
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 18 January 2023
Sec. Reproduction
Volume 13 - 2022 | https://doi.org/10.3389/fendo.2022.1034614
This article is part of the Research TopicEndometriosis: Pathogenesis, Diagnosis and Treatment, volume IIView all 10 articles
 Jean-Philippe Emond1†Patrick Caron1†
Jean-Philippe Emond1†Patrick Caron1† Maja Pušić2Véronique Turcotte1
Maja Pušić2Véronique Turcotte1 David Simonyan3Andrej Vogler4
David Simonyan3Andrej Vogler4 Joško Osredkar5
Joško Osredkar5 Tea Lanišnik Rižner2*‡
Tea Lanišnik Rižner2*‡ Chantal Guillemette1,6*‡
Chantal Guillemette1,6*‡Objectives: Endometriosis (EM) is an estrogen-dominant inflammatory disease linked to infertility that affects women of reproductive age. EM lesions respond to hormonal signals that regulate uterine tissue growth and trigger inflammation and pain. The objective of this study was to evaluate whether estradiol (E2) and its biologically active metabolites are differentially associated with EM given their estrogenic and non-estrogenic actions including proliferative and inflammatory properties.
Design: We performed a retrospective study of 209 EM cases and 115 women without EM.
Methods: Pain-related outcomes were assessed using surveys with validated scales. Preoperative serum levels of estradiol (E2) and estrone (E1), their 2-, 4- and 16- hydroxylated (OH) and methylated (MeO) derivatives (n=16) were measured by mass spectrometry. We evaluated the associations between estrogen levels and EM anatomic sites, surgical stage, risk of EM, and symptoms reported by women. Spearman correlations established the relationships between circulating steroids.
Results: Of the sixteen estrogens profiled, eleven were detected above quantification limits in most individuals. Steroids were positively correlated, except 2-hydroxy 3MeO-E1 (2OH-3MeO-E1). Higher 2OH-3MeO-E1 was linked to an increased risk of EM (Odd ratio (OR)=1.91 (95%CI 1.09-3.34); P=0.025). Ovarian EM cases displayed enhanced 2-hydroxylation with higher 2MeO-E1 and 2OH-E1 levels (P< 0.009). Abdominal, pelvic and back pain symptoms were also linked to higher 2OH-3MeO-E1 levels (OR=1.86; 95%CI 1.06-3.27; P=0.032).
Conclusions: The 2-hydroxylation pathway emerges as an unfavorable feature of EM, and is associated with ovarian EM and pain related outcomes.
Endometriosis (EM) affects approximately 10% of women of reproductive age (1) and is defined by the presence of endometrial glands or stoma outside the uterine cavity. It is a non-malignant disease nonetheless associated with dysmenorrhea, dyspareunia, pelvic pain and infertility due to the presence of ectopic tissue and inflammation (2–4). Endometriotic lesions can be superficial peritoneal, ovarian or deeply infiltrating (5, 6). The etiology of endometriosis is complex (7) and multifactorial thus several theories have been proposed to explain the clinical manifestation of endometriosis; Sampson’s theory of retrograde menstruation, coelomic metaplasia theory, Mullerian rests theory, stem cell theory, impaired immune system theory, and others (8). Endometriosis is considered a chronic inflammatory disease with altered peritoneal environment in patients with endometriosis. The ectopic lesions recruit immune cells which leads to production of pro-inflammatory molecules and cytokines and also promote angiogenesis and innervation and thus contribute to survival of these lesions (9).
EM is an estrogen-dependent disease with molecular hallmarks of genetic predisposition, altered hormonal milieu (estrogen dependence and progesterone resistance) and inflammation (10, 11). Changes in steroid biotransformation pathways have been reported leading to an increased local production of estrogens in endometriosis lesions (12). EM lesions respond to hormonal signals such as estradiol (E2) that regulate uterine tissue growth and triggers inflammation, and that are linked to pain symptoms (13). Excessive inflammation also leads to changes in sex steroid receptors (ERα and ERβ) expression and enhanced estrogen biosynthesis in endometriotic lesions, involving aromatase, sulfatase and other pathways (14–21). Treatment of pelvic pain in EM thus includes the use of nonsteroidal anti-inflammatory drugs, oral contraceptives and progestins.
Estrogens comprise a vast array of hydroxylated (OH) and methoxylated (MeO) catechol estrogen (CE) metabolites with diverse biological activities. The synthesis of CE metabolites from E2 and estrone (E1) involves various metabolic routes, namely the 2-hydroxylation (2OH), 4-hydroxylation (4OH) and 16-hydroxylation (16OH) pathways and the action of the catechol-O-methyltransferase (COMT) to form 2- and 4- MeOCEs (22, 23). Besides acting as ligands of ERα and ERβ, CEs also present non-estrogenic properties (22, 24). MeOCEs have antiangiogenic and antiproliferative actions whereas 4-OHCEs have procarcinogenic properties (22, 25–27). Both the 2OH and 4OH CE derivatives generally have reduced estrogenic effects (24, 28) as opposed to the 16OH pathway that retains most of its estrogenic properties, with a preferential action on the ERβ (24). In addition, E2 was previously found to be associated with pain due to its effects on nerves and inflammation (13). Some CEs present estrogenic activities resembling E2 and they may be prone to cause pain.
Given the suspected biological roles of catechol estrogens, and their associations with several hormone-sensitive diseases including endometrial cancer (29, 30), we hypothesized that circulating levels of E2 and/or its biologically active metabolites were associated with an altered risk of EM (primary objective) and severity of pain symptoms (secondary objective).
The study design corresponded to a retrospective case-control study comprising cases and controls from the same type of population (31). Part of this cohort was described previously (32–34). Patients’ enrolment took place from March 2008 to June 2018 at the Departments of Obstetrics and Gynecology at the University Medical Centre Ljubljana, Slovenia. The study comprised patients who visited gynecologist with problems/symptoms that are indicative for laparoscopy surgery. The inclusion criteria were an indication for a diagnostic laparoscopy for symptoms suggestive of EM such as pain, infertility, ovarian cysts, other gynecological pathologies such as myomas and tubal sterilization. The exclusion criteria were pregnancy, age below 18 years, menopausal status, gynecological malignancies, cancelled surgery, previous hysterectomy, drug abuse and HIV infection (32). Of the 341 women, 17 participants were excluded to manage confounders: six because of missing data on mandatory age and/or BMI, three due to unknown case or control status, four with polycystic ovary syndrome (PCOS) that could impact hormone levels, one due to a prior unidentified menopausal state, and three with significant anomalies of the menstrual cycle of unknown etiology. The remaining cohort of 324 women underwent either diagnostic laparoscopy or laparoscopic tubal sterilization and were divided according to presence (n=209, cases) or absence (n=115, controls) of EM. Controls were further divided into two groups (patients with benign pathologies (n=79) and healthy controls (n=35). Patients with benign pathologies had symptoms suggestive for EM (infertility and/or pain) or other gynecological pathologies. Healthy patients underwent laparoscopic tubal sterilization and had no symptoms suggestive for EM (Figure 1). A post-hoc ANOVA power analysis test (power package and R Statistical Software v4.1.2; R Core Team 2021) estimated that a sample size per group of 36 was suffcient). The clinical characteristics presented in Table 1 included age, body mass index (BMI), type of EM (ovarian, ovarian and peritoneal, peritoneal, and deep infiltrating), rASRM stage of disease (35), smoking status (current, former or never), use of hormonal therapy (last three months), use of oral contraception (last three months), and endometrial phase (secretory or proliferative). Patient-filled surveys using validated numeric rating scales documented the outcomes of “abdominal, pelvic and back pain”, “dysmenorrhea (frequency)”, “dysmenorrhea (intensity)”, “score of dysmenorrhea”, “dyspareunia (frequency)”, “dyspareunia (intensity)” and “dysuria or dyschezia (frequency)” (36, 37). For EM cases, data for pain-related outcomes were available for 98.6% to 99.5% of participants, except for the “score of dysmenorrhea’’ (61.2%), “dysmenorrhea (intensity)” (35.4%), and “dyspareunia (intensity)” (59.3%) outcomes. In control cases, data was available for 86.7% to 97.4% of participants, except for “score of dysmenorrhea’’ (56.5%) and “dyspareunia (intensity)” (55.7%) outcomes. The patient’s characteristics related to pain symptoms are presented in Supplementary Table 1. Pain related outcomes were dichotomized for the statistical analysis. The dichotomization for “abdominal, pelvic and back pain” was “yes or no”. For “dysmenorrhea (frequency)”, “dyspareunia (frequency)” and “dysuria or dyschezia (frequency)”, the dichotomization was “infrequent (never, almost never or sometimes) or frequent (quite often or very often)”. For “dyspareunia (intensity)” and “dysmenorrhea (intensity)”, the dichotomization was “mild (no or slight pain) or moderate to severe (medium or strong pain)”. For the “score of dysmenorrhea”, the dichotomization was “scores of ≤5 or of >5”. All participants provided an informed consent prior to their enrolment. This study was conducted in accordance with the declaration of Helsinki. This study was approved by the National Medical Ethics Committee in Slovenia (#0120-127/2016/6) and the ethics committee of the CHUQc – Université Laval (#2012-993).
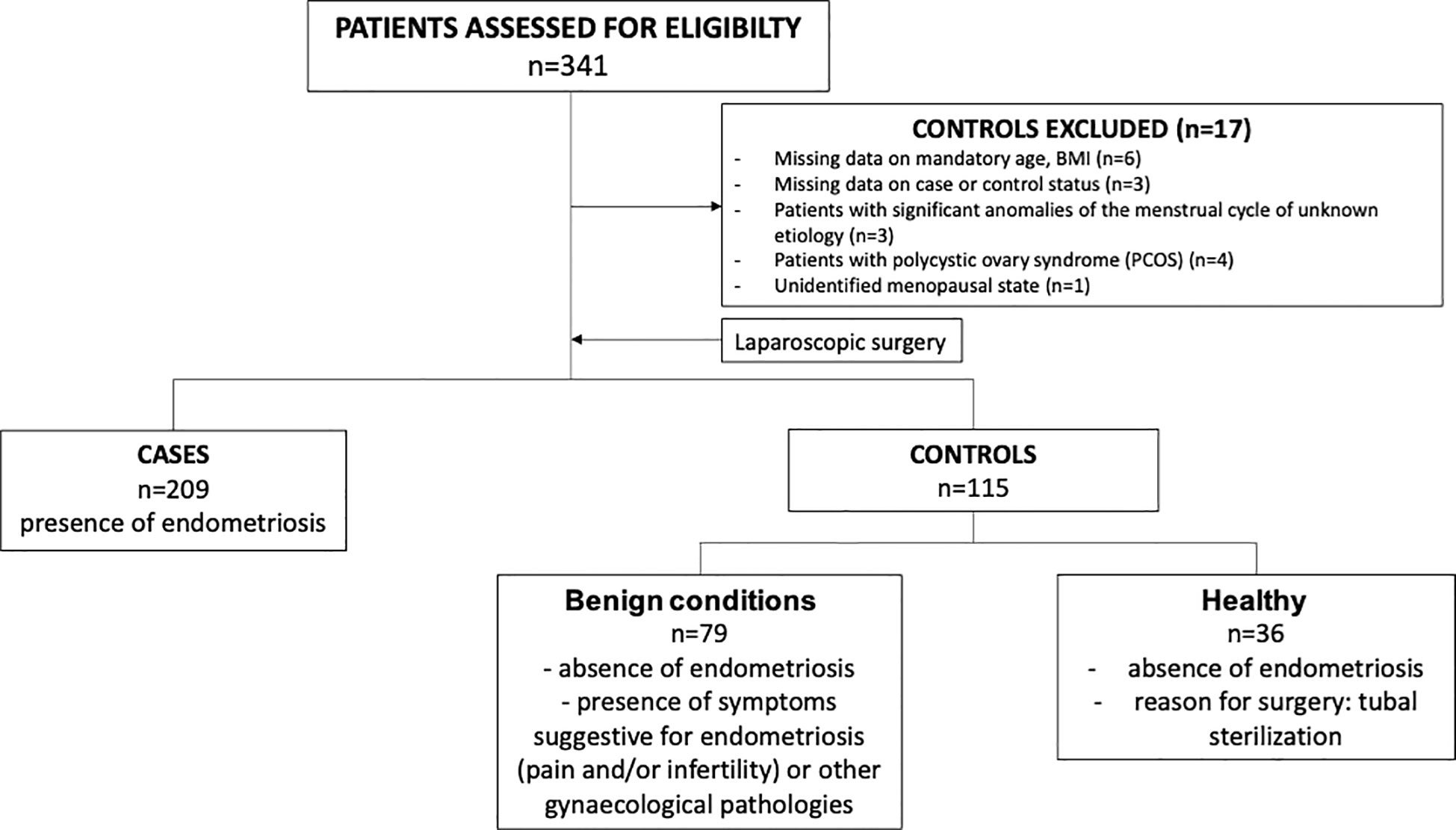
Figure 1 Flowchart of patient cohort.
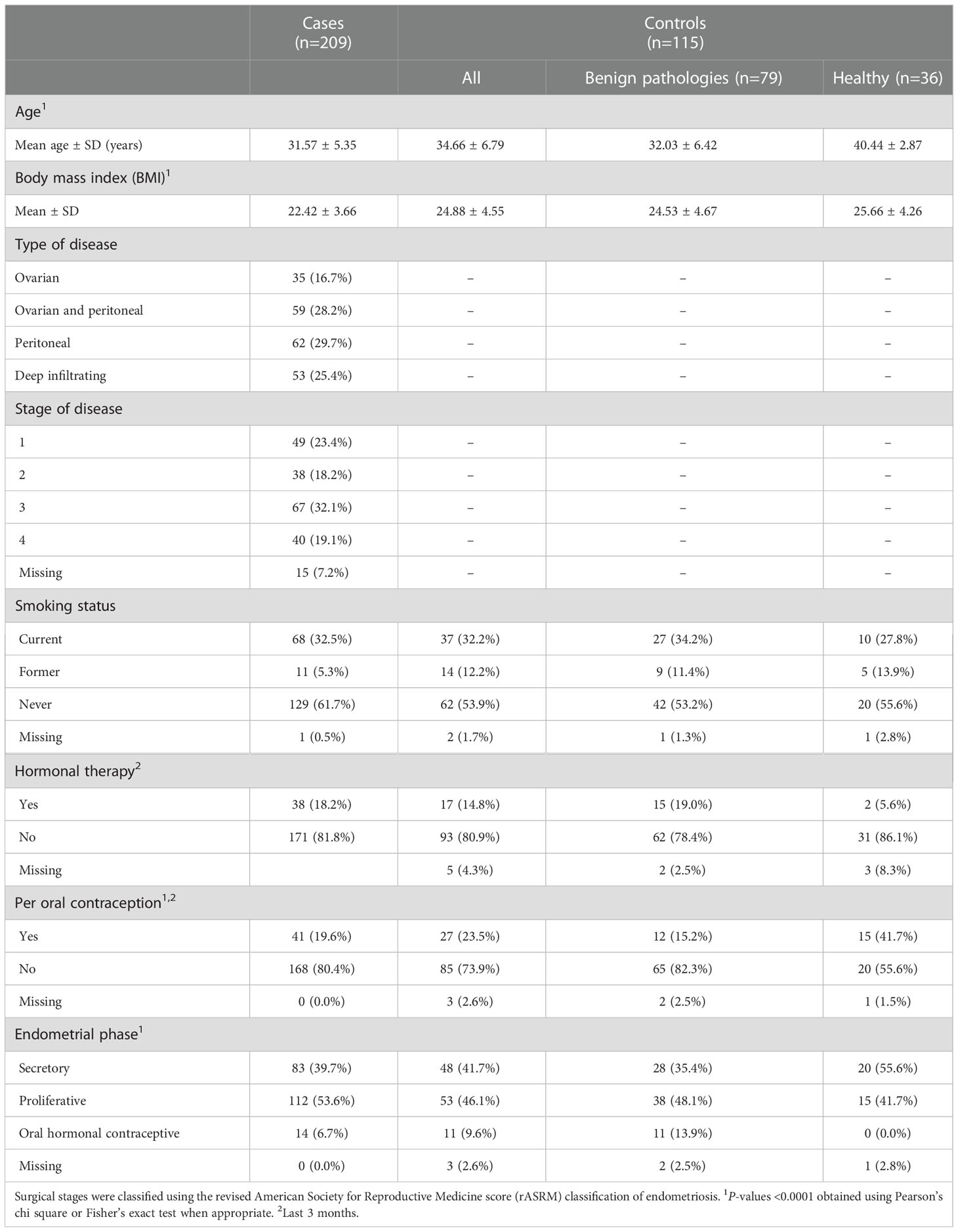
Table 1 Characteristics and clinical data of endometriosis cases (n=209) and controls (n=115).
Blood samples were collected two days prior to surgery as described (32), and following strict standard operating procedures for collection, processing and storage at -80˚C to preserve stability of metabolites such as steroids. Briefly, 4 ml of blood sample was collected by venipuncture from the median cubital vein using BD Vacutainer tubes (#369032; Becton Dickinson and Company, NJ, USA). The collected samples were incubated for no more than 1 h at room temperature and then centrifuged at 1400 × g for 10 min at room temperature. The seperated serum was collected, aliquoted, and stored at -80°C until analysis. Only samples that were frozen/thawed once were used for analysis. A specific set of 16 estrogen derivatives were quantified in 250 μL of serum using a liquid-chromatography tandem mass spectrometry assay (LC-MS/MS) as described (29). The lower limit of quantification (LLOQ) was 5 pg/mL. Sums including all analytes and metabolic ratios were calculated for the different metabolic pathways. Catechol estrogens at levels below LLOQ (even if detected above the limit of detection) were considered undetected.
Differences in estrogen hormone levels between cases and controls, anatomic sites and surgical stages were determined by bivariate analyses on means of log transformed continuous hormone levels. The relationship between hormone levels was assessed using Spearman’s rank-order correlation. Odd ratios (OR) were obtained using dichotomized hormone levels (independent variables) based on the median levels of controls as performed in previous studies (29) in a multivariate logistic regression model, adjusted for age, BMI, smoking status, oral contraception (last three months), hormonal therapy (last three months) and the endometrial phase (secretory or proliferative). Logistic models and Fisher’s scoring were used to determine the ORs for pain related outcomes in cases. P-values were obtained using Pearson’s chi square, Fisher’s exact test, the one-way analysis of covariance F-test corrected with Tukey when appropriate or the Spearman Rho statistic test in the appropriate contexts. Results were considered statistically significant when P < 0.05. Statistical analyses were performed by the statistician (DS) using the software SAS 9.4 by SAS Institute Inc. (Cary, NC, USA). Due to the exploratory nature of the study, no adjustment for multiple comparison was done.
Characteristics of EM and controls are despicted in Table 1. A total of 16 estrogen derivatives were quantified by MS in the serums of 341 women. Most estrogens and their oxidative metabolites (11 out of 16) were above LLOQ, except for 4OH-E2, 17epi-E3, 2MeO-E2, 4MeO-E1 and 4MeO-E2 detected in less than 12% of the cohort. These five estrogens were thus excluded in subsequent statistical analyses (Supplementary Table 2). Levels of estrogens are displayed in Table 2 with E1, E2, 2OH-E1, E3, 16αOH-E1 and 16keto-E2 displaying the highest levels. In addition, 2OH-3MeOE1 levels were higher in cases compared to controls (by 123%; P = 0.02) (Table 2). The analysis of hormone levels according to anatomic sites of EM (Table 3), showed higher levels of 2OH-E1 (by 18%; P = 0.009), 2MeO-E1 (38%; P = 0.002), sum of 2OH (7%; P = 0.013), sum of MeO (23%; P = 0.036), ratio of 2OH/sum E1/E2 (24%; P = 0.023), and ratio of 2OH-E1/16αOH-E1 (101%; P = 0.033) in cases diagnosed with ovarian EM. No evidence of an association was observed in relation to surgical stage (Supplementary Table 3).
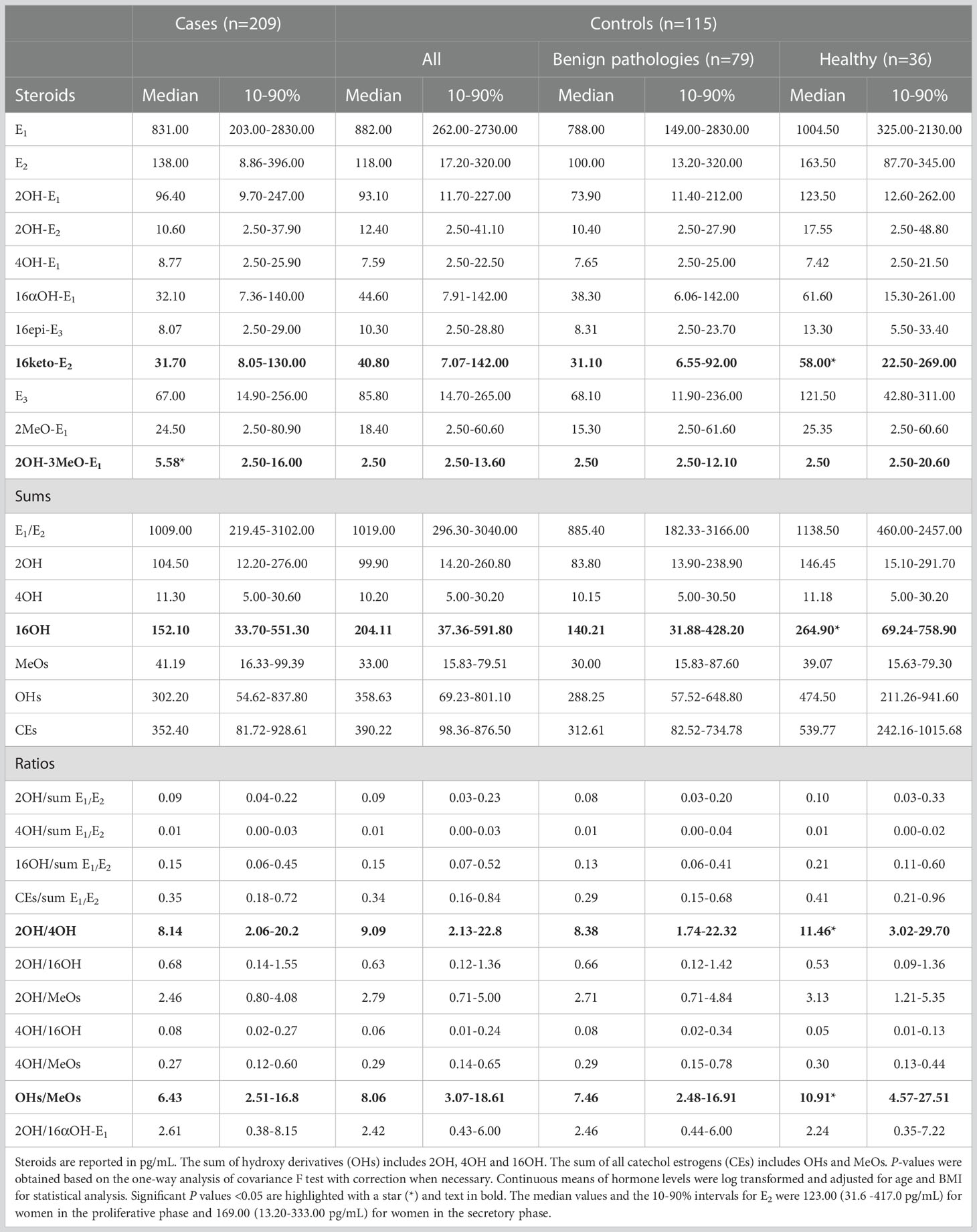
Table 2 Steroid levels for EM cases (n=209) and for controls (n=115) that included subjects with benign pathologies and healthy controls.
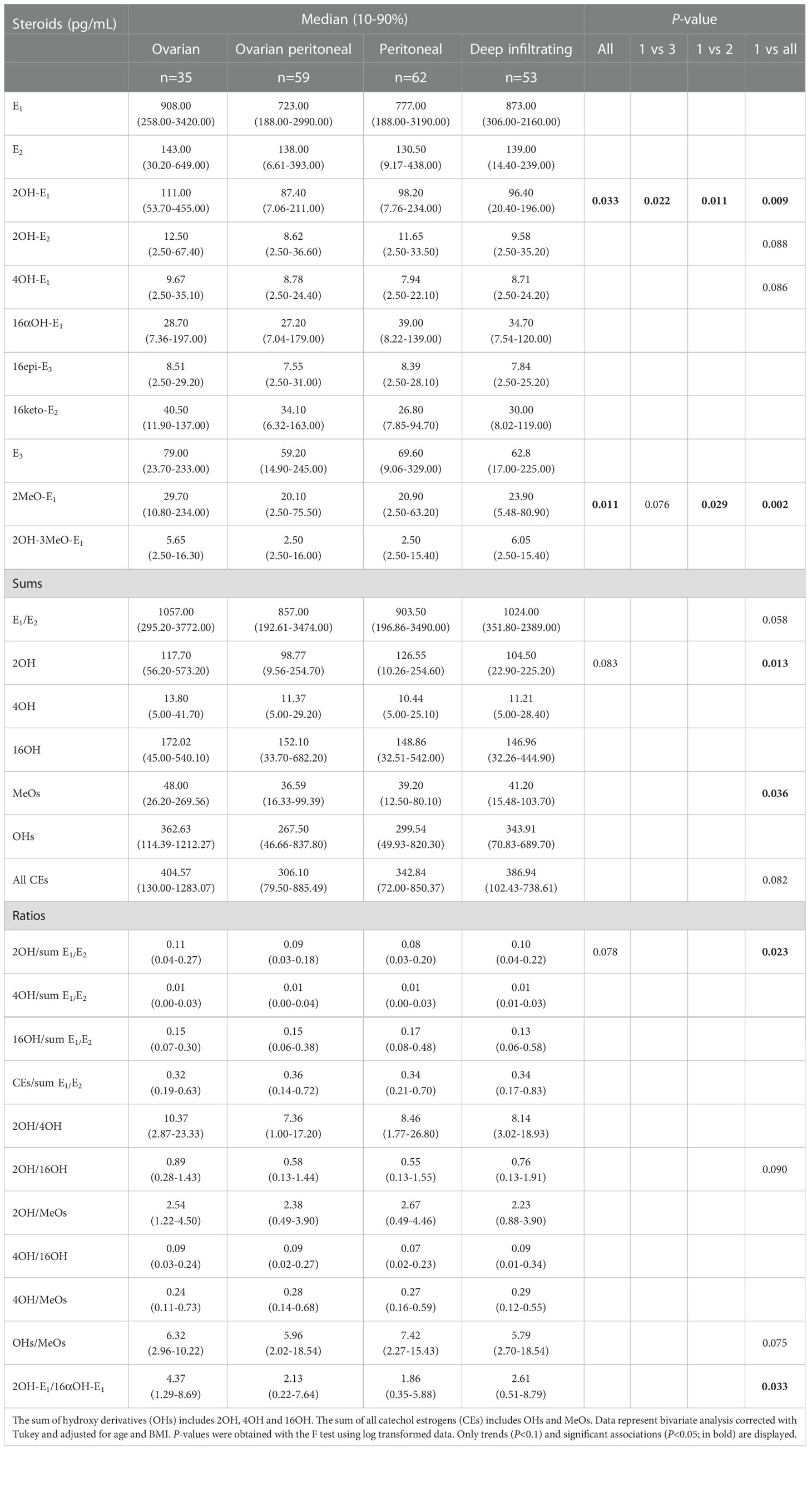
Table 3 Steroid levels according to anatomic sites of disease in 209 endometriosis cases.
The first objective aimed to establish the potential association of estrogens with the risk of developing EM. Women with higher circulating levels of specific catechol estrogens were shown to be more predisposed to EM risk in multivariable analysis adjusted for confounders including age, BMI, tobacco status, contraception, hormonal therapy and endometrial phase, which differ in EM cases compared to controls (Table 1). More specifically, women with higher levels of 2OH-3MeO-E1 had an adjusted OR of 1.91 (95%CI 1.09-3.34; P =0.025). This finding was also observed when restricted to healthy subjects and controls with benign pathologies (OR =2.61 (95%CI 0.84–8.09); P =0.097 and 1.56 (95%CI 0.84–2.91); P =0.164) but did not reached significance. A lower risk of EM was observed in association with elevated 16OH derivatives (with OR values of 0.22 for 16epi-E3 (95%CI 0.06–0.83); P =0.025) and 0.22 for 16keto-E2 (95%CI 0.06–0.84); P =0.027). Since 2OH-3MeO-E1 was the main metabolite associated with the risk of EM, we evaluated whether the correlation of this metabolite with the other estrogens was different between controls and cases. We observed that 2OH-3MeO-E1 was weakly but significantly correlated with 2-OH derivatives in EM cases at 0.20 (P<0.05) but not in controls (Table 4).
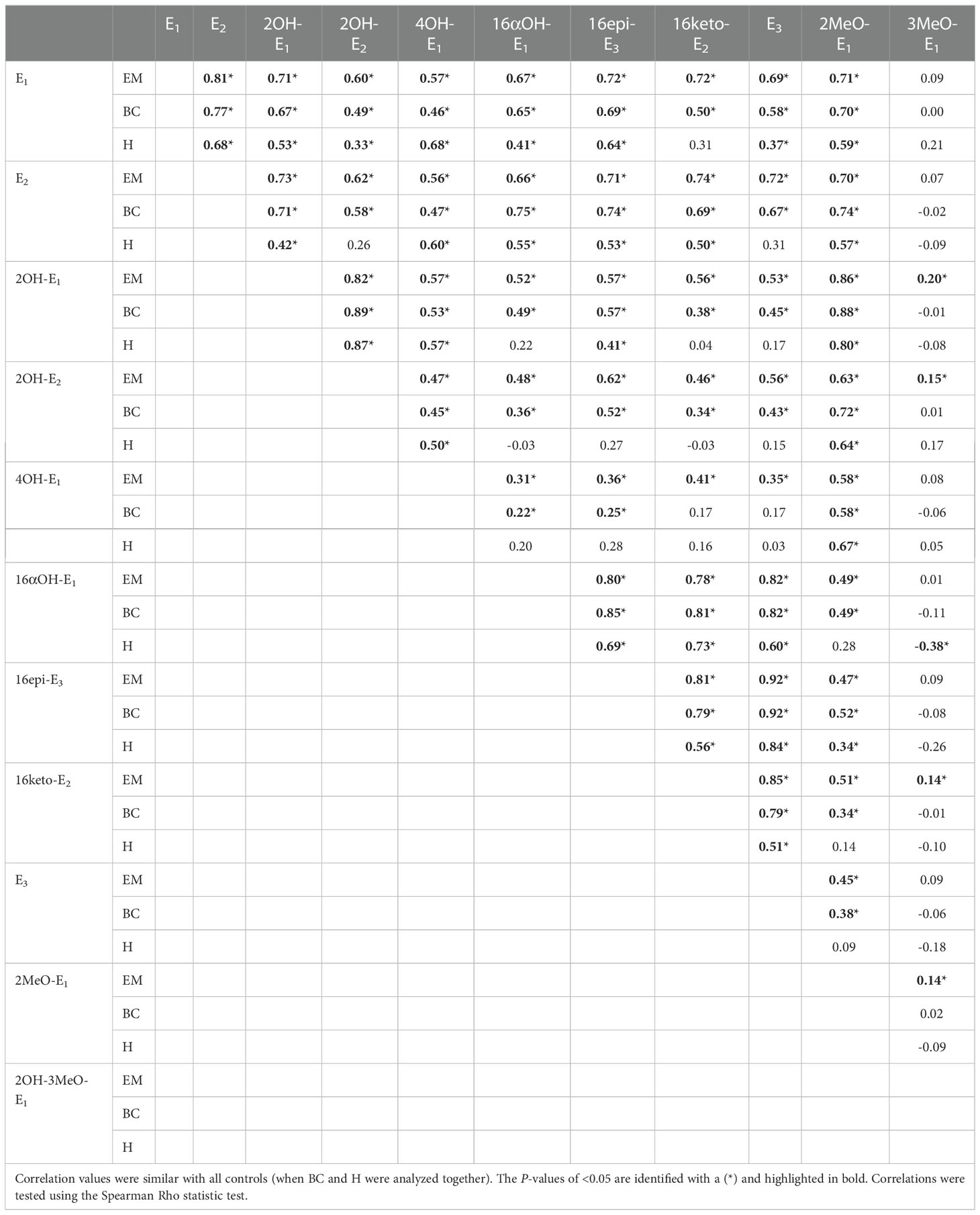
Table 4 Spearman correlation coefficients among endogenous hormone levels in endometriosis cases (EM), benign conditions (BC) and healthy (H).
A secondary objective aimed to explore the relationship between hormone levels and symptoms of pain in EM cases (Table 5). Higher levels of 2OH-3MeO-E1 were associated with the risk of pain in the abdominal, pelvic and back regions (OR =1.86 (95%CI 1.06-3.27) P =0.032). Higher levels of 16αOH-E1 were inversely associated with the risk of pain in the abdominal, pelvic and back regions (OR =0.55 (95%CI 0.31-0.97); P =0.038). More frequent menstrual pain was associated with elevated E1/E2 (OR = 1.90 (95%CI 1.03-3.51); P =0.041) whereas more severe menstrual pain was linked to a higher metabolic ratio of 4OH/sum of E1/E2 (OR =1.95; (95%CI 1.05-3.61); P =0.035) (Table 5). Higher levels of 16keto-E2 were associated with the risk of more severe dyspareunia experienced in the last three months (OR = 2.40 (95%CI 1.02-5.62); P =0.045. Higher levels of 4OH-E1 were associated with a reduced risk dysuria or dyschezia experienced in the last three months (OR =0.32 (95%CI 0.12-0.89); P =0.028) (Supplementary Table 4).
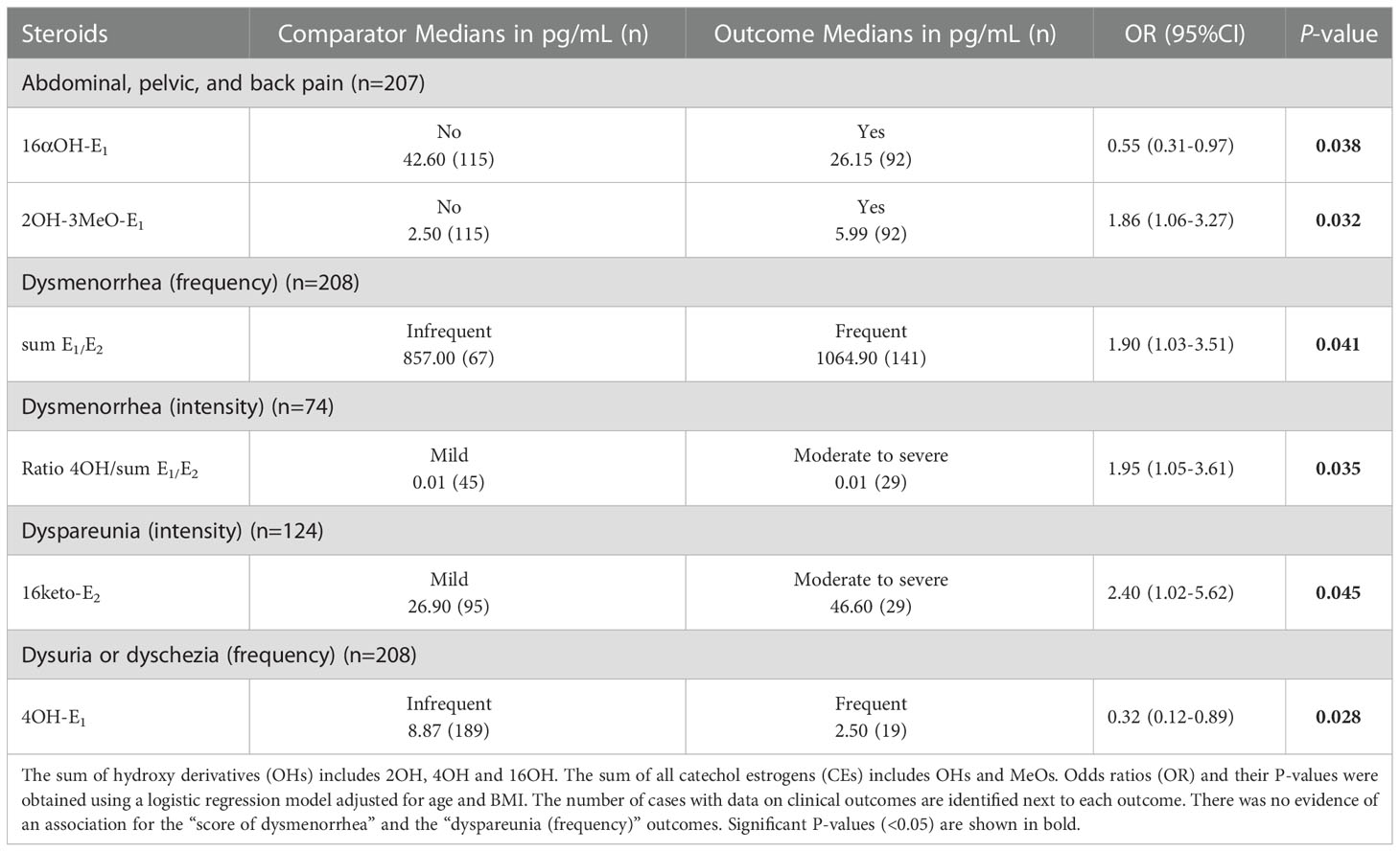
Table 5 Significant associations between pain and steroid levels in EM cases (n=209).
EM is a complex estrogen-sensitive condition characterized by a chronic inflammation process for which the potential role of estrogen metabolites remains to be fully investigated. We report that higher levels of 2OH-3MeO-E1 were associated with an increased risk of EM, with an approximately two-fold higher median level observed in circulation of EM cases compared to controls. An enrichment of the 2OH metabolic pathway, with significantly higher levels of 2OH-E1, 2MeO-E1, sum of MeO and ratio of 2OH-E1/16αOH-E1, was also observed in ovarian EM cases compared to cases affected with lesions at other anatomical sites. A perturbation of estrogen metabolism (2OH-3MeO-E1 and 16αOH-E1) was further associated with pain symptoms.
Estrogens and their receptors play a key role in the pathophysiology of EM. Studies reported higher levels of systemic and locally synthesized estrogens in EM cases promoting the growth of lesions (38). This increase in estrogens was attributed to the secretion of estrogens by the ovaries as well as their autocrine and paracrine action, and an increased aromatase activity in EM lesions that supports local E2 synthesis (15, 17, 39–41). Additional changes in estrogen synthesis, as well as their metabolic and receptor pathways, have also been reported in support of an enhanced local production and action in EM lesions, creating a hyperestrogenic environment that affects hormone receptor function (38, 42–49). These changes may be reflected in circulation of EM cases with higher levels of E2 and/or its metabolites. In our study, 2OH-3MeO-E1 was associated with an increased risk of EM. This observation is consistent with elevated COMT expression in EM lesions (50) leading to the formation of 2OH-3MeO-E1 from its precursor 2OH-E1 (23), potentially contributing to higher systemic levels of this metabolite. In support, we showed that endometrial tissue can contribute to systemic estrogen levels in the context of endometrial cancer that significantly declined after surgery (29). In addition to significant higher circulating levels of 2OH-3MeO-E1metabolites in EM cases compared to controls, higher levels of 2MeO-E1 and the sum of MeOs were observed but they did not reached significance. The biological properties of 2OH-3MeO-E1 have been poorly studied. We further noted that this metabolite was less correlated in circulation with the other estrogen derivatives and particularly in control subjects, suggesting a dysregulation in the presence of EM lesions associated with its precursors such as 2OH-E1, with a higher correlation coefficient for this metabolite in EM cases at 0.20 (P<0.05). In fact, 2OH-3MeO-E1 was higher in cases compared to controls, supporting a potential EM origin. Consistent with our observation, a previous study evaluated a subset of estrogen metabolites in preoperative urine samples of 62 EM cases and 52 controls and found increased levels of the 2OH-3MeO-E1 precursor 2OH-E1 (51). Our findings that the 2OH pathway is significantly more elevated in ovarian EM cases is also consistent with a study that used proton nuclear magnetic resonance (H-NMR) spectroscopy to investigate potential non-invasive metabolomic markers in 31 infertile women with stage II and III EM cases and 15 healthy or control women (52). They found that levels of the antiangiogenic 2MeO-E1/E2 metabolites were higher in EM cases compared to controls. The enrichment of the 2OH metabolic pathway in ovarian EM cases is supported by higher tissular levels of CYP1A1, involved in the conversion of E1 and E2 to 2OH-E1 and 2OH-E2, reported to be 4-fold higher in the ovarian EM group (50, 53). Inversely, the 16OH pathway was inversely associated with EM, consistent with downregulation of the involved enzyme pathways (CYP3A) by inflammation (54, 55).
An estrogenic environment may be associated with more severe pain symptoms (13). Hence, the association between estrogen levels and pain outcomes may not be related only to the effect of estrogens, as E2 metabolites have been documented to present receptor-independent biological activities and may contribute to the maintenance of the inflammatory milieu (16). Previous reports revealed that elevated ERβ is associated with proliferation, inflammation and pain transmission (46, 56, 57), coherent with the positive correlation observed in this study between 16keto-E2 and dyspareunia in EM cases. However, the negative association between 16αOH-E1 and pelvic, abdominal and back pain suggests more complex relationships. A component of pain in EM was shown to be related to inflammatory damage of nerve fibers with neuroprotective roles for ERβ (58–61). Also, a dysregulation of both the ERα and ERβ expression pathways was observed in the ectopic endometrium in EM compared to normal endometrium in favor of a superior ERβ to ERα ratio (46, 62, 63). 16-hydroxylated derivatives are amongst E2 metabolites known to bind the ERβ receptor (24), which may explain the observed association with pain. Other studies showed that the ERα was correlated with symptoms in deep infiltrating EM (64) and that it could favor hyperalgesia by altering calcium release (61). Since the 2OH metabolites are known to bind ERα (24), this could explain the association between pain outcomes and 2OH metabolites, such as 2OH-3MeO-E1. Additional studies are required to uncover the precise biological function of the 2OH-3MeO-E1 metabolite.
This pilot study provides a comprehensive quantification of estrogens in the circulation of EM cases and controls based on a sensitive mass-spectrometry assay. It is comprised of a significant sample size, surgical and histologic confirmation of case and control status, adjustment for confounding factors and examination of pain symptoms. A limitation is the fact that the control group also included patients with gynecological conditions other than EM, which may influence the hormonal milieu (40, 65). Although cases and controls differed in confounding factors such as menstrual phase, these variables were included in the multivariate model for EM risk. Exploratory analyses in relation to pain symptoms were adjusted for age and BMI. Additional studies could provide levels of progesterone and its metabolites, shown to be dysregulated in EM and recognized to counteract the effect of E2 (48, 66), whereas the endometriotic intratissue estrogen levels may not reflect the corresponding systemic levels. Due to the exploratory nature of the study, no correction for multiple testing was applied, but our initial findings warrant replication in other cohorts.
We conclude that the 2OH-3MeO-E1 metabolite represents a potential adverse feature of EM and that the 2OH pathway is associated with the risk of ovarian endometriotic lesions. Data also suggest an association between the 2OH metabolic pathway and the risk of unfavorable pain outcomes.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by National Medical Ethics Committee in Slovenia (#0120-127/2016/6) and the Ethics committee of the CHUQc – Université Laval (#2012-993). The patients/participants provided their written informed consent to participate in this study.
Study concept and design: TR, CG. Patient recruitment and clinical data: MP, AV, JO, TR. Conducted experiments and mass spectrometry: PC, VT. Statistical analyses: DS. Drafting of the manuscript: J-PE, CG. Critical revision of the manuscript for important intellectual content: All authors. Obtaining funding: TR, CG.
This work was supported by research grants from the Canadian Institutes of Health Research (CIHR) (FRN-167269 to CG), the Canada Research Chair Program (CG) and grant from Slovenian Research Agency J3-1755 and EU H2020-MSCA-RISE grant TRENDO (101008193) to TR, J-PE received a studentship award from the Fonds de recherche du Québec – Santé. C.G. holds the Canada Research Chair in Pharmacogenomics (Tier I).
The authors thank all study participants who donated their samples, the personnel from the University Medical Centre Ljubljana, Slovenia, especially, Dr. Martina Ribič Pucelj, Marika Andonova, Vera Troha Poljančič and Tatjana Lončar and the researchers from the Institute of Biochemistry Medical Faculty University of Ljubljana Dr. Katja Vouk, Dr. Vida Kocbek, Dr. Tamara Knific and Dr. Teja Klančič, who contributed to sample and data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.1034614/full#supplementary-material
1. Rowlands IJ, Abbott JA, Montgomery GW, Hockey R, Rogers P, Mishra. GD. Prevalence and incidence of endometriosis in Australian women: A data linkage cohort study. Bjog (2021) 128:657–65. doi: 10.1111/1471-0528.16447
2. Johnson NP, Hummelshoj L, Adamson GD, Keckstein J, Taylor HS, Abrao MS, et al. World endometriosis society consensus on the classification of endometriosis. Hum Reprod (2017) 32:315–24. doi: 10.1093/humrep/dew293
3. Marinho MCP, Magalhaes TF, Fernandes LFC, Augusto KL, Brilhante AVM, Bezerra L. Quality of life in women with endometriosis: An integrative review. J Womens Health (Larchmt) (2018) 27:399–408. doi: 10.1089/jwh.2017.6397
4. Tomassetti C, D'Hooghe T. Endometriosis and infertility: Insights into the causal link and management strategies. Best Pract Res Clin Obstet Gynaecol (2018) 51:25–33. doi: 10.1016/j.bpobgyn.2018.06.002
5. Koninckx PR, Ussia A, Adamyan L, Wattiez A, Donnez J. Deep endometriosis: definition, diagnosis, and treatment. Fertil Steril (2012) 98:564–71. doi: 10.1016/j.fertnstert.2012.07.1061
6. Nisolle M, Donnez J. Peritoneal endometriosis, ovarian endometriosis, and adenomyotic nodules of the rectovaginal septum are three different entities. Fertil Steril (1997) 68:585–96. doi: 10.1016/S0015-0282(97)00191-X
7. Zondervan KT, Becker CM, Koga K, Missmer SA, Taylor RN, Viganò. P. Endometriosis. Nat Rev Dis Primers (2018) 4:9. doi: 10.1038/s41572-018-0008-5
8. Lagana AS, Garzon S, Gotte M, Vigano P, Franchi M, Ghezzi F, et al. The pathogenesis of endometriosis: Molecular and cell biology insights. Int J Mol Sci (2019) 20:5615. doi: 10.3390/ijms20225615
9. Saunders PTK, Horne AW. Endometriosis: Etiology, pathobiology, and therapeutic prospects. Cell (2021) 184:2807–24. doi: 10.1016/j.cell.2021.04.041
10. Bulun SE, Cheng YH, Yin P, Imir G, Utsunomiya H, Attar E, et al. Progesterone resistance in endometriosis: link to failure to metabolize estradiol. Mol Cell Endocrinol (2006) 248:94–103. doi: 10.1016/j.mce.2005.11.041
11. Burney RO, Talbi S, Hamilton AE, Vo KC, Nyegaard M, Nezhat CR, et al. Gene expression analysis of endometrium reveals progesterone resistance and candidate susceptibility genes in women with endometriosis. Endocrinology (2007) 148:3814–26. doi: 10.1210/en.2006-1692
12. Mercorio A, Gianpaolino P, Romano A, Dällenbach P, Pluchino N. Is intracrinology of endometriosis relevant in clinical practice? a systematic review on estrogen metabolism. Front Endocrinol (2022) 13:950866. doi: 10.3389/fendo.2022.950866
13. Greaves E, Temp J, Esnal-Zufiurre A, Mechsner S, Horne AW, Saunders PT. Estradiol is a critical mediator of macrophage-nerve cross talk in peritoneal endometriosis. Am J Pathol (2015) 185:2286–97. doi: 10.1016/j.ajpath.2015.04.012
15. Chantalat E, Valera MC, Vaysse C, Noirrit E, Rusidze M, Weyl A, et al. Estrogen receptors and endometriosis. Int J Mol Sci (2020) 21. doi: 10.3390/ijms21082815
16. Garcia-Gomez E, Vazquez-Martinez ER, Reyes-Mayoral C, Cruz-Orozco OP, Camacho-Arroyo I, Cerbon M. Regulation of inflammation pathways and inflammasome by sex steroid hormones in endometriosis. Front Endocrinol (2019) 10:935. doi: 10.3389/fendo.2019.00935
17. Mori T, Ito F, Koshiba A, Kataoka H, Tanaka Y, Okimura H, et al. Aromatase as a target for treating endometriosis. J Obstet Gynaecol Res (2018) 44:1673–81. doi: 10.1111/jog.13743
18. Noble LS, Simpson ER, Johns A, Bulun SE. Aromatase expression in endometriosis. J Clin Endocrinol Metab (1996) 81:174–9. doi: 10.1210/jcem.81.1.8550748
19. Zeitoun K, Takayama K, Sasano H, Suzuki T, Moghrabi N, Andersson S, et al. Deficient 17beta-hydroxysteroid dehydrogenase type 2 expression in endometriosis: failure to metabolize 17beta-estradiol. J Clin Endocrinol Metab (1998) 83:4474–80. doi: 10.1210/jcem.83.12.5301
20. Gupta D, Hull ML, Fraser I, Miller L, Bossuyt PM, Johnson N, et al. Endometrial biomarkers for the non-invasive diagnosis of endometriosis. Cochrane Database Syst Rev (2016) 4:Cd012165. doi: 10.1002/14651858.CD012165
21. Rizner TL. Noninvasive biomarkers of endometriosis: myth or reality? Expert Rev Mol Diagn (2014) 14:365–85. doi: 10.1586/14737159.2014.899905
22. Cavalieri EL, Rogan EG. Depurinating estrogen-DNA adducts, generators of cancer initiation: Their minimization leads to cancer prevention. Clin Transl Med (2016) 5:12. doi: 10.1186/s40169-016-0088-3
23. Dawling S, Roodi N, Mernaugh RL, Wang X, Parl FF. Catechol-o-methyltransferase (COMT)-mediated metabolism of catechol estrogens: comparison of wild-type and variant COMT isoforms. Cancer Res (2001) 61:6716–22.
24. Zhu BT, Han GZ, Shim JY, Wen Y, Jiang XR. Quantitative structure-activity relationship of various endogenous estrogen metabolites for human estrogen receptor alpha and beta subtypes: Insights into the structural determinants favoring a differential subtype binding. Endocrinology (2006) 147:4132–50. doi: 10.1210/en.2006-0113
25. Fotsis T, Zhang Y, Pepper MS, Adlercreutz H, Montesano R, Nawroth PP, et al. The endogenous oestrogen metabolite 2-methoxyoestradiol inhibits angiogenesis and suppresses tumour growth. Nature (1994) 368:237–9. doi: 10.1038/368237a0
26. Samartzis EP, Imesch P, Twiehaus A, Dubey RK, Leeners B. The estrogen metabolites 2-methoxyestradiol and 2-hydroxyestradiol inhibit endometriotic cell proliferation in estrogen-receptor-independent manner. Gynecol Endocrinol (2016) 32:529–33. doi: 10.3109/09513590.2015.1137094
27. Schumacher G, Neuhaus P. The physiological estrogen metabolite 2-methoxyestradiol reduces tumor growth and induces apoptosis in human solid tumors. J Cancer Res Clin Oncol (2001) 127:405–10. doi: 10.1007/s004320000233
28. Merriam GR, MacLusky NJ, Picard MK, Naftolin F. Comparative properties of the catechol estrogens, I: Methylation by catechol-o-methyltransferase and binding to cytosol estrogen receptors. Steroids (1980) 36:1–11. doi: 10.1016/0039-128X(80)90062-8
29. Audet-Delage Y, Gregoire J, Caron P, Turcotte V, Plante M, Ayotte P, et al. Estradiol metabolites as biomarkers of endometrial cancer prognosis after surgery. J Steroid Biochem Mol Biol (2018) 178:45–54. doi: 10.1016/j.jsbmb.2017.10.021
30. Emond JP, Lacombe L, Caron P, Turcotte V, Simonyan D, Aprikian A, et al. Urinary oestrogen steroidome as an indicator of the risk of localised prostate cancer progression. Br J Cancer (2021) 125:78–84. doi: 10.1038/s41416-021-01376-z
31. Zondervan KT, Cardon LR, Kennedy SH. What makes a good case-control study? design issues for complex traits such as endometriosis. Hum Reprod (2002) 17:1415–23. doi: 10.1093/humrep/17.6.1415
32. Knific T, Vouk K, Vogler A, Osredkar J, Gstöttner M, Wenzl R, et al. Models including serum CA-125, BMI, cyst pathology, dysmenorrhea or dyspareunia for diagnosis of endometriosis. Biomark Med (2018) 12:737–47. doi: 10.2217/bmm-2017-0426
33. Kocbek V, Vouk K, Bersinger NA, Mueller MD, Rižner TL. Panels of cytokines and other secretory proteins as potential biomarkers of ovarian endometriosis. J Mol Diagn (2015) 17:325–34. doi: 10.1016/j.jmoldx.2015.01.006
34. Vouk K, Hevir N, Ribić-Pucelj M, Haarpaintner G, Scherb H, Osredkar J, et al. Discovery of phosphatidylcholines and sphingomyelins as biomarkers for ovarian endometriosis. Hum Reprod (2012) 27:2955–65. doi: 10.1093/humrep/des152
35. Haas D, Shebl O, Shamiyeh A, Oppelt P. The rASRM score and the enzian classification for endometriosis: Their strengths and weaknesses. Acta Obstet Gynecol Scand (2013) 92:3–7. doi: 10.1111/aogs.12026
36. Vincent K, Kennedy S, Stratton P. Pain scoring in endometriosis: entry criteria and outcome measures for clinical trials. report from the art and science of endometriosis meeting. Fertil Steril (2010) 93:62–7. doi: 10.1016/j.fertnstert.2008.09.056
37. Bourdel N, Alves J, Pickering G, Ramilo I, Roman H, Canis M. Systematic review of endometriosis pain assessment: How to choose a scale? Hum Reprod Update (2015) 21:136–52. doi: 10.1093/humupd/dmu046
38. Huhtinen K, Desai R, Stahle M, Salminen A, Handelsman DJ, Perheentupa A, et al. Endometrial and endometriotic concentrations of estrone and estradiol are determined by local metabolism rather than circulating levels. J Clin Endocrinol Metab (2012) 97:4228–35. doi: 10.1210/jc.2012-1154
39. Blakemore J, Naftolin F. Aromatase: Contributions to physiology and disease in women and men. Physiol (Bethesda) (2016) 31:258–69. doi: 10.1152/physiol.00054.2015
40. Rižner TL. The important roles of steroid sulfatase and sulfotransferases in gynecological diseases. Front Pharmacol (2016) 7:30. doi: 10.3389/fphar.2016.00030
41. Utsunomiya H, Cheng YH, Lin Z, Reierstad S, Yin P, Attar E, et al. Upstream stimulatory factor-2 regulates steroidogenic factor-1 expression in endometriosis. Mol Endocrinol (2008) 22:904–14. doi: 10.1210/me.2006-0302
42. Bulun SE, Monsavais D, Pavone ME, Dyson M, Xue Q, Attar E, et al. Role of estrogen receptor-beta in endometriosis. Sem Rep Med (2012) 30:39–45. doi: 10.1055/s-0031-1299596
43. Delvoux B, Groothuis P, D'Hooghe T, Kyama C, Dunselman G, Romano A. Increased production of 17beta-estradiol in endometriosis lesions is the result of impaired metabolism. J Clin Endocrinol Metab (2009) 94:876–83. doi: 10.1210/jc.2008-2218
44. Mori T, Ito F, Koshiba A, Kataoka H, Takaoka O, Okimura H, et al. Local estrogen formation and its regulation in endometriosis. Reprod Med Biol (2019) 18:305–11. doi: 10.1002/rmb2.12285
45. Tang ZR, Zhang R, Lian ZX, Deng SL, Yu K. Estrogen-receptor expression and function in female reproductive disease. Cells (2019) 8:1123. doi: 10.3390/cells8101123
46. Yilmaz BD, Bulun SE. Endometriosis and nuclear receptors. Hum Reprod Update (2019) 25:473–85. doi: 10.1093/humupd/dmz005
47. Smuc T, Pucelj MR, Sinkovec J, Husen B, Thole H, Rizner TL. Expression analysis of the genes involved in estradiol and progesterone action in human ovarian endometriosis. Gynecol Endocrinol (2007) 23:105–11. doi: 10.1080/09513590601152219
48. Smuc T, Rizner TL. Aberrant pre-receptor regulation of estrogen and progesterone action in endometrial cancer. Mol Cell Endocrinol (2009) 301:74–82. doi: 10.1016/j.mce.2008.09.019
49. Rizner TL. Estrogen metabolism and action in endometriosis. Mol Cell Endocrinol (2009) 307:8–18. doi: 10.1016/j.mce.2009.03.022
50. Hevir N, Ribič-Pucelj M, Rižner TL. Disturbed balance between phase I and II metabolizing enzymes in ovarian endometriosis: a source of excessive hydroxy-estrogens and ROS? Mol Cell Endocrinol (2013) 367:74–84. doi: 10.1016/j.mce.2012.12.019
51. Othman ER, Markeb AA, Khashbah MY, Abdelaal II, ElMelegy TT, Fetih AN, et al. Markers of local and systemic estrogen metabolism in endometriosis. Reprod Sci (2021) 28:1001–11. doi: 10.1007/s43032-020-00383-4
52. Ghazi N, Arjmand M, Akbari Z, Mellati AO, Saheb-Kashaf H, Zamani. Z. (1)H NMR- based metabolomics approaches as non- invasive tools for diagnosis of endometriosis. Int J Reprod BioMed (2016) 14:1–8. doi: 10.29252/ijrm.14.1.1
53. Piccinato CA, Neme RM, Torres N, Sanches LR, Cruz Derogis PB, Brudniewski HF, et al. Increased expression of CYP1A1 and CYP1B1 in ovarian/peritoneal endometriotic lesions. Reproduction (2016) 151:683–92. doi: 10.1530/REP-15-0581
54. Harvey RD, Morgan ET. Cancer, inflammation, and therapy: effects on cytochrome p450-mediated drug metabolism and implications for novel immunotherapeutic agents. Clin Pharmacol Ther (2014) 96:449–57. doi: 10.1038/clpt.2014.143
55. Rižner TL. Estrogen biosynthesis, phase I and phase II metabolism, and action in endometrial cancer. Mol Cell Endocrinol (2013) 381:124–39. doi: 10.1016/j.mce.2013.07.026
56. Han SJ, Jung SY, Wu SP, Hawkins SM, Park MJ, Kyo S, et al. Estrogen receptor β modulates apoptosis complexes and the inflammasome to drive the pathogenesis of endometriosis. Cell (2015) 163:960–74. doi: 10.1016/j.cell.2015.10.034
57. Monsivais D, Dyson MT, Yin P, Coon JS, Navarro A, Feng G, et al. ERβ- and prostaglandin E2-regulated pathways integrate cell proliferation via ras-like and estrogen-regulated growth inhibitor in endometriosis. Mol Endocrinol (2014) 28:1304–15. doi: 10.1210/me.2013-1421
58. Sommer C, Leinders M, Üçeyler N. Inflammation in the pathophysiology of neuropathic pain. Pain (2018) 159:595–602. doi: 10.1097/j.pain.0000000000001122
59. Howard FM. Endometriosis and mechanisms of pelvic pain. J Minim Invasive Gynecol (2009) 16:540–50. doi: 10.1016/j.jmig.2009.06.017
60. Kiguchi N, Kobayashi D, Saika F, Matsuzaki S, Kishioka S. Pharmacological regulation of neuropathic pain driven by inflammatory macrophages. Int J Mol Sci (2017) 18:2296. doi: 10.3390/ijms18112296
61. Chen Q, Zhang W, Sadana N, Chen X. Estrogen receptors in pain modulation: Cellular signaling. Biol Sex Differ (2021) 12:22. doi: 10.1186/s13293-021-00364-5
62. Xue Q, Lin Z, Cheng YH, Huang CC, Marsh E, Yin P, et al. Promoter methylation regulates estrogen receptor 2 in human endometrium and endometriosis. Biol Reprod (2007) 77:681–7. doi: 10.1095/biolreprod.107.061804
63. Vouk K, Smuc T, Guggenberger C, Ribič-Pucelj M, Sinkovec J, Husen B, et al. Novel estrogen-related genes and potential biomarkers of ovarian endometriosis identified by differential expression analysis. J Steroid Biochem Mol Biol (2011) 125:231–42. doi: 10.1016/j.jsbmb.2011.03.010
64. Pluchino N, Mamillapalli R, Wenger JM, Ramyead L, Drakopoulos P, Tille JC, et al. Estrogen receptor-α immunoreactivity predicts symptom severity and pain recurrence in deep endometriosis. Fertil Steril (2020) 113:1224–31.e1. doi: 10.1016/j.fertnstert.2020.01.036
65. Vander Borght M, Wyns C. Fertility and infertility: Definition and epidemiology. Clin Biochem (2018) 62:2–10. doi: 10.1016/j.clinbiochem.2018.03.012
Keywords: endometriosis, catechol estrogens, steroids, mass spectrometry, pain symptoms
Citation: Emond J-P, Caron P, Pušić M, Turcotte V, Simonyan D, Vogler A, Osredkar J, Rižner TL and Guillemette C (2023) Circulating estradiol and its biologically active metabolites in endometriosis and in relation to pain symptoms. Front. Endocrinol. 13:1034614. doi: 10.3389/fendo.2022.1034614
Received: 01 September 2022; Accepted: 19 December 2022;
Published: 18 January 2023.
Edited by:
Abdel Halim Harrath, King Saud University, Saudi ArabiaReviewed by:
Silvia Vannuccini, University of Florence, ItalyCopyright © 2023 Emond, Caron, Pušić, Turcotte, Simonyan, Vogler, Osredkar, Rižner and Guillemette. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chantal Guillemette, Y2hhbnRhbC5ndWlsbGVtZXR0ZUBjcmNodWRlcXVlYmVjLnVsYXZhbC5jYQ==; Tea Lanišnik Rižner, dGVhLmxhbmlzbmlrLXJpem5lckBtZi51bmktbGouc2k=
†These authors have contributed equally to this work and share first authorship
‡These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.