
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 28 May 2018
Sec. Translational and Clinical Endocrinology
Volume 9 - 2018 | https://doi.org/10.3389/fendo.2018.00252
This article is part of the Research Topic Classic and Pleiotropic Actions of Vitamin D View all 18 articles
 Mila W. Reginatto1
Mila W. Reginatto1 Bartira M. Pizarro1
Bartira M. Pizarro1 Roberto A. Antunes1,2,3
Roberto A. Antunes1,2,3 Ana C. A. Mancebo2
Ana C. A. Mancebo2 Luísa Hoffmann1
Luísa Hoffmann1 Pâmela Fernandes1Patrícia Areas2Maria I. Chiamolera4Rosane Silva1
Pâmela Fernandes1Patrícia Areas2Maria I. Chiamolera4Rosane Silva1 Maria do Carmo Borges de Souza2
Maria do Carmo Borges de Souza2 Enrrico Bloise5
Enrrico Bloise5 Tânia M. Ortiga-Carvalho1*
Tânia M. Ortiga-Carvalho1*
Purpose: Calcitriol, or 1,25-hydroxycholecalciferol, is the active form of vitamin D. It binds and activates vitamin D receptor (VDR). Infertility and defective folliculogenesis have been observed in female vdr-knockout mice; however, whether VDR polymorphisms affect human ovarian responses to controlled ovarian stimulation (COS) remains unclear. We hypothesized that VDR polymorphisms are associated with infertility and COS responses. Thus, we evaluated the association between the TaqI, BsmI, and FokI VDR polymorphisms and ovarian responses in women undergoing COS.
Methods: In this study, we recruited a control group (n = 121) comprising volunteers with a history of natural conception and a second group of women undergoing COS (n = 70). TaqI, BsmI, and FokI genotyping was performed via restriction fragment length polymorphism analysis or TaqMan qPCR and Sanger sequencing. Intrafollicular 25(OH)D contents were measured in follicular fluid collected from COS patients during oocyte retrieval. Ovarian response parameters were obtained from patient medical records.
Results: There were no significant differences in the genotype frequencies of VDR polymorphisms (TaqI, BsmI and FokI) between the control and COS groups. However, the allele frequency of TaqI (C allele) was significantly lower in the COS group than in the control group (p = 0.02). Follicle number but not oocyte number was lower in patients with TaqI polymorphic (TC/CC) genotypes (p = 0.03). Importantly, the ratio between the number of follicles retrieved and intrafollicular estradiol concentrations was higher in patients with the TC/CC TaqI genotypes (p < 0.02).
Conclusion: We identified an association between the VDR TaqI polymorphism and reduced follicle number in women undergoing COS, suggesting that VDR signaling affects the ovarian response to stimulation via unknown mechanisms.
Calcitriol, or 1,25-hydroxycholecalciferol (1,25(OH)2D), is the active form of vitamin D, a steroid hormone that exerts classical functions in calcium and phosphorus homeostasis and bone mineralization (1). Calcitriol binds its nuclear receptor, vitamin D receptor (VDR) (2), and has an array of actions in the immunological, cardiovascular (3), and reproductive systems of both genders (4). In particular, a number of studies have demonstrated an association between 25-hydroxyvitamin D (25(OH)D) concentrations and different causes of infertility in animals (3, 5–8) and humans (9–14).
VDR expression has been reported in different central (hypothalamus and hypophysis) and peripheral reproductive organs (ovary, uterus, placenta, and oviduct) (13, 15, 16). Evidence linking calcitriol and reproductive function has been demonstrated in 7-week-old female vdr-knockout mice. These animals exhibited uterine hypoplasia, defective folliculogenesis (the absence of mature follicles), and associated infertility (6, 7). Moreover, female vdr-knockout mice exhibited decreased aromatase expression and activity in the ovary, and these effects were associated with elevated serum luteinizing hormone (LH) and follicle-stimulating hormone (FSH) concentrations, indicating a peripheral rather than a central defect (8) and suggesting a role for calcitriol in regulating folliculogenesis.
Genetic alterations in the VDR gene may lead to important defects in gene activation. Alterations were reported to affect calcium metabolism, cell proliferation, and immune function (17). Furthermore, some VDR single-nucleotide polymorphisms (SNPs) may contribute to a genetic predisposition to certain diseases. SNPs present in the VDR gene alter receptor length and decrease its activation in target cells (18). Among these polymorphisms, the best described are TaqI, BsmI, and FokI. TaqI (rs731236, changes T/C, exon 9) and BsmI (rs1544410, changes G/A, intron 8) are present in the 3′ untranslated region (3′ UTR) of the VDR gene and are related to modulation of gene and protein expression of the receptor. The FokI polymorphism (rs2228570, changes T/C, exon 9), in turn, is present in a translated region and effects functional activity by generating a longer VDR protein with reduced transcriptional activity (19).
These polymorphisms have been previously associated with increased risk of developing diabetes (20), tuberculosis (FokI polymorphism) (21), specific cancers (22, 23), and multiple sclerosis (24). Conversely, they were also associated with protection against breast cancer (TaqI polymorphism) (25), osteoporosis (26), and asthma (FokI polymorphism) (27). However, no associations between VDR polymorphisms have been reported in conditions such as osteoporosis (28), colorectal cancer (29), and metabolic syndrome (30). In the context of reproductive medicine, VDR polymorphisms have been associated with polycystic ovarian syndrome and endometriosis (17, 31–38), although these results are inconclusive and require further investigation.
25(OH)D deficiency is now recognized as a pandemic condition (39). In Brazil, 25(OH)D deficiency is largely detected in women of different ages, including elderly and postmenopausal women (40) and women of reproductive age (41). Controlled ovarian stimulation (COS), which aims to increase the success rate of in vitro fertilization (IVF) through stimulation of folliculogenesis, revealed a decrease in the pregnancy (42) and fertilization rates (43) in women with lower 25(OH)D concentrations.
Moreover, other studies have demonstrated that women with replete serum concentrations of 25(OH)D (42) or at least sufficient 25(OH)D in the follicular fluid (FF) had lower pregnancy and fertilization rates (44). A recent study from our group demonstrated that women with lower follicular 25(OH)D concentrations exhibited better outcomes when treated with the COS protocol in that they produced more larger follicles and had higher serum estradiol concentrations (45). Despite these controversial data, in vitro and animal model studies strongly support a significant role of calcitriol in orchestrating reproductive processes and IVF outcomes (46). However, further studies are warranted to demonstrate a causal relationship between 25(OH)D status and infertility.
In the present study, we hypothesized that VDR polymorphisms are associated with infertility and response to COS. The identification of specific VDR polymorphisms that can be shown to be related to infertility and response to COS may help clarify the causes underlying female infertility and poor ovarian response.
Two groups of patients were enrolled for each polymorphism analysis. The control group comprised volunteer women with no history of reproductive disorders. To be included in the control group, volunteers had to declare that they had become pregnant through natural conception at least once and had never experienced any difficulties in conceiving. The COS group consisted of women who underwent COS for intracytoplasmic sperm injection (ICSI) at the Fertipraxis Center for Human Reproduction, a clinic certified by the Brazilian Health Surveillance Authority (ANVISA) and the Latin American Network of Assisted Reproduction (REDLARA). We enrolled 62 controls and 47 COS-treated women in the TaqI polymorphism analysis, 57 controls and 49 COS-treated women in the FokI analysis, and 86 controls and 54 patients in the BsmI analysis.
This study was approved by the local Ethics Committee and was registered on the Brazilian platform of research under the number 02213812.4.0000.5275. All the enrolled subjects (volunteers and patients) provided written informed consent before joining the study. In the COS group, clinical data, including hormone concentrations [serum and follicular estrogen (E2), progesterone (P4), LH, and FSH] and indicators of ovarian response (number of follicles and oocytes retrieved), were obtained from patient medical records. Clinical data for the control group were obtained during patient enrollment and interviews. All patients underwent blood collection for further VDR polymorphism genotyping.
Controlled ovarian stimulation protocols were performed according to the specific clinical requirements of the patients. Briefly, the gonadotropin-releasing hormone antagonist analog cetrorelix acetate (Cetrotide® 0.25 mg, Merck-Serono, Italy) was administered to induce hypophysis suppression, and on the second day of menstruation, ovarian stimulation was initiated with synthetic FSH alone (Gonal-F®, Merck-Serono, Italy; or Bravelle®, Ferring Pharmaceutical, Germany) or FSH and LH (Pergoveris®, Merck-Serono, Italy; or Menopur®, Ferring Pharmaceutical, Germany) treatments. FSH dosage varied from 150 to 300 IU/day, and LH dosage ranged from 75 to 300 IU/day.
When at least one follicle had reached 18 mm or at least two follicles had reached 16 mm (assessed by ultrasound), human chorionic gonadotropin (hCG) (Ovidrel® 250 μg, Merck-Serono, Italy) was administered to mimic LH. Thirty-five hours post-Ovidrel® administration, the oocytes were retrieved, and FF was obtained during the follicular aspiration procedure. In addition, blood samples were collected for VDR genotyping following FF isolation.
Blood (1 ml) was submitted for genomic DNA extraction from peripheral leukocytes via the salting-out technique (47) using a commercial Wizard® Genomic DNA purification kit according to the manufacturer’s instructions (A1120, Promega, Madison, WI, USA). After the extraction, DNA quantity and quality were examined using a NanoPhotometer (Implen, Munchen, Germany).
The genotyping of TaqI (rs731236) and FokI (rs2228570) polymorphisms was performed using the restriction fragment length polymorphism (RFLP) technique. Table 1 shows the primer sequences used for the VDR polymorphism analysis, which were validated through the Primer Blast program to ensure PCR quality; intron-spanning primers were used to avoid contamination with external genomic DNA. To perform the PCR reactions, a commercial kit (GoTaq, Promega, USA) was used and the conditions were as follows: 95°C for 4 min, 35 cycles of 95°C for 30 s, 60°C for 30 s, 72°C for 1 min, and 72°C for 7 min. DNA samples were digested by TaqI and BseGI (Btscl isoschizomers that recognize the same sequence recognized by the FokI) endonucleases (Thermo Scientific, EUA). The mixtures were incubated at 65°C and 55°C, respectively, to promote cleavage. The samples were then subjected to electrophoresis on 2–4% agarose gels to determine the lengths of the fragments and genotyping results (Figures S1 and S2 in Supplementary Material).

Table 1. Sequences of primers used to amplify each polymorphism and their respective fragments with or without endonucleases.
BsmI (rs1544410) polymorphism genotyping was performed using TaqMan Genotyping Master Mix (Applied Biosystems, Foster City, CA, USA, 4371355) and a TaqMan® SNP Genotyping Assay (Applied Biosystems, PN4351379) in a ViiA™ 7 Real-Time PCR System (Applied Biosystems, Foster City, CA, USA). Allele discrimination was analyzed using the ViiA™ 7 software, and genotyping was performed with Genotyping version 3.1 from Thermo Fisher Cloud. Furthermore, Sanger sequencing (Big Dye® Terminator v 3.1 Cycle Sequencing Kit) was performed on the four amplified products for which real-time PCR did not achieve accurate results to confirm the genotyping assay results (Figure S3 in Supplementary Material). The same primers used for amplification were used for genotyping assessment (5′CAACCAAGACTACAAGTACCGCGTCAGTG3′ and 3′AACCAGCGGGAAGAGGTCAAGGG5′) with 1 cycle at 96°C for 1 min, 25 cycles at 96°C for 15 s, 50°C for 15 s, and 60°C for 4 min. Products of the sequencing reactions were assessed in a Genetic Analyzer ABI3500. Sequence analysis was performed using MacVector, version 14.
Follicular fluid collection was performed during oocyte capture, as previously described (45, 49). Briefly, follicle aspiration was undertaken with a transvaginal ultrasound probe as a guide (Medison X8®) and a 17G oocyte aspiration needle (Wallace®) connected to a closed vacuum system under 90 mmHg of negative pressure, which was used to empty the follicles. The follicle exhibiting the largest diameter, greater than 16 mm, was selected, captured and placed in a sterile container. FF was extracted after oocyte detection and subsequently frozen in liquid nitrogen. This technique allowed the collection of fluid from a single follicle and decreased the chance of blood contamination.
FF 25(OH)D concentrations were assessed using an electrochemiluminescence fixation assay (ElecsysTotal Vitamin D total assay, Roche Diagnostics, Brazil). The range of measurements was 3–70 ng/ml. Inter- and intra-assay variations were 5.9 and 5.2%, respectively. This technique is based on competition, and a vitamin D-binding protein binds 25-hydroxycholecalciferol (25(OH)D3) and 25-hyroxyergocalciferol (25(OH)D2).
Genotype and allele frequencies were calculated based on the observed genotypes. Departure from Hardy–Weinberg equilibrium (HWE) in the distribution of the genotypes was estimated with the χ2 test. If the χ2 test resulted in a p value greater than 0.05, the population was considered to be in HWE. The influence of each VDR polymorphism on COS variation was assessed by an odds ratio (OR) analysis. We performed χ2 tests to analyze heterogeneity, and a value of p < 0.05 was considered to indicate statistical significance. The dominant model, in which heterozygous and homozygous minor alleles were grouped, was analyzed.
The Mann–Whitney test was used to investigate possible associations between polymorphisms and ovarian response variables and to test associations between polymorphisms and FF concentrations of 25(OH)D. A p value <0.05 was considered statistically significant. All comparisons were performed using SPSS (version 22) software. Graphics were generated using Prism (version 6) software.
To determine whether the presence of polymorphisms in the VDR gene affected the ovarian response of women undergoing COS, we extracted clinical data from control volunteers who had declared a history of natural conception and from women who underwent the COS protocol and ICSI treatment. The demographic parameters of the control and COS groups are depicted in Table 2.
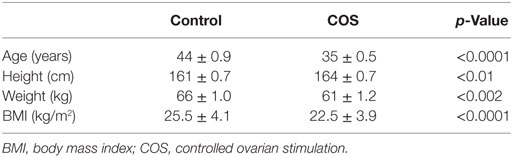
Table 2. Demographic parameters of control and COS groups.
The COS infertility diagnoses in our group were as follows: unexplained (37%), tubal factors (18%), ovarian failure (13%), endometriosis (13%), female anatomical causes (6%), and other causes of infertility (13%), including hypogonadism, colonic surgery, ovarian failure and tubal factors, female endocrine factors, breast cancer, tubal factors and endometriosis, or polycystic ovarian syndrome and endometriosis.
Table 3 shows the genotype frequencies of the VDR polymorphisms studied in the control versus COS groups. No differences were found, and the FokI polymorphism was in HWE (control: p = 0.6, COS: p = 0.23). Table 4 shows the allele frequencies of the VDR polymorphisms studied in the control versus COS groups. No differences were observed in the BsmI and FokI allele frequencies between the control and COS groups. However, the TaqI polymorphism exhibited a higher frequency of the C allele and a lower frequency of the T allele in the COS group [p = 0.02; OR: 1.95 (1.097–3.5)]. We then applied the dominant model and identified a considerable trend in the genotype distribution for the TaqI polymorphism [p = 0.056, OR: 2.106 (0.979–4.53)].
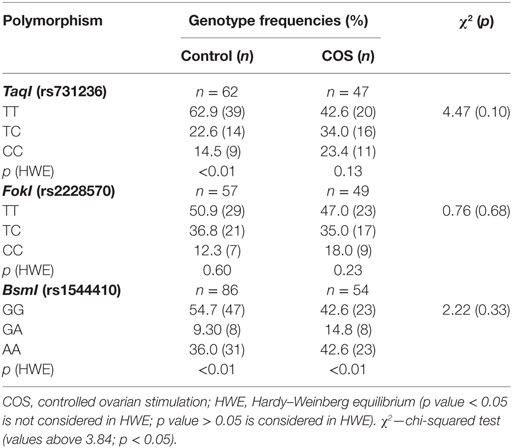
Table 3. Genotype frequencies of VDR polymorphisms.
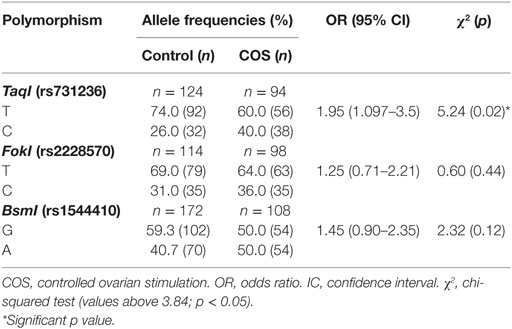
Table 4. Allele frequencies of VDR polymorphisms.
Because an association was detected between infertility and the frequency of TaqI alleles, we next examined whether the TaqI polymorphism is associated with variables related to the COS protocol. We, therefore, sorted the COS group according to genotype based on the dominant model (Table 5). A comparison of the TaqI genotypes did not reveal any differences in LH, FSH, E2, or P4 concentrations on day 1 of the COS protocol. However, there was a trend for women possessing the TC/CC genotypes to have a lower number of antral follicles than were found in women with the TT genotype (p = 0.08). The duration of COS and the FSH dose administered did not differ according to the TaqI genotype (Table 5). Similarly, a comparison of TaqI genotypes at baseline (Table 6) before COS revealed that there were no differences in 25(OH)D, E2, and P4 concentrations on the day of oocyte retrieval.
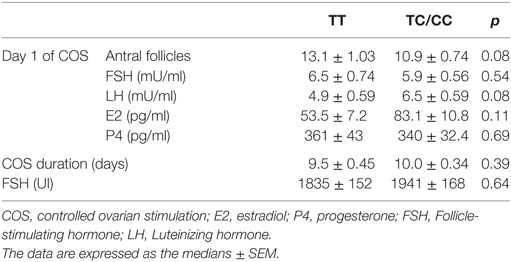
Table 5. Ovarian stimulation-related variables according to TaqI genotype.
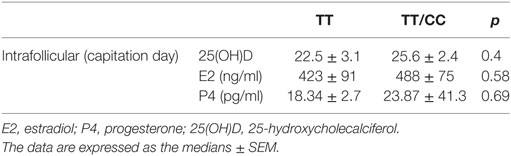
Table 6. Intrafollicular 25(OH)D, E2 and P4 concentrations according to TaqI genotype.
We further analyzed the number of follicles and retrieved oocytes according to the TaqI genotypes (Figure 1). A lower number of mature follicles was found in women with the TC/CC genotypes than in women possessing the TT genotype (p = 0.03). However, we found no significant differences in the number of oocytes retrieved. We also analyzed the serum concentrations of E2 and P4 on the day of hCG administration as well as the ratio of intrafollicular E2 to follicles retrieved according to TaqI genotype (Figure 2). There were no significant associations between TaqI genotypes and serum concentrations of E2 or P4 on the day of hCG administration (Figure 2). However, the ratio of intrafollicular E2 to retrieved follicles was higher in women with TC/CC genotypes than in women with the TT genotype (p < 0.02) (Figure 2). Our analysis of comorbidities between the two groups (TT and TC/CC genotypes) revealed no differences. There were no smokers in either group. Hypertension and diabetes were not found in any of these patients. The only comorbidity found was thyroid dysfunction. In all, 10% of the women with the TT genotype and 14% of the women with the TT/CC genotypes had thyroid dysfunction.
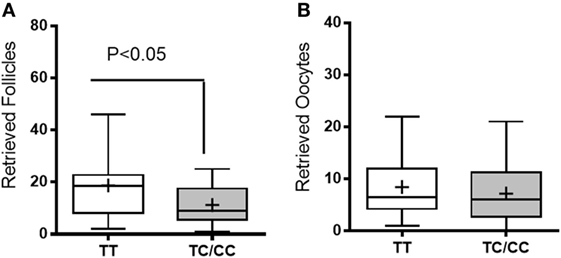
Figure 1. Follicles (A) and retrieved oocytes (B). White bars represent women carrying the TT genotype, whereas gray bars represent women carrying the TC/CC genotypes. Unpaired t-test. The data are presented as the mean ± min and max.
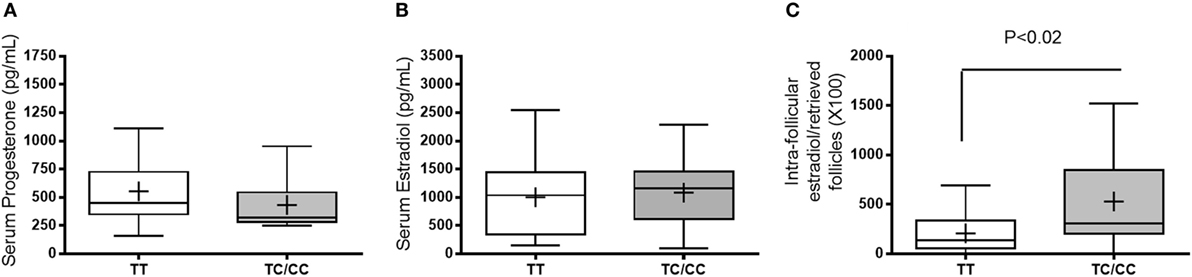
Figure 2. Serum concentrations of progesterone (A) and estradiol (B) on the day of human chorionic gonadotropin administration and the ratio of serum estradiol/to retrieved follicles (C). White bars represent women carrying the TT genotype, whereas the gray bars represent women carrying the TC/CC genotypes. Unpaired t-test. The data are presented as the mean ± min and max.
This work provides the first demonstration of an association between the VDR TaqI polymorphic C allele frequency and decreased follicle production by women exhibiting different causes of infertility. There were no significant differences in the genotype and allele frequencies of the FokI and BsmI polymorphisms between the COS and control groups. Instead, the higher frequencies observed in the group with polymorphic TaqI alleles in the COS group indicates that this VDR polymorphism is a potentially important SNP candidate that may be involved in female fertility.
There is some disagreement in the literature regarding the relationship between VDR polymorphisms and infertility disorders. Several studies have found that there is a negative association between the presence of TaqI, FokI, and BsmI VDR polymorphisms and the risk of developing reproductive disorders, such as polycystic ovarian syndrome and endometriosis (31–35). Conversely, other studies have found positive associations (36–38, 50) or no association at all (17) for these variables, suggesting that there is a need for further studies to clarify this important question.
We did not find an association between follicular 25(OH)D concentrations and any specific TaqI polymorphism allele (C or T), suggesting that these polymorphisms do not alter FF 25(OH)D concentrations. Importantly, while serum concentration of 25(OH)D were not evaluated in this study, recent findings reported by our (49) and other groups (13, 14, 43, 44, 51) have demonstrated that FF accurately reflects plasma 25(OH)D concentrations (14, 44) in both fertile and infertile patients.
The above results indicate a lack of a direct relationship between FF concentrations of 25(OH)D and infertility and suggest that the TaqI polymorphism does have a role in this context. In contrast, some studies have demonstrated an association between the TaqI C allele and decreased serum 25(OH)D concentrations in women with colorectal cancer (52), whereas another study performed in a healthy cohort in India (53) demonstrated that the TaqI C allele was directly associated with higher serum concentrations of 25(OH)D.
However, a study of polycystic ovarian syndrome in Caucasian women (32) found no association between TaqI polymorphic genotypes (TT, TC, CC) and 25(OH)D deficiency. This finding is in line with our results, given that we did not found any associations between TaqI polymorphism genotypes and intrafollicular 25(OH)D concentrations. Altogether, these data highlight the relevance of the TaqI polymorphism under different conditions and suggest the need for further studies investigating the relationship between VDR polymorphisms and 25(OH)D serum concentrations in different pathologies, including infertility disorders.
Our study has some limitations, including the relatively low number of included patients and the fact that we did not genotype all three VDR polymorphisms in all samples we evaluated. We also observed that there was a lack of HWE in the control population due to the exclusion criteria. This decreased the size of the study population and may have contributed to the observed imbalance in genotype and allele frequencies, resulting in a lack of HWE in the study populations. However, the COS population was under HWE and exhibited an association between the TaqI TC/CC polymorphic genotypes and the production of fewer ovarian follicles. These results suggest a possible role of the C allele in determining the number of pre-ovulatory follicles.
The above observation is supported by our data showing a higher ratio of retrieved follicles to intrafollicular E2 in women with TC/CC genotypes than in women carrying the TT genotype, i.e., women who have the TC/TT genotypes exhibited lower E2 availability in pre-ovulatory follicles. This finding demonstrates an important impact of the TaqI polymorphism on follicular development and hormone secretory function.
Recent studies have shown that 25(OH)D is present in FF (15, 19). While there is some controversy regarding the importance of FF 25(OH)D concentrations in positive IVF outcomes [for example, in patients with chemical pregnancies, embryonic implantation problems, chemical pregnancy (β-hCG level higher than 25 mIU/ml), in fertilization rates and in the numbers of embryos transferred and oocytes retrieved] (13, 14, 44), VDR mRNA and 1-α hydroxylase enzyme are expressed in the ovary (i.e., in ovarian cells and granulosa cell cultures) (12, 38), indicating that calcitriol activity affects local synthesis and autocrine and/or paracrine actions in the ovaries.
In conclusion, this study revealed an association between the presence of the C VDR TaqI polymorphism allele and infertility. This association is likely mediated by impaired calcitriol signaling, which may impact the number of follicles in women undergoing COS via mechanisms that are yet to be described.
This study was approved by the local Ethics Committee of the Maternidade Escola of the Federal University of Rio de Janeiro, which was registered on the Brazilian platform of research under the number 02213812.4.0000.5275. All of the enrolled subjects (volunteers and patients) provided written informed consent before joining the study.
Conceptualization of the experiments. Formal analysis. Performed experiments. Writing review and editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling Editor and reviewer PP declared their involvement as co-editors in the Research Topic, and confirm the absence of any other collaboration.
We thank FAPERJ, Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro Rio de Janeiro Research Foundation; the CNPq, Brazilian Council for Scientific and Technological Development, CAPES, Coordination for the Improvement of Higher Education Personnel and Fertipraxis Center for Human Reproduction.
This work was supported by FAPERJ, Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro, Rio de Janeiro Research Foundation (E-26/112.063/2012 and E-26/203.190/2015); the CNPq, Brazilian Council for Scientific and Technological Development (303734/2012-4, 473828/2012-0, and 402343/2012-3); and CAPES, Coordination for the Improvement of Higher Education Personnel.
The Supplementary Material for this article can be found online at https://www.frontiersin.org/articles/10.3389/fendo.2018.00252/full#supplementary-material.
Figure S1. Agarose gel electrophoresis of DNA against a 100 bp DNA ladder (Promega) following PCR amplification and restriction fragment length polymorphism with the TaqI restriction enzyme. (A) Lane 1, uncut band with a length of 495 bp. Lanes 2, 3, 5, and 6 contain uncut 495 bp fragments, indicating that these samples have the TT (homozygous) genotype. Lane 4 contains two bands at 290 and 205 bp, indicating the CC (homozygous) genotype. (B) Lanes 1, 3, 4, 5, and 6 contain 495, 290, and 205 bp fragments, indicating the TC (heterozygous) genotype. Lane 2 contains an uncut band with a length of 495 bp. Lane 7 contains two bands at 290 and 205 bp, indicating the CC (homozygous) genotype.
Figure S2. Agarose gel electrophoresis of DNA against a 100-bp DNA ladder (Promega) following PCR amplification and restriction fragment length polymorphism with the BseGI restriction enzyme. (A) Lane 1 contains an uncut band at 265 bp. Lane 2 contains fragments at 265 bp, indicating the TT (homozygous) genotype. Lane 3 contains two bands at 196 and 69 bp, indicating the CC (homozygous) genotype. (B) Lane 1 contains an uncut band with a length of 265 bp. Lanes 2 and 3 contains fragments at 265 bp, indicating an uncut fragment and, therefore, the TT (homozygous) genotype.
Figure S3. DNA fragment sequences in affected and unaffected individuals. The BamH1 restriction site sequence is underlined, and the arrows indicate the polymorphic site. (A) DNA sequence electropherogram of the wild-type G/G genotype (arrow). (B) DNA sequence electropherogram of the homozygous A/A polymorphism (arrow). (C) DNA sequence electropherogram of the heterozygous G/A polymorphism (arrow).
BMI, body mass index; COS, controlled ovarian stimulation; FF, follicular fluid; E2, estrogen; P4, progesterone; FSH, follicle-stimulating hormone; GnRH, gonadotropin-releasing hormone; hCG, human chorionic gonadotropin; 1,25(OH)2D, 1,25-Hydroxycholecalciferol; 25(OH)D, 25-Hydroxyvitamin D; 25(OH)D3, 25-Hydroxycholecalciferol; 25(OH)D2, 25-Hydroxyergocalciferol; HWE, Hardy–Weinberg equilibrium; IVF, in vitro fertilization; ICSI, intracytoplasmic sperm injection; LH, luteinizing hormone; OR, odds ratio; RFLP, restriction fragment length polymorphism; SNP(s), single-nucleotide polymorphism (s); VDR, vitamin D receptor.
1. Kamen DL, Tangpricha V. Vitamin D and molecular actions on the immune system: modulation of innate and autoimmunity. J Mol Med (Berl) (2010) 88:441–50. doi:10.1007/s00109-010-0590-9
2. Pludowski P, Holick MF, Pilz S, Wagner CL, Hollis BW, Grant WB, et al. Vitamin D effects on musculoskeletal health, immunity, autoimmunity, cardiovascular disease, cancer, fertility, pregnancy, dementia and mortality – a review of recent evidence. Autoimmun Rev (2013) 12(10):976–89. doi:10.1016/j.autrev.2013.02.004
3. DeLuca HF. Overview of general physiologic features and functions of vitamin D. Am J Clin Nutr (2004) 80(6 Suppl):1689S–96S. doi:10.1093/ajcn/80.6.1689S
4. Lerchbaum E, Obermayer-Pietsch B. Vitamin D and fertility: a systematic review. Eur J Endocrinol (2012) 166(5):765–78. doi:10.1530/EJE-11-0984
5. Halloran BP, DeLuca HF. Effect of vitamin D deficiency on fertility and reproductive capacity in the female rat. J Nutr (1980) 110(8):1573–80. doi:10.1093/jn/110.8.1573
6. Yoshizawa T, Handa Y, Uematsu Y, Takeda S, Sekine K, Yoshihara Y, et al. Mice lacking the vitamin D receptor exhibit impaired bone formation, uterine hypoplasia and growth retardation after weaning. Nature (1997) 16(4):391–6. doi:10.1038/ng0897-391
7. Johnson LE, DeLuca HF. Vitamin D receptor null mutant mice fed high levels of calcium are fertile. J Nutr (2001) 131(6):1787–91. doi:10.1093/jn/131.6.1787
8. Kinuta K, Tanaka H, Moriwake T, Aya K, Kato S, Seino Y. Vitamin D is an important factor in estrogen biosynthesis of both female and male gonads. Endocrinology (2000) 141(4):1317–24. doi:10.1210/endo.141.4.7403
9. Yildizhan R, Kurdoglu M, Adali E, Kolusari A, Yildizhan B, Sahin HG, et al. Serum 25-hydroxyvitamin D concentrations in obese and non-obese women with polycystic ovary syndrome. Arch Gynecol Obstet (2009) 280(4):559–63. doi:10.1007/s00404-009-0958-7
10. Somigliana E, Panina-Bordignon P, Murone S, Di Lucia P, Vercellini P, Vigano P. Vitamin D reserve is higher in women with endometriosis. Hum Reprod (2007) 22(8):2273–8. doi:10.1093/humrep/dem142
11. Hahn S, Haselhorst U, Tan S, Quadbeck B, Schmidt M, Roesler S, et al. Low serum 25-hydroxyvitamin D concentrations are associated with insulin resistance and obesity in women with polycystic ovary syndrome. Exp Clin Endocrinol Diabetes (2006) 114(10):577–83. doi:10.1055/s-2006-932856
12. Agic A, Xu H, Altgassen C, Noack F, Wolfler MM, Diedrich K, et al. Relative expression of 1,25-dihydroxyvitamin D3 receptor, vitamin D 1 alpha-hydroxylase, vitamin D 24-hydroxylase, and vitamin D 25-hydroxylase in endometriosis and gynecologic cancers. Reprod Sci (2007) 14(5):486–97. doi:10.1177/1933719107304565
13. Ozkan S, Jindal S, Greenseid K, Shu J, Zeitlian G, Hickmon C, et al. Replete vitamin D stores predict reproductive success following in vitro fertilization. Fertil Steril (2010) 94:1314–9. doi:10.1016/j.fertnstert.2009.05.019
14. Aleyasin A, Hosseini MA, Mahdavi A, Safdarian L, Fallahi P, Mohajeri MR, et al. Predictive value of the level of vitamin D in follicular fluid on the outcome of assisted reproductive technology. Eur J Obstet Gynecol Reprod Biol (2011) 159:132–7. doi:10.1016/j.ejogrb.2011.07.006
15. Nandi A, Sinha N, Ong E, Sonmez H, Poretsky L. Is there a role for vitamin D in human reproduction? Horm Mol Biol Clin Investig (2016) 25(1):15–28. doi:10.1515/hmbci-2015-0051
16. Refaat B, Ahmad J, Idris S, Kamfar FF, Ashshi AM, Batwa SA, et al. Characterisation of vitamin D-related molecules and calcium-sensing receptor in human fallopian tube during the menstrual cycle and in ectopic pregnancy. Cell Tissue Res (2017) 368(1):201–13. doi:10.1007/s00441-016-2519-2
17. Vilarino FL, Bianco B, Lerner TG, Teles JS, Mafra FA, Christofolini DM, et al. Analysis of vitamin D receptor gene polymorphisms in women with and without endometriosis. Hum Immunol (2011) 72(4):359–63. doi:10.1016/j.humimm.2011.01.006
18. Jurutka PW, Remus LS, Whitfield GK, Thompson PD, Hsieh JC, Zitzer H, et al. The polymorphic N terminus in human vitamin D receptor isoforms influences transcriptional activity by modulating interaction with transcription factor IIB. Mol Endocrinol (2000) 14(3):401–20. doi:10.1210/mend.14.3.0435
19. Uitterlinden AG, Fang Y, Van Meurs JBJ, Pols HAP, Van Leeuwen JPTM. Genetics and biology of vitamin D receptor polymorphisms. Gene (2004) 338(2):143–56. doi:10.1016/j.gene.2004.05.014
20. Jia J, Ding H, Yang K, Mao L, Zhao H, Zhan Y, et al. Vitamin D receptor genetic polymorphism is significantly associated with risk of type 2 diabetes mellitus in Chinese Han population. Arch Med Res (2015) 46(7):572–9. doi:10.1016/j.arcmed.2015.09.006
21. Lee YH, Song GG. Vitamin D receptor gene FokI, TaqI, BsmI, and ApaI polymorphisms and susceptibility to pulmonary tuberculosis: a meta-analysis. Genet Mol Res (2015) 14(3):9118–29. doi:10.4238/2015.August.7.21
22. Verbeek W, Gombart AF, Shiohara M, Campbell M, Koeffler HP. Vitamin D receptor: no evidence for allele-specific mRNA stability in cells which are heterozygous for the Taq I restriction enzyme polymorphism. Biochem Biophys Res Commun (1997) 238(1):77–80. doi:10.1006/bbrc.1997.7239
23. Köstner K, Denzer N, Müller CS, Klein R, Tilgen W, Reichrath J. The relevance of vitamin D receptor (VDR) gene polymorphisms for cancer: a review of the literature. Anticancer Res (2009) 29(9):3511–36.
24. Bermúdez-Morales VH, Fierros G, Lopez RL, Martínez-Nava G, Flores-Aldana M, Flores-Rivera J, et al. Vitamin D receptor gene polymorphisms are associated with multiple sclerosis in Mexican adults. J Neuroimmunol (2017) 306:20–4. doi:10.1016/j.jneuroim.2017.01.009
25. Amadori D, Serra P, Masalu N, Pangan A, Scarpi E, Maria Bugingo A, et al. Vitamin D receptor polymorphisms or serum levels as key drivers of breast cancer development? The question of the vitamin D pathway. Oncotarget (2017) 8(8):13142–56. doi:10.18632/oncotarget.14482
26. Mitra S, Desai M, Ikram Khatkhatay M. Vitamin D receptor gene polymorphisms and bone mineral density in postmenopausal Indian women. Maturitas (2006) 55(1):27–35. doi:10.1016/j.maturitas.2006.01.003
27. Despotovic M, Stoimenov TJ, Stankovic I, Basic J, Pavlovic D. Vitamin D receptor gene polymorphisms in Serbian patients with bronchial asthma: a case-control study. J Cell Biochem (2017) 118(11):3986–92. doi:10.1002/jcb.26054
28. Dabirnia R, Mahmazi S, Taromchi A, Nikzad M, Saburi E. The relationship between vitamin D receptor (VDR) polymorphism and the occurrence of osteoporosis in menopausal Iranian women. Clin Cases Miner Bone Metab (2016) 3:190–4. doi:10.11138/ccmbm/2016.13.3.190
29. Budhathoki S, Yamaji T, Iwasaki M, Sawada N, Shimazu T, Sasazuki S, et al. Vitamin D receptor gene polymorphism and the risk of colorectal cancer: a nested case-control study. PLoS One (2016) 11(10):e0164648. doi:10.1371/journal.pone.0164648
30. Hasan HA, AbuOdeh RO, Muda WAMBW, Mohamed HJBJ, Samsudin AR. Association of Vitamin D receptor gene polymorphisms with metabolic syndrome and its components among adult Arabs from the United Arab Emirates. Diabetes Metab Syndr (2017) 11(Suppl 2):S531–7. doi:10.1016/j.dsx.2017.03.047
31. Dasgupta S, Dutta J, Annamaneni S, Kudugunti N, Battini MR. Association of vitamin D receptor gene polymorphisms with polycystic ovary syndrome among Indian women. Indian J Med Res (2015) 142:276–85. doi:10.4103/0971-5916.166587
32. Jedrzejuk D, Łaczmański Ł, Milewicz A, Kuliczkowska-Płaksej J, Lenarcik-Kabza A, Hirnle L, et al. Classic PCOS phenotype is not associated with deficiency of endogenous vitamin D and VDR gene polymorphisms rs731236 (TaqI), rs7975232 (ApaI), rs1544410 (BsmI), rs10735810 (FokI): a case-control study of lower Silesian women. Gynecol Endocrinol (2015) 31(12):976–9. doi:10.3109/09513590.2015.1062865
33. Bagheri M, Abdi Rad I, Hosseini Jazani N, Nanbakhsh F. Vitamin D receptor taqi gene variant in exon 9 and polycystic ovary syndrome risk. Int J Fertil Steril (2013) 7(2):116–21.
34. Lin MW, Tsai SJ, Chou PY, Huang MF, Sun HS, Wu MH. Vitamin D receptor 1a promotor -1521 G/C and -1012 A/G polymorphisms in polycystic ovary syndrome. Taiwan J Obstet Gynecol (2012) 51(4):565–71. doi:10.1016/j.tjog.2012.09.011
35. Wehr E, Trummer O, Giuliani A, Gruber HJ, Pieber TR, Obermayer-Pietsch B. Vitamin D-associated polymorphisms are related to insulin resistance and vitamin D deficiency in polycystic ovary syndrome. Eur J Endocrinol (2011) 164(5):741–9. doi:10.1530/EJE-11-0134
36. Mahmoudi T, Majidzadeh AK, Farahani H, Mirakhorli M, Dabiri R, Nobakht H, et al. Association of vitamin D receptor gene variants with polycystic ovary syndrome: a case control study. Int J Reprod Biomed (Yazd) (2015) 13(12):793–800.
37. El-Shal AS, Shalaby SM, Aly NM, Rashad NM, Abdelaziz AM. Genetic variation in the vitamin D receptor gene and vitamin D serum levels in Egyptian women with polycystic ovary syndrome. Mol Biol Rep (2013) 40(11):6063–73. doi:10.1007/s11033-013-2716-y
38. Szczepańska M, Mostowska A, Wirstlein P, Skrzypczak J, Misztal M, Jagodziński PP. Polymorphic variants in vitamin D signaling pathway genes and the risk of endometriosis-associated infertility. Mol Med Rep (2015) 12(5):7109–15. doi:10.3892/mmr.2015.4309
39. Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr (2008) 87(4):1080S–6S. doi:10.1093/ajcn/87.4.1080S
40. Maeda SS, Borba VZC, Camargo MBR, Silva DMW, Borges JLC, Bandeira F, et al. Recommendations of the Brazilian Society of Endocrinology and Metabology (SBEM) for the diagnosis and treatment of hypovitaminosis D. Arq Bras Endocrinol Metabol (2014) 58(5):411–33. doi:10.1590/0004-2730000003388
41. Lopes VM, Lopes JRC, Brasileiro JPB, de Oliveira I, Lacerda RP, Andrade MRD, et al. Highly prevalence of vitamin D deficiency among Brazilian women of reproductive age. Arch Endocrinol Metab (2016) 61(1):21–7. doi:10.1590/2359-3997000000216
42. Rudick B, Ingles S, Chung K, Stanczyk F, Paulson R, Bendikson K. Characterizing the influence of vitamin D levels on IVF outcomes. Hum Reprod (2012) 27:3321–7. doi:10.1093/humrep/des280
43. Firouzabadi RD, Rahmani E, Rahsepar M, Firouzabadi MM. Value of follicular fluid vitamin D in predicting the pregnancy rate in an IVF program. Arch Gynecol Obstet (2014) 289(1):201–6. doi:10.1007/s00404-013-2959-9
44. Anifandis GM, Dafopoulos K, Messini CI, Chalvatzas N, Liakos N, Pournaras S, et al. Prognostic value of follicular fluid 25-OH vitamin D and glucose levels in the IVF outcome. Reprod Biol Endocrinol (2010) 8:91. doi:10.1186/1477-7827-8-91
45. Antunes RA, Mancebo ACA, Reginatto MW, Deriquehem VAS, Areas P, Bloise E, et al. Lower concentration of follicular fluid vitamin D correlate with a higher number of large ovarian follicles. Reprod Biomed Online (2017) 36(3):277–84. doi:10.1016/j.rbmo.2017.12.010
46. Luk J, Torrealday S, Neal Perry G, Pal L. Relevance of vitamin D in reproduction. Hum Reprod (2012) 27(10):3015–27. doi:10.1093/humrep/des248
47. Miller SA, Dykes DD, Polesky HF. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res (1988) 16:1215. doi:10.1093/nar/16.3.1215
48. Panierakis C, Goulielmos G, Mamoulakis D, Petraki E, Papavasiliou E, Galanakis E. Vitamin D receptor gene polymorphisms and susceptibility to type 1 diabetes in Crete, Greece. Clin Immunol (2009) 133(2):276–81. doi:10.1016/j.clim.2009.08.004
49. Deriquehem VA, Antunes RA, Reginatto MW, Mancebo AC, Areas P, Bloise E, et al. Body weight and 25-hidroxyvitamin D follicular levels: a prospective study of women submitted to in vitro fertilization. JBRA Assist Reprod (2016) 20(3):127–31. doi:10.5935/1518-0557.20160029
50. Siddamalla S, Reddy TV, Govatati S, Erram N, Deenadayal M, Shivaji S, et al. Vitamin D receptor gene polymorphisms and risk of polycystic ovary syndrome in South Indian women. Gynecol Endocrinol (2017) 34(2):161–165. doi:10.1080/09513590.2017.1371128
51. Potashnik G, Lunenfeld E, Levitas E, Itskovitz J, Albutiano S, Yankowitz N, et al. The relationship between endogenous oestradiol and vitamin D3 metabolites in serum and follicular fluid during ovarian stimulation for in-vitro fertilization and embryo transfer. Hum Reprod (1992) 7(10):1357–60. doi:10.1093/oxfordjournals.humrep.a137573
52. Atoum MF, Tchoporyan MN. Association between circulating vitamin D, the Taq1 vitamin D receptor gene polymorphism and colorectal cancer risk among Jordanians. Asian Pac J Cancer Prev (2014) 15(17):7337–41. doi:10.7314/APJCP.2014.15.17.7337
Keywords: calcitriol, VDR polymorphisms, 25(OH)D, TaqI, folliculogenesis, infertility
Citation: Reginatto MW, Pizarro BM, Antunes RA, Mancebo ACA, Hoffmann L, Fernandes P, Areas P, Chiamolera MI, Silva R, Souza MCB, Bloise E and Ortiga-Carvalho TM (2018) Vitamin D Receptor TaqI Polymorphism Is Associated With Reduced Follicle Number in Women Utilizing Assisted Reproductive Technologies. Front. Endocrinol. 9:252. doi: 10.3389/fendo.2018.00252
Received: 29 October 2017; Accepted: 02 May 2018;
Published: 28 May 2018
Edited by:
William B. Grant, Sunlight Nutrition and Health Research Center, United StatesReviewed by:
Barbara Joan Boucher, Queen Mary University of London, United KingdomCopyright: © 2018 Reginatto, Pizarro, Antunes, Mancebo, Hoffmann, Fernandes, Areas, Chiamolera, Silva, Souza, Bloise and Ortiga-Carvalho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tânia M. Ortiga-Carvalho, dGFuaWFvcnRAYmlvZi51ZnJqLmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.