
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
HYPOTHESIS AND THEORY article
Front. Endocrinol. , 13 January 2022
Sec. Bone Research
Volume 12 - 2021 | https://doi.org/10.3389/fendo.2021.800376
This article is part of the Research Topic Diseases in the COVID-19 Epidemic View all 5 articles
 Abeer N. Alshukairi1,2*
Abeer N. Alshukairi1,2* Hazem Doar3
Hazem Doar3 Afaf Al-Sagheir4
Afaf Al-Sagheir4 Mona A. Bahasan5Anas A. Sultan1Mohammad K. Al Hroub6
Mona A. Bahasan5Anas A. Sultan1Mohammad K. Al Hroub6 Dina Itani7Imran Khalid1,2
Dina Itani7Imran Khalid1,2 Mohammed F. Saeedi1Sarah Bakhamis4Laila Layqah8Afnan A. Almutairi1Mona Saifullah7Lama Hefni1Awad Al-Omari2,9Basem M. Alraddadi1,2Salim A. Baharoon10
Mohammed F. Saeedi1Sarah Bakhamis4Laila Layqah8Afnan A. Almutairi1Mona Saifullah7Lama Hefni1Awad Al-Omari2,9Basem M. Alraddadi1,2Salim A. Baharoon10Background: Although genetic diseases are rare, children with such conditions who get infected with COVID-19 tend to have a severe illness requiring hospitalization. Osteogenesis imperfecta (OI) is a rare genetic disorder of collagen resulting in fractures and skeletal deformities. Kyphoscoliosis, restrictive lung disease, and pneumonia worsen the prognosis of patients with OI. The use of bisphosphonate improves bone mineral density (BMD) and reduces fractures in OI. There is no literature describing the impact of COVID-19 in patients with OI.
Methodology: A retrospective multi-center study was performed in three hospitals in Jeddah and Riyadh, Saudi Arabia, from March 1st, 2020, until August 31st, 2021, aiming to evaluate the outcome of COVID-19 in patients with OI. Demographics, vaccination status, underlying kyphoscoliosis, functional status, use of bisphosphonate, BMD, and COVID-19 severity, and course were recorded for all patients.
Results: Twelve cases of confirmed COVID-19 were identified among 146 patients with OI. 9 (75%) of patients were less than 18 years, 6 (50%) were male, 5 (41%) had kyphoscoliosis, and 5 (41%) were wheelchair-bound. 6 (50%) received bisphosphonate, and 7(58%) had normal BMD. All patients had mild disease and did not require hospitalization. None of OI the patients with COVID-19 were fully vaccinated before the infection, and some were ineligible for vaccination.
Conclusion: Patients with OI and COVID-19 in our study recovered without complications, unlike patients with other genetic diseases. Young age and mild illness contributed to the favorable outcome. Half of the patients received bisphosphonate and had normal BMD.
As the COVID-19 pandemic continues to cause new cases worldwide, the epidemiology of SARS-CoV-2 infection is evolving with the emergence of variant strains of concern, in addition to the reporting of an increasing number of cases among children (1, 2). Both adults and children with comorbidities infected with COVID-19 are at risk to develop severe pneumonia requiring hospitalization (3, 4). Although they are rare, children with genetic diseases infected with SAS-CoV-2 infection were more likely to be hospitalized and develop severe illness and intensive care unit admission (5). Studies evaluating the outcome of COVID-19 in adults in Saudi Arabia showed that patients with comorbidities, including diabetes mellitus and cardiovascular diseases, had a severe illness and high mortality (6, 7). The mortality rate among diabetic COVID-19 patients was 20.3% compared to 12.3% in non-diabetic COVID-19 patients (6). On the other hand, studies describing the outcome of COVID-19 in children in Saudi Arabia were variable depending on the study design, disease severity, and inclusion of patients with comorbidities. While studies that included hospitalized COVID-19 children reported 4% mortality among patients requiring intensive care admission (8, 9), studies that included non-hospitalized COVID-19 children described favorable outcomes (10, 11). In the two most extensive studies of COVID-19 in children in Saudi Arabia, only 15% of children had comorbidities (10, 11).
Osteogenesis Imperfecta (OI) is a rare genetic disease that affects type I collagen with variable severity resulting in skeletal abnormalities and variable predisposition to fractures. Based on the genetic classification of OI, mild type I disease was caused by a deficiency of normal collagen. In contrast, lethal type II, severe type III, and moderate type IV diseases had abnormal collagen structure (12). Scoliosis, restrictive lung disease and respiratory tract infections significantly impact the quality of life of patients with OI and are considered important causes of death in a severe form of OI (13). Data on outcomes of OI patients infected with SARS-CoV-2 is limited. Among a cohort of 146 OI patients, we described the favorable outcome of 12 COVID-19 patients and evaluated various factors contributing to their excellent prognosis.
We performed a retrospective study to identify all cases of OI diagnosed and followed in three tertiary care centers in Jeddah and Riyadh in Saudi Arabia. We reviewed their medical records for demographics, functional status, kyphoscoliosis, results of pulmonary function tests, use of calcium, vitamin D, and bisphosphonate, and effects of bone mineral density. We also checked their vaccination status, the type of vaccine, the time of vaccination, and COVID 19 diagnosis within the last 18 months from the Ministry of Health database. Patients with OI confirmed the home isolation clinic nurses called COVID-19 to evaluate COVID-19 disease severity, hospitalization, and outcome. Patients with OI and infected with COVID-19 were included from March 1st, 2020, until August 31st, 2021. The institutional research board approved our study of King Faisal Specialist Hospital and Research Center in Jeddah, Saudi Arabia (IRB-2021-CR-17).
146 patients with OI were included in our study. 119 (82%) were less than 18 years old, with a mean age of 12.9. 97 (66%) were male. 35 (24%) had kyphoscoliosis. 92 (63%) of patients were receiving bisphosphonate. 83 (57%) were vaccine eligible. 55/83 (66%) of vaccine-eligible patients were fully vaccinated. 58/67 (87%) of patients received Pfizer-BioNTech vaccination. 12/146 (8%) of patients with OI had confirmed COVID-19 based on positive SARS-CoV-2 nasopharyngeal PCR (Table 1).
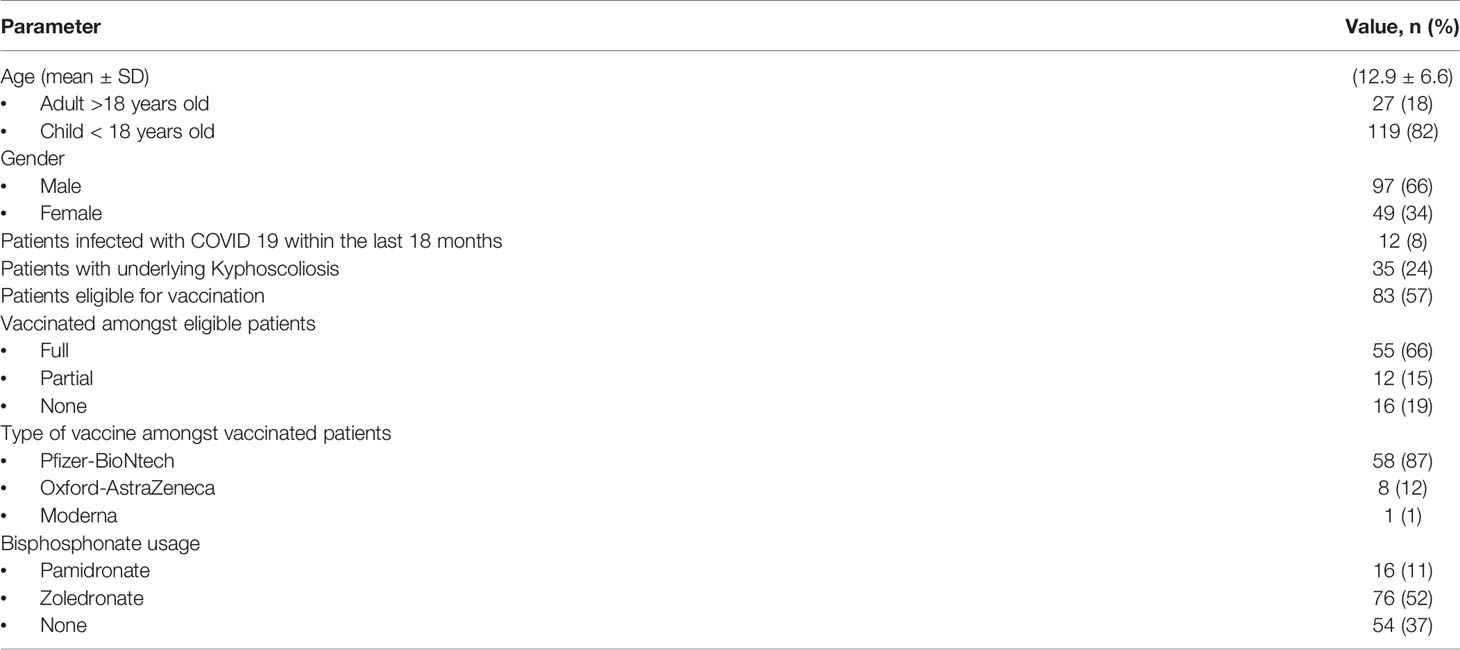
Table 1 Characteristics of patients with Osteogenesis Imperfecta (n = 146).
9 (75%) of patients were less than 18 years, and 6 (50%) were males. 5 (41%) had kyphoscoliosis, 5 (41%) were wheelchair-bound. Pulmonary function tests were performed in only one patient. 6 (50%) were receiving bisphosphonate, 10 (83%) were receiving vitamin D, 7(58%) were receiving calcium, and 7(58%) had normal BMD. All patients did not require hospitalization and recovered with no complications. 11 (91%) patients had mild disease (fever, headache, myalgia, arthralgia, and cough). One patient was asymptomatic. 9 (75%) were eligible for vaccination. 5 (41%) were fully vaccinated. All patients had COVID-19 before or after partial vaccination (Table 2). Figure 1 shows the spine X-ray of case 6, which had severe restrictive lung disease.
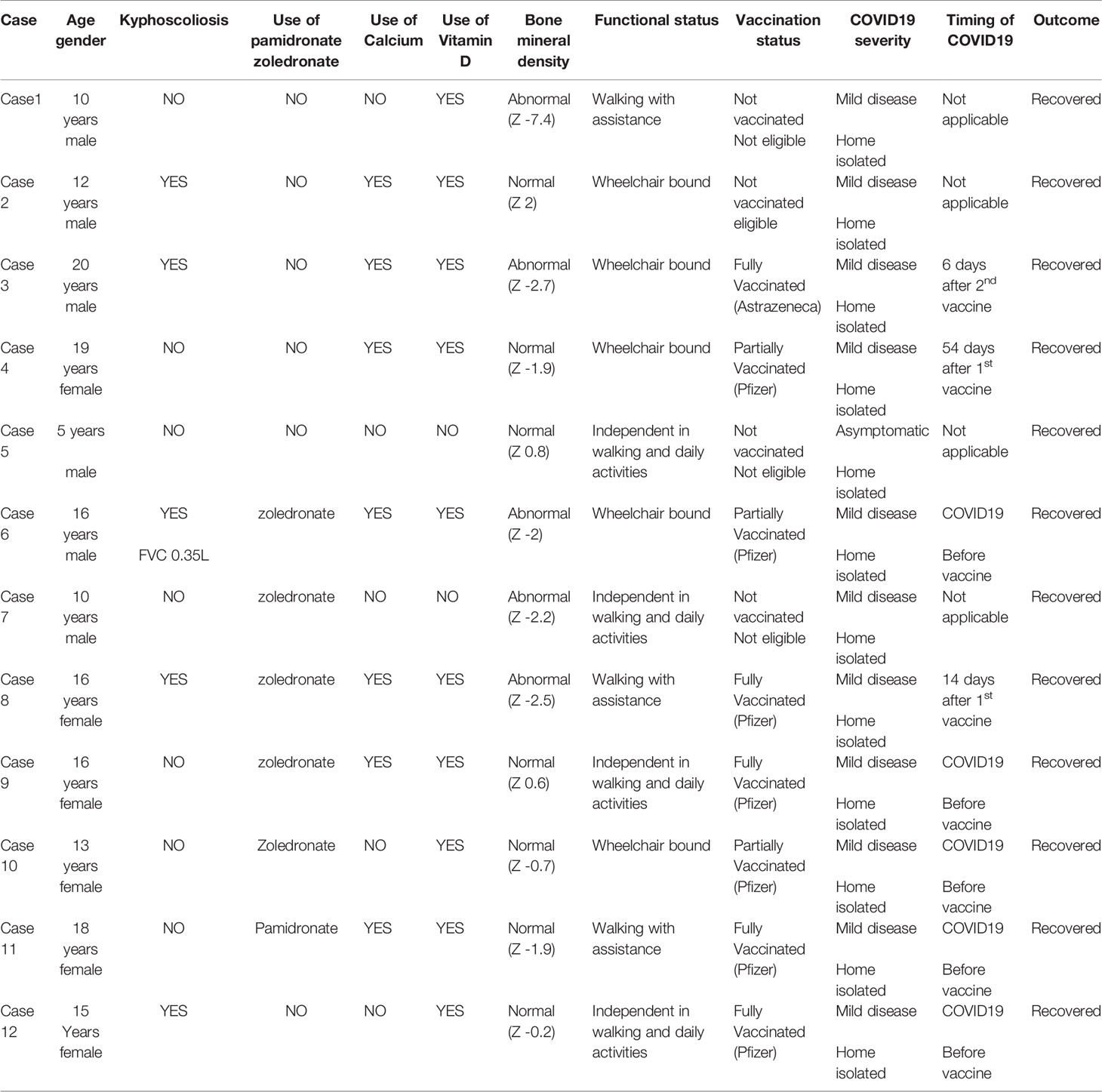
Table 2 Characteristics of patients with Osteogenesis Imperfecta infected with COVID-19 (n = 12).

Figure 1 Whole spine X-ray of a patient with Osteogenesis Imperfecta and infected with COVID-19 showed severe scoliosis and Cobb’s angle of 70 in the thoracic curve.
In our cohort, all patients with OI had mild COVID-19, did not require hospitalization, and recovered without complications. Almost half of the patients develop COVID-19 before vaccination or after partial vaccination during the period of circulating SARS-CoV-2 variants of concern, predominately SARS-CoV-2 Delta virus (14). Nine out of 12 patients were less than 18 years old, 41% were chair bound, and 41% had kyphoscoliosis. 50% of patients received bisphosphonate, and 57% had normal BMN.
A multi-center study evaluated the extent of pulmonary dysfunction among patients with OI and found that patients with severe OI had significant restrictive lung disease even in the absence of kyphoscoliosis. The mean age of the study population was older than our study (15). Unfortunately, the extent of restrictive lung disease among patients with OI could not be evaluated in our research as pulmonary function tests were not performed except in one patient who had severe restrictive lung disease. At the same time, most of them were children and were not cooperative. In addition, patients with OI were not referred to the pulmonary service without respiratory complications. Chronic lung diseases are significant predictors of COVID-19 disease severity and mortality. Most studies evaluated patients with obstructive pulmonary diseases, interstitial lung diseases, and pulmonary vascular diseases with limited data on kyphoscoliosis and restrictive lung diseases (16). Only one case report described the fatal outcome of COVID-19 in a 57 years old male patient with severe restrictive lung disease secondary to advanced idiopathic kyphoscoliosis (17).
The use of bisphosphonate in patients with OI increased bone mineral density, reduced fractures, and improved functional activity (18–20). Recently, several studies described that fractures in adults infected with COVID-19 were associated with a worse outcome compared to non-COVID-19 patients. A meta-analysis showed that COVID-positive patients with hip fractures had significantly higher mortality than COVID-19 negative patients (21). Di Filippo compared the outcome of COVID-19 patients among patients with and without thoracic vertebral fractures retrospectively. COVID-19 patients with vertebral fractures were older, had co-morbidities, required hospitalization, and non-invasive ventilation compared to those without fractures. Although there was no significant mortality difference between COVID-19 patients with and without vertebral fractures, patients with severe fractures had significantly higher mortality than those with mild and moderate fractures (22). Di Filippo defined the osteo-metabolic phenotype of COVID-19 as hypocalcemia, hypovitaminosis D, and vertebral fractures described its poor outcome, and suggested therapeutic and preventive measures such as calcium, vitamin D, and anti-osteoporotic therapy (23). In our cohort of OI, more than two-thirds of patients were started on bisphosphonate since the time of their diagnosis to reduce their fracture risks. Based on animal studies, bisphosphonate was found to have anti-inflammatory and immune-modulating effects, which may improve the outcome of SARS-CoV-2 pneumonia (24). Several observational retrospective case-controlled studies showed conflicting results regarding the impact of bisphosphonate on the development of adult patients hospitalized with COVID-19 pneumonia (25–27). One retrospective study showed that patients on parenteral zoledronate had a low incidence of COVID-19 after adjustment for different confounding factors such as age and comorbidities (25). While another two retrospective studies did not show that prior use of bisphosphonate did improve the outcome and progression to severe disease in COVID-19 adult patients (26, 27). It is worth emphasizing that these studies evaluated the prior use of bisphosphonate and its effect on COVID-19 disease severity without describing the degree of BMD and the presence of fractures.
Patients with rare genetic diseases were adversely affected during the COVID-19 pandemic, with limited access to medical care (28). Brizola E et described their experience in Italy in providing the Phone calls Helpline initiative to follow patients with rare bone diseases remotely during the COVID-19 pandemic. It was successful in answering their concerns and providing them with valuable educational information (29). In our study, among patients with OI eligible for vaccination, 66% of them received two doses of COVID-19 vaccination, though the vaccination of children in Saudi Arabia was only approved on 27th June 2021 (30). In Saudi Arabia, patients with OI were closely followed by the endocrinology service in tertiary care centers. In addition, there was no delay in administering parenteral zoledronate to these patients in the medical day units despite significant hospital limitations benefits during the COVID-19 pandemic. Adult patients with OI that do not require bisphosphonate and orthopedic procedures are transferred to primary care hospitals for future follow-up in different towns. It was challenging to reach their primary physicians to evaluate their status during the COVID-19 pandemic.
Our study was mainly descriptive for the outcome of COVID-10 patients with OI, predominantly children with mild disease. It was limited by the retrospective design and small sample, which did not evaluate predictors for severe COVID-19 illness in patients with OI. While all patients had results of BMN, biochemical parameters including serum calcium and vitamin D levels were not available for all patients. The lack of pulmonary function tests in most patients precludes the objective assessment of restrictive lung disease and its severity, being a significant risk factor for severe COVID-19. Based on our study design, we could not demonstrate whether the use of bisphosphonate could improve the outcome of COVID-19 patients with OI by reducing the rate of fractures and improving BMN.
This is the largest cohort of COVID-19 patients with OI described in the literature. Unlike other patients with genetic diseases, patients with OI in our study recovered from COVID-19 without complications. Young age and mild disease most likely contributed to the successful outcome. Although half of the patients with OI received bisphosphonate and had normal BMD, our study was not designed to evaluate the impact of bisphosphonate use on COVID-19 severity. While the prior use of bisphosphonate did not improve the outcome of COVID-19 adult patients, age and comorbidities were the most critical risk factors for severe COVID-19 pneumonia. Future studies are needed to evaluate the effect of bisphosphonate use and the degree of BMD on the prognosis of hospitalized COVID-19 adult patients. In addition, the outcome of COVID-19 in adult patients requires further investigation.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institutional Research Board, King Faisal Specialist Hospital And Research Center, Jeddah, Saudi Arabia. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
All authors contributed to the study concept, study design, literature review, data collection, data analysis, reviewing, editing, and writing the manuscript. All authors contributed to the article and approved the submitted version.
This work was funded by King Faisal Specialist Hospital and Research Center, Jeddah, Kingdom of Saudi Arabia.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank our patients who contributed to this work.
1. van Oosterhout C, Hall N, Ly H, Tyler KM. COVID-19 Evolution During the Pandemic - Implications of New SARS-CoV-2 Variants on Disease Control and Public Health Policies. Virulence (2021) 12(1):507–8. doi: 10.1080/21505594.2021.1877066
2. Abdool Karim SS, de Oliveira T. New SARS-CoV-2 Variants - Clinical, Public Health, and Vaccine Implications. N Engl J Med (2021) 384(19):1866–8. doi: 10.1056/NEJMc2100362
3. Al-Mutair A, Elhazmi A, Alhumaid S, Ahmad GY, Rabaan AA, Alghdeer MA, et al. Examining the Clinical Prognosis of Critically Ill Patients With COVID-19 Admitted to Intensive Care Units: A Nationwide Saudi Study. Medicina (2021) 57(9):878. doi: 10.3390/medicina57090878
4. Parcha V, Booker KS, Kalra R, Kuranz S, Berra L, Arora G, et al. A Retrospective Cohort Study of 12,306 Pediatric COVID-19 Patients in the United States. Sci Rep (2021) 11(1):10231. doi: 10.1038/s41598-021-89553-1
5. Duarte-Salles T, Vizcaya D, Pistillo A, Casajust P, Sena AG, Lai LYH, et al. Thirty-Day Outcomes of Children and Adolescents With COVID-19: An International Experience. Pediatrics (2021) 148:no. doi: 10.1542/peds.2020-042929
6. Alguwaihes AM, Al-Sofiani ME, Megdad M, Albader SS, Alsari MH, Alelayan A, et al. Diabetes and Covid-19 Among Hospitalized Patients in Saudi Arabia: A Single-Centre Retrospective Study. Cardiovasc Diabetol (2020) 19(1):205. doi: 10.1186/s12933-020-01184-4
7. Shaikh FS, Aldhafferi N, Buker A, Alqahtani A, Ey S, Abdulhamid S, et al. Comorbidities and Risk Factors for Severe Outcomes in COVID-19 Patients in Saudi Arabia: A Retrospective Cohort Study. J Multidiscip Healthc (2021) 14:2169–83. doi: 10.2147/jmdh.s317884
8. Kari J, Shalaby MA, Albanna AS, Alahmadi TS, Sukkar SA, MohamedNur HAH, et al. Coronavirus Disease in Children: A Multicentre Study From the Kingdom of Saudi Arabia. J Infect Public Health (2021) 14(4):543–49. doi: 10.1016/j.jiph.2021.01.011
9. Alnajjar AA, Dohain AM, Abdelmohsen GA, Alahmadi TS, Zaher ZF, Abdelgalil AA. Clinical Characteristics and Outcomes of Children With COVID-19 in Saudi Arabia. Saudi Med J (2021) 42(4):391–8. doi: 10.15537/smj.2021.42.4.20210011
10. Alharbi M, Kazzaz YM, Hameed T, Alqanatish J, Alkhalaf H, Alsadoon A, et al. SARS-CoV-2 Infection in Children, Clinical Characteristics, Diagnostic Findings and Therapeutic Interventions at a Tertiary Care Center in Riyadh, Saudi Arabia. J Infect Public Health (2021) 14(4):446–53. doi: 10.1016/j.jiph.2020.12.034
11. Almuzaini Y, Alsohime F, Subaie YSA, Temsah M, Alsofayan Y, Alamri F, et al. Clinical Profiles Associated With SARS-CoV-2 Infection and Complications From Coronavirus Disease-2019 in Children From a National Registry in Saudi Arabia. Ann Thorac Med (2021) 16(3):280–6. doi: 10.4103/atm.atm_709_20
12. Forlino A, Marini JC. Osteogenesis Imperfecta. Lancet (2016) 387(10028):1657–71. doi: 10.1016/s0140-6736(15)00728-x
13. McAllion SJ, Paterson CR. Causes of Death in Osteogenesis Imperfecta. J Clin Pathol (1996) 49(8):627–30. doi: 10.1136/jcp.49.8.627
14. Alhamlan F, Al-Qahtani A, Obeid D, Aljumaah S, Alghamdi S, Alnafeeh K, et al. SARS-CoV-2 Delta Variant Predominant at a Tertiary-Care Hospital in Saudi Arabia. Res Square Preprint (2021) Version 1. doi: 10.21203/rs.3.rs-779549/v1
15. Tam A, Chen S, Schauer E, Grafe I, Bandi V, Shapiro JR, et al. A Multicenter Study to Evaluate Pulmonary Function in Osteogenesis Imperfecta. Clin Genet (2018) 94:502–11. doi: 10.1111/cge.13440
16. Aveyard P, Gao M, Lindson N, Hartmann-Boyce J, Watkinson P, Young D, et al. Association Between Pre-Existing Respiratory Disease and its Treatment, and Severe COVID-19: A Population Cohort Study. Lancet Respir Med (2021) 9(8):909–23. doi: 10.1016/s2213-2600(21)00095-3
17. Sahu KK, Mishra AK, Martin K, Chastain I. COVID-19 and Restrictive Lung Disease: A Deadly Combo to Trip Off the Fine Balance. Monaldi Arch Chest Dis (2020) 902:no. doi: 10.4081/monaldi.2020.1346
18. Forin V, Arabi A, Guigonis V, Filipe G, Bensman A, Roux C. Benefits of Pamidronate in Children With Osteogenesis Imperfecta: An Open Prospective Study. Joint Bone Spine (2005) 72(4):313–8. doi: 10.1016/j.jbspin.2004.08.011
19. Garganta MD, Jaser SS, Lazow MA, Schoenecker JG, Cobry E, Hays SR, et al. Cyclic Bisphosphonate Therapy Reduces Pain and Improves Physical Functioning in Children With Osteogenesis Imperfecta. BMC Musculoskeletal Disord (2018) 19(1):344. doi: 10.1186/s12891-018-2252-y
20. Biggin A, Munns C. Long-Term Bisphosphonate Therapy in Osteogenesis Imperfecta. Curr Osteoporosis Rep (2017) 15(5):412–8. doi: 10.1007/s11914-017-0401-0
21. Tripathy SK, Varghese P, Panigrahi S, Panda BB, Velagada S, Sahoo S, et al. Thirty-Day Mortality of Patients With Hip Fracture During COVID-19 Pandemic and Pre-Pandemic Periods: A Systematic Review and Meta-Analysis. World J Orthop (2021) 12(1):35–50. doi: 10.5312/wjo.v12.i1.35
22. di Filippo L, Formenti AM, Doga M, Pedone E, Rovere-Querini P, Giustina A. Radiological Thoracic Vertebral Fractures are Highly Prevalent in COVID-19 and Predict Disease Outcomes. J Clin Endocrinol Metab (2021) 106(2):e602–14. doi: 10.1210/clinem/dgaa738
23. di Filippo L, Frara S, Giustina A. The Emerging Osteo-Metabolic Phenotype of COVID-19: Clinical and Pathophysiological Aspects. Nat Rev Endocrinol (2021) 17:445–6. doi: 10.1038/s41574-021-00516-y
24. Brufsky A, Marti JLG, Nasrazadani A, Lotze MT. Boning Up: Amino-Bisphophonates as Immunostimulants and Endosomal Disruptors of Dendritic Cell in SARS-CoV-2 Infection. J Transl Med (2020) 18(1):261. doi: 10.1186/s12967-020-02433-6
25. Blanch-Rubió J, Soldevila-Domenech N, Tío L, Llorente-Onaindia J, Ciria-Recasens M, Polino L, et al. Influence of Anti-Osteoporosis Treatments on the Incidence of COVID-19 in Patients With non-Inflammatory Rheumatic Conditions. Aging (Albany NY) (2020) 12(20):19923–37. doi: 10.18632/aging.104117
26. Atmaca A, Demirci I, Haymana C, Tasci I, Sahin I, Cakal E, et al. No Association of Anti-Osteoporosis Drugs With COVID-19-Related Outcomes in Women: A Nationwide Cohort Study. Osteoporos Int (2021) 32(8):1–10. doi: 10.1007/s00198-021-06067-2
27. Degli Esposti L, Perrone V, Sangiorgi D, Andretta M, Bartolini F, Cavaliere A, et al. The Use of Oral Amino-Bisphosphonates and Coronavirus Disease 2019 (COVID-19) Outcomes. J Bone Mineral Res (2021) 36(11):2177–83. doi: 10.1002/jbmr.4419
28. Chowdhury SF, Sium SMA, Anwar S. Research and Management of Rare Diseases in the COVID-19 Pandemic Era: Challenges and Countermeasures. Front Public Health (2021) 9:640282. doi: 10.3389/fpubh.2021.640282
29. Brizola E, Adami G, Baroncelli GI, Bedeschi MF, Berardi P, Boero S, et al. Providing High-Quality Care Remotely to Patients With Rare Bone Diseases During COVID-19 Pandemic. Orphanet J Rare Dis (2020) 15(1):228. doi: 10.1186/s13023-020-01513-6
30. MOH Begins Vaccinating 12-18 Age Group With Pfizer Vaccine. Ministry of Health. (2021). Available at: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2021-06-27-008.aspx.
Keywords: outcome, bisphosphonate, COVID - 19, fracture, osteogenesis imperfecta
Citation: Alshukairi AN, Doar H, Al-Sagheir A, Bahasan MA, Sultan AA, Al Hroub MK, Itani D, Khalid I, Saeedi MF, Bakhamis S, Layqah L, Almutairi AA, Saifullah M, Hefni L, Al-Omari A, Alraddadi BM and Baharoon SA (2022) Outcome of COVID19 in Patients With Osteogenesis Imperfecta: A Retrospective Multicenter Study in Saudi Arabia. Front. Endocrinol. 12:800376. doi: 10.3389/fendo.2021.800376
Received: 23 October 2021; Accepted: 17 December 2021;
Published: 13 January 2022.
Edited by:
Nicola Veronese, University of Palermo, ItalyReviewed by:
Michaël R Laurent, University Hospitals Leuven, BelgiumCopyright © 2022 Alshukairi, Doar, Al-Sagheir, Bahasan, Sultan, Al Hroub, Itani, Khalid, Saeedi, Bakhamis, Layqah, Almutairi, Saifullah, Hefni, Al-Omari, Alraddadi and Baharoon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abeer N. Alshukairi, YWJlZXIuYWxzaHVrYWlyaUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.