
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Endocrinol., 10 January 2023
Sec. Obesity
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1071489
This article is part of the Research TopicObesogens in the XXI century: emerging health challenges Volume IIView all 6 articles
 Nina Cecilie Øverby1*
Nina Cecilie Øverby1* Elisabet Rudjord Hillesund1
Elisabet Rudjord Hillesund1 Sissel Heidi Helland1Christine Helle1Andrew Keith Wills1Admassu Nadew Lamu1
Sissel Heidi Helland1Christine Helle1Andrew Keith Wills1Admassu Nadew Lamu1 Natalie Garzon Osorio1Henrik Lian1Torunn Iveland Ersfjord1Wim Van Daele1
Natalie Garzon Osorio1Henrik Lian1Torunn Iveland Ersfjord1Wim Van Daele1 Tormod Bjørkkjær1Erlend Nuland Valen1
Tormod Bjørkkjær1Erlend Nuland Valen1 Mekdes Kebede Gebremariam2Erik Grasaas1Charlotte Kiland3Ulrica von Thiele Schwarz4,5Marianne Hope Abel6
Mekdes Kebede Gebremariam2Erik Grasaas1Charlotte Kiland3Ulrica von Thiele Schwarz4,5Marianne Hope Abel6 Penny Love7Karen Campbell7
Penny Love7Karen Campbell7 Harry Rutter1,8Mary Elizabeth Barker1,9,10Frøydis Nordgård Vik1
Harry Rutter1,8Mary Elizabeth Barker1,9,10Frøydis Nordgård Vik1 Anine Christine Medin1
Anine Christine Medin1Disappointingly few efficacious health interventions are successfully scaled up and implemented in real world settings. This represents an evidence-to-practice gap, with loss of opportunity to improve practice. Aiming to improve nutrition in the first 1000 days of life, we have combined four efficacious dietary interventions into a single adapted digital resource (Nutrition Now) for implementation in a Norwegian community setting. Nutrition Now targets pregnant women and parents of 0–2-year-olds with messages focusing on healthy dietary behaviours. Early childhood education and care (ECEC) staff are provided with pedagogical tools addressing healthy food exposure and child food acceptance. Objectives: a) evaluate the effectiveness of provision of the Nutrition Now resource on child diet and diet-related outcomes, with special attention to the influence of socio-economic position, b) gather information on the effectiveness of the implementation process to inform forthcoming scale-up and c) perform trial- and model-based economic evaluations. This is a hybrid type 1 implementation study, focusing on evaluation of effectiveness. A quasi-experimental design with pre- and post-tests, where one municipality gets access to the resource (n~800), while a matched non-equivalent control municipality (n~800) does not, will be used. Effectiveness will be assessed by examining e.g., diet outcomes, developmental outcomes, and feeding practices. The resource will be implemented in ECEC settings and made available to pregnant women and parents through the Norwegian system of maternal and child health (MCH) care. The implementation process includes iterative adjustments and implementation strategies from the implementation framework Expert Recommendations for Implementing Change (ERIC) informed by dialogues with stakeholders. Implementation outcomes (e.g., acceptability and adoption) will be assessed through questionnaires and interviews with parents, ECEC and MCH staff, with particular attention to ethnic diverse groups. Both within-trial and modelling-based economic evaluation will be performed. Nutrition Now will bridge the existing evidence-to-practice gap through rigorous scientific effectiveness evaluation of municipal scale up and inform subsequent county scale up. The study is the first to implement efficacious nutrition interventions in early life with potential for health improvement using technology to maximise the reach and impact of both parental and MCH dietary guidance and ECEC practice.
Clinical Trial Registration: https://www.isrctn.com/, identified ISRCTN10694967.
Research on the effectiveness of dietary interventions and their public health impact in real-world, high-income settings is scarce (1). Further, only a fraction of efficacious health interventions have been successfully scaled up and implemented in real life settings (2). This represents a clear evidence-to-practice gap, with a loss of opportunity to improve practice and an unnecessary waste of resources (3).
The first 1000 days of life, from conception until a child’s second birthday, is a window of opportunity for promoting long-term health and well-being (4). Failure to meet nutritional needs in this period is strongly linked to raised lifelong risk of obesity and non-communicable diseases (NCDs) (5). The importance of diet-related interventions in the first 1000 days can be ascribed to at least three mechanisms operating at different levels. First, unmet demands in this critical phase of early development can affect the size and structure of organs, increasing the risk of developing hypertension, cardiovascular disease, type 2 diabetes, and obesity (6). Extensive growth and neurodevelopment take place in this period, and optimal development depends on the amount and quality of food and nutrients provided (4, 7). Second, adverse nutritional conditions may permanently affect gene expression and program the body towards the development of NCDs (8). Third, dietary preferences and food habits are formed early in life, influenced by feeding practices of parents and others, the variety of foods offered (9), and the socioeconomic, cultural and educational context of the family (10). The public health significance of the first 1000 days is supported by cost-benefit and cost-effectiveness analyses showing large economic and social returns from early-life investment, especially from optimising nutrition (11).
The World Health Organization (WHO) promotes a lifecourse approach to promoting health and eradicating health inequality (12). A lifecourse approach to nutrition focuses on targeting nutrition during sensitive dietary transitions, such as the initiation and maintenance of breastfeeding, the introduction of complementary foods, and the transition to early childhood education and care (ECEC) when meals are eaten outside the home environment and shared with peers (13). These transitions need to be acknowledged and addressed through primary care and an education system, which aims to give parents and ECEC providers knowledge and skills to support their children to acquire dietary habits that promote rather than constrain their future health.
The Norwegian government sets goals to improve population diet and dietary habits in the Norwegian National Action Plan for a Healthier Diet (2017–21), which has since been extended to 2023 (14). The mid-term evaluation report, launched in June 2020, reveals that Norway is not on track to reach these goals and that much remains to be done in all age groups (15). One example is the large increase in the use of commercial baby food pouches, which rose from no usage in 2008 to 61% of 6 months old receiving them almost every day in 2020 (16, 17). These pouches are convenient, but their contents are often high in sugar (18, 19). Frequent use of such products limits texture and flavour learning, prevents use of healthy feeding practices such as responsive feeding, and increases the risk of childhood obesity (18). The inadequate and sometimes complete lack of vegetables served in ECEC settings is another example (20). Further, unacceptably large differences exist across socioeconomic groups regarding diet during pregnancy, infant and child feeding practices and overall diet quality (21, 22).
Dietary care is a complex part of child rearing. Hence, many parents seek out information on diet and feeding practices, some from questionable sources such as social media influencers (23, 24). There is a potential role for primary health services (Maternal and Child Health (MCH) care) to support parents to develop appropriate skills in feeding their child, regardless of background. The INFANT study demonstrated an untapped potential for integrating flexible, evidence-based e-learning resources to support in-person food-based dietary guidance (25). ECEC is another municipal service that is important for child diet, and which represents an opportunity to enhance meal interactions and diet quality. In Norway, most children from 1 to 5 years attend ECEC, including almost 90% of 1–2-year-olds (26). Throughout a child’s total time spent in ECEC an estimated 3000-4000 meals are eaten. Thus, ECEC offer an important setting for exposure to healthy foods; staff’s feeding style and practices may play a significant role in establishing early healthy eating habits in Norway’s children (27). Stakeholders at municipality level can support citizens’ adoption of a healthy diet early in life through strategies, prioritizing efforts and resources that enhance health and wellbeing in target groups.
We have previously developed and reported on the efficacy of four interventions that target diet during pregnancy, parental feeding practices, and ECEC diet quality and meal environment, respectively. All four interventions have shown promising indications of dietary improvement (28–32) (Additional File 1, Table S1). These interventions are digital, largely video-based and grounded in social cognitive theory (33), addressing the interaction between person, environment, and behaviour. In the Nutrition Now project, we have combined these four interventions into one joint e-learning resource (the Nutrition Now resource) for parents, MCH staff and ECEC staff. The Nutrition Now resource will be implemented in one municipality through municipal services for MCH care (age: 0-2 years) and ECEC departments for children aged 1-3 years, as shown in Figure 1, which depicts hypothesised mechanisms to explain how the intervention may work. Increased knowledge, skills, and motivation are thought to improve dietary behaviors and feeding practices that will in turn affect pregnancy, infant and toddler health outcomes. We also aim for the implementation to influence local policy relating to physical and social aspects of the food environment. The ultimate goal of the Nutrition Now project is to reduce the burden of obesity and NCDs and improve health in quality of life in Norway through improved diet and diet-related behavior in the first 1000 days of life (Figure 1).
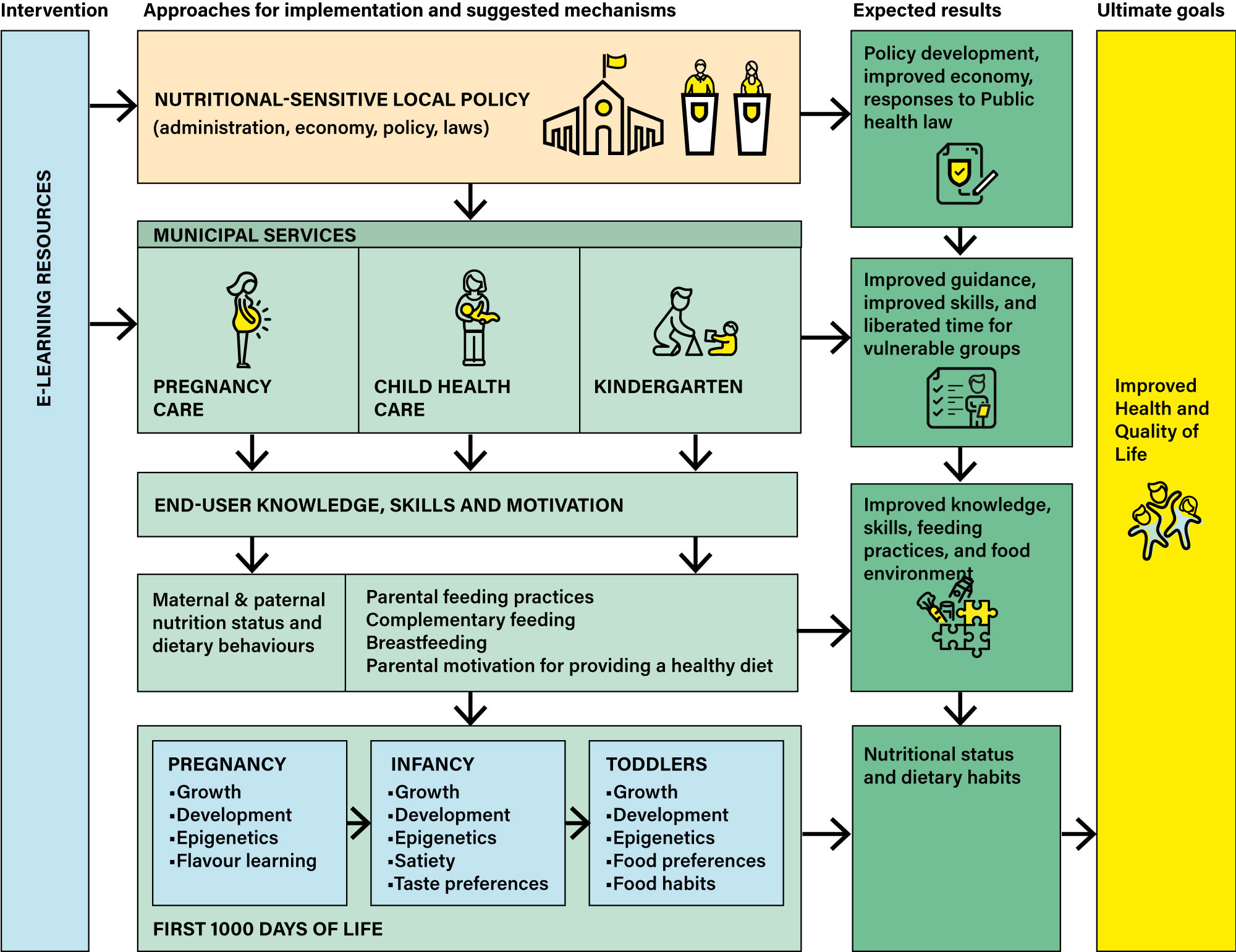
Figure 1 Logic model for Nutrition Now.
The Nutrition Now Project comprises two studies, with the results of the first informing the second. The field of dissemination and implementation research is constantly evolving. While the established standards of evidence for efficacy, effectiveness and scale-up research (34) have more distinct phases of effectiveness and implementation, newer hybrid designs propose to increase the speed of moving research into practice by blending the two stages of effectiveness evaluation and implementation, emphasising either effectiveness or implementation dependent on the type of hybrid study. The current study is a hybrid type 1 study [according to criteria from Curran et al. (35) and Landes et al. (36)] focused primarily on evaluating the effectiveness of providing access to the Nutrition Now resource, and secondly on evaluating implementation and cost-effectiveness. The subsequent study will be a hybrid type 3 study with a primary focus on implementation outcomes (35, 36). Scale up of the Nutrition Now resource to county level will be described in a later paper.
The aim of the study is to assess the impacts on child diet quality of implementing an e-learning resource (the Nutrition Now resource) comprising four digital interventions of known individual efficacy in a community setting.
The three main objectives are to a) evaluate the effectiveness of the Nutrition Now resource on outcomes related to diet and diet-related behaviors in early life, with special attention to the influence of socio-economic position b) observe and gather information on the implementation process to identify implementation strategies for use in a forthcoming scale up, with a special focus on ethnic minority groups and c) perform both trial- and model-based economic evaluations of the implemented Nutrition Now resource.
The outcomes from this study are divided into three main categories: effectiveness outcomes, implementation outcomes, and outcomes from the economic evaluation (Figure 2). The effectiveness and implementation outcomes are measured on both the individual, organisational, and community level. An overview of all outcomes, the evaluation data relating to these outcomes, the level of measurement, and the instruments that will be used to collect the data is shown in Table 1.
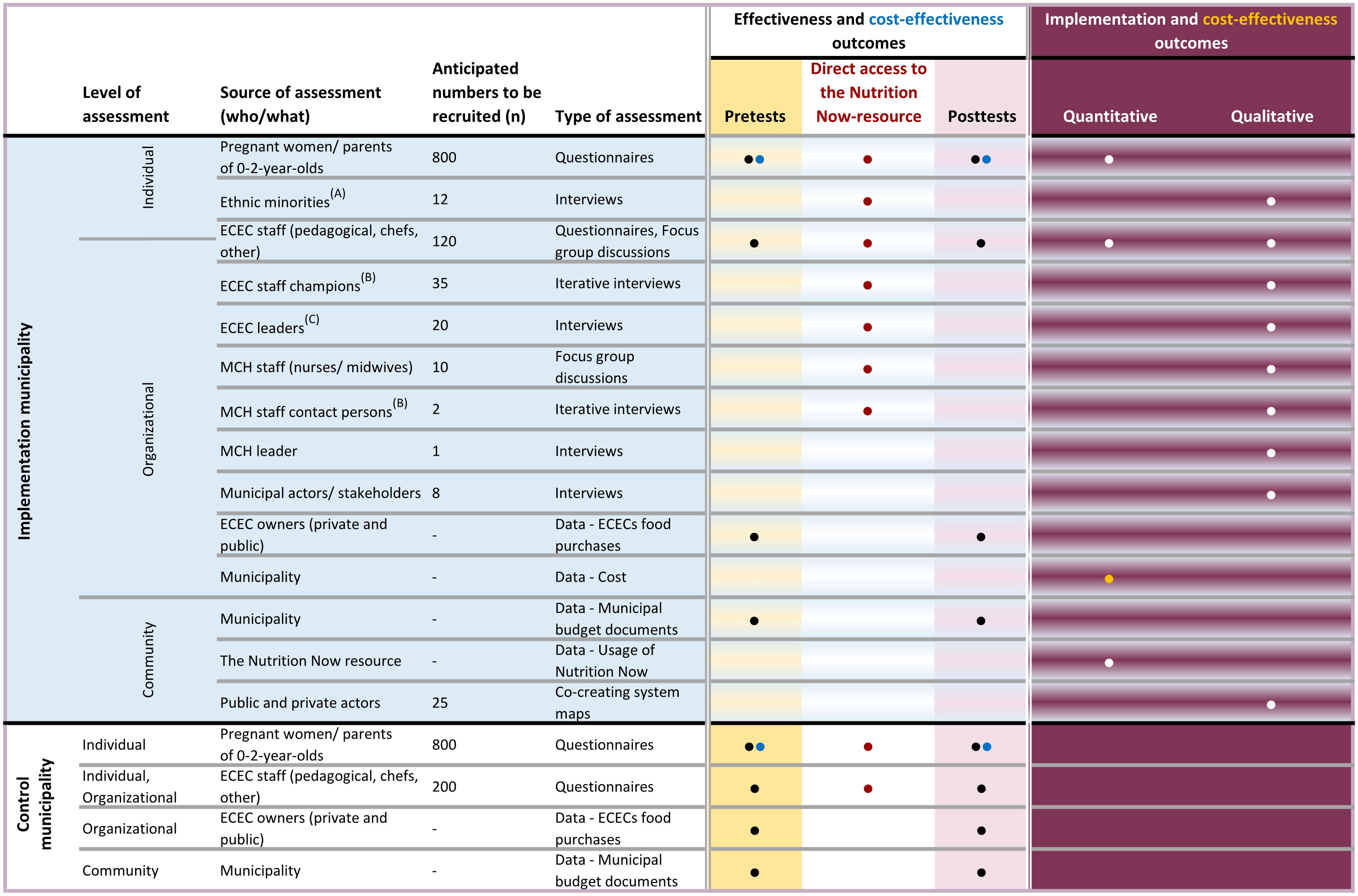
Figure 2 Overview of assessments, participants, and types of outcome measures in the mixed methods Hybrid 1 trial of the Nutrition Now project. (A) Ethnic minorities invited to participate in qualitative interviews in addition to the assessment that applies to all recruited pregnant women/parents of 0-2 year-olds. (B) ECEC staff champions and MCH staff contact persons are appointed staff members invited to participate in short iterative interviews. (C) ECEC leaders provide socio-demographic data for the effectiveness evaluation to be assessed at the ECEC level in addition to qualitative interviews.
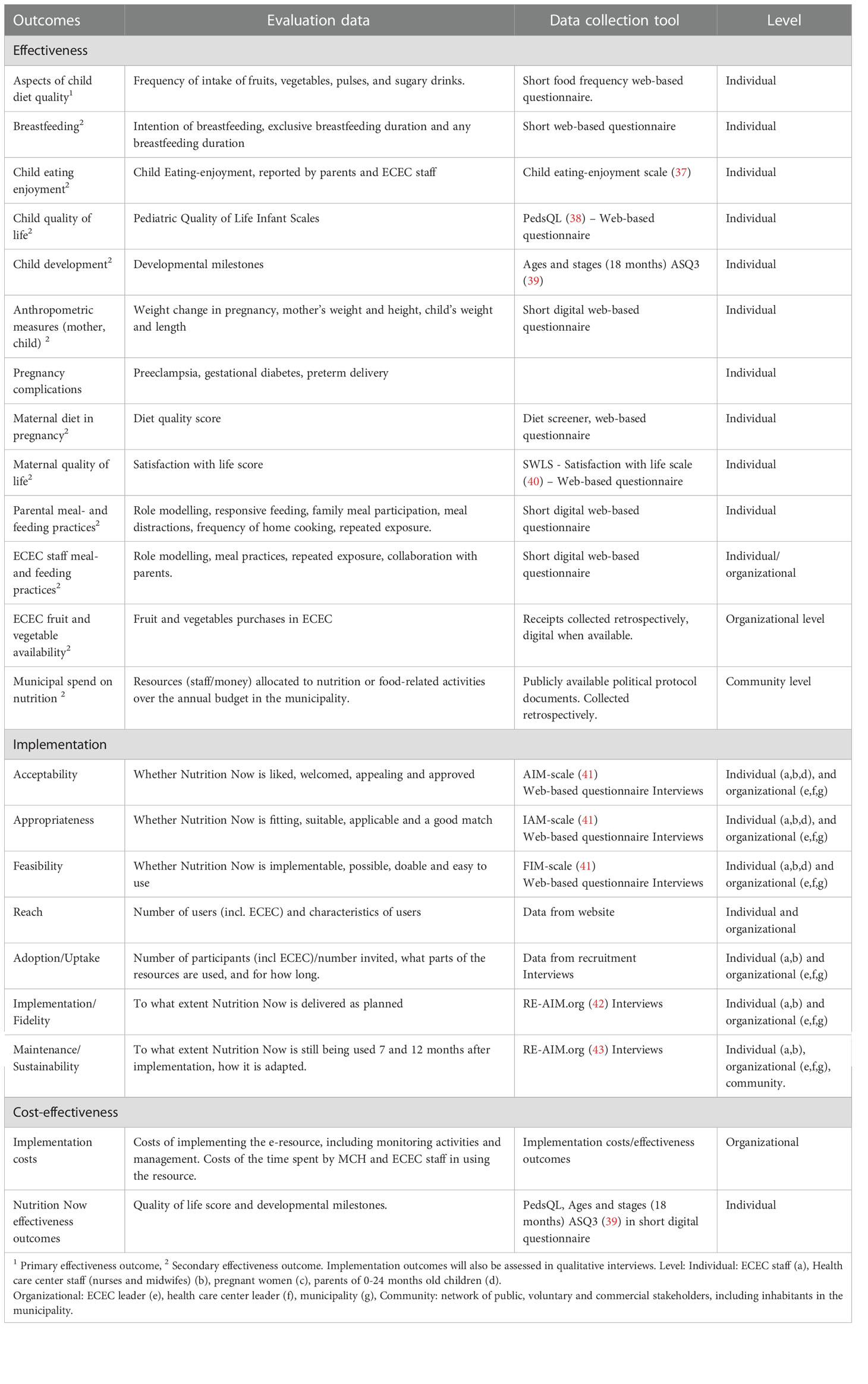
Table 1 Effectiveness, implementation and cost-effectiveness outcomes in Nutrition Now.
The primary effectiveness outcome is aspects of child diet quality, represented by intake of vegetables, fruits and berries, legumes/pulses and sugar sweetened beverages. Secondary outcomes include a) breastfeeding rates (including mixed feeding), b) child eating enjoyment c) health-related quality of life (infant), d) child development measures, e) self-reported anthropometrics (parental and child), f) maternal diet, g) maternal quality-of-life measures h) pregnancy complications, i) parental feeding practices, j) ECEC staff feeding practices k) ECEC fruit and vegetable availability and l) municipal spend on activities related to early childhood nutrition and feeding practices (see Table 1).
Seven outcomes will be used to evaluate the implementation process, including i) reach, ii) adoption, iii) implementation (fidelity), and iv) maintenance, as defined by RE-AIM (44, 45), and v) acceptability, vi) appropriateness and vii) feasibility, as defined by Proctor et al. (46) (Table 1). In addition, we will specifically assess adoption, acceptability, appropriateness, and feasibility in an ethnically diverse sample.
The cost-effectiveness outcomes that will be evaluated are implementation costs in relation to the effectiveness outcomes child health-related quality of life and development measures.
In this hybrid type 1 mixed methods implementation study we use a quasi-experimental design. The CONSORT Extension for pragmatic trials with its checklist was used (47). A single intervention municipality will be given access to the Nutrition Now resource and another control municipality (non-equivalent control) will continue as normal (Figure 2). Data from participants resident in the intervention municipality will be collected in the form of a pretest before they are given access to the Nutrition Now resource. Subsequently post-test data will be collected until the child reaches 2 years of age (See Data collection). Participants in the control municipality will be asked to provide pre- and post-test data but will not receive access to the Nutrition Now resource. Additionally, a time-series design will be used for comparisons within the intervention municipality between groups of participants exposed to the Nutrition Now resource at different levels of duration, and different types of exposure (See Data collection).
Enrolment started September 2022. The anticipated recruitment period is from September 2022-to April 2023, and we envision that the last participant (if recruited in early pregnancy in April 2023) will complete the study in September 2025. The ECECs were recruited prior to September 2022 and MCH personnel and parents will be recruited autumn 2022.
Intervention municipality provision of access to the Nutrition Now resource starts upon enrollment in the study and is expected to continue beyond the study period as long as the municipality finds it useful.
The intervention and control municipalities are situated in different counties in coastal areas in the south of Norway. They have broadly comparable demographics: for example, they are comparable with respect to population size (appr. ~46000 inhabitants), number of births per year (~400), number of ECECs (54 vs 39) as well as education level, income, and family composition (Table 2).
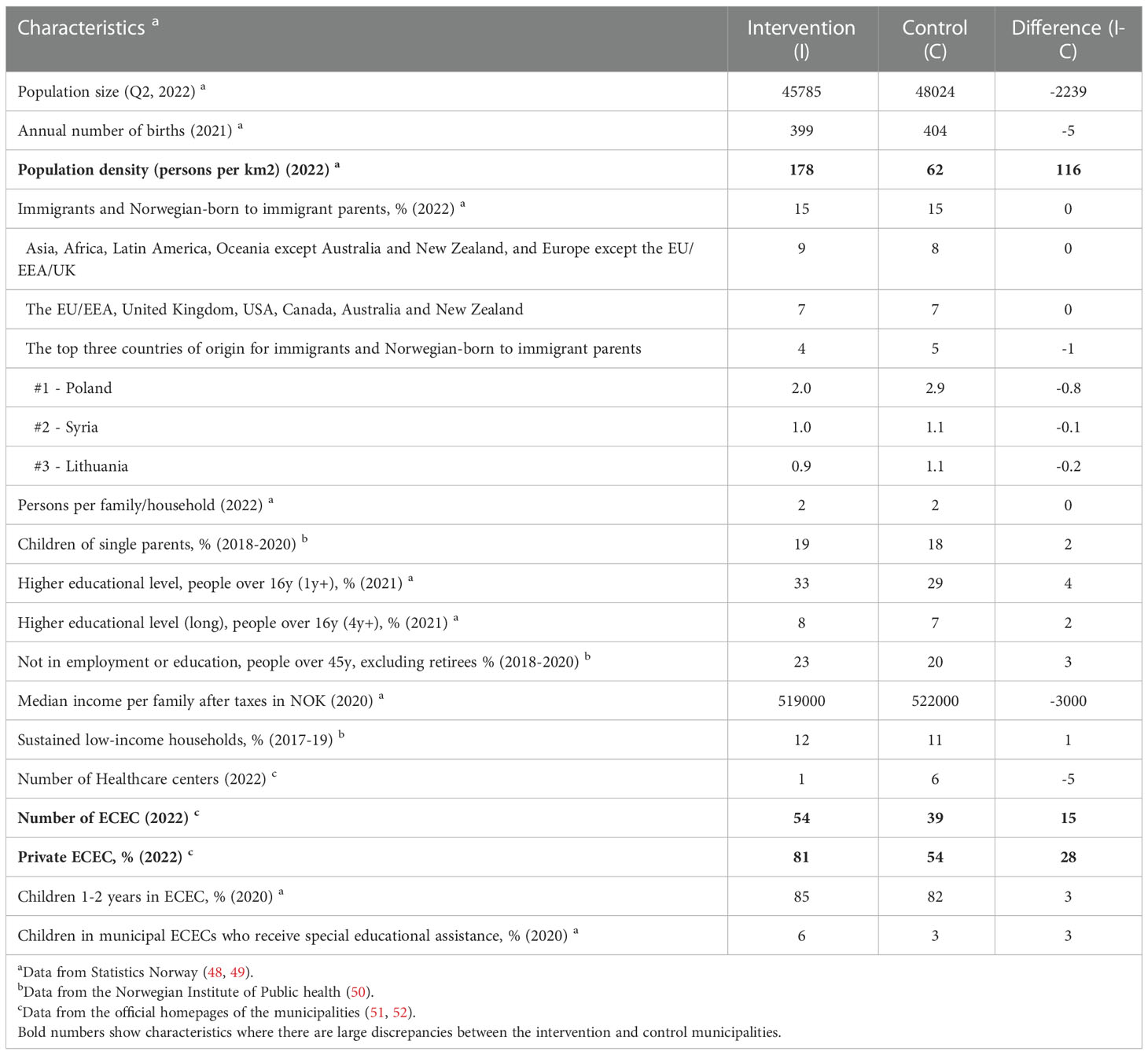
Table 2 Comparability of intervention and control municipalities in the Nutrition Now project (data from 2017-2022).
The participant groups in this project are listed in Figure 2. All pregnant women and parents of 0-2-year-olds living in the intervention or control municipality are eligible for this study. For the sake of simplicity, we will refer to guardians/care givers/parents as parents although all are included in this notion. Further, all MCH nurses and midwives and ECEC leaders working in the intervention or control municipality, staff in ECECs in which the leaders have consented to participate, plus all other relevant municipality staff within public health in the intervention municipality are eligible to participate.
Pregnant women and parents of children aged 0-2 years will be recruited at 1) routine visits to the MCH centre by MCH nurses and midwives, 2) the municipality website and 3) the relevant ECEC’s website, with all routes leading to a registration website where participants are able to give digital consent. We have previously successfully recruited through MCH centres in a similar way (53). Persons from ethnic minority groups will be recruited for participation in in-depth-interviews, representing pregnant women, parents of 0–2-year-olds and parents of 1-2-year-olds in ECEC, via Non-Governmental Organizations and other arenas in the municipality using snowball sampling. ECEC leaders will consent on behalf of their ECEC and will then recruit team leaders at each unit and their staff by forwarding digital invitations to participate in the study. Midwives and public health nurses at the participating MCH centres and municipality stakeholders (public health workers, leaders) will be recruited by digital invitations from the research group.
The sample size in this study is capped by the annual birth rate in the two municipalities (~400 per group, e.g., a total of approx. 800 births each year). The primary effectiveness outcome, aspects child diet quality, exemplified by vegetable intake was used to check that the study would be sufficiently powered. In a previous efficacy trial of 298 1–2-year-olds, we observed a difference in the change from baseline to 6-month follow-up of +0.46 vegetable items per day in favour of the intervention group (n=148). Assuming a participation rate in this study between 50 and 80%, we anticipate a sample size of 510-820 from each municipality, of whom 100-160 will have potentially been exposed to all parts of the Nutrition Now resource (in utero to 2-years of age). The worst-case scenario, with a 50% participation rate and 100 participants being exposed to all parts of the Nutrition Now resource, would enable us to detect a difference in vegetable of intake between groups of 0.5 items per day (alpha of 0.05 and 80% power). We anticipate that several hundred participants will be exposed to the intervention to some extend enabling other comparisons between the intervention and control municipality, with larger participant numbers.
The Nutrition Now resource comprises four efficacious e-learning interventions (details including theoretical underpinning provided in Additional File 1, Table S1) offered through a website targeting different transitions early in life, from pregnancy to child age 2. The content and structure of the original interventions has been modified and adapted to context and user needs (Figure 3) in the relevant settings for this study (family-, MCH centre- and ECEC- settings). The modification also includes offering the Nutrition Now resource in English and Arabic languages in addition to the Norwegian version, as requested from both MCH and ECEC staff (on behalf of parents). Results from other adjustments in the development of the Nutrition Now resource will be described and published in detail elsewhere.
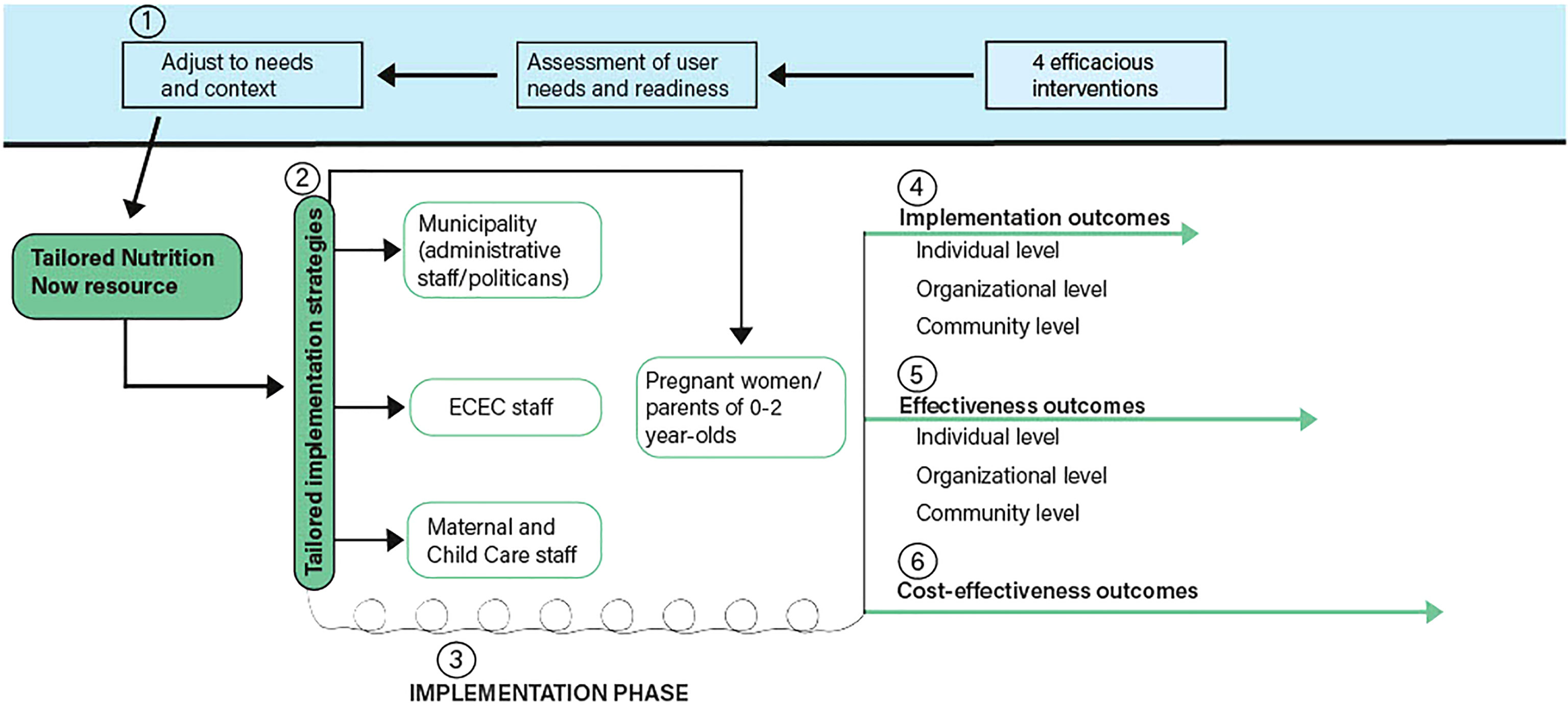
Figure 3 DIEM in the Nutrition Now project.
The Nutrition Now includes topics presented as core components addressing 1) the importance of diet early in life, 2) promotion of breastfeeding, 3), the importance of parental role in food provision and shaping child diet, 4) responsive feeding, 5) shared meals, 6) knowledge and experience of food preparation, 7) sensory play with vegetables, and 8) ECEC collaboration with parents (Additional File 2, Table S2). These topics are presented by videos, graphics, images and “easy to read” texts.
The process of implementing the Nutrition Now resource in the intervention municipality is guided by the Dynamic Integrated Evaluation Model (DIEM), the development of which was led by one of the co-authors (UvTS) (54). We will use the iterative implementation process as proposed in DIEM, in which the planned implementation strategies can be adapted continuously based on collected data during the implementation process. The iterative process builds on employing rapid improvement cycles in a participatory approach that ensures a continuous process of changes. From a practice perspective, self-reflection and continuous development are important, and short, iterative interviews with stakeholders (ECEC and MCH) will serve as support for this (54). Figure 3 shows elements from DIEM alongside the specific elements of the current study.
As shown in Figure 3, the tailored Nutrition Now resource is delivered through implementation strategies (2), already adjusted to needs and context (1) for use in the project’s iterative implementation phase. This enables further adjustments of the strategies as the project is rolled out and yields implementation outcomes continuously (3). Different implementation strategies target MCH staff, ECEC staff, the municipality level, and pregnant women and parents (Figure 3, Tables 3–5).
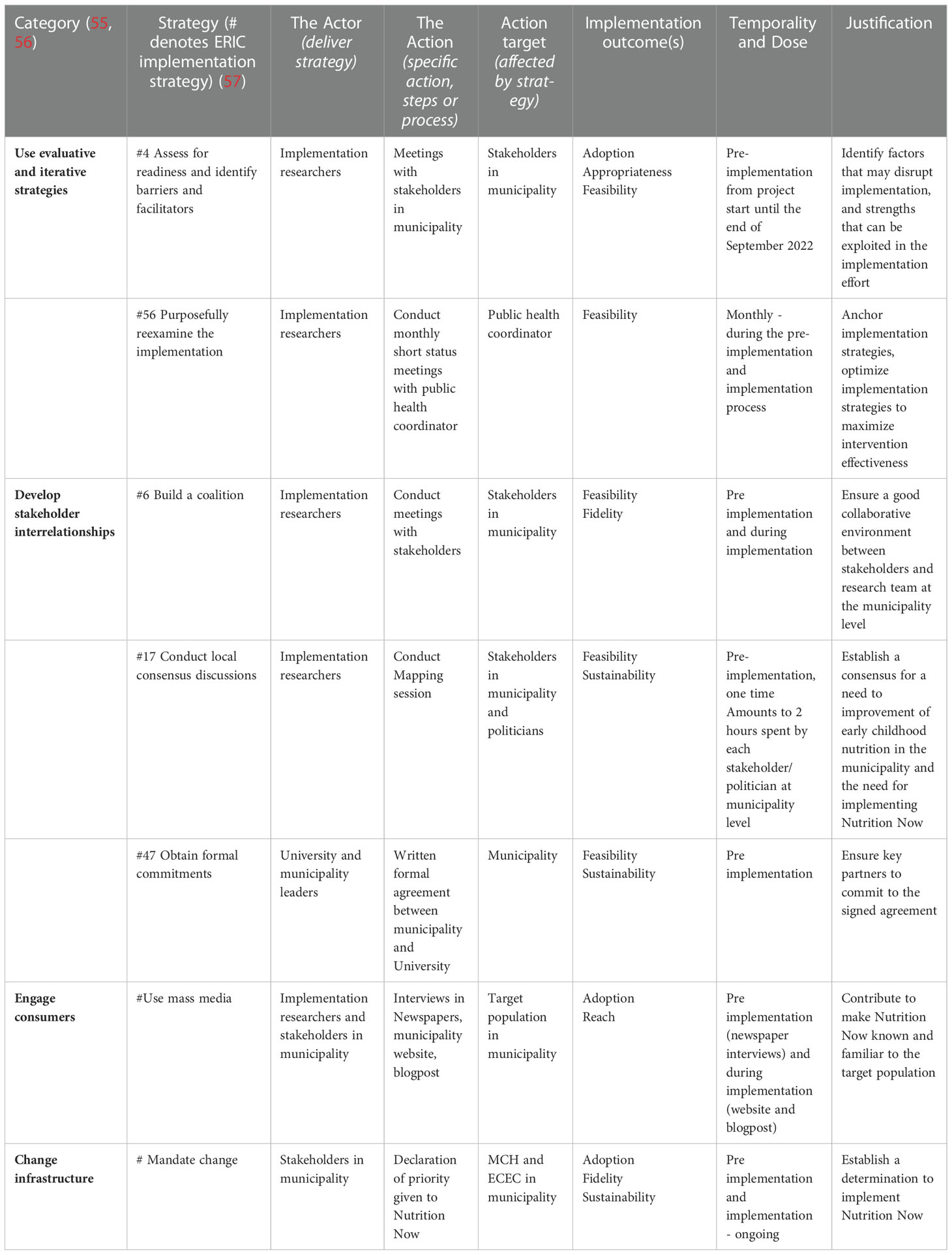
Table 3 Implementation strategies targeting Nutrition Now implementation delivered through Municipality (Organizational level).
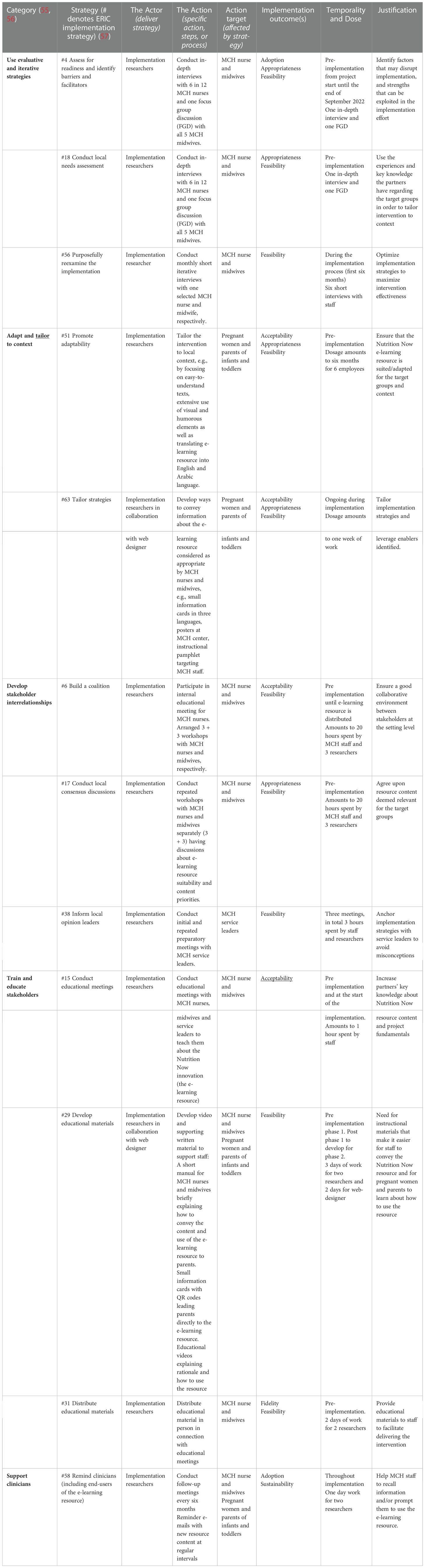
Table 4 Implementation strategies targeting Nutrition Now implementation delivered through Maternal and Child Health (MCH) care center.
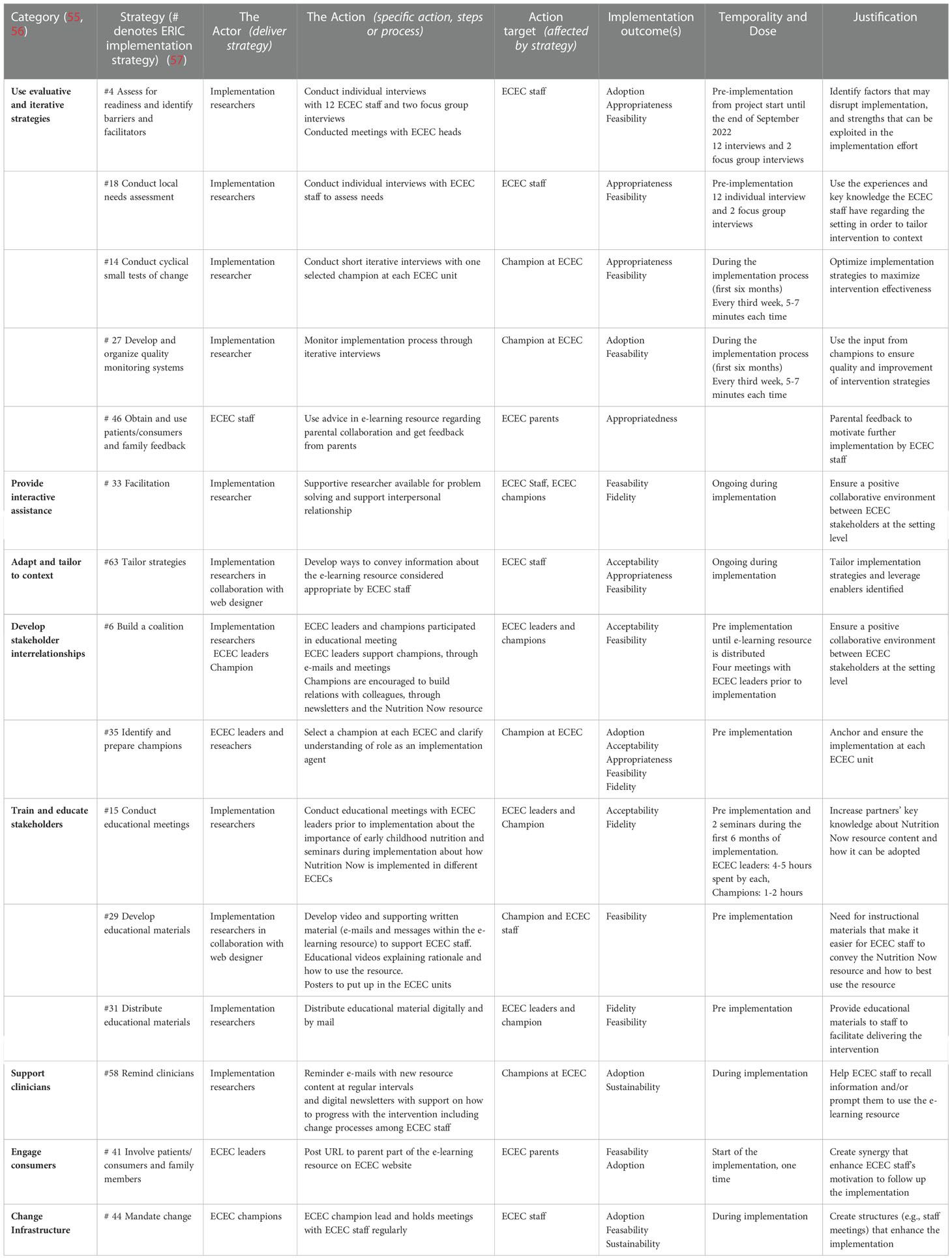
Table 5 Implementation strategies targeting Nutrition Now implementation delivered through Early Childhood Education and Care (ECEC).
Assessing barriers and facilitators to implementation was used in selecting the implementation strategies. A pragmatic approach was used building on previous experience and dialogue with MCH and ECEC staff, considering and balancing feasibility, impact, and cost. Moreover, all implementation strategies are in line with those deemed feasible and important by the ERIC-framework (Expert Recommendations for Implementing Change) (57) and adjusted to context (57) (Tables 3–5). The implementation strategies and their operationalization and justification are presented in Tables 3–5. The strategies are grouped according to the nine categories or clusters developed through a stakeholder participatory approach in the ERIC-study (55).
We will employ a set of seven implementation strategies to target the political and administrative leadership level in the municipality, including assessing barriers and facilitators to implementation, local consensus discussions and coalition building. Close collaboration with the municipal public health coordinator is considered essential for implementation. A co-creation process with stakeholders in the municipality including politicians resulted in a systems-map reflecting what they as a group consider the main determinants of child diet. A pre-existing formal agreement between the University and the intervention municipality facilitated access to the different settings (Table 3).
We have used three strategies targeting pregnant women and parents directly, all of which relate to tailoring and promoting adaptability of the Nutrition Now resource (Table 4). All texts and videos are provided in English and Arabic in addition to Norwegian to reach culturally diverse groups. Regular reminders with emails linking to age specific topic will be sent to the parents to promote use of the Nutrition Now resource.
We also employ a set of implementation strategies targeting MCH staff (Table 4) within the categories “use evaluative and iterative strategies”, “adapt and tailor to context”, “develop stakeholder interrelationships”, “train and educate stakeholder” and “support clinicians”.
We will utilize a set of implementation strategies targeting ECECs (Table 5). These include the categories “use evaluative and iterative strategies”, “provide interactive assistance”, “adapt and tailor to context”, “develop stakeholder interrelationships”, “train and educate stakeholder”, “support clinicians”, “engage consumers” and “change infrastructure”. Identifying team leaders at each ECEC unit is regarded as a crucial strategy as they are important implementation champions to oversee that implementation takes place. They will also participate in short iterative interviews to closely monitor the implementation process.
Quantitative and qualitative data will be collected in the different parts of this study (Figure 2 and Table 1).
Quantitative data for the effectiveness evaluation will be generated from questionnaires and objective measures. Questionnaire data will be obtained from i) pregnant women and parents of 0-2-years-olds, assessed during pregnancy, at child ages 6 weeks, 6 months, 12 months, 18 months, 24 months and ii) ECEC staff, assessed at baseline (pretest) and after 7 months (posttest).
Figure 4 provides an overview of the timeline for data collection for effectiveness outcomes for the parental part of the study, and duration of exposure to the Nutrition Now resource according to point of inclusion in the intervention municipality.
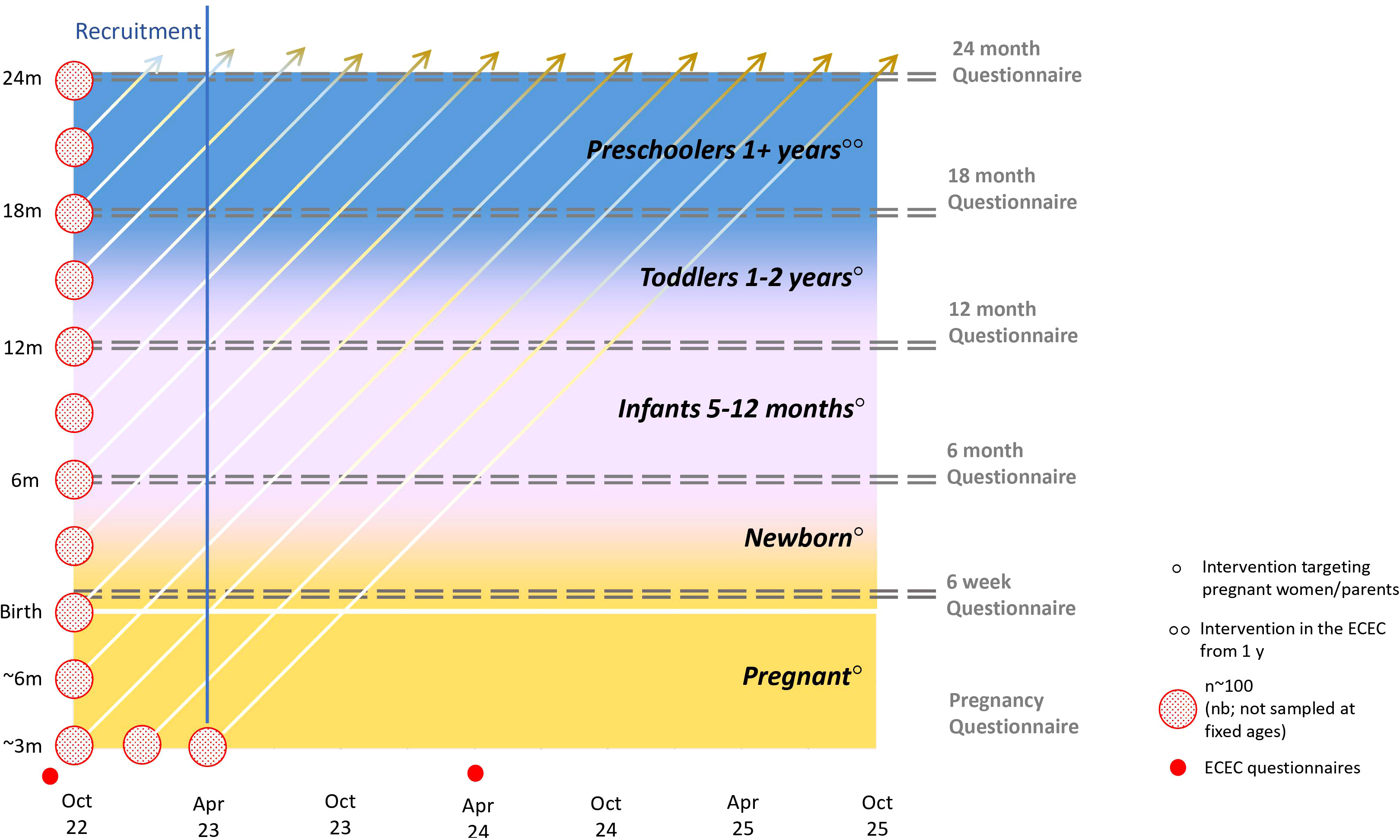
Figure 4 Overview of timeline for data collection, and exposure to the Nutrition Now resource (consisting of e-learning resources targeting different phases in a child’s 1000 first days) in the intervention municipality in the effectiveness trial. Pregnant women and parents of children between 0-2 years of age will be recruited from October 2022 until April 2023 through the MCH centre route. Participants will be exposed to age-appropriate content of the Nutrition Now resource and will be asked to respond to successive age-specific digital questionnaires depending on whether they are pregnant or the child’s age. Participants are given access to the Nutrition Now resource after completing the first questionnaire (pretest). ECEC staff will be recruited and complete the pretest questionnaire in September 2022, before getting access to the Nutrition Now-recourse. The post-test ECEC-staff questionnaire will be distributed seven months into the implementation of the intervention.
Consenting pregnant women (at any time during pregnancy), and parents of children between 0-2 years (at any time in this age interval) will first be asked to complete a short digital questionnaire to provide socio-demographic data in addition to expected due date (for pregnant women), or child’s age (for parents). Thereafter they will be asked to complete a second questionnaire tailored to the age of the child. Access to the Nutrition Now resource will be provided when the age-specific questionnaire is completed. The dose and duration of exposure to the Nutrition Now resource will differ between the participants depending on when they enter the study. Only those who are pregnant when entering the study between October 2022 and April 2023 will potentially be exposed to the whole range of intervention content, whereas a 1-year-old whose parent(s) enter the study in the same period, will be exposed to the “Toddlers 1-2 years” component and, if in ECEC, also the “Preschoolers 1+ years” component (Figure 4). Two-year-olds recruited at the regular health visit will be given access to the “Toddlers 1-2 years” component after completing the 24 months questionnaire.
ECEC leaders and staff will respond to questionnaires when consenting to participate in the study and seven months after getting access to the Nutrition Now resource.
Participants (both parents and ECEC staff) recruited in the control municipality will be asked to complete the same questionnaires as intervention participants but will not have access to the Nutrition Now resource.
Data on food purchase history in the ECECs will be collected from both the ECECs in the intervention and control municipality, for the years 2022 and 2023, to obtain data on fruits and vegetables purchases. Municipal budget data for 2022 and 2023 will be collected to gather info on municipal spend on activities related to early childhood nutrition and feeding practices in both the intervention and control municipality.
Quantitative and qualitative data will be collected to evaluate the implementation process and outcomes. Quantitative data from parents and ECEC staff at seven and 12 months after being enrolled in the study, will be collected using questionnaires with items from the seven implementation outcomes described in Table 1. Additional data will be collected using checklists during iterative interviews with ECEC and MCH during the first six months of the project, and usage data will be collected from the Nutrition Now resource. Evaluation of acceptability, appropriateness, and feasibility of the Nutrition Now resource will be done using a validated and generic questionnaire developed by Weiner et al. (41).
Qualitative data will be collected from short iterative interviews with team leaders in ECEC and contact persons for MCH nurses and midwifes, to promote self-reflection and continuous development. Further, focus group discussions with ECEC and MCH staff will be conducted approximately seven months after start of the implementation period to explore experiences with the implementation strategies. Individual interviews with ECEC leaders and stakeholders at municipality level will also be conducted (Table 1).
In depth description of what motivates and/or hinders use of the Nutrition Now resource will be explored in ethnic minority groups to render the next version of the resource more inclusive. With an anthropological way of interviewing, multi-stage, in-depth, open-ended and ethnographic interviews will be conducted with sub-samples of pregnant women and parents within ethnic minority groups in the intervention municipality to understand how the implementation of the resource works in and affects their everyday life.
Costs related to Nutrition Now resource development, maintenance and implementation will be collected throughout the implementation period using a bottom-up, micro-costing approach which will involve direct enumeration and costing of each intervention input (58).
Evaluating our effectiveness objective requires following a treatment policy estimand strategy (59, 60)- that is the effect of access to the Nutrition Now resource regardless of post-enrolment or intercurrent events such as non-compliance or discontinuation. This necessitates that outcome data be collected regardless of level of engagement and assumes that missing data are missing not at random (MNAR). Statistical models appropriate for de facto estimands will thus be used and the effect of MNAR on our effectiveness estimates will be assessed using sensitivity analyses. Confounding due to the non-randomised nature of the study, e.g., household size and income, parental education, ECEC status (public or private), will be assessed and adjusted for using regression models.
The main comparison will be between children and parents given access to all Nutrition Now components and those in the control municipality. Similar estimators of the Nutrition Now effectiveness will be available from comparisons within the intervention municipality since we will have data on approximately 100 parent-offspring pairs completely unexposed to the Nutrition Now resource as a result of the recruitment design (described above). The latter comparisons will improve causal inference by triangulating the evidence from two designs with different sources of bias (61). In this example they act as a sensitivity analysis to assess bias from residual confounding.
The recruitment strategy also creates variation in the number of components of the Nutrition Now resource each observational unit will be exposed to. Combined with the serial data collection points (pregnancy, 6 weeks, 6, 12, 18 and 24 months), we will be able to assess the effectiveness of each component of the resource in addition to duration of access.
Quantitative: We will report descriptive statistics for implementation outcomes assessed quantitatively [acceptability, appropriateness, feasibility, adoption and reach (Table 1)]. In addition, the number of people accessing the webpage, and sub-pages, and the time spent there, will be automatically registered in the Nutrition Now-resource. Qualitative interview data will be transcribed verbatim and coded deductively informed by the CFIR framework (62) and inductively to capture issues within and outside of this framework. We will use these findings to inform future scale-up at county level.
We will conduct economic evaluation in two ways. First, we will perform a within-trial economic analysis to evaluate the cost-effectiveness of the trial, i.e., trial-specific intervention costs relative to intervention effect on the outcomes selected for the economic evaluation. The within-trial analysis will be a cost–utility analysis (CUA), estimating the incremental cost per quality-adjusted life years (QALYs) gained from being given access to the Nutrition Now resource. QALYs will be generated via measurement of utility values based on the Pediatric Quality of Life Inventory (PedsQL) Infant Scales (13-24 months) (38), a pediatric generic health-related quality of life (HRQoL) instrument. Additionally, cost-effectiveness analysis (CEA) will be performed by calculating incremental cost per unit developmental improvement measured with the widely used developmental screening tool, Ages & Stages Questionnaire (ASQ), validated for use in the Norwegian population (39, 63) (Additional File 2, Table S2).
Second, a decision analytic model will be used to model the potential long-term cost-effectiveness of the Nutrition Now intervention over a lifetime horizon. We will develop a birth cohort simulation model based on estimated exposure-outcome associations in the Norwegian Mother, Father and Child Cohort (64) to explicitly model a set of causal pathways known to link child development to diverse later life outcomes. The model will provide a framework for integrating effectiveness measures from the current study in addition to data from external studies, drawn from targeted literature searches. The decision analytic modelling will adopt a wider societal perspective.
A data management plan (DMP) has been developed and will be published elsewhere. The DMP is an ongoing document throughout the project period and is in accordance with Norwegian Research Council’s (NRC) guidelines. We plan to share anonymized data in the UiA data repository Dataverse. This will be done no later than upon acceptance for publication of the main findings from the final dataset. We will retain our data for five years after data collection has stopped. Hence, our data will be made open access in line with the NRC’s guidelines, prior to three years after the completion of the study. Standard meta-information about the data will be uploaded.
Data from the pregnant women and parents of 0–2-year-olds will be collected using digital questionnaires created and distributed electronically using an encrypted version of the web-tool “Nettskjema” linked to a secure server, the Service for Sensitive Data (TSD, in Norwegian, “Tjeneste for Sensitive Data”). TSD is constructed for storing and processing data in agreement with the Norwegian Personal Data Act and Health Research Act (65). Digital questionnaires created in “Nettskjema” will also be used to collect data from leaders and other staff in the ECEC.
There are several potential challenges the project may face. Recruitment of participants and their continued participation is crucial for both the implementation and effectiveness part of this study. To reduce participant burden and maximise retention, we will keep the questionnaires short, easily comprehensible, and easy to complete. To avoid missing all data in the case of partly completed questionnaires, it will be possible to respond to only a few initial core questions, and still participate. Further, selection bias at recruitment between intervention and control sites may bias intervention estimates. In addition, although the original interventions have shown promising results in previous studies, the impact of the interventions might be more modest in a real-life setting. This dilution of intervention effect is a common finding in effectiveness studies and implementation trials (66), however the iterative approach to the implementation in our study is meant to reduce the chance of such dilution (54, 66).
A major strength of this study is the established efficacy in the original four interventions, the co-creation with the municipality, ECECs and MCH undertaken, and the established capacity and networks built by the research team. This experience will help address challenges along the way. The municipality setting and organization of ECEC and MCH are quite similar in all parts of Norway and thus, we expect that our findings related to the implementation will be generalizable to other Norwegian municipalities. Further, focusing on culturally diverse groups both in the effectiveness and implementation part, will render more culturally diverse and sensitive resources for future approaches.
Nutrition Now will break new ground by (i) systematically implementing and evaluating cumulative effects of successive dietary interventions in the first 1000 days of life in a real-life context, (ii) maximising interdisciplinary collaboration and integrating an anthropological approach with quantitative methods to truly adapt the intervention to context, (iii) bridging the previously described evidence-to-practice gap through rigorous scientific effectiveness evaluation of municipal implementation, (iv) harnessing the benefits of digital, video-based, technology to optimise access to dietary guidance in the municipalities, and (v) taking advantage of existing settings across sectors in municipal care to secure universal reach.
Lifecourse research has tended to be skewed towards epidemiology rather than implementation, and commonly target single transitional phases (67). Our project addresses these scientific shortcomings by implementing and evaluating evidence-based e-learning resources across multiple transitions early in life in a real-world community setting. Few developed interventions proven successful in controlled experimental settings are used to their full potential. Our study integrates four efficacious dietary interventions comprising e-learning resources and applies them in a municipal care setting. If this approach demonstrates public health benefit without increasing care providers’ workload it may provide a valuable contribution to other fields of lifecourse research.
Norway alone has the potential to save 14.8 billion EUR annually in health costs from improvements in population diet (68). According to Norwegian public health law, municipalities and counties are responsible for providing sound public health advice on diet and nutrition (69). MCH nurses and midwives are in a key position to guide parents on diet and nutritional issues, but often lack resources and time (70). ECEC staff are also strategically important as they are responsible for care of children while their parents work or study. Our digital diet interventions (70–72) offer a low-cost complementary tool for public health work in municipalities, and if successfully adapted when scaled-up, have the potential to improve population diet and health and respond to the need for tools and improved skills in childcare and ECECs. By gaining in-depth understanding of factors critical for successful local implementation, we will be ready to advance to county and national implementation, thereby contributing significantly to evidence-based health services in all municipalities in Norway.
We plan to share anonymised data in the UiA deposit Dataverse.
The studies involving human participants were reviewed and approved by Regional Ethics Committee (REC), South-East,cmVrc29yb3N0QG1lZGlzaW4udWlvLm5vLA== Reference number: 322480, and our Faculty Ethical Committee (FEC) and the Norwegian Data Protection Service (NSD) (id-number: FEC. NSD:847590). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
NØ, EH, FN, AM contributed to the conception of Nutrition Now project. NØ is the PI of the project, with AM, EH and FV as co-PIs. All authors contributed to the design of the study. SH, CH, EV, and EH contributed substantially to the development of the Nutrition Now resource, led by NØ. NO, HL, SH, CH, UV, PL, KC, CK, AM, EH, HR, and NØ contributed to the implementation trial, led by FV. NO, HL, CH, MA, EV, EH and NØ contributed to the effectiveness trial, led by AM. TE, MB and NØ contributed to the planning of socio-economic and ethnic diversity focus, led by MG and WV, respectively. AW contributed substantially to data management with EG, led by TB. Work on statistical approaches is led by AM and AW. AL contributed substantially to the cost-effectiveness part, led by EH. NØ developed the first draft of the manuscript, which was further developed by AM, FV, AW and EH. All authors contributed to the article and approved the submitted version.
The project is funded by the Norwegian Research Council, reference number: 320521.
We thank our collaborators in the intervention and control municipality for their important contribution related to the implementation and evaluation process in this study. Further we would like to thank our scientific assistants Julie Nordli and Camilla Bjornes for their work with the implementation strategies questionnaires and development of the digital resource. Thanks also to Bana Haidar for helping us oversee the Arabic versions of the questionnaires and the Nutrition Now resource. Thanks to Egde for developing the digital solution and to Semantix for translating the questionnaires and resource to English and Arabic. We are truly grateful for the great work done by Morten Torjussen and Thomas Andersen at the media department UiA, making the videos and animations. Further we would like to thank Henrik Jagels and Saara Ojanen, UiA, for digital and design help.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.1071489/full#supplementary-material
1. Sarma H, D'Este C, Ahmed T, Bossert TJ, Banwell C. Developing a conceptual framework for implementation science to evaluate a nutrition intervention scaled-up in a real-world setting. Public Health Nutr (2021) 24(S1):s7–s22. doi: 10.1017/S1368980019004415
2. Brownson RC, Colditz GA, Proctor EK. Dissemination and implementation research in health. New York: Oxford (2018).
3. MacDonald M, Pauly B, Wong G, Schick-Makaroff K, van Roode T, Strosher HW, et al. Supporting successful implementation of public health interventions: protocol for a realist synthesis. Syst Rev (2016) 5:54. doi: 10.1186/s13643-016-0229-1
4. Schwarzenberg SJ, Georgieff MK. Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics (2018) 141(2):e20173716. doi: 10.1542/peds.2017-3716
5. Hanson MA, Gluckman PD. Early developmental conditioning of later health and disease: physiology or pathophysiology? Physiol Rev (2014) 94(4):1027–76. doi: 10.1152/physrev.00029.2013
6. Hanson MA, Gluckman PD. Developmental origins of health and disease–global public health implications. Best Pract Res Clin Obstet Gynaecol (2015) 29(1):24–31. doi: 10.1016/j.bpobgyn.2014.06.007
7. Hanson MA, Bardsley A, De-Regil LM, Moore SE, Oken E, Poston L, et al. The international federation of gynecology and obstetrics (FIGO) recommendations on adolescent, preconception, and maternal nutrition: "Think nutrition first". Int J Gynaecol Obstet. (2015) 131 Suppl 4:S213–53. doi: 10.1016/S0020-7292(15)30034-5
8. Cetin I, Bühling K, Demir C, Kortam A, Prescott SL, Yamashiro Y, et al. Impact of micronutrient status during pregnancy on early nutrition programming. Ann Nutr Metab (2019) 74(4):269–78. doi: 10.1159/000499698
9. Birch LL, Doub AE. Learning to eat: birth to age 2 y. Am J Clin Nutr (2014) 99(3):723s–8s. doi: 10.3945/ajcn.113.069047
11. Campbell F, Conti G, Heckman JJ, Moon SH, Pinto R, Pungello E, et al. Early childhood investments substantially boost adult health. Science (2014) 343(6178):1478–85. doi: 10.1126/science.1248429
12. WHO Europe. The life-course approach: from theory to practice. Copenhagen: WHO Europe (2018). p. 107.
13. Darnton-Hill I, Nishida C, James WP. A life course approach to diet, nutrition and the prevention of chronic diseases. Public Health Nutr (2004) 7(1a):101–21. doi: 10.1079/PHN2003584
14. Ministry of Health. National action plan for improved diet (2017-2020). (Oslo: Norwegian Ministry of Health) (2017).
15. Norwegian Institute of Public Health. Mid-evaluation of the national action plan on improved diet (2017-2020). Oslo: Norwegian Institute of Public Health (2020).
16. Myhre J, Andersen LF, Kristiansen AL. SPEDKOST 3 national dietary survey among infants in Norway, 6 months. Oslo: Norwegian Institute of Public Health (2020).
17. Norwegian Institute of Public Health. National dietary survey among infants in Norway, 12 months. Oslo: Norwegian Institute of Public Health (2020).
18. Koletzko B, Bührer C, Ensenauer R, Jochum F, Kalhoff H, Lawrenz B, et al. Complementary foods in baby food pouches: position statement from the nutrition commission of the German society for pediatrics and adolescent medicine (DGKJ, e.V.). Mol Cell Pediatr (2019) 6(1):2. doi: 10.1186/s40348-019-0089-6
19. The Norwegian Consumer Council. Content and labelling of fruit purees for infants and toddlers (In Norwegian). Oslo: The Norwegian Consumer Council (2020).
20. The Norwegian Directorate of Health. Meals, physical activity and health care in kindergarten- a survey among kindergarten staff. Oslo: The Norwegian Directorate of Health (2012).
21. Bjørset VK, Helle C, Hillesund ER, Øverby NC. Socio-economic status and maternal BMI are associated with duration of breast-feeding of Norwegian infants. Public Health Nutr (2018) 21(8):1465–73. doi: 10.1017/S1368980017003925
22. Mekonnen T, Havdal HH, Lien N, O'Halloran SA, Arah OA, Papadopoulou E, et al. Mediators of socioeconomic inequalities in dietary behaviours among youth: A systematic review. Obes Rev (2020) 21(7):e13016. doi: 10.1111/obr.13016
23. Sayakhot P, Carolan-Olah M. Internet Use by pregnant women seeking pregnancy-related information: a systematic review. BMC Pregnancy Childbirth (2016) 16:65. doi: 10.1186/s12884-016-0856-5
24. Slomian J, Bruyère O, Reginster JY, Emonts P. The internet as a source of information used by women after childbirth to meet their need for information: A web-based survey. Midwifery (2017) 48:46–52. doi: 10.1016/j.midw.2017.03.005
25. Laws R, Love P, Hesketh KD, Koorts H, Denney-Wilson E, Moodie M, et al. Protocol for an effectiveness-implementation hybrid trial to evaluate scale up of an evidence-based intervention addressing lifestyle behaviours from the start of life: INFANT. Front Endocrinol (Lausanne) (2021) 12:717468. doi: 10.3389/fendo.2021.717468
26. Statistics Norway. Kindergartens (2022). Available at: https://www.ssb.no/utdanning/barnehager/statistikk/barnehager.
27. Love P, Walsh M, Campbell KJ. Knowledge, attitudes and practices of Australian trainee childcare educators regarding their role in the feeding behaviours of young children. Int J Environ Res Public Health (2020) 17(10):1–117. doi: 10.3390/ijerph17103712
28. Hillesund ER, Bere E, Sagedal LR, Vistad I, Øverby NC. Effect of a diet intervention during pregnancy on dietary behavior in the randomized controlled Norwegian fit for delivery study. J Dev Orig Health Dis (2016) 7(5):538–47. doi: 10.1017/S2040174416000258
29. Helle C, Hillesund ER, Wills AK, Øverby NC. Evaluation of an eHealth intervention aiming to promote healthy food habits from infancy -the Norwegian randomized controlled trial early food for future health. Int J Behav Nutr Phys Act. (2019) 16(1):1. doi: 10.1186/s12966-018-0763-4
30. Blomkvist EAM, Wills AK, Helland SH, Hillesund ER, Øverby NC. Effectiveness of a kindergarten-based intervention to increase vegetable intake and reduce food neophobia amongst 1-year-old children: a cluster randomised controlled trial. Food Nutr Res (2021) 65:1–35. doi: 10.29219/fnr.v65.7679
31. Helland SH, Øverby NC, Myrvoll Blomkvist EA, Hillesund ER, Strömmer S, Barker M, et al. Wow! they really like celeriac! kindergarten teachers' experiences of an intervention to increase 1-year-olds' acceptance of vegetables. Appetite (2021) 166:105581. doi: 10.1016/j.appet.2021.105581
32. Røed M, Medin AC, Vik FN, Hillesund ER, Van Lippevelde W, Campbell K, et al. Effect of a parent-focused eHealth intervention on children's fruit, vegetable, and discretionary food intake (Food4toddlers): Randomized controlled trial. J Med Internet Res (2021) 23(2):e18311. doi: 10.2196/18311.
33. Bandura A. Social cognitive theory: An agentic perspective. Annu Rev Psychol (2001) 52(1):1–26. doi: 10.1146/annurev.psych.52.1.1
34. Gottfredson DC, Cook TD, Gardner FE, Gorman-Smith D, Howe GW, Sandler IN, et al. Standards of evidence for efficacy, effectiveness, and scale-up research in prevention science: Next generation. Prev Sci (2015) 16(7):893–926. doi: 10.1007/s11121-015-0555-x
35. Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care (2012) 50(3):217–26. doi: 10.1097/MLR.0b013e3182408812
36. Landes SJ, McBain SA, Curran GM. An introduction to effectiveness-implementation hybrid designs. Psychiatry Res (2019) 280:112513. doi: 10.1016/j.psychres.2019.112513
37. Ito N, Ainuki T, Akamatsu R. Development of "The child eating-enjoyment scale". J Educ Dev Psychol (2015) 5(1):19. doi: 10.5539/jedp.v5n1p19
38. Varni JW, Limbers CA, Neighbors K, Schulz K, Lieu JE, Heffer RW, et al. The PedsQL™ infant scales: feasibility, internal consistency reliability, and validity in healthy and ill infants. Qual Life Res (2011) 20(1):45–55. doi: 10.1007/s11136-010-9730-5
39. Squires J, Bricker D, Potter L. Revision of a parent-completed development screening tool: Ages and stages questionnaires. J Pediatr Psychol (1997) 22(3):313–28. doi: 10.1093/jpepsy/22.3.313
40. Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess (1985) 49(1):71–5. doi: 10.1207/s15327752jpa4901_13
41. Weiner BJ, Lewis CC, Stanick C, Powell BJ, Dorsey CN, Clary AS, et al. Psychometric assessment of three newly developed implementation outcome measures. Implement Sci (2017) 12(1):108. doi: 10.1186/s13012-017-0635-3
42. RE-AIM. Assessing implementation (2022). Available at: https://re-aim.org/assessing-implementation/.
44. Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, et al. RE-AIM planning and evaluation framework: Adapting to new science and practice with a 20-year review. Front Public Health (2019) 7. doi: 10.3389/fpubh.2019.00064
45. Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health (1999) 89(9):1322–7. doi: 10.2105/AJPH.89.9.1322
46. Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health (2011) 38(2):65–76. doi: 10.1007/s10488-010-0319-7
47. Zwarenstein M, Treweek S, Gagnier JJ, Altman DG, Tunis S, Haynes B, et al. Improving the reporting of pragmatic trials: an extension of the CONSORT statement. Bmj (2008) 337:a2390. doi: 10.1136/bmj.a2390
48. Norway S. Municipality data (In Norwegian: Kommunefakta) (2022). Available at: https://www.ssb.no/kommunefakta/.
49. Norway S. StatBank Norway from statistics Norway (2022). Available at: https://www.ssb.no/en/statbank.
50. Norwegian Institute of Public Health. Public health profiles for municipalities and counties from NIPH (2022). Available at: https://www.fhi.no/en/hn/health-in-the-municipalities/hent-folkehelseprofil-for-kommune-fylke-eller-bydel/ (Accessed December 22 2022)
51. Municipality a. arendal municipality (2022). Available at: https://www.arendal.kommune.no/english/.
52. Municipality l. larvik municipality (2022). Available at: https://www.larvik.kommune.no/.
53. Sagedal LR, Øverby NC, Lohne-Seiler H, Bere E, Torstveit MK, Henriksen T, et al. Study protocol: fit for delivery - can a lifestyle intervention in pregnancy result in measurable health benefits for mothers and newborns? a randomized controlled trial. BMC Public Health (2013) 13:132. doi: 10.1186/1471-2458-13-132
54. von Thiele Schwarz U, Lundmark R, Hasson H. The dynamic integrated evaluation model (DIEM): Achieving sustainability in organizational intervention through a participatory evaluation approach. Stress Health (2016) 32(4):285–93. doi: 10.1002/smi.2701
55. Waltz TJ, Powell BJ, Matthieu MM, Damschroder LJ, Chinman MJ, Smith JL, et al. Use of concept mapping to characterize relationships among implementation strategies and assess their feasibility and importance: results from the expert recommendations for implementing change (ERIC) study. Implement Sci (2015) 10:109. doi: 10.1186/s13012-015-0295-0
56. Proctor EK, Powell BJ, McMillen JC. Implementation strategies: recommendations for specifying and reporting. Implement Sci (2013) 8:139. doi: 10.1186/1748-5908-8-139
57. Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, et al. A refined compilation of implementation strategies: results from the expert recommendations for implementing change (ERIC) project. Implement Sci (2015) 10(1):21. doi: 10.1186/s13012-015-0209-1
58. Gray AM, Clarke PM, Wolstenholme JL, Wordsworth S. Applied methods of cost-effectiveness analysis in health care. New York, NY: OUP Oxford (2011).
59. Ritz C, Rønn B. Estimands: improving inference in randomized controlled trials in clinical nutrition in the presence of missing values. Eur J Clin Nutr (2018) 72(9):1291–5. doi: 10.1038/s41430-018-0207-x
60. Kahan BC, Morris TP, White IR, Carpenter J, Cro S. Estimands in published protocols of randomised trials: urgent improvement needed. Trials (2021) 22(1):686. doi: 10.1186/s13063-021-05644-4
61. Lawlor DA, Tilling K, Davey Smith G. Triangulation in aetiological epidemiology. Int J Epidemiol (2016) 45(6):1866–86. doi: 10.1093/ije/dyw314
62. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci (2009) 4:50. doi: 10.1186/1748-5908-4-50
63. Richter J, Janson H. A validation study of the Norwegian version of the ages and stages questionnaires. Acta Paediatr (2007) 96(5):748–52. doi: 10.1111/j.1651-2227.2007.00246.x
64. Magnus P, Birke C, Vejrup K, Haugan A, Alsaker E, Daltveit AK, et al. Cohort profile update: The Norwegian mother and child cohort study (MoBa). Int J Epidemiol (2016) 45(2):382–8. doi: 10.1093/ije/dyw029
65. University of Oslo. Create a nettskjema for collecting sensitive data to TSD (2022). Available at: https://www.uio.no/english/services/it/research/sensitive-data/help/create-nettskjema.html.
66. Chambers DA, Glasgow RE, Stange KC. The dynamic sustainability framework: addressing the paradox of sustainment amid ongoing change. Implement Sci (2013) 8:117. doi: 10.1186/1748-5908-8-117
67. Jacob CM, Cooper C, Baird J, Hanson M. WHO health evidence network synthesis reports. what quantitative and qualitative methods have been developed to measure the implementation of a life-course approach in public health policies at the national level? (Copenhagen: WHO Regional Office for Europe © World Health Organization) (2019) 2019.
68. The Norwegian Directorate of Health. Societal returns following Norwegian dietary guidelines. Oslo: The Norwegian Directorate of Health (2015).
69. Lovdata. lov om folkehelsearbeid (folkehelseloven) (2011). Available at: https://lovdata.no/dokument/NL/lov/2011-06-24-29.
70. Røed M, Hillesund ER, Vik FN, Van Lippevelde W, Øverby NC. The Food4toddlers study - study protocol for a web-based intervention to promote healthy diets for toddlers: a randomized controlled trial. BMC Public Health (2019) 19(1):563. doi: 10.1186/s12889-019-6915-x
71. Helle C, Hillesund ER, Omholt ML, Øverby NC. Early food for future health: a randomized controlled trial evaluating the effect of an eHealth intervention aiming to promote healthy food habits from early childhood. BMC Public Health (2017) 17(1):729. doi: 10.1186/s12889-017-4731-8
Keywords: digital diet intervention, early life obesity prevention, maternal and child health care, implementation, feeding practices, municipality scale up, the Nutrition Now project protocol
Citation: Øverby NC, Hillesund ER, Helland SH, Helle C, Wills AK, Lamu AN, Osorio NG, Lian H, Ersfjord TI, Van Daele W, Bjørkkjær T, Valen EN, Gebremariam MK, Grasaas E, Kiland C, Schwarz UvT, Abel MH, Love P, Campbell K, Rutter H, Barker ME, Vik FN and Medin AC (2023) Evaluating the effectiveness and implementation of evidence-based early-life nutrition interventions in a community setting a hybrid type 1 non-randomized trial – the Nutrition Now project protocol. Front. Endocrinol. 13:1071489. doi: 10.3389/fendo.2022.1071489
Received: 16 October 2022; Accepted: 15 December 2022;
Published: 10 January 2023.
Edited by:
Giovanna Muscogiuri, University of Naples Federico II, ItalyReviewed by:
Helen McDevitt, Royal Hospital for Children, United KingdomCopyright © 2023 Øverby, Hillesund, Helland, Helle, Wills, Lamu, Osorio, Lian, Ersfjord, Van Daele, Bjørkkjær, Valen, Gebremariam, Grasaas, Kiland, Schwarz, Abel, Love, Campbell, Rutter, Barker, Vik and Medin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nina Cecilie Øverby, bmluYS5jLm92ZXJieUB1aWEubm8=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.