
Articles published with Frontiers have received 12 million total citations
Your research is the real superpower - learn how we maximise its impact through our leading community journals
Explore our impact metrics
ORIGINAL RESEARCH article
Front. Endocrinol., 28 November 2018
Sec. Obesity
Volume 9 - 2018 | https://doi.org/10.3389/fendo.2018.00718
This article is part of the Research TopicMetabolic and Endocrine Consequences of Bariatric/metabolic SurgeryView all 7 articles
 Pedro R. Pereira1,2Marta Guimarães1,2,3Tiago Morais1,2Sofia S. Pereira1,2Mário Nora2,3
Pedro R. Pereira1,2Marta Guimarães1,2,3Tiago Morais1,2Sofia S. Pereira1,2Mário Nora2,3 Mariana P. Monteiro1,2*
Mariana P. Monteiro1,2*Background/Objetives: Obesity and obesity related co-morbidities are well-recognized risks for cardiovascular (CV) disease and mortality. Weight loss improves CV risk factors and the efficacy of bariatric surgery in decreasing CV mortality is now well-established. Our aim was to assess CV risk progression and occurrence of CV events in a cohort of patients that underwent Roux-en-Y gastric bypass (RYGB) for obesity treatment in a single academic public center.
Subjects and Methods: Ten year CV risk was estimated using the Framingham Equation at baseline and 2 years after RYGB surgery in our patients cohort (n = 260). In the subgroup with a follow-up time longer than 4 years after surgery (n = 185; mean 5.4 ± 0.1 years), CV risk adjusted for the time length after RYGB was similarly estimated and the occurrence of CV events for outcome adjudication was monitored during the same time period by reviewing the hospital patients' record, the electronic national health system patient register and our center outpatient clinic records.
Results: Ten year CV risk was significantly reduced 2 years after surgery when compared to baseline, with reductions of 1.65 ± 0.25% in the risk of CV disease. Patients with prior type 2 diabetes and aged 50 years or older experienced a significantly superior CV risk reduction, with diabetic patients experiencing a reduction of their 10–year CV disease risk of 3.58 ± 1.11% vs. a reduction of 1.31 ± 0.20% in non-diabetic patients and with the 10–year risk of CV disease dropping 3.41 ± 0.75% in patients older than 50 vs. a reduction of 0.99 ± 0.18 in patients up to 50 years. For the subgroup of patients with a longer follow-up time, baseline CV risk estimation predicted the occurrence of 6.08 ± 0.56 cardiovascular disease (CVD) events, 3.87 ± 0.39 coronary heart disease (CHD) events, 1.49 ± 0.22 myocardial infarctions (MI), 0.71 ± 0.09 strokes, 0. 28 ± 0.05 deaths from CHD and 0.35 ± 0.05 deaths from CVD. No CV events were adjudicated in this subgroup during follow-up.
Conclusions: RYGB significantly improves CV risk and prevents the occurrence of CV events. For similar weight loss, diabetic and elder patients experience a superior CV risk improvement and may have additional CV benefits after bariatric surgery.
Obesity and obesity-related morbidities are well-established risks for cardiovascular (CV) disease and mortality (1). Obesity has direct effects on CV structure by increasing myocardial fat deposition and altering hemodynamic function (2). In addition, obesity triggers an increased sympathetic activity and a decreased systemic vascular resistance, which result in increased heart rate and cardiac output, generating cardiac overload and eventually leading to left ventricular hypertrophy, atria dilation (3), heart dysfunction and dysrhythmia (4). Moreover, obesity is the central feature of the metabolic syndrome, which includes other CV risk factors such as high blood pressure (BP), lipid abnormalities and altered glucose homeostasis or type 2 diabetes (T2D) (5). Indeed, obese individuals were shown to have at least twice the risk of developing heart failure compared to normal weight individuals (2, 6). Therefore, obesity is undeniably an independent predictor of CV disease (2, 6).
Weight loss allows the improvement of several CV risk factors and was demonstrated not only to decrease overall mortality, but also to specifically prevent CV related mortality (7–9). Bariatric surgery is the most effective means to achieve substantial and sustained weight loss in severely obese patients in whom previous conservative or medical interventions have repeatedly failed (10). Furthermore, there is now considerable evidence derived from prospective trials and meta-analyses that demonstrate the benefits of weight loss attained through bariatric surgery in improving CV risk factors, including reducing BP (11), improving dyslipidemia (12) and ameliorating glycemic control or even inducing clinical remission of T2D (13–15). Moreover, bariatric surgery not only proved to reduce CV risk scores, but also prevents the occurrence of CV events and reduces overall mortality (7, 16). In the Swedish Obesity Subjects Study (SOS study), post-bariatric patients when compared to non-operated weight matched controls, experienced 33% and 53% fewer total and fatal CV events, respectively (17).
Our aim was to evaluate the impact of weight loss attained through Roux-en-Y gastric bypass (RYGB) on CV outcomes by comparing the predicted vs. occurred CV event rate in a cohort of post-RYGB patients attended at a single academic public center.
Subjects enrolled in this study were attended at a single academic public center for Obesity Treatment. To be considered candidates for bariatric surgery patients had to meet the criteria of having a body mass index (BMI) over 40 kg/m2 or over 35 kg/m2 in the presence of obesity-related morbidities, provided previous non-invasive weight loss interventions had failed and there were no contraindications for the proposed surgical intervention. Participants were selected from our prospective database of post bariatric patients operated between 2005 and 2010 (N = 917) based on the following criteria: (1) availability of all clinical and analytical parameters required for CV risk calculation (N = 315) using the Framingham Heart Study (2008) score (as detailed in the section below), (2) having a minimum follow-up time of 2 years after surgery and (3) having a least of one observation in our center per year during the time of follow-up (N = 55 lost to follow-up), yielding the final subset of patients for data analysis (n = 260). To ensure homogeneity of clinical data acquisition and recording in our post-bariatric prospective register, all patients were attended by the same multidisciplinary team that includes endocrinologists, surgeons, psychologists, and nutritionists before and after the RYGB surgery.
The RYGB procedure consisted in the creation of a neo-stomach with an approximate volume of 30 cm3, which was anastomosed to a jejunum loop located 50–60 cm from the ligament of Treitz (gastro-jejunostomy), while the biliopancreatic flow was restored by an entero-enteric anastomosis performed 90 to 120 cm distal to the gastro-jejunostomy. Thereby, RYGB excludes from the gastrointestinal transit approximately 95% of the stomach, the entire duodenum and part of the jejunum.
To estimate CV risk (coronary, cerebrovascular, peripheral arterial disease and heart failure), the updated sex-specific multivariable risk factor algorithm derived from the Framingham Heart Study (2008) was used. This algorithm estimates an individual's overall risk for cardiovascular disease (CVD), as well as the isolated risk for coronary heart disease (CHD), myocardial infarction (MI), stroke, peripheral vascular disease, death from CHD, death from CVD and heart failure in a given period of time spanning from 4 to 10 years. To estimate the risk for each CV event, the Framingham equation uses fasting blood glucose, diagnosis of diabetes, blood pressure, total cholesterol, HDL cholesterol, presence of left ventricular hypertrophy (LVH), tobacco use and family history of CV events (18). Of note that the Framingham algorithm does not specifically include body weight nor BMI for CV risk calculation.
CV risk was estimated before (baseline T0) and 2 years after surgery (T2) in the entire patient cohort. In the subgroup with a follow-up time longer than 4 years after surgery (n = 185; mean 5.4 ± 0.01 years), CV risk adjusted for the time length after RYGB was similarly estimated. Occurrence of CV events was correspondingly monitored in this patient subgroup and for the same time period. The means used for CV event adjudication included: (1) review of hospital patient records for the occurrence of CV events requiring in-hospital admission, (2) review of electronic national health system patient register depicting outpatient clinical records during routine appointments at the general practitioner and (3) review of our center outpatient clinic records. The protocol was reviewed and approved by the Institutional Ethical Review and Hospital Administration Boards in accordance with the recommendations of the Declaration of Helsinki and the European Data Protection Regulations.
Results are presented as mean ± standard error of the mean (Mean ± SEM) unless otherwise specified. D'Agostino & Pearson omnibus test was used to determine the normality of the groups. Comparisons between three or more groups were performed with the Kruskal–Wallis test followed by the Dunn post-hoc test or with One-way ANOVA followed by a Holm-Sidak post-hoc test accordingly to the normality of the data. The difference between two independent experimental groups was evaluated using the unpaired Student t-test or Mann-Whitney U accordingly to the normality of the data. A p < 0.05 was considered statistically significant. All statistical analyzes were performed with the aid of the GraphPad Prism software version 7.00 for windows.
This post-RYGB patient cohort (n = 260) encompassed 91.6% females (n = 238) and 8.4% males (n = 22). At the time of surgery, subjects had a mean age of 42.12 ± 0.62 years and a mean BMI of 43.9 ± 0.4 kg/m2, while 14.9% (n = 39) had been diagnosed with type 2 diabetes (T2D) prior undergoing bariatric surgery. Baseline patient demographics, anthropometric and biochemical features, irrespectively of specific drug treatment for any of these conditions are depicted on Table 1.
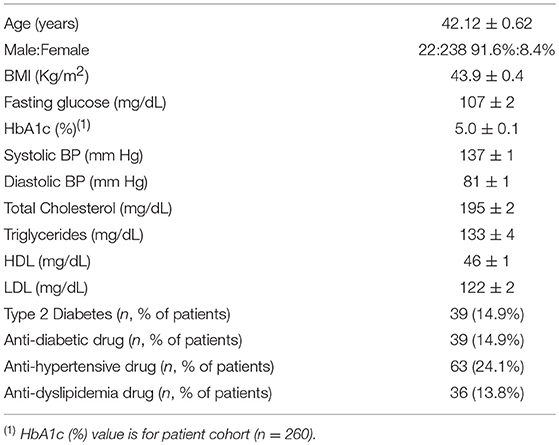
Table 1. Baseline patient demographics, anthropometric and biochemical features.
Patients had an average time after RYGB surgery of 4.41 ± 0.11 years, spanning from a minimum of 2 years to a maximum of 7 years, with the subsequent follow-up time distribution: 4 years 20.7% (n = 54), 5 years 17.3% (n = 44), 6 years 16.9% (n = 43) and 7 years 17.3% (n = 44). A maximum percentage of excess BMI loss [%EBMIL = 100*(BMIBaseline-BMIFollow−up)/(BMIBaseline-25)] of 76.84% ± 1.33% was achieved 2 years after surgery (Table 2). After RYGB surgery there was a significant improvement of several independent CV risk factors, including a decrease in BMI, fasting glucose, total cholesterol, LDL cholesterol, triglycerides, systolic, and diastolic blood pressure, along with an increase in HDL cholesterol (Table 3).
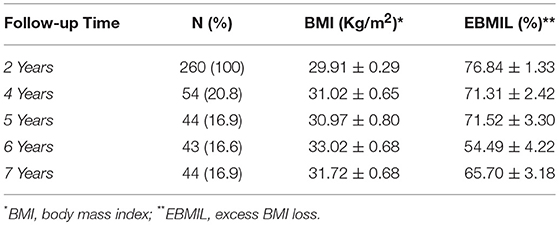
Table 2. Patient population distribution according to follow-up time and corresponding BMI and EBMIL.
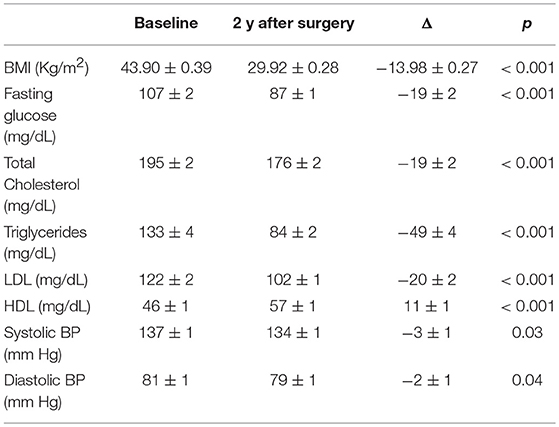
Table 3. Patient anthropometric and biochemical features change from baseline at 2 years of follow-up.
At baseline, the 10-year CV risk predicted by the Framingham Cardiovascular Risk Equation was 7.39 ± 0.48% for CVD, 4.67 ± 0.34% for CHD, 1.99 ± 0.20% for MI, 1.18 ± 0.11% for stroke, 0.58 ± 0.08% for death from CHD and 0.84 ± 0.10% for death from CVD (Figure 1). The 10-year CV risk recalculated 2 years after surgery decreased significantly predicting a risk of 5.74 ± 0.38% for CVD, 3.1 ± 0.22% for CHD, 1.09 ± 0.11% for MI, 1.27 ± 0.10% for stroke, 0.31 ± 0.04% for death from CHD and 0.59 ± 0.07% for death from CVD (Figure 1). Two years after RYGB surgery the 10-year CV risk reduction was statistically significant for most isolated CV events (−1.65 ± 0.25% for CVD, −1.57 ± 0.20% for CHD, −0.91 ± 0.13% for MI, −0.27 ± 0.06% for death from CHD and −0.26 ± 0.06% for death from CVD), with the sole exception of the risk for stroke that did not vary considerably since baseline (0.08 ± 0.08% for stroke; Figure 1).
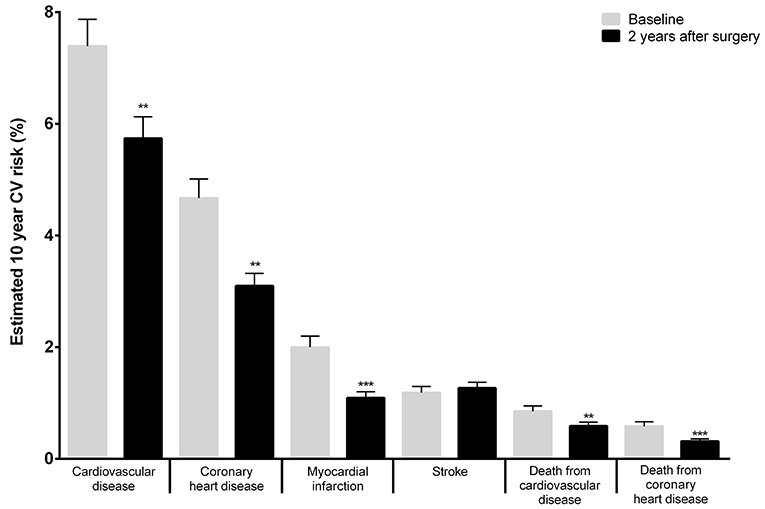
Figure 1. Estimation of the 10-year risk of CV events applying the Framingham Heart Study (2008) score to patients' clinical and analytical features at baseline and 2 years after surgery. As an example, the Framingham Cardiovascular Risk equation predicted a baseline (pre-operative) 10-year risk for CVD events of 7.39 ± 0.49% and 2 years after surgery this risk was of 5.74 ± 0.38% (**p < 0.01; ***p <0.001–baseline vs. 2 years after surgery).
Patients diagnosed with T2D prior to surgery had a significant decrease in 10-year risk for most CV events when compared to non-diabetic individuals, once excluded the risk for stroke (Figure 2). In addition, patient stratification according to age [ < 50 years (n = 182) and ≥ 50 years (n = 82)], showed that the elder group experienced a significant 10-year CV risk reduction when compared to the younger group (Figure 3); these differences prevailed even after excluding T2D patients from the analysis, as the condition was more frequent in the elder patient group (Supplementary Data, Figure S1, Table S1). Apart from fasting glucose levels that decreased significantly in T2D patients as compared to non-diabetic patients, the change from baseline of all other CV risk parameters that were evaluated experienced similar improvements, including BMI (Table 4). Similar findings were observed when the clinical profiles of younger and older patients before and after surgery were compared (Table 5).
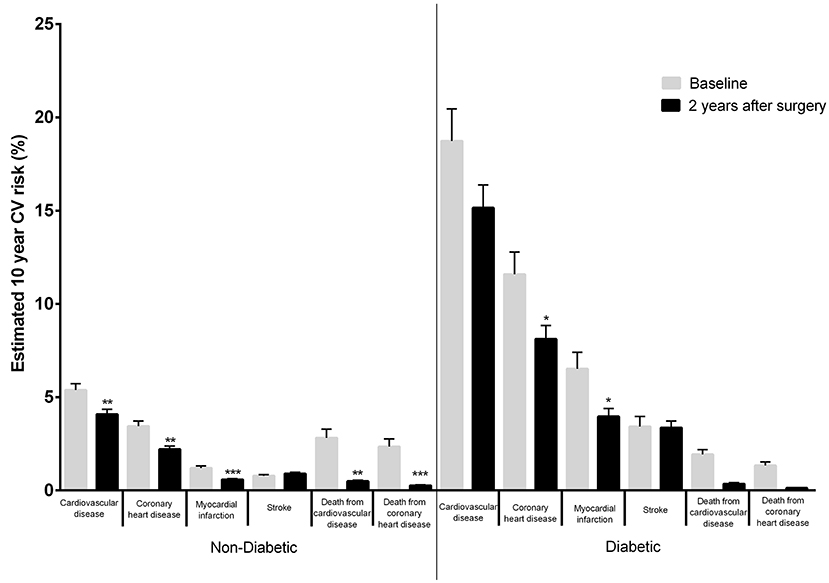
Figure 2. Estimated 10-year CV risk applying the Framingham Heart Study (2008) score to patients' clinical and analytical data at baseline and 2 years after surgery in diabetic and non-diabetic patients. As an example, in non-diabetic patients, the Framingham Cardiovascular Risk equation predicted a pre-surgical 10-year risk of CVD events of 5.39 ± 0.34 and a 10-year risk for CVD events 2 years after surgery of 4.08 ± 0.28% while in diabetic patients, the Framingham Cardiovascular Risk equation predicted a pre-surgical 10-year risk of CVD events of 18.74 ± 1.72% and a 10-year risk for CV events 2 years after surgery of 15.16 ± 1.22% for CVD (*p < 0.05; **p < 0.01; ***p < 0.001–baseline vs. 2 years after surgery).
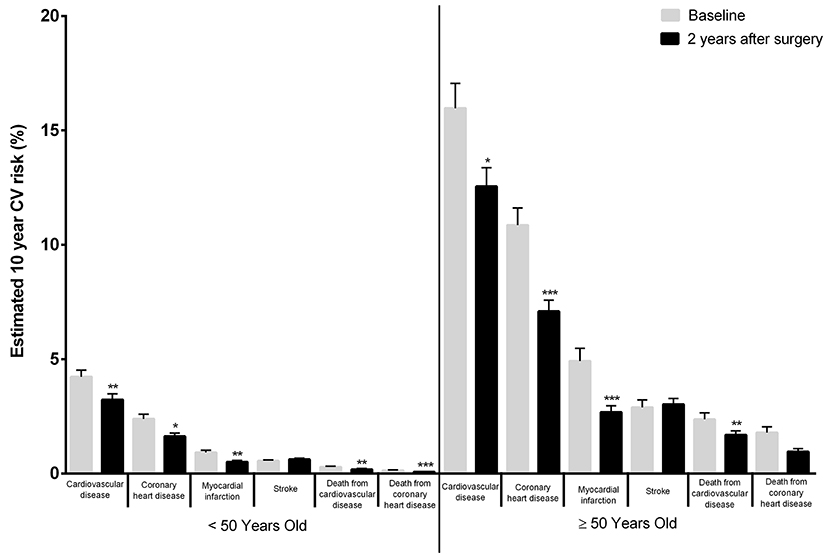
Figure 3. Estimated 10-year CV risk in different age groups applying the Framingham Heart Study (2008) score to patients' clinical and analytical data prior to surgery and 2 years after surgery. As an example, the Framingham Cardiovascular Risk equation predicted a pre-surgical 10-year risk of CVD events of 4.23 ± 0.29% in patients younger than 50 while in patients with at least 50 years the same risk was of 15.97 ± 1.09%. Two years after surgery the 10-year risk of CVD had drop to 3.23 ± 0.25% for patients younger than 50 while for patients with at least 50 years it had drop to 12.55 ± 0.82% (*p < 0.05; **p < 0.01; ***p < 0.001–baseline vs. 2 years after surgery).
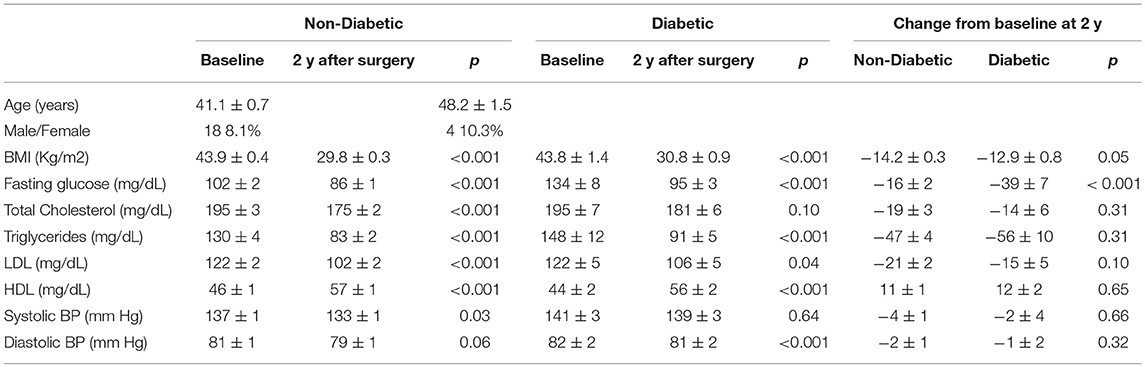
Table 4. Comparison of clinical and biochemical features at baseline and 2 years after surgery according to the presence of type 2 diabetes prior to RYGB surgery.
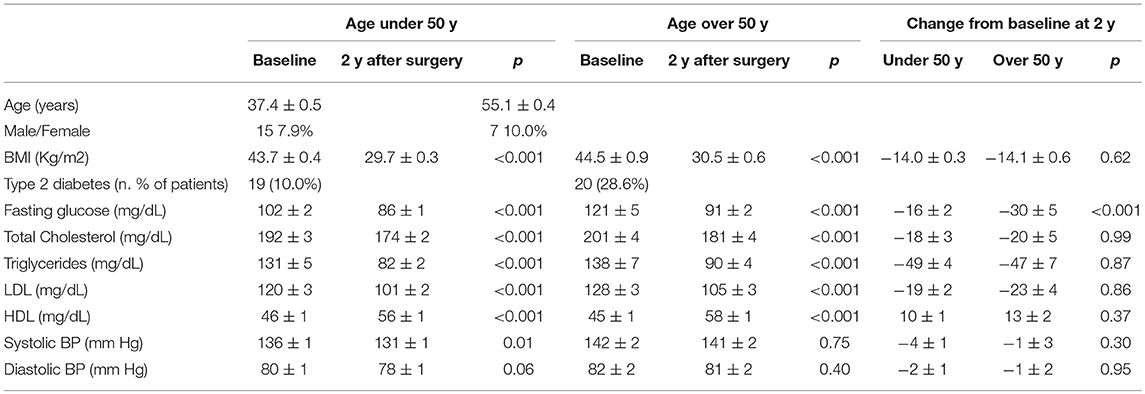
Table 5. Comparison of clinical and biochemical features at baseline and 2 years after surgery according to the patients age at the time of RYGB surgery.
For the subset of patients with more than 4 years of surgery the number of predicted CV events was calculated by adjusting the Framingham Equation to the follow-up time of each individual. Based on the CV risk estimation, 6.08 ± 0.56 CVD events, 3.87 ± 0.39 CHD events, 1.49 ± 0.22 MIs, 0.81 ± 0.09 strokes, 0.28 ± 0.05 deaths from CHD and 0.35 ± 0.05 deaths from CVD were predicted to occur in this subset of patients during the elapsed follow-up time (Figure 4).
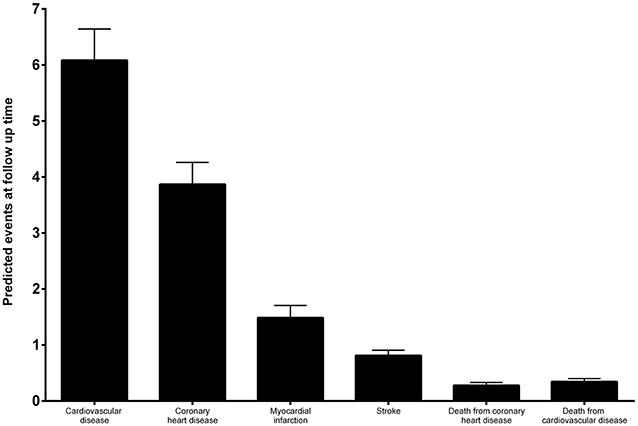
Figure 4. Estimation of the predicted number of CV events during follow-up-time by applying the Framingham Heart Study (2008) score to baseline characteristics of patients with a minimum follow-up of 4 years.
No CV events were adjudicated during follow-up time.
Obesity is often associated with a high CV risk that weight loss can mitigate (8, 19). Bariatric surgery induces substantive and sustained weight reduction, in addition to improving several CV risk factors and decreasing CV events and mortality (17, 20, 21). RYGB is a bariatric surgery procedure widely performed for obesity treatment with a well-established effectiveness profile in inducing weight loss in addition to the ability to prevent or even to revert obesity related disorders, such as T2D and CV diseases (12, 22).
In this study we sought to evaluate the CV outcomes associated with weight loss achieved through RYGB surgery by comparing the predicted vs. occurred CV events in a cohort of patients attended in a single academic public center.
In this patient cohort, RYBG surgery induced a significant and sustained weight loss. The maximum weight reduction was achieved 2 years after surgery with a %EBMIL of 76.84%. At that same time point, the estimated 10-year CV risk also decreased significantly when compared to the estimated 10-year CV risk at baseline before the surgical procedure.
Moreover, CV risk reduction was significantly higher in patients with T2D diagnosed prior to surgery. In fact, the 10-year CV risk reductions with greater magnitude were observed for the risks of CHD, MI and CVD, outdoing the CV risk reductions experienced by non-diabetic patients. The sole exception was for the risk of stroke, which was not significantly altered after the intervention, corroborating earlier data from the SOS study, since weight loss after bariatric surgery has not shown to influence the incidence of stroke (23). Remarkably, this observation is quite consistent with other previous findings including those of large trials to assess the cardiovascular outcomes associated with glucose lowering drugs, such as the EMPA-REG trial, which has demonstrated that empaglifozin has several CV benefits in T2D patients and yet it failed to reduce the risk of stroke (24). Furthermore, weight loss elicited by bariatric surgery was proven to be particularly effective in decreasing the CV risk, as well as preventing CV events and mortality in individuals with high insulin and/or glucose levels at baseline (13, 23). Therefore, our data upholds the previous findings further supporting that T2D obese patients submitted to bariatric surgery may have additional CV benefits, besides the well-known glycemic improvement or even T2D clinical remission (17, 23). Subjects with diabetes are known for carrying a disproportionately higher risk of CV disease when compared to non-diabetic subjects. In fact, a significant proportion of T2D patients experience clinical remission of the disease after several bariatric surgical interventions, such as RYGB, along with a significant improvement of several independent CV risk factors, including blood glucose levels, blood pressure and lipid profile, which synergistically result in an overall decrease of the estimated CV risk (14). Moreover, the weight loss profile of patients with T2D diagnosed prior to RYGB surgery was no different from non-diabetic patients, reinforcing the effectiveness of this weight reducing intervention in T2D patients and the likely dissociation of the observed effects in what concerns body weight and CV risk factors.
Age is one of the most important determinants of CV health (25, 26). In earlier times, several national and international guidance's recommended that weight loss surgical interventions should be restricted to patients under 60 years old based on the concerns of age-related increased surgical risks (27). Nonetheless, as the amount of clinical evidence enlarged, it became recognizable that the surgical outcomes of bariatric surgery, including morbidity and mortality rates, in older patients were not significantly different than those observed in younger ones (28–31). Thus, the number of bariatric procedures performed in older patients has increased over the past decades (32, 33). Our data not only reinforces that weight loss achieved after RYGB in patients over 50 years old are not inferior to the observed in younger patients, but also suggests that the CV benefits in this patient group as compared to the younger ones are also more likely to be superior. This difference persists even after the exclusion of T2D patients from analysis, as the decrease in CV risk was still significantly higher in patients older than 50 years, further suggesting that age could be an additional factor to retrieve benefits from surgery.
The fact that our sample size is relatively small when compared to nationwide epidemiologic studies such as the SOS Study, is in no doubt the major limitation of this current study. However, given that our data refers to a single center population, with similar background demographic and clinical features, submitted to a single bariatric surgery technical procedure by the same multidisciplinary team and delivered the same standards of patient care, allowed the retrieval of robust data information for statistical analysis, and thus valid conclusions can be still be ascertained. Nevertheless, the fact that this was a retrospective review of patient records instead of a prospective study designed to assess CV outcomes with formal event adjudication, implies that the level of evidence retrieved from this study is not as high as it would be if derived from a clinical trial. Besides that, there was a 17.5% loss to follow-up rate of subjects that did not have a minimum of 4 years of follow-up after surgery or a minimum of one observation per year during the follow-up time, although, no significant differences in baseline characteristics between participants with long-term follow-up and drop outs were noticed.
Additionally, our data based on CV risk estimated before RYGB surgery predicted that 6 CVD events would have occurred during the elicited follow-up time if patients had not been intervened. However, there were no CV events adjudicated during the same time period. Overall, there was a significant difference between the estimated CV risk and the actual incidence of CV events observed, while RYGB surgery may have prevented 6 CV events in this patient population.
Weight loss attained trough RYGB surgery was associated with a substantial CV risk reduction and prevented the occurrence of CV events. In addition, diabetic and elder patients experience a superior CV risk reduction and may have additional CV benefits after bariatric surgery, despite depicting similar weight loss and risk factors improvement.
PP, TM, MG, SP, and MM planned and designed the study. PP, MG, and MN conducted data acquisition. TM performed the statistical analysis. PP, TM, and MM participated in analysis and interpretation of data. PP and MM wrote the manuscript; PP, TM, MG, SP, MN, and MM revised the manuscript. All authors approved the submitted version.
UMIB is funded by grants from Foundation for Science and Technology (FCT) Portugal (UID/Multi/00215/2013 and UID/MULTI/0215/2016).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Part of this work was published as Pedro Reis Pereira Master's Thesis, that is available in its entirety online at University of Porto Repository (34).
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2018.00718/full#supplementary-material
1. Prospective Studies C, Whitlock G, Lewington S, Sherliker P, Clarke R, Emberson J, et al. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet (2009) 373:1083–96. doi: 10.1016/S0140-6736(09)60318-4
2. Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, Larson MG, et al. Obesity and the risk of heart failure. N Engl J Med. (2002) 347:305–13. doi: 10.1056/NEJMoa020245
3. Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. J Am Coll Cardiol. (2009) 53:1925–32. doi: 10.1016/j.jacc.2008.12.068
4. Lee GK, Cha YM. Cardiovascular benefits of bariatric surgery. Trends Cardiovas. Med. (2015) 26:280–9. doi: 10.1016/j.tcm.2015.07.006
5. Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome. a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; american heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation (2009) 120:1640–5. doi: 10.1161/circulationaha.109.192644
6. Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation (1983) 67:968–77.
7. Adams TD, Gress RE, Smith SC, Halverson RC, Simper SC, Rosamond WD, et al. Long-term mortality after gastric bypass surgery. N Engl J Med. (2007) 357:753–61. doi: 10.1056/NEJMoa066603
8. Ma C, Avenell A, Bolland M, Hudson J, Stewart F, Robertson C, et al. Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: systematic review and meta-analysis. BMJ (2017) 359:j4849. doi: 10.1136/bmj.j4849
9. Clifton PM, Keogh JB. Effects of different weight loss approaches on CVD risk. Curr Atherosclerosis Rep. (2018) 20:27. doi: 10.1007/s11883-018-0728-8
10. Gloy VL, Briel M, Bhatt DL, Kashyap SR, Schauer PR, Mingrone G, et al. Bariatric surgery versus non-surgical treatment for obesity: a systematic review and meta-analysis of randomised controlled trials. BMJ (2013) 347:f5934. doi: 10.1136/bmj.f5934
11. Livingston EH. Surgical volume impacts bariatric surgery mortality: a case for bariatric surgery centers of excellence. Surgery (2010) 147:751–3. doi: 10.1016/j.surg.2009.10.038
12. Sjostrom L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, Carlsson B, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. (2004) 351:2683–93. doi: 10.1056/NEJMoa03562213
13. Ribaric G, Buchwald JN, McGlennon TW. Diabetes and weight in comparative studies of bariatric surgery vs conventional medical therapy: a systematic review and meta-analysis. Obesity Surg. (2014) 24:437–55. doi: 10.1007/s11695-013-1160-3
14. Nora M, Morais T, Almeida R, Guimaraes M, Monteiro MP. Should Roux-en-Y gastric bypass biliopancreatic limb length be tailored to achieve improved diabetes outcomes? Medicine (2017) 96:e8859. doi: 10.1097/md.0000000000008859
15. Beamish AJ, Olbers T, Kelly AS, Inge TH. Cardiovascular effects of bariatric surgery. Nat Rev Cardiol. (2016) 13:730–43. doi: 10.1038/nrcardio.2016.162
16. Kwok CS, Pradhan A, Khan MA, Anderson SG, Keavney BD, Myint PK, et al. Bariatric surgery and its impact on cardiovascular disease and mortality: a systematic review and meta-analysis. Int J Cardiol. (2014) 173:20–8. doi: 10.1016/j.ijcard.2014.02.026
17. Sjostrom L, Peltonen M, Jacobson P, Sjostrom CD, Karason K, Wedel H, et al. Bariatric surgery and long-term cardiovascular events. JAMA (2012) 307:56–65. doi: 10.1001/jama.2011.1914
18. D'Agostino RB, Sr., Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham heart study. Circulation (2008) 117:743–53. doi: 10.1161/circulationaha.107.699579
19. Vogel JA, Franklin BA, Zalesin KC, Trivax JE, Krause KR, Chengelis DL, et al. Reduction in predicted coronary heart disease risk after substantial weight reduction after bariatric surgery. Am J Cardiol. (2006) 99:222–6. doi: 10.1016/j.amjcard.2006.08.017
20. Chang SH, Stoll CR, Song J, Varela JE, Eagon CJ, Colditz GA. The effectiveness and risks of bariatric surgery: an updated systematic review and meta-analysis, 2003-2012. JAMA Surg. (2014) 149:275–87. doi: 10.1001/jamasurg.2013.3654
21. Sjostrom L, Narbro K, Sjostrom CD, Karason K, Larsson B, Wedel H, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. (2007) 357:741–52. doi: 10.1056/NEJMoa066254
22. Mingrone G, Panunzi S, De Gaetano A, Guidone C, Iaconelli A, Nanni G, et al. Bariatric-metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial. Lancet (2015) 386:964–73. doi: 10.1016/S0140-6736(15)00075-6
23. Romeo S, Maglio C, Burza MA, Pirazzi C, Sjoholm K, Jacobson P, et al. Cardiovascular events after bariatric surgery in obese subjects with type 2 diabetes. Diab Care (2012) 35:2613–7. doi: 10.2337/dc12-0193
24. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. (2015) 373:2117–28. doi: 10.1056/NEJMoa150472025.
25. North BJ, Sinclair DA. The intersection between aging and cardiovascular disease. Circulation Res. (2012) 110:1097–108. doi: 10.1161/circresaha.111.246876
26. Finegold JA, Asaria P, Francis DP. Mortality from ischaemic heart disease by country, region, and age: statistics from World Health Organisation and United Nations. Int J Cardiol. (2013) 168:934–45. doi: 10.1016/j.ijcard.2012.10.046
27. Fried M, Yumuk V, Oppert JM, Scopinaro N, Torres A, Weiner R, et al. Interdisciplinary European guidelines on metabolic and bariatric surgery. Obesity Surg. (2014) 24:42–55. doi: 10.1007/s11695-013-1079-8
28. Giordano S, Victorzon M. Bariatric surgery in elderly patients: a systematic review. Clin Interv Aging (2015) 10:1627–35. doi: 10.2147/CIA.S70313
29. Dunkle-Blatter SE, St Jean MR, Whitehead C, Strodel W, III, Bennotti PN, Still C, et al. Outcomes among elderly bariatric patients at a high-volume center. Surg Obesity Related Dis. (2007) 3:163–9; discussion: 9–70. doi: 10.1016/j.soard.2006.12.004
30. Davidson LE, Adams TD, Kim J, Jones JL, Hashibe M, Taylor D, et al. Association of patient age at gastric bypass surgery with long-term all-cause and cause-specific mortality. JAMA Surg. (2016) 151:631–7. doi: 10.1001/jamasurg.2015.5501
31. Batsis JA, Miranda WR, Prasad C, Collazo-Clavell ML, Sarr MG, Somers VK, et al. Effect of bariatric surgery on cardiometabolic risk in elderly patients: a population-based study. Geriatr Gerontol Int. (2016) 16:618–24. doi: 10.1111/ggi.12527
32. Gonzalez-Heredia R, Patel N, Sanchez-Johnsen L, Masrur M, Murphey M, Chen J, et al. Does age influence bariatric surgery outcomes? Bariatric Surg Pract Patient Care (2015) 10:74–8. doi: 10.1089/bari.2015.0004
Keywords: cardiovascular risk, cardiovascular outcome, obesity, bariatric/metabolic surgery, diabetes
Citation: Pereira PR, Guimarães M, Morais T, Pereira SS, Nora M and Monteiro MP (2018) Diabetic and Elder Patients Experience Superior Cardiovascular Benefits After Gastric Bypass Induced Weight Loss. Front. Endocrinol. 9:718. doi: 10.3389/fendo.2018.00718
Received: 24 July 2018; Accepted: 13 November 2018;
Published: 28 November 2018.
Edited by:
Felipe F. Casanueva, Universidade de Santiago de Compostela, SpainReviewed by:
David Scott, Monash University, AustraliaCopyright © 2018 Pereira, Guimarães, Morais, Pereira, Nora and Monteiro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariana P. Monteiro, bXBtb250ZWlyb0BpY2Jhcy51cC5wdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Frontiers' impact
Your research is the real superpower - learn how we maximise its impact through our leading community journals