 Veronika Valdová
Veronika Valdová Vladimíra Štěpánová2
Vladimíra Štěpánová2 Lenka Lapčíková
Lenka Lapčíková- 1Independent Consultant, Prague, Czechia
- 2NewWaterMeaning, s.r.o., Prague, Czechia
Introduction: Chronic wounds are a significant public health challenge, representing a considerable burden on the healthcare system. There are numerous gaps in knowledge in the treatment of chronic wounds. First, it is difficult to follow patients through different types of care. Wounds in polymorbid, elderly patients often remain unhealed due to the patient succumbing to their primary disease. No reliable data exist regarding the time to wound closure, type of interventions, the use of antibiotics, the nature and rate of complications, or the causes of treatment failures.
Methods: This Post-Market Clinical Follow-Up (PMCF) study is a prospective, multicentric, observational, descriptive, qualitative survey among healthcare professionals that involves 237 patients with acute and chronic wounds treated with superoxide-based wound irrigation solution DebriEcaSan Alfa in real-world settings over 12 weeks, both outpatient and inpatient. The study aimed to collect additional clinical data to confirm the safety, performance, and clinical benefit of DebriEcaSan Alfa.
Results: The Manufacturer collected 237 survey forms from 81 healthcare facilities, nursing homes, and outpatient clinics in the Czech Republic. The most common diagnoses were venous leg ulcer, pressure ulcer, diabetic foot ulcer, and traumatic wound. The most common comorbidities and risk factors were obesity, diabetes mellitus, and peripheral artery disease. Significant improvement was observed in all parameters, including pain, malodor, affected tissues, reduction in wound size, and granulation and epithelization. A marked reduction in size was observed in all wound size categories. 19 (8%) patients healed by end of week 6; and 66 (28%) healed by week 9. 130 (55%) patients were considered healed by week 12.
Discussion: The current clinical practice guidelines refrain from recommending any of the available irrigation solutions and wound dressings due to low-quality evidence. Superoxidized solutions have excellent biocompatibility and are non-cytotoxic, non-sensitizing, not irritating, non-genotoxic, and have broad-spectrum antimicrobial properties. There is no objective baseline to compare the results to, as typical healing times in a comparable population are not accessible. No single standard of care exists in the treatment of chronic wounds, and significant variability in practices exists across the health system.
1 Introduction
Chronic wounds are a significant public health challenge, representing a considerable burden on healthcare systems. The estimated prevalence of chronic wounds is 2.21 per 1,000 population, the majority of which are chronic leg ulcers (Martinengo et al., 2019). The most common types of chronic wounds are diabetic foot ulcers, venous leg ulcers, and pressure ulcers. In diabetic patients, the annual risk of foot ulceration is around 2%, whereas the lifetime risk is 12%–25% (Nagoba et al., 2021). The prevalence of leg ulcers is estimated to range from 0.045% to 1.5% in the United Kingdom (Chaplin, 2020) and 0.08% in Germany (Rüttermann et al., 2013). The prevalence of pressure ulcers in inpatient settings approximates 22% (Dreifke et al., 2015). In Germany, a significant cost of inpatient medical care is spent on treating venous leg ulcers and diabetic foot ulcers (Rüttermann et al., 2013). In the Czech Republic, the incidence and prevalence of chronic wounds and leg ulcers, in particular, follow the trends in other developed countries. The prevalence of patients with diabetes increased from 78 per 1,000 people in 2007 to 88 per 1,000 people in 2017 (UZIS, 2018). Around 4% of diabetics develop diabetic foot syndrome, of which 24% result in amputation (Jirkovská, 2018). Despite the significant impact on the health system and patients’ quality of life, treating chronic wounds remains an under-researched area.
Clinical management of chronic wounds relies on aggressive debridement and exudate and moisture management to facilitate granulation and epithelization to achieve wound closure. There is a consensus that effective debridement, reducing bioburden, and infection control are the cornerstones of the treatment of chronic wounds (Eriksson et al., 2022). Additional interventions include the management of systemic diseases such as diabetes, compression in venous leg ulcers, restoration of arterial inflow in ischemic ulcers, and offloading in diabetic foot ulcers (Schultz et al., 2003). Evidence-based recommendations for patients with infected diabetic foot favor hydrogel and hyperbaric oxygenation (Rüttermann et al., 2013) and advise against the use of medicinal honey, growth factors, silver preparations, bacteriophage therapy, or negative-pressure wound therapy, and antiseptics in general. However, this recommendation is conditional, and the certainty of the evidence is low (Lazzarini et al., 2023; Senneville et al., 2024). Venous leg ulcers are typically treated with compression bandages, debridement, and irrigation with normal saline, water, or antiseptics. Insufficient evidence from randomized clinical trials exists to recommend optimal approaches to cleansing venous leg ulcers (McLain et al., 2021).
A significant variability in wound care practices exists across the health system. A wide variety of products available on the market are empirically used in a variety of clinical contexts, a multitude of deployment methods, and countless combinations. Jones et al. (2007) studied the consistency of current chronic wound care practices in the U.S. and found significant variations in adherence across sites of care delivery (Jones et al., 2007). This lack of consistency makes it very difficult to compare data across facilities. No reliable data exists regarding the time to wound closure, the type of interventions and the sequence and duration of their use, the use of antibiotics, the nature and rate of complications, or the causes of treatment failures. Additionally, very few quality studies focus on the treatment of chronic wounds. Consequently, low-quality evidence results in low-confidence recommendations in clinical guidelines (Eriksson et al., 2022). This lack of evidence further exacerbates the existing problem with the variability of treatment approaches across health systems.
Inaccurate or sporadic reporting does not allow adequate use of data to monitor treatment outcomes. As documented by Pokorná et al. (2017) in her study on cutaneous ulcer diseases and their reporting in acute inpatient care in the Czech Republic, the typical healing times for specific types of ulcers are not easily obtainable from medical records, and no reliable benchmarks currently exist. Pokorná examined data from the National Register of Hospitalized Persons (NRHOSP) and Death Examination Reports from 2007 to 2015 as part of project DRG Restart. She stressed the issue of underreporting hospital-acquired ulcers, and the limited value of incomplete data obtained from the National Health Information System and reference hospitals, making it impossible to calculate the burden of hospitalizations involving chronic wounds. Consequently, it is difficult to consider the impact of ulcer diseases and the cost of treatment across the board (Pokorná et al., 2017).
Moreover, treatment outcomes such as quality of healing, complications, quality of life, burden on healthcare staff, and affordability are inconsistently used across studies and in quality-of-care metrics, making the results difficult to compare (Eriksson et al., 2022). Endpoints for chronic cutaneous ulcer studies are the time to healing, wound size reduction, infection control, the need for amputation, prevention of recurrence, improved functionality, and reduced isolation (Eaglstein et al., 2012). While time to wound closure and wound size reduction are the primary outcomes, a healed wound is not always the expected outcome. In palliative wound care, the desired outcomes include pain and malodor reduction, exudate management, and other quality-of-life measures (Eriksson et al., 2022).
Amputation is an important complication of infected chronic wounds and, especially, diabetic foot ulcers. High amputations are the consequence of late hospitalizations, deep defect or phlegmon, Charcot osteoarthropathy, insufficiently treated infection, severe ischemia of the lower limbs, poorly controlled diabetes, smoking, atherosclerosis, and renal insufficiency. The acceleration of atherosclerosis risk factors after amputation leads to the worsening of cardiovascular diseases, persistent neuropathy complications on the stump of the amputated limb, and premature death (Jirkovská, 2018). Jirkovská’s findings raise important points about the advanced condition often observed at the initial examination regarding wound characteristics, which, combined with patient comorbidities and risk factors, adversely impact treatment outcomes.
Numerous gaps in knowledge exist in treating chronic wounds. While consensus exists about the importance of wound cleansing and debridement (Dayya et al., 2022; Eriksson et al., 2022), no clear recommendations are available regarding the optimal choice and method of use of wound irrigation for diabetic foot (Senneville et al., 2024), infected leg ulcers (National Institute for Health and Care Excellence, 2020) or pressure ulcers (European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance, 2019).
The evidence regarding best wound irrigation practices is sparse, and no official recommendations currently exist from any healthcare organization (Saeg et al., 2021). Irrigation practices vary widely in terms of delivery method, volume, and type of solution. The majority of wound irrigation solutions are cytotoxic, and their efficacy to enhance healing is uncertain (Wilkins and Unverdorben, 2013). Comprehensive systematic reviews by Alonso-Coello et al. (2016b) did not identify any direct evidence to support the use of any specific wound irrigation solutions or wound cleansing techniques. An ideal irrigation solution should be isotonic, nonhemolytic, noncytotoxic, transparent, easy to sterilize, and inexpensive. The ideal antiseptic solution is still debated, although the current literature favors the use of normal saline for non-infected wounds (Gabriel, 2021). The European Pressure Ulcer Advisory Panel (EPUAP) guideline from 2019 recommends the use of antimicrobial solutions to clean pressure injuries with suspected or confirmed infection, such as polyhexamethylene biguanide (PHMB), octenidine dihydrochloride (OCT), superoxidized solution with hypochlorous acid (HOCL) and sodium hypochlorite (NaOCL), and povidone iodine, rather than normal saline, sterile water, or potable tap water. However, the recommendations are based only on expert opinions (European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance, 2019). Other guidelines suggest that topical antiseptics or antimicrobials shall not be routinely used to treat diabetic and pressure ulcers (National Institute for Health and Care Excellence, 2016). No specific advice on wound irrigation methods is given in the 2023 IWGDF Guidelines on the prevention and management of diabetes-related foot disease (Senneville et al., 2024).
The low confidence recommendations stem from the low quality of evidence from wound care studies. As Forster and Pagnamenta (2015) noted in their Cochrane review, designing randomized controlled trials (RCTs) in wound care is challenging due to the significant variability of patient demographics, wound characteristics, comorbidities, and risk factors as well as concurrent therapies and self-care. Therefore, recruiting enough participants with comparable characteristics represents a major challenge. Common limitations of RCTs in wound care include poor baseline characteristics, sample sizes too low to reliably detect differences between treatments, poor reporting of assessor blinding, randomization methods and allocation concealment, and inadequate follow-up. Important endpoints such as pain, malodor, frequency of dressing changes, patient satisfaction, study withdrawals, and adverse events are often not reported. Inappropriate comparators can limit the generalizability of the results to a real-world population. The overall quality of clinical evidence is suboptimal and insufficient to inform clinical practice (Forster and Pagnamenta, 2015).
The organization of healthcare that serves wound care patients produces additional challenges. Most clinical data available in scientific literature and national registries come from hospitalized patients rather than outpatient care. As stated by Pokorná et al. (2017), it is impossible to follow patients through their transition through different types of care, i.e., from the first occurrence of the wound and the first contact with a healthcare professional to outpatient treatment, hospitalization, discharge with or without home care assistance or transfer to a long-term care facility or a nursing home. Each of these care modalities has its own treatment protocols and methods of measuring treatment outcome. Since many chronic wounds develop in polymorbid, elderly patients as a complication of their underlying disease, wounds often remain unhealed due to the patient succumbing to their primary disease. The time to wound closure of complex, non-healing wounds cannot be currently obtained from data gathered within the existing quality management systems. The only obtainable data point is time to discharge, meaning the wound is manageable in an outpatient setting or with the assistance of a homecare nursing service. Similarly, no reliable data from the existing monitoring systems details the type of interventions, the use of antibiotics, the nature and rate of complications, or the causes of treatment failures (Pokorná et al., 2017).
Hence, the present study has been conducted to determine the efficacy and safety of superoxidized solution (DebriEcaSan Alfa) in the treatment of chronic wounds. This Post-Market clinical Follow-Up (PMCF) study is a prospective, multicentric, observational, descriptive, qualitative survey among healthcare professionals. The study involves 237 patients with acute and chronic wounds who were treated with superoxide-based wound irrigation solution DebriEcaSan Alfa (NewWaterMeaning s.r.o.) in real-world settings. The PMCF meets the requirements outlined in the EU Regulation 2017/745 on medical devices. A literature review was performed to update current knowledge about superoxide-based wound irrigation solutions, their antimicrobial and antibiofilm properties, and the state of the art in treating chronic wounds.
2 Materials and methods
2.1 Type of study
This is a post-market clinical follow-up (PMCF) study sponsored and performed by the Manufacturer of DebriEcaSan Alfa, NewWaterMeaning, s.r.o., Czech Republic. Since the product was used within its intended purpose, and the patients were not submitted to invasive or burdensome procedures additional to those performed under the normal conditions of use of the device, no approval of ethics committee was required (Jurrmann, 2023). The study is part of the Manufacturer’s Post-Market Surveillance Plan and it is conducted in compliance with European Medical Device Regulation (EU MDR) 2017/745 (European Commission, 2017).
2.2 Study design
This PMCF is a prospective, multicentric, observational, descriptive, qualitative survey among healthcare professionals that involves 237 patients treated with DebriEcaSan Alfa in real-world settings, both outpatient and inpatient.
2.3 Eligible subjects
Patients of all demographics with acute or chronic wounds of any origin and any duration who were treated with DebriEcaSan Alfa as part of their standard protocol in outpatient and inpatient facilities or nursing homes in the Czech Republic were considered.
2.4 Main outcomes
The study shall provide insight into the characteristics of treated population in terms of age, sex, comorbidities, and risk factors, and the initial wound characteristics in real world settings. The data shall establish baseline in terms of expected healing times and complication rates for different types of chronic wounds, especially wounds that are large, deep, and infected, and wounds in patients with multiple comorbid conditions. Important outcomes are the reduction of wound size, malodor, pain, patient’s comfort, and ease of use for healthcare personnel.
2.5 PMCF plan
The survey form enquires about the patient’s demographics, basic diagnosis, comorbidities and risk factors, characteristics of the wound at initial examination, and at weeks 3, 6, 9, and 12, methods of use of DebriEcaSan Alfa, treatment outcome, complications, commentary, consent and signature. Case studies are supported by imagery that documents the healing process (where patient consent to share images exists). Data was collected from healthcare professionals using a survey form. The current dataset concerns survey forms collected between January 2019 and December 2023. The study is still ongoing.
2.6 Assessment
The data collected from healthcare professionals through survey forms was compiled in an Excel spreadsheet and presented in a series of graphs and tables. Each component was evaluated in the context of existing evidence, including information held by the Manufacturer and data from scientific literature.
2.7 Review of literature
The Manufacturer regularly screens databases PubMed, Prospero, Cochrane Database of Systematic Reviews, NICE guidelines, and ClinicalTrials.gov for publications as part of its post-market surveillance activities to update its technical documentation, specifically Biological Compatibility Assessment, Clinical Evaluation, and Post-market Clinical Follow-Up for superoxidized solutions and gels. An overview of accumulated knowledge is provided along with an update for the monitoring period from 1 October 2021 to 30 September 2023.
2.8 Eligibility criteria
Articles focusing on the use superoxidized solutions in wound irrigation, their antimicrobial efficacy and cytotoxicity were sought. In vivo and in vitro studies were considered to evaluate the cytotoxicity and antimicrobial properties of superoxidized solutions. Clinical practice guidelines, systematic reviews and meta-analyses, and focused review articles were screened to establish the current standard of care and state-of-the-art in the treatment of chronic and non-healing wounds. Clinical studies comparing different irrigation and antiseptic solutions in the treatment of acute and chronic wounds were examined to review the safety and efficacy of superoxidized solutions in the context of other available products in different clinical scenarios. Articles published in selected scientific electronic databases from 1 October 2021 to 30 September 2023 were considered.
2.9 Exclusion criteria
Publications that did not discuss a relevant device and purpose of use, studies which did not focus on the use of superoxidized solutions in wound care, those published outside of the indicated period, and publications that do not contribute to the state of the art were excluded.
2.10 Search strategy
Electronic scientific databases PubMed, Prospero, Cochrane Database of Systematic Reviews, NICE guidelines, and ClinicalTrials.gov were electronically searched and subsequently hand searched to retrieve relevant sources. English was chosen as the search language. The search strategy was implemented via the following steps: an initial search was performed using the keywords: “superoxidized solution,” OR “neutral electrolyzed water,” OR “hypochlorous acid,” AND “chronic wound,” OR “diabetic foot ulcer” OR “venous leg ulcer” OR “pressure ulcer” in electronic databases. The results of the initial search were combined into a single set. Duplicities were removed and then the titles, abstracts and full texts of the obtained articles were independently assessed for final inclusion.
2.11 Data extraction
Data were independently extracted from studies included in the review. Extracted data included: relevant device, relevant purpose of use, study population, sample size, country, and outcomes relevant to the literature review objectives.
3 Results
3.1 Review of scientific literature
The search generated 381 references that are possibly relevant to the antimicrobial efficacy and cytotoxicity of superoxidized solutions and their use in wound care. Once titles and abstracts, where available, had been assessed, hard copies of 83 papers were examined, including publications obtained from lists of references. Two systematic reviews (Dumville et al., 2017; Peters et al., 2020) and eight studies were considered relevant for the review of antimicrobial topical treatment of diabetic foot ulcers. Twenty publications were used to extract information on antimicrobial properties of superoxidized solutions and eight to report on biological compatibility.
3.1.1 Superoxidized solutions in the treatment of chronic wounds
The International Working Group on the Diabetic Foot expert panel periodically conducts a systematic review of the published evidence relating to the interventions for managing infection in the diabetic foot (Peters et al., 2012; Peters et al., 2016; Peters et al., 2020). The latest update included 53 studies on the use of surgical procedures, topical antiseptics, negative pressure wound therapy, and hyperbaric oxygen. Of these, three studies discussed the use of superoxidized solutions. In two studies (Martínez-De Jesús, 2007; Piaggesi et al., 2010), using superoxidized water was associated with a better outcome than soap or povidone iodine; however, both studies had a high risk of bias. No benefit has been reported with any other intervention. One additional unblinded study was found comparing superoxidized solution alone and oral levofloxacin with either normal saline or superoxidized solution (Landsman et al., 2011). No significant differences in the rate of clinical success were found. The authors noted that weak trial designs, incomplete reporting, and possible sources of bias limit the generalizability of the evidence. Overall, there is currently no trial data to justify the adoption of any particular therapeutic approach in diabetic patients with infection of either soft tissue or bone of the foot. Dumville et al. (2017), in their Cochrane systematic review, reached a similar conclusion that the relative effects of antimicrobial topical treatments remain uncertain, and no recommendations can be made. Of the 22 randomized controlled trials included in the review, five studies compared superoxidized solutions with either povidone iodine (Piaggesi et al., 2010; Kapur and Marwaha, 2011), normal saline (Hadi et al., 2007; Bowling et al., 2011) or soap (Martínez-De Jesús, 2007). Very low certainty evidence pointed to a slight advantage of the use of antimicrobial topical treatments compared to non-antimicrobial ones (Dumville et al., 2017). Overall, insufficient trial data exist to justify the adoption of any particular therapeutic approach in diabetic foot. The evidence is limited by weak trial designs, incomplete reporting, and possible sources of bias. Additional two single-arm studies with Microdacyn for the treatment of pressure ulcers (Hans, 2022) and diabetic foot ulcers (Walia et al., 2021) were found. These two studies did not affect the overall quality of evidence as presented by Peters et al. (2020), Peters et al. (2016), Peters et al. (2020), and Dumville et al. (2017) (see Table 1).
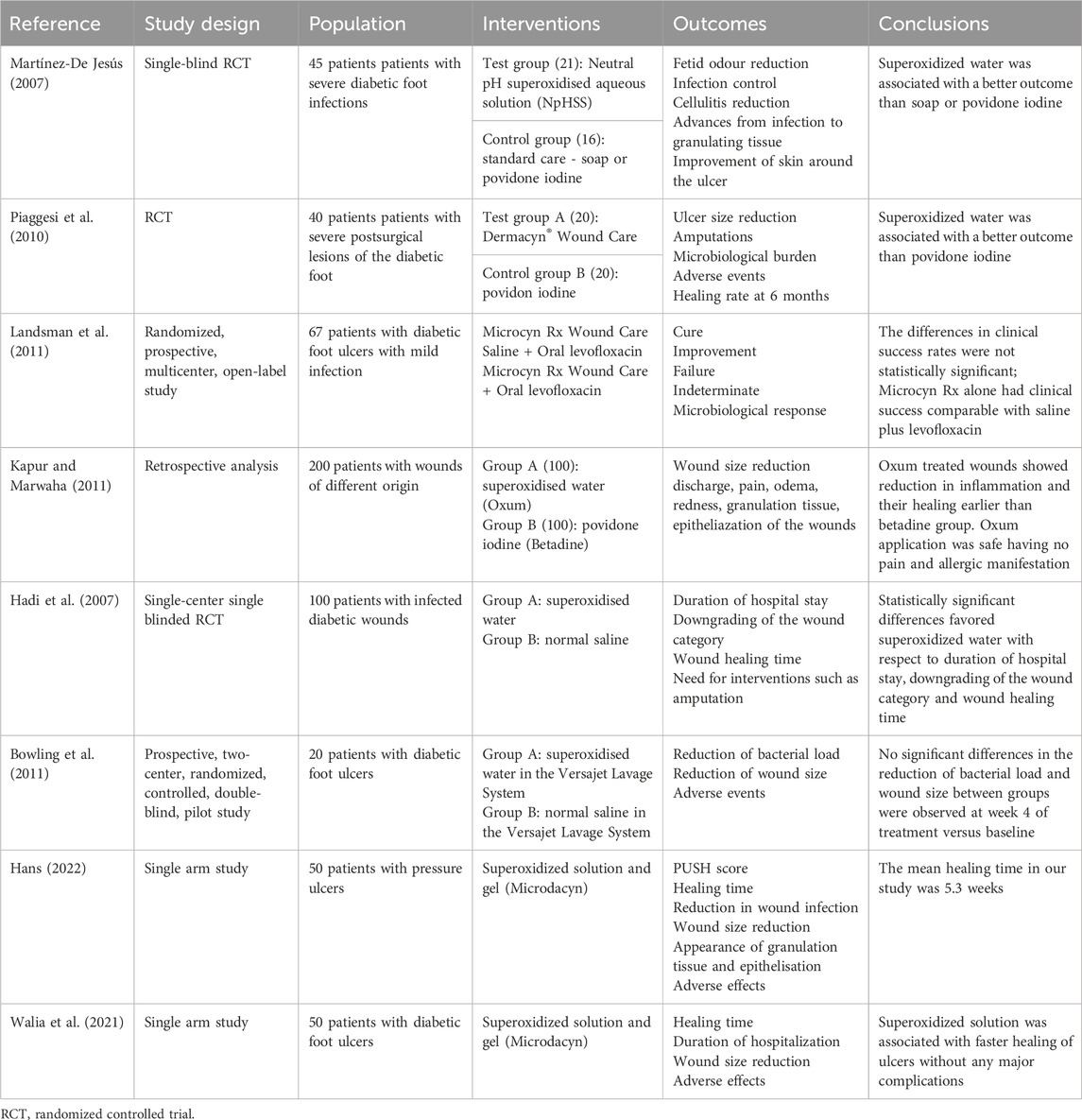
Table 1. Superoxidized solutions (SOS) in the treatment of chronic wounds.
3.1.2 Antimicrobial properties of superoxidized solutions
The mechanism of action of superoxidized solutions on bacteria is based on damage to cells by a high oxidation-reduction potential and their lysis by the action of osmotic pressure. Superoxidized solutions contain a mixture of inorganic oxidants such as hypochlorous acid (HClO), hypochlorous acidic ion (ClO-), chlorine (Cl2), hydroxide (OH), and ozone (O3). Neutral superoxidized solutions contain free oxygen radicals similar to those produced in mitochondria during ATP production and in secretory granules of leukocytes. Superoxidized solutions kill microorganisms directly through their oxidative capacity as they react with the cell wall and membrane and signal protease activation through pH-dependent NADPH oxidase. Exposure of bacteria to oxidative compounds with an ORP between +650 mV and 700 mV induces oxidative stress, resulting in bactericidal effect within a few seconds (Cloete et al., 2009; Armstrong, 2017).
Zinkevich et al. (2000) investigated the mechanism of action of antimicrobial properties of Sterilox, using E. coli and analyzing protein and nucleic acid damage. Within 5 min of exposure, the solution destroyed chromosomal and plasmid DNA, RNA, and surface proteins. No intact cells were seen after 5 min of exposure. Within 30 s of exposure, Sterilox entered the cell, causing structural and functional damage to the cell membrane and the cell wall, resulting in swelling. The eventual rupture of the cell wall occurs within 5 min of exposure, causing leakage of cytoplasm and the destruction of proteins, DNA, and RNA (Zinkevich et al., 2000).
HOCl increases oxygenation at wound sites and breaks down biofilm by nonspecifically targeting biomolecules on bacterial cell membranes. HOCL increases permeability of the bacterial cell membrane, damaging the cell integrity. HOCL attacks the microbe cell membrane by dissolving the protective membrane of the biofilm (Gold et al., 2020).
Physiologically, HOCl is produced in the respiratory burst of activated neutrophils. HOCl is a potent oxidant, capable of oxidizing thiol groups and thioethers and halogenating amine groups to form monochloramines and dichloramines. HOCl covalently modifies key amino acid residues of Matrix Metalloproteinase 7 (MMP-7) within the cell. Higher HOCl-to-protein ratios eventually inactivate MMP-7. HOCl exerts a rapid and selective inhibition on RNA and DNA synthesis. It may disrupt membrane/DNA interactions needed for replication, alter the DNA template itself, inactivate enzymes of the replication system, or even inhibit the synthesis of critical proteins required for DNA replication and cell division. HOCl targets methionine residues in proteins of phagocytosed bacteria. The formation of oxidized methionine is strongly associated with bacterial killing (Armstrong et al., 2015).
Superoxidized solutions are effective against a number of aerobic and facultatively aerobic bacteria, anaerobic bacteria, viruses, bacterial spores, bacteriophages and Eukaryotes. They also show good efficacy against biofilms (see Table 2).
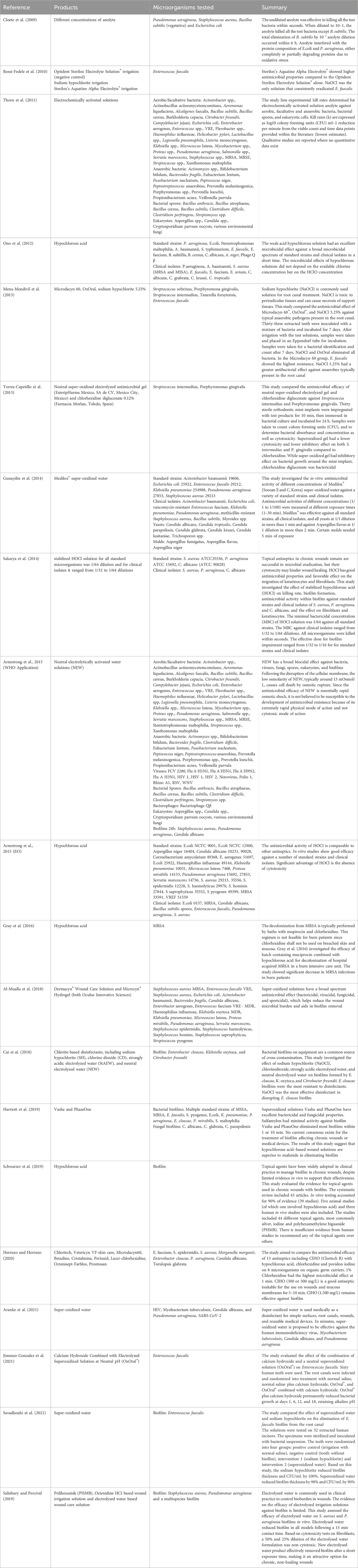
Table 2. Antimicrobial properties of superoxidized solutions reported in literature.
3.1.3 Biocompatibility of superoxidized solutions
Wound irrigation solutions offer the first line of defense against microbial colonization of the wound. Intimate contact with viable wound cells is inevitable, so it is vital that wound irrigation solutions demonstrate good cell compatibility. Cytotoxic effects of a wound dressing would reduce the viability, proliferation, and migration of cells involved in the wound healing process, leading to decreased healing rate. Cytotoxicity data derived from in vitro studies must be interpreted with caution, as any cytotoxic effects observed in cultured cell types can be magnified and may not reflect the clinical setting. Overall, the evidence points to minimal or low cytotoxicity of superoxidized solutions. Superoxidized solutions do not induce skin sensitization or irritation in animal studies despite the high oxido-reduction potential (ORP) and antimicrobial activity (see Table 3).
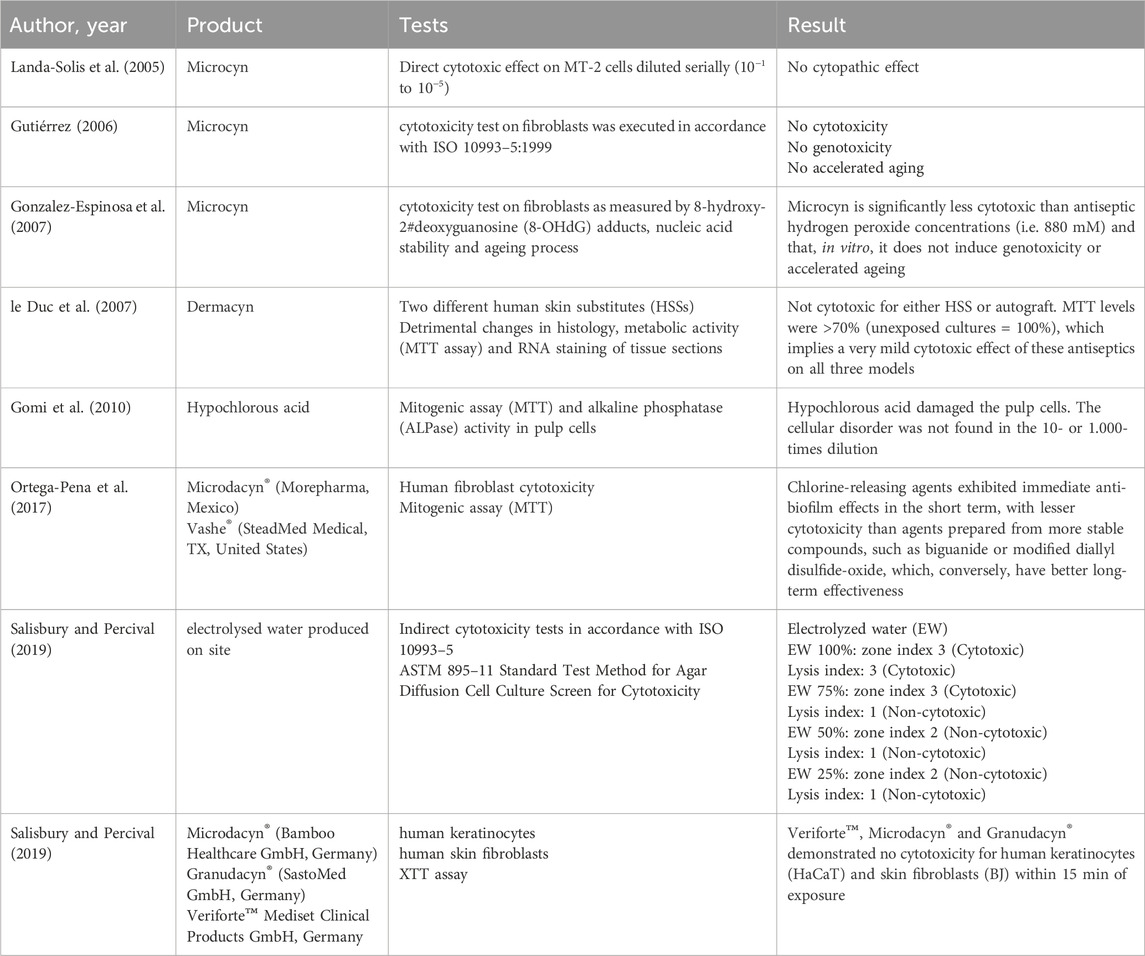
Table 3. Overview of cytotoxicity of superoxidized solutions identified in literature.
3.2 Survey respondents
The Manufacturer collected 237 survey forms from 81 different healthcare facilities, nursing homes, and outpatient clinics located in 57 towns and cities around the Czech Republic. The majority of forms (214) were filled in and signed by nurse practitioners.
3.3 Characteristics of the treated population
Of the 237 patients, 115 were male and 122 were female. More men were represented in the younger categories than women (see Figure 1).
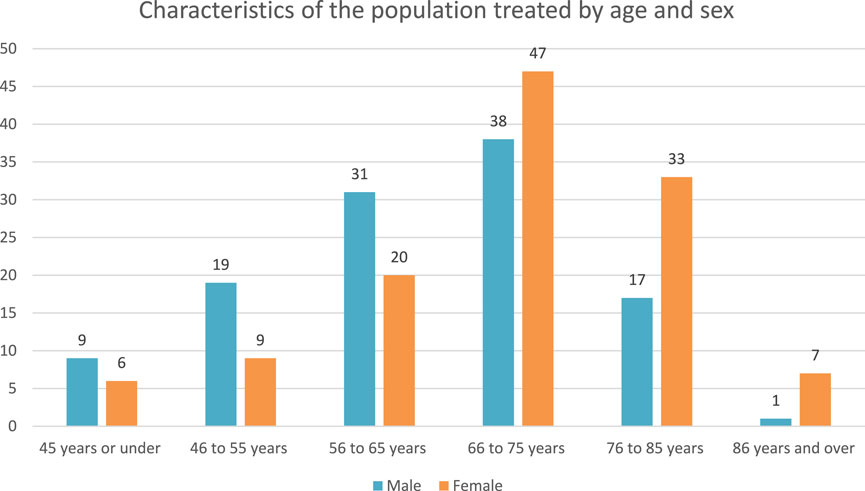
Figure 1. Patient characteristics by age and sex.
The most common basic diagnoses were venous leg ulcer (91; 38%), pressure ulcer (41; 17%), diabetic foot ulcer (28; 12%), and traumatic wound (18; 8%) (see Figure 2).
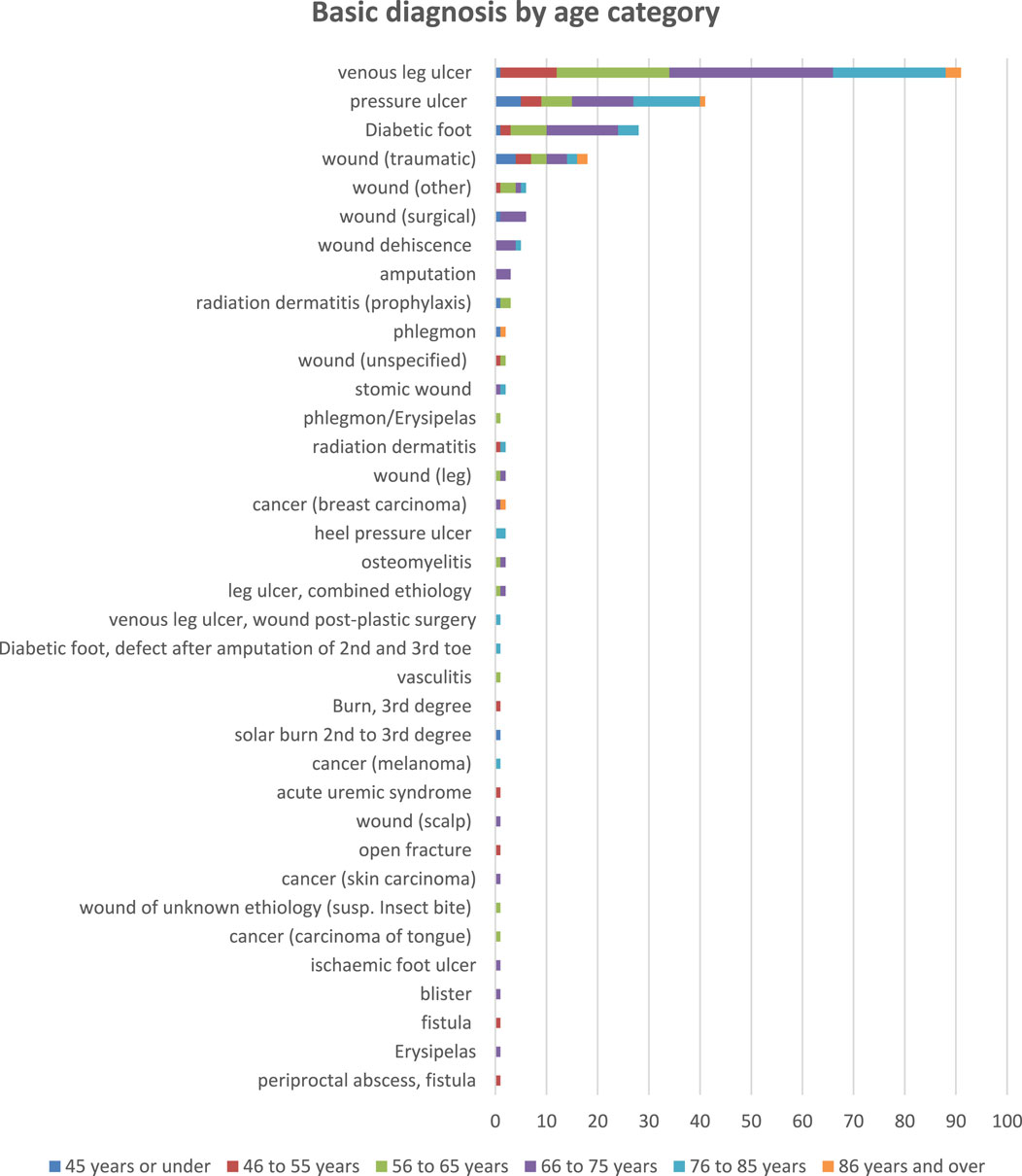
Figure 2. Patient characteristics: Basic diagnosis by age category.
Of the 237 patients, 99 (42%) had body mass index (BMI) over 30, 90 (38%) suffered from diabetes mellitus, 79 (33%) had peripheral artery disease (PAD), to include ischemic foot or critical limb ischemia (CLI), 73 (31%) smoked tobacco, 27 (11%) had cancer, 22 (9%) were alcoholics, 22 (9%) had hypertension, 12 (5%) were on corticosteroid treatment, 7 (3%) had varicose veins, 6 (3%) suffered from chronic venous insufficiency, and 5 (2%) had COVID-19. Only 19 (8%) of the 237 included patients had no reported comorbidities and no risk factors (see Figure 3).
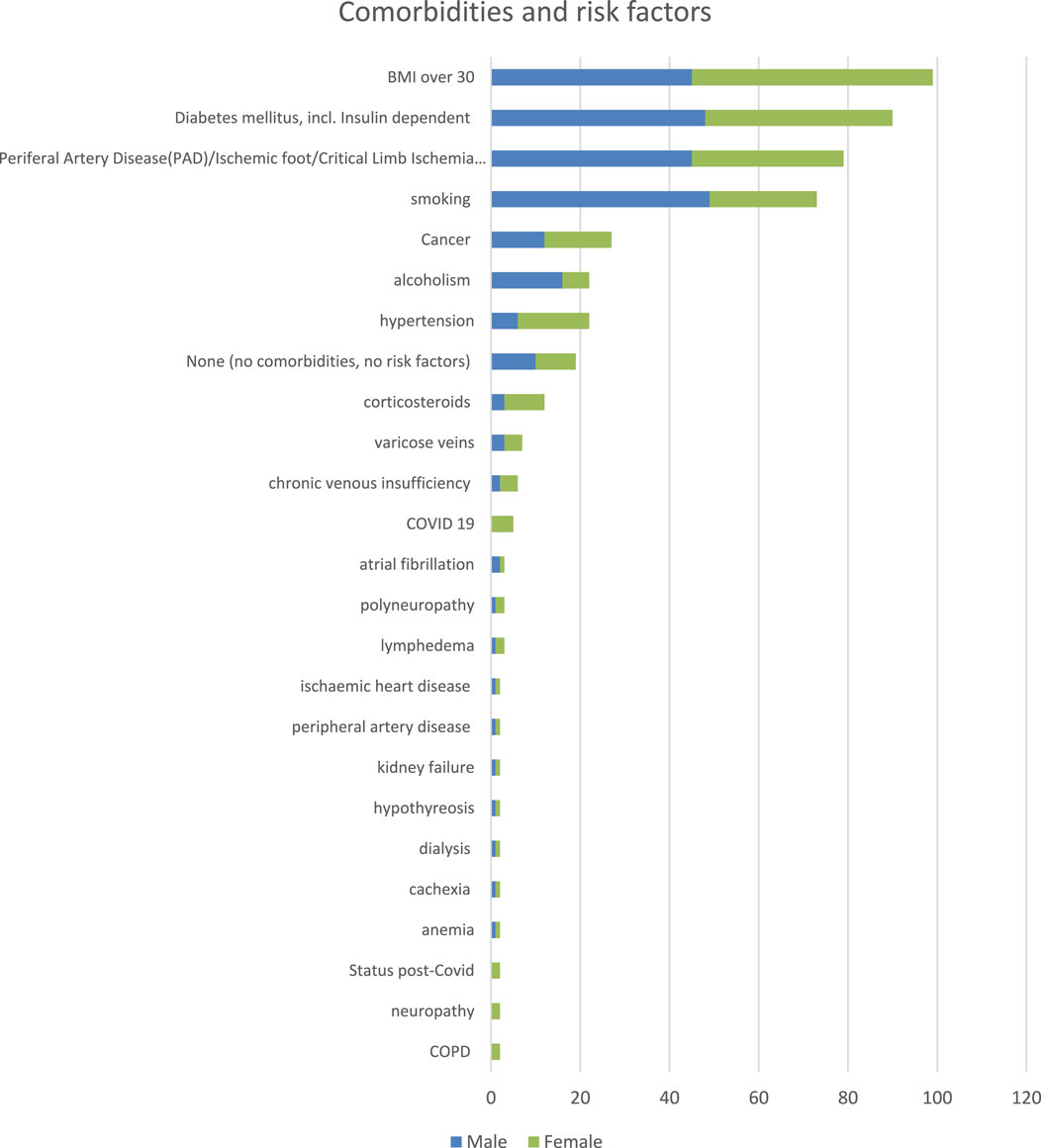
Figure 3. Patient characteristics: Comorbidities and risk factors.
3.4 Time lag between the appearance of the wound and initial examination
The time lag between the injury and the first visit when treatment with DebriEcaSan Alfa was initiated varied greatly between the patients. Only 39 (16%) patients presented with their wounds within a week. Another 94 (40%) patients came with wounds older than 1 week but within 3 months (See Table 4). A significant number of patients (55, 23%) presented with chronic, non-healing wounds that were older than 3 months. Of these, 27 patients had wounds older than 2 years at initial examination, including 5 patients whose wounds lasted 10 years or more. There is no difference between men and women when it comes to the time lag between the first appearance of the wound and the time of initial examination. The wounds that were older than 3 months at the time of presentation (55 patients) tended to be complex, large, and with symptoms of infection (see Table 5). The 49 patients who presented with wounds where the time lag was unknown had significant comorbidities and risk factors and wounds that were often large, deep, and with symptoms of infection (see Table 6).
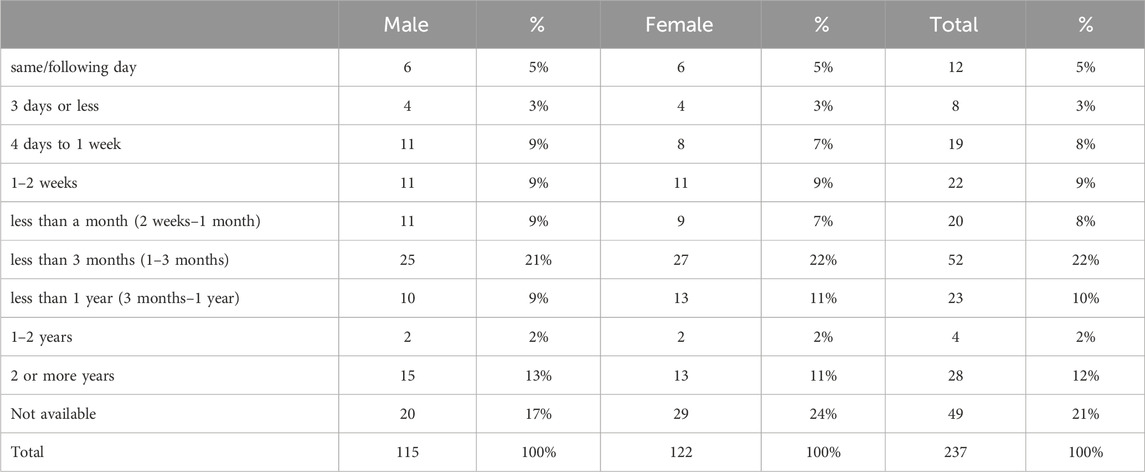
Table 4. The time lag between the injury and the first visit.
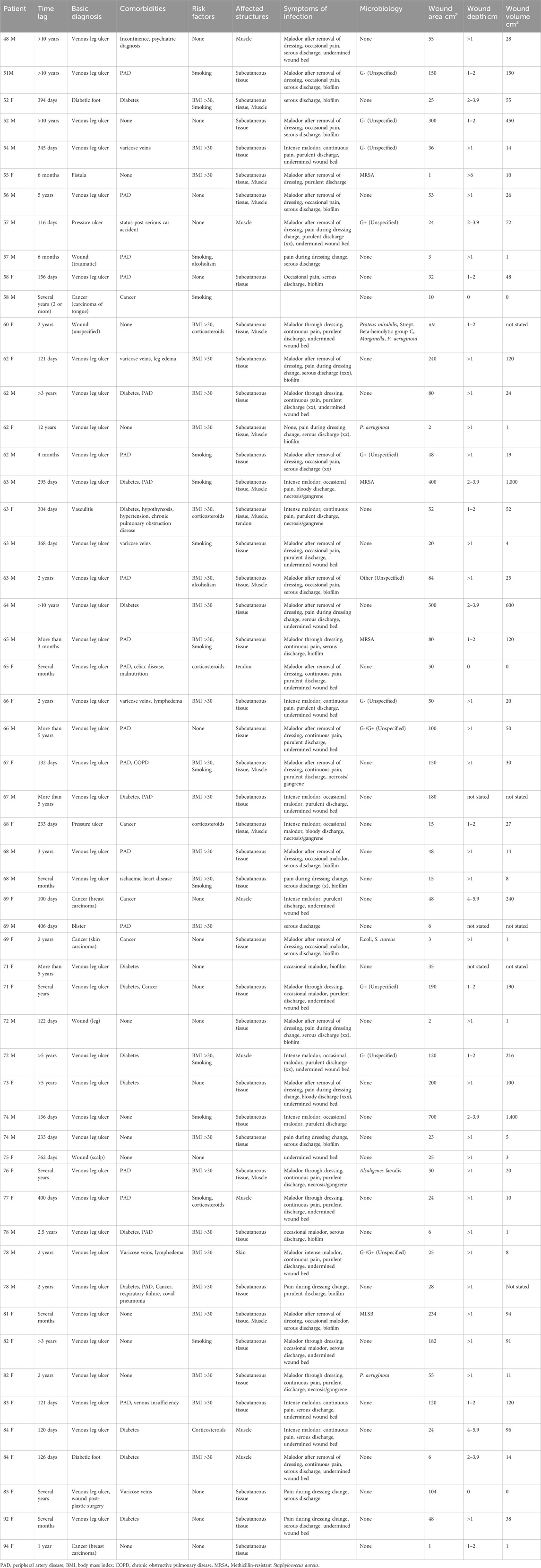
Table 5. Characteristics of wounds older than 3 months at first presentation.
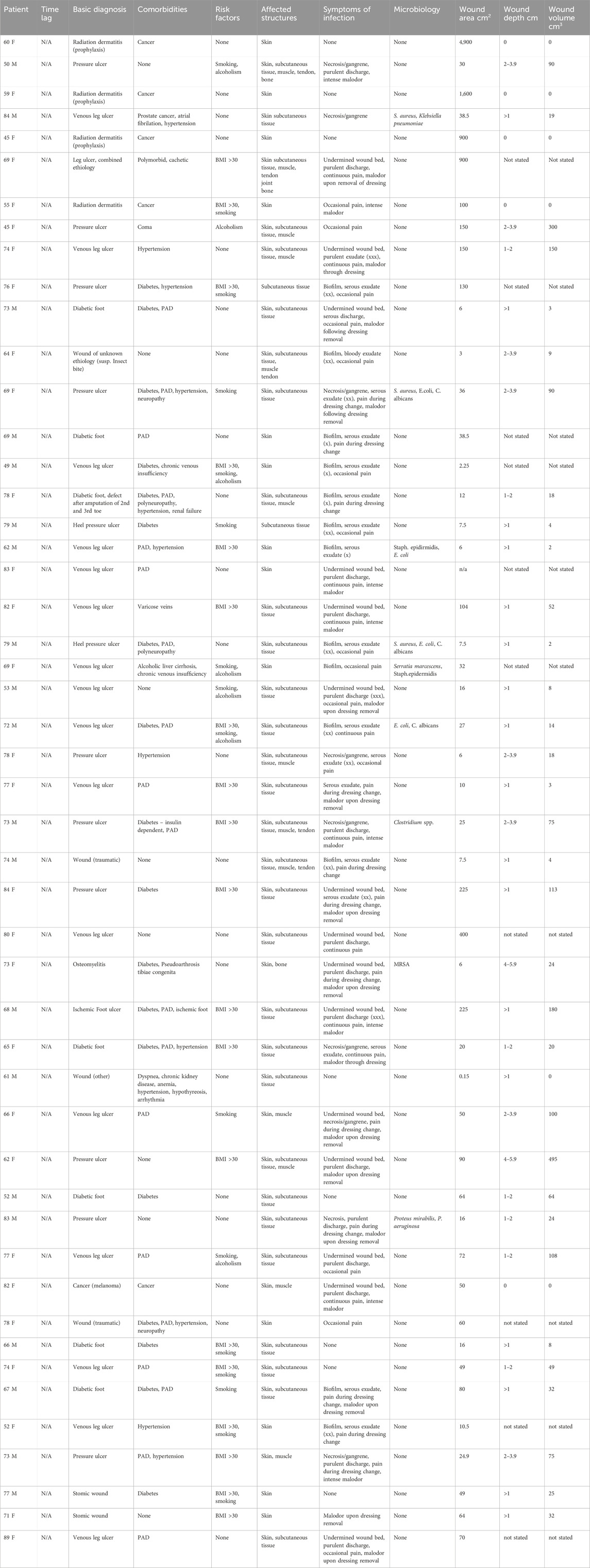
Table 6. Characteristics of wounds where time lag between wound first appearance and initial presentation was not known.
3.5 Methods of use of DebriEcaSan Alfa
The most common method of use was soaking a piece of gaze or other material in the irrigation solution and leaving it in the wound for 10–20 min before proceeding with a dressing change. 211 respondents applied this method. The remaining users reported spraying, irrigating, or flushing the wound with DebriEcaSan Alfa before applying primary dressing, typically a gel. The reported exposure time ranged from 1 min to 3 h. The frequency of dressing changes ranged from 5-times a day to once a week. DebriEcaSan Alfa is typically used with barrier cream to protect the wound edges and other primary and secondary dressing. Additional interventions included surgical debridement, necrectomy, and larval therapy. Of the 239 patients, 77 were treated with intravenous and oral antibiotics.
3.6 Wound healing
3.6.1 Affected tissues
The number of patients with wounds affecting subcutaneous tissue steadily decreased from 183 at the initial examination to 171 at week 3, 158 at week 6, 109 at week 9, and 56 at week 12. Similarly, the number of wounds affecting muscle decreased from 92 at the initial examination to 58 at week 3, 38 at week 6, 26 at week 9, and 7 at week 12. There is a downward trend for wounds affecting the tendon from the initial 22 to 9 at week 3, 6 at week 6, 4 at week 9, and 1 at week 12. The number of wounds affecting joints and bones also decreased over time (see Figure 4).
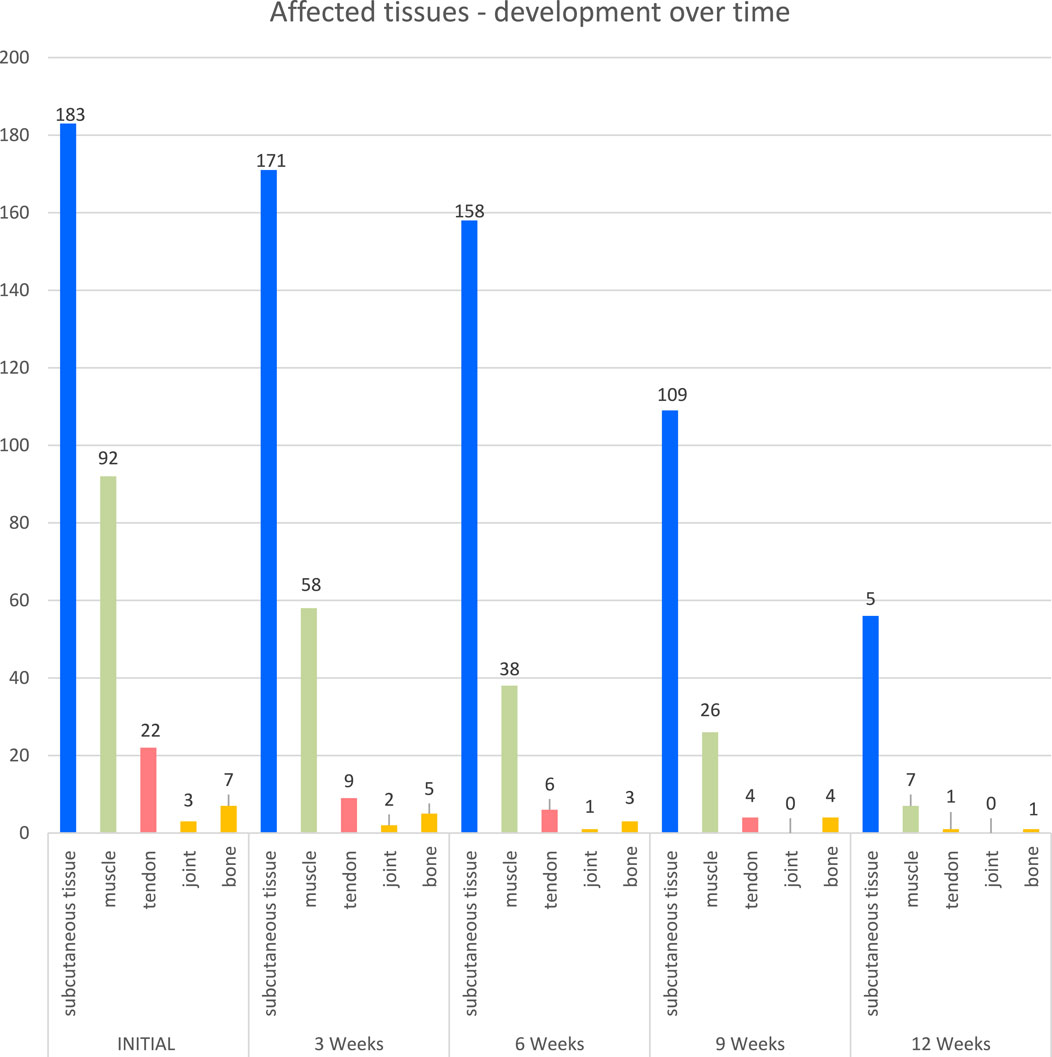
Figure 4. Affected tissues.
3.6.2 Symptoms of infection
3.6.2.1 Symptoms of infection
The number of patients with wounds with biofilm increased by week 3 from 69 (29%) to 118 (50%). After this peak, there is a downward trend from week 3 to week 12. The number of wounds with undermined wound beds decreased from 75 (32%) at the initial examination to 15 (16%) at 6 weeks, 3 (1%) at 9 weeks, and 2 (1%) at 12 weeks. Similarly, the number of patients with necrotic, gangrenous wounds dropped from 58 (24%) at the initial examination to 19 (8%) at weeks, 5 (2%) at 6 weeks, 3 (1%) at 9 weeks, and 0 at 12 weeks. The number of patients with no symptoms of infection steadily grew from 35 (15%) at the initial examination to 65 (27%) at week 3, 121 (51%) at week 6, 159 (67%) at week 9, and 199 (84%) at week 12. A significant number of patients had infected wounds: 69 (29%) presented with biofilm, 75 (32%) had undermined wound beds, and 58 (24%) had wounds that were necrotic or gangrenous. The number of wounds with infection symptoms steadily decreased over the 12 weeks of treatment (see Figure 5). Of the 118 patients with biofilm at week 3, only 8 reported microbiological findings: Bacteroides fragilis (1), Enterobacter cloacae, (1), Staphylococcus aureus (3), Proteus mirabilis (1), and Pseudomonas aeruginosa (1).
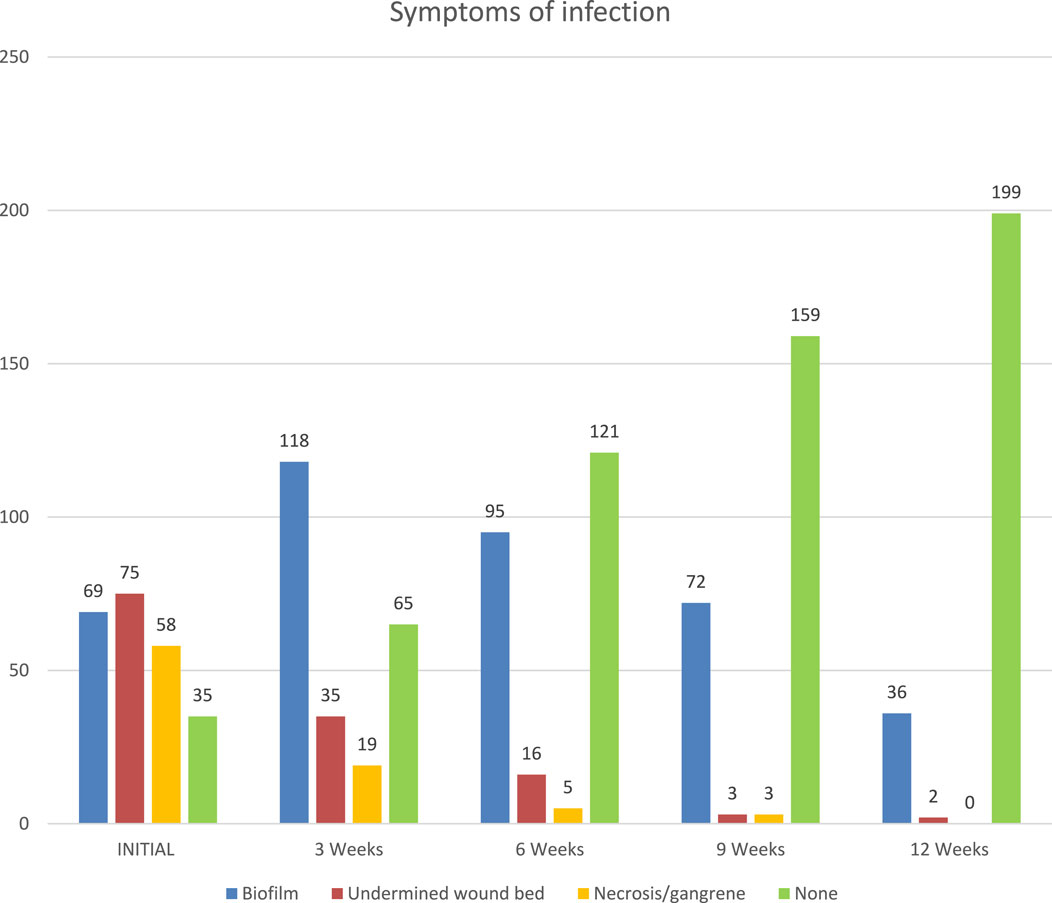
Figure 5. Symptoms of infection: biofilm, undermined wound bed, necrosis/gangrene.
3.6.2.2 Exudate
The number of wounds with purulent, and bloody exudate decreased over time, partly changing to serous exudate, before clearing up completely. The number of wounds with no exudate increased from 30 (13%) during the initial examination to 188 (79%) at week 12. 102 (43%) patients presented with wounds secerning serous exudate; 25 (11%) had bloody exudate weeping from their wounds, and 81 (34%) showed purulent discharge. The number of wounds with purulent, and bloody exudate decreased over time, partly changing to serous exudate, before clearing up completely. The number of wounds with no exudate increased from 30 during the initial examination to 188 at week 12 (see Figure 6).
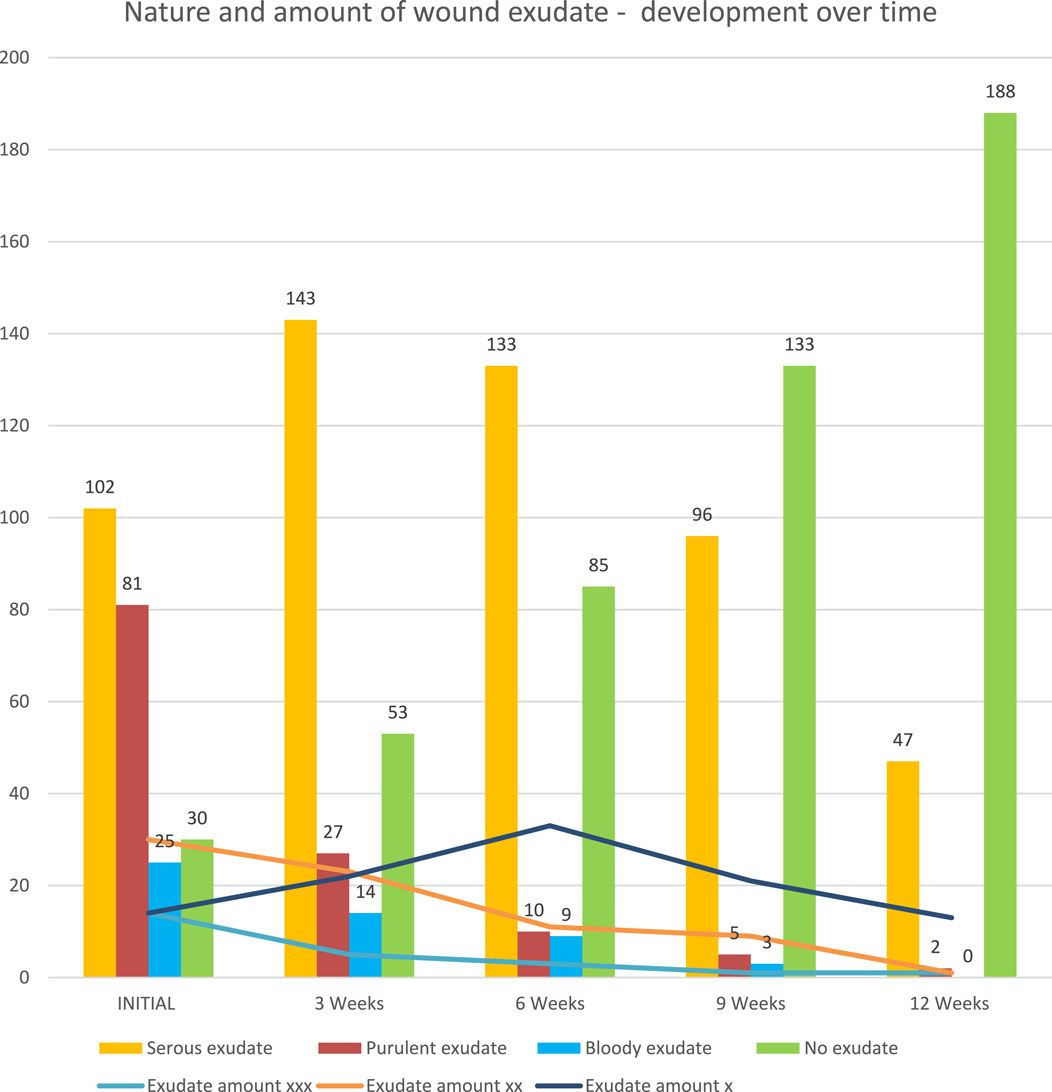
Figure 6. Nature and amount of wound exudate–development over time (graph).
3.6.2.3 Pain
The intensity and number of patients reporting pain decreased over the monitoring period. At the initial examination, only 36 (15%) patients reported no pain. This number increased to 77 (32%) at week 3, 132 (56%) at week 6, 173 (73%) at week 9, and 209 (88%) at week 12. Pain reported by patients decreased in intensity and numbers. At the initial examination, 36 (15%) patients reported no pain. This number increased to 77 (32%) at week 3, 132 (56%) at week 6, 173 (73%) at week 9, and 209 (88%) at week 12. At initial examination, 51 (22%) patients reported continuous pain, 64 (27%) experienced pain during dressing change, and 86 (36%) stated their pain was intermittent (See Figure 7).
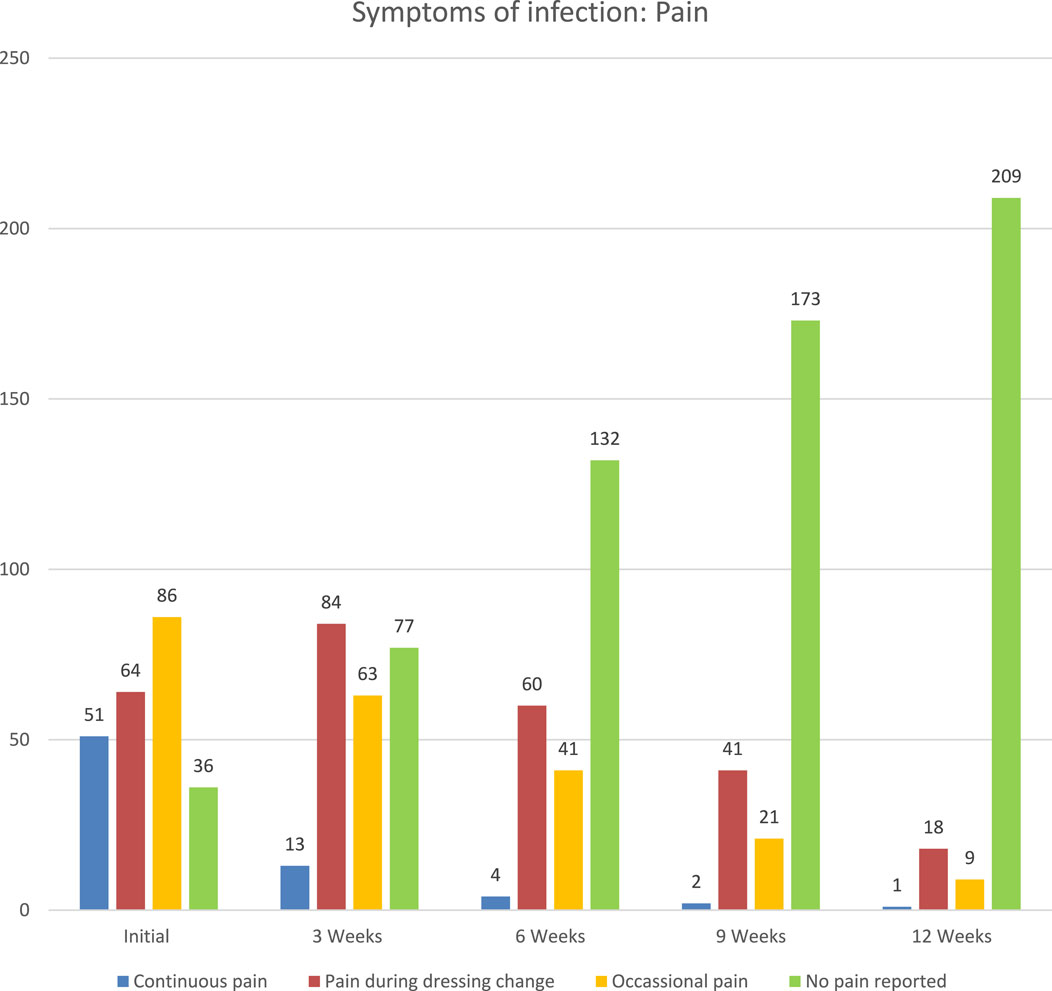
Figure 7. Reported pain over time.
3.6.2.4 Malodor
Malodor was effectively eliminated within the first 3 weeks of treatment in the majority of patients. Intense malodor dropped from 37 (16%) at the initial examination to 6 (3%) at 3 weeks and 1 at 6 weeks. Wounds without malodor increased from 101 (43%) at the initial examination to 166 (70%) at week 3, 197 (83%) at week 6, 204 (86%) at week 9, and 223 (94%) at week 12. Initially, intense malodor affected 37 (16%) patients. An additional 27 (11%) patients reported malodor through dressing and 72 (30%) experienced malodor upon dressing removal. Malodor was effectively eliminated within the first 3 weeks of treatment in the majority of patients. The number of patients whose wounds expressed intense malodor dropped from 37 at the initial examination to 6 at 3 weeks and 1 at 6 weeks. The number of patients with wounds without malodor increased from 101 at the initial examination to 166 at week 3, 197 at week 6, 204 at week 9, and 223 at week 12 (See Figure 8).
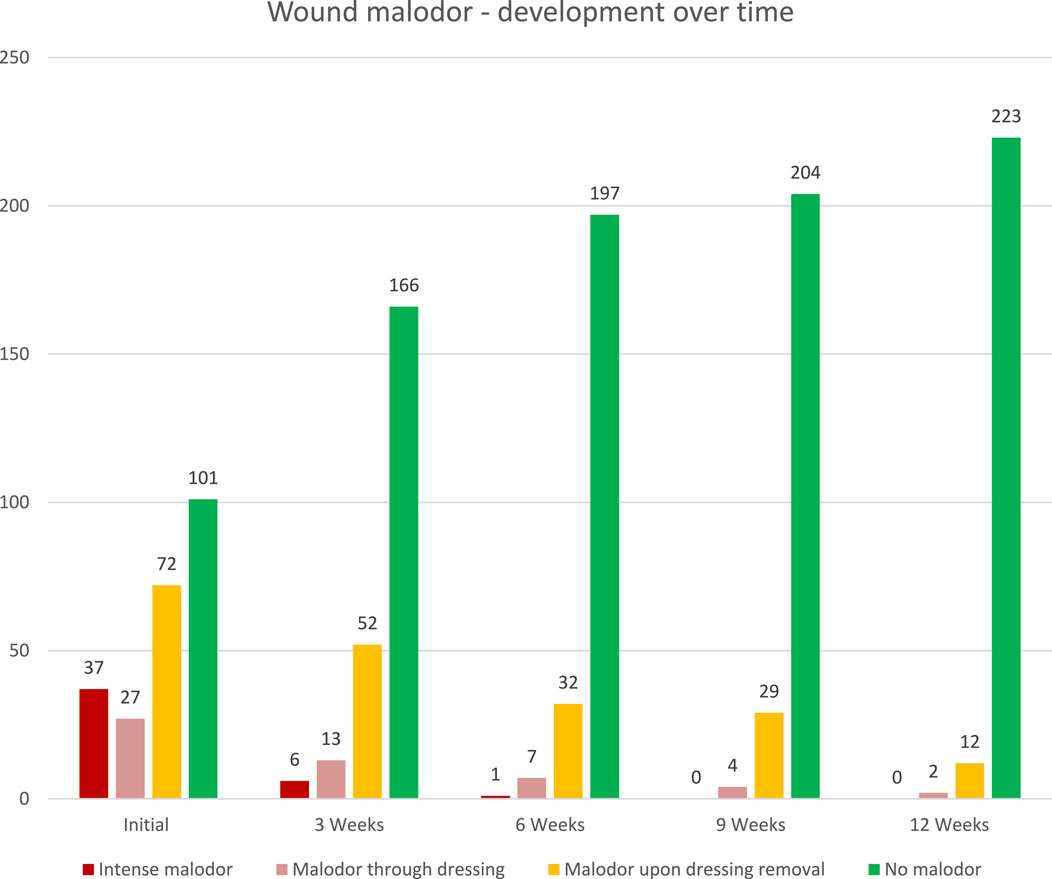
Figure 8. Wound malodor–development over time (graph).
3.6.3 Wound microbiology
The majority of patients (179 out of 237) did not have any wound microbiology performed. The pathogens isolated from the 60 tested patients included S. aureus, Staphylococcus haemolyticus, Staphylococcus epidermidis, MRSA, MLSB, Streptococcus dysgalactiae, Streptococcus Beta-hemolytic group C, Escherichia coli, Alcaligenes faecalis, Enterococcus cloacae, Enterococcus faecalis, P. mirabilis, Proteus vulgaris, P. aeruginosa, Morganella spp., Klebsiella pneumoniae, Klebsiella oxytoca, Serratia marcescens, Serratia odorifera, Clostridium Hathewayi, Clostridium spp., Corynebacterium Striatum, and Candida albicans.
13 patients were tested in week three. The bacterial isolates included E. cloacae (1), S. aureus (4), P. aeruginosa (4), Streptococcus haemolyticus (1), K. pneumoniae (1), P. mirabilis (1), B. fragilis (1) and Corynebacterium striatum (1). Isolates cultivated in week 6 included S. aureus (2), P. aeruginosa (3), E. coli (2), and K. pneumoniae (1). Bacterial isolates from week 9 included Escheria coli (2), Staphylococcus cohnii (1), and Enterobacter faecalis (1). A combined infection caused by Staphyloccocus capitis and B. fragilis was detected in one patient in week 12.
3.6.4 Wound healing: wound size and wound closure
3.6.4.1 Granulation and epithelization
The progress of granulation and epithelization over the course of treatment shows steady increase in granulation tissue and epithelization. No hypergranulation was observed (Table 7).
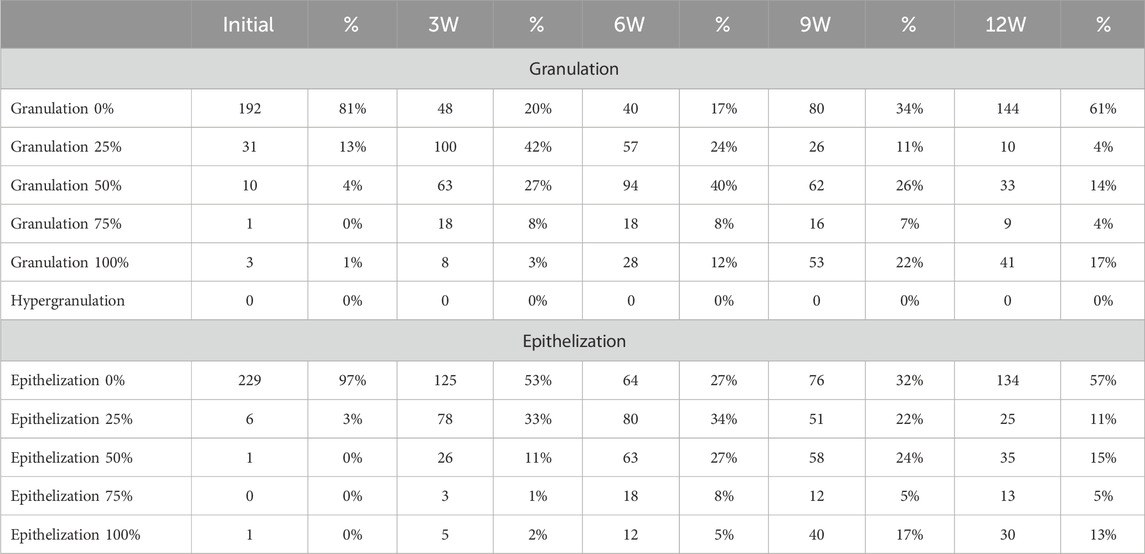
Table 7. Wound granulation and epithelization–development over time.
3.6.4.2 Wound size and depth
The wounds are routinely measured as part of standard treatment protocols. However, the methodology may differ from one facility to another. Some healthcare establishments routinely take photographs to document progress. A significant number of patients presented with large and deep wounds. At the initial presentation, 85 (36%) patients presented with wounds that were larger than 50 cm2, of which 8 (3%) had wounds larger than 500 cm2 and 16 (7%) between 200 and 499 cm2 (see Figure 7). A marked reduction in wound surface area size was observed in all wound size categories (see Table 8). 24 patients presented with large, deep and complex wounds. The healing times and outcomes reflect the nature and origin of the wounds, underlying disease and complications. This cohort illustrates the typical challenges experienced when measuring outcomes in wound healing (Table 9). Wound depth was stratified into ranges 0 (superficial), <1 cm, 1-1.9 cm, 2-3.9 cm, 4-5.9 cm, and >6 cm. Wound depth gradually decreased over the course of 12 weeks even in the most complex patients (Table 10). 19 (8%) patients healed by end of week 6; and 66 (28%) healed by week 9. 130 (55%) patients were considered healed by week 12. 23 (10%) patients were transferred to a different facility, 9 (4%) underwent surgery, 7 (3%) had treatment changed, and 5 (2%) died of their underlying disease. 63 (27%) patients were still healing at week 12 (see Table 11).
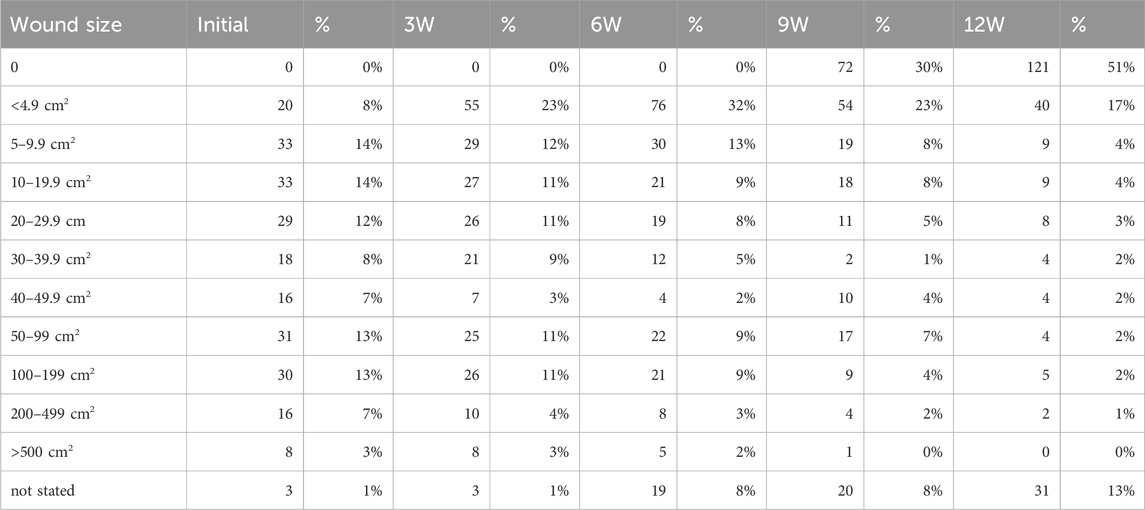
Table 8. Wound surface area size: development over time.
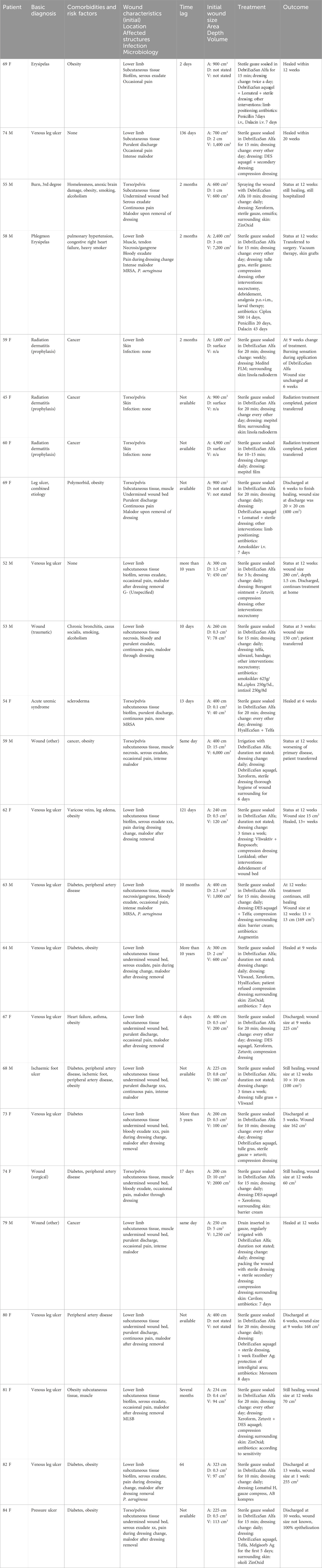
Table 9. Overview of wound characteristics and outcomes of patients with large wounds.
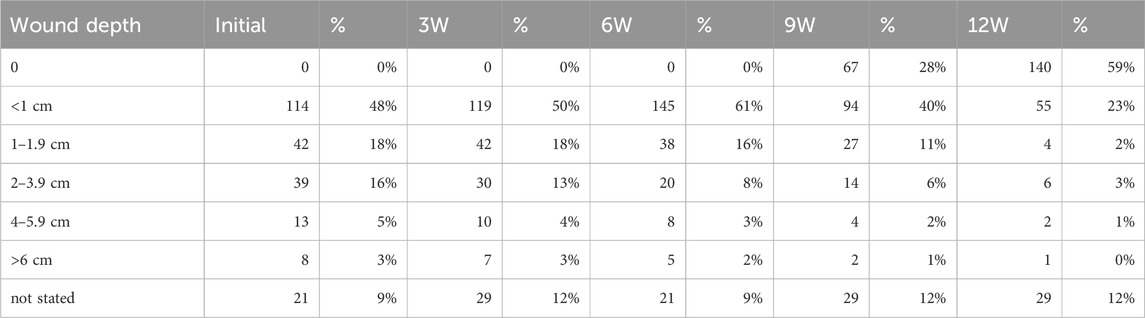
Table 10. Wound depth.
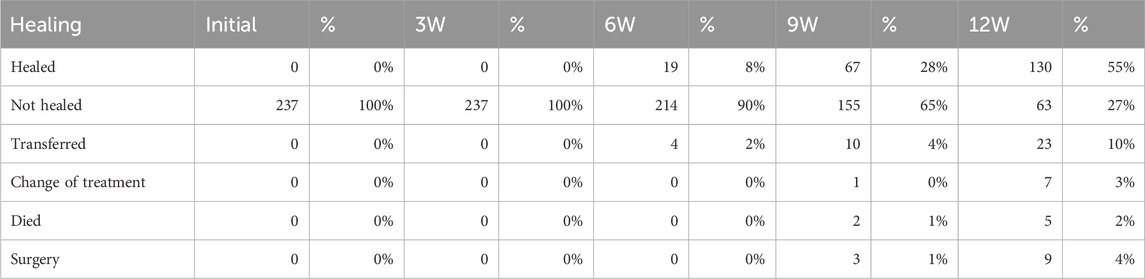
Table 11. Wound healing.
3.6.4.3 Healed wounds
Healing time is one of the most important clinical outcomes in wound care. However, an accurate reading is difficult to obtain because the patients typically only stay in the same facility for part of the duration of their treatment. Moreover, only a minority of wounds are the primary reason for hospitalization but rather a comorbidity or a complication of treatment. In this study, the wounds were marked by healthcare staff as healed either upon complete closure of the wound, where possible, or at discharge from the hospital to a different type of facility or home care when the wound no longer required advanced care. This inconsistency causes a discrepancy between declared wound size and healing status. Hence, wounds that are almost healed at the point of transfer or dismissal are considered healed. More accurate readings can only be obtained from health data across multiple care systems.
3.6.4.4 Case report
A case report of a 64-year-old obese, diabetic male with venous leg ulcer demonstrates how a large defect (20 × 15 cm) healed over the course of 4 months with daily treatment with DebriEcaSan Alfa, DebriEcaSan aquagel, Xeroform, and compression dressing Vliwazel (see Figures 9A–D).
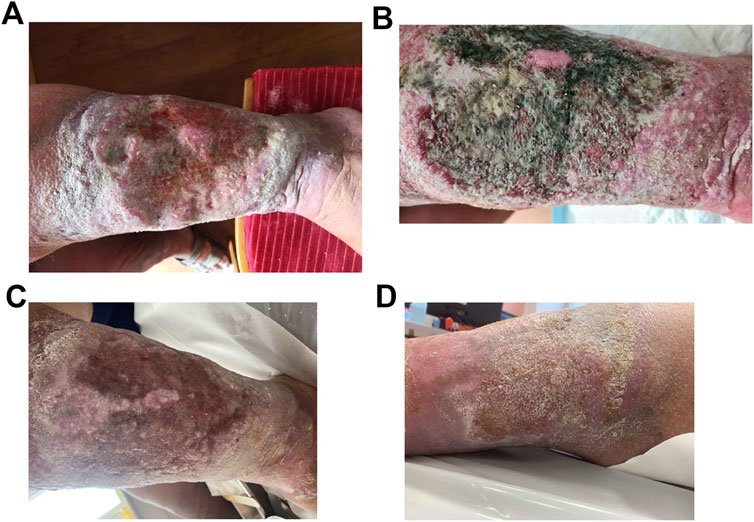
Figure 9. (A) Venous leg ulcer in a 64-year-old male patient (18 July 2022). (B) Infected venous leg ulcer (22 August 2022). (C) Significantly improved venous leg ulcer (19 September 2022). (D) Healed venous leg ulcer (21 November 2022).
3.6.5 Venous leg ulcer: A case report
A 64-year-old male patient, S.P., was treated at the Dobrovskeho Polyclinic, 1st surgical clinic, Brno, for a venous leg ulcer. The patient’s medical history included obesity, diabetes, and limited mobility of the lower extremities. The patient presented with severe limb edema but was unwilling to use a compression bandage. The patient was able to walk a short distance without aid but breathless. Difficulty breathing was also apparent at rest during prolonged conversation. The patient was not following the diabetic diet he was prescribed. The patient was adequately hydrated, calm, oriented, had a good memory, and was communicating adequately. The patient reported intermittent pain at the site of ulceration and is currently without pain medication.
The patient presented at the surgery with a venous leg ulcer on the lateral side of his left lower limb, size 20 × 15 cm, with an undermined wound bed without signs of ascendent infection. Sterile gauze soaked with wound irrigation solution DebriEcaSan Alfa was applied into the wound for 15–20 min, followed by primary gel dressing DebriEcaSan aquagel, a petrolatum-based fine mesh gauze containing 3% bismuth tribromophenate Xeroform, and compression dressing Vliwazel. The dressing was changed every 24 h.
A month later, the venous leg ulcer, size 20 × 15 cm, with sweet malodor and signs of infection. Cultivation revealed P. mirabilis. In addition to the existing treatment protocol, the patient received systemic antibiotics.
Two months after the initial presentation, the ulcer showed marked improvement, with a reduction in size (both surface area and depth) to 10 × 5 cm and minimal secretion. The wound shows granulation and epithelization progressing from the edges. The treatment protocol includes sterile gauze soaked in DebriEcaSan Alfa applied to the wound for 15–20 min, followed by DebriEcaSan aquagel, Xeroform dressing, and compression dressing Vliwazel. The dressing was changed every 24 h.
Four months after the initial presentation, the ulcer healed completely.
3.6.6 Complications, adverse events
In total, ten patients experienced complications as reported on the form, most of which related to the underlying condition. Three patients experienced adverse events that have a plausible causal relationship to DebriEcaSan Alfa: maceration of wound edges (64 M with pressure ulcer), burning and itching (59 F with radiation dermatitis), and burning and stinging (70 F with venous leg ulcer).
4 Discussion
The use of antiseptics for wound irrigation remains controversial and no authoritative recommendation currently exists for the use of specific solutions and methods for the irrigation of pressure ulcers (European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance, 2019), infected leg ulcers (National Institute for Health and Care Excellence, 2020), and diabetic foot ulcers (Saeg et al., 2021; Eriksson et al., 2022; Senneville et al., 2024).
In this PMCF study, we found that superoxidized solution DebriEcaSan Alfa is safe and effective in the treatment of acute and chronic wounds, leading to wound size reduction, improved granulation and epithelization, and decrease in microbial load, leading to the reduction of malodor and pain.
As documented in numerous in vitro studies, various brands of superoxidized solutions are effective against a number of aerobic, facultatively aerobic, and anaerobic bacteria, viruses, bacterial spores, bacteriophages and fungi (Cloete et al., 2009; Rossi-Fedele et al., 2010; Thorn et al., 2011; Ono et al., 2012; Mena-Mendivil et al., 2013; Torres-Capetillo et al., 2013; Gunaydin et al., 2014; Sakarya et al., 2014; Armstrong et al., 2015; Gray et al., 2016; Al-Mualla et al., 2018; Herruzo and Herruzo, 2020; Aranke et al., 2021; Jimenez-Gonzalez et al., 2021). They also show good efficacy against biofilms (Gold et al., 2020; Sakarya et al., 2014; Armstrong et al., 2015; Al-Mualla et al., 2018; Cai et al., 2018; Harriott et al., 2019; Schwarzer et al., 2019; Savadkouhi et al., 2021; Salisbury and Percival, 2019). DebriEcaSan Alfa demonstrated similar microbicidal properties in vitro, including P. aeruginosa, S. aureus, Enterococcus hirae, and E.coli K12, Candida albicans, Aspergillus brasiliensis (niger), Mycobacterium avium and Mycobacterium terrae. The majority of evidence of the antimicrobial efficacy of superoxidized solutions comes from in-vitro studies. Due to this lack of evidence from human in-vivo studies, no recommendations exist to support one irrigation solution over the others using clinical endpoints, such as time to heal, reduction of wound bioburden, elimination of infection, or the rate of complications. Superoxidized solutions have minimal to low cytotoxicity and are widely recognized as non-sensitizing and non-irritating (Landa-Solis et al., 2005; Gutiérrez, 2006; Gonzalez-Espinosa et al., 2007; le Duc et al., 2007; Gomi et al., 2010; Ortega-Pena et al., 2017; Salisbury and Percival, 2019; Severing et al., 2019). DebriEcaSan Alfa was proven to be non-cytotoxic and non-irritating.
The patient demographics included in the study was a representative sample of wound patients in regard to age, sex, basic diagnosis, comorbidities, and risk factors. The majority of the patients included in the study were adults, older adults and the elderly. Of the 237 patients treated with DebriEcaSan Alfa, only a small minority were younger than 45 years of age. Both sexes are equally represented. The most common diagnoses were venous leg ulcer (91; 38%), pressure ulcer (41; 17%), diabetic foot ulcer (28; 12%), and traumatic wound (18; 8%).
Diabetic patients are more likely to develop polymicrobial wound infections due to impaired leucocyte function and suboptimal inflammatory response (Burgess et al., 2021), leading to poor formation of granulation tissue and delayed wound healing. Obesity adversely affects healing through poor vascularization of adipose tissue, oxidative stress, abnormalities in the function of immune mediators, and nutritional deficiencies (Pierpont et al., 2014). Unsurprisingly, diabetes (90; 38%), obesity (99; 42%), peripheral artery disease (79; 33%), and tobacco use (73; 31%) turned out to be the most frequently cited conditions in non-healing wounds. This patient risk profile is consistent with data reported from literature (Pokorna, 2017).
The wound characteristics varied greatly in terms of wound severity, size, chronicity, and the presence of infection. The wounds that were older than 3 months at the time of presentation tended to be complex, large, deep, and with symptoms of infection.
The severity and size of the wounds decrease steadily during the 12 weeks of treatment, with improvement apparent in all aspects of wound healing, from tissues affected to symptoms of infection, malodor, and pain. Somewhat unexpectedly, DebriEcaSan Alfa was typically used not as an irrigation solution but as a poultice. Healthcare staff left material soaked in the solution for 10–20 min before proceeding with a dressing change, in an apparent attempt to utilize antimicrobial function of DebriEcaSan Alfa to combat wound infection. This fact only became apparent due to the survey questions that prompted the respondents to describe how they use the product in clinical practice, without making any suggestions regarding its correct use. None of the current clinical guidelines recommends poultice as the preferred method of application. About a third (77 out of 239 patients) received oral or intravenous antibiotics. Additional interventions included surgical debridement, necrectomy, and larval therapy. As documented by Pokorna (2017), the paucity of data available through official reporting systems makes it impossible to establish baseline. The overall severity of a case is defined by detailed characteristics and grading of the wound itself, as well as the patient’s comorbid conditions, and their ability for self-care. The severity of a case directly impacts the expected healing times, the rate and nature of complications, and healing outcomes. This level of detail cannot be obtained from existing databases for comparison. Without such baseline, it is impossible to tell how specific interventions perform in comparison to alternative treatment options.
Pain and malodor are measures very important to patients, yet, available literature remains largely silent on these endpoints. No data on the duration of treatment and cost of treatment is available in national registries. This dataset provides an important benchmark needed for comparison in future studies.
Clinical research in wound care faces specific challenges. Typically, patients with extensive medical histories present with chronic, complex wounds that require interventions that are highly visible and difficult to blind. Different staff members treat the patients over an extended period, and often across multiple care settings. Treatment is often modified in response to the stage of healing and emerging complications, making each wound an experiment. A chronic wound is often not a primary reason for hospitalization but a comorbidity or, in the case of pressure ulcers, a complication of hospitalization. Moreover, a treatment protocol is often modified upon transfer to a different healthcare setting, such as discharge from acute care to a long-term care facility, outpatient, or home care. Additional limitations in medical device studies are of a regulatory nature.
The most common experimental and non-experimental designs used in wound care (Stephenson, 2022), include parallel randomized controlled trials and cross-over trials. Cluster trials assign a specific treatment protocol to all patients within a specific facility. Randomized controlled trials are relatively rare in the field of wound care due to challenges with blinding and appropriate sample sizes. Additional options include quasi-experimental designs, cohort studies, and case-control studies. Even observational studies can provide a high level of evidence. The most common design in wound care is a single-sample study, also called a “pre-post” or “paired” design, where the patients act as their own control. Here, the researchers collect data points pre- and post-intervention, such as wound pH and change of wound size from baseline (Stephenson, 2022).
The Food and Drug Administration (FDA) issued guidance on generating real-world evidence to support regulatory submissions for medical devices. For example, RWE can be used as a historical control, a prior in a Bayesian trial. RWE can also serve as a control group or provide evidence for expanding the device labeling to include additional indications for use or to add new information on safety and effectiveness (FDA, 2017).
This PMCF study offers valuable insight into the real-world use of wound irrigation solution DebriEcaSan Alfa (NewWater Meaning s.r.o.) in the Czech Republic. The data show that the patients who present with chronic wounds tend to suffer from multitude of comorbidities and risk factors that interfere with the healing process. The wounds also tend to be large, deep, complex, and often infected at the initial examination. A significant number of patients presented with wounds that were many months and even years old. DebriEcaSan Alfa is typically used on a soaked sterile gauze and applied for several minutes to increase its antimicrobial effect as opposed to simple irrigation as suggested by the manufacturer. This practice observed in clinical settings emphasizes the importance of biological compatibility, especially low cytotoxicity in combination with broad antimicrobial activity.
The observed clinical effect seems intuitively favorable. However, there is no objective baseline to compare the results to, as typical healing times in a comparable population are not accessible. No single standard of care exists in the treatment of chronic wounds, and significant variability in practices exists across the health system.
In the future, adequately designed and powered studies are needed to produce sufficient quality of evidence to provide confident recommendations in the product used and methods employed in wound irrigation.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the studies involving humans because This is a post-market clinical follow-up (PMCF) study within the scope of the device’s intended purpose that does not submit the patients to invasive or burdensome procedures additional to those performed under the normal conditions of use of the device performed by the manufacturer of DebriEcaSan Alfa, NewWaterMeaning, s.r.o., Czech Republic. The study is part of the Manufacturer’s Post-Market Surveillance Plan and it is conducted in compliance with European Medical Device Regulation (EU MDR) 2017/745, Article 74. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
VV: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing–original draft, Writing–review and editing. VŠ: Conceptualization, Funding acquisition, Resources, Supervision, Writing–review and editing. LL: Data curation, Project administration, Writing–review and editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article. The study was funded by NewWaterMeaning, s.r.o., the Czech Republic, the manufacturer of DebriEcaSan Alfa. No government funding was used.
Conflict of interest
Author VV was an independent consultant for NewWaterMeaning, s.r.o. Authors VŠ and LL were employed by NewWaterMeaning, s.r.o.
The authors declare that this study received funding from NewWaterMeaning, s.r.o. The funder had the following involvement in the study: data collection and the writing of this article. The funder was not involved in the study design, analysis, interpretation of data, or the decision to submit it for publication.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdsfr.2024.1402684/full#supplementary-material
References
Al-Mualla, S., Farhat, R. A., Juma, R., and Tarnow, P. (2018). Antimicrobial super oxidised solutions and laser therapy: a novel wound healing approach. Wounds Middle East 5, 36–41.
Alonso-Coello, P., Oxman, A. D., Moberg, J., Brignardello-Petersen, R., Akl, E. A., Davoli, M., et al. (2016b). GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: clinical practice guidelines. BMJ 353, i2089. doi:10.1136/bmj.i2089
Alonso-Coello, P., Schünemann, H. J., Moberg, J., Brignardello-Petersen, R., Akl, E. A., Davoli, M., et al. (2016a). GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: introduction. BMJ 353, i2016. doi:10.1136/bmj.i2016
Aranke, M., Moheimani, R., Phuphanich, M., Kaye, A. D., Ngo, A. L., Viswanath, O., et al. (2021). Disinfectants in interventional practices. Curr. Pain Headache Rep. 25, 21. doi:10.1007/s11916-021-00938-3
Armstrong, D. G., 2017. Application for inclusion on 2017 WHO EML electromicyn solution and hydrogel (stabilised, pH neutral, super-oxidised hypochlorous acid) topical antimicrobial wound healing agent.
Armstrong, D. G., Bohn, G., Glat, P., Kavros, S. J., Kirsner, R., Snyder, R., et al. (2015). Expert recommendations for the use of hypochlorous solution: science and clinical application. Ostomy Wound Manage 61, 2–19.
Bowling, F. L., Crews, R. T., Salgami, E., Armstrong, D. G., and Boulton, A. J. (2011). The use of superoxidized aqueous solution versus saline as a replacement solution in the versajet lavage system in chronic diabetic foot ulcers: a pilot study. J. Am. Podiatric Med. Assoc. 101 (2), 124–126. doi:10.7547/1010124
Burgess, J. L., Wyant, W. A., Abdo Abujamra, B., Kirsner, R. S., and Jozic, I. (2021). Diabetic wound-healing science. Med. Kaunas. 57 (10), 1072. doi:10.3390/medicina57101072
Cai, L., Wang, H., Liang, L., Wang, G., Xu, X., and Wang, H. (2018). Response of formed-biofilm of Enterobacter cloacae, Klebsiella oxytoca, and Citrobacter freundii to chlorite-based disinfectants. J. Food Sci. 83, 1326–1332. doi:10.1111/1750-3841.14149
Chaplin, S. (2020). NICE on antimicrobial prescribing for leg ulcer infection. United Kingdom: Prescriber, 27–30.
Cloete, T. E., Thantsha, M. S., and Kirkpatrick, R. (2009). The antimicrobial mechanism of electrochemically activated water against Pseudomonas aeruginosa and Escherichia coli as determined by SDS-PAGE analysis. J. Appl. Microbiol., 379–384. doi:10.1111/j.1365-2672.2009.04233.x
Dayya, D., O’Neill, O., Habib, N., Moore, J., Iyer, K., and Huedo-Medina, T. B. (2022). Debridement of diabetic foot ulcers: public health and clinical implications – a systematic review, meta-analysis, and meta-regression. BMJ Surg. Interventions, and Health Technol. 4, 0000811–e122. doi:10.1136/bmjsit-2021-000081
Dreifke, M. B., Jayasuriya, A. A., and Jayasuriya, A. C. (2015). Current wound healing procedures and potential care. Mater. Sci. Eng. C Mater. Biol. Appl. 48, 651–662. doi:10.1016/j.msec.2014.12.068
Dumville, J., Lipsky, B., Hoey, C., and Cruciani, M. (2017). Topical antimicrobial agents for treating foot ulcers in people with diabetes (Review). Cochrane, 1–134. doi:10.1002/14651858.CD011038.pub2
Eaglstein, W. H., Kirsner, R. S., and Robson, M. C. (2012). Food and Drug Administration (FDA) drug approval end points for chronic cutaneous ulcer studies. Wound Repair Regen. 20 (6), 793–796. doi:10.1111/j.1524-475X.2012.00849.x
Eriksson, E., Liu, P. Y., Schultz, G. S., Martins-Green, M. M., Tanaka, R., Weir, D., et al. (2022). Chronic wounds: treatment consensus. Wound Repair Regen. 30 (2), 156–171. doi:10.1111/wrr.12994
European Commission, 2017. Regulation (EU) 2017/745 of the European parliament and of the council of 5 april 2017 on medical devices, amending directive 2001/83/EC, regulation (EC) No 178/2002 and regulation (EC) No 1223/2009 and repealing council directives 90/385/EEC and 93/42/EEC
European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance (2019). “Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The international guideline,” in EPUAP/NPIAP/PPPIA. Editor E. Haesler
FDA (2017). Use of real-world evidence to support regulatory decision-making for medical devices. FDA.
Forster, R., and Pagnamenta, F. (2015). Dressings and topical agents for arterial leg ulcers. Cochrane Database Syst. Rev. 2015 (6), CD001836. doi:10.1002/14651858.CD001836.pub3
Gabriel, A. (2021). Wound irrigation. Medscape. Available at: https://emedicine.medscape.com/article/1895071-overview August 27, 2021).
Gold, M. H., Andriessen, A., Bhatia, A. C., Bitter Jr, P., Chilukuri, S., Cohen, J. L., et al. (2020). Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J. Cosmet. Dermatology 19, 270–277. doi:10.1111/jocd.13280
Gomi, K., Makino, T., Suzuki, S., Hasegawa, M., Maeda, N., and Arai, T. (2010). Microbicidal and cytotoxic effects of functional water in vitro. Quintessence Int. 41, e166–e172.
Gonzalez-Espinosa, D., Perez-Romano, L., Guzman-Soriano, B., Arias, E., Bongiovanni, C. M., and Gutierrez, A. A. (2007). Effects of pH-neutral, super-oxidised solution on human dermal fibroblasts in vitro. Int. Wound J. 4, 241–250. doi:10.1111/j.1742-481X.2007.00331.x
Gray, D., Foster, K., Cruz, A., Kane, G., Toomey, M., Bay, C., et al. (2016). Universal decolonization with hypochlorous solution in a burn intensive care unit in a tertiary care community hospital. Am. J. Infect. Control 44, 1044–1046. doi:10.1016/j.ajic.2016.02.008
Gunaydin, M., Esen, S., Karadag, A., Unal, N., Yanik, K., Odabasi, H., et al. (2014). In vitro antimicrobial activity of Medilox® super-oxidized water. Ann. Clin. Microbiol. Antimicrob. 13, 29. doi:10.1186/1476-0711-13-29
Gutiérrez, A. A. (2006). The science behind stable, super-oxidized water. Exploring the various applications of super-oxidized solutions. Wounds Suppl. January 2006 Wounds, 7–10. Available at: https://www.researchgate.net/publication/286739558_The_science_behind_stable_super-oxidized_water_Exploring_the_various_applications_of_super-oxidized_solutions.
Hadi, S. F., Khaliq, T., Bilal, N., Sikandar, I., Saaiq, M., Aurangzeb, S., et al. (2007). Treating infected diabetic wounds with superoxidized water as antiseptic agent: a preliminary experience. J. Coll. Physicians Surg. - Pak. 17 (12), 740–743.
Hans, P. (2022). Role and evaluation of superoxidised solution and gel (microdacyn) in the treatment of pressure ulcers. J. Cardiovasc. Dis. Res.
Harriott, M. M., Bhindi, N., Kassis, S., Summitt, B., Perdikis, G., Wormer, B. A., et al. (2019). Comparative antimicrobial activity of commercial wound care solutions on bacterial and fungal biofilms. Ann. Plastic Surg. 83, 404–410. doi:10.1097/SAP.0000000000001996
Herruzo, R., and Herruzo, I. (2020). Antimicrobial efficacy of a very stable hypochlorous acid formula compared to other antiseptics used in treating wounds. in vitro study on microorganisms with or without biofilm. J. Hosp. Infect., 1–15. doi:10.1016/j.jhin.2020.01.013
Jimenez-Gonzalez, H. A., Nakagoshi-Cepeda, M. A. A., Nakagoshi-Cepeda, S. E., Urrutia-Baca, V. H., De La Garza-Ramos, M. A., Solis-Soto, J. M., et al. (2021). Antimicrobial effect of calcium hydroxide combined with electrolyzed superoxidized solution at neutral pH on Enterococcus faecalis growth. BioMed Res. Int. 2021, 6960143–6960148. doi:10.1155/2021/6960143
Jirkovská, J. (2018). “Doporučený postup péče o pacienty se syndromem diabetické nohy,” in Česká diabetologická společnost.
Jones, K. R., Fennie, K., and Lenihan, A. (2007). Evidence-based management of chronic wounds. Adv. Skin and Wound Care 20 (11), 591–600. doi:10.1097/01.ASW.0000284936.32707.8d
Jurrmann (2023). Post-Market Clinical Follow-up: Best Practices for PMCF. Johner Institute. Available at: https://blog.johner-institute.com/regulatory-affairs/post-market-clinical-follow-up-pmcf/.
Kapur, V., and Marwaha, A. K. (2011). Evaluation of effect and comparison of superoxidised solution (Oxum) vs povidone iodine (Betadine). Indian J. Surg. 73 (1), 48–53. doi:10.1007/s12262-010-0189-y
Landa-Solis, C., Gonzalez-Espinosa, D., Guzman-Soriano, B., Snyder, M., Reyes-Teran, G., Torres, K., et al. (2005). Microcyn: a novel super-oxidized water with neutral pH and disinfectant activity. J. Hosp. Infect. 61, 291–299. doi:10.1016/j.jhin.2005.04.021
Landsman, A., Blume, P. A., Jordan, D. A., Vayser, D., and Gutierrez, A. (2011). An open-label, three-arm pilot study of the safety and efficacy of topical Microcyn Rx wound care versus oral levofloxacin versus combined therapy for mild diabetic foot infections. J. Am. Podiatr. Med. Assoc. 101, 484–496. doi:10.7547/1010484
Lazzarini, P. A., Raspovic, A., Prentice, J., Commons, R. J., Fitridge, R. A., Charles, J., et al. (2023). Australian evidence-based guidelines for the prevention and management of diabetes-related foot disease: a guideline summary. Med. J. Aust. 219 (10), 485–495. doi:10.5694/mja2.52136
le Duc, Q., Breetveld, M., Middelkoop, E., Scheper, R. J., Ulrich, M. M. W., and Gibbs, S. (2007). A cytotoxic analysis of antiseptic medication on skin substitutes and autograft. Br. J. Dermatology 157, 33–40. doi:10.1111/j.1365-2133.2007.07990.x
Martinengo, L., Olsson, M., Bajpai, R., Soljak, M., Upton, Z., Schmidtchen, A., et al. (2019). Prevalence of chronic wounds in the general population: systematic review and meta-analysis of observational studies. Ann. Epidemiol. 29, 8–15. doi:10.1016/j.annepidem.2018.10.005
Martínez-De Jesús, F. R., Ramos-De la Medina, A., Remes-Troche, J. M., Armstrong, D. G., Wu, S. C., Lázaro-Martínez, J. L., et al. (2007). Efficacy and safety of neutral pH superoxidised solution in severe diabetic foot infections. Int. Wound J. 4 (4), 353–362. doi:10.1111/j.1742-481X.2007.00363.x
McLain, N. E., Moore, Z. E., and Avsar, P. (2021). Wound cleansing for treating venous leg ulcers. Cochrane Database Syst. Rev. 3 (3), CD011675. doi:10.1002/14651858.CD011675.pub2
Mena-Mendivil, E. D., Flores-Trevino, J. J., Rodríguez-Delgado, I., and de la Garza-Ramos, M. A. (2013). Antimicrobial effect of Microdacyn 60, OcOral, and sodium hypochlorite 5.25% in anaerobic bacteria. J. Pharmacogn. Phytotherapy 5, 114–119. Available at: https://api.semanticscholar.org/.
Nagoba, B., Gavkare, A., Rayate, A., Mumbre, S., Rao, A., Warad, B., et al. (2021). Role of an acidic environment in the treatment of diabetic foot infections: a review. World J. Diabetes 12 (9), 1539–1549. doi:10.4239/wjd.v12.i9.1539
National Institute for Health and Care Excellence (NICE) (2016). NICE Chronic wounds: advanced wound dressings and antimicrobial dressings. Evidence summary. Available at: www.nice.org.uk/guidance/esmpb2 (Accessed March 30, 2016).
National Institute for Health and Care Excellence (NICE) (2020). Leg ulcer infection: antimicrobial prescribing. NICE Guideline NG152. Available at: www.nice.org.uk/guidance/ng152 (Accessed February 11, 2020).
Ono, T., Yamashita, K., Murayama, T., and Sato, T. (2012). Microbicidal effect of weak acid hypochlorous solution on various microorganisms. Biocontrol Sci. 17 (3), 129–133. doi:10.4265/bio.17.129
Ortega-Pena, S., Hidalgo-González, C., Robson, M. C., and Krötzsch, E. (2017). In vitro microbicidal, anti-biofilm and cytotoxic effects of different commercial antiseptics. Int. Wound J. 14, 470–479. doi:10.1111/iwj.12625
Peters, E. J., Lipsky, B. A., Aragon-Sanchez, J., Boyko, E. J., Diggle, M., Embil, J. M., et al. (2016). Interventions in the management of infection in the foot in diabetes: a systematic review. Diabetes/metabolism Res. Rev. 32, 145–153. doi:10.1002/dmrr.2706
Peters, E. J. G., Lipsky, B. A., Berendt, A. R., Embil, J. M., Lavery, L. A., Senneville, E., et al. (2012). A systematic review of the effectiveness of interventions in the management of infection in the diabetic foot. Diabetes Metab. Res. Rev. 28 (Suppl. 1), 142–162. doi:10.1002/dmrr.2247
Peters, E. J. G., Lipsky, B. A., Senneville, É., Abbas, Z. G., Aragón-Sánchez, J., Diggle, M., et al. (2020). Interventions in the management of infection in the foot in diabetes: a systematic review. Diabetes Metab. Res. Rev. 36 (Suppl. 1), e3282. doi:10.1002/dmrr.3282
Piaggesi, A., Goretti, C., Mazzurco, S., Tascini, C., Leonildi, A., Rizzo, L., et al. (2010). A randomized controlled trial to examine the efficacy and safety of a new super-oxidized solution for the management of wide postsurgical lesions of the diabetic foot. Int. J. Low. Extrem Wounds 9 (1), 10–15. doi:10.1177/1534734610361945
Pierpont, Y. N., Dinh, T. P., Salas, R. E., Johnson, E. L., Wright, T. G., Robson, M. C., et al. (2014). Obesity and surgical wound healing: a current review. ISRN Obes. 2014, 638936. doi:10.1155/2014/638936
Pokorná, A., Pavlík, T., Bortlíček, Z., Uher, M., Kovalčíková, P., Hlostová, M., et al. (2017). Vředová onemocnění kůže a jejich vykazování v datech akutní lůžkové péče. Ústav zdravotnických informací a statistiky ČR Institut biostatistiky a analýz, Lékařská fakulta, Masarykova univerzita. Presented at Conference DRG Restart 2017 on 29th November 2017.
Rossi-Fedele, G., Poli de Figueiredo, J. A., Steier, L., and Canullo, L. (2010). Antimicrobial effect of super-oxidized water and sodium hypochlorite against Enterococcus faecalis. Endod. Pract. U. S. 7. doi:10.1590/s1678-77572010000500012
Rüttermann, M., Nink-Grebe, B., Burckhardt, M. B., and Maier-Hasselmann, A. (2013). Local treatment of chronic wounds: in patients with peripheral vascular disease, chronic venous insufficiency, and diabetes. Dtsch. Ärzteblatt Int. 110, 25–31. doi:10.3238/arztebl.2013.0025
Saeg, F., Schoenbrunner, A. R., and Janis, J. E. (2021). Evidence-based wound irrigation: separating fact from fiction. Plast. Reconstr. Surg. 148 (4), 601e–614e. doi:10.1097/PRS.0000000000008331
Sakarya, S., Ozturk, B., Gunay, N., Ertugrul, B., and Karakulak, M. (2014). Hypochlorous acid: an ideal wound care agent with powerful microbicidal, antibiofilm, and wound healing potency. Wounds 26, 342–350.
Salisbury, A.-M., and Percival, S. L. (2019). The efficacy of an electrolysed water formulation on biofilms. Adv. Exp. Med. Biol. 1214, 1–8. doi:10.1007/5584_2018_207
Savadkouhi, S. T., Maram, M. M., Bagher, M. P., Afkar, M., and Fazlyab, M. (2021). In vitro activity of superoxide water on viability of Enterococcus faecalis biofilm on root canal wall. Iran. Endod. J. 16, 189–192. doi:10.22037/iej.v16i3.32503
Schultz, G. S., Sibbald, R. G., Falanga, V., Ayello, E. A., Dowsett, C., Harding, K., et al. (2003). Wound bed preparation: a systematic approach to wound management. Wound Repair Regen. 11 (Suppl. 1), S1–S28. doi:10.1046/j.1524-475x.11.s2.1.x
Schwarzer, S., James, G. A., Goeres, D., Bjarnsholt, T., Vickery, K., Percival, S., et al. (2019). The efficacy of topical agents used in wounds for managing chronic biofilm infections: a systematic review. J. Infect. 80, 261–270. doi:10.1016/j.jinf.2019.12.017
Senneville, É., Albalawi, Z., van Asten, S. A., Abbas, Z. G., Allison, G., Aragón-Sánchez, J., et al. (2024). IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Diabetes Metab. Res. Rev. 40 (3), e3687. doi:10.1002/dmrr.3687
Severing, A.-L., Rembe, J.-D., Koester, V., and Stuermer, E. K. (2019). Safety and efficacy profiles of different commercial sodium hypochlorite/hypochlorous acid solutions (NaClO/HClO): antimicrobial efficacy, cytotoxic impact and physicochemical parameters in vitro. J. Antimicrob. Chemother. 1, 365–372. doi:10.1093/jac/dky432
Stephenson, J. (2022). Study designs in wound care. WCET J. - Portuguese Ed. 42. doi:10.33235/wcet.42.1.12-15
Thorn, R. M. S., Lee, S. W. H., Robinson, G. M., and Greenman, J. (2011). Electrochemically activated solutions: evidence for antimicrobial efficacy and applications in healthcare environments. Eur. J. Clin. Microbiol. and Infect. Dis. 23. doi:10.1007/s10096-011-1369-9
Torres-Capetillo, E., Carrillo-Fuentevilla, R., De la Garza-Ramos, M. A., and Hernández, R. M. (2013). Antimicrobial efficacy of neutral super-oxidized electrolyzed gel versus chlorhexidine digluconate 0.12% in biofilm formation on orthodontic miniimplants: an in vitro study. J. Pharmacogn. Phytotherapy 5, 64–71.
UZIS (2018). Zdravotnictví ČR: stručný přehled činnosti oboru diabetologie a endokrinologie za období 2007–2017. NZIS Report č. K/1 (08/2018).
Walia, B. S., Pankaj, D., Navjot, S., Sanjeev, S., and Babu Lal Sunkaria, M. S. (2021). Study of efficacy of superoxidised solution and gel (microdacyn) in the treatment of diabetic foot ulcer. Eur. J. Mol. and Clin. Med. 08 (04).
Wilkins, R. G., and Unverdorben, M. (2013). Wound cleaning and wound healing: a concise review. Adv. Skin. Wound Care 26 (4), 160–163. doi:10.1097/01.ASW.0000428861.26671.41
Keywords: neutral electrolyzed water, superoxidized solution, wound irrigation, chronic wound, hypochlorous acid, venous leg ulcer, diabetic foot, pressure ulcer
Citation: Valdová V, Štěpánová V and Lapčíková L (2025) The safety and efficacy of neutral electrolyzed water solution for wound irrigation: post-market clinical follow-up study. Front. Drug Saf. Regul. 4:1402684. doi: 10.3389/fdsfr.2024.1402684
Received: 18 March 2024; Accepted: 23 December 2024;
Published: 16 January 2025.
Edited by:
Alessandro Mugelli, University of Florence, ItalyReviewed by:
Bidita Khandelwal, Sikkim Manipal University, IndiaElisabetta Bigagli, University of Florence, Italy
Copyright © 2025 Valdová, Štěpánová and Lapčíková. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Veronika Valdová, dmVyb25pa2F2QGVyZXRlLXpvZS5jb20=