 Jingxin Mao
Jingxin Mao Qinghai Zhang
Qinghai Zhang Haiyan Zhang
Haiyan Zhang Ke Zheng5
Ke Zheng5 Rui Wang
Rui Wang Guoze Wang
Guoze Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Endocrinol. , 15 May 2020
Sec. Thyroid Endocrinology
Volume 11 - 2020 | https://doi.org/10.3389/fendo.2020.00265
Purpose: To explore the risk factors that may predict the lymph node metastasis potential of these lesions and new prevention strategies in papillary thyroid carcinoma patients.
Materials and Methods: In total, 9,369 papillary thyroid carcinoma patients with 37.17% lymph node metastasis were analyzed (Revman 5.3 software) in this study. The PubMed and Embase databases were used for searching works systematically that were published through to January 22, 2020.
Results: Several factors were related to the increased risk of lymph node metastasis in patients with papillary thyroid carcinoma: age <45 years (pooled OR = 1.52, 95% CI = 1.14–2.01, p <0.00001); gender = male (pooled OR = 1.68, 95% CI = 1.51–1.87, p <0.00001); multifocality (pooled OR = 2.05, 95% CI = 1.45–2.89, p <0.0001); tumor size ≥1.0 cm (pooled OR = 3.53, 95% CI = 2.62–4.76, p <0.00001); tumor location at the upper pole 1/3 (pooled OR =1.46, 95% CI = 1.04–2.04, p = 0.03); capsular invasion + (pooled OR = 3.48, 95% CI = 1.69–7.54, p = 0.002); and extrathyroidal extension + (pooled OR = 2.03, 95% CI= 1.78–2.31, p <0.00001). However, tumor bilaterality (pooled OR = 0.85, 95% CI = 0.54–1.34, p = 0.49) and Hashimoto's thyroditis (pooled OR = 1.08, 95% CI = 0.79–1.49, p = 0.62) showed no correlation with lymph node metastasis in papillary thyroid carcinoma patients.
Conclusion: The systematic review and meta-analysis defined several significant risk factors of lymph node metastasis in papillary thyroid cancer patients: age (<45 years), gender (male), multifocality, tumor size (>1 cm), tumor location (1/3 upper), capsular invasion, and extra thyroidal extension. Bilateral tumors and Hashimoto's thyroiditis were unrelated to lymph node metastasis in patients with papillary thyroid cancer.
Thyroid carcinoma (TC) is the most frequent endocrine malignancy, accounting for approximately 3.8% of all newly diagnosed cancer (1). The incidence of TC has increased rapidly in recent 30 years with a female to male ratio of 3:1 (2, 3). Papillary thyroid carcinoma (PTC), medullary thyroid carcinoma (MTC), follicular thyroid carcinoma (FTC), and ana-plastic thyroid carcinoma (ATC) are the four main types of thyroid carcinoma (4). In addition, papillary thyroid microcarcinoma (PTMC) belongs to PTC. According to the histological classification of thyroid tumors by the World Health Organization (WHO), PTMC is defined as tumors with a maximum size of 10 mm or smaller (5). PTC is also the most familiar type of thyroid carcinoma, accounting for nearly 90% of all thyroid carcinomas with excellent prognoses (6). The general 10-year survival rate for middle-aged person with PTC is about from 80 to 95%, which is also related to an indolent clinical course (7).
Ultrasonography (US) and contrast-enhanced computerized tomography (CT) are commonly used but not especially accurate in clinical diagnosis of PTC, with low sensitivities of 38.9 and 27.5%, respectively (8). Following American Thyroid Association (ATA), fine-needle aspiration biopsy (FNAB) is considered to be the primary means of identifying benign and malignant nodules and selecting patients for surgery in clinical practice (9). In clinically diagnosis, the US or CT assistance during FNAB may enhance precision of cytological sampling and confirm nodal metastasis and may thus significantly reduce the false-negative diagnostic rate (10, 11).
Nowadays, the main treatment of primary/recurrent/advanced PTC is still reliant on surgical resection of total thyroidectomy (TT) (12). The radioiodine ablation (RAI) and lifelong levothyroxine therapy are commonly performed in intermediate- and high-risk patients (13). Although, PTC exhibit indolent behavior and bring a relatively low disease-specific mortality, with early-dissemination to local lymph nodes and oppression to organs, recurrence is comparatively common locally and distantly (14). In addition, the identification of risk factors of PTC is helpful for surgeons to evaluate the status of lymph nodes in PTC patients and determine whether preventive central lymph node dissection (CLND) is needed (15). Therefore, there is an urgent need for the identification risk factors that may predict the metastasis potential of these lesions and new prevention strategies. We conducted a systematic review and meta-analysis to assess the clinical characteristics of patients with PTC.
The relevant published articles, including those of the PubMed and Embase databases, were used for identification up until January 22, 2020. The following keywords were used in searching: “risk factor OR predictive factor” AND “papillary thyroid carcinoma OR papillary thyroid microcarcinoma OR PTC OR PTMC.” Relevant articles were used to broaden the search scope, and all retrieved studies, reviews, and conference abstracts were retrieved by the computer. If multiple published studies describe the same population, we extracted only the most complete or recent one. Two authors (Jing-xin Mao and Qing-hai Zhang) independently completed the selection process and resolved the differences through discussion.
The selection strategy used the several criteria: (a) prospective or retrospective original studies; (b) English language studies; (c) pathological confirmation of PTC during or after operation; and (d) available data on PTC risk factors and sufficient forms of data extraction to calculate the pooled OR.
Several exclusion criteria were adapted to exclude studies from meta-analysis: (a) reviews, case reports, editorials, letters to editors, meetings, or conference records; (b) studies included patients with thyroid cancer (e.g., FTC, MTC, or ATC) other than PTC; (c) insufficient data (e.g., <30 patients in the research); (d) research using big data (e.g., using SEER study data); (e) patients with a family history of thyroid cancer; and (f) studying period beyond 15 years.
Two authors (Ke Zheng and Rui Wang) abstracted the following data from the included articles: first author, countries of study, years of publication, study design, study population (PTC or PTMC), number of cases, surgical intervention, and PTC-related risk factors. Age, gender, multifocal, tumor size, location, vascular invasion, thyroiditis (ETE), bilateral, and Hashimoto's thyroiditis (HT) were the risk factors of LNM in PTC patients. The Newcastle-Ottawa quality assessment scale was used to assess the quality of the research (16).
Statistical analysis of all meta analyses were performed using Ravman Manager version 5.3 (Cochrane Collaboration, Oxford, UK). The magnitude of the effect of each study was calculated by the odds ratio (OR) or the weighted mean difference (WMD) of the 95% confidence interval (CI) briefly. A p-value of <0.05 was considered statistically significant unless otherwise specified. In addition, the heterogeneity was quantified using the Q-test and the I2 statistic. When p > 0.1 and I2 <50%, a fixed-effect model was applied; otherwise, a random-effects model was used. The Begg funnel plot was used to test for possible publication bias.
After searching, a total of 2,375 studies were initially considered for inclusion in the meta-analysis. A total of 287 studies were excluded due to language and repetition. In addition, 394 studies were excluded in the form of reviews, case reports, editorials, letters to the editor, and summaries of conference or meeting proceedings. After investigating the titles and abstracts of the remaining 1,640 studies, a full review of 54 articles were evaluated. After a full review, a total of 21 studies that met our selection criteria were finally included in our meta-analysis. The selection flowchart of research is presented in Figure 1. The basic characteristics of the studies was included in Table 1. In all the risk factor analyses, no significant asymmetry was found in Begg's funnel plot.
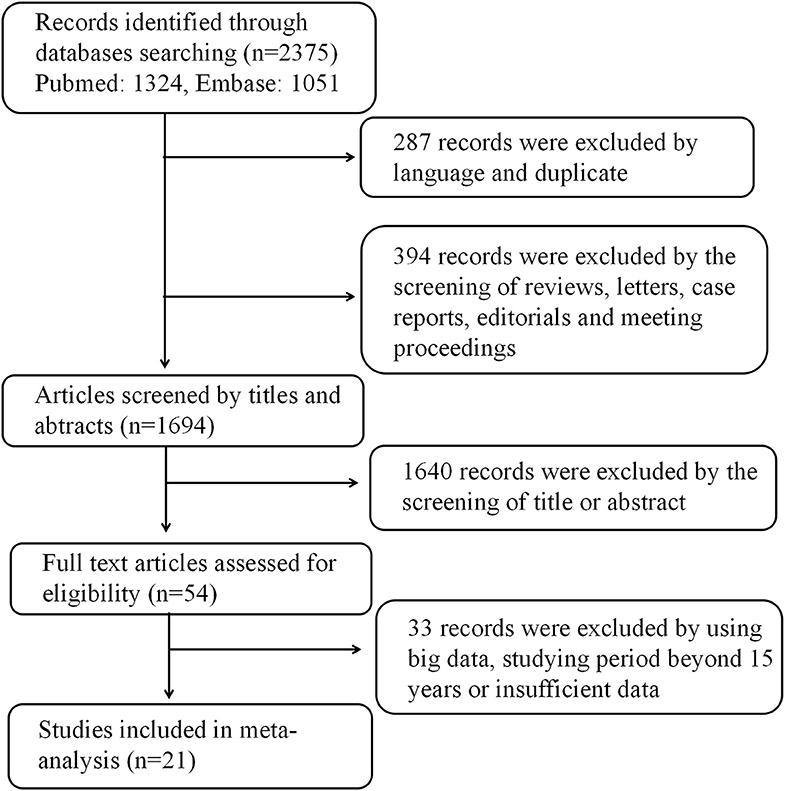
Figure 1. Flow chart of the study selection process.
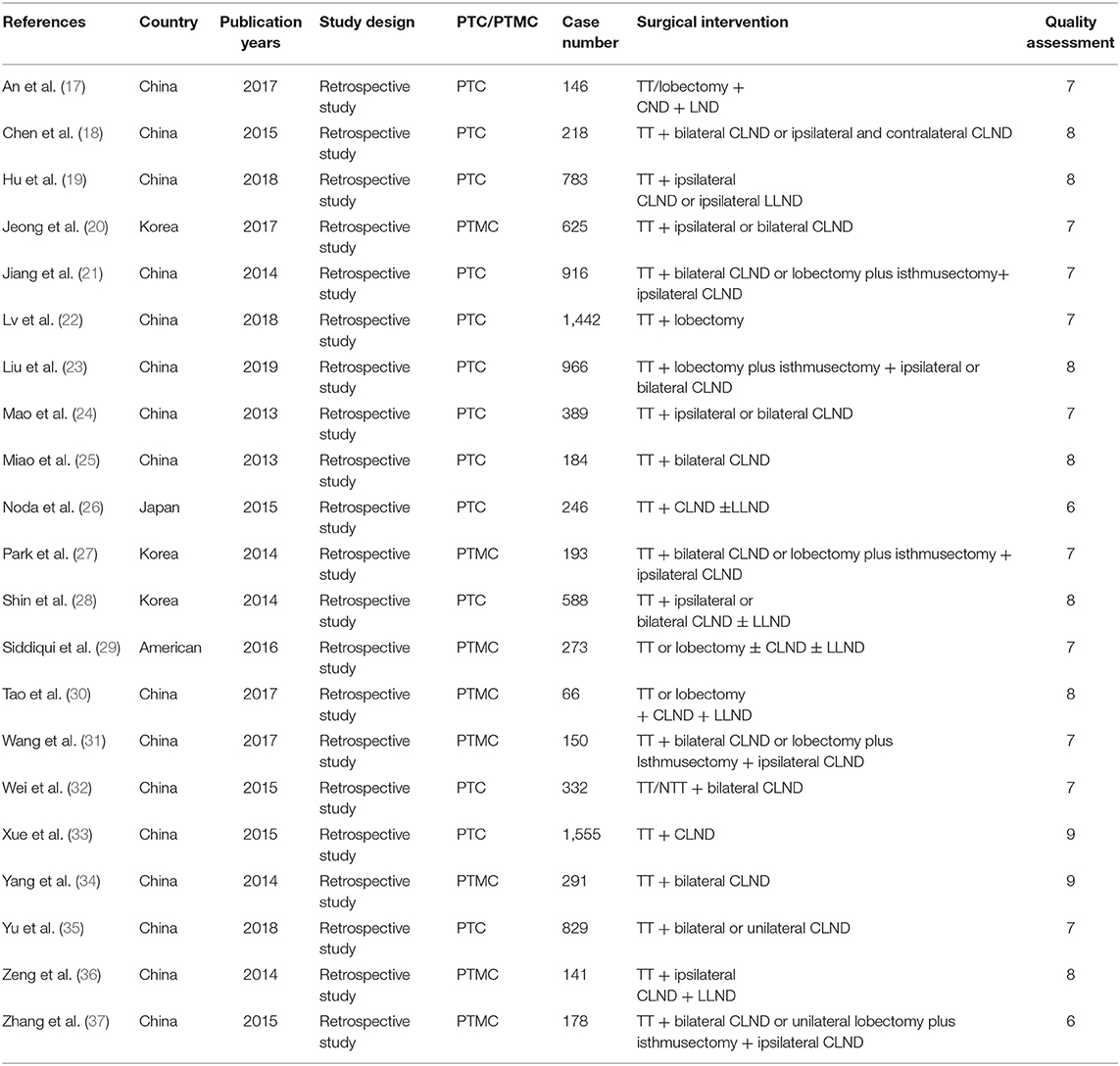
Table 1. Basic characteristics of included studies.
The prevalence of LNM population was clinicopathological variable in each study, ranging from 13.94 to 63.72%. Overall, LNM was confirmed among 3,482 patients of totally 9,369 PTC patients in this systematic review and meta-analysis.
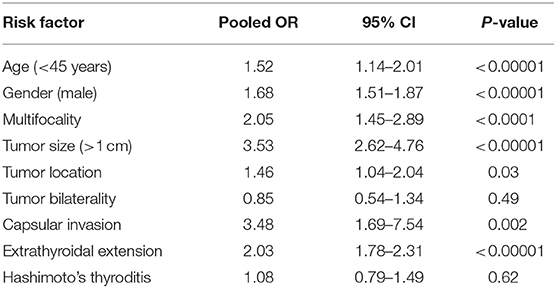
Table 2. Risk factors for lymph node metastasis in PTC patients.
A random-effects model was utilized in the analysis (p = 0.004, I2 = 89%). Among patients with PTC, the rate of LNM was 40.12% in patients <45 years and 34.25% in the patients ≥45 years. The results indicated that age <45 years was related to an increased rate of LNM in PTC patients (pooled OR = 1.52, 95% CI = 1.14–2.01, p <0.00001) (Figure 2).
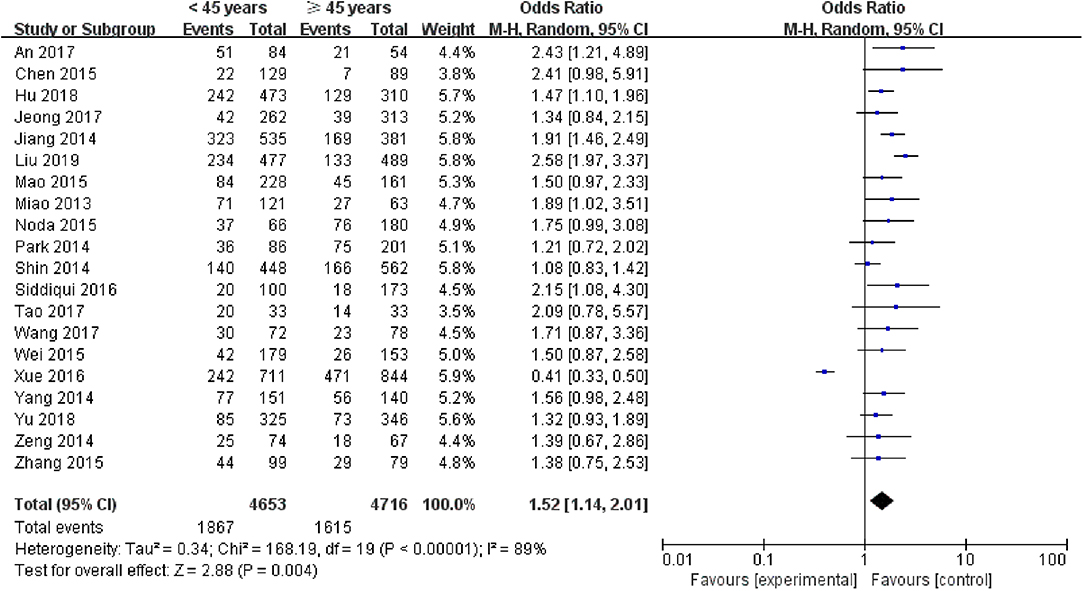
Figure 2. Forest plots of the association between age and PTC.
A fixed-effects model was applied to analyze the data (p = 0.03, I2 = 44%). The prevalence of LNM in male PTC patients was significantly higher than that in female PTC patients (pooled OR = 1.68, 95% CI = 1.51–1.87, p <0.00001) (Figure 3).
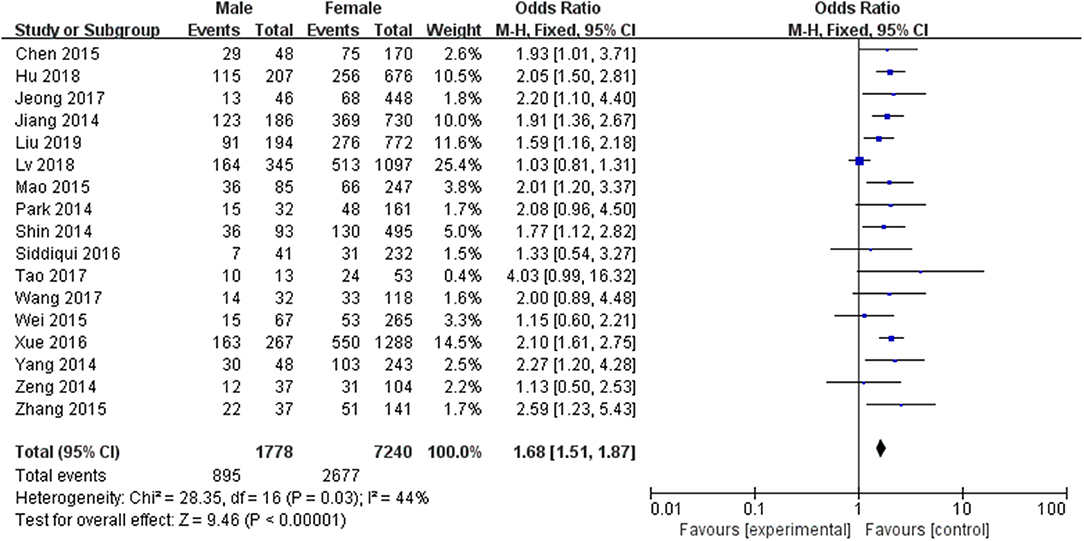
Figure 3. Forest plots of the association between gender and PTC.
A random-effects model was utilized in the analysis (p <0.00001, I2 = 89%). Thirteen included studies were evaluated. It was indicated that multifocality was significantly higher in association with LNM in PTC patients (pooled OR = 2.05, 95% CI = 1.45–2.89, p <0.0001) (Figure 4)
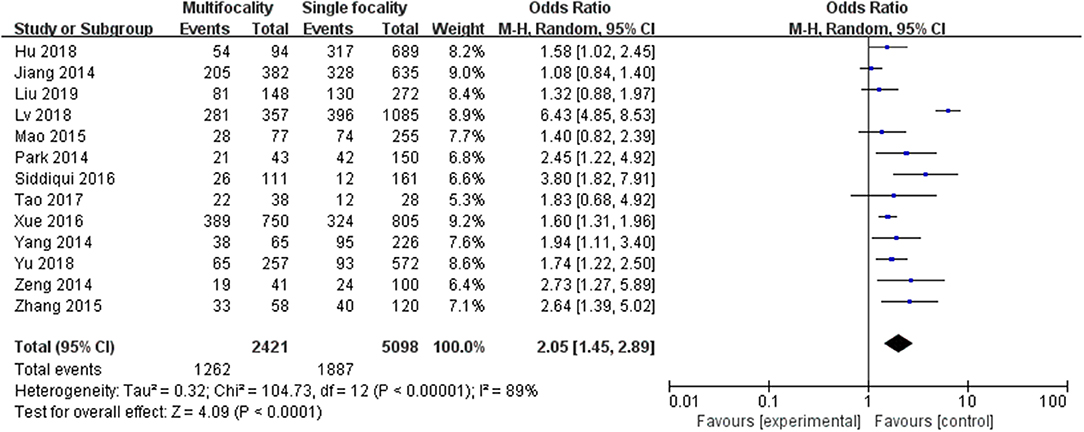
Figure 4. Forest plots of the association between multifocality and PTC.
A random-effects model was utilized to analyze the data (p <0.0001, I2 = 79%). Eight included studies were investigated. It was found that tumor size ≥1.0 cm was associated with a significantly higher LNM for PTC than tumors <1.0 cm (pooled OR = 3.53, 95% CI = 2.62–4.76, p <0.00001) (Figure 5).
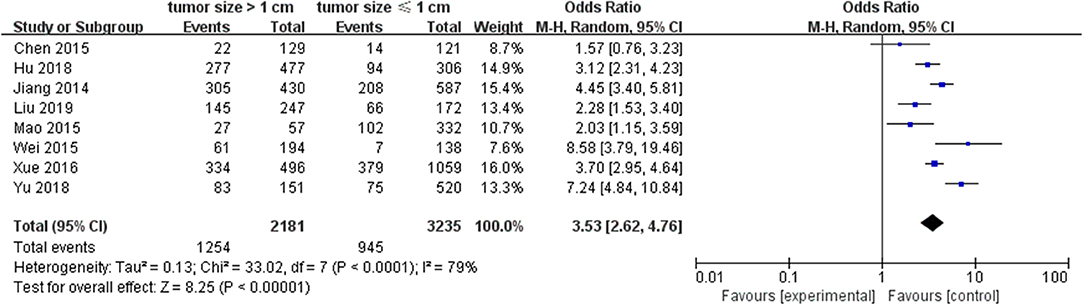
Figure 5. Forest plots of the association between tumor size and PTC.
A random-effects model was applied in the analysis (p = 0.0003, I2 = 78%). Thyroid were divided into three areas including upper pole, middle pole, and lower pole. The upper pole 1/3 is divided into one category, and the middle and lower pole 2/3 are divided into one category. It was found that upper pole 1/3 was significantly associated with a high rate of LNM in PTC patients (pooled OR = 1.46, 95% CI = 1.04–2.04, p = 0.03) (Figure 6).
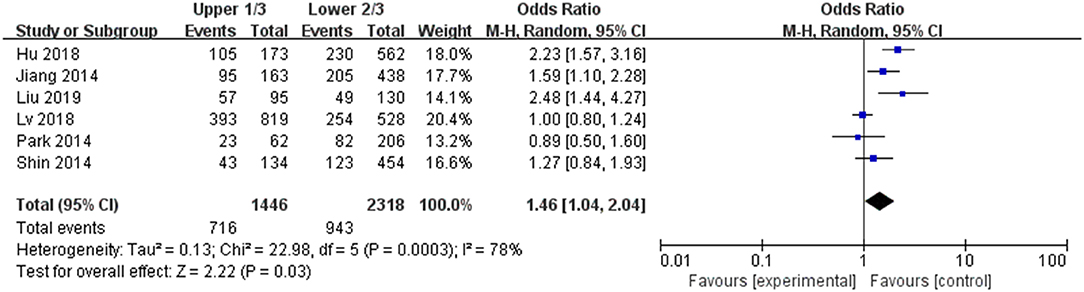
Figure 6. Forest plots of the association between location and PTC.
A fixed-effects model was utilized to analyze the data (p <0.00001, I2 = 84%). Eight included studies were evaluated for tumor bilaterality. It was found that both of unilateral tumors and bilateral tumors were not related to LNM in PTC patients (pooled OR = 0.85, 95% CI = 0.54–1.34, p = 0.49) (Figure 7).
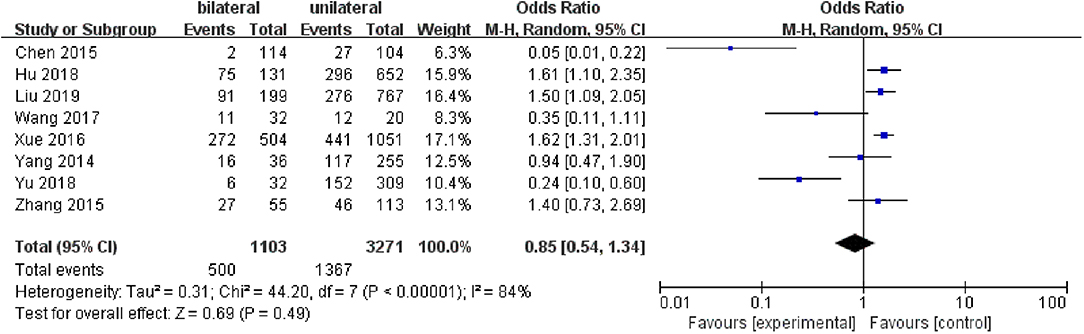
Figure 7. Forest plots of the association between bilateral tumors and PTC.
A fixed-effects model was applied in the analysis involving capsular invasion (p <0.00001, I2 = 91%). Five included studies were investigated. Capsular invasion exhibited a relatively high odds ratio for LNM in PTC patients (pooled OR = 3.48, 95% CI = 1.69–7.54, p = 0.002) (Figure 8).
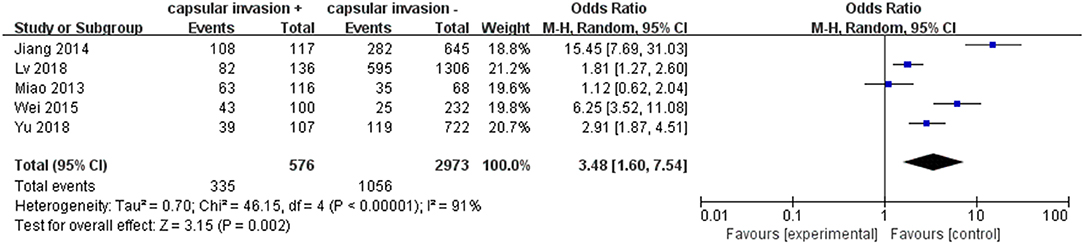
Figure 8. Forest plots of the association between capsular invasion and PTC.
A random-effects model was used to analyze the data (p = 0.45, I2 = 0%). Eight included studies were investigated in this analysis. ETE was related to LNM in PTC patients (pooled OR = 2.03, 95% CI = 1.78–2.31, p <0.00001) (Figure 9).
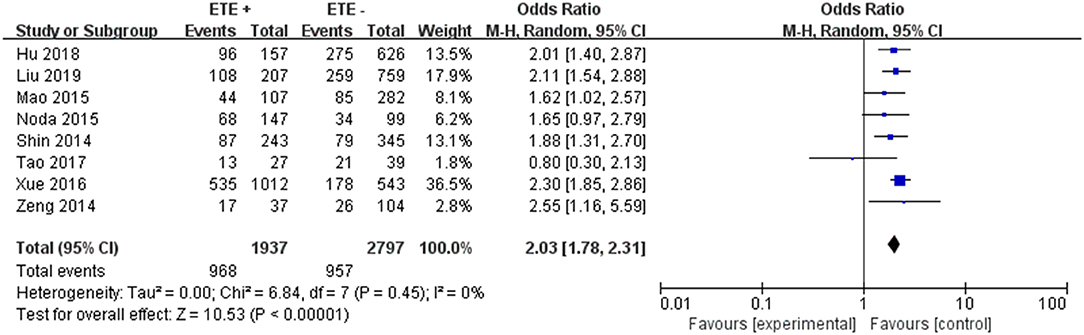
Figure 9. Forest plots of the association between ETE and PTC.
A fixed-effects model was utilized in the analysis (p = 0.02, I2 = 67%). It was demonstrated that Hashimoto's thyroditis was not significantly related to LNM in PTC patients (pooled OR = 1.08, 95% CI = 0.79–1.49, p = 0.62) (Figure 10).
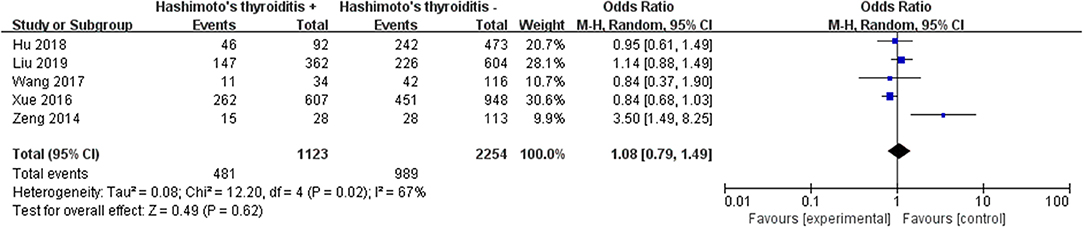
Figure 10. Forest plots of the association between HT and PTC.
PTC derived from follicular cells is considered to be the most common malignant thyroid tumor, mostly occurring between 30 and 40 years old, and its 10-year survival rate is above 95% (38). However, PTC is also a common thyroid cancer that is considered to be the biological characteristic of metastasizing to the surrounding neck lymph nodes (39). In addition, lymph node metastasis has been reported as a major risk factor for recurrence in PTC patients who had regional at the time of diagnosis (40). According to the malignant results of preoperative US and FNA biopsy (e.g., whether lymph nodes metastasis was confirmed), the surgical treatment of patients was finally evaluated. Moreover, although PTC is considered to be a benign tumor that may have a good response to the treatment, some still develop recurrences that may be fatal (41). Therefore, it is necessary to continuously improve risk stratification system clinicopathological features of PTC that are associated with LNM.
A systematic review was conducted using Ravman Manager version 5.3 for systematic reviews and meta-analysis. In the meta-analysis we carried out, LNM was surveyed in 36.12% of patients with PTC. Patients with PTMC were also included in our review. In the present study, LNM was significantly related to the following clinicopathologic risk factors: age, gender, tumor size, tumor location, multifocality, capsular invasion, and ETE.
Age is a major prognostic factor for risk of LNM and recurrence in patients with PTC (42). Previous meta-analysis also demonstrated that age <45 years was related to the increased risk of LNM in PTC patients (43). In the present meta-analysis, it indicated that the patients age <45 years with PTC may have the increased risk of LNM in clinical practice (pooled OR = 1.52). Even though age ≥45 years is usually associated with a poor prognosis (LNM) and increased risk of recurrence, it was also reported that age <45 years is a poor predictor of prognosis of LNM in PTC patients (44). Therefore, whether an younger than 45 years old can be shown to be related to the increased risk of LNM in PTC patients still needs to be investigated in studies with a larger sample size.
Although the morbidity of thyroid cancer is relatively higher in women, the rates of PTC-induced malignancies and mortality are higher in men (45). In assessing patients with thyroid nodules, male sex is considered a risk factor for LNM, which may be suggestive of PTC (46). Based on the analysis result, we concluded that the gender of male was a significant risk factor for LNM in PTC patients (pooled OR = 1.68).
Among the clinical and pathological features that can be evaluated before and during surgery, tumor size is an important factor for tumor node metastasis (TNM) staging, and large tumors (tumor size >1 cm) are more vulnerable to aggression (47). In clinical diagnosis, a tumor size ≤ 1 cm represented microPTC/PTMC. According to the ATA guidelines, the PTMC exhibited less of a risk of LNM, and surgery for most PTMC was thus not recommended (9). However, it was also reported that LNM accounted for 64% of patients in the diagnosis of PTMC (48). Moreover, when LNM is found in PTMC patients, prophylactic central lymph node dissection (PCLND) is the standard treatment in clinical practice. In addition, LNM is also associated with higher risk of distant metastasis and about 11–22% risk of recurrence, especially for cervical lymph nodes (49). Therefore, TT combined with PCLND should be performed for PTMC patients presenting with LNM especially tumor size >1 cm (50). On account of our analysis data, PTC patients with tumor size >1 cm were at relatively higher risk of developing LNM than those with a tumor size ≤ 1 cm (pooled OR = 3.53). Previous research demonstrated that tumor size (>1 cm) is the best predictor of microcentric and lateral LNM, which was markedly affected lymph node recurrence in multivariate logistic analysis (51). Hence, careful lymph node dissection is strongly recommended for tumor size >1 cm in PTC patients even if it is considered as the preventive measure.
Multifocality is also considered an important risk factor for LNM in PTC patients. In addition, it was reported that the prognostic value of multifocality is particularly significant in PTC patients with tumor size >1 cm (52). Previous research has demonstrated that tumor multifocality is an independent risk factor of LNM in PTC patients after TT (53). Our finding was consistent with previous studies that the risk of LNM was higher in multifocality patients rather than single focality in PTC patients (pooled OR = 2.05). The result indicates that multifocality is an indicator of the aggressiveness of PTC tumors, showing a higher tendency for regional LNM. Therefore, multifocality may be associated with the state of disease progression, including risk stratification, management guidelines, and post-treatment monitoring in patients with PTC (54).
Six studies were analyzed for the correlation between tumor location and LNM in PTC patients. LNM was confirmed in 674 (46.74%) of 1,442 patients with upper 1/3 and in 985 (42.42%) of 2,322 patients with lower 2/3. According to our analysis data, the risk of LNM was conferred higher in patients with upper 1/3 than in those lower 2/3 (pooled OR = 1.46). In previous research, it was revealed that LNM was related to tumor location in upper 1/3 of the thyroid which is consistent with us (55). Nowadays, US combined with FNAB is usually used in the diagnosis of PTMC (tumor size ≤ 1 cm) patients by experienced doctors (10, 11). The tumor location of PTMC is one of the most important issues to determine whether active monitoring should be carried out. According to ATA guideline, an active surveillance approach as a management option is adopted for those low-risk PTMC patients (9). In clinical diagnosis, if the small tumor is located in the center of the thyroid lobe without LNM or thyroid capsule invasion, it can only be monitored by watching. Ito et al. published an article concluding that the characteristics that are not suitable for active surveillance included clinical LNM, distant metastasis, symptoms of recurrent laryngeal nerve or tracheal invasion, high-grade malignancy, and the presence of progression signs (i.e., gradually enlarged tumor size and the appearance of LNM) during active surveillance (56). In addition, it was also demonstrated that the 1/3 upper pole was the greatest independent factor that correlated with LNM in PTMC patients (57). Therefore, we suggest that, in cases with an upper 1/3 pole that are also invasive and include LNM, surgery should be performed; cases with a lower 2/3 pole that is non-invasive and without LNM should be monitored.
The relationship between tumor bilaterality and LNM in PTC patients was analyzed in eight studies. To reduce the risk of complications from PCLND and the potential to clear metastatic disease, bilateral central lymph node dissection (CLNM) rather than unilateral central lymph node dissection has been chosen for central neck dissection (58). In present study, there was no significant correlation (pooled OR = 0.85) between bilaterality and LNM in PTC patients.
Vascular invasion has been reported as a marker of an increased tendency toward hematogenic invasion and consequent increase in the relative percentage of LNM in patients with PTC which means a poorer prognosis ultimately (59). In addition, it was also reported that the presence of tumor capsular invasion does not adversely influence biological behavior (e.g., LNM) or survival of PTC (60). In our meta-analysis, it was found that capsular invasion was associated with LNM in PTC patients (pooled OR = 3.48).
In the presence of risk factors suggesting a possible increase in biological invasiveness, adequate postoperative treatment and close follow-up are essential. Tumor prognosis is related to the extent of extrathyroid expansion. The prognosis for patients with severely dilated extrathyroid disease is worse than patients with local microdilatation visible on histopathological examination (61). Previous research demonstrated that ETE have poorer prognosis including LNM than those without ETE in PTC patients (62). Our finding was consistent with previous studies that ETE was the increased risk of LNM in PTC patients (pooled OR = 2.03).
Previous studies suggest that the coexistence of HT is not related to LNM in PTC patients (63). However, it was also reported that there was a trend in patients with PTC and HT getting a better prognosis on which HT may have protected against central and lateral LNM (64). Our data demonstrated that there was no correlation between HT and LNM in PTC patients (pooled OR = 1.08).
According to the research, PTC is also considered to be a genetically driven disease. Therefore, it is necessary to understand the molecular mechanisms of the BRAFV600E mutation and TERT promoter, which is reported upon in association with PTC. The activation mutation of serine threonine kinase v-RAF mouse sarcoma virus oncogene B1 (BRAF) is an important biomarker in human benign and malignant tumors, and most mutations affect BRAFV600 in exon 15 of BRAF gene (65). The BRAFV600E mutation occurs in 30–80% PTC patients, which is the most common carcinogenic mutation (66). In addition, BRAFV600E mutation is related to failure, recurrence, distant metastasis, and mortality in PTC treatment, which is considered an effective target for thyroid cancer (67). TERT is a catalytic subunit of telomerase that plays a dominant role in cell immortality and tumorigenesis (68). A mutation of TERT promoter was found in about 7.5% of PTCs, which induced the abnormal activation of telomerase is closely related to the invasive clinical behavior of papillary carcinoma (69). Moreover, it was revealed that TERT promoter mutation is a major indicator of extremely poor prognosis and aggressive clinicopathological characteristics (13). It also demonstrated that coexistence of BRAFV600E and TERT promoter mutations are the most aggressive subgroup in PTCs patients, while PTCs with BRAF or TERT alone are less aggressive (70). Above all, to research those genetical mutations related to PTC may also help stratify patients into distinct risk groups and better assess patients' outcome.
Although the meta-analysis has explored several clinical and pathological predictors of LNM risk that may help surgeons choose appropriate treatment strategies in PTC patients, there are still some limitations that exist in our study. Firstly, there were only 21 studies that were included for predicting the risk of LNM in PTC patients. Secondly, the operation performed by different doctors may also have influence on the accuracy of data analysis, even following the standard mode and operation quality. Thirdly, most patients included in the study were from the same continent (Asia).
Taken together, this meta-analysis investigated the following risk factors of LNM in PTC patients including age (<45 years), gender (male), multifocality, tumor size (>1 cm), tumor location (1/3 upper), capsular invasion, and ETE. Bilateral tumors and HT were not correlated with LNM in PTC patients. In addition, BRAFV600E and TERT promoter mutations are also considered as the risk factors, which can help stratify PTC patients and better assess their prognosis.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
GW conceived and designed the project. JM, QZ, and HZ conducted the statistical analysis/meta-analysis and wrote the paper. KZ and RW abstracted the total data from the included articles. All authors contributed to manuscript revision, read, and approved the submitted version.
This work was supported by the first-class discipline construction project in Guizhou Province—Public Health and Preventive Medicine (No. 2017 [85]) and Science and Technology Support Program Project of Guizhou Province, China, 2017 (2044), (2860), 2018 (2349).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
ATA, American Thyroid Association; ATC, Ana-plastic thyroid carcinoma; CLNM, Central lymph node metastasis; CND, Central neck dissection; CT, Computerized tomography; CI, Confidence index; ETE, Extra thyroidal extension; FNAB, Fine-needle aspiration biopsy; FTC, follicular thyroid carcinoma; HT, Hashimoto thyroiditis; LLND, Lateral lymph node dissection; LLNM, Lateral lymph node metastasis; LND, lymph node dissection; MTC, medullary thyroid carcinoma; NTT, Nearly total thyroidectomy; OR, Odd ratio; PTC, Papillary thyroid carcinoma; PTMC, Papillary thyroid microcarcinoma; PCLND, Prophylactic central lymph node dissection; RAI, Radioiodine ablation; SD, Standard deviation; TC, Thyroid carcinoma; TT, Total thyroidectomy; TNM, Tumor node metastasis; US, Ultrasound; WMD, Weighted mean difference; WHO, World Health Organization.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics. CA Cancer J Clin. (2017) 67:7–30. doi: 10.3322/caac.21387
2. Mao Y, Xing M. Recent incidences and differential trends of thyroid cancer in the USA. Endocr Relat Cancer. (2016) 23:313–22. doi: 10.1530/ERC-15-0445
3. Morris LGT, Sikora AG, Tosteson TD, Davies L. The increasing incidence of thyroid cancer: the influence of access to care. Thyroid. (2013) 23:885–91. doi: 10.1089/thy.2013.0045
4. Mazeh H, Sippel RS. Familial nonmedullary thyroid carcinoma. Thyroid. (2013) 23:1049–56. doi: 10.1089/thy.2013.0079
5. Kim BY, Jung CH, Kim JW, Lee SW, Kim CH, Kang SK, et al. Impact of clinicopathologic factors on subclinical central lymph node metastasis in papillary thyroid microcarcinoma. Yonsei Med J. (2012) 53:924–6. doi: 10.3349/ymj.2012.53.5.924
6. Agrawal N, Akbani R, Aksoy BA, Ally A, Arachchi H, Asa SL, et al. Integrated genomic characterization of papillary thyroid carcinoma. Cell. (2014) 159:676–90. doi: 10.1016/j.cell.2014.09.050
7. Markovina S, Grigsby PW, Schwarz JK, DeWees T, Moley JF, Siegel BA, et al. Treatment approach, surveillance, and outcome of well-differentiated thyroid cancer in childhood and adolescence. Thyroid. (2014) 24:1121–6. doi: 10.1089/thy.2013.0297
8. Kim SK, Woo JW, Park I, Lee JH, Choe JH, Kim JH, et al. Computed tomography-detected central lymph node metastasis in ultrasonography node-negative papillary thyroid carcinoma: is it really significant? Ann Surg Oncol. (2016) 24:442–9. doi: 10.1245/s10434-016-5552-1
9. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. (2016) 26:1–133. doi: 10.1089/thy.2015.0020
10. Rizzo M, Sindoni A, Rossi RT, Bonaffini O, Panetta S, Scisca C, et al. Annual increase in the frequency of papillary thyroid carcinoma as diagnosed by fine-needle aspiration at a cytology unit in sicily. Hormones. (2013) 12:46–57. doi: 10.1007/BF03401286
11. Jun HH, Kim SM, Kim BW, Lee YS, Chang HS, Park CS. Overcoming the limitations of fine needle aspiration biopsy: detection of lateral neck node metastasis in papillary thyroid carcinoma. Yonsei Med J. (2015) 56:182–87. doi: 10.3349/ymj.2015.56.1.182
12. Grant CS. Recurrence of papillary thyroid cancer after optimized surgery. Gland Surg. (2015) 4:52−62. doi: 10.3978/j.issn.2227-684X.2014.12.06
13. Rosario PW, Furtado MDS, Filho AFCM, Lacerda RX, Calsolari MR. Value of diagnostic radioiodine whole-body scanning after initial therapy in patients with differentiated thyroid cancer at intermediate and high risk for recurrence. Thyroid. (2012) 22:1165–9. doi: 10.1089/thy.2012.0026
14. Yip J, Orlov S, Orlov D, Vaisman A, Hernández KG, Etarsky D, et al. Predictive value of metastatic cervical lymph node ratio in papillary thyroid carcinoma recurrence. Head Neck. (2012) 35:592–8. doi: 10.1002/hed.23047
15. Yuan J, Li J, Chen X, Zhong Z, Chen Z, Yin Y, et al. Predictors of lymph nodes posterior to the right recurrent laryngeal nerve metastasis in patients with papillary thyroid carcinoma. Medicine. (2017) 96:e7908. doi: 10.1097/MD.0000000000007908
16. Wells G, Shea B, O'Connell J. The Newcastle-Ottawa Scale (NOS) for Assessingthe Quality of Nonrandomised Studies in Meta-Analyses. (2017). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed June 9, 2017).
17. An C, Zhang X, Wang S, Zhang Z, Yin Y, Xu Z, et al. Efficacy of superselective neck dissection in detecting metastasis in patients with cN0 papillary thyroid carcinoma at high risk of lateral neck metastasis. Med Sci Monit. (2017) 23:2118–26. doi: 10.12659/MSM.900273
18. Chen Q, Zou XH, Wei T. Prediction of ipsilateral and contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma: a retrospective study. Gland Surg. (2015) 4:288–94. doi: 10.3978/j.issn.2227-684X.2015.05.06
19. Hu D, Zhou J, He W, Peng J, Cao Y, Ren H, et al. Risk factors of lateral lymph node metastasis in cN0 papillary thyroid carcinoma. World J Surg Oncol. (2018) 16:1–6. doi: 10.1186/s12957-018-1336-3
20. Jeong SY, Kim YS, Kim KC. Predictive factors for central neck lymph node metastasis in patients with papillary thyroid microcarcinoma without suspicious metastasis by preoperative ultrasonography. J Endocr Surg. (2017) 17:114–21. doi: 10.16956/jes.2017.17.3.114
21. Jiang LH, Chen C, Tan Z, Lu XX, Hu SS, Wang QL, et al. Clinical characteristics related to central lymph node metastasis in cN0 papillary thyroid carcinoma: a retrospective study of 916 patients. Int J Endocrinol. (2014) 2014:1–6. doi: 10.1155/2014/385787
22. Lv T, Zhu C, Di Z. Risk factors stratifying malignancy of nodules in contralateral thyroid lobe in patients with pre-operative ultrasound indicated unilateral papillary thyroid carcinoma: a retrospective analysis from single centre. Clin Endocrinol. (2017) 88:279–84. doi: 10.1111/cen.13506
23. Liu C, Xiao C, Chen J, Li X, Feng Z, Gao Q, et al. Risk factor analysis for predicting cervical lymph node metastasis in papillary thyroid carcinoma: a study of 966 patients. BMC Cancer. (2019) 19:1–10. doi: 10.1186/s12885-019-5835-6
24. Mao LN, Wang P, Li ZY, Wang Y, Song ZY. Risk factor analysis for central nodal metastasis in papillary thyroid carcinoma. Oncol Lett. (2015) 9:103–7. doi: 10.3892/ol.2014.2667
25. Miao S, Mao X, Pei R, Xiang C, Lv Y, Shi Q, et al. Predictive factors for different subgroups of central lymph node metastasis in unilateral papillary thyroid Carcinoma. ORL. (2013) 75:265–73. doi: 10.1159/000354267
26. Noda S, Onoda N, Morisaki T, Kashiwagi S, Takashima T, Hirakawa K. The significance the predictive factors of microscopic lymph node metastasis in patients with clinically node negative papillary thyroid cancer: a retrospective cohort study. Int J Surg. (2015) 20:52–7. doi: 10.1016/j.ijsu.2015.06.023
27. Park JP, Roh JL, Lee JH, Baek JH, Gong G, Cho KJ, et al. Risk factors for central neck lymph node metastasis of clinically noninvasive, node-negative papillary thyroid microcarcinoma. Am J Surg. (2014) 208:412–8. doi: 10.1016/j.amjsurg.2013.10.032
28. Shin HJ, Kim EK, Moon HJ, Yoon JH, Han KH, Kwak JY. Can increased tumoral vascularity be a quantitative predicting factor of lymph node metastasis in papillary thyroid microcarcinoma? Endocrine. (2013) 47:273–82. doi: 10.1007/s12020-013-0131-8
29. Siddiqui S, White MG, Antic T, Grogan RH, Angelos P, Kaplan EL, et al. Clinical and pathologic predictors of lymph node metastasis and recurrence in papillary thyroid microcarcinoma. Thyroid. (2016) 26:807–15. doi: 10.1089/thy.2015.0429
30. Tao Y, Wang C, Li L, Xing H, Bai Y, Han B, et al. Clinicopathological features for predicting central and lateral lymph node metastasis in papillary thyroid microcarcinoma: analysis of 66 cases that underwent central and lateral lymph node dissection. Mol Clin Oncol. (2016) 6:49–55. doi: 10.3892/mco.2016.1085
31. Wang YF, Han J, Lv YT, Zhang GC. Risk factors analysis of lymph node metastasis in central zone of papillary thyroid microcarcinoma. Biomed Res. (2017) 28:9567–70.
32. Wei T, Chen R, Zou X, Liu F, Li Z, Zhu J. Predictive factors of contralateral paratracheal lymph node metastasis in unilateral papillary thyroid carcinoma. Eur J Surg Oncol. (2015) 41:746–50. doi: 10.1016/j.ejso.2015.02.013
33. Xue S, Wang P, Liu J, Li R, Zhang L, Chen G. Prophylactic central lymph node dissection in cN0 patients with papillary thyroid carcinoma: a retrospective study in China. Asian Surg. (2016) 39:131–6. doi: 10.1016/j.asjsur.2015.03.015
34. Yang Y, Chen C, Chen Z, Jiang J, Chen Y, Jin L, et al. Prediction of central compartment lymph node metastasis in papillary thyroid microcarcinoma. Clin Endocrinol. (2014) 81:282–8. doi: 10.1111/cen.12417
35. Yu QA, Ma DK, Liu KP, Wang P, Xie CM, Wu YH, et al. Clinicopathologic risk factors for right paraesophageal lymph node metastasis in patients with papillary thyroid carcinoma. J Endocrinol Invest. (2018) 41:1333–8. doi: 10.1007/s40618-018-0874-4
36. Zeng R, Zhang W, Gao E, Cheng P, Huang G, Zhang X, et al. Number of central lymph node metastasis for predicting lateral lymph node metastasis in papillary thyroid microcarcinoma. Head Neck. (2013) 36:101–6. doi: 10.1002/hed.23270
37. Zhang LY, Liu ZW, Liu YW, Gao WS, Zheng CJ. Risk factors for nodal metastasis in cN0 papillary thyroid microcarcinoma. Asian Pac J Cancer Prev. (2015) 16:3361–3. doi: 10.7314/APJCP.2015.16.8.3361
38. Arianpoor A, Asadi M, Amini E, Ziaeemehr A, Ahmadi Simab S, Zakavi SR. Investigating the prevalence of risk factors of papillary thyroid carcinoma recurrence and disease-free survival after thyroidectomy and central neck dissection in Iranian patients. Acta Chir Belg. (2019) 25:1–6. doi: 10.1080/00015458.2019.1576447
39. Zaydfudim V, Feurer ID, Griffin MR, Phay JE. The impact of lymph node involvement on survival in patients with papillary and follicular thyroid carcinoma. Surgery. (2008) 144:1070–8. doi: 10.1016/j.surg.2008.08.034
40. Kim SY, Kim BW, Pyo JY, Hong SW, Chang HS, Park CS. Macrometastasis in papillary thyroid cancer patients is associated with higher recurrence in lateral neck nodes. World J Surg. (2017) 42:123–9. doi: 10.1007/s00268-017-4158-5
41. Guerra A, Rosaria Sapio M, Marotta V, Campanile E, Ilaria Moretti M, Deandrea M, et al. Prevalence of RET/PTC rearrangement in benign and malignant thyroid nodules and its clinical application. Endocr J. (2011) 58:31–8. doi: 10.1507/endocrj.K10E-260
42. Ito Y, Miyauchi A, Kihara M, Takamura Y, Kobayashi K, Miya A. Relationship between prognosis of papillary thyroid carcinoma patient and age: a retrospective single-institution study. Endocr J. (2012) 59:399–405. doi: 10.1507/endocrj.EJ12-0044
43. Liu LS, Liang J, Li JH, Liu X, Jiang L, Long JX, et al. The incidence and risk factors for central lymph node metastasis in cN0 papillary thyroid microcarcinoma: a meta-analysis. Eur Arch Oto Rhino Laryngol. (2016) 274:1327–38. doi: 10.1007/s00405-016-4302-0
44. Adam MA, Pura J, Goffredo P, Dinan MA, Reed SD, Scheri RP, et al. Presence and number of lymph node metastases are associated with compromised survival for patients younger than age 45 years with papillary thyroid cancer. J Clin Oncol. (2015) 33:2370–5. doi: 10.1200/JCO.2014.59.8391
45. Rahbari R, Zhang L, Kebebew E. Thyroid cancer gender disparity. Future Oncol. (2010) 6:1771–9. doi: 10.2217/fon.10.127
47. Tuttle RM, Haddad RI, Ball DW, Byrd D, Dickson P, Duh QY, et al. Thyroid carcinoma, version 2. J Natl Compr Canc Netw. (2014) 12:1671–80. doi: 10.6004/jnccn.2014.0169
48. Roti E, degli Uberti EC, Bondanelli M, Braverman LE. Thyroid papillary microcarcinoma: a descriptive meta-analysis study. Eur J Endocrinol. (2008) 159:659–73. doi: 10.1530/EJE-07-0896
49. Bernet V. Approach to the patient with incidental papillary microcarcinoma. J Clin Endocrinol Metab. (2010) 95:3586–92. doi: 10.1210/jc.2010-0698
50. Yan B, Hou Y, Chen D, He J, Jiang Y. Risk factors for contralateral central lymph node metastasis in unilateral cN0 papillary thyroid carcinoma: a meta-analysis. Int J Surg. (2018) 59:90–8. doi: 10.1016/j.ijsu.2018.09.004
51. Ito Y, Fukushima M, Higashiyama T, Kihara M, Takamura Y, Kobayashi K, et al. Tumor size is the strongest predictor of microscopic lymph node metastasis and lymph node recurrence of N0 papillary thyroid carcinoma. Endocr J. (2012) 60:113–7. doi: 10.1507/endocrj.EJ12-0311
52. Kim KJ, Kim SM, Lee YS, Chung WY, Chang HS, Park CS. Prognostic significance of tumor multifocality in papillary thyroid carcinoma and its relationship with primary tumor size: a retrospective study of 2,309 consecutive patients. Ann Surg Oncol. (2014) 22:125–31. doi: 10.1245/s10434-014-3899-8
53. Wang F, Yu X, Shen X, Zhu G, Huang Y, Liu R, et al. The prognostic value of tumor multifocality in clinical outcomes of papillary thyroid cancer. J Clin Endocr Metab. (2017) 102:3241–50. doi: 10.1210/jc.2017-00277
54. Choi WR, Roh JL, Gong G, Cho KJ, Choi SH, Nam SY, et al. Multifocality of papillary thyroid carcinoma as a risk factor for disease recurrence. Oral Oncol. (2019) 94:106–10. doi: 10.1016/j.oraloncology.2019.05.023
55. Chai Y J, Kim S, Choi JY, Koo DH, Lee KE, Youn YK. Papillary thyroid carcinoma located in the isthmus or upper third is associated with delphian lymph node metastasis. World J Surg. (2013) 38:1306–11. doi: 10.1007/s00268-013-2406-x
56. Ito Y, Miyauchi A, Oda H. Low-risk papillary microcarcinoma of the thyroid: a review of active surveillance trials. Eur J Surg Oncol. (2018) 44:307–15. doi: 10.1016/j.ejso.2017.03.004
57. Xiang D, Xie L, Xu Y, Li Z, Hong Y, Wang P. Papillary thyroid microcarcinomas located at the middle part of the middle third of the thyroid gland correlates with the presence of neck metastasis. Surgery. (2015) 157:526–33. doi: 10.1016/j.surg.2014.10.020
58. Sadowski BM, Snyder SK, Lairmore TC. Routine bilateral central lymph node clearance for papillary thyroid cancer. Surgery. (2009) 146:696–705. doi: 10.1016/j.surg.2009.06.046
59. Falvo L, Catania A, D'Andrea V, Marzullo A, Giustiniani MC, De Antoni E. Prognostic importance of histologic vascular invasion in papillary thyroid carcinoma. Ann Surg. (2005) 241:640–6. doi: 10.1097/01.sla.0000157317.60536.08
60. Furlan JC, Bedard YC, Rosen IB. Significance of tumor capsular invasion in well-differentiated thyroid carcinomas. Am Surg. (2007) 73:484–91.
61. Radowsky JS, Howard RS, Burch HB, Stojadinovic A. Impact of degree of extrathyroidal extension of disease on papillary thyroid cancer outcome. Thyroid. (2014) 24:241–4. doi: 10.1089/thy.2012.0567
62. Park JS, Chang JW, Liu L, Jung SN, Koo BS. Clinical implications of microscopic extrathyroidal extension in patients with papillary thyroid carcinoma. Oral Oncol. (2017) 72:183–7. doi: 10.1016/j.oraloncology.2017.02.008
63. Kim EY, Kim WG, Kim WB, Kim TY, Kim JM, Ryu JS, et al. Coexistence of chronic lymphocytic thyroiditis is associated with lower recurrence rates in patients with papillary thyroid carcinoma. Clin Endocrinol. (2009) 71:581–6. doi: 10.1111/j.1365-2265.2009.03537.x
64. Zhu Y, Zheng K, Zhang H, Chen L, Xue J, Ding M, et al. The clinicopathologic differences of central lymph node metastasis in predicting lateral lymph node metastasis and prognosis in papillary thyroid cancer associated with or without hashimoto's thyroiditis. Tumor Biol. (2015) 37:8037–45. doi: 10.1007/s13277-015-4706-2
65. Capper D, Preusser M, Habel A, Sahm F, Ackermann U, Schindler G, et al. Assessment of BRAFV600E mutation status by immunohistochemistry with a mutation-specific monoclonal antibody. Acta Neuropathol. (2011) 122:11–9. doi: 10.1007/s00401-011-0841-z
66. Lucas G, Jessica RP, Cesar SF, Maiaro CRM, Desirée RP, Palloma PA, et al. BRAFV600E mutation in prognostication of papillary thyroid cancer (PTC) recurrence. Gland Surg. (2016) 5: 495–505. doi: 10.21037/gs.2016.09.09
67. Goedert L, Plaça JR, Fuziwara CS, Machado MCR, Plaça DR, Almeida PP, et al. Identification of long noncoding RNAs deregulated in papillary thyroid cancer and correlated with BRAFV600E mutation by bioinformatics integrative analysis. Sci Rep. (2017) 7:1662. doi: 10.1038/s41598-017-01957-0
68. Hartl DM, Ghuzlan AA, Chami L, Leboulleux S, Schlumberger M, Travagli JP. High rate of multifocality and occult lymph node metastases in papillary thyroid carcinoma arising in thyroglossal duct cysts. Ann Surg Oncol. (2009) 16:2595–601. doi: 10.1245/s10434-009-0571-9
69. Horn S, Figl A, Rachakonda PS, Fischer C, Sucker A, Gast A, et al. TERT promoter mutations in familial and sporadic melanoma. Science. (2013) 339:959–61. doi: 10.1126/science.1230062
Keywords: papillary thyroid carcinoma (PTC), lymph node metastasis (LNM), risk factor, prognostic factor, meta-analysis
Citation: Mao J, Zhang Q, Zhang H, Zheng K, Wang R and Wang G (2020) Risk Factors for Lymph Node Metastasis in Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. Front. Endocrinol. 11:265. doi: 10.3389/fendo.2020.00265
Received: 22 January 2020; Accepted: 09 April 2020;
Published: 15 May 2020.
Edited by:
Alessandro Antonelli, University of Pisa, ItalyReviewed by:
Jeffrey Knauf, Cornell University, United StatesCopyright © 2020 Mao, Zhang, Zhang, Zheng, Wang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guoze Wang, d2FuZ2d6NTY3OEAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.