 Christoph Reiners1*
Christoph Reiners1* Rita Schneider1Tamara Platonova2Mikhail Fridman2Uwe Malzahn1Uwe Mäder1Alexis Vrachimis3†Tatiana Bogdanova4Jolanta Krajewska5Rossella Elisei6
Rita Schneider1Tamara Platonova2Mikhail Fridman2Uwe Malzahn1Uwe Mäder1Alexis Vrachimis3†Tatiana Bogdanova4Jolanta Krajewska5Rossella Elisei6 Fernanda Vaisman7
Fernanda Vaisman7 Jasna Mihailovic8
Jasna Mihailovic8 Gracinda Costa9
Gracinda Costa9 Valentina Drozd2
Valentina Drozd2- 1University Hospital, Würzburg, Germany
- 2The International Fund “Help for Patients With Radiation-Induced Thyroid Cancer ‘ARNICA”’, Minsk, Belarus
- 3University Hospital, Münster, Germany
- 4Institute of Endocrinology and Metabolism, Kiev, Ukraine
- 5M. Sklodowska-Curie National Research Institute of Oncology, Gliwice, Poland
- 6University Hospital, Pisa, Italy
- 7National Cancer Institute, Rio de Janeiro, Brazil
- 8Institute of Oncology Voijvodina, Sremska Kamenica, Serbia
- 9University Hospital, Coimbra, Portugal
Published studies on the risk of radiation-induced second primary malignancy (SPM) after radioiodine treatment (RAI) of differentiated thyroid cancer (DTC) refer mainly to patients treated as middle-aged or older adults and are not easily generalizable to those treated at a younger age. Here we review available literature on the risk of breast cancer as an SPM after RAI of DTC with a focus on females undergoing such treatment in childhood, adolescence, or young adulthood. Additionally, we report the results of a preliminary international survey of patient registries from academic tertiary referral centers specializing in pediatric DTC. The survey sought to evaluate the availability of sufficient patient data for a potential international multicenter observational case–control study of females with DTC given RAI at an early age. Our literature review identified a bi-directional association of DTC and breast cancer. The general breast cancer risk in adult DTC survivors is low, ~2%, slightly higher in females than in males, but presumably lower, not higher, in those diagnosed as children or adolescents than in those diagnosed at older ages. RAI presumably does not substantially influence breast cancer risk after DTC. However, data from patients given RAI at young ages are sparse and insufficient to make definitive conclusions regarding age dependence of the risk of breast cancer as a SPM after RAI of DTC. The preliminary analysis of data from 10 thyroid cancer registries worldwide, including altogether 6,449 patients given RAI for DTC and 1,116 controls, i.e., patients not given RAI, did not show a significant increase of breast cancer incidence after RAI. However, the numbers of cases and controls were insufficient to draw statistically reliable conclusions, and the proportion of those receiving RAI at the earliest ages was too low.In conclusion, a potential international multicenter study of female patients undergoing RAI of DTC as children, adolescents, or young adults, with a sufficient sample size, is feasible. However, breast cancer screening of a larger cohort of DTC patients is not unproblematic for ethical reasons, due to the likely, at most slightly, increased risk of breast cancer post-RAI and the expected ~10% false-positivity rate which potentially produced substantial “misdiagnosis.”
Introduction
Treatment of differentiated thyroid cancer (DTC) in childhood, adolescence, or early adulthood with surgery, radioiodine (iodine-131, I-131) therapy (RAI), and thyroid hormone replacement achieves 10-year survival rates of 95%, with relatively low recurrence rates of 10–30% (1). However, an excellent long-term survival may be partly offset by an increased risk for second primary malignancy (SPM) related to RAI or other causes.
According to a systematic review by Clement et al. (2), the risk for SPM is increased after RAI of DTC. For many years, the gastrointestinal tract (salivary glands, stomach, and colorectum), the genitourinary tract (kidneys and bladder), and the hematopoetic system (blood cells) have been considered to be at risk to develop SPM after RAI (2–4). However, a recent meta-analysis did not find an increased risk of solid cancers after RAI (5).
Since I-131 is concentrated by the sodium iodide symporter and that molecule is expressed in the mammary gland (6), the female breast may receive relevant radiation doses between 0.2 and 2 Gy from repeated courses, with cumulative activities of 1–15 GBq (7). Based on the recently introduced radiation risk assessment tool of the United States National Cancer Institute, a dose of 2 Gy to the breast of a 10-year-old girl hypothetically doubles her lifetime risk for breast cancer, whereas in a 50-year-old woman, the risk increases only by 20% (8).
Objective and Scope
Published studies on the risk of radiation-induced SPM, including breast cancer in DTC, refer mainly to middle-aged and older adult survivors. These studies are not easily generalizable to those treated as children, adolescents, or young adults since the patients who are still growing are more sensitive to radiation, and the patients treated earlier in life may have a longer potential latency period. Therefore, we here (1) review available literature on the risk of breast cancer as an SPM (A) independent of the type of treatment of RAI and (B) after RAI of DTC, with a focus on young females, and (2) report the results of our preliminary international multi-registry survey to evaluate the availability of patient data for a sufficiently powered multicenter international study of DTC patients given RAI as children, adolescents, or young adults. This research project was sponsored by the German Federal Office for Radiation Protection.
Review of the Literature
Methods
The literature included in the analysis was identified by two independent reviewers (VD and RS), principally using an automated literature search for English language papers published from 1984 to 2018 regarding breast cancer after RAI of DTC. The search was carried out using the online Medline (PubMed), Cochrane, and Embase databases. The main search terms were “thyroid” OR “breast” OR “mamma” AND “cancer” OR “malignancy” OR “carcinoma” OR “tumor” AND “second primary malignancy” AND “radioiodine therapy.” Besides the automated search, a manual search for additional relevant publications was made of the bibliographies of the papers identified automatically.
Systematic reviews, meta-analyses, cohort studies, and case–control studies were included. Case reports, single-center studies with small databases or study samples (N < 500), narrative reviews of the literature, editorials, and letters to the editor were excluded. Also excluded were publications regarding studies not differentiating between synchronous and metachronous SPMs.
From the publications fulfilling the inclusion criteria, the following information (if available) were extracted:
• First author, date, country
• Setting (e.g., hospital registry and population-based registry), single-center or multicenter design
• Duration of the study and of the follow-up time
• Study sample characteristics (number, gender, and age of patients/controls), exclusion criteria in the study
• DTC characteristics (histology and TNM stage)
• Surgery, RAI yes/no, cumulative I-131 activity as a surrogate for radiation dose
• SPM (of all kinds/breast cancer) before/after RAI
• Latency period, age dependency, dose dependency of SPM, and breast cancer incidence (correlation with I-131 activity)
• Risk estimates for secondary breast cancer after DTC (independent of treatment) and for secondary breast cancer after RAI of DTC, expressed as one or more of the following:
◦ absolute number
◦ excess absolute risk
◦ excess relative risk
◦ observed/expected incidence (O/E)
◦ odds ratio
◦ relative risk
◦ standardized incidence ratio (SIR)
◦ incidence rate ratio
◦ hazard ratio (HR)
with corresponding 95% confidence interval (CI).
Because of the heterogeneity and the variable design of the studies in the literature, only a qualitative and not a pooled analysis was performed.
Results
Publications Included
Using the search strategy described above, a total of 233 citations were found (Figure 1), 169 of which were excluded because the publications were unrelated to DTC, represented duplicate publication of the same studies, or were otherwise deemed not to be relevant. In addition to the 64 publications located through the automated search that were deemed to be of potential interest based on their abstracts, a manual search considering the bibliographies of the review articles retrieved 35 citations deemed to be of potential interest based on their abstracts. Thus, 99 full-text articles were read, of which 59 were excluded for the following reasons: small number of clinical observations by single centers (n = 12), case reports (n = 11), letters to the editor (n = 4), and unclear specification if the breast cancer was diagnosed before or after DTC (n = 32) (the papers could be excluded on more than one grounds).
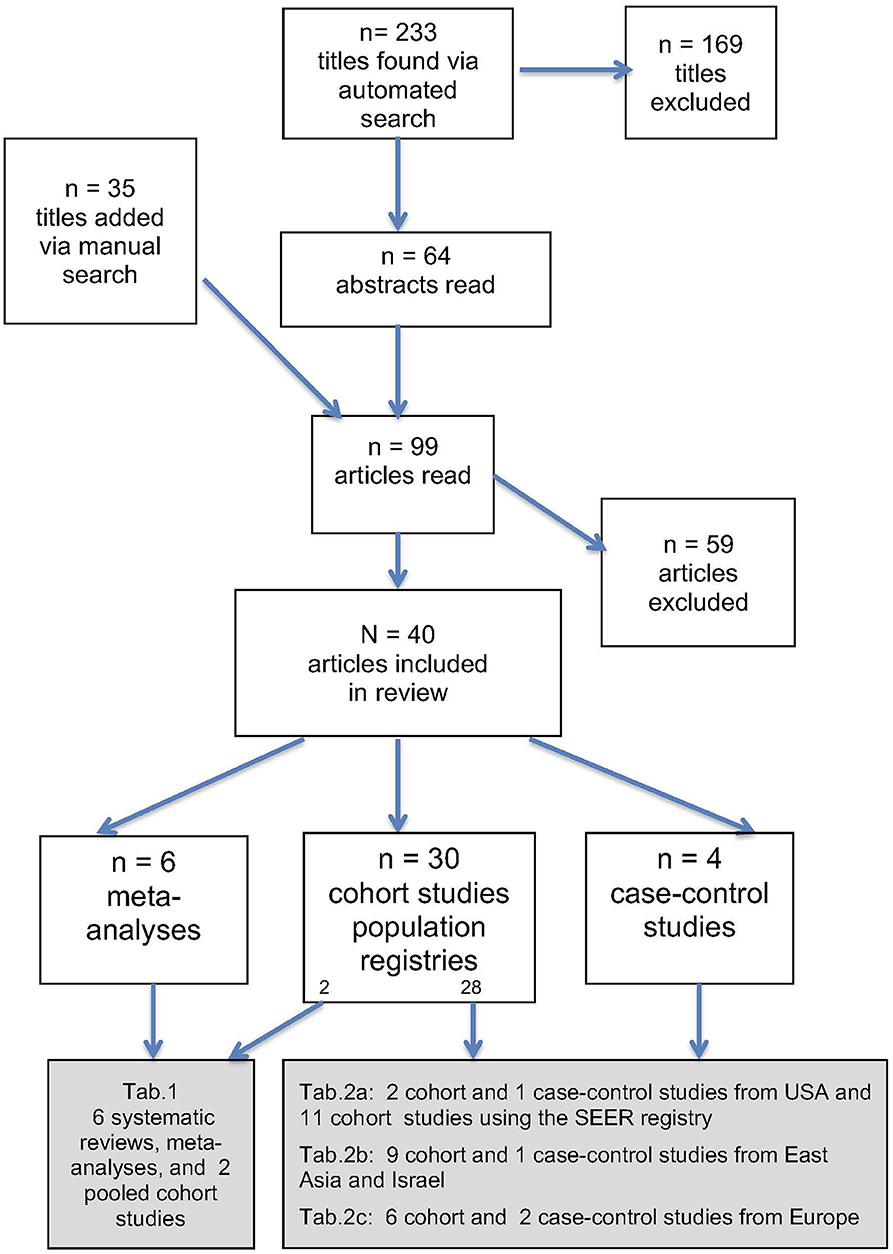
Figure 1. Flow diagram describing the literature search process.
Thus, altogether 40 publications were included in our analysis (Figure 1); they are cited and summarized in four tables. The main criterion for the assignment of a publication to a particular table was the type of study: Table 1—systematic reviews and meta-analyses and Table 2—cohort or case–control studies. Since the majority of the studies analyzed were large single-center cohort or case–control studies, resulting in a large number of publications, such articles were assigned to “sub-tables” according to the region of origin (Table 2A—USA, Table 2B—East Asia and Israel, and Table 2C—Europe). Within the tables, the studies are arranged according (1) to country of origin and (2) year of publication (chronological order from earliest to most recent).
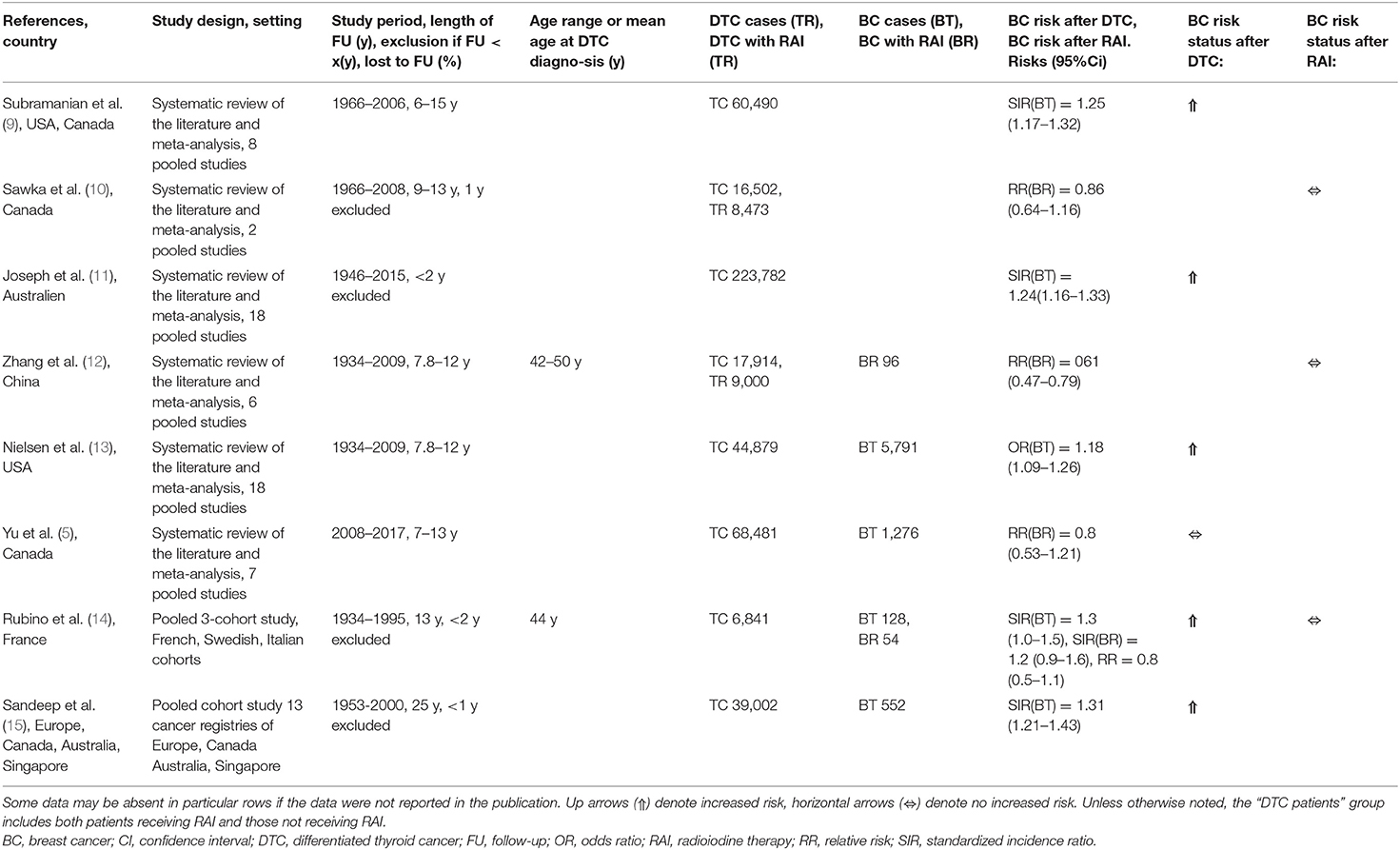
Table 1. Breast cancer risk in DTC survivors and/or DTC survivors given RAI: systematic reviews, meta-analyses, and internationally pooled cohort studies.
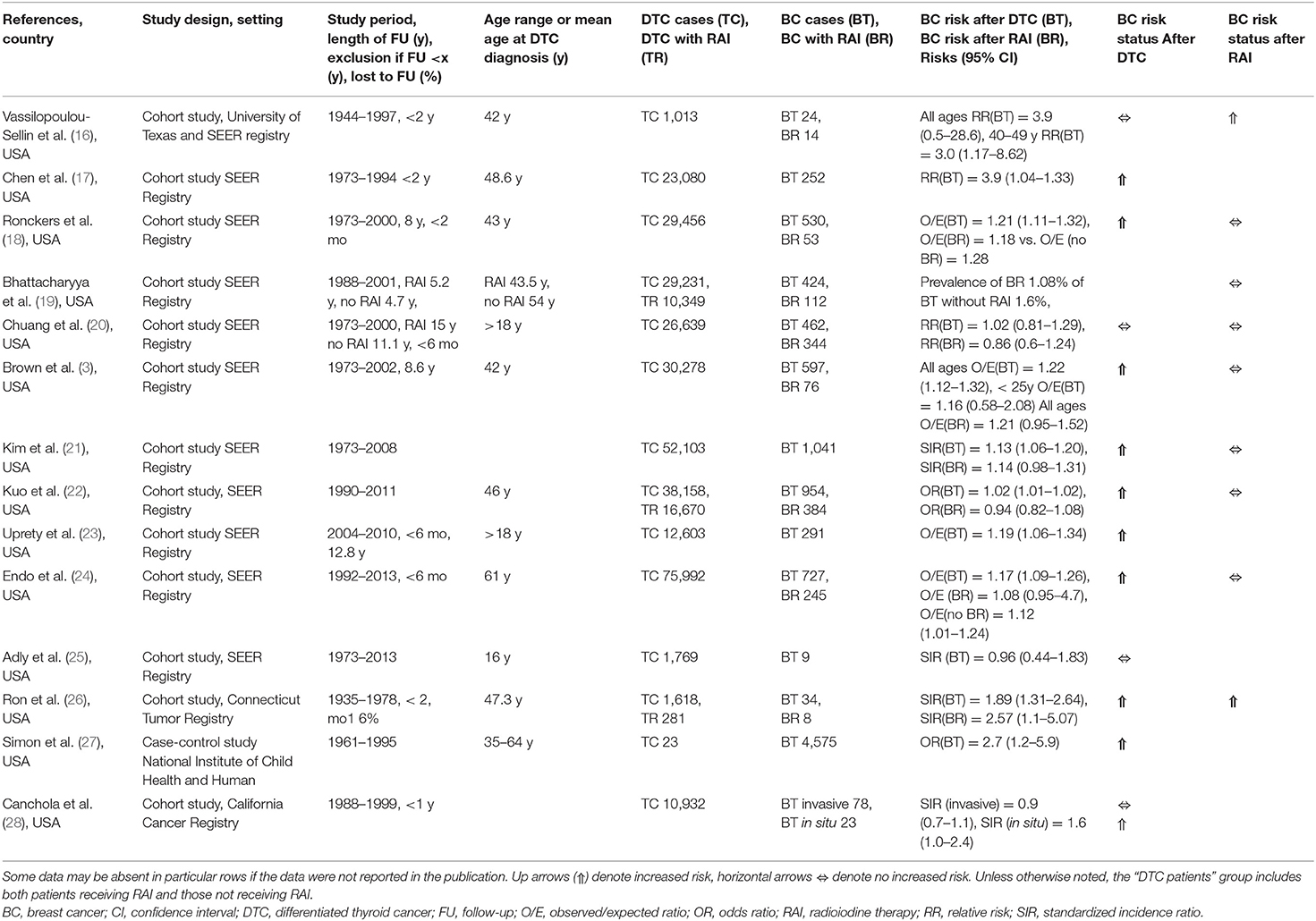
Table 2A. Breast cancer risk in DTC survivors and/or DTC survivors given RAI: cohort and case-control studies from USA.
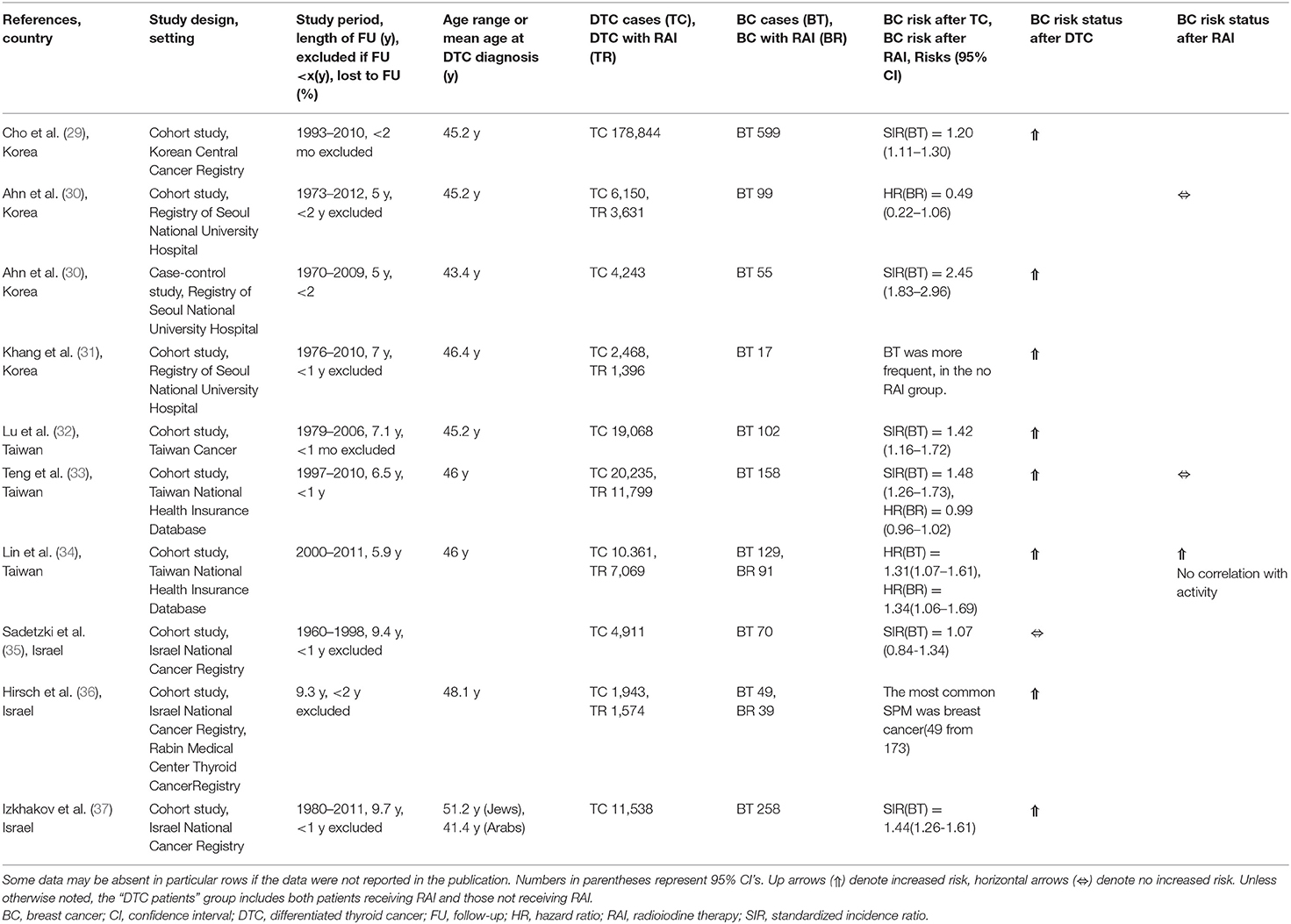
Table 2B. Breast cancer risk in DTC survivors and/or DTC survivors given RAI: cohort and case-control studies from Asia.
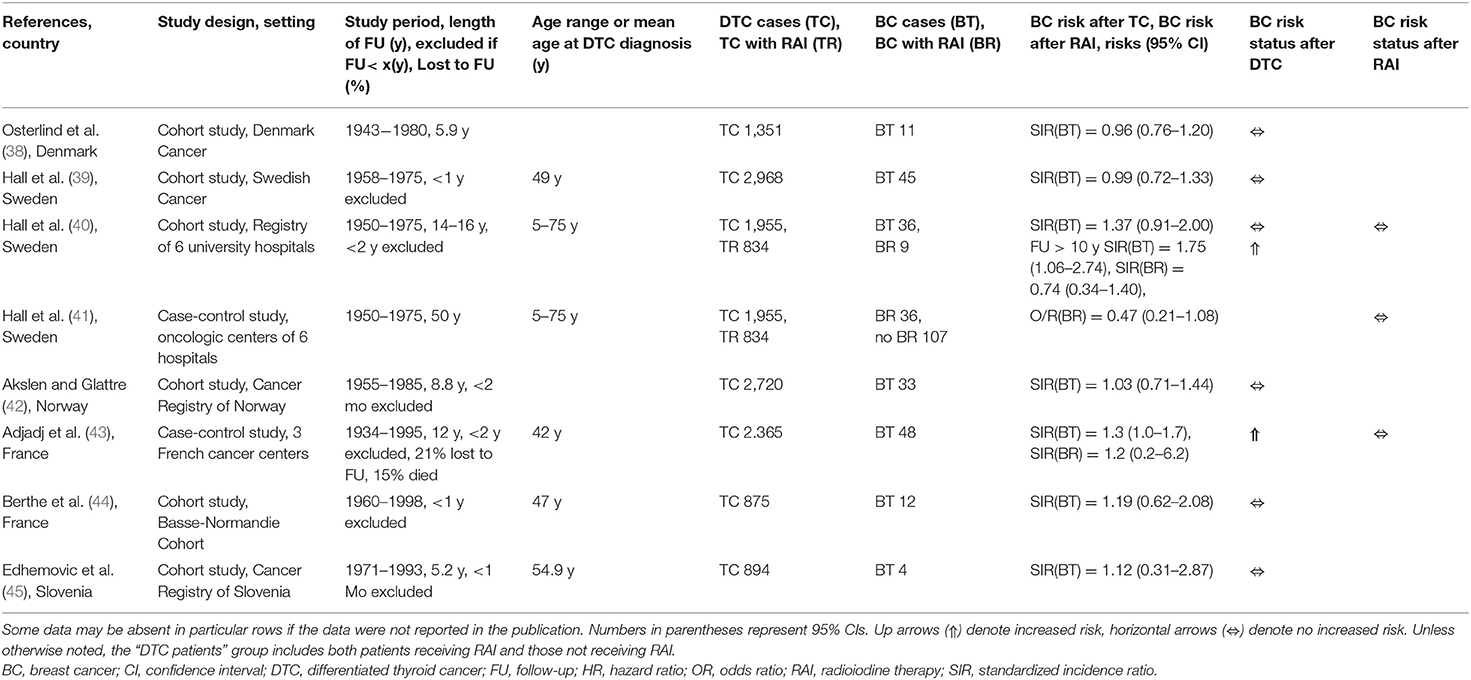
Table 2C. Breast cancer risk in DTC survivors and/or DTC survivors given RAI: cohort and case-control studies from Europe.
Specifically, Table 1 is a list of the results of six systematic reviews and meta-analyses. In addition, two large multinational pooled cohort studies are shown.
The majority of the included published studies (n = 28) were cohort studies of large population-based tumor registries (Tables 2A–2C). The US Surveillance, Epidemiology, and End Results (SEER) Registry (Table 2A) served as the database for 11 publications. Besides the studies using the SEER registry, Table 2A presents three other American analyses: one single-center cohort study, one cohort study analyzing the SEER database plus a local registry, and one case–control study.
Seven cohort studies (Table 2B) from East Asia also used large registries, e.g., the databases of the Korean Central Cancer Registry, the Taiwanese National Health Insurance, and the Taiwanese National Cancer Registry. Three cohort studies (Table 2B) analyzed the Israel National Cancer Registry. From Europe (Table 2C), six large cohort studies were found.
Finally, four case–control studies (Tables 2B, 2C) were included in our review, the largest of which included more than 4,000 cases (46).
A considerable proportion of the articles tried to take the patients' age at the diagnosis of DTC into consideration. However, only two studies focused on the risk of breast cancer after RAI for DTC in children and adolescents (3, 25).
It should be mentioned that, of 40 studies, 22 dealt with the general risk of breast cancer after DTC, not taking into account the form of treatment. Fourteen of the 40 studies dealt both with the general risk and the RAI-dependent risk. Conversely, four studies considered only the risk of breast cancer after treatment of DTC with RAI.
Risk of Breast Cancer After DTC (Independent of Therapy)
Three large meta-analyses and two large pooled cohort studies (Table 1) revealed a generally increased risk for breast cancer as an SPM in DTC patients, too, with significant SIRs of about 1.2 (9, 11, 13–15). Interestingly, only one of the meta-analyses gave an indication to exclude such an effect (5).
Eight of the 12 cohort studies examining the SEER registry and other registries from the USA (Table 2A) also described significant, if weak, increases of breast cancer risk in DTC survivors, with SIRs of ca. 1.2 or O/E values of ca. 1.2 (3, 17, 18, 21–24, 26).
On the other hand, three studies on the SEER registry (16, 20, 25) and two other cohort studies from the USA (25, 28) did not reveal such increases of breast cancer risk in DTC survivors (Table 2A).
Slightly higher, and again significant, increases of breast cancer risk in patients after a diagnosis of DTC have been described by nine of 17 cohort and case–control studies from East Asia, Israel, and Europe (Tables 2B, 2C) (29, 31–34, 36, 37, 43, 46). The SIRs in these studies ranged between 1.3 and 1.5, with the exception of 2.5 in patients from a Korean registry (Table 2B) (46).
On the contrary, seven of the same 17 studies (Tables 2B, 2C), including one from Israel (35), four from Scandinavia (38–40, 42) as well as two from France and Slovenia (44, 45), did not show an increased general risk for breast cancer in DTC patients. Hall et al. (40) did find such an association, but only in their subgroup at follow-up of >10 years (Table 2C).
Studies looking at age as a risk modifier and comparing subgroups of adult patients suggested no clear age dependency of SIRs (Table 2A) (3, 16, 25). Brown et al. (3) compared the risk of breast cancer in two groups of relatively young DTC survivors, those younger than 25 years of age and those 25–49 years of age, respectively (Table 2A). The authors only found a significantly increased risk for breast cancer in the older group. A similar observation was made by Vassilopoulou-Sellin et al. (16), who found an increased risk for breast cancer in women ages 40–49 years, but not in younger patients (Table 2A). Most interestingly for our survey regarding age-related risks, the only study specifically addressing young patients, an analysis of the SEER database performed by Adly et al. (25), did not find an increased risk for breast cancer in patients younger than age 20 years at the time of DTC diagnosis and who were followed up for up to 40 years (Table 2A).
Few studies have investigated the latency times between diagnosis of DTC and detection of breast cancer. The above-mentioned study of the Korean National University Hospital, Seoul, database with the highest SIR, 2.5 (Table 2B) (46), reported in patients older than 30 years a mean latency time between diagnoses of DTC and breast cancer of 6.6 (minimum–maximum, 3.3–7.8) years. In patients diagnosed with DTC when younger than age 30 years, the mean latency time was considerably longer, 17.9 (minimum–maximum, 13.9–20.4) years.
Studies Comparing Breast Cancer Risk in Patients With DTC Receiving vs. Not Receiving RAI
The first cohort study describing an increased risk for breast cancer after DTC, that of Ron et al. (26), already focused on radiation as a risk factor for the former malignancy and reported a significantly increased SIR of 2.6 after radiation therapy (Table 2A). However, in the study of Ron et al. (26), the group of patients with radiation treatment was small (n = 8) and the type of treatment (percutaneous radiation therapy, RAI) was not specified.
On the contrary, two meta-analyses and one large pooled cohort study (Table 1) comparing the risk of breast cancer as an SPM in DTC patients given or not given RAI did not find an increased risk after RAI (10, 12, 14).
The absence of an association between RAI of DTC and breast cancer was confirmed by all seven studies on the risk of breast cancer after such treatment upon examining the US SEER Registry (Table 2A) (3, 18–22, 24). The same conclusions were drawn in five of six studies in other countries, e.g., Korea and Taiwan (Table 2B) (30, 33), the Scandinavian nations (40, 41), and France (Table 2C) (43).
In detail, Ahn et al. (30) noted that the risk of breast cancer was not associated with RAI (Table 2B); even for relatively high cumulative activities of ≥4.4 GBq, no effect was demonstrated. Lin et al. (34) showed that there was a small increase of breast cancer risk in DTC patients post-RAI (Table 2B), but not as high as that associated with DTC per se. Most importantly, in patients receiving cumulative activities of >4.4 GBq in comparison to patients receiving <4.4 GBq, the risk for breast cancer was not increased.
Brown et al. (3) did not find a correlation with RAI in any age group or when comparing breast cancer risk in two subgroups of relatively young patients after DTC—those <25 years old vs. those 25–49 years of age, respectively (Table 2A). Of interest is that Vassilopoulou-Sellin et al. (16) found, independent of RAI, an increased risk for breast cancer in women aged 40–49, but not in younger patients (Table 2A).
Adly et al. (25) also analyzed the SEER Registry data but focused on young patients (Table 2A). These investigators concluded that the overall risk of all kinds of SPM was significantly increased (SIR 1.5; 95%CI, 1.08–1.98) in patients undergoing RAI for DTC, being higher in females and White patients. Additionally, the cumulative incidence of all kinds of SPM after RAI of DTC in children appeared to increase steadily with survival after the primary treatment. The overall risk of SPM in patients with RAI was found to be significantly higher than expected compared to the risk in the general population. Based on this study, the pediatric thyroid cancer survivors are at an increased risk of developing SPM of the organs highly exposed to radiation by RAI: salivary glands, gums, and other parts of the mouth, the stomach, as well as the kidneys. By contrast, a significant increase of breast cancer as SPM in patients given RAI as children was not observed (SIR 0.96; 95%CI, 0.44–1.83).
International Multi-registry Survey
Participating Registries and Study Design
The second part of this report addresses a survey of patient registries from institutions known by the authors to specialize in treating children and adolescents with DTC. This preliminary study evaluated the availability of sufficient patient data to conduct an adequately powered international multicenter observational case–control study regarding breast cancer risk in female DTC survivors who were treated with RAI at a young age. Altogether eight academic tertiary referral centers from Germany, Ukraine, Poland, Italy, Brazil, Serbia, and Portugal agreed to participate. In addition, the German-Belarusian Foundation “ARNICA” contributed two separate datasets, one from their registry and the other from a dedicated smaller database which was set up for a “pilot study” that sought to test the feasibility of a multicenter international study on breast cancer risk in DTC survivors (Drozd et al., submitted). The nine institutions participating in the registry survey were:
• Foundation “ARNICA,” Minsk, Belarus (feasibility study sample and routine registry)
• Institute of Endocrinology and Metabolism, Kiev, Ukraine
• Instituto Nacional do Cancer—INCA, Rio de Janeiro, Brazil
• Institute of Oncology Vojvodina, Department of Nuclear Medicine, Sremska Kamenica, Serbia
• Department of Nuclear Medicine, University Hospital, Coimbra, Portugal
• Department of Nuclear Medicine, University Hospital, Münster, Germany
• Department of Endocrinology, University Hospital, Pisa, Italy
• Clinic of Nuclear Medicine and Endocrine Tumors, M. Sklodowska-Curie Memorial Cancer Center and Institute of Oncology, Gliwice, Poland
• Department of Nuclear Medicine, University Hospital, Würzburg, Germany
In the registry survey, in 2014–2015, the participating centers answered questionnaires requesting the most relevant information regarding breast cancer in female survivors of DTC, particularly those receiving RAI at an early age. These queries included the database's total number of female DTC survivors diagnosed during childhood or adolescence with or without a history of RAI, the percentage of DTC survivors who were ages <18 or <40 years of age at the time of the primary treatment, the cumulative activity of I-131 administered for RAI, and the follow-up regimen after RAI. Queries were also made regarding the incidence of SPM, specifically breast cancer, both before and after the DTC diagnosis. The registry study was performed with anonymous, aggregated patient data.
The pilot observational cohort study alluded to above was performed in collaboration with the Foundation “ARNICA” and other organizations in Belarus and Germany in 2016–2017 (Drozd et al., submitted). In this feasibility study, selected female patients given RAI for their DTC in childhood or adolescence and control patients not given RAI underwent clinical, imaging, and laboratory examinations as part of a screening program for breast cancer. As noted previously, the dedicated database that was created for the pilot study also was analyzed in the present study. To avoid duplicate publication, any patients in the dedicated database who also were in the Foundation “ARNICA” Registry were excluded from all analyses of the latter.
Number and Origin of Patients and Controls
Tables 3A, 3B show the key aggregated data for each of the nine centers and 10 databases included in our survey. The cohorts comprised altogether 7,565 female DTC survivors given RAI (“RAI patients,” n = 6,449) or not given RAI (“controls”, n = 1,116). The number of RAI patients per institution varied considerably from 15 to 1,644 and the number of controls from 0 to 419.
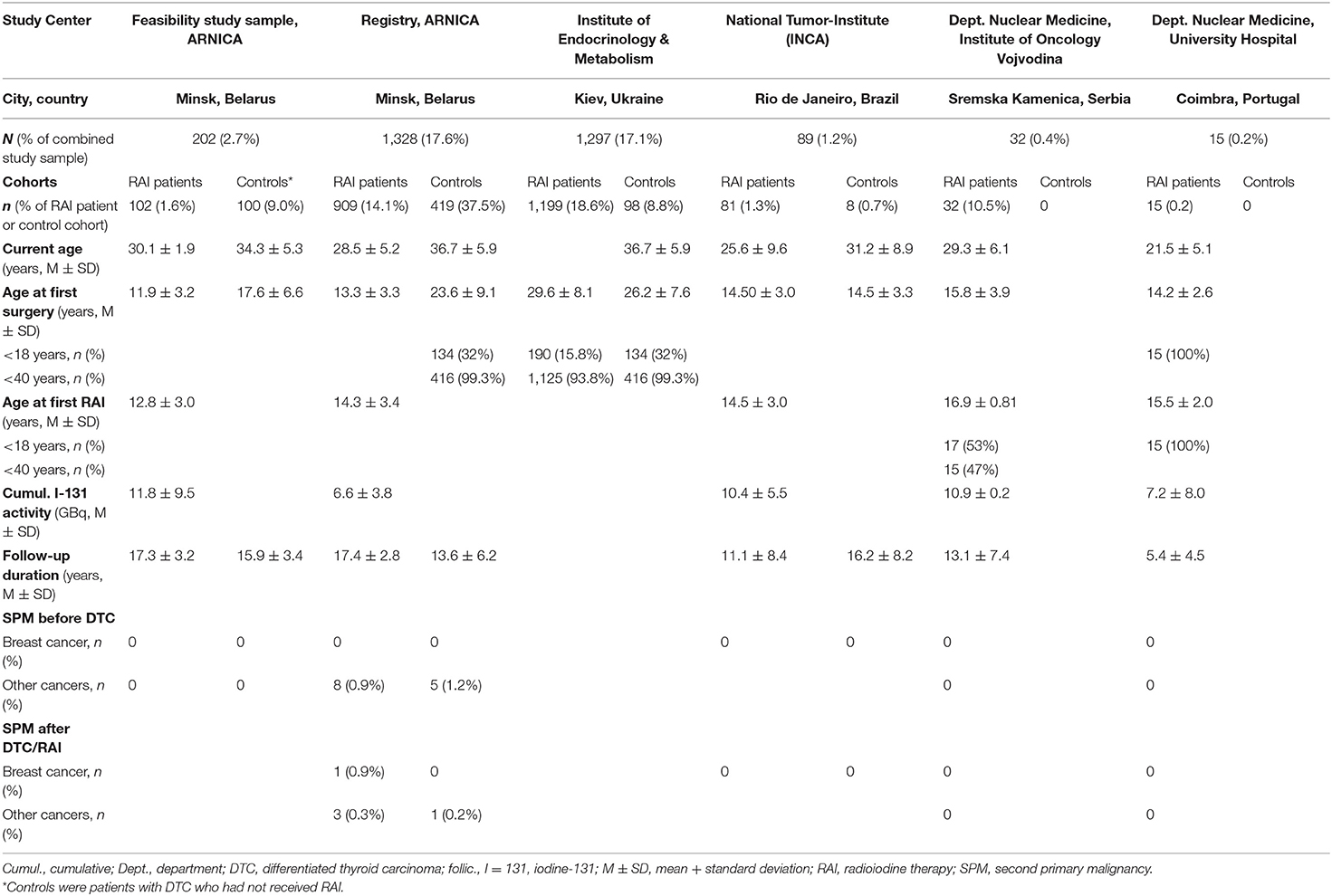
Table 3A. Registry survey: RAI patient and control cohort characteristics by center - young age groups.
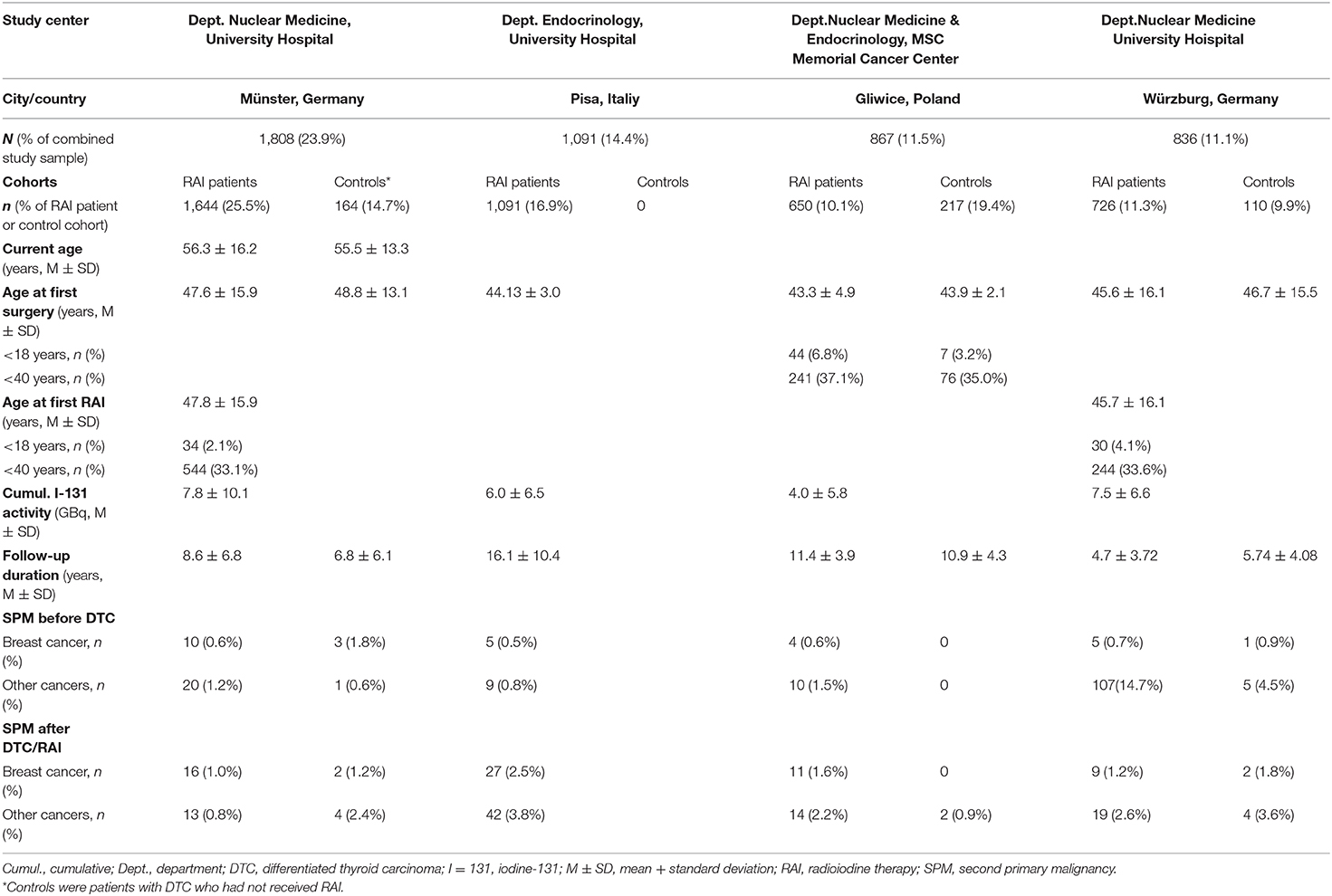
Table 3B. Registry survey: RAI patient and control cohort characteristics by center - all age groups.
The three largest groups of RAI patients, with more than 1,000 cases each, were contributed by the participating centers in Münster, Kiev, and Pisa. By contrast, by far the largest “no RAI” control group was provided by the Foundation “ARNICA,” Minsk, with a total of more than 500 controls (pilot study database plus registry). Table 3A is firstly a list of the three cohorts from Minsk and Kiev, which included a considerable proportion of young patients who developed DTC after the Chernobyl reactor accident in 1986 (1, 47).
Cohort Characteristics
It is apparent from Tables 3A, 3B that not all information was provided by all centers. However, the data supplied seemed to suffice to answer the survey's most important questions about the number and the main characteristics of the patients/survivors under observation.
Age Distribution
The data in Tables 3A, 3B are listed according to the patients' and the controls' ages at the time of the first treatment (surgery and/or RAI). Table 3A shows the young patient groups from five centers, who were between 12 and 16 years of age at the time of their initial treatment. Only the patients and the controls from Kiev were older, with mean ages of 26–30 years. However, because the Kiev cohorts included 16% of patients and 32% of controls not older than 18 years, we present their data in Table 3A, too, directly adjacent to the data from Minsk.
The cohorts from the four other centers (Table 3B), which together contributed approximately two-thirds of the RAI patients (4,110/6,449), mirrored the typical age distribution for patients with DTC, with mean ages at surgery/first RAI between 43 and 48 years.
Cumulative I-131 Activity
Except for the cohort from Kiev, all centers reported their cumulative activity of I-131 (in GBq) administered for RAI (Tables 3A, 3B). The mean cumulative activities of the centers in Minsk (registry), Würzburg, Münster, and Coimbra ranged between 6.0 and 10.0 GBq, whereas the highest mean cumulative activities, >10–12 GBq, were applied in patients from Minsk (pilot study sample) as well as in Rio de Janeiro and Sremska Kamenica. The relatively high cumulative activities can be explained by the young age of the patient cohorts from Belarus, Brazil, and Serbia. That demographic characteristic presumably corresponded to a relatively aggressive disease and hence to high rates of nodal or distant metastases or both, requiring a greater I-131 activity to be effectively treated.
Duration of Follow-Up
Eight of the nine centers (Tables 3A, 3B) provided information about the mean duration of follow-up after RAI in RAI patients and after surgery in controls (when available). On average, the centers in Minsk and Pisa had the longest mean follow-up times, slightly over 15 years. The mean follow-up times of the centers in Gliwice, Rio de Janeiro, and Sremska Kamenica ranged between 11 and 13 years. The shortest follow-up times were reported from Münster, with about 9 years, and Würzburg and Coimbra, with about 5 years.
Second Primary Malignancies
Again, eight of the nine centers provided data about SPM and breast cancer before and after the diagnosis of DTC (Tables 3A, 3B). There was considerable inhomogeneity of the data reported, which can be explained by the age distribution of the different cohorts. In the very young cohorts from Minsk (pilot study sample), Rio de Janeiro, Sremska Kamenica, and Coimbra, no breast cancer cases were reported in patients or controls. The relatively large cohorts of patients (n = 909) and controls (n = 419) of the Minsk registry included a low number of breast cancer cases, eight and five, respectively, before the diagnosis of DTC. After the DTC diagnosis, there was one additional case of breast cancer and three additional cases of other SPM in the RAI patient group as compared to no case of breast cancer and one case of another SPM in the control group.
The rates of SPM and breast cancer were higher in the much older cohorts from Würzburg, Münster, Gliwice, and Pisa. The rates before and after the diagnosis of DTC reported by the latter three centers were very similar, ranging between 0.5 and 2.5% (median, 0.9%) for breast cancer and 0.6–4.5% (median, 1.9%) for SPM other than breast cancer. The exceptionally high rate of other malignancies before DTC in the Würzburg cohort may be explained, at least partially, by detection bias due to the existence of a comprehensive local clinical cancer registry and a follow-up program. In that cohort, systematic differences in the cumulative incidences of breast cancer and other SPM between RAI patients and controls were not recognizable.
Discussion
Literature Review
Breast Cancer Risk in Differentiated Thyroid Cancer Patients Generally Increased, Influence of RAI Questionable
In a comprehensive systematic review and meta-analysis, Nielsen et al. (13) investigated the relationship between breast cancer and DTC. Interestingly, these authors, in line with earlier investigators (17, 48), described a bi-directional association, meaning that the risk of breast cancer was increased in patients with DTC and vice versa.
The majority of studies addressing this issue that are referenced here (22/34) indicate that there is a generally increased risk for breast cancer after diagnosis of DTC, independent of therapy. This observation was reflected in five of six systematic reviews, meta-analyses, and pooled studies (Table 1). The observation also was echoed in eight of 12 cohort studies using the SEER registry or other registries from the USA (Table 2A) and nine of 16 studies analyzing other registries (Tables 2B, 2C).
In the general population of the USA, breast cancer risk in women below age 45 years corresponds to approximately one case in 87, or 1.2% (49). To give a rough estimate of the risk in DTC survivors, a SIR of 1.5, the maximum value for 90% of the studies listed in Table 1, would mean that, with the diagnosis of DTC, the general risk of 1.2% could be increased by 50%, to ~1.8%, in women younger than 45 years of age.
However, the only study specifically focusing on children and adolescents younger than 20 years old does not suggest an increased breast cancer risk in patients with DTC (25). There is some indication that the latency times for breast cancer after DTC in young patients are much longer than in adults, often lasting 20 years or more, so that the studies examining this risk have to focus on long observation times (30).
Beyond the generally increased risk for breast cancer in DTC survivors independent of treatment, a history of RAI seems not to have any additional influence on this risk (Tables 1, 2A, 2C), based on published findings of all SEER studies, all meta-analyses, and nearly all cohort studies from a variety of countries. There are two exceptions describing an increased risk in cohorts after RAI, but correlations of the degree of risk with the therapeutic activity of I-131 were not found (26, 34). Two additional studies examined the possibility of a higher risk of breast cancer in young patients given RAI, which was not confirmed (3, 16).
Assessing the hypothesis of a generally increased risk for SPMs other than breast cancer in DTC patients/survivors was not an objective of the present study. However, in young (as well as adult) DTC patients after RAI, a generally increased risk for SPM seems to exist, specifically in organs and tissues relatively highly irradiated by RAI, e.g., salivary glands, gums, and other parts of the mouth, the stomach, and the kidneys (25).
Limitations and Weaknesses of Published Studies
Concerning the risk of breast cancer in DTC survivors given RAI at a young age—the original focus of this review—data are inconclusive for many reasons. A general problem of critically reviewing publications from, e.g., tumor registries is that non-independent data sets from identical registries are analyzed and published repeatedly. This plays an important role in the context of our review because 11 of 40 studies utilized the SEER registry and, similarly, three studies from Korea, two studies from Taiwan, three studies from Israel, and two studies from Sweden all refer to the same respective databases from those countries (Tables 2A, 2C). As expected, the systematic reviews and the meta-analyses used these same databases, too. To give an example, the six such studies cited here (Table 1) in five cases include patients from Hall et al. (39–41), in four cases include those of Rubino et al. (14), and in three cases each were the samples of Adjadj et al. (43), Berthe et al. (44), and Brown et al. (3).
Generally, the risk for breast cancer in DTC patients independent of therapy may be overestimated since the samples in 36 studies on the general risk of breast cancer in DTC patients included a large proportion of patients who were treated with RAI. Therefore, the studies' estimates of breast cancer risk in “all DTC survivors” might be conservatively high—because any increased risk due to RAI would materially elevate risk in the overall group.
Detection bias is possibly the most relevant limitation for most of the studies published since patients with a cancer diagnosis tend to participate more strictly in cancer screening programs, e.g., for breast cancer. Detection bias, by the way, may be the cause for the surprisingly high rate, 14.7%, of SPM other than breast cancer before the diagnosis of DTC in the Würzburg registry. Another limitation of the literature is that the published studies often did not differentiate between synchronous and metachronous SPMs; indeed that is one reason why more than 30 papers were excluded from this literature review.
In addition, when comparing DTC patients after RAI with DTC controls without a history of that treatment, selection may have introduced a relevant bias. That is because the indication for RAI depends on tumor stage, and RAI usually is not performed in patients with the frequently favorable stage pT1N0M0 (50). Conversely, patients treated with RAI tend to suffer from more advanced DTC, and this propensity for more aggressive malignancy may also be reflected in a predisposition for SPM such as breast cancer.
Only one case–control study (28) investigated the risk of breast carcinoma in situ vs. invasive breast cancer in DTC patients, separately describing such an increased risk for carcinoma in situ only (Table 2A).
Latency times between radiation exposure and manifestation of solid cancers tend to require a minimum of 4–5 years, with the consequence that SPM presenting earlier probably is not radiation-induced. In some studies that we evaluated, the patients were excluded if the SPM appeared within a month, several months, or even longer periods of up to 2 years after the diagnosis of DTC—which may be still too short an exclusion threshold.
On the other hand, maximum latency times for radiation-induced SPM may reach up to 30–40 years after treatment. The studies analyzed here had mostly relatively short mean observation times of <10 years (n = 12 studies; median, 7 years) and less often long follow-up times of 10–20 years (n = 7 studies, median 12 years). According to the American Thyroid Association's “Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer,” the minimum follow-up time for studies on outcomes and long-term side effects of DTC therapy in children and adolescents should be at least 10 years (50).
A severe drawback in the context of potentially RAI-induced breast cancer in DTC patients is that data about the therapeutic activity of I-131 (in mCi or GBq) are mostly not reported. Moreover, this activity is merely a surrogate for the radiation dose to breast tissue (in Gy), which only can be determined by individual measurements of uptake and effective half-time of I-131 in the body and the breast specifically. Regarding radiation exposure in general, a history of frequent diagnostic radiological examinations or accidental irradiation (e.g., in the case of Chernobyl) may play an important role, confounding the interpretation of the impact of RAI.
Nielsen et al. (13) discussed possible confounders influencing breast cancer risk after DTC, including genetic susceptibility, obesity, and hormones (estrogen and thyroid-stimulating hormone). Different histological subtypes of DTC should be studied separately, given findings thus far regarding genetic tumor profiles. Up to now, some studies have been published about obesity as common risk factor for DTC and breast cancer [e.g., (51)]. As to the role of estrogens and thyroid-stimulating hormone as common risk factors for DTC and breast cancer, a number of in vitro and animal studies have been published, but only a few studies in humans (52–54). In any case, levothyroxine therapy, aiming at thyroid-stimulating hormone suppression in patients with advanced DTC, is suspected to increase breast cancer risk independent of DTC (55). In addition, endocrine disruptors like nitrate may play a role in the pathogenesis of DTC and breast cancer (56, 57).
While six of nine cohort and case–control studies published from 1984 to 2000 did not show an increased risk for breast cancer after DTC, 15 of 17 studies published in 2000 and later demonstrated such an increased risk. It may be speculated that, in the later period, which is characterized by a sharp increase in DTC incidence worldwide, some common risk factors such as endocrine disruptors may have affected the incidence of breast cancer as well as DTC.
Finally, with respect to the scope of this review, to obtain an estimate of the risk of breast cancer as an SPM after RAI of DTC with a focus on young females, it is difficult to draw proper conclusions. That is because only two studies referenced here concentrated on those given such therapy as children or adolescents (3, 25). These studies described an increasing risk with age after adolescence for different types of SPM after RAI for DTC; however, these tumor entities did not include breast cancer.
Since the data are not sufficient to draw any conclusions about age dependence of breast cancer risk after RAI of DTC, it seems to be reasonable and necessary to evaluate whether relevant data in large-enough samples of young DTC patients can be collected in a systematic international multicenter survey which should be carried out as a case–control study applying multivariate statistical methods.
International Multi-Registry Survey
Our registry study was performed with the goal of assessing the potential sample size for a larger and more detailed study, allowing firmly evidence-based conclusions to be drawn on the real risk of breast cancer before and after treatment of DTC with RAI in young females. One important finding of our survey was that usually registries covering the whole age spectrum of patients with DTC contain only very low percentages of those <18 years old, ranging between 2 and 7% (the situation in Münster, Würzburg, and Gliwice registries in our survey). Since dedicated registries of children and adolescents with DTC are rare and tend to contain only low numbers of cases, it might not to be possible to restrict the limit of “young age” at the time of RAI to 18 years. To ensure the recruitment of a sample size enabling sufficient statistical power, the age limit at the time of RAI probably should be increased to 40 years, which would cover about 35% of patients with DTC.
Based on the maximum breast cancer rates in our registry survey (see Section Cumulative I-131 Activity) and on published data (5), it is assumed that—independent of treatment—about 2% of female DTC survivors develop breast cancer. As noted earlier, RAI for DTC with cumulative activities of 10–15 GBq I-131 corresponds to radiation doses to the female breast of between 2 and 3 Gy, which may double/triple the lifetime risk for breast cancer (8). We estimated that sample sizes of at least 4,340 cases below age 40 years at the time of RAI and 660 controls will be necessary under the assumption of an HR of 2.76 to reject the zero hypothesis of no effect of RAI, with a power of 80% (58).
Taking into account that about 3,200 of the patients in this registry study already met the age <40 years criterion, it seems to be feasible to recruit 30% more cases by including additional patients from other DTC specialist centers in Germany and abroad. Regarding the controls not receiving RAI, this survey already identified 650 of the 660 necessary patients for a subsequent study.
Conclusions
To summarize today's state of knowledge, independent of DTC treatment, there appears to be a bi-directional association of DTC itself and breast cancer. Nonetheless, the risk of breast cancer in adult DTC survivors is low, about 2%, slightly higher in females than in males, but based on the literature, presumably lower in children and adolescents than in older age groups. RAI is assumed not to substantially influence the lifetime risk of breast cancer after DTC, but data from those given such treatment as children or adolescents are sparse.
The literature review and multicenter registry survey reported here lead to the following recommendation: an international multicenter study with a sufficiently high number of female DTC survivors is feasible; that study should have a case–control design and include female patients <40 years of age with DTC diagnosed 20–30 years earlier. For reasons of compliance and practicability, such a design should be preferred over a longitudinal study lasting several decades.
However, especially given the likely at most slightly increased risk for breast cancer after RAI, breast cancer screening of a large cohort of female DTC survivors who received breast doses between 0.2 and 2 Gy from cumulative RAI activities of 1–15 GBq I-131 (7) is not unproblematic for ethical reasons. These reasons are related to an expected high rate of false-positive findings of ultrasonographic screening for breast cancer—in the range of 10%—and a resultant uncertain frequency of “misdiagnosis.” On similar grounds, the International Late Effects of Childhood Cancer Guideline Harmonization Group does not recommend routine breast cancer surveillance in female childhood, adolescent, or young adult cancer survivors treated with chest radiation doses <10 Gy (59). Such concerns apply in an even more pronounced way to the control cohort not affected by RAI-related radiation exposure as a potential risk-increasing factor. Hence, RAI patients and controls should be especially actively involved in choices regarding breast cancer screening, in a “shared decision-making” approach, and particular attention should be paid to the education of potential study participants regarding this possible issue (60).
Author Contributions
CR contributed to concept development, study management, critical review of the literature, and editing of the final manuscript. RS contributed to study management, literature search, critical review of the literature, and language editing. TP contributed to the management and the analysis of thyroid cancer database in Minsk. MF contributed to the histology review of thyroid cancer database in Minsk. UMä contributed to the supply of registry data from Würzburg. UMa contributed to the statistical analysis and writing the statistics section of the manuscript. AV contributed to the supply of registry data from Münster. TB contributed to the supply of registry data from Kiev. JK contributed to the supply of registry data from Gliwice. RE contributed to the supply of registry data from Pisa. FV contributed to the supply of registry data from Rio de Janeiro. JM contributed to the supply of registry data from Sremska Kamenica. GC contributed to the supply of registry data from Coimbra. VD contributed to the study management, literature search, critical review of the literature, supply of feasibility study data from Minsk, and drafting of the manuscript. All authors contributed to the critical review. All authors contributed to the article and approved the submitted version.
Funding
This project was funded by the German Federal Office for Radiation Protection (File Number 35615S424). The funder played no role in determining the content of the manuscript or in the decision regarding whether to submit the manuscript for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
An English language medical editor, Robert J. Marlowe, Spencer-Fontayne Corporation, Jersey City, NJ, USA, assisted in the revision of the original version of this paper.
References
1. Reiners C, Biko J, Haenscheid H, Hebestreit H, Kirinjuk S, Baranowski O, et al. Twenty-five years after Chernobyl: outcome of radioiodine treatment in children and adolescents with very-high risk radiation induced differentiated thyroid carcinoma. J Clin Endocrinol Metab. (2013) 98:3039–48. doi: 10.1210/jc.2013-1059
2. Clement SC, Peeters RP, Ronckers CM, Links TP, van den Heuvel-Eibrink MM, Nieveen van Dijkum EJ, et al. Intermediate and long-term adverse effects of radioiodine therapy for differentiated thyroid carcinoma – A systematic review. Cancer Treat Rev. (2015) 41:925–34. doi: 10.1016/j.ctrv.2015.09.001
3. Brown AP, Chen J, Hitchcock YJ, Szabo A, Shrieve DC, Tward JD. The risk of second primary malignancies up to three decades after the treatment of differentiated thyroid cancer. J Clin Endocrinol Metab. (2008) 93:504–15. doi: 10.1210/jc.2007-1154
4. Kumagai A, Reiners C, Drozd V, Yamashita S. Childhood thyroid cancers and radioactive iodine therapy: necessity of precautious radiation health risk management. Endocr J. (2007) 54:839–47. doi: 10.1507/endocrj.K07E-012
5. Yu CY, Saeed O, Goldberg AS, Farooq S, Fazelzad R, Goldstein DP, et al. A systematic review and meta-analysis of subsequent malignant neoplasm risk after radioactive iodine treatment of thyroid cancer. Thyroid. (2018) 288:1662–73. doi: 10.1089/thy.2018.0244
6. Poole VL, McCabe CJ. Iodide transport and breast cancer. J Endocrinol. (2015) 227:R1–12. doi: 10.1530/JOE-15-0234
7. Travis CC, Stabin MG. 131I ablation treatment in young females after the Chernobyl accident. J Nucl. (2006) 47:1723–7.
8. United States National Cancer Institute. RadRat Tool (2020). Available online at: https://radiationcalculators.cancer.gov/radrat/ (accessed April 19, 2020).
9. Subramanian S, Goldstein DP, Parlea L, Thabane L, Ezzat S, Ibrahim-Zada I, et al. Second primary malignancy risk in thyroid cancer survivors: a systematic review and meta-analysis. Thyroid. (2007) 17:1277–88. doi: 10.1089/thy.2007.0171
10. Sawka AM, Thabane L, Parlea L, Ibrahim-Zada I, Tsang RW, Brierely JD, et al. Second primary malignancy risk after radioactive iodine treatment for thyroid cancer: a systematic review and meta-analysis. Thyroid. (2009) 19:451–7. doi: 10.1089/thy.2008.0392
11. Joseph K, Edirimanne S, Eslick G. The association between breast cancer and thyroid cancer: a meta-analysis. Breast Canc Res Treat. (2015) 152:173–81. doi: 10.1007/s10549-015-3456-6
12. Zhang Y, Liang J, Li H, Cong H, Lin Y. Risk of second primary breast cancer after radioactive iodine treatment in thyroid cancer: a systematic review and meta-analysis. Nucl Med Commun. (2016) 37:110–5. doi: 10.1097/MNM.0000000000000419
13. Nielsen SM, White MG, Hung S, Aschebrok-Kilfoy B, Kaplan EL, Angelos P, et al. the breast-thyroid cancer link: a systematic review and meta-analysis. Cancer Epidemiol Biomark. (2016) 25:231–8. doi: 10.1158/1055-9965.EPI-15-0833
14. Rubino C, de Vathaire F, Dottorini ME, Hall P, Schvartz C, Couette JE, et al. Second primary malignancies in thyroid cancer patients. Br J Cancer. (2003) 89:1638–44. doi: 10.1038/sj.bjc.6601319
15. Sandeep TC, Strachan MW, Reynolds RM, Brewster DH, Scél G, Pukkala E, et al. Second primary cancers in thyroid cancer patients: a multinational record linkage study. J Clin Endocrinol Metab. (2006) 91:1819–25. doi: 10.1210/jc.2005-2009
16. Vassilopoulou-Sellin R, Palmer L, Taylor S, Cooksley CS. Incidence of breast carcinoma in women with thyroid carcinoma. Cancer. (1999) 85:696–705. doi: 10.1002/(SICI)1097-0142(19990201)85:3<696::AID-CNCR20>3.0.CO;2-4
17. Chen AY, Levy L, Goepfert H, Brown BW, Spitz MR, Vassilopoulou-Sellin R. The development of breast cancer in women with thyroid cancer. Cancer. (2001) 92:225–31. doi: 10.1002/1097-0142(20010715)92:2<225::AID-CNCR1313>3.0.CO;2-B
18. Ronckers CM, McCarron P, Ron E. Thyroid cancer and multiple primary tumors in the SEER cancer registries. Int J Cancer. (2005) 117:281–8. doi: 10.1002/ijc.21064
19. Bhattacharyya N, Chien W. Risk of second primary malignancy after radioactive iodine treatment for differentiated thyroid carcinoma. Ann Otol Rhinol Laryngol. (2006) 15:607–10. doi: 10.1177/000348940611500806
20. Chuang S-C, Hashibe M, Yu G-P, Le AD, Cao W, Hurwitz EL, et al. Radiotherapy for primary thyroid cancer as a risk factor for second primary cancers. Cancer Lett. (2006) 238:42–52. doi: 10.1016/j.canlet.2005.06.015
21. Kim C, Bi X, Pan D, Chen Y, Carling T, Ma S, et al. The risk of second cancers after diagnosis of primary cancer is elevated in thyroid microcarcinomas. Thyroid. (2013) 23:575–82. doi: 10.1089/thy.2011.0406
22. Kuo JH, Chabot JA, Lee JA. Breast cancer in thyroid cancer survivors: an analysis of the surveillance, epidemiology, and end results-9 database. Surgery. (2016) 159:23–30. doi: 10.1016/j.surg.2015.10.009
23. Uprety D, Khanal A, Arjyal L, Bista A, Basnet B, Kandel P, et al. The risk of secondary primary malignancy in early stage differentiated thyroid cancer: a US population-based study. Acta Oncol. (2016) 55:1375–7. doi: 10.1080/0284186X.2016.1196829
24. Endo M, Liu JR, Dougan M, Lee JS. Incidence of second malignancies in patients with papillary thyroid cancer from surveillance, epidemiology, and end results 13 datasets. J Thyroid Res. (2018) 2018:8765369. doi: 10.1155/2018/8765369
25. Adly MH, Soby M, Rezak MR, Ishak M, Afifi MA, Shafie AE, et al. Risk of second malignancies among survivors of pediatric thyroid cancer. Int J Clin Oncol. (2018) 23:625–33. doi: 10.1007/s10147-018-1256-9
26. Ron E, Curtis R, Hoffman DA, Flannery JT. Multiple primary breast and thyroid cancer. Br J Cancer. (1984) 49:87–92. doi: 10.1038/bjc.1984.13
27. Simon MS, Tang M-T, Bernstein L, Norman SA, Weiss L, Burkman TM, et al. Do thyroid disorders increase the risk of breast cancer? Cancer Epidemiol Biomark. (2002) 11:1574–8.
28. Canchola AJ, Horn-Ross PL, Purdie DM. Risk of second primary malignancies in women with papillary thyroid cancer. Am J Epidemiol. (2006) 163:521–7. doi: 10.1093/aje/kwj072
29. Cho YY, Lim J, Oh C-M, Ryu J, Jung K-W, Chung J-H, et al. Elevated risks of subsequent primary malignancies in patients with thyroid cancer: a nationwide, population-based study in Korea. Cancer. (2015) 121:259–68. doi: 10.1002/cncr.29025
30. Ahn HY, Min HS, Yeo Y, Ma SH, Hwang Y, An JH, et al. Radioactive iodine therapy did not significantly increase the incidence and recurrence of subsequent breast cancer. J Clin Endocrinol Metab. (2015) 100:3486–93. doi: 10.1210/JC.2014-2896
31. Khang AR, Cho SW, Choi HS, Ahn HY, Yoo WS, Kim KW, et al. The risk of second primary malignancy is increased in differentiated thyroid cancer patients with a cumulative (131)I dose over 37 GBq. Clin Endocrinol. (2015) 83:117–23. doi: 10.1111/cen.12581
32. Lu C-H, Lee K-D, Chen P-T, Chen C-C, Kuan F-C, Huang C-E, et al. Second primary malignancies following thyroid cancer: a population-based study in Taiwan. Eur J Endocrinol. (2013) 169:577–85. doi: 10.1530/EJE-13-0309
33. Teng CJ, Hu YW, Chen SC, Yeh CM, Chiang HL, Chen TJ, et al. Use of radioactive iodine for thyroid cancer and risk of second primary malignancy: a nationwide population-based study. J Nat Cancer Inst. (2016) 08:1–8. doi: 10.1093/jnci/djv314
34. Lin CY, Lin CL, Huang WS, Kao CH. Risk of breast cancer in patients with thyroid cancer receiving or not receiving I-131treatment: a nationwide population-based cohort study. J Nucl Med. (2016) 57:685–90. doi: 10.2967/jnumed.115.164830
35. Sadetzki S, Calderon-Margalit R, Peretz C, Novikov I, Barchan M, Papa MZ. Second primary breast and thyroid cancers (Israel). Cancer Causes Control. (2003) 14:367–75. doi: 10.1023/A:1023908509928
36. Hirsch D, Shohat T, Gorsheim A, Robenshtok E, Shimon I, Benbassat C. Incidence of non- thyroidal primary malignancy and the association with I-131 treatment in patients with differentiated thyroid cancer. Thyroid. (2016) 26:1110–6. doi: 10.1089/thy.2016.0037
37. Izhakov E, Barchana M, Lipshitz I, Silverman BG, Stern N, Keinan-Boker L. Trends of second primary malignancy in patients with thyroid cancer: a population based cohort study in Israel. Thyroid. (2017) 27:793. doi: 10.1089/thy.2016.0481
38. Osterlind A, Olsen JH, Lynge E, Ewertz M. Second cancer following cutaneous melanoma and cancers of the brain, thyroid, connective tissue, bone and eye in Denmark, 1943-1989. Nat Cancer Inst Monogr. (1985) 68:361–88.
39. Hall P, Holm LE, Lundell G. Second primary tumors following thyroid cancer. A Swedish record linkage study. Acta Oncol. (1990) 29:869–73. doi: 10.3109/02841869009096381
40. Hall P, Holm LE, Lundell G, Bjelkengren G, Larsson LG, Lindberg S, et al. Cancer risks in thyroid cancer patients. Brit J Cancer. (1991) 64:159–63. doi: 10.1038/bjc.1991.261
41. Hall P, Holm L-E, Undell G, Ruden B-I. Tumors after radiotherapy for thyroid cancer. A case-control study within a cohort of thyroid cancer patients. Acta Oncologica. (1992) 31:403–7. doi: 10.3109/02841869209088279
42. Akslen LA, Glattre E. Second malignancies in thyroid cancer patients: a population-based survey of 3658 cases from Norway. Eur J Cancer. (1992) 28:91–195. doi: 10.1016/S0959-8049(05)80085-1
43. Adjadj E, Rubino C, Shamsaldim A, Le MG, Schlumberger M, de Vathaire F. The risk of multiple primary breast and thyroid carcinomas - role of the radiation dose. Cancer. (2003) 98:1309–17. doi: 10.1002/cncr.11626
44. Berthe E, Henry-Amar M, Michels JJ, Rame JP, Berthet P, Babin E, et al. Risk of second primary cancer following differentiated thyroid cancer. Eur J Nucl Med Mol Imaging. (2004) 31:685–91. doi: 10.1007/s00259-003-1448-y
45. Edhemovic I, Volk N, Auersperg M. Second primary cancers following thyroid cancer in Slovenia. A population-based cohort study. Eur J Cancer. (1998) 3:1813–4.
46. An JH, Hwangbo Y, Ahn HY, Keam B, Lee KE, Han W, et al. A possible association between thyroid cancer and breast cancer. Thyroid. (2015) 35:1330–8. doi: 10.1089/thy.2014.0561
47. Fridman M, Drozd V, Demidchik YL, Levin L, Branovan D. Second primary malignancy in Belarus patients with post-Chernobyl papillary thyroid carcinoma. Thyroid. (2015) 25(Suppl. 1):A22–3.
48. Van Fossen VL, Wilhelm SM, Eaton JL, McHenry CR. Association of thyroid, breast and renal cell cancer: a population-based study of the prevalence of second malignancies. Ann Surg Oncol. (2013) 20:1341–7. doi: 10.1245/s10434-012-2718-3
49. Anders CK, Johnson R, Litton J, Phillips M, Bleyer A. Breast cancer before age 40 years. Semin Oncol. (2009) 36:237–49. doi: 10.1053/j.seminoncol.2009.03.001
50. Francis GL, Waguespack SG, Bauer AJ, Angelos P, Benvenga S, Cerutti JM, et al. Management guidelines for children with thyroid nodules and differentiated thyroid cancer. Pediatrics. (2018) 142:716–59. doi: 10.1089/thy.2014.0460
51. Xu L, Port M, Landi S, Gemignani F, Cipollini M, Elisei R, et al. Obesity and the risk of papillary thyroid cancer: a pooled analysis of three case-control studies. Thyroid. (2014) 24:966–74. doi: 10.1089/thy.2013.0566
52. Henderson BE, Ross R, Bernstein L. Estrogens as a cause of human cancer: the Richard and Hinda Rosenthal Foundation award lecture. Cancer Res. (1988) 48:246–53.
53. Fang Y, Yao L, Sun J, Yang R, Chen Y, Tian J, et al. Does thyroid dysfunction increase the risk of breast cancer? A systematic review and meta-analysis. J Endocrinol Invest. (2017) 40:1035–47. doi: 10.1007/s40618-017-0679-x
54. Weng C-H, Okawa ER, Roberts MB, Park SK, Umbricht CB, Manson JAE, et al. Breast cancer risk in postmenopausal women with medical history of thyroid disorder in the women's health initiative. Thyroid. (2020) 30:519–30. doi: 10.1089/thy.2019.0426
55. Hercbergs A, Mousa SA, Leinung M, Lin HY, Davis P. Thyroid hormone in the clinic and breast cancer. Horm Cancer. (2018) 9:139–43. doi: 10.1007/s12672-018-0326-9
56. Veselik DJ, Divekar S, Dakshanamurthy S, Storchan GB, Turner JM, Graham KL, et al. Activation of estrogen receptor-alpha by the anion nitrite. Cancer Res. (2008) 68:3950–8. doi: 10.1158/0008-5472.CAN-07-2783
57. Drozd VM, Branovan I, Shiglik N, Biko J, Reiners C. Thyroid cancer induction: nitrates as independent risk factors or risk modulators after radiation exposure, with a focus on the Chernobyl accident. Eur Thyroid J. (2018) 7:67–74. doi: 10.1159/000485971
58. Reiners C, Schneider R, Drozd V, Dedovich T, Leonova T, Mitjukova T, et al. Brustkrebsrisioko nach Radiojodtherapie des Schilddrüsenkarzinoms. Bundesamt für Strahlenschutz Forschungsvorhaben. (2018). Available online at: http://doris.bfs.de/jspui/handle/urn:nbn:de:0221-2019013117429 (accessed April 19, 2020).
59. Mulder RL, Kremer LCM, Hudson MM, Bhatia S, Landier W. Recommendations for breast cancer surveillance for female childhood, adolescent and young adult cancer survivors treated with chest radiation: a report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. (2013) 14:e621–9. doi: 10.1016/S1470-2045(13)70303-6
Keywords: differentiated thyroid carcinoma, radioiodine therapy, iodine-131, long-term complications, young females, childhood and adolescence, second primary malignancy, breast cancer
Citation: Reiners C, Schneider R, Platonova T, Fridman M, Malzahn U, Mäder U, Vrachimis A, Bogdanova T, Krajewska J, Elisei R, Vaisman F, Mihailovic J, Costa G and Drozd V (2020) Breast Cancer After Treatment of Differentiated Thyroid Cancer With Radioiodine in Young Females: What We Know and How to Investigate Open Questions. Review of the Literature and Results of a Multi-Registry Survey. Front. Endocrinol. 11:381. doi: 10.3389/fendo.2020.00381
Received: 23 January 2020; Accepted: 14 May 2020;
Published: 10 July 2020.
Edited by:
Jacqueline Jonklaas, Georgetown University, United StatesReviewed by:
Joanna Klubo-Gwiezdzinska, National Institutes of Health (NIH), United StatesYevgeniya Kushchayeva, University of South Florida, United States
Copyright © 2020 Reiners, Schneider, Platonova, Fridman, Malzahn, Mäder, Vrachimis, Bogdanova, Krajewska, Elisei, Vaisman, Mihailovic, Costa and Drozd. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christoph Reiners, cmVpbmVyc19jQHVrdy5kZQ==
†Present address: Alexis Vrachimis, German Oncology Center, Limassol, Cyprus