
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Endocrinol. , 24 January 2020
Sec. Cancer Endocrinology
Volume 11 - 2020 | https://doi.org/10.3389/fendo.2020.00010
 Angela Dardano1*
Angela Dardano1* Giuseppe Daniele1
Giuseppe Daniele1 Roberto Lupi1Niccolò Napoli2Daniela Campani3Ugo Boggi2Stefano Del Prato1Roberto Miccoli1
Roberto Lupi1Niccolò Napoli2Daniela Campani3Ugo Boggi2Stefano Del Prato1Roberto Miccoli1Background: Nesidioblastosis and insulinoma are disorders of the endocrine pancreas causing endogenous hyperinsulinemic hypoglycemia. Their coexistence is very unusual and treatment represents a still unresolved dilemma.
Case Description: The patient was a 43-year-old Caucasian woman, with a 2-year history of repeated severe hypoglycemic events. The diagnostic work-up was strongly suggestive of insulinoma and the patient was submitted to surgical treatment carried out laparoscopically under robotic assistance. However, surgical exploration and intraoperative ultrasonography failed to detect a pancreatic tumor. Resection was therefore carried out based on the results of selective intra-arterial calcium stimulation test, following a step-up approach, eventually leading to a pancreatoduodenectomy at the splenic artery. The histopathology examination and the immunohistochemical staining were consistent with adult-onset nesidioblastosis. After surgery, the patient continued to experience hypoglycemia with futile response to medical treatments (octreotide, calcium antagonists, diazoxide, and prednisone). Following multidisciplinary evaluation and critical review of a repeat abdominal computed tomography scan, a small nodular lesion was identified in the tail of the pancreas. The nodule was enucleated laparoscopically and the pathological examination revealed an insulinoma. In spite of the insulinoma resection, glycemic values were only partially restored, with residual nocturnal hypoglycemia. Administration of uncooked cornstarch (1.25 g/kg body weight) at bedtime was associated with significant improvement of interstitial glucose levels (p < 0.0001) and reduction of nocturnal hypoglycemia episodes (p = 0.0002).
Conclusions: This report describes a rare coexistence of adult-onset nesidioblastosis and insulinoma, suggesting the existence of a wide and continuous spectrum of proliferative β-cell changes. Moreover, we propose that uncooked cornstarch may offer an additional approach to alleviate the hypoglycemic episodes when surgery is impracticable/unaccepted.
Nesidioblastosis and insulinoma represent the main cause of endogenous hyperinsulinemic hypoglycemia in infants and in apparently healthy adults, respectively (1). Adult-onset nesidioblastosis is very rare (2, 3) and its cause is still unknown. The combination of nesidioblastosis and insulinoma is clinically relevant as each of these pathological entities is rare. We herein describe an unusual case of adult-onset nesidioblastosis coexisting with an insulin-secreting pancreatic adenoma. We also report our preliminary experience on the management of persistent hyperinsulinemic hypoglycemia with uncooked cornstarch.
A 43-year-old Caucasian woman was referred to our Clinic because of a history of repeated hypoglycemic episodes fulfilling the Whipple's triad. The lady reported an initial episode of difficult wakening up associated with temporary amnesia that resolved with carbohydrate intake. Afterwards, the patient experienced frequent episodes of hypoglycemia with prevalence of neuroglycopenic symptoms. Such episodes occurred both in fasting as well as post-prandial state and were relieved by the intake of simple and complex carbohydrates. Capillary blood glucose measurements at the time of these episodes were often <2.78 mmol/L. There was no family history of diabetes mellitus and the patient did not smoke or drink alcohol. On admission, physical examination revealed class I obesity (31 kg/m2). Fasting plasma glucose and hemoglobin A1c values were 2.94 mmol/L and 26 mmol/M, respectively. The results of the laboratory workup for rare forms of hypoglycemia were all within the normal range. No sulfonylureas were detected in the urine and search of serum anti-insulin and anti-insulin receptor antibodies was negative. During a consecutive 72-h fasting, plasma glucose reached 2 mmol/L after 18 h, with no suppression of plasma insulin (82.6 pmol/L) and C-peptide concentrations (1.7 nmol/L), compatible with autonomous insulin secretion. Both an abdominal ultrasound and high-resolution contrast-enhanced computed tomography scan were negative for insulinoma and an indium111-octreotide scan did not show focal abnormalities. Magnetic resonance imaging examination was not performed due to claustrophobia. 68Ga somatostatin receptor PET/CT and glucagon-like peptide-1 (GLP-1) receptor scintigraphy were not performed as they were not available in our Center. The patient then underwent a selective catheterization of the gastroduodenal, splenic, and superior mesenteric arteries with selective arterial calcium stimulation (calcium gluconate 0.025 mEq/kg body weight) and hepatic venous sampling for insulin determination (4). A selective positive response of inappropriate insulin secretion in the region of the gastroduodenal artery was suggestive for an insulinoma of the head/neck of the pancreas (Table 1). Because of the recurrent severe hypoglycemic episodes and the results of calcium stimulation test, the patient was scheduled for robotic assisted surgery in March 2015. Surgical exploration and intraoperative ultrasonography with a dedicated endoscopic ultrasound probe failed to identify a pancreatic tumor. Based on the results of calcium stimulation test, the pancreatic neck was resected first and sent for frozen section evaluation. As no tumor was identified by frozen section, resection was extended a couple of centimeters to the left. As frozen section histology showed again no tumor and considering that the results of calcium stimulation test indicated the tail of the pancreas as the site at the lowest probability to hide the insulinoma, the surgical procedure was completed by removing the head of the pancreas (i.e., pancreatoduodenectomy at the splenic artery). Because of the small size of the pancreatic duct and the extremely soft consistency of the pancreatic stump coupled with well-evident fatty infiltration, a pancreatic anastomosis was not performed, and a controlled external fistula was instead created by inserting a small catheter into the pancreatic duct. Macroscopic examination revealed regular architecture of the pancreas head measuring 4 × 3.5 × 3.5 cm; no tumor was identified. Microscopic examination showed a diffuse increase in islet tissue forming islets of various size (Figure 1A). In the same area, small and medium sized islets were associated with proliferating pancreatic ductules, forming ductuloinsular complexes (Figure 1B). The majority of medium and large sized islets had irregular margins. Immunohistochemistry revealed that the hyperplastic islets were positive for chromogranin A and synaptophysin; glucagon was evidenced in the periphery of the islets and insulin was positive in the majority of islet cells (Figure 1C). The morphologic and immunohistochemical findings were consistent with adult-onset nesidioblastosis. In spite of the surgery, there was no reduction of circulating plasma levels of insulin with persistence of the hypoglycemic episodes requiring during hospitalization parenteral glucose infusion and parenteral nutrition. Treatments with somatostatin analogs and calcium antagonists were futile, while diazoxide was withdrawn due to gastrointestinal intolerance and severe fluid retention. A slight reduction of the severity of hypoglycemia was obtained only with prednisone (40 mg daily). Because of recurrent episodes of infections, related to the presence of external pancreatic fistula, and the occurrence of new episodes of severe hypoglycemia, the option of a second surgery, including completion pancreatectomy, was properly discussed with the patient. In preparation for the second surgery, patient repeated an abdominal computed tomography scan that detected 1 cm nodular lesion in the pancreatic tail far from the pancreatic duct. In January 2017 the patient underwent laparoscopic enucleation of the small pancreatic tumor. During the same procedure the external pancreatic fistula was converted into a pancreatogastrostomy. Frozen sections and subsequent histology documented a well-differentiated, insulin-secreting neuroendocrine tumor, grade 1, measuring 1 × 0.6 × 0.4 cm (Figure 1D). Although the incidence of insulinoma in multiple endocrine neoplasia type 1 (MEN-1) is relatively uncommon (5, 6), an endocrine work-up was also pursued. She had no family history of insulinoma or MEN-1; her PTH level was 4.24 pmol/L (normal range, 0.84–4.24 pmol/L), IGF-1 level 15.4 nmol/L (normal range, 7.0–26 nmol/L), PRL level 13.16 μg/L (normal range, 2–25 μg/L), cortisol level 356.04 nmol/L (normal range, 184.92–623.76 nmol/L), ACTH level 3.74 pmol/L (normal range, <11 pmol/L), and calcium level was 2.24 mmol/L (normal range, 2.1–2.5 mmol/L). To this date, the patient did not wish to perform any other test, but a possible genetic analysis will be discussed in the future. Upon discharge, the patient was equipped with the FreeStyle Libre Flash Glucose Monitoring System (Abbot Diabetes Care, Alameda, California, USA) that documented recurrent nocturnal hypoglycemia. Coincidentally with hypoglycemic episodes, plasma insulin concentrations were 71.3 pmol/L and C-peptide 1.15 nmol/L. In the attempt to reduce the rate and severity of hypoglycemia uncooked cornstarch (1.25 g/kg body weight) was administered at bedtime. After 14 day of uncooked cornstarch supplementation, interstitial glucose levels increased from 4.6 ± 1.83 mmol/L to 5.3 ± 1.62 mmol/L (p < 0.0001) along with remarkable reduction of nocturnal hypoglycemia episodes (i.e., glucose ≤ 2.78 mmol/L from 8 p.m. to 8 a.m.; p = 0.0002). The uncooked cornstarch was well-tolerated with no gastrointestinal side effects. As the patient was hesitant toward any further surgical procedure, she was closely monitored. At 1-year follow-up, no pancreatic exocrine insufficiency or diabetes was observed, and a high definition contrast enhanced abdominal computed tomography showed a normal residual pancreatic tissue.

Table 1. Results of selective intra-arterial calcium injection of the major pancreatic arteries with hepatic venous sampling.
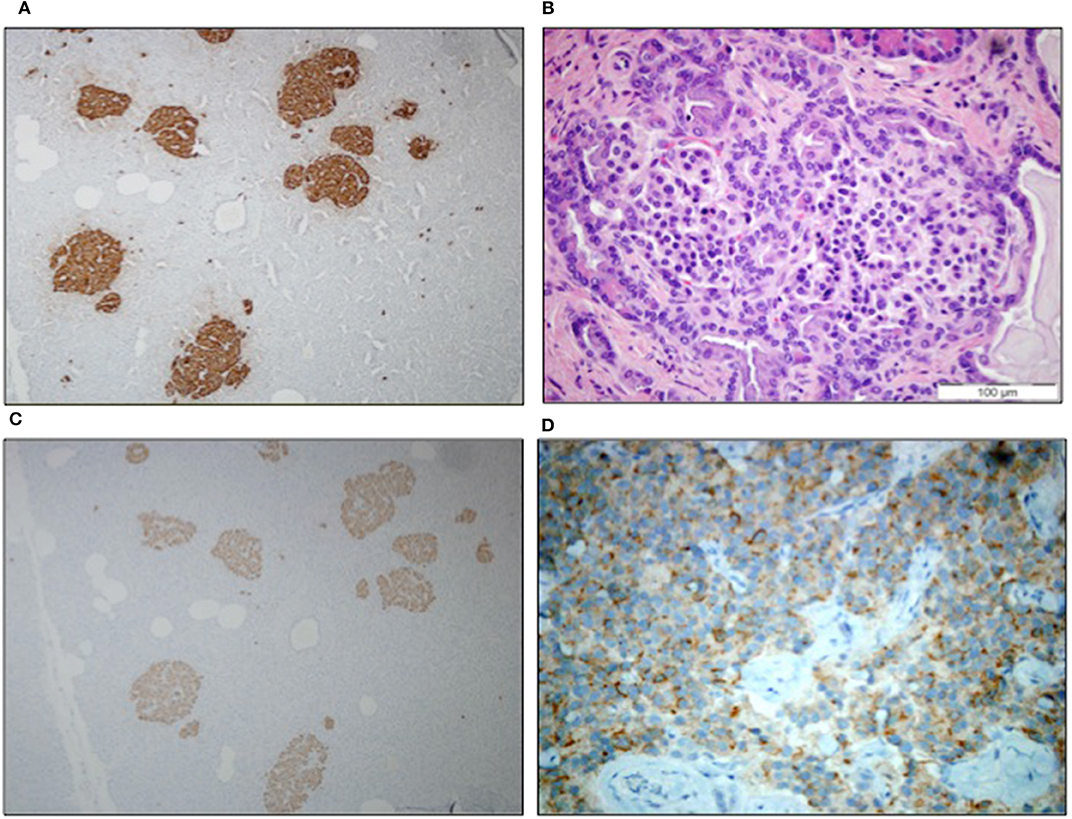
Figure 1. (A) Immunostaining of chromogranin highlighted the enlarged and irregular islets (10x); (B) ductuloinsular complexes haematoxylin-eosin staining (40x); (C) islets with diffuse positivity for insulin (10x); and (D) neuroendocrine tumor immunoreactive for insulin (10x).
Plasma glucose was measured by the glucose oxidase reaction (Glucose Oxidase Analyzer). Plasma insulin and C-peptide were measured by a radioimmunoassay (PANTEC srl Turin, Italy). Cortisol was measured by chemiluminescent Immuno Assays (CLIA). PTH, ACTH, IGF-1, and PRL levels were measured by immunochemiluminometric assay (ICMA). Calcium level was measured by standard method.
Insulinoma is the most frequent cause of hyperinsulinemic hypoglycemia in adults (1) while adult-onset nesidioblastosis accounts for only 0.5–5% of all cases of hyperinsulinemic hypoglycemia in adulthood (2, 3). The pathogenesis of adult-onset nesidioblastosis is unclear, and several mechanisms have been postulated, including dysregulation of β-cell function (7), increased production of growth factors and/or expression of their receptors (8) as well as unidentified genetic variants (9). Nesidioblastosis has been also claimed to be caused by increased levels of β-cell trophic factors in subjects undergoing bariatric surgery (10).
Here we describe an unusual case of adult-onset nesidioblastosis coexisting with an insulin-secreting pancreatic adenoma. The association of these two entities is a rare clinical finding. To the best of our knowledge, the association between nesidioblastosis and neoplastic diseases of the endocrine pancreas has been described in just a few cases (11–21). The peculiarity of our case is that the diagnoses of nesidioblastosis and insulinoma were not concomitant. Though we cannot rule out that early diagnostic procedures may have failed identifying the pancreatic neoplasia, our case suggests that the two conditions may arise at different time accounting for a wide and continuous spectrum of proliferative β-cell changes. In keeping with this view, a progression from nesidioblastosis to pancreatic tumor has been observed in experimental models (22). Moreover, induction of nesidioblastosis can enhance pancreatic carcinogenesis (23), and a spectrum of proliferation from nesidioblastosis to islet cell hyperplasia to multiple tumors to metastases has previously been reported (24). An insulinoma relapse on the background of a nesidioblastosis has been recently described (25), although identification of molecular mechanisms underlying this transition still remains to be established. Our case is another example of how complex it can be to differentiate an insulinoma from nesidioblastosis as the clinical presentation can be similar, and imaging studies inconclusive. Adult-onset nesidioblastosis is more commonly characterized by post-prandial hypoglycemia (2). In our case, symptoms developed both in the absorptive and post-absorptive state though positive fasting test was supportive of the diagnosis of insulinoma. The overlap of these clinical features made the diagnosis more difficult and uncertain. Imaging studies are generally negative in nesidioblastosis, but insulinomas can be too small to be detected (26). New non-invasive options such as 68Ga somatostatin receptor PET/CT and the more recent GLP-1 scintigraphy could have been useful to confirm the localization of the suspected insulinoma. PET/CT scanning with 68Ga labeled somatostatin analogs, however, is only positive in 25–31% of insulinoma patients (27). Scintigraphy with radiolabeled GLP-1 receptor analogs has been proposed as a second-line imaging option (28) because insulinomas frequently overexpress this receptor (29, 30) and its performance could offer an opportunity (6). Unfortunately, this method is not available everywhere. In our case, the patient should have performed the test and she refused to be moved away. Nonetheless the ability of this procedure to discriminate a focal insulinoma from diffuse nesidioblastosis has not been validated yet. When pre-operative imaging studies are negative, the intra-arterial calcium stimulation test is recommended (31). If the test allows regionalization, the diagnostic algorithm suggests confirming the localization by intraoperative methods. If localization is not achieved, a pancreatic tail resection for histologic evaluation is recommended (31). Our patient underwent an intra-arterial calcium stimulation test showing extremely high insulin release at the neck region, very high at the pancreatic body level, high at the pancreatic head, and low/normal at the tail region. The insulin gradient indicated the tail of the pancreas as the site with the lowest probability to host the insulinoma and a decision to resect the pancreatic neck was made, as a deviation from current recommendation, because of the suggestive very high insulin release from that region. Obviously, we could not exclude the possibility of a focal nesidioblastosis generating a gradient across selective arterial vessel stimulation, mimicking firing of a local insulin secreting adenoma, while detection of diffuse insulin response during selective arterial stimulation is more suggestive of nesidioblastosis (32).
Our case is instrumental in highlightening difficulties of the treatment of nesidioblastosis. While the gold-standard therapy for insulinoma is its surgical enucleation, that for nesidioblastosis is controversial. Therapeutic options include low-carbohydrate diet in combination with drugs such as diazoxide, octreotide, steroids, or nifedipine as it has been reported in isolated case reports. Pasireotide, a somatostatin analog used for treatment of acromegaly in adults, has been recently used with some success, though treatment protocol is not yet standardized (25, 33). Nonetheless the majority of the patients with nesidioblastosis undergo surgery though the degree of resection is still a matter of debate. Indeed, there is a very fine balance between removing too much or to little pancreatic tissue as too little may not be associated with significant improvement of the hypoglycemic syndrome and too much may cause pancreatogenic diabetes. Current literature supports a 60–89% resection of the pancreas (i.e., distal or subtotal pancreatectomy) with a >10% risk of subsequent diabetes and a 70% success rate of achieving normoglycemia (34). Our patient initially underwent pancreatoduodenectomy at the splenic artery and, 2 years later, to enucleation of an insulinoma in the pancreatic remnant. She did not develop diabetes, but she continued suffering of low plasma glucose levels. The patient was hesitant toward any further surgical procedure and common medical therapy was either ineffective or associated with side effects, but an improvement was obtained with the use of uncooked cornstarch administered at bedtime. In the early 1980s, uncooked cornstarch was introduced as an alternative to continuous nocturnal nasogastric glucose and frequent daytime feedings for maintaining normoglycemia in glycogen storage disease. This approach is still the mainstay of therapy (35–37). Uncooked cornstarch is a low-glycemic index carbohydrate characterized by slow intestinal degradation and absorption. It takes 4–6 h for the cornstarch to be completely digested. As a source of slowly releasable carbohydrates, uncooked cornstarch produces low glucose peaks and maintains blood glucose stable during fasting. It is given intermittently to provide stable blood glucose concentrations, reducing swings of insulin secretion (35, 36). Based on these properties, the effectiveness of uncooked cornstarch in preventing hypoglycaemia has been demonstrated in several conditions (37–39), including type 1 and type 2 diabetes (40, 41). Uncooked cornstarch has been used in few cases of children with nesidioblastosis (42), but its clinical efficacy in adult-onset nesidioblastosis was not previously assessed. Fourteen days after beginning bedtime cornstarch combined with personalized diet, our patient showed a remarkable reduction of nocturnal hypoglycemia episodes and an increase in glucose levels, without any relevant side effect.
In conclusion, our case report shows that: (1) nesidioblastosis and insulinoma can occur in the same patient; (2) preoperative diagnosis of both conditions is difficult, but, if diagnosis is established, it may have much influence on treatment choice; (3) uncooked cornstarch can be considered in patients with persistent hypoglycemia particularly when surgery is impracticable/unaccepted and pharmacologic therapy is ineffective.
All datasets generated for this study are included in the article/supplementary material.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
AD collected the data and wrote the manuscript with the support of GD and RM. SDP and UB overviewed the discussion. DC analyzed the specimen and provided the pictures. NN reviewed CT scan. RL performed lab measurements. All authors discussed the case and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank Dr. Pollina for histological support.
1. Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. (2009) 94:709–28. doi: 10.1210/jc.2008-1410
2. Anlauf M, Wieben D, Perren A, Sipos B, Komminoth P, Raffel A, et al. Persistent hyperinsulinemic hypoglycemia in 15 adults with diffuse nesidioblastosis: diagnostic criteria, incidence, and characterization of beta-cell changes. Am J Surg Pathol. (2005) 29:524–33. doi: 10.1097/01.pas.0000151617.14598.ae
3. Jabri AL, Bayard C. Nesidioblastosis associated with hyperinsulinemic hypoglycemia in adults: review of the literature. Eur J Intern Med. (2004) 15:407–10. doi: 10.1016/j.ejim.2004.06.012
4. Brändle M, Pfammatter T, Spinas GA, Lehmann R, Schmid C. Assessment of selective arterial calcium stimulation and hepatic venous sampling to localize insulin-secreting tumours. Clin Endocrinol. (2001) 55:357–62. doi: 10.1046/j.1365-2265.2001.01335.x
5. Thakker RV, Newey PJ, Walls GV, Bilezikian J, Dralle H, Ebeling PR, et al. Clinical practice guidelines for Multiple Endocrine Neoplasia Type 1 (MEN1). J Clin Endocrinol Metab. (2012) 97:2990–3011. doi: 10.1210/jc.2012-1230
6. Falconi M, Eriksson B, Kaltsas G, Bartsch DK, Capdevila J, Caplin M, et al. ENETS consensus guidelines update for the management of patients with functional pancreatic neuroendocrine tumors and non-functional pancreatic neuroendocrine tumors. Neuroendocrinology. (2016) 103:153–71. doi: 10.1159/000443171
7. Dravecka I, Lazurova I. Nesidioblastosis in adults. Neoplasma. (2014) 61:252–6. doi: 10.4149/neo_2014_047
8. Rumilla KM, Erickson LA, Service FJ, Vella A, Thompson GB, Grant CS, et al. Hyperinsulinemic hypoglycemia with nesidioblastosis: histologic features and growth factor expression. Mod Pathol. (2009) 22:239–45. doi: 10.1038/modpathol.2008.169
9. Klöppel G, Anlauf M, Raffel A, Perren A, Knoefel WT. Adult diffuse nesidioblastosis: genetically or environmentally induced? Hum Pathol. (2008) 39:3–8. doi: 10.1016/j.humpath.2007.09.010
10. Service GJ, Thompson GB, Service FJ, Andrews JC, Collazo-Clavell ML, Lloyd RV. Hyperinsulinemic hypoglycemia with nesidioblastosis after gastric-bypass surgery. N Engl J Med. (2005) 353:249–54. doi: 10.1056/NEJMoa043690
11. White SA, Sutton CD, Robertson GS, Furness PN, Dennison AR. Incidental adult nesidioblastosis after distal pancreatectomy for endocrine microadenoma. Eur J Gastroenterol Hepatol. (2000) 12:1147–9. doi: 10.1097/00042737-200012100-00013
12. Zhao X, Stabile BE, Mo J, Wang J, French SW. Nesidioblastosis coexisting with islet cell tumor and intraductal papillary mucinous hyperplasia. Arch Pathol Lab Med. (2001) 125:1344–7. doi: 10.1043/0003-9985(2001)125<1344:NCWICT>2.0.CO;2
13. Kaczirek K, Soleiman A, Schindl M, Passler C, Scheuba C, Prager G, et al. Nesidioblastosis in adults: a challenging cause of organic hyperinsulinism. Eur J Clin Invest. (2003) 33:488–92. doi: 10.1046/j.1365-2362.2003.01158.x
14. Dissanayake AS, Jones V, Fernando DJ. Adult hyperinsulinaemic hypoglycaemia caused by coexisting nesidioblastosis and insulinoma. Eur J Intern Med. (2008) 19:303. doi: 10.1016/j.ejim.2007.09.017
15. Rosman J, Bravo-Vera R, Sheikh A, Gouller A. Metastatic insulinoma in an adult patient with underlying nesidioblastosis. J Endocrinol Invest. (2007) 30:521–4. doi: 10.1007/BF03346338
16. Bright E, Garcea G, Ong SL, Madira W, Berry DP, Dennison AR. An unusual case of concurrent insulinoma and nesidioblastosis. JOP. (2008) 9:649–53.
17. Yu R, Nissen NN, Dhall D, Heaney AP. Nesidioblastosis and hyperplasia of alpha cells, microglucagonoma, and nonfunctioning islet cell tumor of the pancreas: review of the literature. Pancreas. (2008) 36:428–31. doi: 10.1097/MPA.0b013e31815ceb23.
18. Gupta RA, Patel RP, Nagral S. Adult onset nesidioblastosis treated by subtotal pancreatectomy. JOP. (2013) 14:286–8. doi: 10.6092/1590-8577/1352
19. Valli V, Blandamura S, Pastorelli D, Merigliano S, Sperti C. Nesidioblastosis coexisting with non-functioning islet cell tumour in an adult. Endokrynol Pol. (2015) 66:356–60. doi: 10.5603/EP.2015.0045
20. De Sousa SM, Haghighi KS, Qiu MR, Greenfield JR, Chen DL. Synchronous nesidioblastosis, endocrine microadenoma, and intraductal papillary mucinous neoplasia in a man presenting with hyperinsulinemic hypoglycemia. Pancreas. (2016) 45:154–9. doi: 10.1097/MPA.0000000000000430
21. Orujov M, Lai KK, Forse CL. Concurrent adult-onset diffuse β-cell nesidioblastosis and pancreatic neuroendocrine tumor: a case report and review of the literature. Int J Surg Pathol. (2019) 27:1–7. doi: 10.1177/1066896919858129
22. Götz W, Schucht C, Roth J, Theuring F, Herken R. Endocrine pancreatic tumors in MSV-SV40 large T transgenic mice. Am J Pathol. (1993) 142:1493–503.
23. Pour PM, Kazakoff K. Stimulation of islet cell proliferation enhances pancreatic ductal carcinogenesis in the hamster model. Am J Pathol. (1996) 149:1017–25.
24. Leong AS, Slavotinek AH, Higgins BA. Nesidioblastosis, islet cell hyperplasia, and adenomatosis in a case of metastasizing insulinoma: contribution to the genesis of the islets of Langerhans. Diabetes Care. (1980) 3:537–42. doi: 10.2337/diacare.3.4.537
25. Dauriz M, Maneschi C, Castelli C, Tomezzoli A, Fuini A, Landoni L, et al. A Case report of insulinoma relapse on background nesidioblastosis: a rare cause of adult hypoglycemia. J Clin Endocrinol Metab. (2019) 104:773–8. doi: 10.1210/jc.2018-02007
26. Mehrabi A, Fischer L, Hafezi M, Dirlewanger A, Grenacher L, Diener MK, et al. A systematic review of localization, surgical treatment options, and outcome of insulinoma. Pancreas. (2014) 43:675–86. doi: 10.1097/MPA.0000000000000110
27. Sharma P, Arora S, Karunanithi S, Khadgawat R, Durgapal P, Sharma R, et al. Somatostatin receptor based PET/CT imaging with 68Ga- DOTA-Nal3-Octreotide for localisation of clinically and biochemically suspected insulinoma. Q J Nucl Med Mol Imaging. (2016) 60:69–76.
28. Christ E, Wild D, Ederer S, Béhé M, Nicolas G, Caplin ME, et al. Glucagon-like peptide-1 receptor imaging for the localisation of insulinomas: a prospective multicentre imaging study. Lancet Diabetes Endocrinol. (2013) 1:115–22. doi: 10.1016/S2213-8587(13)70049-4.
29. Sowa-Staszczak A, Pach D, Mikołajczak R, Mäcke H, Jabrocka-Hybel A, Stefanska A, et al. Glucagon-like peptide-1 receptor imaging with [Lys40(Ahx-HYNIC- 99mTc/EDDA)NH2]-exendin-4 for the detection of insulinoma. Eur J Nucl Med Mol Imaging. (2013) 40:524–31. doi: 10.1007/s00259-012-2299-1.
30. Cases AI, Ohtsuka T, Fujino M, Ideno N, Kozono S, Zhao M, et al. Expression of glucagon-like Peptide 1 receptor and its effects on biologic behavior in pancreatic neuroendocrine tumors. Pancreas. (2014) 43:1–6. doi: 10.1097/MPA.0b013e3182a71537
31. Rafael A, Krausch MM, Anlauf M, Wieben D, Braunstein S, Klöppel G, et al. Diffuse nesidioblastosis as a cause of hyperinsulinemic hypoglycemiain adults: a diagnostic and therapeutic challenge. Surgery. (2007) 141:179–84 doi: 10.1016/j.surg.2006.04.015
32. Thompson SM, Vella A, Thompson GB, Rumilla KM, Service FJ, Grant CS, et al. Selective arterial calcium stimulation with hepatic venous sampling differentiates insulinoma from nesidioblastosis. J Clin Endocrinol Metab. (2015) 100:4189–97. doi: 10.1210/jc.2015-2404
33. Schwetz V, Horvath K, Kump P, Lackner C, Perren A, Forrer F, et al. Successful medical treatment of adult nesidioblastosis with pasireotide over 3 years: a case report. Medicine. (2016) 95:e3272. doi: 10.1097/MD.0000000000003272
34. Witteles RM, Straus FH II, Sugg SL, Koka MR, Costa EA, Kaplan EL. Adult-onset nesidioblastosis causing hypoglycemia: an important clinical entity and continuing treatment dilemma. Arch Surg. (2001) 136:656–63. doi: 10.1001/archsurg.136.6.656
35. Chen YT, Cornblath M, Sidbury JB. Cornstarch therapy in type I glycogen storage disease. N Engl J Med. (1984) 310:171-5.
36. Smit GPA, Berger P, Potasnick R, Moses SW, Fernandes J. The dietary treatment of children with type I glycogen storage disease with slow release carbohydrate. Ped Res. (1984) 18:879–81.
37. Heller S, Worona L, Consuelo A. Nutritional therapy for glycogen storage diseases. J Pediatr Gastroenterol Nutr. (2008) 47:S15–21. doi: 10.1097/MPG.0b013e3181818ea5
38. Lechner K, Aulinger B, Brand S, Waldmann E, Parhofer KG. Hydrothermally modified slow release corn starch: a potential new therapeutic option for treating hypoglycemia in autoimmune hypoglycemia (Hirata's disease). Eur J Clin Nutr. (2015) 69:1369–70. doi: 10.1038/ejcn.2015.151
39. Lembo E, Lupoli R, Ciciola P, Creanza A, Silvestri E, Saldalamacchia G, et al. Implementation of low glycemic index diet together with cornstarch in post-gastric bypass hypoglycemia: two case reports. Nutrients. (2018) 10:E670. doi: 10.3390/nu10060670
40. Axelsen M, Wesslau C, Lönnroth P, Arvidsson Lenner R, Smith U. Bedtime uncooked cornstarch supplement prevents nocturnal hypoglycaemia in intensively treated type 1 diabetes subjects. J Intern Med. (1999) 245:229–36. doi: 10.1046/j.1365-2796.1999.00432.x
41. Axelsen M, Lönnroth P, Lenner RA, Taskinen MR, Smith U. Suppression of nocturnal fatty acid concentrations by bedtime carbohydrate supplement in type 2 diabetes: effects on insulin sensitivity, lipids, and glycemic control. Am J Clin Nutr. (2000) 71:1108–14. doi: 10.1093/ajcn/71.5.1108
Keywords: persistent hyperinsulinemic hypoglycemia, adult-onset β-cell nesidioblastosis, insulinoma, surgery, management
Citation: Dardano A, Daniele G, Lupi R, Napoli N, Campani D, Boggi U, Del Prato S and Miccoli R (2020) Nesidioblastosis and Insulinoma: A Rare Coexistence and a Therapeutic Challenge. Front. Endocrinol. 11:10. doi: 10.3389/fendo.2020.00010
Received: 02 September 2019; Accepted: 07 January 2020;
Published: 24 January 2020.
Edited by:
Roberta Malaguarnera, University of Catanzaro, ItalyReviewed by:
Giovanni Luca, University of Perugia, ItalyCopyright © 2020 Dardano, Daniele, Lupi, Napoli, Campani, Boggi, Del Prato and Miccoli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Angela Dardano, YW5nZWxhLmRhcmRhbm9AdW5pcGkuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.