 Emma Eklund1
Emma Eklund1 Lena Ekström2John-Olof Thörngren2Magnus Ericsson2Bo Berglund3
Lena Ekström2John-Olof Thörngren2Magnus Ericsson2Bo Berglund3 Angelica Lindén Hirschberg1,4*
Angelica Lindén Hirschberg1,4*- 1Department of Women's and Children's Health, Division of Obstetrics and Gynecology, Karolinska Institutet, Stockholm, Sweden
- 2Department of Laboratory Medicine, Division of Clinical Pharmacology, Karolinska Institutet, Karolinska University Hospital, Stockholm, Sweden
- 3Department of Internal Medicine, Karolinska Institutet, Karolinska University Hospital Solna, Stockholm, Sweden
- 4Department of Gynecology and Reproductive Medicine, Karolinska University Hospital, Stockholm, Sweden
Background: The second to fourth digit ratio (2D:4D ratio) is suggested to be a negative correlate of prenatal testosterone. Little is known about the role of the 2D:4D ratio in relation to serum and urinary androgens for physical performance in female athletes. We aimed to compare the 2D:4D ratio in female Olympic athletes with sedentary controls, and to investigate the 2D:4D ratio in relation to serum and urinary androgens and physical performance in the athletes.
Methods: This cross-sectional study included 104 Swedish female Olympic athletes participating in power, endurance and technical sports and 117 sedentary controls. The 2D:4D ratio was calculated using direct digit measurements. Serum androgens and urinary androgen metabolites were analyzed by liquid chromatography-tandem mass spectrometry. The athletes performed standardized physical performance tests and body composition was established by dual-energy X-ray absorptiometry.
Results: The 2D:4D ratio was significantly lower in the athletes compared with controls although serum testosterone levels were comparable between groups and within normal reference values. The 2D:4D ratio correlated negatively with urinary levels of testosterone glucuronide and 5α- and 5βAdiol-17G, whereas there were no correlations to serum androgen levels. Furthermore, the 2D:4D ratio correlated negatively with strength tests and positively with 3,000-meter running in the athletes.
Conclusion: Female Olympic athletes had a lower 2D:4D ratio, possibly reflecting a higher prenatal androgen exposure, than sedentary controls. Furthermore, the 2D:4D ratio was related to urinary levels of androgen metabolites and physical performance in the athletes but not to serum androgen levels. It is suggested that the 2D:4D ratio could reflect androgen metabolism and may be of importance for sporting success in female athletes.
Introduction
Prenatal testosterone and estrogen levels are suggested to influence the formation of the second to fourth digit ratio (2D:4D ratio), with high environmental levels of androgens during fetal life being associated with a low 2D:4D ratio (1–3). However, this concept has recently been debated (4–7). The digit ratio, proposed as a sexually dimorphic trait (2, 8, 9), is believed to be set during the first trimester of fetal development (2, 10) and does not change substantially with age (9). Furthermore, the 2D:4D ratio has been associated with Differences of Sex Development (DSD) (11, 12).
The digit ratio has also been suggested to be related to physical performance (13, 14). Previous studies have shown that male athletes have a lower 2D:4D ratio than non-athletes (15–19). However, only a few previous studies have investigated the digit ratio in female athletes in comparison to controls (15, 19–21). An association between the 2D:4D ratio and physical performance have been demonstrated in female athletes for alpine skiing (18), endurance running (22) fencing (23) and rowing (24). Similarly, positive correlations between the 2D:4D ratio and physical fitness (25), and sporting ability (26) have been demonstrated in women taking part in leisure sports. These reports are either based on rather small study groups and/or not including populations of Olympic athletes.
Androgens are considered beneficial for athletic performance by exerting positive effects on muscle tissue, erythropoiesis, immune system, and behavioral patterns, and may also contribute to a decreased risk of injuries and increased health status in athletes (27). In women, the active androgens testosterone and dihydrotestosterone (DHT) are synthesized in the ovaries and the adrenal glands, and by conversion in peripheral tissue of precursor androgens produced in the adrenal cortex, such as androstenedione (A4), dehydroepiandrosterone (DHEA), its sulfate (DHEAS) and 5-androstene-3β, 17β-diol (5-DIOL) (28). Androgens are finally mainly metabolized by uridine diphospho (UDP)-glucuronosyl transferases (UGTs) and to some extent by sulfotransferases (SULTs) and excreted in urine (29).
We have recently published data showing that female Olympic athletes have higher levels of serum androgen precursors compared to controls and that serum androgens are positively associated with physical performance in the athletes (30). These results are of relevance for the ongoing discussion regarding hyperandrogenism in female athletes (27). Adult serum androgens have also been studied in relation to the 2D:4D ratio in non-athletic populations of men and women, demonstrating inconclusive results (31, 32). No previous studies have examined the 2D:4D ratio in relation to the androgen profile in both serum and urine, as well as physical performance in female top athletes.
The aim of the present study was to investigate the 2D:4D ratio in female Olympic athletes and untrained controls, and to study the 2D:4D ratio in relation to the androgen profile in serum and urine and physical performance in the athletes.
Materials and Methods
Study Population
The present study included a representative population of Swedish female Olympic athletes (n = 104) participating in the summer or winter Olympic games, and 117 controls, for whom digit measurements were obtained (30). The controls were age- and body mass index (BMI)—matched, having a maximum of 2 h endurance and/or strength training per week and no prior participation in elite level competition. All participants were > 18 years of age. Olympic athletes were recruited in connection with pre-Olympic training camps and controls recruited via advertisement (recruitment was conducted from November 2011 to April 2015). The subjects were investigated at the Women's Health Research Unit, Karolinska University Hospital or in connection with pre-Olympic training camps. All participants filled out a general health questionnaire including training hours per week, and hormonal contraceptive use and for the athletes' information concerning sport discipline, age at training debut and age at elite level debut was obtained. Data on menstrual function was collected via questionnaire and confirmed by measurement of serum hormones for participants not using hormonal contraceptives. Blood- and urine samples were collected in a fasted, rested state, between 07.00 and 10.00 am and stored at −20°C until further analysis.
The project was approved by the Regional Ethics Committee (EPN 2011/1426-32). Informed written consent was obtained from all participants.
2D:4D Ratio
Digit measurement expressed in millimeters (mm) was performed for digit two (2D) and digit four (4D) (Figure 1) using a Vernier digital caliper 0–150 mm (USA, Cocraft) with a precision of 0.01 mm. Digit length was directly measured from the mid-point of the proximal crease of the proximal phalanx to the distal tip of the distal phalanx for 2D and 4D (9, 15) on both left (n = 103 athletes, n = 116 controls) and right hand (n = 104 athletes, n = 117 controls). The 2D:4D ratio was calculated by dividing 2D length by 4D length. In addition, right minus left 2D:4D ratio (Dr-l), suggested as an additional negative marker for prenatal testosterone, was calculated (2). The digits were independently measured by two raters. For rater A, the intraobserver agreement was 0.90 for right hand and 0.90 for left hand. For rater B, the corresponding intraobserver agreement was 0.93 and 0.96, respectively. The inter-rater correlation was 0.87 for the right hand and 0.85 for the left hand (33).
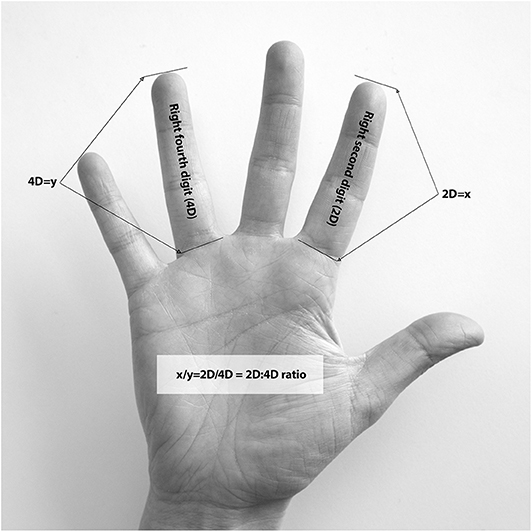
Figure 1. Measurement and calculation of the second to fourth digit (2D:4D) ratio.
Body Composition
For 65 athletes and 100 controls, body composition [bone mineral density (BMD) (g/cm2), fat mass (%), lean mass (kg)] was established by dual-energy X-ray absorptiometry (DXA), Lunar Prodigy Advance (GE Healthcare, Madison, WI) at the Karolinska University Hospital, Solna as previously described (30).
Physical Performance
Athletes were offered standardized physical performance tests managed by the SOC at Bosön, Stockholm, Sweden. They participated in physical performance tests measuring explosive power [countermovement jump (CMJ) (n = 57), squat jump (SJ) (n = 58)], strength (bench press (n = 45), chins (n = 49)) and 3,000 meters running (n = 20).
Serum Steroid Profile
Serum levels of androgens [testosterone, DHEA, DHEAS, DHT, A4 and 17- alpha-hydroxyprogesterone (17-OHP)] and estradiol (E2) were determined by liquid chromatography-tandem mass spectrometry (LC-MS/MS) at the Endoceutics laboratory, Quebec, Canada, as previously described (34). Free androgen index was calculated (testosterone nmol/L divided by sex hormone-binding globulin (SHBG) nmol/L * 100). Follicle- stimulating hormone (FSH), luteinizing hormone (LH), anti-müllerian hormone (AMH) and SHBG were determined by electrochemiluminiscence immunoassay at the Department of Clinical Chemistry, Karolinska University Hospital as previously described (30).
Urinary Steroid Profile
For 93 athletes, urinary samples were obtained and urinary levels of conjugated (glucuronide and sulfated) androgens [testosterone (T-G, T-S), epitestosterone (EpiT-G, EpiT-S), androsterone (ADT-G, ADT-S), etiocholanolone (Etio-G, Etio-S), DHEA-G, DHEA-S, 5α-androstane-diol (5αAdiol-3G and 5αAdiol-17G) and 5β-androstane-diol (5βAdiol- 3G and 5βAdiol-17G)] were determined by LC-MS/MS as previously described (35) at the accredited doping laboratory, Department of Laboratory Medicine, Karolinska Hospital Huddinge. Specific gravity (SG) was measured for all urine samples by a Digital Urine SG Refractometer (ATAGO UG1, Tokyo, Japan). Using a correction formula, Ccorrected = Cmeasured * ((1.020–1)/(SG−1)), each sample was corrected to a specific gravity of 1.020, adjusting for urine dilution. Limit of detection (LOD) was estimated to be below 0.4 μg/mL for all analytes. For two athletes a urine sample was not obtained and for nine athletes the amount of urine was insufficient for analysis. Testosterone:epitestosterone (T:E) ratio was calculated by dividing testosterone glucuronide (T-G) by epitestosterone glucuronide (EpiT-G).
Statistical Analyses
Statistical analyses were performed using Statistica™ 13 software (Statsoft® Inc., Tulsa, OK, USA). Continuous data was presented as mean ± SD or as median and interquartile range (25th−75th percentile) depending on distribution. Comparison of the 2D:4D ratio and body composition between groups was performed using the student's t-test. The proportion of women using hormonal contraceptives and having menstrual dysfunction was calculated by Chi-Square test and type of sport by Fisher's exact test. Effect size for continuous variables was calculated using Cohen's d and for categorical variables with Phi = √(Chi-2/n). Correlations were evaluated by Spearman's rank- order correlation or Pearson's correlation. P-values < 0.05 were considered significant.
Results
General Characteristics of Female Athletes and Controls
Female athletes and controls were similar regarding age and BMI (Table 1). As expected, training hours/week was significantly higher among athletes compared to controls (Table 1). Age at training debut was 9.34 ± 4.74 years and age at elite debut was 17.56 ± 3.32 years for the athletes. As previously published, hormonal contraceptive use was similar between groups, but menstrual dysfunction was significantly more common among female athletes compared to controls (30). Furthermore, the Olympic athletes demonstrated a more anabolic body composition, including higher total BMD, lower body fat percent and higher amount of lean mass compared to the controls (30) (Table 1). In addition, as previously published, the athletes had significantly lower levels of estrone and higher serum levels of the androgen precursors DHEA and 5-DIOL than controls (30). However, both groups had serum steroid levels within the normal range (30).
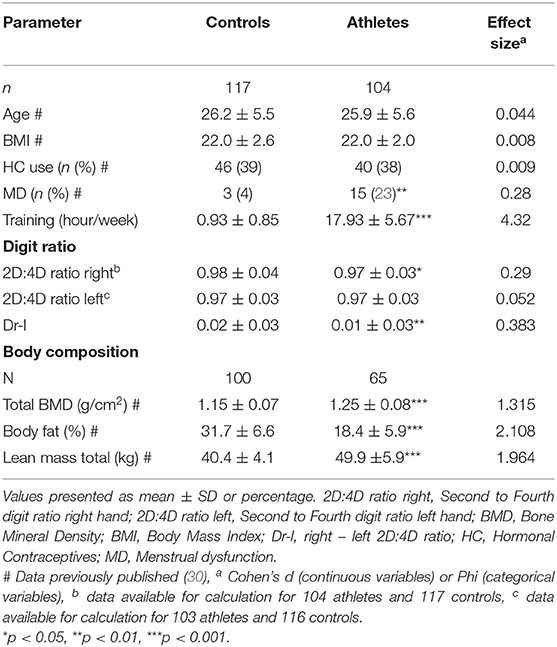
Table 1. General characteristics and body composition in Olympic athletes and controls.
2D:4D Ratio in Relation to Serum and Urinary Androgen Levels in Athletes and Controls
The 2D:4D ratio right hand was significantly lower in the female Olympic athletes than the controls (p < 0.05) (Table 1, Figure 2). Furthermore, the athletes demonstrated a significantly lower Dr-l compared to the controls (Table 1). No significant correlations were found between serum androgen levels and the 2D:4D ratio in the controls or the female Olympic athletes. However, in the athlete group, there were significant negative correlations between the 2D:4D ratio right hand and the urinary steroid metabolites T-G, 5αAdiol-17G and 5βAdiol-17G, see Figures 3A–C. However, there were no corresponding correlations for Dr-l.
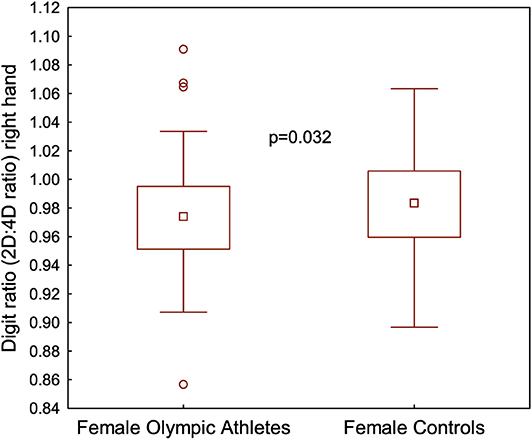
Figure 2. Digit ratio (2D:4D ratio) right hand expressed in millimeters (mm) for female Olympic athletes (n = 104) and female controls (n = 117).
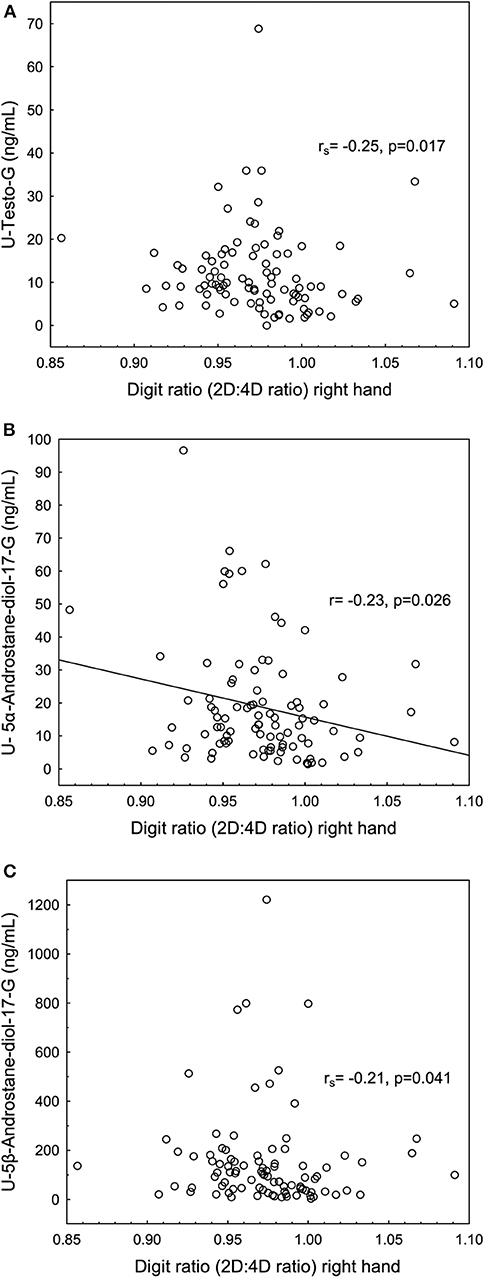
Figure 3. Significant negative correlations between the second to fourth digit ratio (2D:4D ratio) right hand expressed in millimeters (mm) and (A) urine testosterone glucuronide (U-Testo-G) (ng/mL), (B) U−5α- Androstane-diol-17G (5aAdiol- 17G) and (C) U-5β- Androstane-diol-17G (5βAdiol-17G) in female Olympic athletes.
2D:4D Ratio, Urinary Androgens and Physical Performance in Athletes
Significant negative correlations were found between the 2D:4D ratio right hand and bench press and chins, see Figures 4A,B and a significant positive correlation between the 2D:4D ratio right hand and 3,000 meters running performance see Figure 4C. No significant correlations were found between Dr-l and physical performance.
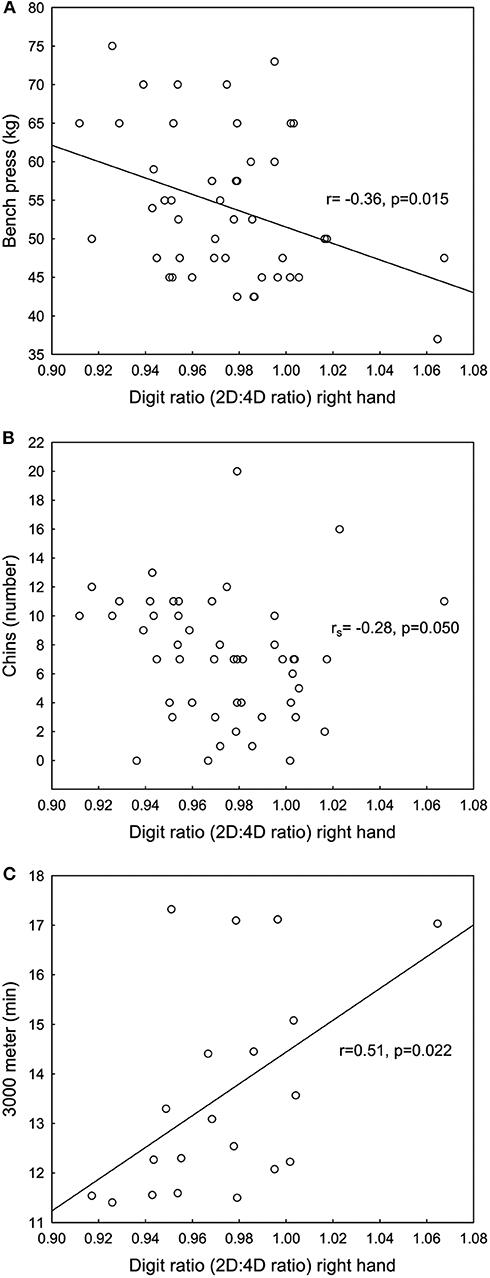
Figure 4. Significant negative correlations between the second to fourth digit ratio (2D:4D ratio) right hand and (A) bench press and (B) chins and a significant positive correlation between the 2D:4D ratio right hand and (C) 3,000 meters running measured in minutes for female Olympic athletes.
In turn, 5αAdiol-3G and 5βAdiol-17G correlated positively to chins (rs = 0.33, p < 0.05 and rs = 0.37, p < 0.05, respectively) and Etio-G correlated negatively to running time 3,000 m (rs = −0.51, p < 0.05).
Discussion
To our knowledge, this is the first study investigating the 2D:4D ratio in relation to both the serum and urinary androgen profile and physical performance in female top athletes. We found a lower 2D:4D ratio right hand, suggesting a higher prenatal androgen exposure, in female Olympic athletes than untrained controls. In addition, we found negative correlations between the 2D:4D ratio and the urinary steroid profile, and both these variables correlated significantly with physical performance including strength tests and middle-distance running in the female Olympic athletes.
Few previous investigations (15, 19–21) have reported data on the 2D:4D ratio in female athletes compared with controls. These studies have been performed in female athletes at national level (20), varsity athletes (non- elite athletes) (15), college tennis players (21) and youth handball players (19) demonstrating a significantly lower digit ratio for the athletes compared to controls. However, our study is the first including a large number of female Olympic athletes and untrained controls. In agreement with most previous studies, we found significant differences in the 2D:4D ratio only for the right hand (15, 19, 21). It has been demonstrated that the right hand shows a greater sex difference than the left hand leading to the suggestion that the right hand is more representative of prenatal androgen influence (8).
The relation between prenatal androgen exposure and the 2D:4D ratio is supported by an association between a low 2D:4D and high levels of fetal testosterone relative to estradiol in amniotic fluid in humans (1). Furthermore, male human fetuses have higher androgen levels in amniotic fluid (36) and significantly lower 2D:4D ratio than female fetuses (10). However, a relationship between the 2D:4D ratio and adult sex hormone levels have not been confirmed (31, 32). In agreement, we found no correlation between serum androgen levels and the 2D:4D ratio. More recent studies suggest that the digit ratio is not correlated to resting serum androgen levels, but could be associated with androgen levels in response to physical training (2, 37). However, in our study data was collected in a resting state and not in close connection to training or competition.
On the other hand, we found for the first time, significant negative correlations between the 2D:4D ratio and several urinary androgen metabolites (T-G, 5αAdiol-17G, 5βAdiol-17G). Our findings could reflect a possible difference in androgen phase II metabolism depending on 2D:4D ratio among female athletes. As opposed to the circulatory androgens, the urinary androgen concentrations are dependent on the expression and activity of phase II enzymes i.e., UGTs and SULTs. T-G, 5βAdiol-17G and 5αAdiol-17Gs are all conjugated at the 17β- OH-position preferable by UGT2B17, whereas T-G and 5αAdiol-17G may also be inactivated by UGT2B15, UGT2A1, and UGT1A4 (38, 39). The expression and activity of UGT2B17 and UGT2B15 are known to be higher in men than in women (40, 41). It is possible that polymorphisms in UGTs and other androgen metabolizing enzymes, as well as other factors that determine the expression and activity of UGTs, may be associated with the androgen load of the fetus in the first trimester. Several fetal UGTs are expressed already in the first trimester (42). Further studies are warranted to establish any putative link between phase II metabolism and the 2D:4D ratio.
In support of a role of prenatal androgen exposure for physical performance, we found significant correlations between the 2D:4D ratio and athletic performance tests in the Olympic athletes. Previous studies on 2D:4D ratio and physical performance have focused on male athletes (16, 17, 22), whereas there is more limited research in female athletes. The few previous studies in female athletes have demonstrated significant correlations between a lower 2D:4D ratio and faster rowing times (24), faster skiing times (18), better endurance running performance (22) and better national fencing rank (23). In our study of top-level female athletes, the 2D:4D ratio was significantly related to both strength tests and 3,000 m running, a test mainly representative of aerobic capacity.
There are several possible underlying mechanisms for the association between the 2D:4D ratio and athletic performance. We and others have previously demonstrated associations between adult serum androgen levels and muscle mass and strength in female athletes (30, 43, 44). However, we found no correlations between serum androgen levels and the 2D:4D ratio. In contrast, there were correlations between the 2D:4D ratio and urinary steroid metabolites, which in turn correlated to physical performance tests. As urinary androgen levels are dependent on androgen metabolizing enzymes, these urinary metabolites are more representative for the androgen metabolism than circulating androgens. Furthermore, the androgen metabolism is dependent on genetic variations. We hypothesize that genetic variation of the androgen metabolism and thereby androgen activity, could influence both the development of the 2D:4D ratio during fetal life and the predisposition for physical performance.
In conclusion, we found a lower 2D:4D ratio related to urinary androgen levels and physical performance in female Olympic athletes. The association between the digit ratio and urinary androgen levels, but not serum androgen levels, may indicate that the 2D:4D ratio reflects variations in androgen metabolism rather than absolute circulating androgen levels. A low digit ratio was associated with increased aerobic and strength performance in the athletes. Although the link between the 2D:4D ratio and physical performance, is still not fully clarified, our results suggest that prenatal androgen exposure, in addition to the adult androgen levels, may be of importance for athletic capacity in female Olympic athletes.
Data Availability Statement
All datasets generated for this study are included in the article/supplementary material.
Ethics Statement
The studies involving human participants were reviewed and approved by the Regional Ethics Committee (EPN 2011/1426-32). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
EE, BB, and AH were involved in the concept/design of the study, acquisition of data, and data analysis. J-OT and ME performed the quantification of urinary androgens. EE, BB, LE, J-OT, ME, and AH were involved in the manuscript preparation, critical revision of the article and approval of the article. All authors listed met the conditions required for full authorship.
Funding
The study was financed by grants from the Swedish Research Council (2017-02051), the Swedish Research Council for Sport Science, the Clinical Scientist Training Programme and the clinical research internship programme, Karolinska Institutet.
Conflict of Interest
BB is the medical director for the Swedish Olympic Committee (SOC) and AH is medical adviser to the SOC, the International Association of Athletic Federation (IAAF) and the International Olympic Committee (IOC). The results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank research midwifes, Berit Legerstam and Liselott Blomberg at the Women's Health Research Unit, Karolinska University Hospital for their support and help with collecting data. We would also like to thank coaches and athletes for their help, curiosity and inspiration. Furthermore, we thank laboratory technicians at the Doping laboratory for their help with urinary analyses, statistician Elisabeth Berg for knowledge and continuous help with statistical analyses and the SOC for support and promotion of this scientific work.
References
1. Lutchmaya S, Baron-Cohen S, Raggatt P, Knickmeyer R, Manning JT. 2nd to 4th digit ratios, fetal testosterone and estradiol. Early Hum Dev. (2004) 77:23–8. doi: 10.1016/j.earlhumdev.2003.12.002
2. Manning J, Kilduff L, Cook C, Crewther B, Fink B. Digit ratio (2D:4D): a biomarker for prenatal sex steroids and adult sex steroids in challenge situations. Front Endocrinol. (2014) 5:9. doi: 10.3389/fendo.2014.00009
3. Zheng Z, Cohn MJ. Developmental basis of sexually dimorphic digit ratios. Proc Natl Acad Sci USA. (2011) 108:16289–94. doi: 10.1073/pnas.1108312108
4. Swift-Gallant A, Johnson BA, Di Rita V, Breedlove SM. Through a glass, darkly: human digit ratios reflect prenatal androgens, imperfectly. Horm Behav. (2020) 120:104686. doi: 10.1016/j.yhbeh.2020.104686
5. McCormick CM, Carre JM. Facing off with the phalangeal phenomenon and editorial policies: a commentary on swift-gallant, Johnson, Di Rita and Breedlove 2020. Horm Behav. (2020) 120:104710. doi: 10.1016/j.yhbeh.2020.104710
6. Richards G. What is the evidence for a link between digit ratio (2D:4D) and direct measures of prenatal sex hormones? Early Hum Dev. (2017) 113:71–2. doi: 10.1016/j.earlhumdev.2017.08.003
7. Manning JT, Fink B. Are there any “direct” human studies of digit ratio (2D:4D) and measures of prenatal sex hormones? Early Hum Dev. (2017) 113:73–4. doi: 10.1016/j.earlhumdev.2017.09.003
8. Hönekopp J, Watson S. Meta-analysis of digit ratio 2D:4D shows greater sex difference in the right hand. Am J Hum Biol. (2010) 22:619–30. doi: 10.1002/ajhb.21054
9. Manning JT, Scutt D, Wilson J, Lewis-Jones DI. The ratio of 2nd to 4th digit length: a predictor of sperm numbers and concentrations of testosterone, luteinizing hormone and oestrogen. Human Reprod. (1998) 13:3000–4. doi: 10.1093/humrep/13.11.3000
10. Malas MA, Dogan S, Evcil EH, Desdicioglu K. Fetal development of the hand, digits and digit ratio (2D:4D). Early Hum Dev. (2006) 82:469–75. doi: 10.1016/j.earlhumdev.2005.12.002
11. Rivas MP, Moreira LM, Santo LD, Marques AC, El-Hani CN, Toralles MB. New studies of second and fourth digit ratio as a morphogenetic trait in subjects with congenital adrenal hyperplasia. Am J Hum Biol. (2014) 26:559–61. doi: 10.1002/ajhb.22545
12. van Hemmen J, Cohen-Kettenis PT, Steensma TD, Veltman DJ, Bakker J. Do sex differences in CEOAEs and 2D:4D ratios reflect androgen exposure? A study in women with complete androgen insensitivity syndrome. Biol Sex Differ. (2017) 8:11. doi: 10.1186/s13293-017-0132-z
13. Tester N, Campbell A. Sporting achievement: what is the contribution of digit ratio? J Pers. (2007) 75:663–77. doi: 10.1111/j.1467-6494.2007.00452.x
14. Hönekopp J, Schuster M. A meta-analysis on 2D:4D and athletic prowess: Substantial relationships but neither hand out-predicts the other. Personal Individual Diff. (2010) 48:4–10. doi: 10.1016/j.paid.2009.08.009
15. Giffin NA, Kennedy RM, Jones ME, Barber CA. Varsity athletes have lower 2D:4D ratios than other university students. J Sports Sci. (2012) 30:135–8. doi: 10.1080/02640414.2011.630744
16. Bennett M, Manning JT, Cook CJ, Kilduff LP. Digit ratio (2D:4D) and performance in elite rugby players. J Sports Sci. (2010) 28:1415–21. doi: 10.1080/02640414.2010.510143
17. Manning JT, Taylor RP. Second to fourth digit ratio and male ability in sport: implications for sexual selection in humans. Evol Hum Behav. (2001) 22:61–9 doi: 10.1016/S1090-5138(00)00063-5
18. Manning JT. The ratio of 2nd to 4th digit length and performance in skiing. J Sports Med Phys Fit. (2002) 42:446–50.
19. Baker J, Kungl AM, Pabst J, Strauss B, Busch D, Schorer J. Your fate is in your hands? Handedness, digit ratio. (2D:4D), and selection to a national talent development system. Laterality. (2013) 18:710–8. doi: 10.1080/1357650X.2012.755992
20. Pokrywka L, Rachon D, Suchecka-Rachon K, Bitel L. The second to fourth digit ratio in elite and non-elite female athletes. Am J Hum Biol. (2005) 17:796–800. doi: 10.1002/ajhb.20449
21. Hsu CC, Su B, Kan NW, Lai SL, Fong TH, Chi CP, et al. Elite collegiate tennis athletes have lower 2D: 4D ratios than those of nonathlete controls. J Strength Condit Res Natl Strength Condition Assoc. (2015) 29:822–5. doi: 10.1519/JSC.0000000000000681
22. Manning JT, Morris L, Caswell N. Endurance running and digit ratio (2D:4D): implications for fetal testosterone effects on running speed and vascular health. Am J Hum Biol. (2007) 19:416–21. doi: 10.1002/ajhb.20603
23. Voracek M, Reimer B, Dressler SG. Digit ratio (2D:4D) predicts sporting success among female fencers independent from physical, experience, and personality factors. Scand J Med Sci Sports. (2010) 20:853–60. doi: 10.1111/j.1600-0838.2009.01031.x
24. Hull MJ, Schranz NK, Manning JT, Tomkinson GR. Relationships between digit ratio (2D:4D) and female competitive rowing performance. Am J Hum Biol. (2015) 27:157–63. doi: 10.1002/ajhb.22627
25. Hönekopp J, J TM, Muller C. Digit ratio (2D:4D) and physical fitness in males and females: evidence for effects of prenatal androgens on sexually selected traits. Horm Behav. (2006) 49:545–9. doi: 10.1016/j.yhbeh.2005.11.006
26. Paul SN, Kato BS, Hunkin JL, Vivekanandan S, Spector TD. The big finger: the second to fourth digit ratio is a predictor of sporting ability in women. Br J Sports Med. (2006) 40:981–3. doi: 10.1136/bjsm.2006.027193
27. Handelsman DJ, Hirschberg AL, Bermon S. Circulating testosterone as the hormonal basis of sex differences in athletic performance. Endocr Rev. (2018) 39:803–29. doi: 10.1210/er.2018-00020
28. Burger HG. Androgen production in women. Fertil Steril. (2002) 77 (Suppl. 4):S3–5 doi: 10.1016/S0015-0282(02)02985-0
29. W.Schänzer. Metabolism of anabolic androgen steroids. Clin Chem. (1996) 42:1001–20. doi: 10.1093/clinchem/42.7.1001
30. Eklund E, Berglund B, Labrie F, Carlstrom K, Ekstrom L, Hirschberg AL. Serum androgen profile and physical performance in women Olympic athletes. Br J Sports Med. (2017) 51:1301–8. doi: 10.1136/bjsports-2017-097582
31. Muller DC, Giles GG, Bassett J, Morris HA, Manning JT, Hopper JL, et al. Second to fourth digit ratio (2D:4D) and concentrations of circulating sex hormones in adulthood. Reprod Biol Endocrinol. (2011) 9:57. doi: 10.1186/1477-7827-9-57
32. Hönekopp J, Bartholdt L, Beier L, Liebert A. Second to fourth digit length ratio (2D:4D) and adult sex hormone levels: new data and a meta-analytic review. Psychoneuroendocrinology. (2007) 32:313–21. doi: 10.1016/j.psyneuen.2007.01.007
33. Savic I, Frisen L, Manzouri A, Nordenstrom A, Linden Hirschberg A. Role of testosterone and Y chromosome genes for the masculinization of the human brain. Human Brain Mapp. (2017) 38:1801–14. doi: 10.1002/hbm.23483
34. Ke Y, Bertin J, Gonthier R, Simard JN, Labrie F. A sensitive, simple and robust LC-MS/MS method for the simultaneous quantification of seven androgen- and estrogen-related steroids in postmenopausal serum. J Steroid Biochem Mol Biol. (2014) 144 Pt B:523–34. doi: 10.1016/j.jsbmb.2014.08.015
35. Mullen JE, Thorngren JO, Schulze JJ, Ericsson M, Garevik N, Lehtihet M, et al. Urinary steroid profile in females - the impact of menstrual cycle and emergency contraceptives. Drug Test Anal. (2016) 9:1034–42. doi: 10.1002/dta.2121
36. van de Beek C, Thijssen JH, Cohen-Kettenis PT, van Goozen SH, Buitelaar JK. Relationships between sex hormones assessed in amniotic fluid, and maternal and umbilical cord serum: what is the best source of information to investigate the effects of fetal hormonal exposure? Horm Behav. (2004) 46:663–9. doi: 10.1016/j.yhbeh.2004.06.010
37. Crewther BT, Cook CJ. The digit ratio (2D:4D) relationship with testosterone is moderated by physical training: evidence of prenatal organizational influences on activational patterns of adult testosterone in physically-active women. Early Hum Dev. (2019) 131:51–5. doi: 10.1016/j.earlhumdev.2019.02.008
38. Sten T, Kurkela M, Kuuranne T, Leinonen A, Finel M. UDP-glucuronosyltransferases in conjugation of 5alpha- and 5beta-androstane steroids. Drug Metab Dispos. (2009) 37:2221–7. doi: 10.1124/dmd.109.029231
39. Turgeon D, Carrier JS, Levesque E, Hum DW, Belanger A. Relative enzymatic activity, protein stability, and tissue distribution of human steroid-metabolizing UGT2B subfamily members. Endocrinology. (2001) 142:778–87. doi: 10.1210/endo.142.2.7958
40. Gallagher CJ, Balliet RM, Sun D, Chen G, Lazarus P. Sex differences in UDP-glucuronosyltransferase 2B17 expression and activity. Drug Metab Dispos. (2010) 38:2204–9. doi: 10.1124/dmd.110.035345
41. Ekstrom L, Gok E, Johansson M, Garle M, Rane A, Schulze J. Doping and genetic testing: sex difference in UGT2B15 expression, testosterone glucuronidation activity and urinary testosterone/ epitestosterone glucuronide ratio. Curr Pharmacogenom Personal Med. (2012) 10:125–31. doi: 10.2174/187569212800626403
42. Ekstrom L, Johansson M, Rane A. Tissue distribution and relative gene expression of UDP-glucuronosyltransferases (2B7, 2B15, 2B17) in the human fetus. Drug Metab Dispos. (2013) 41:291–5. doi: 10.1124/dmd.112.049197
43. Hagmar M, Berglund B, Brismar K, Hirschberg AL. Hyperandrogenism may explain reproductive dysfunction in olympic athletes. Med Sci Sports Exerc. (2009) 41:1241–8. doi: 10.1249/MSS.0b013e318195a21a
Keywords: 2D:4D ratio, testosterone, physical performance, androgen metabolites, female athletes
Citation: Eklund E, Ekström L, Thörngren J-O, Ericsson M, Berglund B and Hirschberg AL (2020) Digit Ratio (2D:4D) and Physical Performance in Female Olympic Athletes. Front. Endocrinol. 11:292. doi: 10.3389/fendo.2020.00292
Received: 18 November 2019; Accepted: 17 April 2020;
Published: 12 May 2020.
Edited by:
Flavio Adsuara Cadegiani, Federal University of São Paulo, BrazilReviewed by:
Martin Voracek, University of Vienna, AustriaJohn Thomas Manning, Swansea University, United Kingdom
Copyright © 2020 Eklund, Ekström, Thörngren, Ericsson, Berglund and Hirschberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Angelica Lindén Hirschberg, YW5nZWxpY2EubGluZGVuLWhpcnNjaGJlcmdAc2xsLnNl