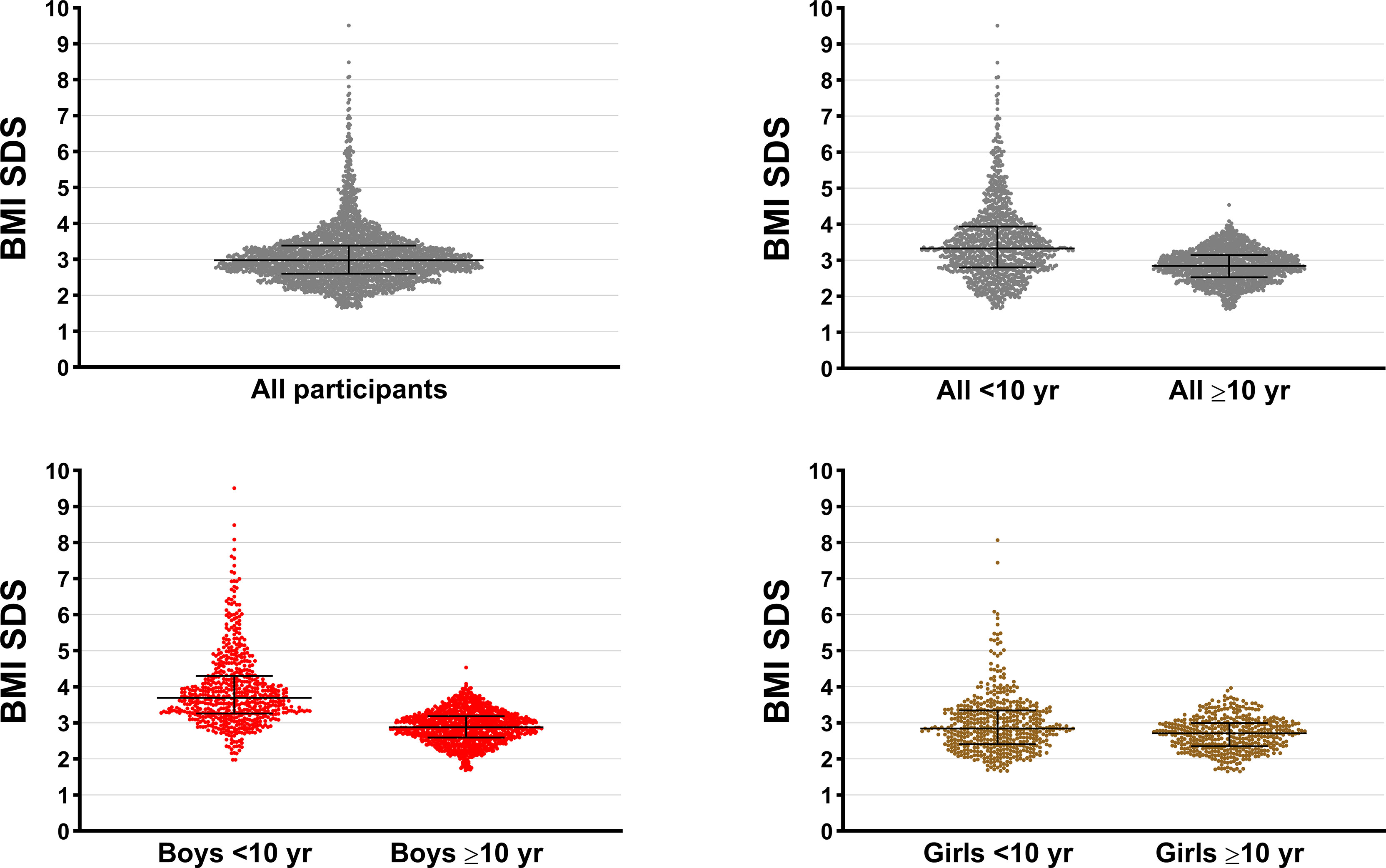
Figure 1 Distribution of body mass index SD scores (BMI SDS) among our study population of children and adolescents with obesity assessed in 2008–2017 in Hangzhou (Zhejiang Providence, China). Horizontal bars represent the median and the interquartile range.
As shown in Table 3, there was a high incidence of cardiometabolic comorbidities among children and adolescents with obesity in China over the 10-year period covered by this study. Among boys and girls, these included type 2 diabetes (2.6% and 3.6%, respectively), abnormal glycaemia (33.6% and 35.5%), hypertension (33.9% and 32.0%), and dyslipidaemia (35.2% and 39.6%), with almost all boys (99.6%) and girls (98.5%) having central obesity (Table 3).
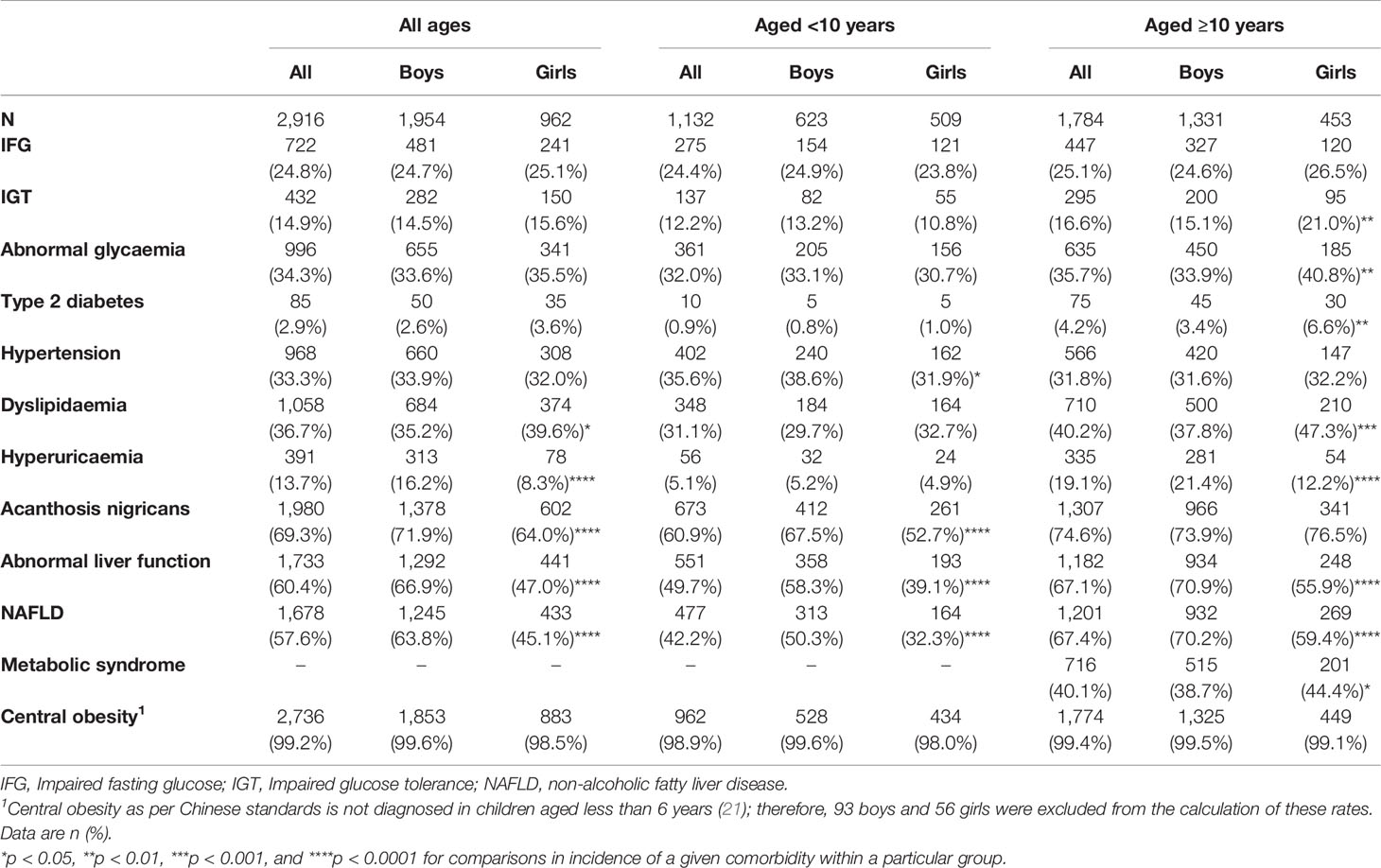
Table 3 Incidence of cardiometabolic comorbidities among children and adolescents with obesity assessed between 2008 and 2017 in Hangzhou (Zhejiang Province, China).
There was a greater proportion of boys than girls with hyperuricaemia (16.2% vs. 8.3%, respectively; p < 0.0001), acanthosis nigricans (71.9% vs. 64.0%; p < 0.0001), abnormal liver function (66.9% vs. 47.0%; p < 0.0001), and NAFLD (63.8% vs. 45.1%; p < 0.0001), with these sex differences largely observed in the two age groups (Table 3). Among children aged <10 years, there was a greater incidence of hypertension in boys than girls (38.6% vs. 31.9%; p = 0.021) (Table 3). In addition, the incidence of obesity-related comorbidities was greater among patients aged ≥10 years than in the younger group (Table 3). Notably, 38.7% of boys and 44.4% of girls aged ≥10 years had metabolic syndrome (Table 3).
When the two 5-year periods (2008–2012 vs. 2013–2017) were compared, among the younger boys, there was a higher incidence of impaired fasting glucose, abnormal glycaemia, acanthosis nigricans, and, in particular, hypertension (Table 4). These differences were underpinned by higher SBP (+6.2 mmHg; 95% CI 4.3, 8.0 mmHg), DBP (+2.3 mmHg; 95% CI 1.0, 3.7 mmHg), fasting glucose (+0.20 mmol/L; 95% CI 0.13, 0.27 mmol/L), and a Matsuda index that was 18% lower (95% CI −1.3%, −31.6%) in 2013–2017 (Table 5). Conversely, the incidence of dyslipidaemia was lower in the later period, likely associated with HDL +7.3% higher (+0.09 mmol/L; 95% CI 0.05, 0.14 mmol/L) and possibly slightly lower triglycerides (Table 5).
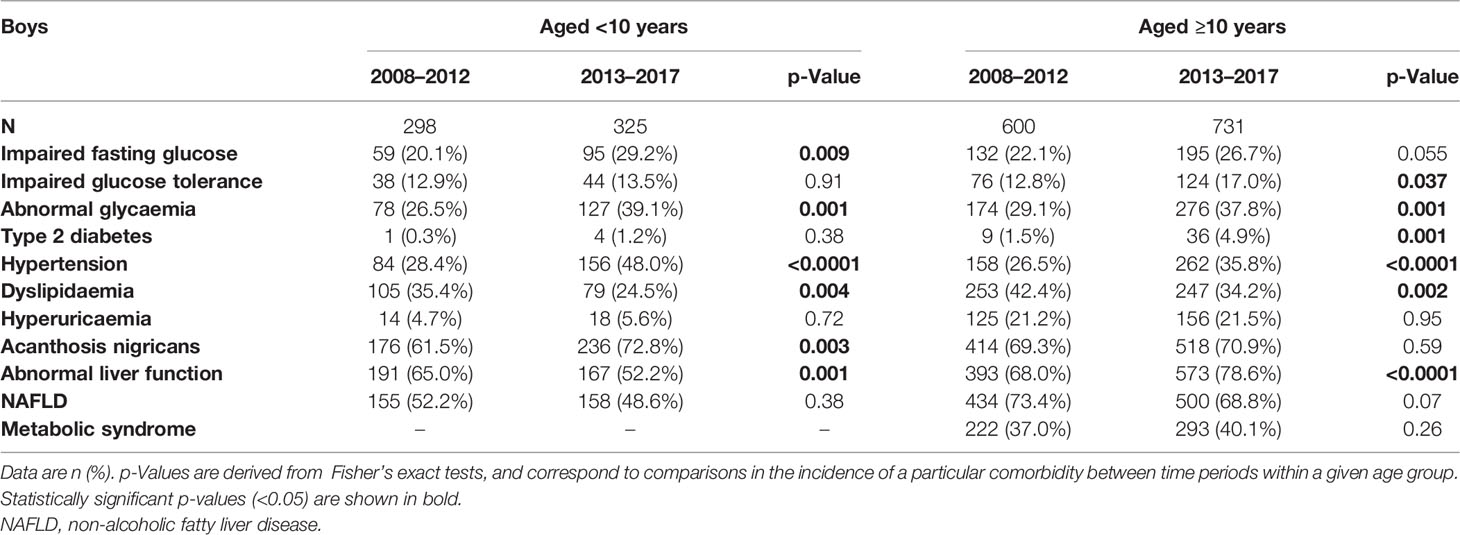
Table 4 Incidence of cardiometabolic comorbidities among Chinese boys with obesity assessed between 2008 and 2017 in Hangzhou (Zhejiang Province, China).

Table 5 Cardiometabolic parameters among Chinese boys with obesity assessed between 2008 and 2017 in Hangzhou (Zhejiang Province, China).
In the older group of boys, in 2013–2017, there was a higher incidence of hypertension, abnormal liver function, and abnormal glycaemia, including type 2 diabetes (4.9% vs. 1.5%; Table 4). As seen among the younger boys, these comorbidities were more frequent in the later period in association with higher SBP (+4.3 mmHg; 95% CI 2.9, 5.8 mmHg), DBP (+2.3 mmHg; 95% CI 1.3, 3.4 mmHg), fasting glucose (+0.13 mmol/L; 95% CI 0.07, 0.19 mmol/L), fasting insulin (+14%; 95% CI 5%, 24%), and lower Matsuda index (−15%; 95% CI −5%, −25%) in 2013–2017 (Table 5).
Among the younger girls, there were proportionally fewer patients with abnormal liver function in 2013–2017 (Table 6), but the rate of hypertension was 2-fold higher (41.7% vs. 20.3%), which was associated with higher SBP (+9.2 mmHg; 95% CI 7.2, 11.3 mmHg) and DBP (+2.6 mmHg; 95% CI 1.0, 4.2 mmHg) (Table 7). In addition, girls in the second period had fasting glucose concentrations 0.15 mmol/L higher (95% CI 0.04, 0.26 mmol/L) and Matsuda index 28% lower (95% CI −10%, −42%) (Table 7).
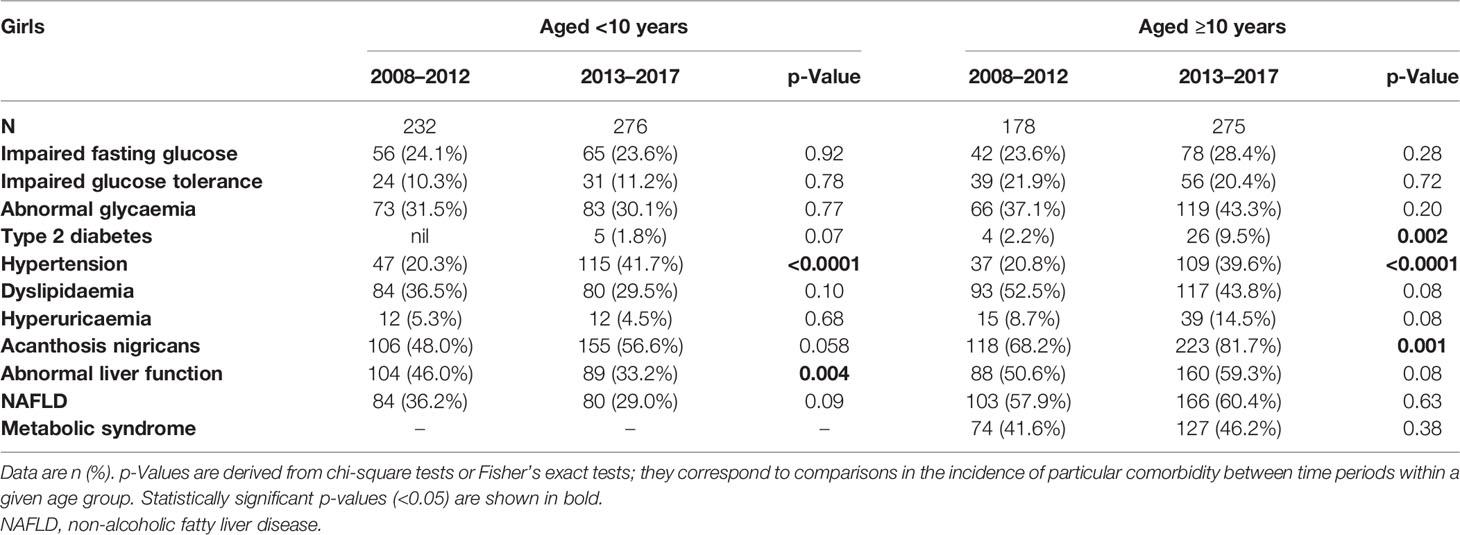
Table 6 Incidence of cardiometabolic comorbidities among Chinese girls with obesity assessed between 2008 and 2017 in Hangzhou (Zhejiang Province, China).

Table 7 Cardiometabolic parameters among girls with obesity assessed between 2008 and 2017 in Hangzhou (Zhejiang Province, China).
For girls aged 10 years or older, there was a higher incidence of acanthosis nigricans, hypertension, and a 4.5-fold higher incidence of type 2 diabetes affecting nearly 10% of girls in 2013–2017 (9.5% vs. 2.2%) (Table 6). In this older group of girls, there were other clinical parameters worse in 2013–2017 than in 2008–2012, including higher waist-to-height ratio (+0.011; 95% CI 0.000, 0.022), SBP (+4.8 mmHg; 95% CI 2.4, 7.2 mmHg), DBP (+4.6 mmHg; 95% CI 2.8, 6.3 mmHg), LDL (+0.26 mmol/L; 95% CI 0.13, 0.39 mmol/L), and fasting insulin (+28%; 95% CI 9%, 50%) but lower Matsuda index (−42%; 95% CI −26%, −54%) (Table 7). Conversely, HDL was higher (+0.07 mmol/L; 95% CI 0.02, 0.11 mmol/L) and the cholesterol:HDL ratio lower (−0.21; 95% CI −0.41, −0.02) (Table 7).
To our knowledge, this was the largest single-centre cross-sectional study (n = 2,916) to comprehensively assess obesity-related comorbidities among children and adolescents with severe obesity in China. There was a high incidence of a range of cardiometabolic comorbidities, including abnormal glycaemia, hypertension, dyslipidaemia, hyperuricaemia, acanthosis nigricans, abnormal liver function, and NAFLD. These findings are not surprising given the strong association between higher BMI during adolescence and increased risk for cardiometabolic complications (15, 29). Our paediatric population characterised by very high BMI SDS illustrates the extent of the potential impacts of childhood obesity (and related comorbidities) on public health in China and elsewhere, a growing challenge that has been previously underestimated (30, 31).
In 2013, the prevalence of metabolic syndrome in Chinese children with obesity was 28.8% (32), in contrast to our observed rates of 40.1% and 46.2% for boys and girls, respectively, in 2013–2017. The much higher incidence in our study population is not surprising given that most of our patients had severe obesity. Other common comorbidities in our study included abnormal liver function, NAFLD, and acanthosis nigricans. The latter, in particular, is highly prevalent and a specific clinical sign of insulin resistance, a key component of the metabolic syndrome (33, 34). Our patients also had insulin sensitivity assessed with the Matsuda index, a robust measure to examine abnormalities in glucose metabolism in children and adolescents with obesity (35). Previous studies have also shown high rates of disorders in glucose metabolism among asymptomatic children and adolescents with obesity (36). Here, we also observed an apparent reduction in insulin sensitivity and an associated increase in fasting glucose levels between the two 5-year periods (2008–2012 vs. 2013–2017); these findings suggest that children with severe obesity are displaying increasing levels of impairment in glucose metabolism and possibly increased risk of progressing to type 2 diabetes.
The growing problem of childhood obesity seems to be underpinning the increasing burden of NAFLD. In our study, 2 out of 3 boys aged 10 years or older displayed liver function abnormalities and/or were affected by NAFLD. In a study on ≈15,000 children and adolescents from 6 centres throughout China, we identified elevated liver enzymes associated with metabolic syndrome features, highlighting the role of chronic insulin resistance and metabolic syndrome in the aetiology of liver injury in Chinese youth (37). While we have no data on the clinical history of our patients (particularly in regard to weight gain over time), our findings are not surprising given that, after 2 years of age, obesity progressively increases the risk of developing NAFLD in adolescence (38). Therefore, it is important to monitor liver function and the potential development of NAFLD over time among children and adolescents with obesity, specifically liver function tests and liver ultrasound (39, 40).
The link between obesity and hypertension is well established (41, 42). The reported prevalence of hypertension in schoolchildren with obesity was approximately 11% in the United States (43). In Greece, a study on 2,655 schoolchildren aged 9–13 years showed higher rates of hypertension of 25.3% and 20.8% for girls and boys, respectively (44). Among Chinese youth, Cao (2009) reported rates of hypertension of 11.5% in girls and 21.7% in boys with obesity aged 12 to 17 years (45). The higher rates of hypertension among our patients (33.3%) would be expected given their obesity severity, as alluded to earlier. For example, Lo et al. showed that the odds of hypertension were 2.7 times greater in children with severe obesity compared to those with moderate obesity (46). Notably, the incidence of hypertension increased between 2008–2012 and 2013–2017 among our patients, irrespective of sex or age, reflecting corresponding increases in SBP and DBP over time. The reasons for the changing incidence of hypertension over time are unclear, particularly in the absence of differences in obesity levels. It is possible that changes in dietary habits and physical activity levels could explain, at least in part, the worsening rates of hypertension in the latest period. However, this cannot be ascertained in our study population, as such information was not recorded. Nonetheless, independent of the underlying causes of our observed trend, blood pressure should be monitored in the long-term (47) among paediatric patients with obesity, as a longer duration of hypertension increases the cardiovascular risk and end-organ damage (48).
Of note, the ratio of boys to girls in our study was approximately 2:1. It is plausible that this could reflect some bias among parents, who would be more likely to identify weight issues in boys than in girls. Previously, in a study of more than 20,000 children and adolescents from 6 centres across China, we reported that parents were more likely to overestimate the BMI status of girls compared to boys (49). However, the child’s sex was not associated with the parents’ ability to correctly identify an obesity issue or, most importantly in the context of the present study, of seeking treatment for their child if weight issues were identified (49). Most likely, the overrepresentation of boys in our study is simply a reflection of the greater prevalence of obesity in boys in the general population: in 2013, the prevalence of obesity in children and adolescents in China was 6.9% among boys and 2.8% among girls (50).
The main limitation of our study was the lack of complete data on pubertal development, which was only recorded on approximately 80% of our study population; thus, our study cohort was stratified using a relatively arbitrary age threshold, as used for the classification of the metabolic syndrome (22). While there was no selection bias by study investigators since all patients were self-reported (by their parents), the BMI SDS 10th percentile among our patients was 2.27, illustrating that our study population was skewed towards the upper end of the BMI SDS spectrum, consisting primarily of individuals with severe obesity. This is not surprising, as we have shown that Chinese caregivers are more likely to identify problems with excess weight in children with severe obesity (49). Nonetheless, this means that our observed incidence of obesity-related comorbidities cannot be readily extrapolated to children and adolescents with more moderate levels of obesity. Another limitation of our study was a potential regional bias; our patients were assessed in east China, and the prevalence of obesity-related comorbidities may differ in other regions of the country. Lastly, this was a cross-sectional study, as longitudinal data were not available; since comparisons between the two study periods were made between two different groups of patients, we cannot ascertain the progression of obesity-related comorbidities in individual patients over time. Nevertheless, our study is particularly valuable due to the comprehensive range of clinical assessments performed (e.g., blood pressure, OGTT, and liver ultrasound) and the large number of children and adolescents assessed.
In conclusion, our study shows a high incidence of obesity-related cardiometabolic comorbidities among Chinese children and adolescents with severe obesity over 10 years, including hypertension, NAFLD, and abnormalities in glucose metabolism. It was particularly concerning that rates of several comorbidities rose markedly over the study period, highlighting the need to address the obesity epidemic early in life in China and elsewhere to prevent the development of obesity-related comorbidities and, subsequently, of overt disease.
The data presented in this article are not readily available because of the conditions of the ethics approval. The anonymized data on which this article was based could be made available to other investigators upon bona fide request, and following all the necessary approvals (including ethics) of the detailed study proposal and statistical analyses plan. Requests to access the dataset should be directed to Prof. Junfen Fu, ZmpmNjhAemp1LmVkdS5jbg==.
This study was approved by the Medical Ethics Committee of the Children's Hospital of Zhejiang University School of Medicine (No. 2020-IRB-098). Written informed consent was obtained from parents (or caregivers) and verbal or written consent from each child as appropriate to their age. This study was performed following all applicable institutional and international guidelines and regulations for medical research, in line with the principles of the Declaration of Helsinki (51).
JF was responsible for funding acquisition. JF, JD, JW, HL, BJ, and JY contributed to the study design. JW, HL, JY, KH, WW, and GD carried out the clinical assessments. JW, HL, JY, BJ, and JD were responsible for data curation and analyses, with results critically reviewed by JF, VC, KH, WW, and GD. JW, VC, and JD wrote the manuscript with critical input from all other authors. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This work was supported by the National Key Research and Development Program of China (No. 2021YFC2701901 and No. 2016YFC1305301), the National Natural Science Foundation of China (No. 81570759 and 81270938), the Fundamental Research Funds for the Central Universities (2020XZZX002-22), the Research Fund of Zhejiang Major Medical and Health Science and Technology and National Ministry of Health (WKJ-ZJ-1804), Zhejiang Provincial Natural Science Foundation of China (LQ20H070003), Zhejiang Provincial Key Disciplines of Medicine (Innovation Discipline, 11-CX24), and Zhejiang Province Natural Sciences Foundation Zhejiang Society for Mathematical Medicine (LSZ19H070001). JD was supported by a travel fellowship from the New Zealand–China Non-Communicable Diseases Research Collaboration Centre.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bluher M. Obesity: Global Epidemiology and Pathogenesis. Nat Rev Endocrinol (2019) 15:288–98. doi: 10.1038/s41574-019-0176-8
2. Ezzati M, Bentham J, Di Cesare M, Bilano V, Bixby H, Zhou B, et al. Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity From 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128.9 Million Children, Adolescents, and Adults. Lancet (2017) 390:2627–42. doi: 10.1016/S0140-6736(17)32129-3
3. Jaacks LM, Vandevijvere S, Pan A, McGowan CJ, Wallace C, Imamura F, et al. The Obesity Transition: Stages of the Global Epidemic. Lancet Diabetes Endocrinol (2019) 7:231–40. doi: 10.1016/S2213-8587(19)30026-9
4. Pan XF, Wang L, Pan A. Epidemiology and Determinants of Obesity in China. Lancet Diabetes Endocrinol (2021) 9:373–92. doi: 10.1016/s2213-8587(21)00045-0
5. Capital Institute of Pediatrics, Coordinating Study Group of Nine Cities on the Physical Growth and Development of Children. A National Epidemiological Survey on Obesity of Children Under Seven Years of Age in Nine Cities of China in 2016. Zhonghua Er Ke Za Zhi (2018) 56:745–52. doi: 10.3760/cma.j.issn.0578-1310.2018.10.006
6. Morales Camacho WJ, Molina Diaz JM, Plata Ortiz S, Plata Ortiz JE, Morales Camacho MA, Calderon BP. Childhood Obesity: Aetiology, Comorbidities, and Treatment. Diabetes Metab Res Rev (2019) 35:e3203. doi: 10.1002/dmrr.3203
7. Wühl E. Hypertension in Childhood Obesity. Acta Paediatr (2019) 108:37–43. doi: 10.1111/apa.14551
8. Tropeano A, Corica D, Li Pomi A, Pepe G, Morabito LA, Curatola SL, et al. The Metabolic Syndrome in Pediatrics: Do We Have a Reliable Definition? A Systematic Review. Eur J Endocrinol (2021) 185:265–78. doi: 10.1530/eje-21-0238
9. Twig G, Zucker I, Afek A, Cukierman-Yaffe T, Bendor CD, Derazne E, et al. Adolescent Obesity and Early-Onset Type 2 Diabetes. Diabetes Care (2020) 43:1487–95. doi: 10.2337/dc19-1988
10. Ma RC, Lin X, Jia W. Causes of Type 2 Diabetes in China. Lancet Diabetes Endocrinol (2014) 2:980–91. doi: 10.1016/s2213-8587(14)70145-7
11. Nazare JA, Smith JD, Borel AL, Haffner SM, Balkau B, Ross R, et al. Ethnic Influences on the Relations Between Abdominal Subcutaneous and Visceral Adiposity, Liver Fat, and Cardiometabolic Risk Profile: The International Study of Prediction of Intra-Abdominal Adiposity and Its Relationship With Cardiometabolic Risk/Intra-Abdominal Adiposity. Am J Clin Nutr (2012) 96:714–26. doi: 10.3945/ajcn.112.035758
12. Kodama K, Tojjar D, Yamada S, Toda K, Patel CJ, Butte AJ. Ethnic Differences in the Relationship Between Insulin Sensitivity and Insulin Response: A Systematic Review and Meta-Analysis. Diabetes Care (2013) 36:1789–96. doi: 10.2337/dc12-1235
13. Calcaterra V, Verduci E, Cena H, Magenes VC, Todisco CF, Tenuta E, et al. Polycystic Ovary Syndrome in Insulin-Resistant Adolescents With Obesity: The Role of Nutrition Therapy and Food Supplements as a Strategy to Protect Fertility. Nutrients (2021) 13:1848. doi: 10.3390/nu13061848
14. Pulgaron ER. Childhood Obesity: A Review of Increased Risk for Physical and Psychological Comorbidities. Clin Ther (2013) 35:A18–32. doi: 10.1016/j.clinthera.2012.12.014
15. Weihrauch-Bluher S, Schwarz P, Klusmann JH. Childhood Obesity: Increased Risk for Cardiometabolic Disease and Cancer in Adulthood. Metabolism (2019) 92:147–52. doi: 10.1016/j.metabol.2018.12.001
16. Hangzhou Municipal Bureau of Statistics. Hangzhou Statistical Yearbook 2018. Hangzhou: China Statistics Press (2018).
17. Hangzhou Municipal Bureau of Statistics. Hangzhou Statistical Yearbook 2009. Hangzhou: China Statistics Press (2009).
18. de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO Growth Reference for School-Aged Children and Adolescents. Bull WHO (2007) 85:660–7. doi: 10.2471/Blt.07.043497
19. Maki KC, Rains TM, Dicklin MR, Bell M. Repeatability of Indices of Insulin Sensitivity and Secretion from Standard Liquid Meal Tests in Subjects with Type 2 Diabetes Mellitus or Normal or Impaired Fasting Glucose. Diabetes Technol Ther (2010) 12:895–900. doi: 10.1089/dia.2010.0083
20. Arslanian S, Bacha F, Grey M, Marcus MD, White NH, Zeitler P. Evaluation and Management of Youth-Onset Type 2 Diabetes: A Position Statement by the American Diabetes Association. Diabetes Care (2018) 41:2648–68. doi: 10.2337/dci18-0052
21. Subspecialty Group of Endocrinologic, Hereditary and Metabolic Diseases, The Society of Pediatrics, Chinese Medical Association, Subspecialty Group of Cardiology, The Society of Pediatrics, et al. The Definition of Metabolic Syndrome and Prophylaxis and Treatment Proposal in Chinese Children and Adolescents. Zhonghua Er Ke Za Zhi (2012) 50:420–2. doi: 10.3760/cma.j.issn.0578-1310.2012.06.005
22. Zimmet P, Alberti KG, Kaufman F, Tajima N, Silink M, Arslanian S, et al. The Metabolic Syndrome in Children and Adolescents - an IDF Consensus Report. Pediatr Diabetes (2007) 8:299–306. doi: 10.1111/j.1399-5448.2007.00271.x
23. Fatty Liver and Alcoholic Liver Disease Study Group of the Chinese Liver Disease Association. Guidelines for Diagnosis and Treatment of Nonalcoholic Fatty Liver Diseases. Chin J Hepatol (2006) 14:161–3. doi: 10.3760/j.issn.1007-3418.2006.03.001
24. Loeffler LF, Navas-Acien A, Brady TM, Miller ER 3rd, Fadrowski JJ. Uric Acid Level and Elevated Blood Pressure in US Adolescents: National Health and Nutrition Examination Survey, 1999-2006. Hypertension (2012) 59:811–7. doi: 10.1161/hypertensionaha.111.183244
25. Jin B, Lin H, Yuan J, Dong G, Huang K, Wu W, et al. Abdominal Adiposity and Total Body Fat as Predictors of Cardiometabolic Health in Children and Adolescents With Obesity. Front Endocrinol (2020) 11:579. doi: 10.3389/fendo.2020.00579
26. Lopez-Alvarenga JC, Chittoor G, Paul SFD, Puppala S, Farook VS, Fowler SP, et al. Acanthosis Nigricans as a Composite Marker of Cardiometabolic Risk and its Complex Association With Obesity and Insulin Resistance in Mexican American Children. PLoS One (2020) 15:e0240467. doi: 10.1371/journal.pone.0240467
27. Stoddart ML, Blevins KS, Lee ET, Wang W, Blackett PR. Association of Acanthosis Nigricans With Hyperinsulinemia Compared With Other Selected Risk Factors for Type 2 Diabetes in Cherokee Indians: The Cherokee Diabetes Study. Diabetes Care (2002) 25:1009–14. doi: 10.2337/diacare.25.6.1009
28. Rothman KJ. No Adjustments are Needed for Multiple Comparisons. Epidemiology (1990) 1:43–6. doi: 10.1097/00001648-199001000-00010
29. Caprio S, Santoro N, Weiss R. Childhood Obesity and the Associated Rise in Cardiometabolic Complications. Nat Metabol (2020) 2:223–32. doi: 10.1038/s42255-020-0183-z
30. Bass R, Eneli I. Severe Childhood Obesity: An Under-Recognised and Growing Health Problem. Postgraduate Med J (2015) 91:639–45. doi: 10.1136/postgradmedj-2014-133033
31. Wickham EP, DeBoer MD. Evaluation and Treatment of Severe Obesity in Childhood. Clin Pediatr (2015) 54:929–40. doi: 10.1177/0009922814565886
32. Chinese Work Group of Pediatric Metabolic S. Prevalence of Metabolic Syndrome of Children and Adolescent Students in Chinese Six Cities. Zhonghua Er Ke Za Zhi (2013) 51:409–13.
33. Nehus E, Mitsnefes M. Childhood Obesity and the Metabolic Syndrome. Pediatr Clin North Am (2019) 66:31–43. doi: 10.1016/j.pcl.2018.08.004
34. Maguolo A, Maffeis C. Acanthosis Nigricans in Childhood: A Cutaneous Marker That Should Not be Underestimated, Especially in Obese Children. Acta Paediatr (2020) 109:481–7. doi: 10.1111/apa.15031
35. Yeckel CW, Weiss R, Dziura J, Taksali SE, Dufour S, Burgert TS, et al. Validation of Insulin Sensitivity Indices From Oral Glucose Tolerance Test Parameters in Obese Children and Adolescents. J Clin Endocrinol Metab (2004) 89:1096–101. doi: 10.1210/jc.2003-031503
36. de Assunção SNF, Sorte NCAB, Alves CDD, Mendes PSA, Alves CRB, Silva LR. Glucose Alteration and Insulin Resistance in Asymptomatic Obese Children and Adolescents. J Pediatr (2018) 94:268–72. doi: 10.1016/j.jped.2017.06.008
37. Wang J, Qu HQ, Huang K, Wu W, Wang C, Liang L, et al. High Prevalence of Elevated Serum Liver Enzymes in Chinese Children Suggests Metabolic Syndrome as a Common Risk Factor. J Paediatr Child Health (2020) 56:1590–6. doi: 10.1111/jpc.15038
38. Cuzmar V, Alberti G, Uauy R, Pereira A, Garcia C, De Barbieri F, et al. Early Obesity: Risk Factor for Fatty Liver Disease. J Pediatr Gastroenterol Nutr (2020) 70:93–8. doi: 10.1097/Mpg.0000000000002523
39. Kumar S, Kelly AS. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clin Proc (2017) 92:251–65. doi: 10.1016/j.mayocp.2016.09.017
40. Huang JS, Barlow SE, Quiros-Tejeira RE, Scheimann A, Skelton J, Suskind D, et al. Childhood Obesity for Pediatric Gastroenterologists. J Pediatr Gastroenterol Nutr (2013) 56:99–109. doi: 10.1097/MPG.0b013e31826d3c62
41. de Giorgis T, Marcovecchio ML, Giannini C, Chiavaroli V, Chiarelli F, Mohn A. Blood Pressure From Childhood to Adolescence in Obese Youths in Relation to Insulin Resistance and Asymmetric Dimethylarginine. J Endocrinol Invest (2016) 39:169–76. doi: 10.1007/s40618-015-0351-2
42. Zhai Y, Li WR, Shen C, Qian F, Shi XM. Prevalence and Correlates of Elevated Blood Pressure in Chinese Children Aged 6-13 Years: A Nationwide School-Based Survey. BioMed Environ Sci (2015) 28:401–9. doi: 10.3967/bes2015.057
43. Moyer VA, Force USPST. Screening for Primary Hypertension in Children and Adolescents: U.S. Preventive Services Task Force Recommendation Statement. Pediatrics (2013) 132:907–14. doi: 10.1542/peds.2013-2864
44. Karatzi K, Protogerou AD, Moschonis G, Tsirimiagou C, Androutsos O, Chrousos GP, et al. Prevalence of Hypertension and Hypertension Phenotypes by Age and Gender Among Schoolchildren in Greece: The Healthy Growth Study. Atherosclerosis (2017) 259:128–33. doi: 10.1016/j.atherosclerosis.2017.01.027
45. Cao ZQ, Zhu L, Zhang T, Wu L, Wang Y. Blood Pressure and Obesity Among Adolescents: A School-Based Population Study in China. Am J Hypertens (2012) 25:576–82. doi: 10.1038/ajh.2012.5
46. Lo JC, Chandra M, Sinaiko A, Daniels SR, Prineas RJ, Maring B, et al. Severe Obesity in Children: Prevalence, Persistence and Relation to Hypertension. Int J Pediatr Endocrinol (2014) 2014:3. doi: 10.1186/1687-9856-2014-3
47. Khan L. Pediatric Hypertension. Pediatr Ann (2020) 49:e155–60. doi: 10.3928/19382359-20200320-01
48. Ruilope LM, Chagas AC, Brandao AA, Gomez-Berroteran R, Alcala JJ, Paris JV, et al. Hypertension in Latin America: Current Perspectives on Trends and Characteristics. Hipertens Riesgo Vasc (2017) 34:50–6. doi: 10.1016/j.hipert.2016.11.005
49. Butler ÉM, Suhag A, Hong Y, Liang L, Gong C, Xiong F, et al. Parental Perceptions of Obesity in School Children and Subsequent Action. Childhood Obes (2019) 15:459–67. doi: 10.1089/chi.2018.0338
50. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, Regional, and National Prevalence of Overweight and Obesity in Children and Adults During 1980-2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet (2014) 384:766–81. doi: 10.1016/S0140-6736(14)60460-8.
Keywords: abnormal liver function, acanthosis nigricans, blood pressure, China, glucose metabolism, hypertension, insulin sensitivity, NAFLD
Citation: Wang J, Lin H, Chiavaroli V, Jin B, Yuan J, Huang K, Wu W, Dong G, Derraik JGB and Fu J (2022) High Prevalence of Cardiometabolic Comorbidities Among Children and Adolescents With Severe Obesity From a Large Metropolitan Centre (Hangzhou, China). Front. Endocrinol. 13:807380. doi: 10.3389/fendo.2022.807380
Received: 02 November 2021; Accepted: 28 February 2022;
Published: 19 May 2022.
Edited by:
Elpis Vlachopapadopoulou, Panagiotis & Aglaia Kyriakou Children’s Hospital, GreeceReviewed by:
Tommaso Aversa, University of Messina, ItalyCopyright © 2022 Wang, Lin, Chiavaroli, Jin, Yuan, Huang, Wu, Dong, Derraik and Fu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junfen Fu, ZmpmNjhAemp1LmVkdS5jbg==; José G. B. Derraik, ai5kZXJyYWlrQGF1Y2tsYW5kLmFjLm56
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.