 Katharina Mörwald1
Katharina Mörwald1 Elmar Aigner2,3Peter Bergsten4
Elmar Aigner2,3Peter Bergsten4 Susanne M. Brunner1,2,5Anders Forslund6Joel Kullberg7Hakan Ahlström7
Susanne M. Brunner1,2,5Anders Forslund6Joel Kullberg7Hakan Ahlström7 Hannes Manell4Kirsten Roomp8Sebastian Schütz1,2Fanni Zsoldos1Wilfried Renner8Dieter Furthner2,9Katharina Maruszczak1,2Stephan Zandanell2,3
Hannes Manell4Kirsten Roomp8Sebastian Schütz1,2Fanni Zsoldos1Wilfried Renner8Dieter Furthner2,9Katharina Maruszczak1,2Stephan Zandanell2,3 Daniel Weghuber1,2*
Daniel Weghuber1,2* Harald Mangge10†
Harald Mangge10†- 1Department of Pediatrics, University Hospital Salzburg, Paracelsus Medical University, Salzburg, Austria
- 2Obesity Research Unit, University Hospital Salzburg, Paracelsus Medical University, Salzburg, Austria
- 3First Department of Medicine, University Hospital Salzburg, Paracelsus Medical University, Salzburg, Austria
- 4Department of Medical Cell Biology, University Uppsala, Uppsala, Sweden
- 5Research Program for Receptor Biochemistry and Tumor Metabolism, Department of Pediatrics, University Hospital Salzburg, Paracelsus Medical University, Salzburg, Austria
- 6Department of Women's and Children's Health, University Uppsala, Uppsala, Sweden
- 7Department of Surgical Sciences, Radiology, University Uppsala, Uppsala, Sweden
- 8Luxembourg Center for Systems Biomedicine, University Luxembourg, Luxembourg, Luxembourg
- 9Department of Pediatrics and Adolescent Medicine, Salzkammergut-Klinikum, Vöcklabruck, Austria
- 10Clinical Institute for Medical and Chemical Laboratory Diagnosis, Medical University Graz, Graz, Austria
Non-alcoholic fatty liver disease (NAFLD) contributes essentially to the burden of obesity and can start in childhood. NAFLD can progress to cirrhosis and hepatocellular carcinoma. The early phase of NAFLD is crucial because during this time the disease is fully reversible. Pediatric NAFLD shows unique features of histology and pathophysiology compared to adults. Changes in serum iron parameters are common in adult NAFLD and have been termed dysmetabolic iron overload syndrome characterized by increased serum ferritin levels and normal transferrin saturation; however, the associations of serum ferritin, inflammation, and liver fat content have been incompletely investigated in children. As magnetic resonance imaging (MRI) is an excellent measure for the degree of liver steatosis, we applied this method herein to clarify the interaction between ferritin and fatty liver in male adolescents. For this study, one hundred fifty male pediatric patients with obesity and who are overweight were included. We studied a subgroup of male patients with (n = 44) and without (n = 18) NAFLD in whom we determined liver fat content, visceral adipose tissue, and subcutaneous adipose tissue extent with a 1.5T MRI (Philips NL). All patients underwent a standardized oral glucose tolerance test. We measured uric acid, triglycerides, HDL-, LDL-, total cholesterol, liver transaminases, high sensitive CRP (hsCRP), interleukin-6, HbA1c, and insulin. In univariate analysis, ferritin was associated with MRI liver fat, visceral adipose tissue content, hsCRP, AST, ALT, and GGT, while transferrin and soluble transferrin receptor were not associated with ferritin. Multivariate analysis identified hsCRP and liver fat content as independent predictors of serum ferritin in the pediatric male patients. Our data indicate that serum ferritin in male adolescents with obesity is mainly determined by liver fat content and inflammation but not by body iron status.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is the most common liver disease in children and adolescents (1). The prevalence of pediatric NAFLD has swiftly increased paralleling the obesity epidemic. Estimations from epidemiological studies suggest that 7–10% of all and up to 30% of children with obesity are affected (2–4). It is dependent on age, ethnicity, and specific genetic determinants and is the highest in children with obesity with up to 38% (5, 6). The global prevalence of NAFLD was estimated to be 25.2% (95% CI: 22.10–28.65) with the highest prevalence in the Middle East and South America and the lowest in Africa. Metabolic comorbidities associated with NAFLD included obesity (51.34%; 95% CI: 41.38–61.20), type 2 diabetes (T2D, 22.51%; 95% CI: 17.92–27.89), hyperlipidemia (69.16%; 95% CI: 49.91–83.46%), hypertension (39.34%; 95% CI: 33.15–45.88), and metabolic syndrome (42.54%; 95% CI: 30.06–56.05) (7). Fibrosis progression proportion, and mean annual rate of progression in NASH were 40.76% (95% CI: 34.69–47.13) and 0.09 (95% CI: 0.06–0.12). Mechanisms leading to NAFLD include metabolic changes in glucose and lipid homeostasis, disturbed metabolic responses in context of a genetic predisposition, and an excess energy intake (8).
Serum ferritin is a reliable marker for body iron stores in the clinical routine. It is however, also strongly influenced by inflammatory stimuli, which significantly limits the use and interpretation of high serum ferritin concentrations. In the context of the metabolic syndrome and NAFLD, both iron stores and subclinical inflammation may therefore determine ferritin concentrations in any individual patient. Counteracting stimuli such as increased iron demand during growth and impaired iron uptake in obesity may further complicate the picture in a given patient (9). In adult studies, hyperferritinemia has been documented in obesity-related chronic inflammatory conditions such as type 2 diabetes mellitus, metabolic syndrome, and NAFLD. The histological evidence of hepatic iron accumulation has been reported to associate with hepatic fibrosis and advanced disease severity in adult patients with NAFLD, although, subsequent studies have not confirmed this association. Hence, results regarding the role of iron in human NAFLD remain inconclusive (10–12). Pediatric NAFLD shows unique features in liver histology and pathophysiology in comparison to adults (12, 13). In keeping with this, children with obesity and NAFLD exhibit no or only a rather mild intra-hepatic iron deposition. Furthermore, juveniles who are obese, frequently and typically have normal serum ferritin concentrations, hence the characteristic features of the dysmetabolic iron overload syndrome are usually not observed in children and adolescents (14–18). The association of ferritin concentrations with insulin resistance, abdominal obesity, and parameters of the metabolic syndrome and NAFLD have been extensively studied in adults (19) but only rarely in children (20–24). So far, the majority of previous pediatric studies applied ultrasound or liver enzymes as surrogates of NAFLD severity (10, 16). To date, there is a lack of studies accurately assessing the relationship between hepatic steatosis, associated markers of subclinical inflammation, and ferritin in pediatric patients. Although magnetic resonance imaging (MRI) has been shown to more reliably capture the degree of steatosis (25), only data from a South Korean study applying MRI in a pediatric age group exist so far (26).
Taken together the data of the role of ferritin as a potential marker of fatty liver disease in childhood are limited (27). The aim of this study was to assess how and to which extent ferritin is related to metabolic changes linked to obesity, in particular liver fat content.
Materials and Methods
Study Population, and Design
Between October 2012 and December 2016, we recruited 339 patients in an obesity specialist clinic in Salzburg (Austria) as part of the BETA JUDO study (BETA cell function in Juvenile Diabetes and Obesity, FP7-HEALTH-2011-two-stage, project number: 279153) in a cross-sectional study design. The inclusion criteria of patients were that they had to be in between the age of 10–18 years, overweight or obese according to the WHO criteria (BMI-SDS > 1). The exclusion criteria was a lack of consent or if the patients had any chronic liver disease. To this end, endocrine disorders (thyroid disease, diabetes type I), autoimmune, viral (viral hepatitis, HIV), or hereditary causes (Wilson disease, hereditary hemochromatosis, alpha-1 antitrypsin deficiency, celiac disease, lysosomal acid lipase deficiency) of liver disease, use of steatogenic drugs were excluded as confounders of elevated serum ferritin in all patients with increased serum transaminases (ALT, AST) >40 U/L. Patients did not report any alcohol intake. Full laboratory data sets of 150 male patients with obesity or are overweight were included out of which 62 male patients (35.4%) underwent additional MRI (liver fat content, abdominal visceral, and subcutaneous fat) and were selected for further investigations. Data of female patients (n = 164) were excluded due to potentially lower ferritin levels because of menorrhea.
Height and weight were assessed by means of a standardized, calibrated scale (Seca). BMI and BMI-SDS were calculated according to the WHO 2006–2007 reference population. Waist circumference (cm) and hip circumference (cm) were measured using a flexible tape. Blood pressure was measured twice, using a standardized clinical aneroid sphygmomanometer. Puberty staging was done according to Tanner and subjects were grouped as prepubertal (group 1 = Tanner I), pubertal (group 2 = Tanner II–IV), and postpubertal (group 3 = Tanner V). The ethical approvals for the study were obtained from the ethical committee of Salzburg (Number: 1544/2012). The study was carried out according to the Declaration of Helsinki. Written informed consent was achieved from all participants and at least one of their caregivers.
Blood Sampling and Biochemical Analyses
Following an overnight fast, after blood sampling for all parameters but postprandial glucose, all patients underwent a standardized oral glucose tolerance test (OGTT, glucose dosage 1.75g/kg body weight) over 180 min as previously described (28, 29). OGTT was performed according to standard procedures by setting an intravenous line in an antecubital vein and subsequent blood draws were performed via this line at nine different time points after glucose challenge. Ferritin, soluble transferrin receptor, transferrin, iron, uric acid, triglycerides, HDL cholesterol, total cholesterol, and liver transaminases were measured using an enzymatic photometric test (Modular Analytics System, P-Modul, 917 by Roche Diagnostics). The evaluation of LDL cholesterol also required an enzymatic photometric test using Integra Manual by Roche Diagnostics. High sensitive CRP (hsCRP) was examined by an immunologic turbidimetric test (COBAS-Integra by Roche Diagnostics) and Interleukin 6 by an enzyme-linked immunosorbent assay (Modular Analytics System, E-Modul by Roche Diagnostics). HbA1c was measured by reversed-phase chromatography and lipoprotein (a) by a turbidimetric test (COBAS-Integra by Roche Diagnostics). Samples underwent immediate centrifugation at 2,500 g for 10 min at 4°C, subsequently aliquoted and frozen at −80°C. Plasma was consecutively used for the analysis of insulin in the central lab in Uppsala. Single-plex ELISA-kits for each analyte were used (Mercodia AB®, Uppsala, Sweden).
Magnetic Resonance Imaging (MRI)
MRI-examinations were performed to determine liver fat content (LFC) and volumes of abdominal visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT) as previously described (29). All exams were performed using 1.5 T clinical MRI-systems from Philips Medical System (Netherlands) after a light meal and in close proximity to the OGTT. Water-fat imaging techniques were used throughout. The scans were done over 16 cm along the craniocaudal axis and centered on the L1 vertebra. The adipose tissue volumes were determined using a fully automated segmentation method that uses a filtering technique to separate VAT from SAT. Liver fat image reconstruction was done by a multi-resolution version of a method that employs a whole-image optimization approach (30). A single operator trained by an experienced radiologist performed the measurements by manual segmentation in the axial slices of the water images using the software ImageJ (version 1.42q, http://rsbweb.nih.gov/ij/).
Definition of NAFLD
Patients with NAFLD had a liver fat content ≥5%, as measured by MRI. As previously described, a liver fat content cutoff of ≥5% and therefore a close relation between histopathological changes and liver fat fraction in MR-imaging have been promoted by various groups (31–36).
Statistical Analysis
The data were analyzed descriptively showing results with mean and standard deviation for metric variables and number and percentages for categorical variables. Due to non-normality of the data, all group differences were assessed with non-parametric methods, namely Wilcoxon's test for unpaired samples. For assessing connections between variables, linear regression in univariate as well as multivariate case was applied. The coefficients are indicating the change of the dependent variable when the describing variable is changing by one unit. Additionally, standard errors and p-values are presented. All results are presented along with 95%-Confidence Intervals. Tests are performed at a significance level of 5%. P-values are corrected with Bonferroni method for multiple testing. In multiple regression, the variance inflation factor was used as an indicator of multicollinearity. All calculations were done with R (Version 3.6.0).
Results
General Group Characteristics
Table 1 shows descriptive data of the 150 male adolescents with obesity and are overweight. Mean age of juveniles with overweight/obesity was 13.02 ± 1.97 years and 80.7% were staged as pubertal. Mean BMI was 31.39 ± 6.73 kg/m2 and mean liver fat content as measured by MRI was 13.15 ± 12.30% (based on 62 subjects). Mean ferritin value was 57.33 ± 26.55 μg/L in the overweight/obese group.
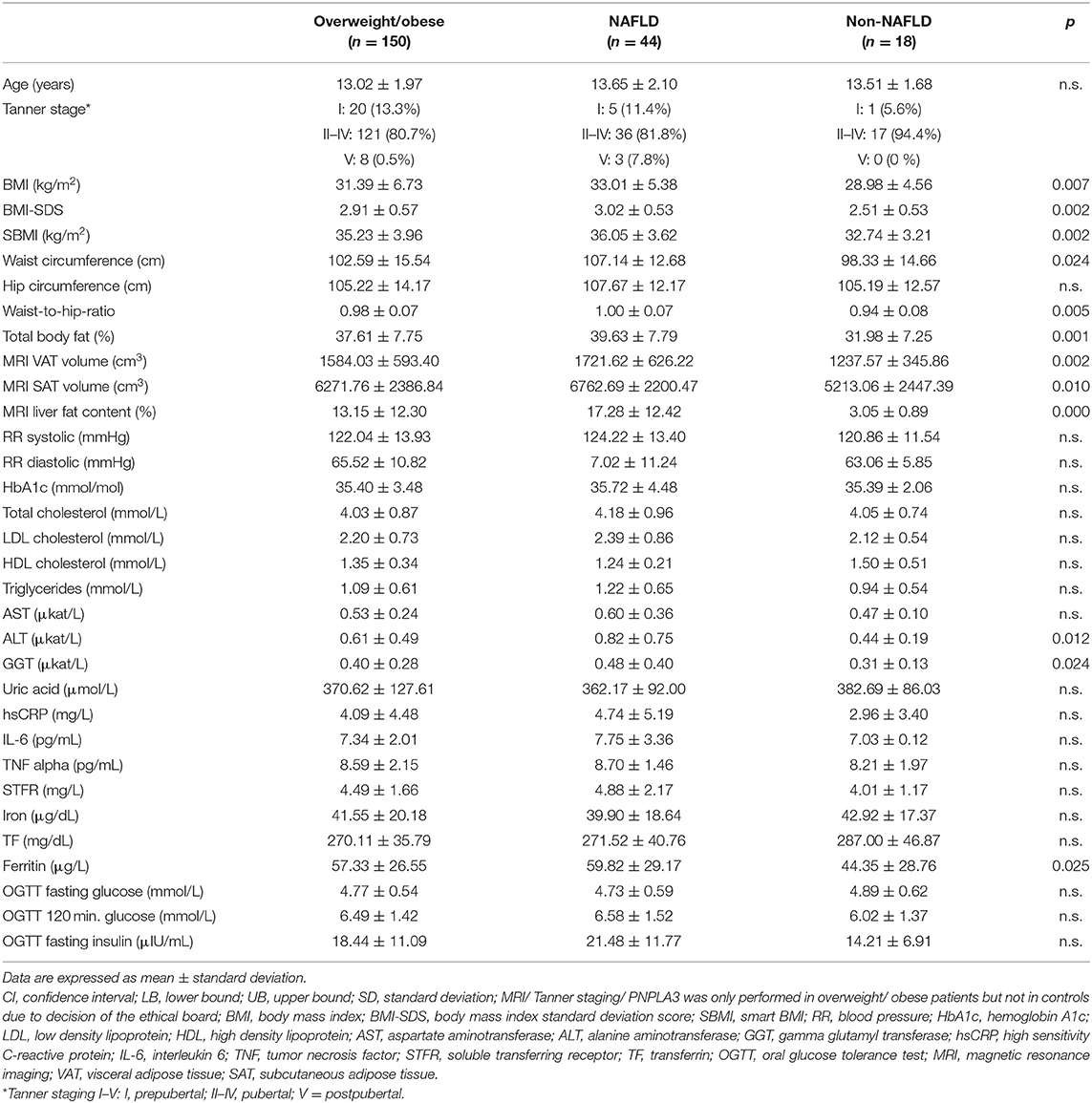
Table 1. Descriptive data of all male patients, with and without NAFLD as determined by MRI.
NAFLD Group Characteristics
Descriptive data of 44 male adolescents with NAFLD and 18 without NAFLD (defined by liver fat content ≥5 and <5%, respectively) are shown in Table 1. In Table 2, descriptive data of the 62 male NAFLD patients are presented and categorized into quartiles of liver fat content, resulting in the following cut-offs: 25% = 3.9% liver fat content, 50% = 6.6% liver fat content, 75% = 20.4% liver fat content. Data are means with standard deviations, and p-values for the highest quartile in differentiation to the remaining three quartiles. Mean age and pubertal staging are similar between quartiles. BMI-SDS and SBMI is significantly higher in the highest quartile compared to the other three. In summary, characteristics of the metabolic syndrome showed a “metabolically unhealthier” phenotype in quartile 4, although only 2-h-glucose level in an oral glucose tolerance test was significantly different between the highest quartiles and the other remaining quartiles. Liver transaminases rise alongside to quartiles and show significantly higher levels in quartile 4. Inflammatory parameters show higher levels in quartile 4, without reaching a significant difference. Measured by MRI, liver fat, and visceral adipose tissue content are significantly elevated in quartile 4.
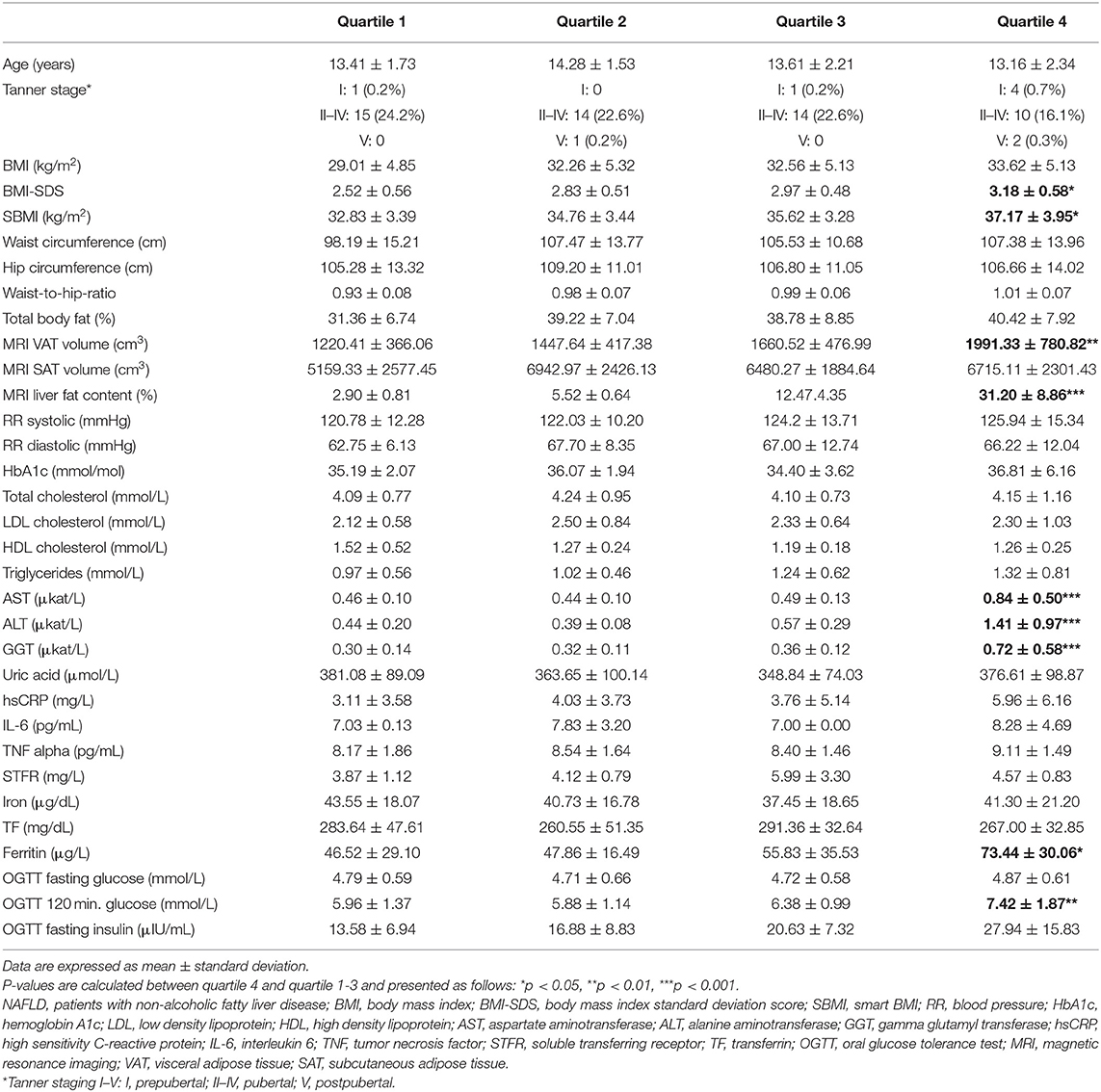
Table 2. Descriptive data of male NAFLD patients (defined according to liver fat content ≥ 5%, n = 62) categorized into quartiles of liver fat content (cut-offs: 25% = 3.8925%, 50% = 6.62%, 75% = 20.435%).
Ferritin as Cardiometabolic Risk Factor Independent of Iron Overload
Concerning iron metabolism, ferritin was significantly higher between NAFLD and non-NAFLD groups and in quartile 4 compared to the lower quartiles. In contrast, standard indicators of iron metabolism like soluble transferrin receptor, serum iron, and transferrin were similar between groups. In univariate analysis (Table 3), ferritin was directly correlated with MRI liver fat and visceral adipose tissue content as well as hsCRP, AST, ALT, and GGT. In multivariate analysis (Table 4), we tested which parameter best predicted serum ferritin in male obese and overweight juveniles. We included parameters with a significant correlation to ferritin from the univariate analysis into the multivariate model. Further, with an adjusted R-squared as criterion, none of the other covariates described any more of the variance in ferritin (data not shown). ALT, AST, and GGT were excluded from multivariate analysis due to multicollinearity. For multivariate analysis, we therefore chose hsCRP, MRI liver fat content, and MRI visceral adipose tissue content as variables, of which hsCRP and liver fat content independently predicted ferritin. Of note, liver fat content was positively correlated with visceral adipose tissue (coefficient 0.36). However, there was no indication of multicollinearity (variance inflation factor, data not shown).
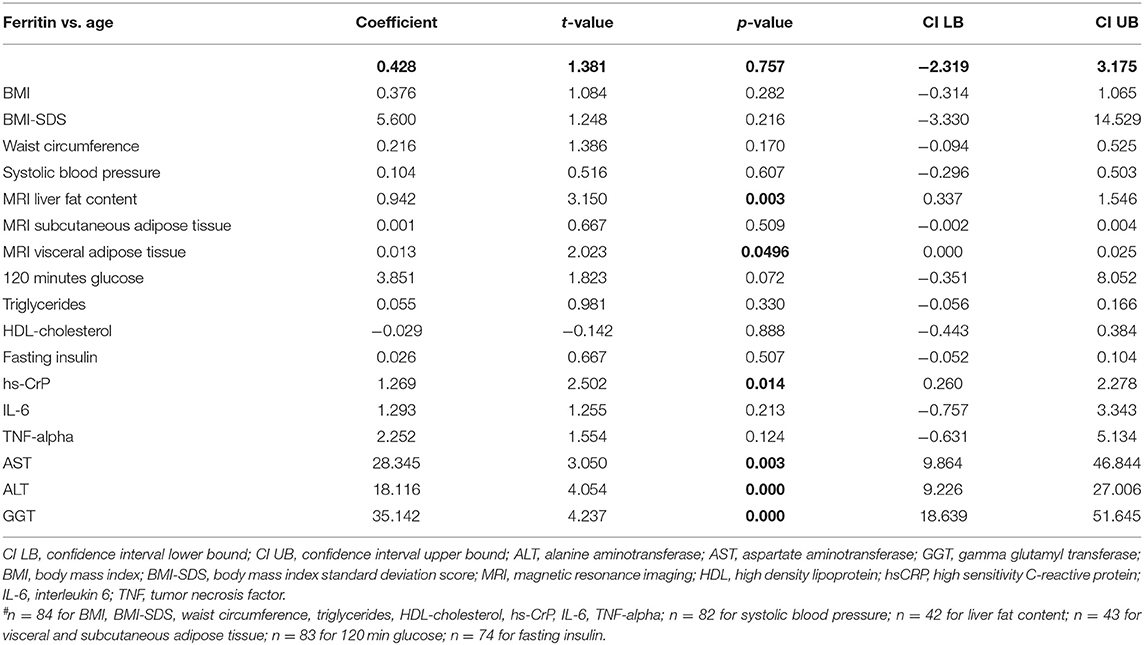
Table 3. Univariate analyses in male overweight/ obese patients (n = 85#).
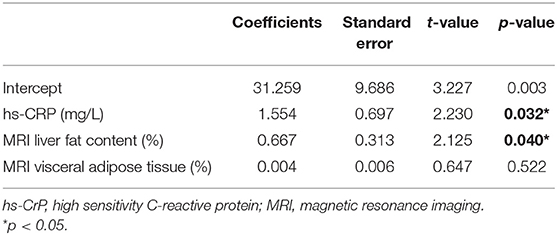
Table 4. Multivariate regression analysis: predictors of ferritin in a male overweight/obese pediatric cohort (n = 42).
Discussion
Obesity is increasing worldwide (37) and young people are particularly affected. This is alarming because young obese people will suffer from serious diseases later in life such as myocardial infarction, stroke, or cancer. As people become increasingly older, it is vital to remain in a healthy condition as you age (37). Liver disease contributes essentially to the pathologic burden of obesity and can start as early as in childhood. Fat accumulation in the liver is a hallmark of non-alcoholic fatty liver disease (NAFLD) which rapidly increases worldwide (38). NAFLD can progress from steatosis (NAFL) to steatohepatitis (NASH), cirrhosis, and hepatocellular carcinoma (HCC).
Approximately one-third of adult patients with NAFLD have a disturbed iron homeostasis but iron excess is to the best of our knowledge absent in pediatric NAFLD. Systemic iron overload associates with elevated serum ferritin and normal or mildly elevated transferrin saturation. The histological iron deposition pattern in these patients shows iron deposition in both hepatocytes and liver macrophages or only one of these cells, and has been named dysmetabolic iron overload syndrome (DIOS). Negative long-term effects of the hepatic iron deposition on the clinical course of NAFLD may occur because iron catalyzes the formation of toxic hydroxyl radicals, which mediate cellular damage potentially augmenting fibrosis progression in NAFLD (39). Conversely, reduction of body iron can restore insulin sensitivity, and epidemiological evidence suggests that it delays the onset of complications such as type 2 diabetes mellitus, cardiovascular disease, and advanced liver disease. Iron accumulation in adult NAFLD is due to inhibition of iron mobilization from hepatocytes and Kupffer cells. The impaired iron export relates to inflammation and metabolic derangements and involves key iron regulators such as hepcidin and ferroportin (40). We therefore aimed to elucidate whether serum ferritin links to indicators of body iron status or metabolic parameters in a well-characterized obese male children cohort. We observed that liver fat content determined by MRI and hsCRP were the best predictors of serum ferritin in male pediatric patients with obesity. These results show that already in childhood and adolescence serum ferritin increases after metabolic derangements with special importance of fat storage in the liver and reactive metabolic inflammation. Despite increased ferritin, the main indicators of increasing body iron stores and erythropoietic iron demand like soluble transferrin receptor, serum iron, and transferrin remained unchanged over quartiles. Adolescence is an important period of nutritional vulnerability and iron needs are elevated because of intensive growth and muscular development. However, this increased iron use might protect metabolically unhealthy young males from the development of actual iron overload (41). This further strengthens the suggestion that serum ferritin may be rather linked to metabolic inflammation (40) and not to a dysmetabolic iron overload syndrome which although may develop later in life in these subjects.
Moreover, the identification of potential biomarkers of the NAFLD and metabolic syndrome are an important clinical agenda. Hepatic fat content is an important estimate of systemic metabolic health. Our study revealed that MRI-assessed liver fat content and hsCRP best predicted serum ferritin values. These results suggest that ferritin may serve as a marker of early fatty liver disease in childhood obesity, at least in males. This is of interest, as non-invasive surrogate scores such as the fatty liver index have been shown to poorly predict liver fat content in children with obesity (42).
Limitation
The cross-sectional study design does not provide reliable information about causal relationships. Possibly, ferritin may be elevated because of accumulation of liver fat or ferritin may itself contribute causally to liver fat accumulation. Moreover, in more severe NAFLD, low degree of hepatic steatosis can be due to replacement of liver fat by fibrotic tissue (43). It is not possible to draw conclusions on underlying liver disease severity from our data. By assessing liver fat content by MRI in our patients, we could not distinguish steatosis and fibrosis. Ultimately, NAFLD/NASH is a diagnosis of exclusion, and liver biopsy is required to confirm the diagnosis, stage the disease, rule out other liver diseases, and determine the need for and urgency of aggressive therapy. In addition, due to missing values and thus reduced statistical power the results of the regression analysis must be interpreted cautiously. A further inherent limitation of ferritin as a marker of metabolic changes is that it is solely applicable in males due to the overwhelming impact of menstrual blood loss on iron parameters in female adolescents.
Conclusion
We showed herein that serum ferritin concentrations in male adolescents are related to hepatic lipid accumulation as verified by MRI and hsCRP as a marker of concomitant metabolic inflammation. These findings suggest that inflammation is already present in early phases of fatty liver disease and that elevated ferritin may link more closely to the development of adverse metabolic and inflammatory consequences of overweight and obesity than to iron status. Our results add novel information to the interpretation of serum ferritin concentrations in male adolescents with obesity as serum ferritin appears to increase in serum more in relation to liver fat and inflammation than to body iron stores. The clinical use of serum ferritin as a marker for NAFLD in children remains to be elucidated in future investigations including the evaluation of liver disease severity.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics commitee Salzburg, Austria. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
KMö and SB was involved in data acquisition and manuscript preparation. HA, AF, JK, HMane, and FZ was involved in data acquisition. EA and WR was involved in manuscript preparation. PB was involved in data acquisition and headed the Beta-JUDO study. KR was involved in data acquisition and storage. DW and HMang were both involved in manuscript preparation and data acquisition. All authors contributed to the article and approved the submitted version. DF, KMa, and SZ contributed to interpretation of data and manuscript revision.
Funding
This work was supported by Seventh Framework Programme (Grant EU-FP 7: 2007–2013; grant number 279153).
Conflict of Interest
DW has received consultant fees from Novo Nordisk. HA and JK are cofounders, stock owners, and employees of Antaros Medical, Mölndal, Sweden.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Crespo M, Lappe S, Feldstein AE, Alkhouri N. Similarities and differences between pediatric and adult nonalcoholic fatty liver disease. Metabolism. (2016) 65:1161–71. doi: 10.1016/j.metabol.2016.01.008
2. Anderson EL, Howe LD, Jones HE, Higgins JP, Lawlor DA, Fraser A. The prevalence of non-alcoholic fatty liver disease in children and adolescents: a systematic review and meta-analysis. PLoS One. (2015) 10:e0140908. doi: 10.1371/journal.pone.0140908
3. Bellentani S, Scaglioni F, Marino M, Bedogni G. Epidemiology of non-alcoholic fatty liver disease. Dig Dis. (2010) 28:155–61. doi: 10.1159/000282080
4. Feldstein AE, Charatcharoenwitthaya P, Treeprasertsuk S, Benson JT, Enders FB, Angulo P. The natural history of non-alcoholic fatty liver disease in children: a follow-up study for up to 20 years. Gut. (2009) 58:1538–44. doi: 10.1136/gut.2008.171280
5. Farrell GC, Wong VW, Chitturi S. NAFLD in Asia–as common and important as in the West. Nat Rev Gastroenterol Hepatol. (2013) 10:307–18. doi: 10.1038/nrgastro.2013.34
6. Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther. (2011) 34:274–85. doi: 10.1111/j.1365-2036.2011.04724.x
7. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. (2016) 64:73–84. doi: 10.1002/hep.28431
8. Abenavoli L, Milic N, Di Renzo L, Preveden T, Medic-Stojanoska M, De Lorenzo A. Metabolic aspects of adult patients with nonalcoholic fatty liver disease. World J Gastroenterol. (2016) 22:7006–16. doi: 10.3748/wjg.v22.i31.7006
9. Aigner E, Feldman A, Datz C. Obesity as an emerging risk factor for iron deficiency. Nutrients. (2014) 6:3587–600. doi: 10.3390/nu6093587
10. Nelson JE, Wilson L, Brunt EM, Yeh MM, Kleiner DE, Unalp-Arida A, et al. Relationship between the pattern of hepatic iron deposition and histological severity in nonalcoholic fatty liver disease. Hepatology. (2011) 53:448–57. doi: 10.1002/hep.24038
11. Kowdley KV, Nelson J. Reply: to PMID 21953442. Hepatology. (2013) 57:2095. doi: 10.1002/hep.26073
12. George DK, Goldwurm S, MacDonald GA, Cowley LL, Walker NI, Ward PJ, et al. Increased hepatic iron concentration in nonalcoholic steatohepatitis is associated with increased fibrosis. Gastroenterology. (1998) 114:311–8. doi: 10.1016/S0016-5085(98)70482-2
13. Schwimmer JB, Deutsch R, Kahen T, Lavine JE, Stanley C, Behling C. Prevalence of fatty liver in children and adolescents. Pediatrics. (2006) 118:1388–93. doi: 10.1542/peds.2006-1212
14. Manco M, Alisi A, Real JF, Equitani F, DeVito R, Valenti L, et al. Early interplay of intra-hepatic iron and insulin resistance in children with non-alcoholic fatty liver disease. J Hepatol. (2011) 55:647–53. doi: 10.1016/j.jhep.2010.12.007
15. Feldman A, Aigner E, Weghuber D, Paulmichl K. The potential role of iron and copper in pediatric obesity and nonalcoholic fatty liver disease. Biomed Res Int. (2015) 2015:287401. doi: 10.1155/2015/287401
16. Seltzer CC, Mayer J. Serum iron and iron-binding capacity in adolescents. Ii. Comparison of Obese and Nonobese Subjects. Am J Clin Nutr. (1963) 13:354–61. doi: 10.1093/ajcn/13.6.354
17. del Giudice EM, Santoro N, Amato A, Brienza C, Calabro P, Wiegerinck ET, et al. Hepcidin in obese children as a potential mediator of the association between obesity and iron deficiency. J Clin Endocrinol Metab. (2009) 94:5102–7. doi: 10.1210/jc.2009-1361
18. Demircioglu F, Gorunmez G, Dagistan E, Goksugur SB, Bekdas M, Tosun M, et al. Serum hepcidin levels and iron metabolism in obese children with and without fatty liver: case-control study. Eur J Pediatr. (2014) 173:947–51. doi: 10.1007/s00431-014-2268-8
19. Zelber-Sagi S, Nitzan-Kaluski D, Halpern Z, Oren R. NAFLD and hyperinsulinemia are major determinants of serum ferritin levels. J Hepatol. (2007) 46:700–7. doi: 10.1016/j.jhep.2006.09.018
20. Aigner E, Hinz C, Steiner K, Rossmann B, Pfleger J, Hohla F, et al. Iron stores, liver transaminase levels and metabolic risk in healthy teenagers. Eur J Clin Invest. (2010) 40:155–63. doi: 10.1111/j.1365-2362.2009.02238.x
21. Abril-Ulloa V, Flores-Mateo G, Sola-Alberich R, Manuel-y-Keenoy B, Arija V. Ferritin levels and risk of metabolic syndrome: meta-analysis of observational studies. BMC Public Health. (2014) 14:483. doi: 10.1186/1471-2458-14-483
22. Lee BK, Kim Y, Kim YI. Association of serum ferritin with metabolic syndrome and diabetes mellitus in the South Korean general population according to the Korean National Health and Nutrition Examination Survey (2008). Metabolism. (2011) 60:1416–24. doi: 10.1016/j.metabol.2011.02.008
23. Shim YS, Kang MJ, Oh YJ, Baek JW, Yang S, Hwang IT. Association of serum ferritin with insulin resistance, abdominal obesity, and metabolic syndrome in Korean adolescent and adults: the Korean National Health and Nutrition Examination Survey, 2008 to 2011. Medicine (Baltimore). (2017) 96:e6179. doi: 10.1097/MD.0000000000006179
24. Sheu WH, Chen YT, Lee WJ, Wang CW, Lin LY. A relationship between serum ferritin and the insulin resistance syndrome is present in non-diabetic women but not in non-diabetic men. Clin Endocrinol (Oxf). (2003) 58:380–5. doi: 10.1046/j.1365-2265.2003.01729.x
25. Middleton MS, Van Natta ML, Heba ER, Alazraki A, Trout AT, Masand P, et al. Diagnostic accuracy of magnetic resonance imaging hepatic proton density fat fraction in pediatric nonalcoholic fatty liver disease. Hepatology. (2018) 67:858–72. doi: 10.1002/hep.29596
26. Na JH, Park SW, Kang Y, Koh H, Kim S. The clinical significance of serum ferritin in pediatric non-alcoholic fatty liver disease. Pediatr Gastroenterol Hepatol Nutr. (2014) 17:248–56. doi: 10.5223/pghn.2014.17.4.248
27. Yi KH, Hwang JS, Lim SW, Lee JA, Kim DH, Lim JS. Ferritin level is associated with metabolic syndrome and elevated alanine aminotransferase in children and adolescents. J Pediatr Endocrinol Metab. (2016) 29:1337–44. doi: 10.1515/jpem-2016-0045
28. Forslund A, Staaf J, Kullberg J, Ciba I, Dahlbom M, Bergsten P. Uppsala longitudinal study of childhood obesity: protocol description. Pediatrics. (2014) 133:e386–93. doi: 10.1542/peds.2013-2143
29. Staaf J, Labmayr V, Paulmichl K, Manell H, Cen J, Ciba I, et al. Pancreatic fat is associated with metabolic syndrome and visceral fat but not beta-cell function or body mass index in pediatric obesity. Pancreas. (2017) 46:358–65. doi: 10.1097/MPA.0000000000000771
30. Berglund J, Kullberg J. Three-dimensional water/fat separation and T2* estimation based on whole-image optimization–application in breathhold liver imaging at 1.5 T. Magn Reson Med. (2012) 67:1684–93. doi: 10.1002/mrm.23185
31. Weghuber D, Roden M, Franz C, Chmelik M, Torabia S, Nowotny P, et al. Vascular function in obese children with non-alcoholic fatty liver disease. Int J Pediatr Obes. (2011) 6:120–7. doi: 10.3109/17477161003792580
32. Burgert TS, Taksali SE, Dziura J, Goodman TR, Yeckel CW, Papademetris X, et al. Alanine aminotransferase levels and fatty liver in childhood obesity: associations with insulin resistance, adiponectin, and visceral fat. J Clin Endocrinol Metab. (2006) 91:4287–94. doi: 10.1210/jc.2006-1010
33. Szczepaniak LS, Nurenberg P, Leonard D, Browning JD, Reingold JS, Grundy S, et al. Magnetic resonance spectroscopy to measure hepatic triglyceride content: prevalence of hepatic steatosis in the general population. Am J Physiol Endocrinol Metab. (2005) 288:E462–8. doi: 10.1152/ajpendo.00064.2004
34. Di Martino M, Pacifico L, Bezzi M, Di Miscio R, Sacconi B, Chiesa C, et al. Comparison of magnetic resonance spectroscopy, proton density fat fraction and histological analysis in the quantification of liver steatosis in children and adolescents. World J Gastroenterol. (2016) 22:8812–9. doi: 10.3748/wjg.v22.i39.8812
35. Schwimmer JB, Dunn W, Norman GJ, Pardee PE, Middleton MS, Kerkar N, et al. SAFETY study: alanine aminotransferase cutoff values are set too high for reliable detection of pediatric chronic liver disease. Gastroenterology. (2010) 138:1357–64.e1–2. doi: 10.1053/j.gastro.2009.12.052
36. Manning P, Murphy P, Wang K, Hooker J, Wolfson T, Middleton MS, et al. Liver histology and diffusion-weighted MRI in children with nonalcoholic fatty liver disease: a MAGNET study. J Magn Reson Imaging. (2017) 46:1149–58. doi: 10.1002/jmri.25663
37. Kachur S, Lavie CJ, de Schutter A, Milani RV, Ventura HO. Obesity and cardiovascular diseases. Minerva Med. (2017) 108:212–28. doi: 10.23736/S0026-4806.17.05022-4
38. Kolodziejczyk AA, Zheng D, Shibolet O, Elinav E. The role of the microbiome in NAFLD and NASH. EMBO Mol Med. (2019) 11:e9302. doi: 10.15252/emmm.201809302
39. Yao J, Dai Y, Zhang J, Zhang X, Zheng R. Association between serum ferritin level and nonalcoholic fatty liver disease in a non-obese Chinese population: a cross-sectional study. Clin Lab. (2019) 65. doi: 10.7754/Clin.Lab.2019.181250
40. Datz C, Muller E, Aigner E. Iron overload and non-alcoholic fatty liver disease. Minerva Endocrinol. (2017) 42:173–83. doi: 10.23736/S0391-1977.16.02565-7
41. Mesias M, Seiquer I, Navarro MP. Iron nutrition in adolescence. Crit Rev Food Sci Nutr. (2013) 53:1226–37. doi: 10.1080/10408398.2011.564333
42. Koot BG, van der Baan-Slootweg OH, Bohte AE, Nederveen AJ, van Werven JR, Tamminga-Smeulders CL, et al. Accuracy of prediction scores and novel biomarkers for predicting nonalcoholic fatty liver disease in obese children. Obesity (Silver Spring). (2013) 21:583–90. doi: 10.1002/oby.20173
43. Permutt Z, Le TA, Peterson MR, Seki E, Brenner DA, Sirlin C, et al. Correlation between liver histology and novel magnetic resonance imaging in adult patients with non-alcoholic fatty liver disease - MRI accurately quantifies hepatic steatosis in NAFLD. Aliment Pharmacol Ther. (2012) 36:22–9. doi: 10.1111/j.1365-2036.2012.05121.x
Keywords: liver fat content, serum ferritin, pediatric obesity, non-alcocholic fatty liver disease, pediatric nonalcoholic fatty liver disease
Citation: Mörwald K, Aigner E, Bergsten P, Brunner SM, Forslund A, Kullberg J, Ahlström H, Manell H, Roomp K, Schütz S, Zsoldos F, Renner W, Furthner D, Maruszczak K, Zandanell S, Weghuber D and Mangge H (2020) Serum Ferritin Correlates With Liver Fat in Male Adolescents With Obesity. Front. Endocrinol. 11:340. doi: 10.3389/fendo.2020.00340
Received: 11 February 2020; Accepted: 30 April 2020;
Published: 18 June 2020.
Edited by:
Claudio Chiesa, National Research Council (Cnr), ItalyReviewed by:
Chang-Mo Oh, Kyung Hee University, South KoreaPathik Mayur Parikh, Zydus Cadila, India
Ludovico Abenavoli, University of Catanzaro, Italy
Sanal MG, Institute of Liver and Biliary Sciences, India
Copyright © 2020 Mörwald, Aigner, Bergsten, Brunner, Forslund, Kullberg, Ahlström, Manell, Roomp, Schütz, Zsoldos, Renner, Furthner, Maruszczak, Zandanell, Weghuber and Mangge. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Weghuber, ZC53ZWdodWJlckBzYWxrLmF0
†Senior author