
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 19 January 2023
Sec. Pediatric Endocrinology
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1089160
This article is part of the Research Topic Endocrine and Cardiometabolic Alterations in Pediatric Patients with Chronic Diseases View all 7 articles
 Lourdes Balcázar-Hernández1†
Lourdes Balcázar-Hernández1† Hebert Huerta-Martínez2†
Hebert Huerta-Martínez2† Eulalia Garrido Magaña2Elisa Nishimura-Meguro2Abigail Jiménez Márquez2
Eulalia Garrido Magaña2Elisa Nishimura-Meguro2Abigail Jiménez Márquez2 Aleida Rivera-Hernández2*
Aleida Rivera-Hernández2*Objective: The requirement of a chronic treatment and the increase in life expectancy in children with type 1 diabetes (T1D) leads to the possibility of caregiver burden. The aim of our study was to evaluate the burden in primary informal caregivers (PIC) of children and adolescents with type 1 diabetes and its association with depression, family dysfunction, and glycemic control.
Materials and methods: A retrospective study was performed in PIC of children and adolescents with T1D. Zarit Burden Interview Scale (ZBIS) was used to evaluate caregiver burden. Beck Depression Inventory (BDI-II) was used to evaluate depression in PIC, and the Family APGAR questionnaire was used to evaluate the family functionality.
Results: A total of 100 PIC of children and adolescents with T1D were included. Caregiver burden was found in 33% of caregivers. The total score of the Zarit scale was 41 (34–49); 19% had mild caregiver burden, and 14% had severe caregiver burden. According to the BDI-II, 82% had minimal depression, 11% mild depression, 5% moderate depression, and 2% severe depression. Family function was good in 69%; 13% had moderate dysfunction, and 18% had severe dysfunction. A positive correlation between caregiver burden and BDI-II score (r = 0.84; p = 0.001) and the grade of depression (r = 0.87; p = 0.001) was found. A logistic regression model showed that BDI-II score was associated with caregiver burden (OR 1.14; 95% CI 1.061–1.23; p = 0.001). A BDI-II cut off of 9 or more had a sensibility and specificity of 58% and 28%, respectively, for caregiver burden [AUC 0.751 (0.64–0.85); p = 0.001]. A BDI-II score ≥9 was a predictor of caregiver burden (OR 3.4; 95% CI 1.4–8.1; p = 0.008).
Conclusion: Caregiver burden is present in more than one third of the PIC of patients with T1D and is associated with depression. A BDI-II score ≥9 is a predictor of caregiver burden which may be a point to take into account in the integral approach to the patient with T1D and his or her family nucleus.
Type 1 diabetes (T1D) is a chronic autoimmune disease characterized by pancreatic beta cell destruction, leading to hyperglycemia and to a lifelong insulin-dependent state. The genetic susceptibility combined with environmental factors plays a crucial role in T1D pathophysiology (1). T1D is one of the most frequent chronic diseases in childhood and its incidence is increasing worldwide. In Mexico, the incidence of T1D in children and adolescents is fluctuating, with a reported incidence of 3.4 to 2.8 per 100,000 between 2000 and 2018 in subjects under 20 years of age, which represents an important health problem in our population (2).
The advent of insulin has made it possible to extend the life expectancy of patients with T1D; however, this estimate may vary depending on the population studied and the age at diagnosis of T1D (3, 4).
The increase in life expectancy leads to the need for primary informal caregivers (PIC) and, with it, the possibility of caregiver burden.
Informal caregivers are a critical resource for their recipients and an essential component of health care systems. An informal caregiver, often a family member, provides care to someone with whom he or she has a personal relationship, and is usually unpaid (5).
The PIC face psychosocial challenges that include high levels of psychological symptomatology, reduced social connectedness, and caregiver burden (6). Caregiver burden represents the degree to which caregivers perceive that caring for their patient has had an adverse effect on their emotional, social, financial, physical, and spiritual functioning (7).
It has been reported that caregivers with a high level of emotional overload show a worse self-perception of their health and a higher probability of presenting emotional disorders (8). Some research has documented that depression is the most frequent disorder in PIC, along with anxiety, despondency, and discouragement (9, 10). However; most reports have been in caregivers of adult patients.
In Mexico, most of the medical care in the pediatric population corresponds to the family, particularly in children with T1D. Despite this, little is known about the emotional impact of chronic diseases on PIC. In our population, all caregivers of adult patients with chronic pain have been reported to have multiple symptoms of depression (11); however, information about caregiver burden in caregivers of children and adolescents with chronic illness is lacking.
The aim of our study was to evaluate the burden in PIC of children and adolescents with type 1 diabetes and its association with depression, family dysfunction, and glycemic control.
A cross-sectional study was performed in PIC of children and adolescents with T1D enrolled in the clinic of diabetes at a Pediatric Tertiary Care Center in Mexico City between June 2018 and January 2020. Sociodemographic variables of PIC included age, gender, marital status, relationship to the patient, schooling, socioeconomic level, and occupation. PIC with a previous diagnosis of psychiatric disorder were excluded, as well as those in which complete information was not obtained.
The glycemic control was determinate by glycated hemoglobin (HbA1c). Patients with HbA1c 7.5% or below were considered under control and those with HbA1c >7.5% were considered with decontrolled diabetes (12). HbA1c and time of evolution of T1D was evaluated at the time of caregiver burden evaluation.
The Zarit Burden Interview Scale (ZBIS) was used to evaluate caregiver burden. ZBIS is a validated questionnaire in our population (internal consistency: Cronbach alpha coefficient of 0.84). A score ≤46 excluded caregiver burden, a score between 47 and 55 indicated low caregiver burden, and a score ≥56 indicated intense caregiver burden (13).
The Beck Depression Inventory (BDI-II) was used to evaluate depression in PIC. This inventory has been validated in our population (internal consistency: Cronbach alpha coefficient of 0.87) (29). According to the recommendations in our population, depression was categorized in: minimal depression (score form 0–9), mild (score from 10 to 16), moderate (score from 17 to 29 items puntos), and severe (score from 30 to 63) (14, 15).
The Family APGAR questionnaire was used to evaluate family functionality. The five functional components of the Family APGAR were: Adaptability, Partnership, Growth, Affection, and Resolve. Family function can be categorized as “good” (score from 7 to 10), “moderate dysfunction” (score from 4 to 6), or “severe dysfunction” (score from 0 to 3) (16).
The ZBIS, BDI-II, and Family APGAR questionnaire were performed on those PIC who agreed to participate in the study by the same expert investigator during the doctor’s appointment of patients with T1D. These questionnaires are not routinely administered at the medical visit. Demographic, clinical, and biochemical data were obtained during the routine appointment and from the electronic medical records by the same investigator.
The continuous variables were described as median and interquartile range (IQR). For the categorical variables, proportions were used (expected frequency, prevalence). Two-sample t-test or Mann–Whitney U test were used to compare continuous variables according to the distribution, and for the categorical variables, the χ2 test was used. Correlations of quantitative variables were performed using the Spearman’s rank test. Multivariable logistic regression adjusted by BDI-II score and grade of depression was used to identify risk factors for caregiver burden. An ROC curve was used to estimate the sensibility and specificity of the BDI-II cutoff point for predicting caregiver burden. The area under the ROC curve (AUC), positive predictive value (PPV), negative predictive value (NPV), and likelihood ratios (LR+ and LR-) were used to the measure of test performance. All statistical tests were two-tailed; p < 0.05 was considered statistically significant. We used IBM SPSS Statistics V25.0 (IBM SPSS ®, EEUU) and STATA V14 (StataCorp ®, EEUU) as statistical software.
Of a total of 110 potential PIC of children and adolescents with T1D, 100 were included. Of the excluded PIC, eight had a diagnosis of anxiety and/or depression and in two the information obtained was incomplete.
The age at diagnosis was 11 years (7–14); 89% were women. The evolution time of T1D since the diagnosis was 2.2 (1–4.7) years, and 18% had an adequate control of diabetes in the last 6 months (Table 1).
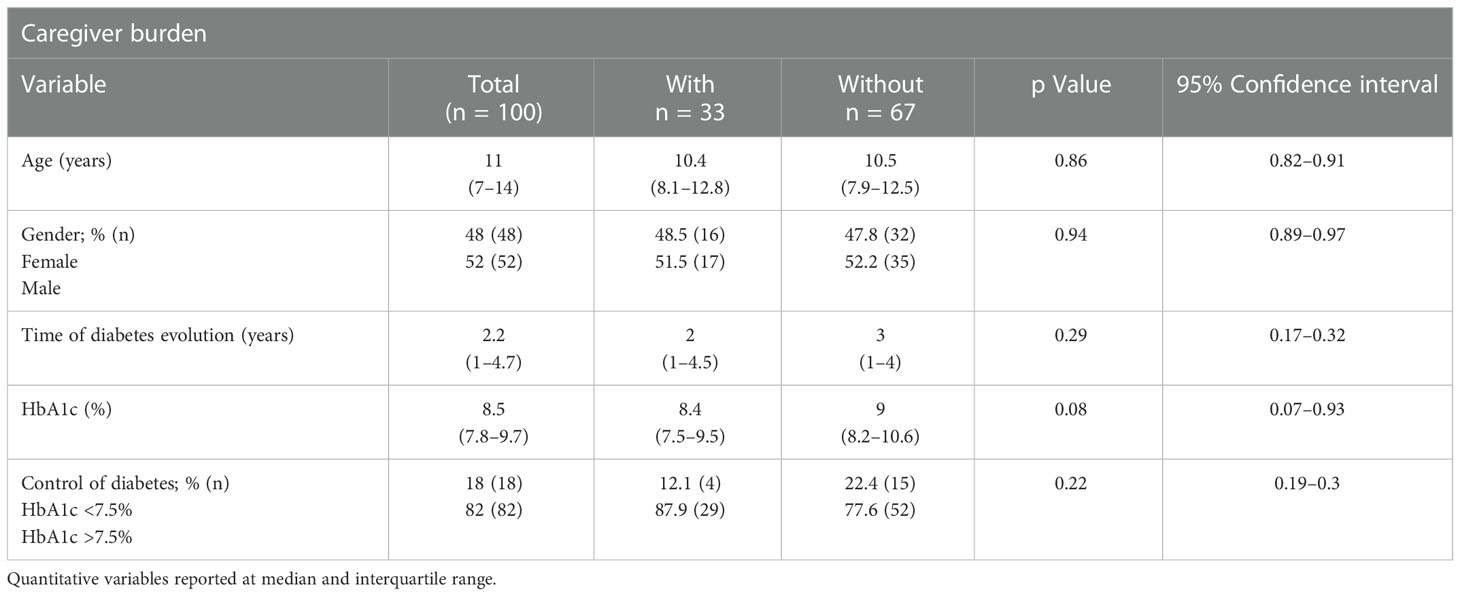
Table 1 Characteristics of children and adolescents with type 1 and differences according to the presence of burden in their primary informal caregivers.
The age at diagnosis was 40 years (36–46); 89% were women. Of the caregivers, 80% were represented by the patient’s mother, 55% had a paid employment in their role as primary caregiver, and 58% attended the “Diabetes Boot Camp” program. The characteristics of caregivers are summarized in Table 2. Caregiver burden was found in 33% (95% CI 0.23–0.4).
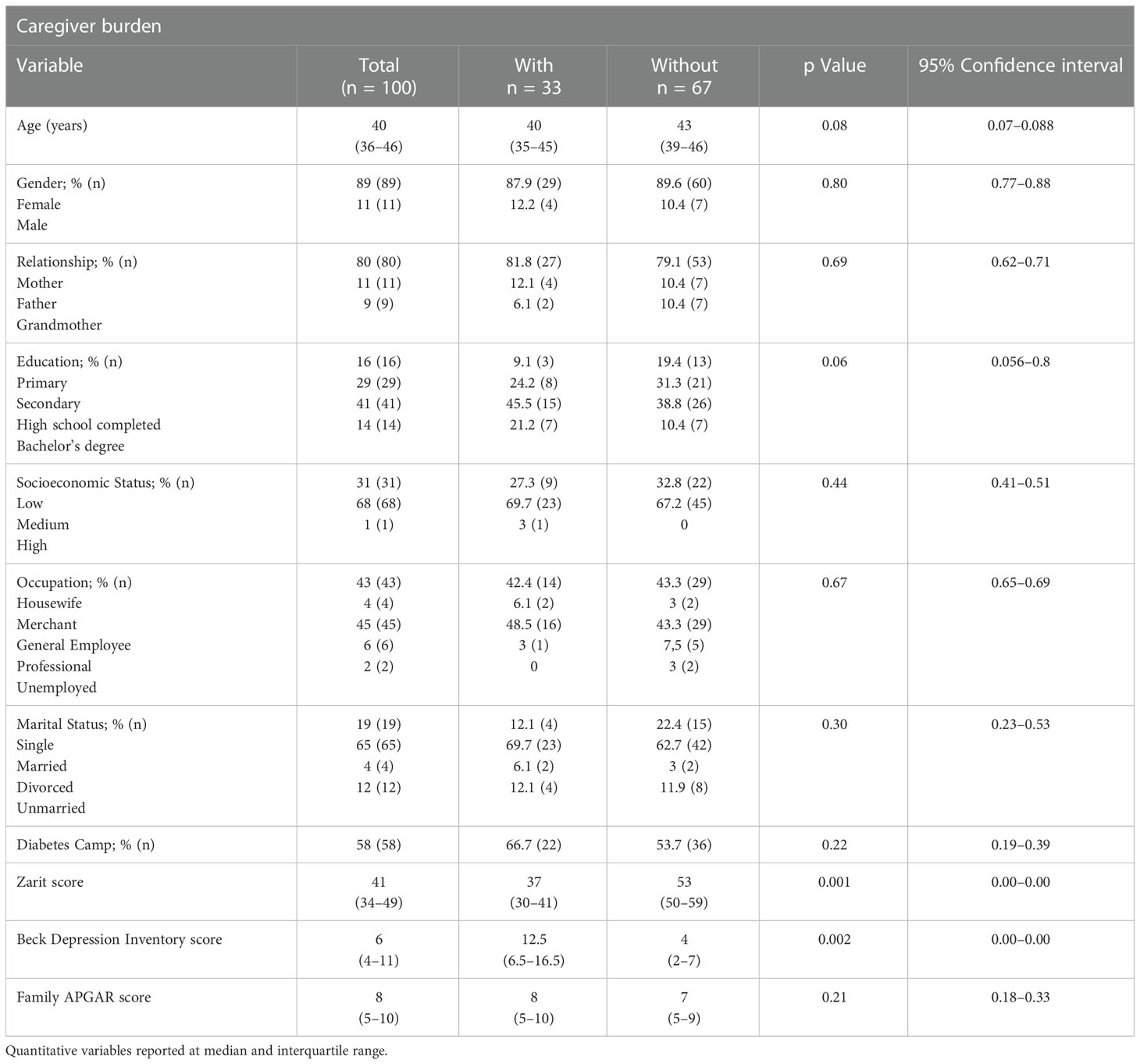
Table 2 Characteristics of primary informal caregivers and differences according to the presence of caregiver burden.
Caregiver burden was found in 33% of caregivers (95% CI 0.23–0.4). The total score of Zarit scale was 41 (34–49); 19% had mild caregiver burden and 14% had severe caregiver burden. Sixty-six percent of caregivers with burden corresponded to patients older than 10 years. The items with the highest scores were: fear of the future, feeling that the patient is dependent, and feeling of having to do more and better. The most affected subscales were interpersonal functioning and self-care activities.
According to the BDI-II, 82% had minimal depression, 11% mild depression, 5% moderate depression, and 2% severe depression. The total BDI-II score was 7 (4–11).
The APGAR score was 8 (5–10). Family function was good in 69%; 13% had moderate dysfunction and 18% had severe dysfunction.
The most affected subscales in PIC with burden were self-care according to ZBIS (78.7%), somatic-affective area (63.6%) according to BDI-II, and partnership (12%) according to APGAR questionnaire (Table 3).
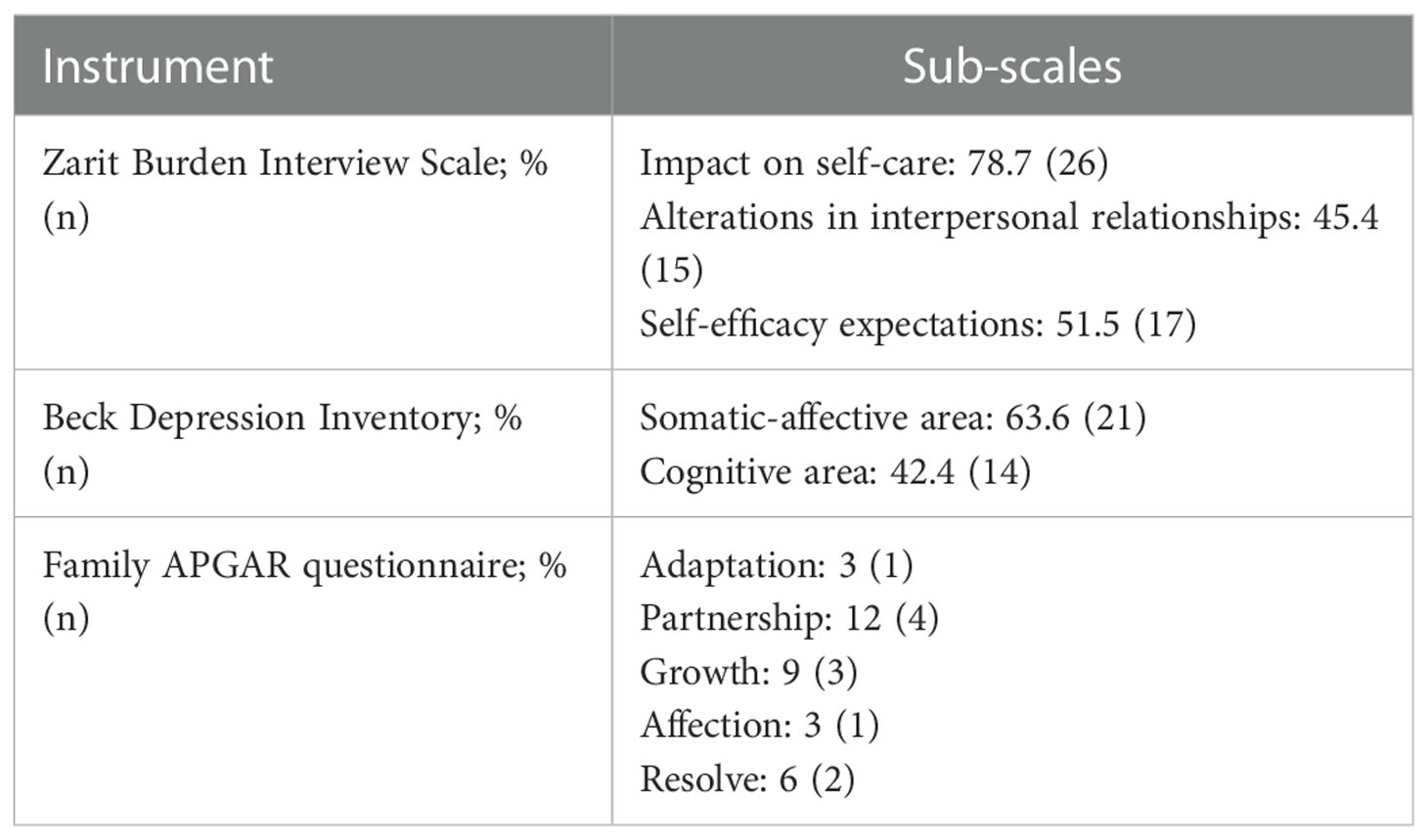
Table 3 Sub-scales of the Zarit Burden Interview Scale, Beck Depression Inventory and Family APGAR questionnaire affected in burdened caregivers (n = 33).
Caregivers with burden were younger than those without burden [40 (35–45) vs. 43 (39–46); p = 0.08]. On the other hand, BDI-II score was higher in caregivers with burden compared to those without burden [12.5 (6.5–16.5) vs. 4 (2–7); p = 0.002]. There were no differences in gender, relationship, scholarliness, occupation, marital status, family APGAR score, and patient clinical parameters as age, gender, and diabetes control (Tables 1, 2). There were no differences in age [11 (7.5–14) vs. 10.5 (5.5–13) years; p = 0.67, 95% CI 0.56–0.8], time of diabetes evolution [3 (2–5.7) vs. 3.2 (1.5–5) years; p = 0.79, 95% CI 0.63–0.85], HbA1c [8.3 (7.9–9.4) vs. 9.8 (7.9–11.25) %; p = 0.23, 95% CI 0.19–0.39], and control of diabetes (p = 0.90, 95% CI 0.85–0.96) of patients comparing PIC with mild and severe burden.
A strong positive correlation between caregiver burden (ZBIS) and BDI-II score (r=0.84; p = 0.001) and the grade of depression (r = 0.87; p = 0.001) was found. There were not association between caregiver burden, sociodemographic variables of caregivers, family APGAR score and clinical characteristics of patients (Table 4). A logistic regression model adjusted by BDI-II score and grade of depression showed that BDI-II score was associated with caregiver burden (OR 1.14; 95% CI 1.061–1.23; p = 0.001), without evidence of association with the grade of depression (OR 1.06; 95% CI 0.45–33.7; p = 0.09).
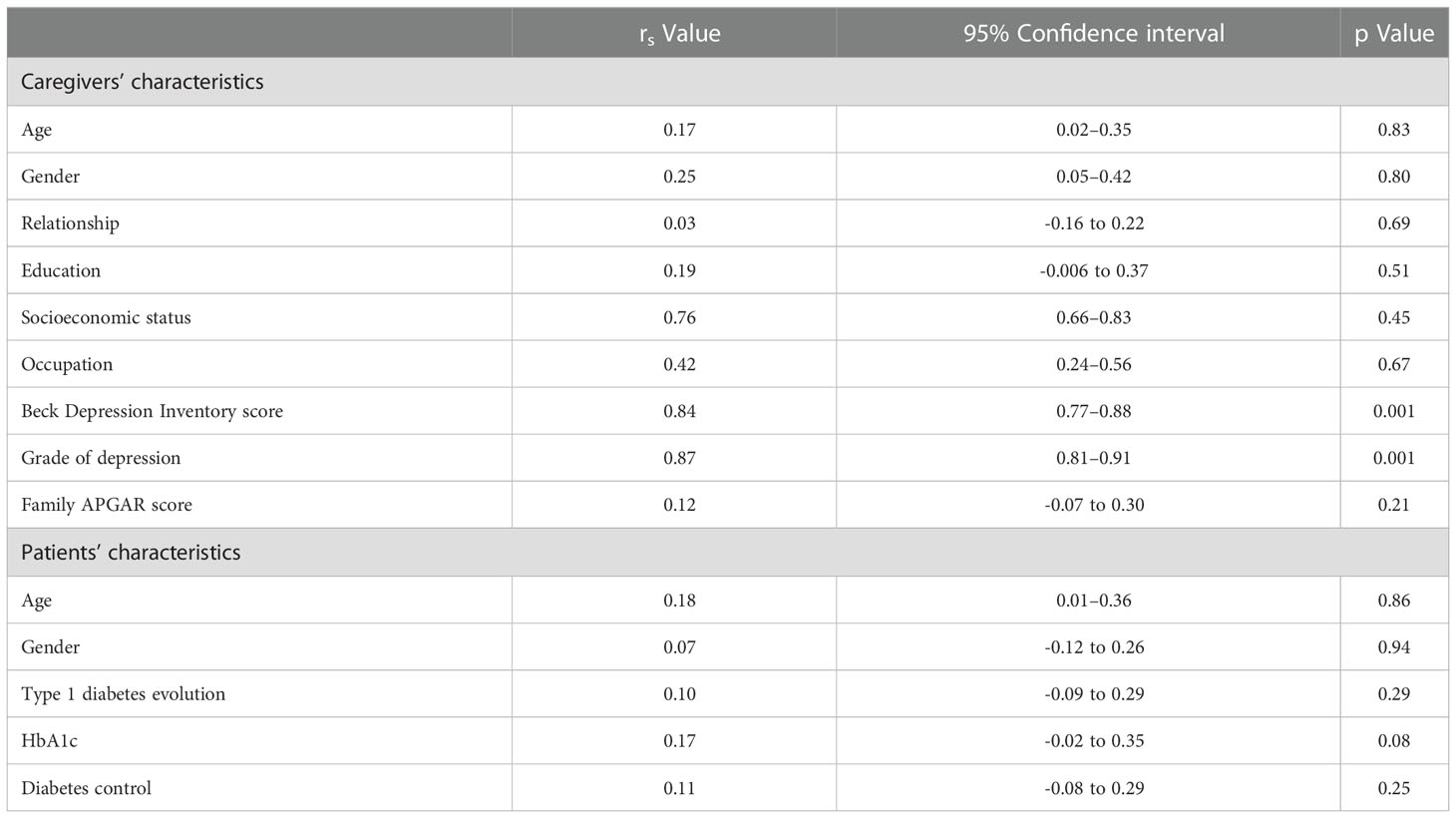
Table 4 Associations between caregiver burden and sociodemographic variables of caregivers, the Beck Depression Inventory score, the family APGAR score, and clinical characteristics of patients.
A BDI-II cut off of 9 or more had a sensibility and specificity of 58 and 72%, respectively, for caregiver burden [AUC 0.751 (95% CI 0.64–0.85); p = 0.0001], with a PPV of 50%, a NPV of 77%, a LR+ of 2.07, and a LR- of 0.58 (post odds +1.02), with a post-test probability of caregiver burden of 50%. A BDI-II score ≥9 was a predictor of caregiver burden (OR 3.4; 95% CI 1.4–8.1; p = 0.008).
In this study, we show that more than one third of the PIC of patients with T1D have caregiver burden according to the Zarit scale. In PIC the main areas affected are interpersonal functioning and self-care activities. Likewise, most patients have depression despite a good family function.
Supporting children with T1D is complex and requires a great deal of effort on the part of the caregiver. There are five inter-related support needs in children with T1D: children need time to adjust to the diagnosis, need supportive relationships, need an opportunity for meaningful participation and appropriate protection, need to engage and explore, and need to feel supported, but not different (17).
The complexity of these needs represents a challenge for the caregiver of the child and adolescent with T1D, which can lead to emotional disturbances such as burden, anxiety, and stress. Mothers of children with newly diagnosed diabetes experience negative consequences in their occupational situation, and this inequality can have long-term negative consequences for their mental health and future economic situation (18).
A recent study reported that 68.9% of mothers of children and adolescents with T1D present moderate to severe burden (19). In our population, the frequency was lower, probably related to the fact that caregivers have emotional tools that allow them to cope with T1D in a better way compared to other populations; however, it is important to highlight that this study was conducted in a tertiary hospital, which implies that patient care may be more supervised, requiring replication of this study design in other populations, taking our finding as a reference.
In children with chronic disease, children’s number of medicines and injections, a diagnosis of attention-deficit/hyperactivity disorder in addition to the primary medical condition, frequent primary care provider and emergency room visits, and lower child self-efficacy were predictors of increased caregiver burden (20). Some factors have been associated with caregiver burden in patients with T1D. An inverse correlation between burden and physical health, social relationships, psychological health, environment, and quality of life has been evidenced (19).
Kobos et al. reported that the level of burden in caregivers of children with T1D correlated with the child’s age, the professional status and level of education of the parents, the number of glycemic tests at nighttime, the frequency of hyperglycemic episodes, and the number of hospitalizations (21); however, in our study there was no significant correlation with any of these variables; likewise, we did not observe a higher number of hospitalizations or a lower educational level of the PIC.
In our study, we evidenced an association of caregiver burden and BDI-II score. These data have not been previously published in the pediatric population with D1T, providing a novel finding and a turning point for future studies. We showed that a BDI-II score ≥9 was a predictor of caregiver burden; however, this data should be taken with caution due to low sensibility and specificity despite an acceptable AUC, low PPV, and small increase in the probability of caregiver burden according to the likelihood ratio.
The caregiver’s burden has consequences in other aspects of his or her life. Caregiver burden has been negatively associated with parents’ quality of life. Resilience serves as a moderator between caregiver burden and mental health, and it is positively associated with life quality. The benefit of high resilience for better mental health in parents with caregiver burden has been proposed (22).
In families with very young children with T1D, parental perceptions of the burden of managing diabetes are common and could be mitigated by tailored education programs that increase parent knowledge, bolster parents’ confidence in themselves, and increase trust in their secondary caregivers to manage diabetes. Reduced parental burden and increased caregiver knowledge may positively impact a child’s glycemic control, as well as improve parent and child quality of life (23)
Among the strengths of our study is the availability of information in a relatively acceptable sample size given the rarity of the disease, as well as the application of three instruments adequately validated in the studied population, which assesses caregiver burden, depression, and family functionality in a small studied population of primary caregivers. In addition, we found an association of caregiver burden with BDI-II scores and, indirectly, with depression. Limitations include its cross-sectional nature, the low sensitivity and specificity of the BDI-II score found in the ROC curve to predict caregiver burden, the difficulty in identifying the direction between depression and caregiver burden, as well as possible selection biases, especially because it was conducted in a tertiary hospital.
Our study denotes the importance of the routine application of instruments aimed at the diagnosis of burden or depression in ICP, and with it, the application of timely prevention or treatment strategies that could influence the long-term prognosis of patients with T1D.
Caregiver burden is present in more than one-third of the PIC of patients with T1D and is associated with depression. A BDI-II score ≥9 is a predictor of caregiver burden which may be a point to take into account in the integral approach to the patient with T1D and his or her family nucleus.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The project was reviewed and approved by the ethics and research committee of the Hospital de Pediatría Dr. Silvestre Frenk Freund, Centro Médico Nacional Siglo XXI of the Instituto Mexicano del Seguro Social. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
All authors contributed substantially to the conception and design of the study, the collection and analysis of data, and the review and editing of the draft. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Primavera M, Giannini C, Chiarelli F. Prediction and prevention of type 1 diabetes. Front Endocrinol (2020) 11:248. doi: 10.3389/fendo.2020.00248
2. Wacher NH, Gómez-Díaz RA, Ascencio-Montiel IJ, Rascón-Pacheco RA, Aguilar-Salinas CA, Borja-Aburto VH. Type 1 diabetes incidence in children and adolescents in Mexico: Data from a nation-wide institutional register during 2000-2018. Diabetes Res Clin Pract (2020) 159:107949. doi: 10.1016/j.diabres.2019.107949
3. Ou HT, Yang CY, Wang JD, Hwang JS, Wu JS. Life expectancy and lifetime health care expenditures for type 1 diabetes: A nationwide longitudinal cohort of incident cases followed for 14 years. Value Health (2016) 19(8):976–84. doi: 10.1016/j.jval.2016.05.017
4. Bhutta ZA, Salam RA, Gomber A, Lewis-Watts L, Narang T, Mbanya JC, et al. A century past the discovery of insulin: global progress and challenges for type 1 diabetes among children and adolescents in low-income and middle-income countries. Lancet. (2021) 398(10313):1837–50. doi: 10.1016/S0140-6736(21)02247-9
5. National Research Council (US) Committee on the Role of Human Factors in Home Health Care. The role of human factors in home health care: Workshop summary. In: Informal caregivers in the united states: Prevalence, caregiver characteristics, and ability to provide care. Washington (DC: National Academies Press (US (2010). Available at: https://www.ncbi.nlm.nih.gov/books/NBK210048.
6. Price ML, Surr CA, Gough B, Ashley L. Experiences and support needs of informal caregivers of people with multimorbidity: a scoping literature review. Psychol Health (2020) 35(1):36–69. doi: 10.1080/08870446.2019.1626125
7. Zarit SH, Todd PA, Zarit JM. Subjective burden of husbands and wives as caregivers: a longitudinal study. Gerontologist. (1986) 26(3):260–6. doi: 10.1093/geront/26.3.260
8. Mittelman MS, Roth DL, Haley WE, Zarit SH. Effects of a caregiver intervention on negative caregiver appraisals of behavior problems in patients with alzheimer’s disease: results of a randomized trial. J Gerontol B Psychol Sci Soc Sci (2004) 59(1):P27–34. doi: 10.1093/geronb/59.1.p27
9. Gálvez Mora J, Ras Vidal E, Hospital Guardiola I, Vila Córcoles A. Perfil del cuidador principal y valoración del nivel de ansiedad y depresión [Profile of the main caregiver and assessment of the level of anxiety and depression]. Aten Primaria. (2003) 31(5):338–9. doi: 10.1016/s0212-6567(03)79191-4
10. Sherwood PR, Given CW, Given BA, von Eye A. Caregiver burden and depressive symptoms: analysis of common outcomes in caregivers of elderly patients. J Aging Health (2005) 17(2):125–47. doi: 10.1177/0898264304274179
11. Alfaro-Ramírez del Castillo OI, Morales-Vigil T, Vázquez-Pineda F, Sánchez-Román S, Ramos-del Río B, Guevara-López U. Sobrecarga, ansiedad y depresión en cuidadores primarios de pacientes con dolor crónico y terminales [Burden, anxiety and depression in patient’s caregivers with chronic pain and in palliative care]. Rev Med Inst Mex Seguro Soc (2008) 46(5):485–94.
12. American Diabetes Association Professional Practice Committee, Draznin B, Aroda VR, Bakris G, Benson G, Brown FM, et al. 6. glycemic targets: Standards of medical care in diabetes-2022. Diabetes Care (2022) 45(Suppl 1):S83–96. doi: 10.2337/dc22-S006
13. Montero X, Jurado S, Valencia A, Mendez J, Mora M. Escala de carga del cuidador de zarit. evidencia validez en México. (2014) 11:71–85. doi: 10.5209/rev_PSIC.2014.v11.n1.44918
14. Jurado S. La estandarización del inventario de depresión de beck para los residentes de la ciudad de méxico. Salud Mental. (1998) 21:26–31.
15. González DA, Reséndiz A, Reyes-Lagunes I. Adaptation of the BDI-II in Mexico. Salud Ment (Mex). (2015) 38(4):237–44. doi: 10.17711/SM.0185-3325.2015.033
16. Zurita-Cruz JN, Nishimura-Meguro E, Villasís-Keever MA, Hernández-Méndez ME, Garrido-Magaña E, Rivera-Hernández AJ. Influence of the informal primary caretaker on glycemic control among prepubertal pediatric patients with type 1 diabetes mellitus. J Pediatr (Rio J). (2017) 93(2):136–41. doi: 10.1016/j.jped.2016.06.008
17. DeCosta P, Grabowski D, Skinner TC. The psychosocial experience and needs of children newly diagnosed with type 1 diabetes from their own perspective: a systematic and narrative review. Diabetes Med (2020) 37(10):1640–52. doi: 10.1111/dme.14354
18. Dehn-Hindenberg A, Saßmann H, Berndt V, Biester T, Heidtmann B, Jorch N, et al. Long-term Occupational Consequences for Families of Children With Type 1 Diabetes: The Mothers Take the Burden. Diabetes Care. 2021 Dec ; 44 (12):2656–2663. doi: 10.2337/dc21-0740
19. Gallegos E, Harmon KB, Lee G, Qi Y, Jewell VD. A descriptive study of the quality of life and burden of mothers of children and adolescents with type 1 diabetes. Occup Ther Health Care (2022) 21:1–17. doi: 10.1080/07380577.2022.2038401
20. Javalkar K, Rak E, Phillips A, Haberman C, Ferris M, Van Tilburg M. Predictors of caregiver burden among mothers of children with chronic conditions. Children (Basel). (2017) 4(5):39. doi: 10.3390/children4050039
21. Kobos E, Imiela J. Factors affecting the level of burden of caregivers of children with type 1 diabetes. Appl Nurs Res (2015) 28(2):142–9. doi: 10.1016/j.apnr.2014.09.008
22. Luo D, Gu W, Bao Y, Cai X, Lu Y, Li R, et al. Resilience outstrips the negative effect of caregiver burden on quality of life among parents of children with type 1 diabetes: An Application of Johnson-Neyman Analysis. J Clin Nurs. 2021 Jul; 30(13-14):1884–1892. doi: 10.1111/jocn.15739
23. Commissariat PV, Harrington KR, Whitehouse AL, Miller KM, Hilliard ME, Van Name M, et al. “I’m essentially his pancreas”: Parent perceptions of diabetes burden and opportunities to reduce burden in the care of children <8 years old with type 1 diabetes. Pediatr Diabetes (2020) 21(2):377–83. doi: 10.1111/pedi.12956
Keywords: type 1 diabetes mellitus, caregiver burden, primary informal caregivers, depression, family dysfunction
Citation: Balcázar-Hernández L, Huerta-Martínez H, Garrido Magaña E, Nishimura-Meguro E, Jiménez Márquez A and Rivera-Hernández A (2023) Burden in primary informal caregivers of children and adolescents with type 1 diabetes: Is it associated with depression, family dysfunction, and glycemic control? Front. Endocrinol. 13:1089160. doi: 10.3389/fendo.2022.1089160
Received: 04 November 2022; Accepted: 27 December 2022;
Published: 19 January 2023.
Edited by:
Jessie Zurita-Cruz, Hospital Infantil de México Federico Gómez, MexicoReviewed by:
Mario Enrique Rendon Macias, Panamerican University, MexicoCopyright © 2023 Balcázar-Hernández, Huerta-Martínez, Garrido Magaña, Nishimura-Meguro, Jiménez Márquez and Rivera-Hernández. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aleida Rivera-Hernández, cmloYTAzMDZAeWFob28uY29tLm14
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.