
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 10 January 2023
Sec. Obesity
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1100354
This article is part of the Research TopicThe Impact of Adipose Tissue Dysfunction on Cardiovascular and Renal Disease, Volume IIView all 12 articles
 Zhi-Ying He1Xiao Gu1Lin-Jia Du1
Zhi-Ying He1Xiao Gu1Lin-Jia Du1 Xiang Hu1Xing-Xing Zhang1Li-Juan Yang1Ying-Qian Li1Jing Li1Lin-Yu Pan1
Xiang Hu1Xing-Xing Zhang1Li-Juan Yang1Ying-Qian Li1Jing Li1Lin-Yu Pan1 Bo Yang2,3
Bo Yang2,3 Xue-Jiang Gu1,3*†
Xue-Jiang Gu1,3*† Xiu-Li Lin4*†
Xiu-Li Lin4*†Introduction: The aim of this study was to investigate the associations of neck circumference (NC) and neck-to-height (NHR) with diabetic kidney disease (DKD) in Chinese patients with type 2 diabetes mellitus (T2DM).
Materials and methods: A total of 2,615 patients with prevalent T2DM were enrolled. NHR was calculated through NC (cm) divided by height (cm), and prevalent DKD was defined as the urinary albumin-to-creatinine ratio (UACR) ≥ 30 mg/g or the estimated glomerular filtration rate (eGFR) < 60 ml/min per 1.73 m2 in the absence of other primary kidney diseases.
Results: The levels of NC and NHR were higher in DKD patients compared with non-DKD patients (38.22 vs. 37.71, P = 0.003; 0.232 vs. 0.227, P < 0.001, respectively). After full adjustments, individuals at the highest tertile of NHR had higher odds of DKD than those at the lowest tertile (multivariate-adjusted OR = 1.63, 95% CI: 1.22, 2.18), but this association was not pronounced with NC (multivariate-adjusted OR = 1.24, 95% CI: 0.87, 1.76). Individuals at the highest tertile of NHR had lower eGFR (β = -4.64, 95% CI: -6.55, -2.74) and higher UACR levels (β = 0.27, 95% CI: 0.10, 0.45) than those at the lowest tertile. The adverse association between NHR and prevalent DKD remained statistically significant among most of the subgroups analyzed and no interaction effects were observed.
Conclusion: The increase in NHR was adversely and independently associated with DKD in this Chinese T2DM population.
Diabetic kidney disease (DKD), as one of the most common chronic complications of diabetes, is developed in about 20 - 40% of patients with diabetes (1). Patients with DKD are more likely to progress to end-stage renal disease (ESRD), as well as have a higher risk of cardiovascular diseases (CVD) and all-cause mortality (2, 3). It is vital to discover potential markers to identify patients at a higher risk of DKD.
Obesity is proved to be an important risk factor for kidney damage. Adipose tissue releases a mass of signaling molecules, including inflammatory and hormonal factors, which are critical for inter-organ crosstalk. The communication between adipocytes and the kidney, known as the adipo-renal axis is critical for normal kidney function and the effective response of the kidney to injury (4, 5). Meanwhile, plenty of anthropometric indices of obesity, such as body mass index (BMI), waist circumference (WC), waist-to-hip ratio (WHR), and the Chinese visceral adiposity index (CVAI) have already been reported to be related to DKD (6–8).
Upper-body subcutaneous fat, a unique fat depot independent of generalized and central adiposity, could present extra risk for metabolic disorders (9, 10). Evidence to date have suggested that upper-body subcutaneous fat could always be estimated by neck circumference (NC) (11), which as a simple anthropometric index is not affected by clothing or feeding. However, NC as a regional obesity indicator, could not take the overall body fat distribution fully into account. Neck-to-height ratio (NHR), adjusted for the discrepancies in NC attributable to different heights, shows its advantage in reflecting the whole body fat distribution based on height. And accumulating evidence from clinical studies supported that NHR was a better index for the assessment of upper-body subcutaneous fat than NC in patients with metabolic disorders (12–14). Of note, population-based studies that focused on the relationship between upper-body subcutaneous fat and kidney damage are limited. In populations without diabetes, clinical findings suggested that NC was associated with indicators of kidney dysfunction (15–17). Only a Chinese study targeted subjects with diabetes showed that NC was positively associated with the prevalence of DKD (8). Furthermore, there has been no population-based studies to investigate the association between NHR and renal damage.
Therefore, the goal of our study was to explore the associations of NC and NHR with DKD in patients with type 2 diabetes mellitus (T2DM).
A total of 3267 adults were enrolled from National Metabolic Management Center (MMC) (18, 19) in the First Affiliated Hospital of Wenzhou Medical University from January 2017 to May 2021. 3067 subjects were diagnosed with T2DM according to the diagnostic criteria of World Health Organization (WHO) (20). The exclusion criteria were as followed: 1) patients without data of NC, height measurements, serum creatinine or the urinary albumin–to–creatinine ratio (UACR); 2) patients with acute or chronic nephritis, IgA nephropathy, or other primary kidney diseases, or had kidney space-occupying surgeries before. Finally, 2615 patients were included in the present study. An overview of the patients selected was presented in Figure 1.
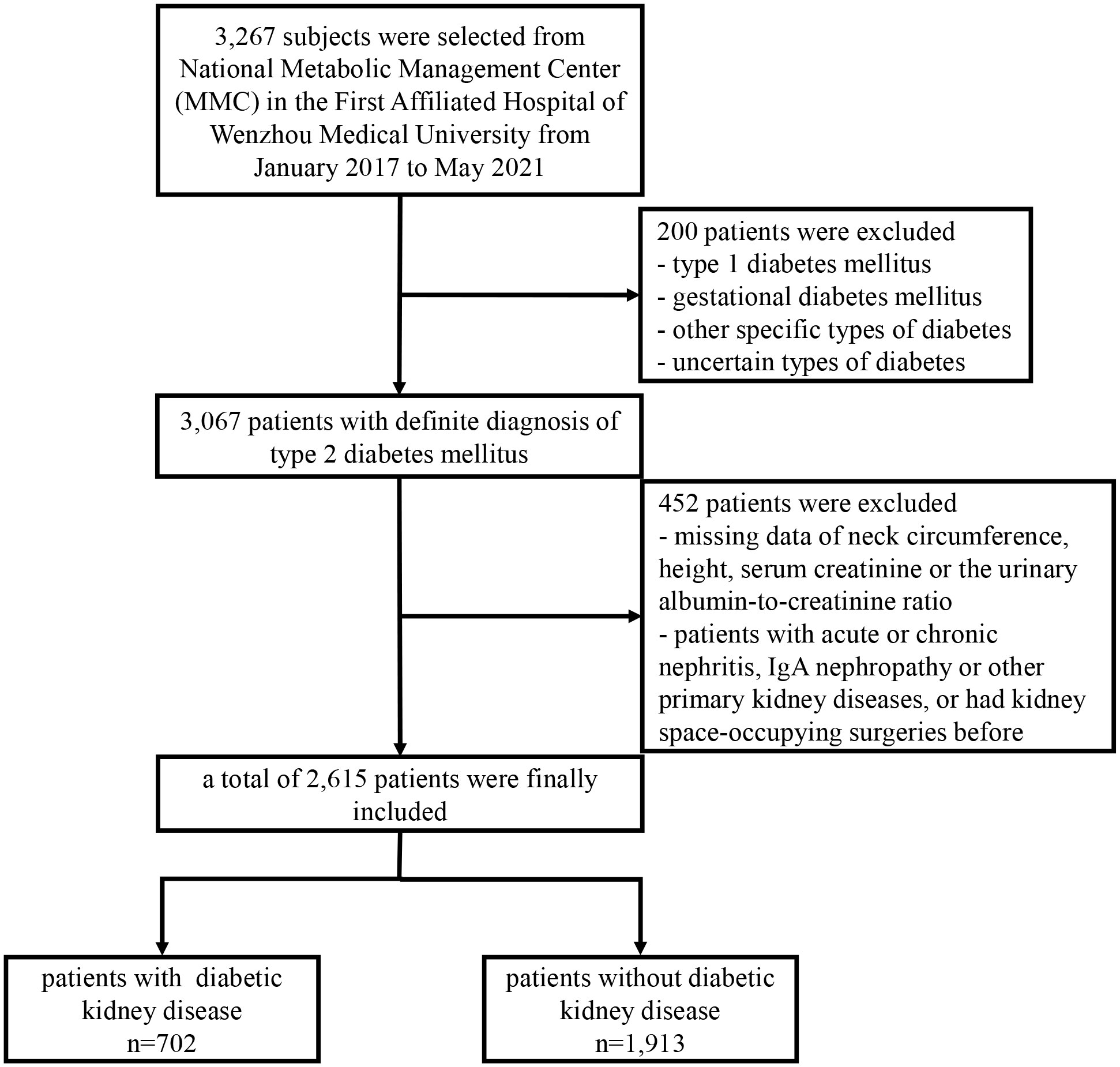
Figure 1 Flowchart of study participants included.
The study was approved by the Ethics Committee in Clinical Research of the First Affiliated Hospital of Wenzhou Medical University (No: KY2021-173), and all participants have been given written informed consent.
Including systolic blood pressure (SBP), diastolic blood pressure (DBP), weight, height, WC and NC were measured by trained staff according to standard protocols. Body weight and standing height were measured accurate to the 0.1 kg and 0.1 cm without shoes or heavy clothes. WC was measured at the midpoint between the lowest rib and the iliac crest. NC was measured with the upper border of a flexible tape placed below the laryngeal prominence and circled vertically to the long axis of the neck (9). BMI was calculated through body weight (kg) divided by the square of height (m2). NHR was calculated through NC (cm) divided by height (cm).
Biochemical indicators, including fasting plasma glucose (FBG), glycosylated hemoglobin A1c (HbA1c), triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and uric acid (UA) were assayed through venous blood samples obtained in the morning after an overnight fast (≥ 8h). Non-HDL-c was calculated through TC minus HDL-C. Serum creatinine (Cr), urinary albumin and urinary creatinine were measured with an automatic biochemical analyzer (Beckmann AU 5800). UACR was ratios of urinary albumin to urinary creatinine, the estimated glomerular filtration rate (eGFR) was calculated according to the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (21).
Diabetes duration, lifestyle factors including education attainment, current smoking and drinking and medication history were all obtained by standardized questionnaires.
DKD was defined as UACR ≥ 30 mg/g or eGFR < 60 ml/min per 1.73 m2, meanwhile in the absence of other primary kidney diseases as suggested by the ADA recommendations (1). Overweight/general obesity was defined as BMI ≥ 24 kg/m2, and central obesity was defined as WC ≥ 90 cm for men, ≥ 85 cm for women, all according to the Guideline for the Prevention and Treatment of Type 2 Diabetes Mellitus in China (22). Hypertension was defined as SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg, or undergoing antihypertensive medication currently (23). Dyslipidemia was defined as TG ≥ 2.3 mmol/L, or TC ≥ 6.2 mmol/L, or HDL-c < 1.0 mmol/L, or LDL-c ≥ 4.1 mmol/L, or non-HDL-c ≥ 4.9 mmol/L, suggested by the 2016 Chinese Guidelines for the Management of Dyslipidemia in Adults (24).
All statistical analyses were performed by SPSS version 26.0 software (IBM Corporation). Data were displayed as means ± standard deviation or as median (interquartile range) for continuous variables, numbers and percentage for categorical variables. Discrepancies between subjects with and without DKD were analyzed using Student’s t test for normally distributed continuous variables, Mann-Whitney U test for abnormally distributed continuous variables, and chi-square test for categorical variables. Multivariable logistic regression models were applied to investigate the relationship between DKD and the tertiles of NC and NHR, odds ratios (ORs) and 95% confidence intervals (CIs) were provided. In addition, multivariable linear regression models were used for eGFR and log-transformed UACR (LnUACR) in relation to the tertiles of NHR. Subgroup analyses were conducted to test the potential interactions between NHR and the other cardiometabolic factors on DKD. For regression models that mentioned above: age and sex were adjusted for in model 1; age, sex, diabetes duration, smoking and drinking status, SBP, TC, FBG were adjusted for in model 2; age, sex, diabetes duration, smoking and drinking status, SBP, TC, FBG, BMI, WC, antidiabetic agents currently and antihypertensive agents currently were adjusted for in model 3. All P values were two-sided and considered statistically significant when < 0.05.
There were 702 (26.85%) patients with DKD and 1913 (73.15%) patients without DKD enrolled in the present study. NC and NHR levels were significantly higher in patients with DKD compared to those without (38.22 vs. 37.71, P = 0.003; 0.232 vs. 0.227, P < 0.001). In contrast to patients without DKD, those with DKD were older, less educated, and had longer diabetes duration, higher proportions of women and non-smokers, as well as had higher levels of SBP, DBP, BMI, WC, FBG, TG, TC, Cr, UACR, UA, current antidiabetic agents, current antihypertensive agents usage and lower height, eGFR (all P < 0.05). There were no statistical differences in current drinking status, HbA1c, HDL-c or LDL-c between the two groups (Table 1).
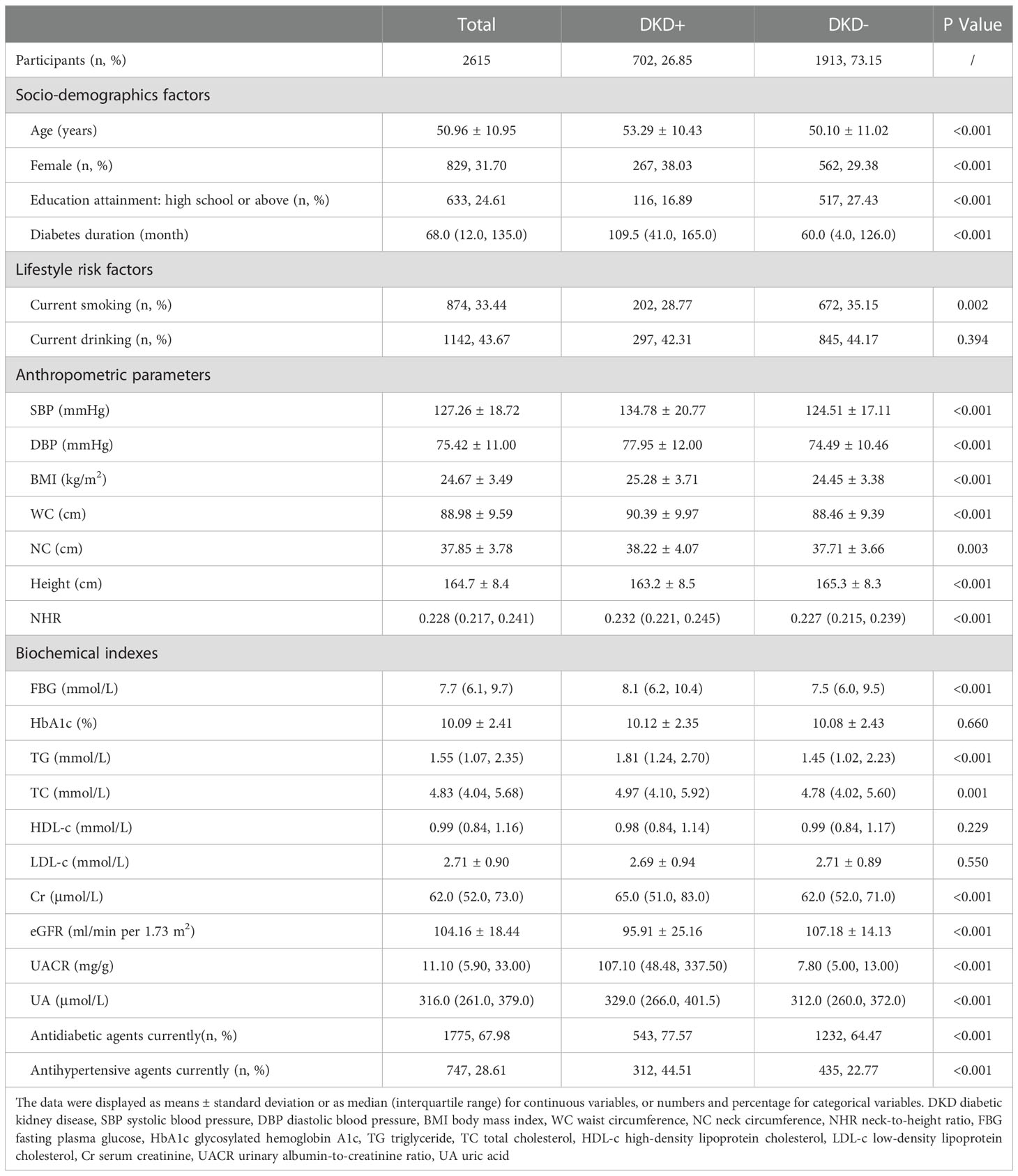
Table 1 Baseline characteristics of study participants based on DKD status.
As shown in Table 2, after full adjustments for age, sex, diabetes duration, smoking and drinking status, SBP, TC, FBG, BMI, WC, antidiabetic agents currently and antihypertensive agents currently, the highest tertile of NC was not associated with prevalent DKD compared to the lowest tertile of NC (OR = 1.24, 95% CI: 0.87, 1.76). However, patients at the highest tertile of NHR were 1.63 times more likely to have DKD (OR = 1.63, 95% CI: 1.22, 2.18) than those at the lowest tertile of NHR in the same full-adjusted model.
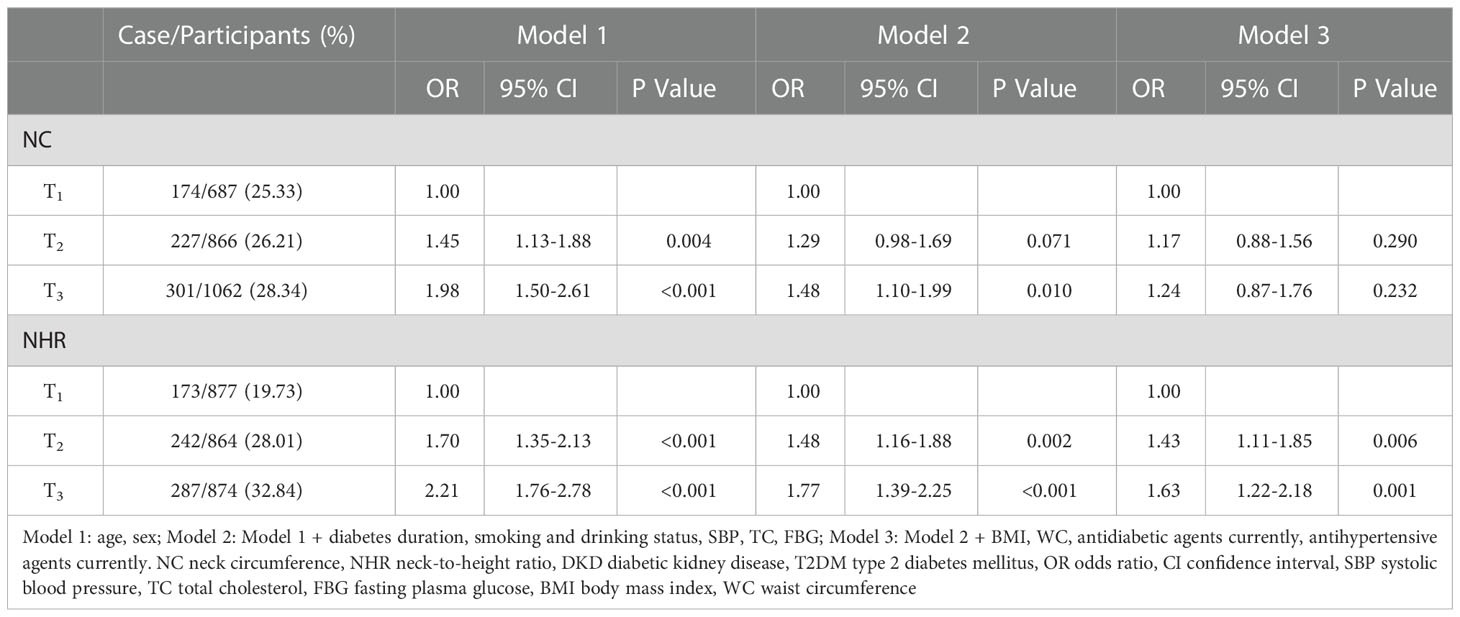
Table 2 Associations of NC and NHR with the prevalence of DKD in patients with T2DM.
The secondary analyses were further performed to explore the associations of NHR with levels of eGFR and UACR. Compared with the lowest one, the highest tertile of NHR was significantly associated with lower eGFR level (β = -4.64, 95% CI: -6.55, -2.74) and higher LnUACR level (β = 0.27, 95% CI: 0.10, 0.45) after full adjustments (Table 3).
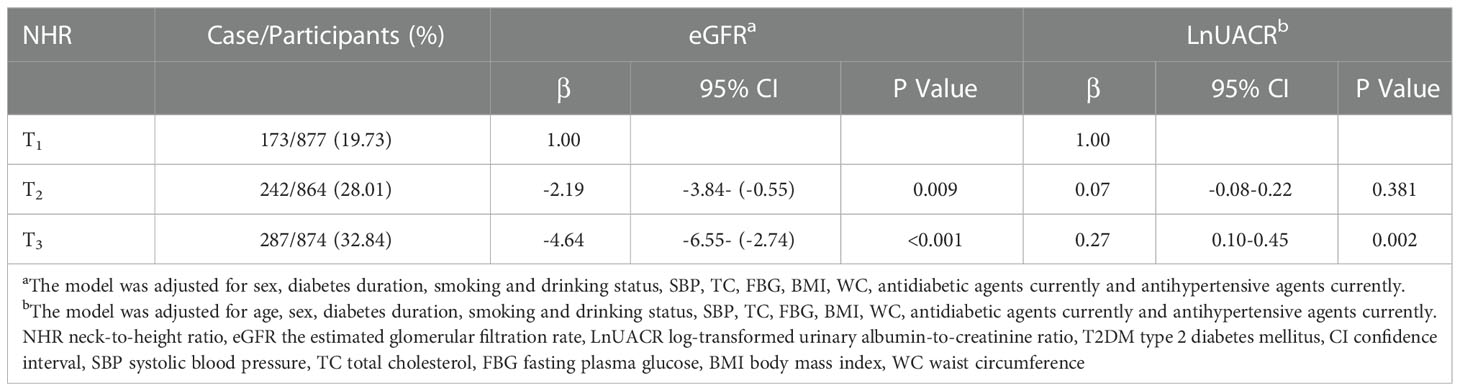
Table 3 Associations between NHR and eGFR/LnUACR level in patients with T2DM.
Interaction effects were analyzed in strata of sex, age, diabetes duration, overweight/general obesity, central obesity, hypertension, and dyslipidemia after total adjustments. As presented in Table 4, participants at the highest tertile of NHR remained at a higher risk of DKD than those at the lowest tertile among most of the strata analyzed, except in those with older age, shorter diabetes duration, central obesity, and in those without overweight/general obesity or dyslipidemia. No interactive effects were observed in any of these strata (all P for interaction > 0.05)
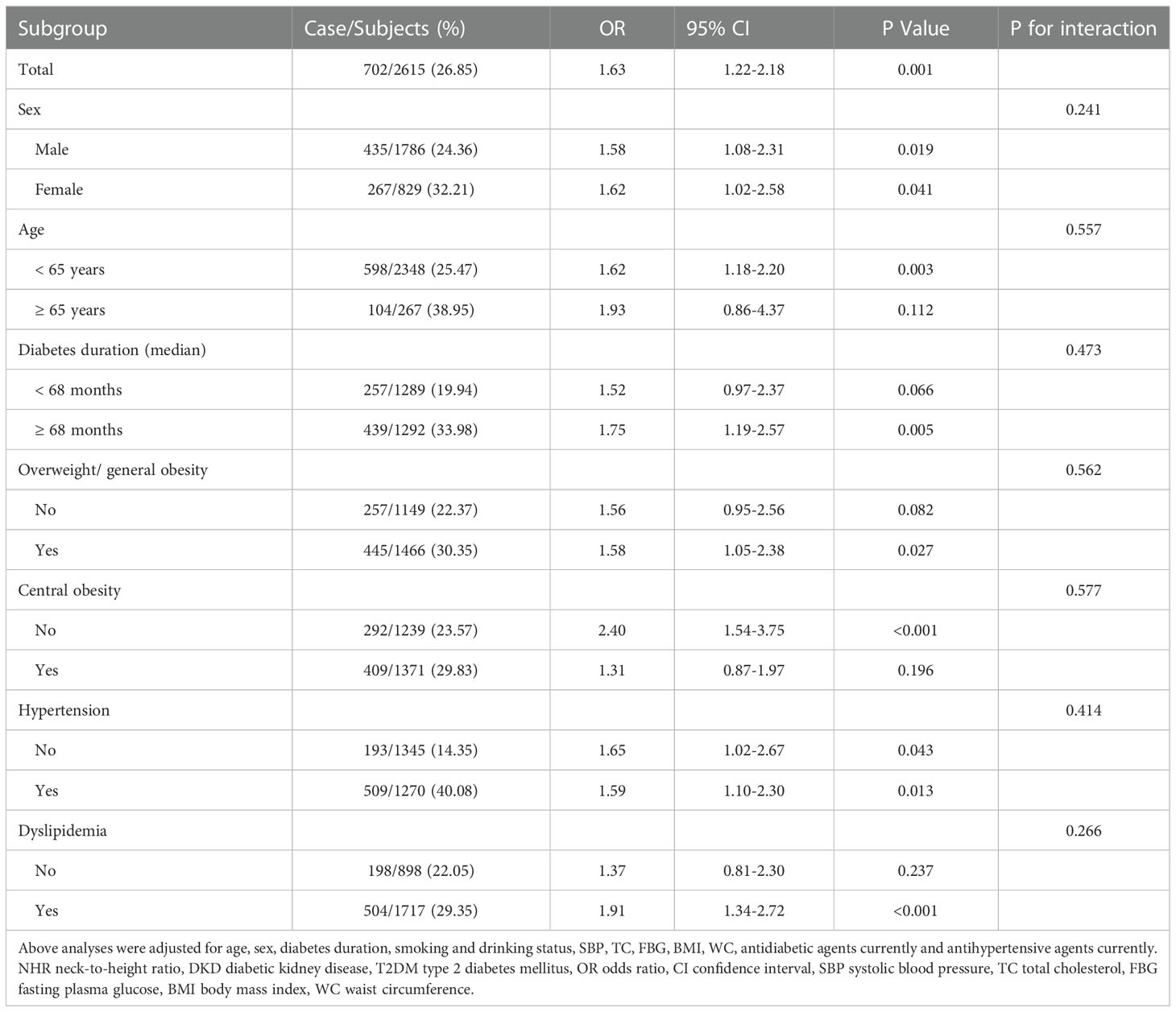
Table 4 Subgroup analyses on the association of NHR with the prevalence of DKD in T2DM patients.
The current study was the first population-based epidemiological study to investigate the associations of NC and NHR, as indicators of upper-body subcutaneous fat, with prevalent DKD in Chinese population with T2DM. Our major finding indicated that NHR, instead of NC, was positively associated with the presence of DKD in patients with T2DM, independent of cardiometabolic risk factors. The increase in NHR was also related to a decrease in eGFR and an increase in UACR levels. Such discoveries suggested that NHR might be a potential indicator for identifying patients at a higher risk of DKD.
Studies about the relationship between NC and kidney dysfunction were limited and inconsistent. A research based on the general Chinese adults found the negative association between NC and eGFR (16). Similarly, a Korean community-based study also showed that eGFR was decreased in subjects with higher NC (17). However, a study including 177 patients with high cardiometabolic risk indicated that larger NC was related to the higher eGFR level (15). The disagreements with these studies might due to different health conditions of populations enrolled and distinct influencing factors considered. A Chinese research hold by Wan et al. showed that NC was positively associated with prevalent DKD, but without further adjusted for WC (8). WC, a proxy for central obesity, was found to be closely related to microalbuminuria and renal damage in patients with diabetes (25–27). Thereby, in order to testify the independent effect of NC on DKD, the impact of WC should be considered. Of note, our study found that the connection between NC and DKD disappeared with adjustments for WC. Moreover, in Xue et al.’s study (16), the negative association of NC with eGFR no longer existed in subjects with diabetes, which suggested that the relationship between NC and eGFR might be concealed by the strongly harmful effect of hyperglycemia on renal function. These results indicated that NC might be unstable and inaccurate to reveal kidney damage in patients with diabetes.
Likewise, several other studies have showed that in contrast to NC, NHR was more closely related to metabolic disorders, such as arterial stiffness, liver stiffness, obstructive sleep apnea syndrome (OSAS) and metabolic syndrome (MetS) (12, 13, 28–30). A community-based study demonstrated that the increase in NHR, rather than NC was related to higher brachial-ankle pulse wave velocity (baPWV) (12). An Indian study revealed that NC and NHR were both great indicators for MetS, but as to cardiovascular risk prediction, NHR was more plausible (29). It’s conceivable that NHR is more reliable than NC to represent for upper-body subcutaneous fat, since it considers the effect of height on whole body fat distribution. However, no studies to date have been done to explore the relationship of NHR with kidney dysfunction in any population. Our study based on Chinese patients with T2DM discovered that NHR was positively associated with prevalent DKD after full adjustments. What’s more, none of the interaction effects of cardiometabolic risk factors, which were all found to be closely related to DKD (1, 7, 31, 32), on the association between NHR and DKD were observed in our study. It indicated that the influence of NHR on DKD was not interfered by these cardiometabolic risk factors and further revealed the relative independence and stability of NHR in its relationship with DKD. Additionally, in consideration of BMI and WC as indicators for generalized and central fat accumulations respectively, our findings might indirectly prove that upper-body subcutaneous fat accumulation, represented by NHR, was indeed the unique fat site, which could confer extra metabolic risks beyond generalized and central obesity (33, 34).
The mechanisms for the association between excessive upper-body subcutaneous fat and the increasing risk of DKD remained unclear. Firstly, upper-body subcutaneous fat releases the majority of free fatty acids (FFAs) (35, 36), which could lead to the endothelial dysfunction and motivate the production of reactive oxygen species (37, 38), thereby having pathogenic effects on kidney, especially on tubulointerstitium (39) and podocytes (40–42). Secondly, larger upper-body subcutaneous fat is closely related to the increasing risk of IR (10, 43). While insulin sensitivity of the glomerular podocytes is vital for normal renal function (44), and previous studies have discovered that IR did propel the development of DKD (45, 46). Thirdly, patients with larger upper-body subcutaneous fat are more likely to have OSAS (47), the latter would accelerate the progress of DKD and other diabetic microvascular complications via promoting oxidative and nitrosative stress (48–50). At last, Mangge et al. proposed that nuchal fat accumulation, by secreting inflammatory cytokines and adipokines (51), might accelerate cell turnover and mitochondrial activity, thus result in telomeres damage and shortening (52). Shorter pieces of telomeres lead to senescent cells and ultimately influence phenotypes and functions of organs (53). Previous studies discovered that patients with shorter telomere length developed increased microalbuminuria, reduced eGFR and impaired kidney function (54–56). Telomere shortening may be another cause for the renal damage due to excessive upper-body subcutaneous fat.
There were several limitations in our study. Firstly, it was a cross-sectional study, causality between NHR and DKD cannot be established. Secondly, our study participants were from a single center and the great majority of them were hospitalized for relative poor glycemic control, it’s generalizability should be verified by involving outpatients or community patients in the future. Thirdly, direct adipose tissue measurements, such as CT or MRI are required to verify the authenticity of NHR. Cohort studies with larger and multicentric samples should also be done.
The present study demonstrated that the higher levels of NHR was significantly associated with the higher presence of DKD in Chinese patients with T2DM, independent of cardiometabolic risk factors. NHR might be a potential indicator for screening renal dysfunction in patients with T2DM, which needs more prospective studies to be confirmed in the future.
The datasets are available from the corresponding author on reasonable request. Requests to access these datasets should be directed to X-JG, Z3V4dWVqaWFuZ0B3bXUuZWR1LmNu.
The study involving human participants were reviewed and approved by the Ethics Committee in Clinical Research of the First Affiliated Hospital of Wenzhou Medical University. The patients/participants provided their written informed consent to participate in this study.
Z-YH has made substantial contributions to the draft of the manuscript, and analysis of data. Z-YH, XG, L-JD, Y-QL, JL, and L-YP have made acquisition of data. XH, X-XZ, L-JY, BY, X-JG, and X-LL have been involved in revising the manuscript. X-JG and X-LL have given final approval of the version to be published. All authors contributed to the article and approved the submitted version.
This study was supported by the Key Research and Development Program of Zhejiang (2021C03069), the Natural Science Foundation of Zhejiang Province (LY20H070003), the National Natural Science Foundation of China (81900737), the Basic Scientific Research Program of Wenzhou Medical University, China (KYYW202015).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. American Diabetes Association. 11. microvascular complications and foot care. Diabetes Care (2019) 42(Suppl 1):S124–S38. doi: 10.2337/dc19-S011
2. Molitch ME, DeFronzo RA, Franz MJ, Keane WF, Mogensen CE, Parving H-H, et al. Nephropathy in diabetes. Diabetes Care (2004) 27 Suppl 1:S79–83. doi: 10.2337/diacare.27.2007.s79
3. Fox CS, Matsushita K, Woodward M, Bilo HJG, Chalmers J, Heerspink HJL, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis. Lancet (9854) 2012:1662–73:380. doi: 10.1016/S0140-6736(12)61350-6
4. Zhu Q, Scherer PE. Immunologic and endocrine functions of adipose tissue: Implications for kidney disease. Nat Rev Nephrol. (2018) 14(2):105–20. doi: 10.1038/nrneph.2017.157
5. Brennan E, Kantharidis P, Cooper ME, Godson C. Pro-resolving lipid mediators: regulators of inflammation, metabolism and kidney function. Nat Rev Nephrol. (2021) 17(11):725–39. doi: 10.1038/s41581-021-00454-y
6. Jiang W, Wang J, Shen X, Lu W, Wang Y, Li W, et al. Establishment and validation of a risk prediction model for early diabetic kidney disease based on a systematic review and meta-analysis of 20 cohorts. Diabetes Care (2020) 43(4):925–33. doi: 10.2337/dc19-1897
7. Man REK, Gan ATL, Fenwick EK, Gupta P, Wong MYZ, Wong TY, et al. The relationship between generalized and abdominal obesity with diabetic kidney disease in type 2 diabetes: A multiethnic Asian study and meta-analysis. Nutrients (2018) 10(11):1685. doi: 10.3390/nu10111685
8. Wan H, Wang Y, Xiang Q, Fang S, Chen Y, Chen C, et al. Associations between abdominal obesity indices and diabetic complications: Chinese visceral adiposity index and neck circumference. Cardiovasc Diabetol (2020) 19(1):118. doi: 10.1186/s12933-020-01095-4
9. Preis SR, Massaro JM, Hoffmann U, D'Agostino RB, Levy D, Robins SJ, et al. Neck circumference as a novel measure of cardiometabolic risk: The framingham heart study. J Clin Endocrinol Metab (2010) 95(8):3701–10. doi: 10.1210/jc.2009-1779
10. Liang J, Teng F, Li Y, Liu X, Zou C, Wang Y, et al. Neck circumference and insulin resistance in Chinese adults: The cardiometabolic risk in Chinese (CRC) study. Diabetes Care (2013) 36(9):e145–e6. doi: 10.2337/dc13-1114
11. Cielo CM, Keenan BT, Wiemken A, Tapia IE, Kelly A, Schwab RJ. Neck fat and obstructive sleep apnea in obese adolescents. Sleep (2021) 44(11):zsab158. doi: 10.1093/sleep/zsab158
12. Yang X, Chen S, Zhou Z, Qiu Y, Zhang J, Wu Y, et al. Neck-to-height ratio and arterial stiffness in Chinese adults: cross-sectional associations in a community-based cohort. J Hypertens (2021) 39(6):1195–202. doi: 10.1097/HJH.0000000000002751
13. Mirr M, Skrypnik D, Bogdański P, Owecki M. Newly proposed insulin resistance indexes called TyG-NC and TyG-NHtR show efficacy in diagnosing the metabolic syndrome. J Endocrinol Invest. (2021) 44(12):2831–43. doi: 10.1007/s40618-021-01608-2
14. Ho AW, Moul DE, Krishna J. Neck circumference-height ratio as a predictor of sleep related breathing disorder in children and adults. J Clin Sleep Med (2016) 12(3):311–7. doi: 10.5664/jcsm.5572
15. Liu Y-F, Chang S-T, Lin W-S, Hsu J-T, Chung C-M, Chang J-J, et al. Neck circumference as a predictive indicator of CKD for high cardiovascular risk patients. BioMed Res Int (2015) 2015:745410. doi: 10.1155/2015/745410
16. Xue J, Li B, Wang J, Yu S, Wang A, An P, et al. Association between neck circumference and the risk of decreased estimated glomerular filtration rate in the general population of China: A cross-sectional study. BioMed Res Int (2020) 2020:3496328. doi: 10.1155/2020/3496328
17. Yoon C-Y, Park JT, Jhee JH, Kee YK, Seo C, Lee M, et al. Neck circumference predicts renal function decline in overweight women: A community-based prospective cohort study. Med (Baltimore). (2016) 95(36):e4844. doi: 10.1097/MD.0000000000004844
18. Zhang Y, Wang Y, Ning G, He P, Wang W. Protecting older people: A high priority during the COVID-19 pandemic. Lancet (2022) 400(10354):729–30. doi: 10.1016/S0140-6736(22)01530-6
19. Zhang Y, Wang W, Ning G. Metabolic management center: An innovation project for the management of metabolic diseases and complications in China. J Diabetes. (2019) 11(1):11–3. doi: 10.1111/1753-0407.12847
20. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabetes Med (1998) 15(7):539–53. doi: 10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
21. Andrassy KM. Comments on 'KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease'. Kidney Int (2013) 84(3):622–3. doi: 10.1038/ki.2013.243
22. Zhu D-L. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Diabetes Mellitus (2021) 13(04):315–409. doi: 10.3760/cma.j.cn115791-20210221-00095
23. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J (2018) 39(33):3021–104. doi: 10.1093/eurheartj/ehy339
24. Zhu J-R, Gao R-L. 2016 Chinese guidelines for the management of dyslipidemia in adults. J Geriatr Cardiol (2018) 15(1):1–29. doi: 10.11909/j.issn.1671-5411.2018.01.011
25. Retnakaran R, Cull CA, Thorne KI, Adler AI, Holman RR. Risk factors for renal dysfunction in type 2 diabetes: U.K. prospective diabetes study 74. Diabetes (2006) 55(6):1832–9. doi: 10.2337/db05-1620
26. de Boer IH, Sibley SD, Kestenbaum B, Sampson JN, Young B, Cleary PA, et al. Central obesity, incident microalbuminuria, and change in creatinine clearance in the epidemiology of diabetes interventions and complications study. J Am Soc Nephrol. (2007) 18(1):235–43. doi: 10.1681/ASN.2006040394
27. Zhao Q, Yi X, Wang Z. Meta-analysis of the relationship between abdominal obesity and diabetic kidney disease in type 2 diabetic patients. Obes Facts. (2021) 14(4):338–45. doi: 10.1159/000516391
28. Mondal SA, Dutta D, Kumar M, Singh P, Basu M, Selvan C, et al. Neck circumference to height ratio is a reliable predictor of liver stiffness and nonalcoholic fatty liver disease in prediabetes. Indian J Endocrinol Metab (2018) 22(3):347–54. doi: 10.4103/ijem.IJEM_31_18
29. Selvan C, Dutta D, Thukral A, Nargis T, Kumar M, Mukhopadhyay S, et al. Neck height ratio is an important predictor of metabolic syndrome among Asian indians. Indian J Endocrinol Metab (2016) 20(6):831–7. doi: 10.4103/2230-8210.192927
30. Katz SL, Blinder H, Naik T, Barrowman N, Narang I. Does neck circumference predict obstructive sleep apnea in children with obesity? Sleep Med (2021) 78:88–93. doi: 10.1016/j.sleep.2020.12.018
31. Giandalia A, Giuffrida AE, Gembillo G, Cucinotta D, Squadrito G, Santoro D, et al. Gender differences in diabetic kidney disease: Focus on hormonal, genetic and clinical factors. Int J Mol Sci (2021) 22(11):5808. doi: 10.3390/ijms22115808
32. Petter B, Laure E, Kara SH, Lori ML, Kristen JN, Maria R, et al. Effects of metabolic factors, race-ethnicity, and sex on the development of nephropathy in adolescents and young adults with type 2 diabetes: Results from the TODAY study. Diabetes Care (2021) 45(5):1056–64. doi: 10.2337/dc21-1085
33. Freedman DS, Rimm AA. The relation of body fat distribution, as assessed by six girth measurements, to diabetes mellitus in women. Am J Public Health (1989) 79(6):715–20. doi: 10.2105/AJPH.79.6.715
34. Ben-Noun LL, Laor A. Relationship between changes in neck circumference and cardiovascular risk factors. Exp Clin Cardiol (2006) 11(1):14–20.
35. Nielsen S, Guo Z, Johnson CM, Hensrud DD, Jensen MD. Splanchnic lipolysis in human obesity. J Clin Invest. (2004) 113(11):1582–8. doi: 10.1172/JCI21047
36. Guo Z, Hensrud DD, Johnson CM, Jensen MD. Regional postprandial fatty acid metabolism in different obesity phenotypes. Diabetes (1999) 48(8):1586–92. doi: 10.2337/diabetes.48.8.1586
37. Ghosh A, Gao L, Thakur A, Siu PM, Lai CWK. Role of free fatty acids in endothelial dysfunction. J BioMed Sci (2017) 24(1):50. doi: 10.1186/s12929-017-0357-5
38. Inoguchi T, Li P, Umeda F, Yu HY, Kakimoto M, Imamura M, et al. High glucose level and free fatty acid stimulate reactive oxygen species production through protein kinase c–dependent activation of NAD(P)H oxidase in cultured vascular cells. Diabetes (2000) 49(11):1939–45. doi: 10.2337/diabetes.49.11.1939
39. Kamijo A, Kimura K, Sugaya T, Yamanouchi M, Hase H, Kaneko T, et al. Urinary free fatty acids bound to albumin aggravate tubulointerstitial damage. Kidney Int (2002) 62(5):1628–37. doi: 10.1046/j.1523-1755.2002.00618.x
40. Allison SJ. Podocyte biology: Free fatty acid-induced macropinocytosis in podocytes. Nat Rev Nephrol. (2015) 11(7):386. doi: 10.1038/nrneph.2015.76
41. Chung J-J, Huber TB, Gödel M, Jarad G, Hartleben B, Kwoh C, et al. Albumin-associated free fatty acids induce macropinocytosis in podocytes. J Clin Invest. (2015) 125(6):2307–16. doi: 10.1172/JCI79641
42. Xu S, Nam SM, Kim JH, Das R, Choi SK, Nguyen TT, et al. Palmitate induces ER calcium depletion and apoptosis in mouse podocytes subsequent to mitochondrial oxidative stress. Cell Death Dis (2015) 6:e1976. doi: 10.1038/cddis.2015.331
43. Chen Y, Zheng X, Ma D, Zheng S, Han Y, Su W, et al. Neck circumference is a good predictor for insulin resistance in women with polycystic ovary syndrome. Fertil Steril. (2021) 115(3):753–60. doi: 10.1016/j.fertnstert.2020.07.027
44. Welsh GI, Hale LJ, Eremina V, Jeansson M, Maezawa Y, Lennon R, et al. Insulin signaling to the glomerular podocyte is critical for normal kidney function. Cell Metab (2010) 12(4):329–40. doi: 10.1016/j.cmet.2010.08.015
45. Karalliedde J, Gnudi L. Diabetes mellitus, a complex and heterogeneous disease, and the role of insulin resistance as a determinant of diabetic kidney disease. Nephrol Dial Transplant. (2016) 31(2):206–13. doi: 10.1093/ndt/gfu405
46. Penno G, Solini A, Orsi E, Bonora E, Fondelli C, Trevisan R, et al. Insulin resistance, diabetic kidney disease, and all-cause mortality in individuals with type 2 diabetes: A prospective cohort study. BMC Med (2021) 19(1):66. doi: 10.1186/s12916-021-01936-3
47. Onat A, Hergenç G, Yüksel H, Can G, Ayhan E, Kaya Z, et al. Neck circumference as a measure of central obesity: Associations with metabolic syndrome and obstructive sleep apnea syndrome beyond waist circumference. Clin Nutr (2009) 28(1):46–51. doi: 10.1016/j.clnu.2008.10.006
48. Misra A, Shrivastava U. Obstructive sleep apnea and diabetic nephropathy. Diabetes Technol Ther (2016) 18(7):405–7. doi: 10.1089/dia.2016.0147
49. Adderley NJ, Subramanian A, Toulis K, Gokhale K, Taverner T, Hanif W, et al. Obstructive sleep apnea, a risk factor for cardiovascular and microvascular disease in patients with type 2 diabetes: Findings from a population-based cohort study. Diabetes Care (2020) 43(8):1868–77. doi: 10.2337/dc19-2116
50. Tahrani AA, Ali A, Raymond NT, Begum S, Dubb K, Altaf Q-A, et al. Obstructive sleep apnea and diabetic nephropathy: A cohort study. Diabetes Care (2013) 36(11):3718–25. doi: 10.2337/dc13-0450
51. Mangge H, Herrmann M, Almer G, Zelzer S, Moeller R, Horejsi R, et al. Telomere shortening associates with elevated insulin and nuchal fat accumulation. Sci Rep (2020) 10(1):6863. doi: 10.1038/s41598-020-63916-6
52. Al-Attas OS, Al-Daghri NM, Alokail MS, Alfadda A, Bamakhramah A, Sabico S, et al. Adiposity and insulin resistance correlate with telomere length in middle-aged arabs: The influence of circulating adiponectin. Eur J Endocrinol (2010) 163(4):601–7. doi: 10.1530/EJE-10-0241
53. Tsirpanlis G. Cellular senescence, cardiovascular risk, and CKD: A review of established and hypothetical interconnections. Am J Kidney Dis (2008) 51(1):131–44. doi: 10.1053/j.ajkd.2007.07.035
54. Bansal N, Whooley MA, Regan M, McCulloch CE, Ix JH, Epel E, et al. Association between kidney function and telomere length: The heart and soul study. Am J Nephrol. (2012) 36(5):405–11. doi: 10.1159/000343495
55. Tentolouris N, Nzietchueng R, Cattan V, Poitevin G, Lacolley P, Papazafiropoulou A, et al. White blood cells telomere length is shorter in males with type 2 diabetes and microalbuminuria. Diabetes Care (2007) 30(11):2909–15. doi: 10.2337/dc07-0633
Keywords: upper-body subcutaneous fat, neck-to-height ratio, neck circumference, diabetic kidney disease, interactive analysis
Citation: He Z-Y, Gu X, Du L-J, Hu X, Zhang X-X, Yang L-J, Li Y-Q, Li J, Pan L-Y, Yang B, Gu X-J and Lin X-L (2023) Neck-to-height ratio is positively associated with diabetic kidney disease in Chinese patients with type 2 diabetes mellitus. Front. Endocrinol. 13:1100354. doi: 10.3389/fendo.2022.1100354
Received: 16 November 2022; Accepted: 19 December 2022;
Published: 10 January 2023.
Edited by:
Cheng-Chao Ruan, Fudan University, ChinaCopyright © 2023 He, Gu, Du, Hu, Zhang, Yang, Li, Li, Pan, Yang, Gu and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiu-Li Lin, d3psaW54aXVsaUAxNjMuY29t; Xue-Jiang Gu, Z3V4dWVqaWFuZ0B3bXUuZWR1LmNu
†These authors have contributed equally to this work and share correspondence authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.