 Kjersti Kvernebo-Sunnergren1,2*†
Kjersti Kvernebo-Sunnergren1,2*† Carina Ankarberg-Lindgren2†
Carina Ankarberg-Lindgren2† Karin Åkesson1,3
Karin Åkesson1,3 Mats X. Andersson2,4
Mats X. Andersson2,4 Lena Samuelsson5Lovisa Lovmar5
Lena Samuelsson5Lovisa Lovmar5 Jovanna Dahlgren2
Jovanna Dahlgren2- 1Department of Pediatrics, Ryhov County Hospital, Jönköping, Sweden
- 2Department of Pediatrics, Göteborg Pediatric Growth Research Center, Institute of Clinical Sciences, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 3Division of Pediatrics, Department of Clinical and Experimental Medicine, Linköping University Hospital, Linköping, Sweden
- 4Department of Biological and Environmental Sciences, University of Gothenburg, Gothenburg, Sweden
- 5Department of Clinical Pathology and Genetics, Sahlgrenska University Hospital, Gothenburg, Sweden
Background: Intrauterine growth retardation and short stature are common features in Silver-Russell syndrome (SRS). Despite recombinant growth hormone (rGH) treatment, poor pubertal height gain, affecting adult height (AH), is common. This study investigated whether growth patterns and estrogen concentrations are associated with AH outcome in rGH treated SRS males.
Methods: In this retrospective longitudinal single-center study, 11 males with SRS were classified as non-responders (NR = 6) or responders (R = 5), depending on AH adjusted for midparental height. Epigenetic analysis and longitudinal growth measures, including bone age, rGH related parameters, pubertal development, gonadotropins and estrogen concentrations, were analyzed until AH.
Results: Pubarche before 9 years was only observed in one NR. At 10 years of age, there was no difference in gonadotropins between NR and R. However, estradiol (E2) concentrations at 10 years of age showed a strong association to AH adjusted for MPH (r = −0.78, p < 0.001). Serum E2 (pmol/L) was significantly higher in NR at ages 10 years [median (range) 2 (<2–5) vs. <2 (<2)], 12 years [23 (10–57) vs. 2 (<2–2)] and 14 years [77 (54–87) vs. 24 (<2–38)] but not at 16 years. Birth weight standard deviation score (SDS) was lower in NR [−4.1 (−4.7 to −2.1) vs. −2.7 (−3.3 to −1.7)]. Weight gain (SDS) until pubertal onset was greater in NR [2.4 (1.4–3.5) vs. 0.8 (−0.4 to 1.7)] and pubertal height gain (SDS) was lower in NR [−1.0 (−2.7–0.4) vs. 0.1 (−0.1 to 1.1)]. At AH, a number of NR and R had high E2 concentrations and small testes.
Conclusion: Increased E2 concentrations at age 10, 12, and 14 years were associated to less pubertal height gain, thus affecting AH. Due to the small number of patients, the results need to be confirmed in larger cohorts. The finding of impaired testicular development stresses the need of hormonal evaluation as a complement to clinical and radiological assessment when predicting AH in males with SRS.
Introduction
Silver-Russell syndrome (SRS) is a rare syndromic growth disorder characterized by intrauterine growth restriction, relative macrocephaly, prominent forehead, hemihypotrophy, and a variety of minor malformations including increased risk of hypospadias in boys (1–4). A diagnosis of SRS is based on clinical observations, and a consensus statement offering recommendations on diagnostic approach and management was published in 2017 (2). Epigenetic changes such as 11p15 and maternal uniparental disomy of chromosome 7 are found in some but not all individuals (5). Untreated, adult height (AH) in SRS males is reported to be −3.7 standard deviation score (SDS) (3). Most children with SRS do not suffer from growth hormone deficiency (GHD) but nevertheless benefit from recombinant GH (rGH) treatment, gaining 1.2–1.4 SDS (6–8). Although SRS is a rare disorder, children with SRS in several aspects are a subgroup of children born small for gestational age (SGA) and may serve as a model for how intrauterine and post-natal growth is associated to height gain and hormonal changes later in life.
Early or premature adrenarche has been reported to be more frequent in the SRS population than in the general population (9). Although age at pubertal onset occurs within the normal range, children with SRS seem to enter puberty at the younger end of the spectrum (2). Furthermore, clinical observations claim that SRS children progress through puberty faster than normally expected (2). Regardless of rGH treatment, there seems to be a steeper decline in height SDS from pubertal onset to AH in SRS patients than that in non-SRS patients born SGA with a trend toward a greater height gain in patients with materna uniparental disomy of chromosome 7 and clinical SRS than in 11p15 (6). One explanation for this may be the effects of sex steroids and in particular estrogens on skeletal maturation, leading to pubertal growth spurt at low concentrations in early puberty and growth plate closure at higher estradiol (E2) concentrations in late puberty (10–13).
The hypothesis of this study was that impaired pubertal height gain affecting AH is associated to increased estrogen concentrations before pubertal onset. We evaluated the associations between growth-patterns from birth, GH-related parameters, pubertal development, prepubertal and pubertal gonadotropin, and estrogen concentrations as well as AH outcome in rGH treated boys with SRS.
Materials and Methods
Study Population
Nineteen consecutively referred males born 1988 to 2004 diagnosed with SRS were identified at the national Swedish Centre of reference for SRS at Queen Silvia Children's Hospital in Gothenburg. Eleven of those were longitudinally followed and had reached AH, representing the study subjects. All patients were Caucasian, which was likely due to the demographic of the Swedish population at the time. GH status had been evaluated by both arginine-insulin-tolerance test (AITT) and a 12- to 24-h spontaneous GH secretion test and GHD was defined with a level below a cut-off value corresponding to <10 μg/L, using monoclonal 22 kDa GH-antibodies (14). In one patient referred to the NR group, only a GH spontaneous secretion profile was performed, and in one patient referred to the R group, only an AITT was performed; in both cases with normal results. All subjects had been treated with rGH from an early age (2–6 years) until AH due to SGA and/or GHD indication. When re-evaluating the SRS diagnosis according to current diagnostic standards (2), all patients had ≥4 Netchine-Harbison scores; Tables 1, 2.
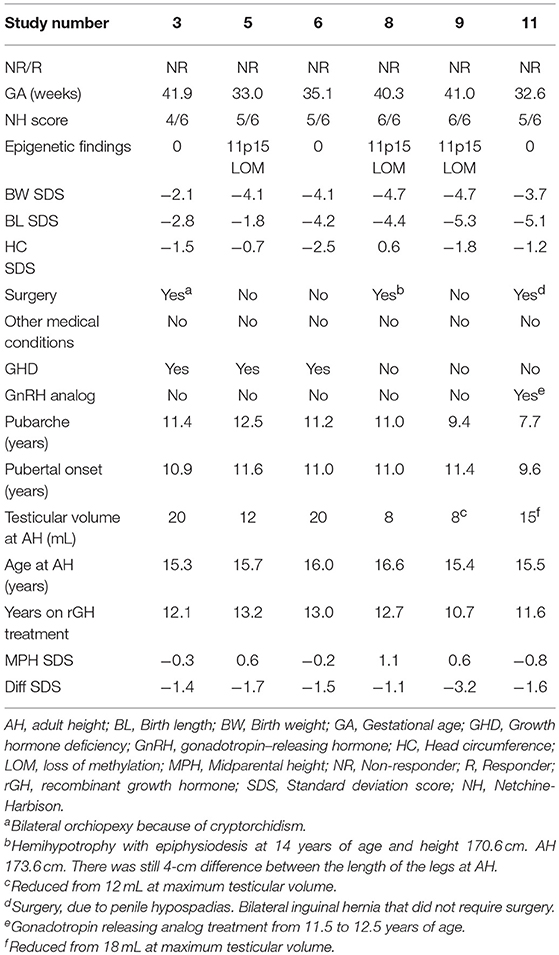
Table 1. Patient characteristics for non-responders (NR).
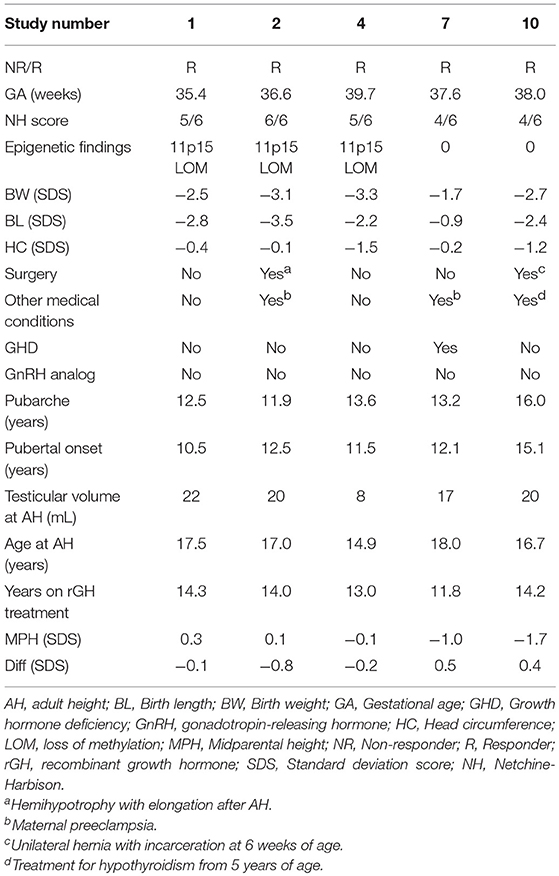
Table 2. Patient characteristics for responders (R).
Depending on AH (SDS) adjusted for mid parental height (MPH), participants were retrospectively divided into one of two groups; six subjects with AH (SDS) >1 SDS below MPH were defined as non-responders (NR), and five subjects with AH (SDS) ≤1 SDS below MPH were defined as responders (R). AH (SDS) was calculated as AH in cm converted to SDS at 18 years of age (15) and MPH (SDS) was calculated as the mean of maternal and paternal AH (SDS). According to the European Agency for the Evaluation of Medicinal Products, rGH treatment may be considered in SGA patients without catch-up growth deviating more than −1 SDS from MPH, thus indicating that height within −1 SDS from MPH should be considered normal (16). The definitions of NR and R do not account for the overall Δ height (SDS) gain during rGH treatment per se, but the definitions account for whether a height close to MPH was reached by AH. Figure 1 exemplifies growth patterns (15) observed in R and NR. For patient characteristics, see Tables 1, 2.
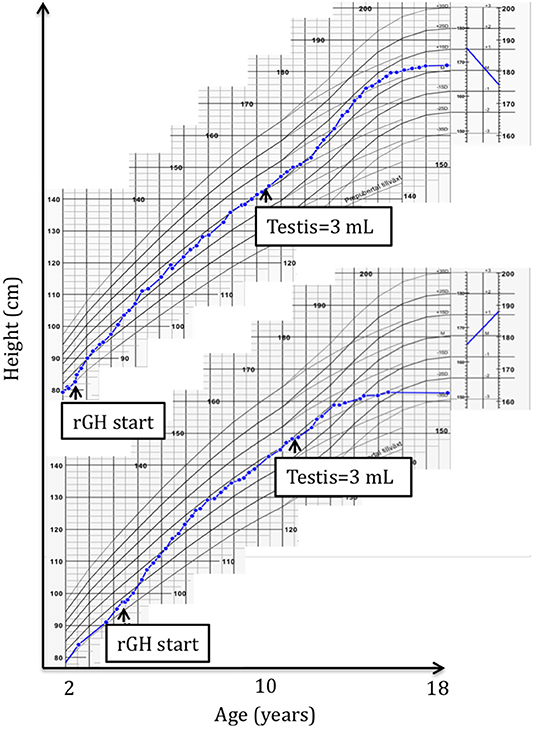
Figure 1. A typical responder (R) height growth chart (top) compared to a typical non-responder (NR) height growth chart (bottom) (15). Start of recombinant growth hormone (rGH) treatment and pubertal onset are pointed out.
Study Protocol
Data on gestational age as well as birth weight (BW), birth length and head circumference were obtained from birth charts and converted to SDS according to Niklasson et al. (17). Blood samples were drawn in the morning (8–11 h) at the start and end of the rGH treatment period and once every year during rGH treatment. After separation, sera were stored at −80°C until analyzed. The stored blood was used to assess changes in epigenetic factors and concentrations of luteinizing hormone (LH), follicle stimulating hormone (FSH), and estrogens at different ages. Other data were collected from patient records. Height, weight and pubertal status were routinely recorded until AH, which was defined as a growth velocity of less than 1 cm/year. Bone age (BA) was assessed from rGH start until 12 years at which age most patients had reached pubertal onset, using standardized routine X-rays that were assessed by a single radiologist using the Tanner-Whitehouse 2 (TW2) method (18). When there were two X-rays equally close to the target age, BA was extrapolated from two sets of samples. Data on the duration of rGH therapy, the individual adjusted rGH dose and the Δ insulin like growth factor-I (IGF-I) (SDS) (19) after 1 year of treatment are shown in Table 3.
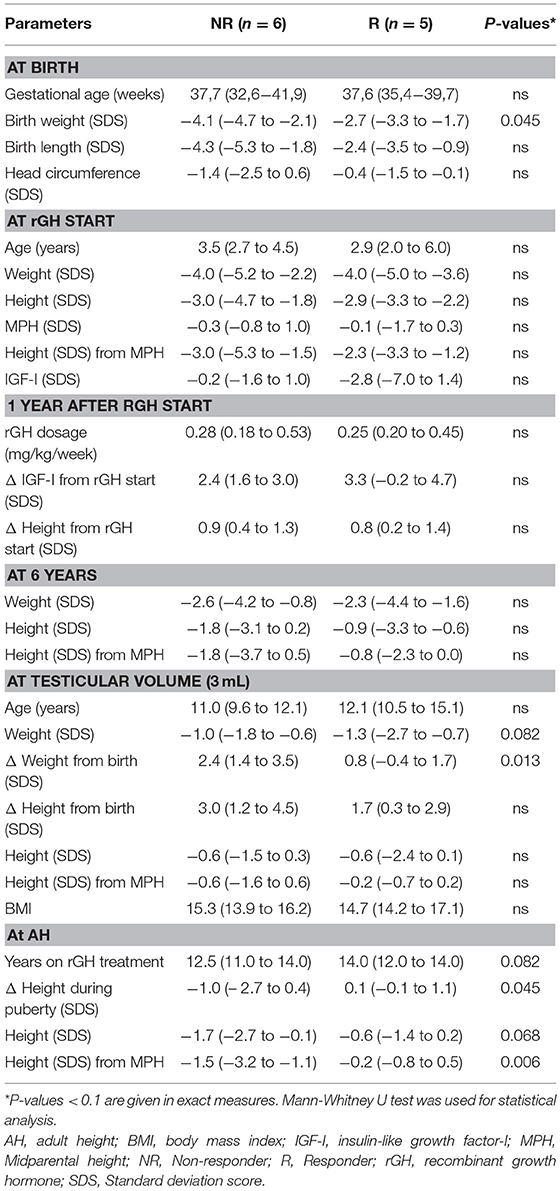
Table 3. Clinical data [median (range)] for non-responders (NR) and responders (R).
Pubertal Classification
Signs of early adrenarche defined as pubarche before the age of 9 years were recorded (9). Pubertal stages were classified according to the largest testis using an orchidometer (20), and pubertal onset was defined by a testicular volume of ≥3 mL. This definition was chosen because of substantial evidence indicating that the hypothalamic-pituitary-gonadal (HPG) axis is activated at a testicular volume of 3 mL (21–23).
Hormone Analysis
Serum LH and FSH concentrations were determined using chemiluminescent microparticle immunoassay (Architect i2000SR, Abbott Scandinavia). Limit of detection (LOD) was 0.1 IU/L for LH and 0.05 IU/L for FSH. Total coefficient of variation (CV) for LH was 7% at 7 IU/L and 50 IU/L and for FSH 6% at 15 and 45 IU/L, respectively. Serum concentrations of estrone (E1) and E2 were simultaneously determined by high-sensitive gas chromatography-tandem mass spectrometry (GC-MS/MS) from Agilent Technologies, Montréal, Canada. LOD was 9 pmol/L for E1 and 2 pmol/L for E2, as previously described (24). Total CV for E1 was 14% for 38 pmol/L and 12% for 100 pmol/L. For E2 the total CV was 19% for 8 pmol/L and 6% for ≥36 pmol/L. Serum IGF-I concentrations were determined by radioimmunoassay (Mediagnost GmbH, Tübingen, Germany). LOD for IGF-I was 0.064 μg/L, and the total CV were 20% and 14% at concentrations of 33 and 179 μg/L, respectively.
Genetic Analysis
DNA was extracted from peripheral blood lymphocytes, and methylation levels were determined by methylation-sensitive multiplex ligation-dependent probe amplification (MS-MLPA, commercial kit ME30 and ME032 from MRC-Holland; SeqPilot software from JSI Medical Systems GmbH). The ME030 kit targets differently methylated regions on chromosome 11p15, and the ME032 kit targets differently methylated regions on chromosome 6q24, chromosome 7p12.1 and 7q32.2 and chromosome 14q32.2. Methylation levels at each locus were intra-sample normalized and then compared to methylation levels observed in healthy reference samples. A methylation level below 0.5 on chromosome 11p15 was considered indicative of loss of methylation (LOM) (25).
Statistical Analysis
Data are expressed as median (range), if not stated otherwise. Hormone concentrations below the LOD were set to LOD/2. Statistical comparisons were conducted between groups at ages closest to 6, 8, 10, 12, 14, and 16 years using the Mann-Whitney U test. IBM SPSS Software Corp. (USA) (version 24) was used for statistical analysis. Associations between E2 at 10 years of age and AH adjusted for MPH was analyzed by simple linear regression analysis using Pearson's correlation coefficient with 95% confidence intervals. Figures were drawn using Origin 9.0 (OriginLab Corp., Northampton, MA, USA). A p-value below 0.05 was considered significant.
Ethics
This study was carried out in accordance with recommendations of the Regional ethical review board in Gothenburg (449-16). The Regional ethical review board of Gothenburg approved the protocol. Written and informed consent was obtained from the parents and retrospectively from the patients at adult age in accordance with the Declaration of Helsinki.
Results
Clinical data including genetic findings for the study group are presented as individual data in Tables 1, 2 and grouped data in Table 3.
Growth Data
BW (SDS) was significantly lower in NR compared to R. Although there was no significant difference in weight or body mass index (BMI) at pubertal onset between the groups, weight gain from birth to pubertal onset was greater in the NR group; Table 3. At the beginning of rGH treatment no significant difference in height (SDS) was observed. Furthermore, height gain during puberty was lower in NR, resulting in impaired AH in NR; Table 3.
GH and IGF-I Status
GHD was confirmed in one R and three NR; Tables 1, 2. At the beginning of rGH treatment, there was no significant difference in IGF-I (SDS) concentrations between the two groups. Changes in IGF-I (SDS), height (SDS) and weekly rGH dose (mg/kg) at start and after 1 year of treatment, as well as the number of years with treatment, were similar in both groups; Table 3.
Estrogen Levels Relative to Age and Puberty
E2 concentrations at 10 years of age showed a strong correlation to AH adjusted for MPH (r = −0.78, p < 0.001); Figure 2.
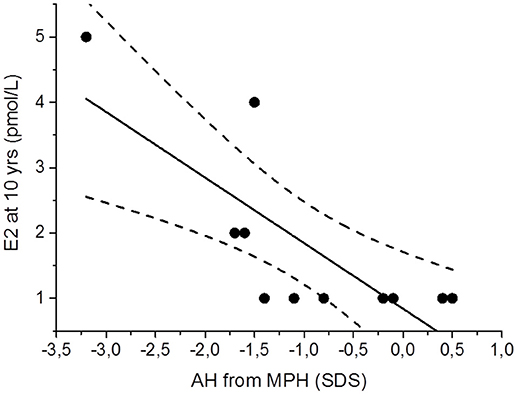
Figure 2. Scatter plot presenting the association between serum estradiol (E2) concentrations at 10 years (yrs) and adult height (AH) adjusted for mid parental height (MPH) in 11 males with Silver-Russell Syndrome. Linear regression analysis (95% confidence bands as dashed lines) yielded a strong negatively correlation: r = −0.78, p < 0.001.
Before 10 years of age, both groups had similar E2 concentrations and E2/E1 ratios; Figures 3A,B. Only one subject in the NR group had a testicular volume of 3 mL at age 10. Nevertheless, the median E2 concentration was higher in the NR group than in the R group [2 (<2–5) vs. <2 (<2) pmol/L; P = 0.034] at this age; Figure 3A. This discrepancy between the two groups was even more evident at the ages of 12 years [23 (10–57) vs. 2 (<2–2) pmol/L; P = 0.006] and 14 years [77 (54–87) vs. 24 (<2–38) pmol/L; P = 0.006]. Moreover, at 12 and 14 years of age, the median E2/E1 ratio was higher in the NR group [0.34 (0.14–0.48) vs. 0.04 (0.01–0.14); P = 0.006 and 0.52 (0.38–1.03) vs. 0.15 (0.02–0.47); P = 0.018]; Figure 3B. At 16 years of age, samples from 9 patients were available (with one patient missing from each group). At this age, there was a borderline significant difference in the E2/E1 ratio with a higher ratio in the NR group [0.76 (0.45–0.95) vs. 0.34 (0.07–0.65); P = 0.050]; however, there were no differences in the E2 concentrations between the two groups; Figures 3A,B.
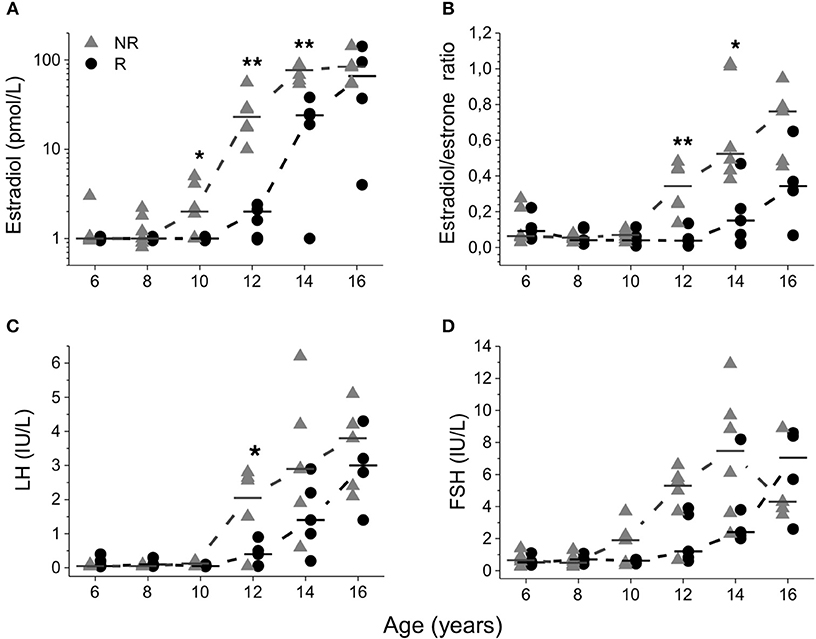
Figure 3. Serum estradiol concentrations (A), estradiol/estrone ratio (B), luteinizing hormone (LH) (C), and follicle stimulating hormone (FSH) (D) plotted relative to age. Median values were calculated and denoted as a line for each group and age. Triangles represent non-responders (NR) and circles represent responders (R). Differences between groups are shown as *p < 0.05 and **p < 0.01.
Although NR had earlier age at pubarche [11.1 (7.7–12.5) vs. 13.2 (11.9–16.0); P = 0.011], pubarche before the age of 9 years was uncommon and only observed in one NR. In two NR and one R, pubarche was observed before onset of puberty. Moreover, although no age difference was seen at pubertal onset between the groups, NR had a significantly larger testicular volume at 12 years of age [6 (3–10) vs. 3 (3–6) mL; P = 0.011]; Figure 4A. Furthermore, at 12 years LH (IU/L) was higher in NR [2.1 (0.1–2.8) vs. 0.4 (0.1–0.9); P = 0.032] but no significant difference was seen in LH at 10 years in NR 0.2 (<0.1–0.2) vs. R < 0.1 (<0.1); Figure 3C. After 12 years of age no significant differences were seen in LH concentrations and no significant differences were seen in FSH (IU/L) concentrations at any age; Figure 3D. At 16 years of age there was one missing data from each group.
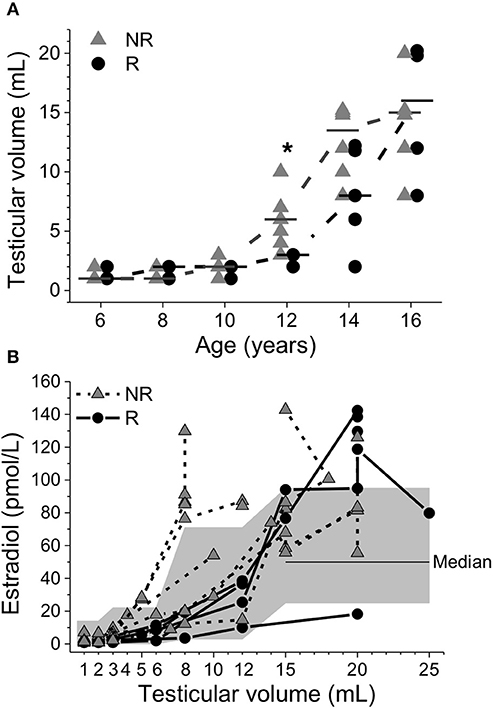
Figure 4. Testicular volume plotted relative to age (A). Median values were calculated and denoted as a line for each group and age. Triangles represent non-responders (NR) and circles represent responders (R). Differences between groups are shown as *p < 0.05. Serum estradiol concentrations plotted relative to testicular volume (B). The gray area depicts reference intervals for healthy boys during pubertal development (24).
Figure 4B shows that beginning at a testicular volume of 5 mL, some NR had E2 concentrations above reference intervals for boys during pubertal development (24). At the end of puberty, patients from both groups, except for one R, had E2 concentrations above the median reference value for adolescent males. At AH, the testicular volume of 1/5 of R and 3/6 of NR did not reach a normal adult testicular volume (≥15 mL). In 2/6 of NR, the testicular volume decreased after the age of 16 years; see Tables 1, 2 for individual data.
Bone Age
No significant differences in BA were found between NR and R, at age 6, 8 or 10 years [5.0 (3.4–6.9) vs. 4.9 (3.8–5.7); 8.1 (5.0–10.4) vs. 7.3 (6.5–7.9); and 10.8 (7.5–12.3) vs. 9.3 (9.1–10.5) years, respectively]. There were no differences in BA between groups at pubertal onset [13.0 (9.1–13.9) vs. 12.8 (10–14.3) years] or chronological age of 12 years [12 (11.4–14.1) vs. 11.7 (11.5–13.3) years]. X-rays were missing in one NR and one R at 12 years of age, at which point both patients had a testicular volume of 3 mL.
Discussion
The main finding of this study was the association between E2 concentrations at 10 years of age and AH outcome adjusted for MPH. NR not reaching MPH despite rGH treatment had lower BW and higher E2 concentrations at ages 10, 12, and 14 years. Increased median E2 concentrations in NR were observed two years earlier compared to R. Moreover, the median loss in height of 1.0 SDS during puberty in NR compared to R, who gained 0.1 SDS, indicated that the difference in AH outcome was caused by incomplete pubertal growth spurt in the NR group. At the end of puberty, several patients from both groups had E2 concentrations above the reference interval for healthy adolescent males. Small adult testicular volumes were observed in a number of patients, and some NR even developed reduced testicular volumes at the end of puberty. Differences in variables related to rGH treatment could not explain the impaired AH outcome in NR. To our knowledge, this is the first publication describing estrogen concentrations during rGH treatment in males with SRS.
The effect of estrogens particularly E2, on bone maturation with subsequent fusion of growth plates is well known (10–13). Although both groups had high E2 concentrations at AH, NR had increasing E2 concentrations 2 years earlier than R. The lack of difference in E2 at 16 years of age reflects that the earlier increase in E2 concentrations rather than high E2 concentrations at AH per se affect AH outcome. In children with SRS, early delay of BA followed by rapid acceleration at 8 to 9 years of age has been reported (2). No significant differences were observed in BA between the two groups, which may have been due to the small number of patients or the fact that BA is not a reliable predictor of height potential in children born SGA (26). Declining height SDS during puberty has been observed in both untreated and in rGH-treated non-SRS children who were born SGA (27, 28). However, despite rGH treatment SRS patients seem to have a steeper decline in height SDS during pubertal spurt compared to non-SRS patients born SGA (6). The results of this study show that only the subgroup of patients with significantly higher E2 concentrations at ages 10, 12, and 14 years and increased E2/E1 ratios at 12 and 14 years had impaired pubertal growth spurt and negatively affected AH. Although accelerated BA in NR was not found in this study, early estrogen exposure in NR is a probable explanation of impaired pubertal height gain and shorter AH through premature bone maturation (10–13).
In the present study a significantly lower BW and greater weight gain from birth to the beginning of puberty was seen in NR. Central adiposity, low BW and rapid weight gain in early childhood may lead to, decreased insulin sensitivity, increased IGF-I concentrations and higher concentrations of adrenal androgens (29). Furthermore, central adiposity affects aromatase activity converting androgens to estrogens and 17β-hydroxysteroid dehydrogenase converting E1 to E2 (30). Interestingly, IGF-II, showing downregulated expression in patients with 11p15 LOM (4, 5, 31, 32), appears to be a potent inhibitor of aromatase activity (33). Our results show that NR who had a significantly lower BW and greater weight catch-up from birth to puberty compared to R did not have significantly higher BMI or weight at pubertal onset. Hence, we believe that BW rather than weight or BMI at pubertal onset explains the difference in Δ weight until start of puberty.
Increased steroid synthesis in the adrenal- and/or gonadal-gland might contribute to the higher E2 concentrations seen in NR through conversion of androgens to estrogens (30). It has been suggested that children born SGA, due to events occurring during fetal development, may show long-term alterations in the hypothalamic-pituitary-adrenal axis that lead to alterations in adrenal activity with earlier and more aggressive adrenarche (2, 4, 31, 32, 34, 35). Furthermore, Binder et al. recently published a retrospective study concluding that early adrenarche is more frequent in rGH treated boys with SRS, but no compromising effect was seen on AH (9). In our study, however pubarche did not occur until after pubertal onset in most patients and in only one NR before the age of 9 years. On the other hand, other publications report disturbed regulation of the HPG axis associated to BW and postnatal growth. Moreover, although normal pubertal timing was reported in boys born SGA (36), hypogonadism was found in adult SGA males without postnatal catch-up growth (37), suggesting that BW and postnatal growth are associated with gonadal function. The results of the current study indicate impaired gonadal function in a number of patients, at least at the end of puberty. The low LH concentrations seen in both groups until the age of 10 years do not indicate that early activation of the HPG axis is present, although there seems to be a more rapid progression through puberty with significantly earlier age at pubarche, and at 12 years of age, both higher LH concentrations and larger testicular volumes in NR. The higher E2 concentrations and lack of difference in LH concentrations at 10 years of age may be due to the small number of patients or reflect a gonadal dysfunction independent of activation of the HPG axis.
The high E2 concentrations observed in both groups by the end of puberty at adult testicular volumes are similar to references for adult males rather than adolescent males (38, 39). A substantial proportion of patients unexpectedly did not reach normal adult testicular volume, and some NR even exhibited a reduction of testicular volume. Together with the finding of high E2 concentrations these results indicate an element of disturbed gonadal function. Hypogonadism has been reported to be frequently present in SRS males in adult life (40), and might be present already during fetal life, explaining the increased risk of male congenital defects of external genitalia, which is reported in as many as 40% of male patients with SRS (2). Taking this in to account, only assessing testicular volume might underestimate the pubertal stage and is unreliable for estimating pubertal development in this group of patients, as testicular function and volume probably are affected already at earlier age.
Determination of estrogen concentrations in children is challenging because serum concentrations of E2 are very low during childhood. The strengths of this study were however the use of a highly sensitive GC-MS/MS-based method, as well as the longitudinal design with repeated serum sampling enabling the identification of the timing of the changes in estrogen secretion patterns. Moreover, epigenetic changes in our cohort were similar to findings reported in larger cohorts, implying that our cohort is a representative SRS population. The results of this study are interesting considering that despite the small number of patients, we found significant differences in BW, weight gain from birth until pubertal onset, prepubertal and early pubertal estrogen concentrations and pubertal height gain between the groups, suggesting a relationship to AH outcome.
The weaknesses of this study are the limited number of patients and the retrospective design and subgrouping of the patients in two groups based on outcome. However, the results of this study have important clinical implications. First, measurements of E2 concentrations with MS/MS rather than clinical assessment of testicular volumes are necessary in order to identify the timing and pace of the biological maturation process in SRS males. Secondly, the results of this study show that the timing of increased estrogen concentrations in SRS males seems to affect pubertal growth spurt and AH, but this needs to be confirmed in larger cohorts.
In conclusion, less pubertal height gain and impaired AH in the NR group were found to be associated with early increase in E2 concentrations and higher E2/E1 ratio. The discrepancies between testicular volumes and E2 concentrations in NR and R reinforce the need for hormonal evaluation as a complement to clinical examination and radiological assessment in SRS males during childhood and puberty when predicting AH.
Author Contributions
JD was responsible for care and treatment of the patients. KK-S, CA-L, and JD contributed to the study design. CA-L and MA were responsible for the mass spectrometry analysis. LS and LL were responsible for the epigenetic analysis. KK-S, CA-L, and JD contributed to the interpretation and analysis of data. KK-S wrote the first draft of the manuscript. CA-L, JD, and KÅ contributed to the final writing and revising of the manuscript and checked for important intellectual content. All authors approved of the final manuscript as submitted.
Funding
This work was financed by grants from Futurum - the Academy for Health and Care, Region Jönköping County (FUTURUM-575601, FUTURUM-765281, FUTURUM-578061, FUTURUM-709351), Pfizer (WI 182827), IngaBritt and Arne Lundberg Research Foundation (2015-103) and the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (ALFGBG-507931).
Conflict of Interest Statement
JD received unrestricted grants from Pfizer.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the patients and their parents for participation in the study, the skillful nurses and the laboratory at GP-GRC. We also thank Futurum-the Academy for Health and Care, Region Jönköping County for statistical support.
References
1. Price SM, Stanhope R, Garrett C, Preece MA, Trembath RC. The spectrum of Silver-Russell syndrome: a clinical and molecular genetic study and new diagnostic criteria. J Med Genet. (1999) 36:837–42.
2. Wakeling EL, Brioude F, Lokulo-Sodipe O, O'Connell SM, Salem J, Bliek J, et al. Diagnosis and management of Silver-Russell syndrome: first international consensus statement. Nat Rev Endocrinol. (2017) 13:105–24. doi: 10.1038/nrendo.2016.138
3. Wollmann HA, Kirchner T, Enders H, Preece MA, Ranke MB. Growth and symptoms in Silver-Russell syndrome: review on the basis of 386 patients. Eur J Pediatr. (1995) 154:958–68. doi: 10.1007/BF01958638
4. Dias RP, Nightingale P, Hardy C, Kirby G, Tee L, Price S, et al. Comparison of the clinical scoring systems in Silver-Russell syndrome and development of modified diagnostic criteria to guide molecular genetic testing. J Med Genet. (2013) 50:635–9. doi: 10.1136/jmedgenet-2013-101693
5. Eggermann T, Begemann M, Binder G, Spengler S. Silver-Russell syndrome: genetic basis and molecular genetic testing. Orphanet J Rare Dis. (2010) 5:19. doi: 10.1186/1750-1172-5-19
6. Smeets CC, Zandwijken GR, Renes JS, Hokken-Koelega AC. Long-term results of GH treatment in Silver-Russell Syndrome (SRS): do they benefit the same as Non-SRS Short-SGA? J Clin Endocrinol Metab. (2016) 101:2105–12. doi: 10.1210/jc.2015-4273
7. Binder G, Liebl M, Woelfle J, Eggermann T, Blumenstock G, Schweizer R. Adult height and epigenotype in children with Silver-Russell syndrome treated with GH. Hormone Res Paediatr. (2013) 80:193–200. doi: 10.1159/000354658
8. Toumba M, Albanese A, Azcona C, Stanhope R. Effect of long-term growth hormone treatment on final height of children with Russell-Silver syndrome. Hormone Res Paediatr. (2010) 74:212–7. doi: 10.1159/000295924
9. Binder G, Schweizer R, Blumenstock G, Ferrand N. Adrenarche in Silver-Russell syndrome: timing and consequences. J Clin Endocrinol Metab. (2017) 102:4100–8. doi: 10.1210/jc.2017-00874
10. Borjesson AE, Lagerquist MK, Windahl SH, Ohlsson C. The role of estrogen receptor alpha in the regulation of bone and growth plate cartilage. Cell Mol Life Sci. (2013) 70:4023–37. doi: 10.1007/s00018-013-1317-1
11. Shim KS. Pubertal growth and epiphyseal fusion. Annals Pediatr Endocrinol Metab. (2015) 20:8–12. doi: 10.6065/apem.2015.20.1.8
12. Emons J, Chagin AS, Savendahl L, Karperien M, Wit JM. Mechanisms of growth plate maturation and epiphyseal fusion. Hormone Res Paediatr. (2011) 75:383–91. doi: 10.1159/000327788
13. Perry RJ, Farquharson C, Ahmed SF. The role of sex steroids in controlling pubertal growth. Clin Endocrinol. (2008) 68:4–15. doi: 10.1111/j.1365-2265.2007.02960.x
14. Jansson C, Boguszewski C, Rosberg S, Carlsson L, Albertsson-Wikland K. Growth hormone (GH) assays: influence of standard preparations, GH isoforms, assay characteristics, and GH-binding protein. Clin Chem. (1997) 43(6 Pt 1):950–6.
15. Wikland KA, Luo ZC, Niklasson A, Karlberg J. Swedish population-based longitudinal reference values from birth to 18 years of age for height, weight and head circumference. Acta paediatrica (2002) 91:739–54. doi: 10.1111/j.1651-2227.2002.tb03322.x
16. Clayton PE, Cianfarani S, Czernichow P, Johannsson G, Rapaport R, Rogol A. Management of the child born small for gestational age through to adulthood: a consensus statement of the International societies of pediatric endocrinology and the growth hormone research society. J Clin Endocrinol Metab. (2007) 92:804–10. doi: 10.1210/jc.2006-2017
17. Niklasson A, Ericson A, Fryer JG, Karlberg J, Lawrence C, Karlberg P. An update of the Swedish reference standards for weight, length and head circumference at birth for given gestational age (1977-1981). Acta Paediatr. Scandinavica (1991) 80:756–62. doi: 10.1111/j.1651-2227.1991.tb11945.x
18. Tanner JM, Whitehouse RH, Cameron N, Marshall W, Healy M, Goldstein H. Assesment of Skeletal Matuity and Prediction of Adult Height (TW2 Method). 2nd Edn. New York, NY: Academic Press (1983).
19. Lofqvist C, Andersson E, Gelander L, Rosberg S, Blum WF, Albertsson Wikland K. Reference values for IGF-I throughout childhood and adolescence: a model that accounts simultaneously for the effect of gender, age, and puberty. J Clin Endocrinol Metab. (2001) 86:5870–6. doi: 10.1210/jcem.86.12.8117
20. Prader A. Testicular size: assessment and clinical importance. Triangle Sandoz J Med Sci. (1966) 7:240–3.
21. Mul D, Fredriks AM, van Buuren S, Oostdijk W, Verloove-Vanhorick SP, Wit JM. Pubertal development in The Netherlands 1965-1997. Pediatr Res. (2001) 50:479–86. doi: 10.1203/00006450-200110000-00010
22. Ankarberg-Lindgren C, Norjavaara E. Changes of diurnal rhythm and levels of total and free testosterone secretion from pre to late puberty in boys: testis size of 3 ml is a transition stage to puberty. Eur J Endocrinol. (2004) 151:747–57. doi: 10.1530/eje.0.1510747
23. Albertsson-Wikland K, Rosberg S, Lannering B, Dunkel L, Selstam G, Norjavaara E. Twenty-four-hour profiles of luteinizing hormone, follicle-stimulating hormone, testosterone, and estradiol levels: a semilongitudinal study throughout puberty in healthy boys. J Clin Endocrinol Metab. (1997) 82:541–9.
24. Ankarberg-Lindgren C, Dahlgren J, Andersson MX. High-sensitivity quantification of serum androstenedione, testosterone, dihydrotestosterone, estrone and estradiol by gas chromatography-tandem mass spectrometry with sex- and puberty-specific reference intervals. J Steroid Biochem Mol Biol. (2018) 183:116–24. doi: 10.1016/j.jsbmb.2018.06.005
25. Priolo M, Sparago A, Mammi C, Cerrato F, Lagana C, Riccio A. MS-MLPA is a specific and sensitive technique for detecting all chromosome 11p15.5 imprinting defects of BWS and SRS in a single-tube experiment. Eur J Hum Genet. (2008) 16:565–71. doi: 10.1038/sj.ejhg.5202001
26. Lee PA, Chernausek SD, Hokken-Koelega AC, Czernichow P. International Small for Gestational Age Advisory Board consensus development conference statement: management of short children born small for gestational age, April 24-October 1, 2001. Pediatrics (2003) 111(6 Pt 1):1253–61. doi: 10.1542/peds.111.6.1253
27. Renes JS, Willemsen RH, Mulder JC, Bakker-van Waarde WM, Rotteveel J, Oostdijk W, et al. New insights into factors influencing adult height in short SGA children: results of a large multicentre growth hormone trial. Clin Endocrinol. (2015) 82:854–61. doi: 10.1111/cen.12677
28. Lazar L, Pollak U, Kalter-Leibovici O, Pertzelan A, Phillip M. Pubertal course of persistently short children born small for gestational age (SGA) compared with idiopathic short children born appropriate for gestational age (AGA). Eur J Endocrinol. (2003) 149:425–32. doi: 10.1530/eje.0.1490425
29. Verkauskiene R, Petraitiene I, Albertsson Wikland K. Puberty in children born small for gestational age. Hormone Res Paediatr. (2013) 80:69–77. doi: 10.1159/000353759
30. Tchernof A, Mansour MF, Pelletier M, Boulet MM, Nadeau M, Luu-The V. Updated survey of the steroid-converting enzymes in human adipose tissues. J Steroid Biochem Mol Biol. (2015) 147:56–69. doi: 10.1016/j.jsbmb.2014.11.011
31. Netchine I, Rossignol S, Dufourg MN, Azzi S, Rousseau A, Perin L, et al. 11p15 imprinting center region 1 loss of methylation is a common and specific cause of typical Russell-Silver syndrome: clinical scoring system and epigenetic-phenotypic correlations. J Clin Endocrinol Metab. (2007) 92:3148–54. doi: 10.1210/jc.2007-0354
32. Eggermann K, Bliek J, Brioude F, Algar E, Buiting K, Russo S, et al. EMQN best practice guidelines for the molecular genetic testing and reporting of chromosome 11p15 imprinting disorders: Silver-Russell and Beckwith-Wiedemann syndrome. Eur J Hum Genet. (2016) 24:1377–87. doi: 10.1038/ejhg.2016.45
33. Nestler JE. Insulin-like growth factor II is a potent inhibitor of the aromatase activity of human placental cytotrophoblasts. Endocrinology (1990) 127:2064–70. doi: 10.1210/endo-127-5-2064
34. Tappy L. Adiposity in children born small for gestational age. Int J Obesity (2005) 30 (Suppl 4):S36–40. doi: 10.1038/sj.ijo.0803517
35. Dahlgren J, Boguszewski M, Rosberg S, Albertsson-Wikland K. Adrenal steroid hormones in short children born small for gestational age. Clin Endocrinol. (1998) 49:353–61. doi: 10.1046/j.1365-2265.1998.00514.x
36. Hernandez MI, Mericq V. Impact of being born small for gestational age on onset and progression of puberty. Best Pract Res Clin Endocrinol Metab. (2008) 22:463–76. doi: 10.1016/j.beem.2008.02.003
37. Cicognani A, Alessandroni R, Pasini A, Pirazzoli P, Cassio A, Barbieri E, et al. Low birth weight for gestational age and subsequent male gonadal function. J Pediatr. (2002) 141:376–9. doi: 10.1067/mpd.2002.126300
38. Nelson RE, Grebe SK, DJ OK, Singh RJ. Liquid chromatography-tandem mass spectrometry assay for simultaneous measurement of estradiol and estrone in human plasma. Clin Chem. (2004) 50:373–84. doi: 10.1373/clinchem.2003.025478
39. Kushnir MM, Rockwood AL, Bergquist J, Varshavsky M, Roberts WL, Yue B, et al. High-sensitivity tandem mass spectrometry assay for serum estrone and estradiol. Am J Clin Pathol. (2008) 129:530–9. doi: 10.1309/LC03BHQ5XJPJYEKG
Keywords: small for gestational age, estrogens, puberty, mass spectrometry, hypogonadism, gonadotropins, Silver-Russell syndrome, adult height
Citation: Kvernebo-Sunnergren K, Ankarberg-Lindgren C, Åkesson K, Andersson MX, Samuelsson L, Lovmar L and Dahlgren J (2018) Hyperestrogenism Affects Adult Height Outcome in Growth Hormone Treated Boys With Silver-Russell Syndrome. Front. Endocrinol. 9:780. doi: 10.3389/fendo.2018.00780
Received: 20 August 2018; Accepted: 11 December 2018;
Published: 21 December 2018.
Edited by:
Mohamad Maghnie, Università di Genova, ItalyReviewed by:
Laura Audí, Vall d'Hebron Research Institute (VHIR), SpainStefano Zucchini, Policlinico S. Orsola Malpighi, Italy
Copyright © 2018 Kvernebo-Sunnergren, Ankarberg-Lindgren, Åkesson, Andersson, Samuelsson, Lovmar and Dahlgren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kjersti Kvernebo-Sunnergren, a2plcnN0aS5rdmVybmViby5zdW5uZXJncmVuQGd1LnNl
†These authors share first authorship