 Caihong Xin1†
Caihong Xin1† Xin Sun
Xin Sun
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 19 November 2021
Sec. Thyroid Endocrinology
Volume 12 - 2021 | https://doi.org/10.3389/fendo.2021.766516
Background: Cystatin C (CysC) is often used to diagnose and monitor renal diseases. Although some studies have investigated the association between serum CysC levels and thyroid diseases, their reported results were inconsistent. Therefore, the relationship between CysC levels and thyroid diseases remains controversial.
Aim: This meta-analysis aimed to statistically evaluate serum CysC levels in patients with thyroid diseases.
Methods: A literature search was conducted using the PubMed, Web of Science, Embase, EBSCO, and Wiley Online Library databases. The following search terms were used for the title or abstract: “Cystatin C” or “CysC” in combination with the terms “thyroid disease”, “thyroid function”, “hypothyroidism”, or “hyperthyroidism”. The results of the systematic analysis were presented as standardized mean differences (SMDs) with corresponding 95% confidence intervals (CIs).
Results: Eleven articles (1,265 cases and 894 controls) were included in the meta-analysis. The results of the meta-analysis showed that the serum CysC levels of patients with hyperthyroidism were significantly higher than those of the controls (SMD: 1.79, 95% CI [1.34, 2.25]), and the serum CysC levels of patients with hypothyroidism were significantly lower than those of the controls (SMD −0.59, 95% CI [−0.82, −0.36]). Moreover, the treatment of thyroid diseases significantly affected serum CysC levels.
Conclusions: To the best of our knowledge, this meta-analysis is the first to evaluate serum CysC levels in patients with thyroid diseases. Our findings suggest that thyroid function affects serum CysC levels and that serum CysC may be an effective marker for monitoring thyroid diseases.
Systematic Review Registration: PROSPERO [https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=258022], identifier CRD42021258022].
Cystatin C (CysC), a small-molecule protein belonging to the cysteine protease inhibitor superfamily, is produced by all nucleated cells. Compared with serum creatinine, changes in CysC levels can sensitively reflect changes in the glomerular filtration rate (GFR). Therefore, it is often used in the diagnosis and evaluation of kidney diseases (1). Studies have shown that serum CysC is a sensitive biomarker for detecting changes in GFR and identifying mild kidney diseases (2, 3). Moreover, patients with diabetes, chronic obstructive pulmonary disease, ischemic stroke, and myocardial infarction have been reported to have higher serum CysC levels than healthy individuals (4–7).
Thyroid diseases, including hyperthyroidism and hypothyroidism, are common endocrine system diseases. Thyroid hormones have a great influence on renal hemodynamics, water–salt balance, ion transport, renal tubular secretion, and reabsorption (8). Few studies have investigated the association between serum CysC levels and thyroid diseases. Some authors reported that the serum CysC levels of patients with hyperthyroidism and hypothyroidism were higher and lower, respectively, although the results were inconsistent (9–11). Therefore, the relationship between serum CysC levels and thyroid diseases remains controversial. This meta-analysis aimed to statistically evaluate serum CysC levels in patients with thyroid diseases. In addition, we used serum CysC levels for treatment monitoring.
We searched the following electronic databases: Web of Science, Embase, PubMed, EBSCO, and Wiley Online Library databases. The following search terms were used for the title or abstract: “Cystatin C” or “CysC” in combination with the terms “thyroid disease”, “thyroid function”, “hypothyroidism”, or “hyperthyroidism”. All studies published between 1980 and 2021 were included in the search. In addition, the references of the retrieved articles were examined to identify additional eligible studies, excluding unpublished studies. The completed Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist is presented in Supplementary Data (Table S1). This systematic review and meta-analysis was registered in PROSPERO (registration number: CRD42021258022).
The studies included in this meta-analysis met the following criteria: (1) a case–control or cohort design; (2) detailed data about serum CysC levels in patients with thyroid disease and controls; and (3) published in English.
Two researchers independently extracted general information from the included articles, such as the first author, publication year, study period, region, study design, and details of cases and controls. The Newcastle–Ottawa Scale is a risk assessment tool for observational studies recommended by the Cochrane Collaboration (12, 13). Quality of evidence was also assessed using the Grade of Recommendations Assessment, Development, and Evaluation (GRADE) approach (14). The two researchers independently assessed the studies through discussion, compared their findings, and resolved any differences by consensus. If no consensus was reached, a third researcher resolved the difference.
The results of the systematic analysis were presented as standardized mean differences (SMDs) with corresponding 95% confidence intervals (CIs). Heterogeneity among studies was assessed using Cochran’s Q test and I2 statistic. I2 of <50% was considered to have low or moderate heterogeneity, and a fixed-effects model was used. Otherwise, heterogeneity was considered high, and a random-effects model was used for the analysis. We additionally performed a sensitivity analysis to evaluate the influence of any given study on the pooled estimate. Publication bias was evaluated using Egger’s test. A P-value of <0.05 was considered to indicate statistical significance. All statistical analyses were performed using Stata version 12.0 (College Station, TX, USA).
In total, 298 studies were retrieved from the PubMed, Web of Science, Embase, EBSCO, and Wiley Online Library databases. No articles from the reference lists were included in this study. After screening, 11 articles comprising 1,265 cases and 894 controls were selected (9, 15–24). The inclusion criteria for full-text selection are presented in Figure 1. The characteristics of the selected studies are summarized in Table 1.
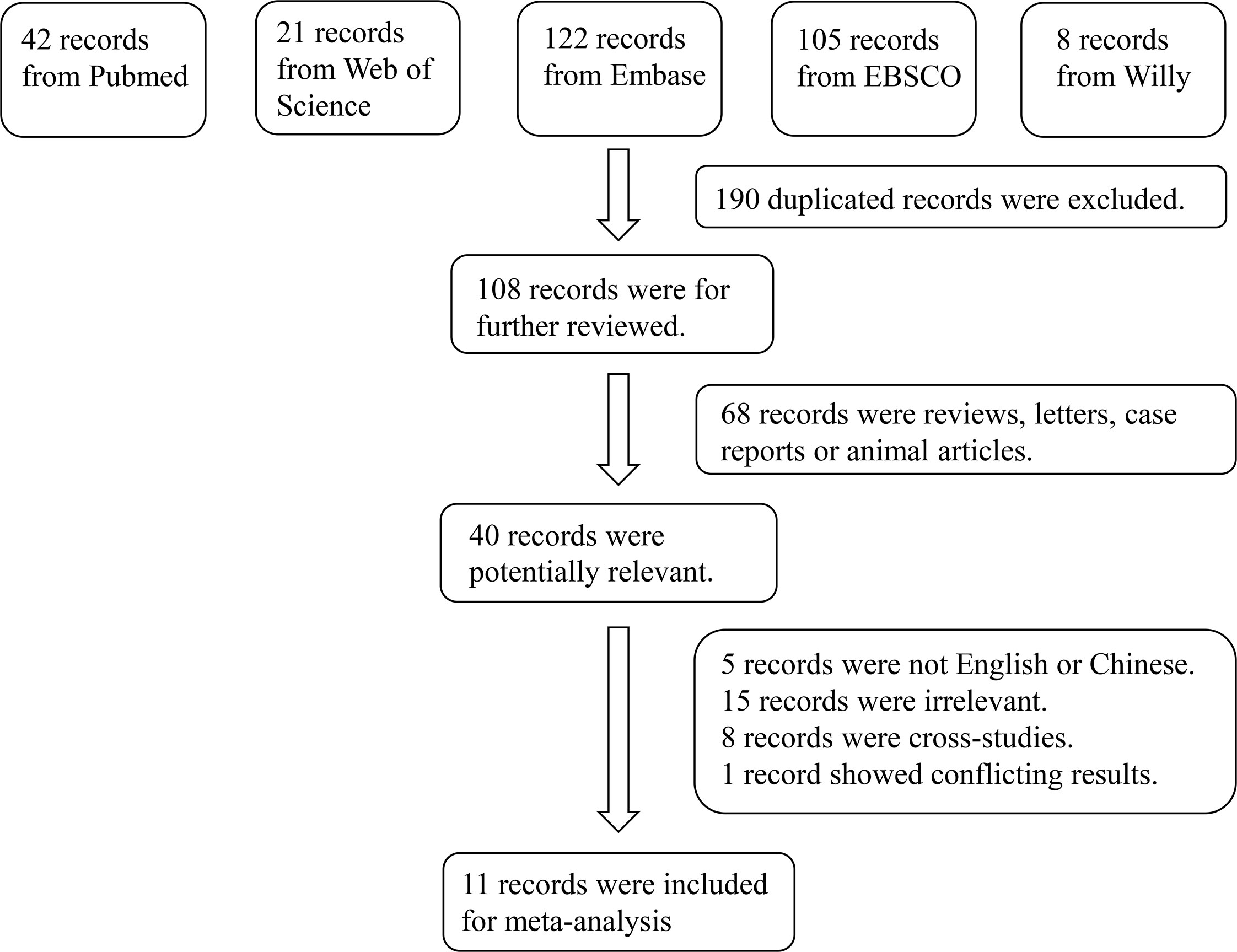
Figure 1 Flowchart of the detailed procedure for the inclusion or exclusion of selected studies.
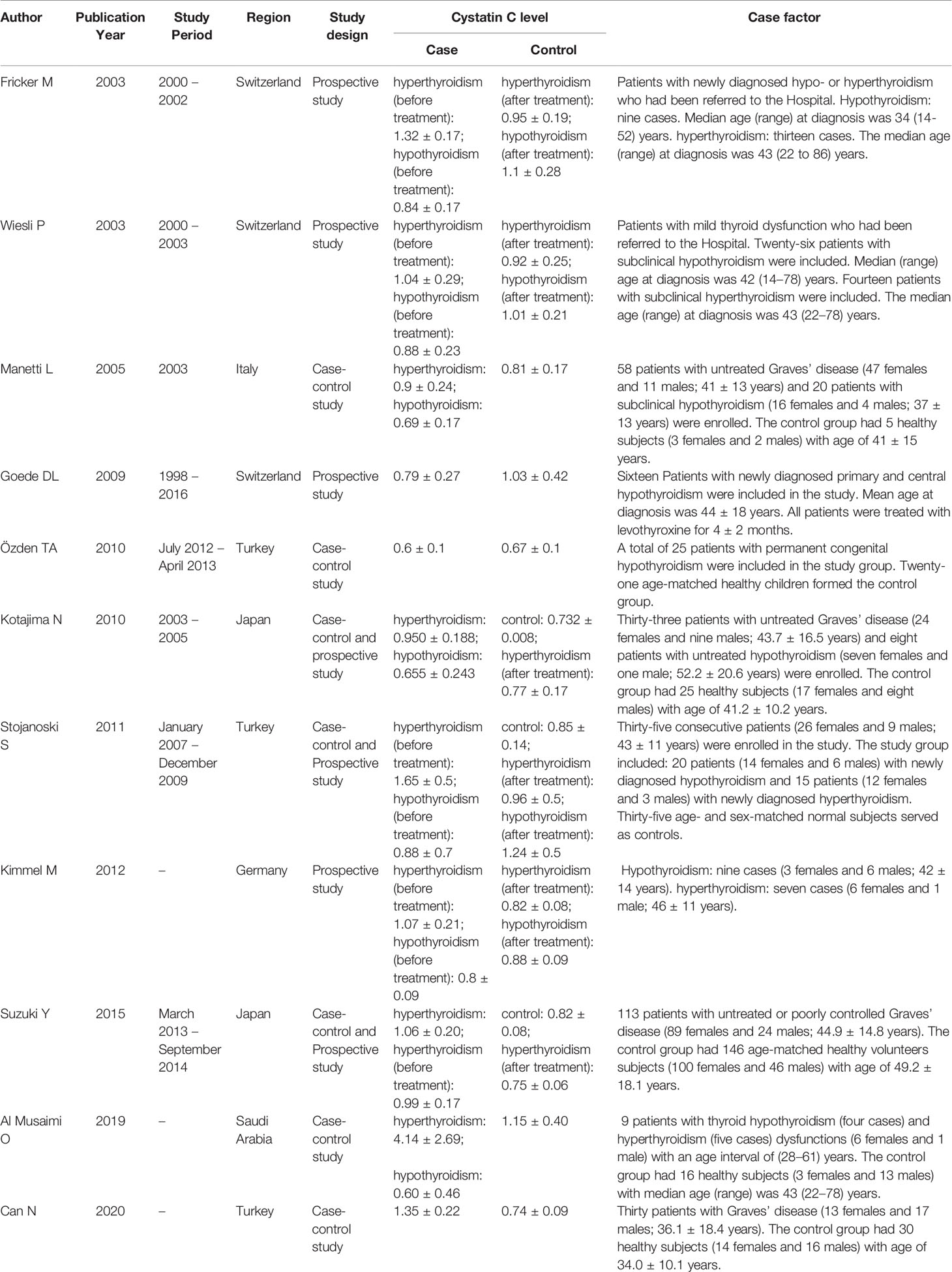
Table 1 Study characteristics of the published studies included in the meta-analysis.
The results of the meta-analysis revealed that the serum CysC levels of patients with hyperthyroidism were significantly higher than those of the controls (SMD: 1.79, 95% CI [1.34, 2.25]). The forest plots and funnel plots of serum CysC levels of patients with hyperthyroidism compared with those of controls are presented in Figure 2. The serum CysC levels of patients with hypothyroidism were significantly lower than those of the controls [SMD −0.59, 95% CI (−0.82, −0.36)]. The forest plots and funnel plots of serum CysC levels of patients with hypothyroidism compared with those of controls are presented in Figure 3.
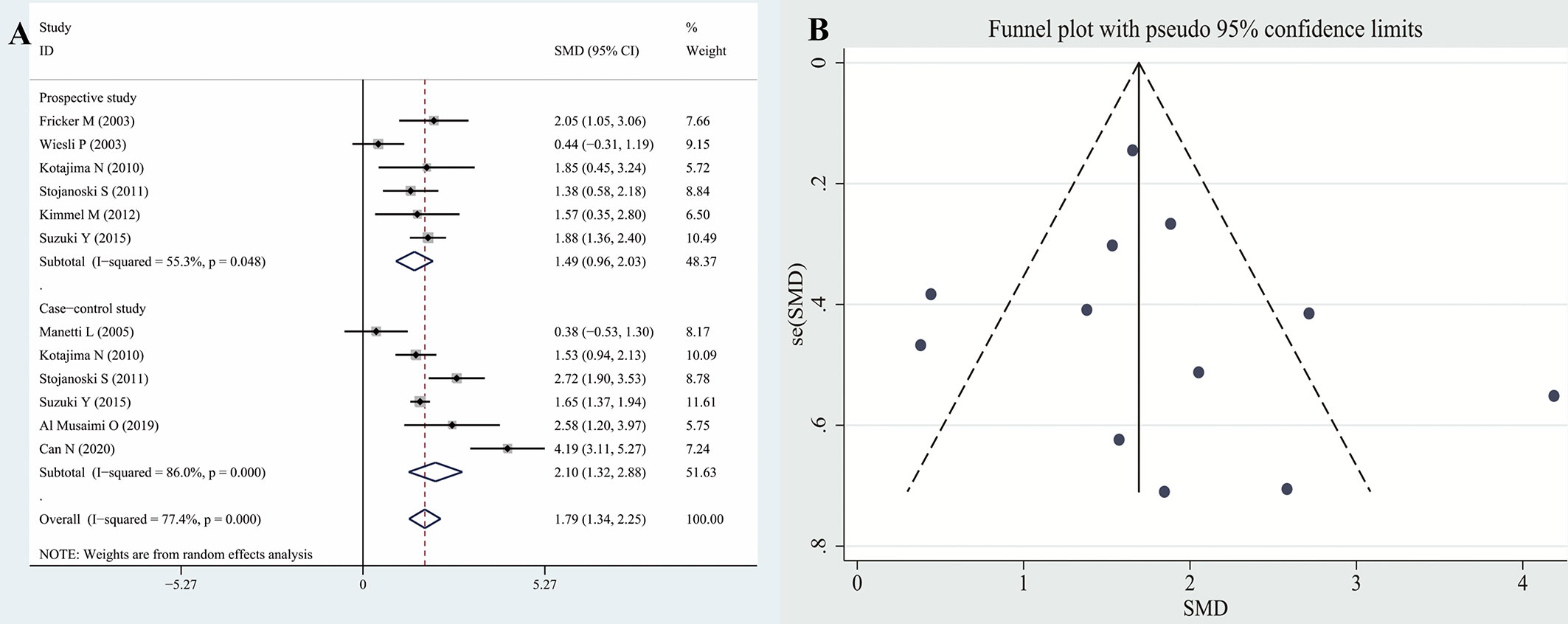
Figure 2 Forest plots and funnel plots of serum CysC in patients with hyperthyroidism compared with controls. Diamond represents the SMDs at 95% CI. (A) Forest plots; (B) Funnel plots. CysC, Cystatin C; SMD, standardized mean difference; CI, confidence interval.
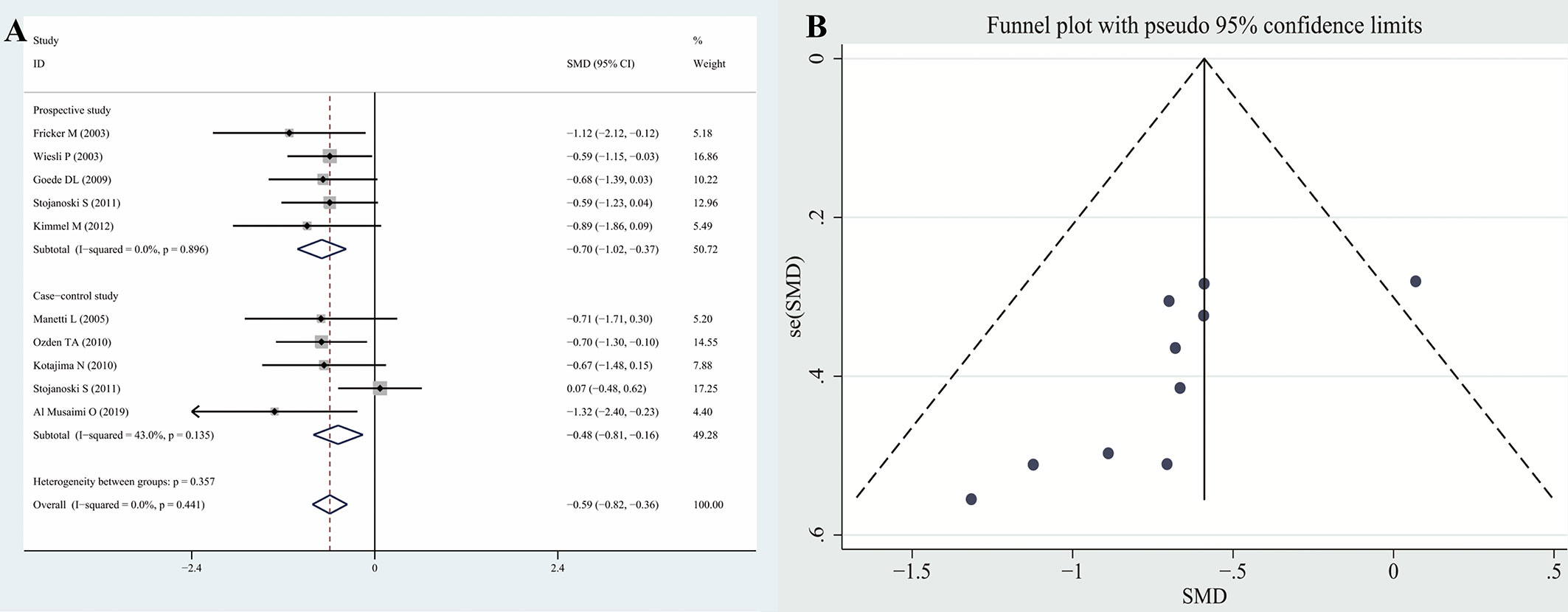
Figure 3 Forest plots and funnel plots of serum CysC in patients with hypothyroidism compared with controls. Diamond represents the pooled SMDs at 95% CI. (A) Forest plots; (B) Funnel plots. CysC, Cystatin C; SMD, standardized mean difference; CI, confidence interval.
A sensitivity analysis was performed to examine the influence of each study. We found no significant difference between the results of the sensitivity analysis and our previous estimates, indicating that our statistical results were relatively credible (Figure 4). Articles obtained from the databases were carefully and comprehensively searched. Egger’s test was also conducted to determine whether potential publication bias existed in the reviewed literature. While no publication bias was observed in the hyperthyroidism group (P > 0.05), some publication bias might have existed in the hypothyroidism group (P < 0.05). Using the approach recommended by the GRADE system, the certainty of the evidence for studies in the meta-analysis was evaluated as low or very low.
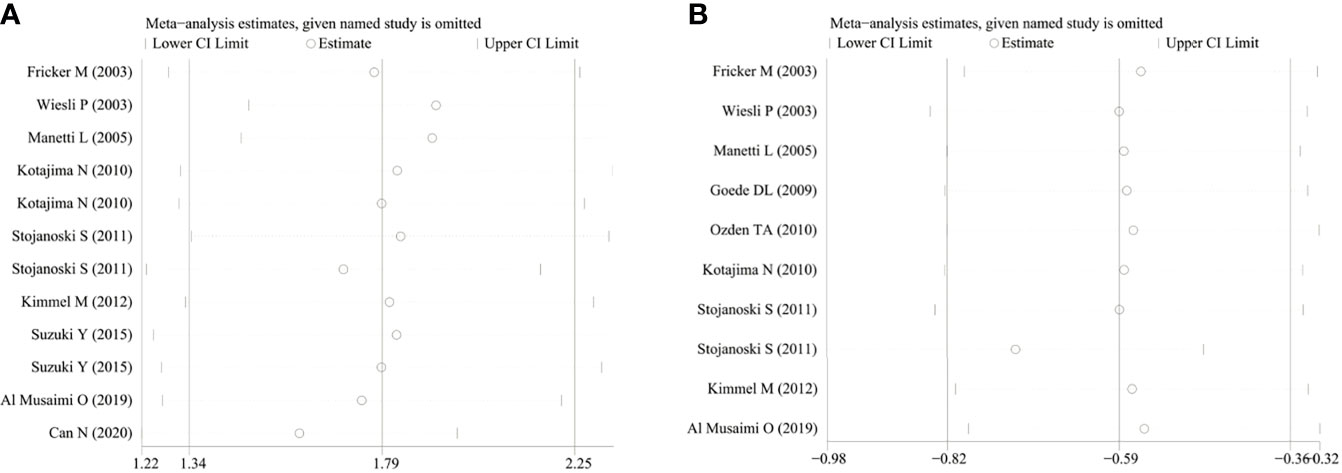
Figure 4 The sensitivity analysis results of serum CysC in patients with hyperthyroidism and hypothyroidism compared with controls. (A) Hyperthyroidism; (B) Hypothyroidism. CysC, Cystatin C.
This meta-analysis evaluated the serum CysC levels of patients with thyroid diseases. Although some studies have investigated the association between serum CysC levels and thyroid diseases, their results were inconsistent. In this meta-analysis, 11 independent studies were included and analyzed. We concluded that the serum CysC levels of patients with hyperthyroidism and those with hypothyroidism were significantly higher and lower than those of the controls, respectively. The treatment of thyroid diseases also significantly affected the serum CysC levels, making CysC a potentially effective marker for monitoring the treatment of thyroid diseases.
CysC is a nonglycosylated protein with 120 amino acid residues. CysC production is more stable than creatinine production and is not affected by inflammation, bilirubin, and triglycerides, as well as sex, age, muscle mass, or diet. CysC, owing to its small molecular weight and positive charge, can freely pass through the glomerular filtration membrane and is almost completely reabsorbed in the proximal convoluted tubules. After reabsorption, it is completely catabolized and no longer returns to the blood circulation. Further, CysC is not secreted by the renal tubules and its production rate in the tissue is constant (1, 25). The kidney is the only organ that clears CysC in circulation. Blood CysC levels are determined by glomerular filtration, and inter-individual differences are small. The difference between the highest value in the population and the normal average value was <3–4 standard deviations. CysC is a new index that can reflect GFR with high specificity, good accuracy, and sensitivity compared with the creatinine clearance rate. It is an ideal endogenous marker that reflects the changes in GFR (26, 27).
Fricker et al. reported that an increase in the thyroid hormone content in the blood of patients with hyperthyroidism can promote the synthesis of Na+ - K+ - ATPase in many cells of the body, increase the basal metabolic rate and oxygen consumption, accelerate the cell renewal rate/metabolic rate, and promote the secretion of CysC by nucleated cells, thereby accelerating the production rate of CysC. Under the condition of normal renal function, the increase in serum CysC levels in patients with hyperthyroidism is not caused by renal injury but is related to increased basal metabolic rate and oxygen consumption (15).
Studies have shown that the serum transforming growth factor-β1 (TGF-β1) levels are significantly increased in patients with Graves’ disease and that there is a positive correlation between TGF-β1 and thyroid hormone levels. In addition, TGF-β1 levels decreased in patients with Graves’ disease after treatment. Studies have also reported that serum TGF-β1 levels in patients with hypothyroidism were significantly decreased. TGF-β1 stimulates vascular smooth muscle cells to secrete CysC. In vivo, TGF-β1 stimulated the secretion of CysC and increased the expression of CysC mRNA in HepG2 cells. Notably, T3 stimulated Hep-G2 cells to produce CysC in a dose-dependent manner (19). TGF-β1 treatment has been shown to upregulate CysC transcription in mouse embryonic cells and 3T3-L1 fibroblasts (28–30). Schmid et al. used a T3-responsive osteoblast cell line to investigate whether T3 stimulates the production of CysC in vitro and reported that T3 increased the expression and accumulation of CysC mRNA in the culture medium in a dose- and time-dependent manner. It was considered that the increased production of CysC induced by T3 may be related to an increased demand for cell metabolism and proteolysis control (31).
In our study, we noted that even mild thyroid dysfunction (subclinical hyperthyroidism/hypothyroidism) affected the serum CysC levels of patients. Due to the limited number of reports (only one paper) on subclinical thyroid diseases, we could not perform subgroup analysis. Thus, more studies on serum CysC levels and subclinical thyroid diseases are warranted.
This meta-analysis firstly aimed to statistically evaluate serum CysC levels in patients with thyroid diseases. However, this study has some limitations. Due to the lack of case-control studies with a large sample population, most studies included in this meta-analysis were studies with a small sample population. Further, some studies did not use healthy controls controlled for body mass index. Different CysC detection methods were used among the studies, and the heterogeneity among studies on hyperthyroidism was high, partly due to different severities of hyperthyroidism being analyzed. These factors may have affected our results. Therefore, the results obtained herein should be interpreted cautiously, as further research is needed.
To the best of our knowledge, this meta-analysis is the first to evaluate serum CysC levels in patients with thyroid diseases. Our findings suggest that thyroid function affects serum CysC levels and that serum CysC may be an effective marker to monitor the treatment of thyroid diseases. More high-quality studies are needed to better support the association between serum CysC levels and thyroid diseases.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
XS designed the study. BS and XS searched databases and collected the data. HF and JX assessed the quality of the study. XS performed the analysis. HF and JX wrote the manuscript. All authors contributed to the article and approved the submitted version.
This research was financially supported by the Natural Science Foundation of Jiangsu Province (grant No. SBK2020040002).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Enago for English-language editing.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2021.766516/full#supplementary-material
Supplementary Table 1 | Preferred reporting items for systematic review and meta-analyses (PRISMA) checklist.
Supplementary Table 2 | Full electronic search strategy for Pubmed.
1. Abrahamson M, Olafsson I, Palsdottir A, Ulvsbäck M, Lundwall A, Jensson O, et al. Structure and Expression of the Human Cystatin C Gene. Biochem J (1990) 268:287–94. doi: 10.1042/bj2680287
2. Dharnidharka VR, Kwon C, Stevens G. Serum Cystatin C Is Superior to Serum Creatinine as a Marker of Kidney Function: A Meta-Analysis. Am J Kidney Dis (2002) 40(2):221–6. doi: 10.1053/ajkd.2002.34487
3. Laterza OF, Price CP, Scott MG. Cystatin C: An Improved Estimator of Glomerular Filtration Rate? Clin Chem (2002) 48(5):699–707. doi: 10.1093/clinchem/48.5.699
4. Bi M, Huang Z, Li P, Cheng C, Huang Y, Chen W. The Association Between Elevated Cystatin C Levels With Myocardial Infarction: A Meta-Analysis. Int J Clin Exp Med (2015) 8(11):20540–7.
5. Wang Y, Li W, Yang J, Zhang M, Tian CE, Ma M, et al. Association Between Cystatin C and the Risk of Ischemic Stroke: A Systematic Review and Meta-Analysis. J Mol Neurosci (2019) 69(3):444–9. doi: 10.1007/s12031-019-01373-1
6. Ma C, Duan C, Huang R, Tang H. Association of Circulating Cystatin C Levels With Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Arch Med Sci (2020) 16(3):648–56. doi: 10.5114/aoms.2019.83511
7. Chai L, Feng W, Zhai C, Shi W, Wang J, Yan X, et al. The Association Between Cystatin C and COPD: A Meta-Analysis and Systematic Review. BMC PULM Med (2020) 20(1):1–11. doi: 10.1186/s12890-020-01208-5
8. Simeoni M, Cerantonio A, Pastore I, Liguori R, Greco M, Foti D, et al. The Correct Renal Function Evaluation in Patients With Thyroid Dysfunction. J Endocrinol Invest (2016) 39(5):495–507. doi: 10.1007/s40618-015-0402-8
9. Wiesli P, Schwegler B, Spinas GA, Schmid C. Serum Cystatin C Is Sensitive to Small Changes in Thyroid Function. Clin Chim Acta (2003) 338(1-2):87–90. doi: 10.1016/j.cccn.2003.07.022
10. Ye Y, Gai X, Xie H, Jiao L, Zhang S. Impact of Thyroid Function on Serum Cystatin C and Estimated Glomerular Filtration Rate: A Cross-Sectional Study. Endocr Pract (2013) 19(3):397–403. doi: 10.4158/EP12282.OR
11. Suzuki Y, Matsushita K, Seimiya M, Yoshida T, Sawabe Y, Ogawa M, et al. Paradoxical Effects of Thyroid Function on Glomerular Filtration Rate Estimated From Serum Creatinine or Standardized Cystatin C in Patients With Japanese Graves’ Disease. Clin Chim Acta (2015) 451(Pt B):316–22. doi: 10.1016/j.cca.2015.10.018
12. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (Accessed 2014 Aug 5).
13. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Available at: http://www.cochrane-handbook.org (Accessed 2014 Aug).
14. Grading Quality of Evidence and Strength of Recommendations in Clinical Practice Guidelines. Part 1 of 3. An Overview of the GRADE Approach and Grading Quality of Evidence About Interventions – Pubmed [Internet]. (Accessed 2020 Jul 7).
15. Fricker M, Wiesli P, Brandle M, Schwegler B, Schmid C. Impact of Thyroid Dysfunction on Serum Cystatin C. Kidney Int (2003) 63(5):1944–7. doi: 10.1046/j.1523-1755.2003.00925.x
16. Manetti L, Pardini E, Genovesi M, Campomori A, Grasso L, Morselli LL, et al. Thyroid Function Differently Affects Serum Cystatin C and Creatinine Concentrations. J Endocrinol Invest (2005) 28(4):346–9. doi: 10.1007/BF03347201
17. Goede DL, Wiesli P, Brändle M, Bestmann L, Bernays RL, Zwimpfer C, et al. Effects of Thyroxine Replacement on Serum Creatinine and Cystatin C in Patients With Primary and Central Hypothyroidism. SWISS Med WKLY (2009) 139(23-24):339–44.
18. Özden TA. Effect of Hypo-and Euthyroid Status on Serum Cystatin C Levels-Original Article. J Clin Res Pediatr E (2010) 2(4):155–8. doi: 10.4274/jcrpe.v2i4.155
19. Kotajima N, Yanagawa Y, Aoki T, Tsunekawa K, Morimura T, Ogiwara T, et al. Influence of Thyroid Hormones and Transforming Growth Factor-Beta1 on Cystatin C Concentrations. J Int Med Res (2010) 38(4):1365–73. doi: 10.1177/147323001003800418
20. Stojanoski S, Gjorceva DP, Gruev T, Ristevska-Miceva S, Ristevska N. Impact of Thyroid Dysfunction on Serum Cystatin C, Serum Creatinine and Glomerular Filtration Rate. Macedonian J Med Sci (2011) 15; 4(1):25–30. doi: 10.4158/EP12282.OR
21. Kimmel M, Braun N, Alscher MD. Influence of Thyroid Function on Different Kidney Function Tests. Kidney Blood Pressure Res (2012) 35(1):9–17. doi: 10.1159/000329354
22. Suzuki Y, Matsushita K, Seimiya M, Yoshida T, Sawabe Y, Ogawa M, et al. Paradoxical Effects of Thyroid Function on Glomerular Filtration Rate Estimated From Serum Creatinine or Standardized Cystatin C in Patients With Japanese Graves’ Disease. Clin Chim Acta (2015) 451:316–22. doi: 10.1016/j.cca.2015.10.018
23. Al Musaimi O, Abu-Nawwas AH, Al Shaer D, Khaleel NY, Fawzi M. Influence of Age, Gender, Smoking, Diabetes, Thyroid and Cardiac Dysfunctions on Cystatin C Biomarker. Medicina Familia SEMERGEN (2019) 45(1):44–51. doi: 10.1016/j.semerg.2018.07.005
24. Can N, Ozsoy E, Kobat SG, Yusufoglu E, Ilhan N, Demir T. Serum Cystatin C Concentrations in Patients With Graves’ Ophthalmopathy. Korean J Ophthalmol (2020) 34(5):398–403. doi: 10.3341/kjo.2020.0006
25. Mussap M, Plebani M. Biochemistry and Clinical Role of Human Cystatin C. Crit Rev Clin Lab Sci (2004) 41:467–550. doi: 10.1080/10408360490504934
26. Coll E, Botey A, Alvarez L, Poch E, Quinto L, Saurina A, et al. Serum Cystatin C as a New Marker for Noninvasive Estimation of Glomerular Filtration Rate and as a Marker for Early Renal Impairment. Am J Kidney Dis (2000) 36:29–34. doi: 10.1053/ajkd.2000.8237
27. Astor BC, Levey AS, Stevens LA, Van Lente F, Selvin E, Coresh J. Method of Glomerular Filtration Rate Estimation Affects Prediction of Mortality Risk. J Am Soc Nephrol (2009) 20:2214–22. doi: 10.1681/ASN.2008090980
28. Solem M, Rawson C, Lindburg K, Barnes D. Transforming Growth Factor β Regulates Cystatin C in Serum-Free Mouse Embryo (SFME) Cells. Biochem Biophys Res Commun (1990) 172:945–51. doi: 10.1016/0006-291X(90)90767-H
29. Afonso S, Tovar C, Romagnano L, Babiarz B. Control and Expression of Cystatin C by Mouse Decidual Cultures. Mol Reprod Dev (2002) 61:155–163. doi: 10.1002/mrd.1142
30. Sokol JP, Schiemann WP. Cystatin C Antagonizes Transforming Growth Factor β Signaling in Normal and Cancer Cells. Mol Cancer Res (2004) 2:183–195.
Keywords: cystatin C, CysC, thyroid disease, systematic review, meta-analysis
Citation: Xin C, Xie J, Fan H, Sun X and Shi B (2021) Association Between Serum Cystatin C and Thyroid Diseases: A Systematic Review and Meta-Analysis. Front. Endocrinol. 12:766516. doi: 10.3389/fendo.2021.766516
Received: 29 August 2021; Accepted: 23 October 2021;
Published: 19 November 2021.
Edited by:
Marco António Campinho, Universidade do Algarve, PortugalReviewed by:
Sebastjan Bevc, Maribor University Medical Centre, SloveniaCopyright © 2021 Xin, Xie, Fan, Sun and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xin Sun, c3VueGluNzdAMTI2LmNvbQ==; Bimin Shi, c2hpYmltaW5AMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.