
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Drug Saf. Regul., 07 November 2023
Sec. Respiratory Drug Safety
Volume 3 - 2023 | https://doi.org/10.3389/fdsfr.2023.1291471
This article is part of the Research TopicTreatment of Comorbidities of Asthma and Its SafetyView all 5 articles
 Barbara Bonnesen1
Barbara Bonnesen1 Jens-Ulrik S. Jensen1,2
Jens-Ulrik S. Jensen1,2 Alexander G. Mathioudakis3,4
Alexander G. Mathioudakis3,4 Alexandru Corlateanu5
Alexandru Corlateanu5 Pradeesh Sivapalan1,2*
Pradeesh Sivapalan1,2*Asthma is a highly heterogenous disease which researchers over time have attempted to classify into different phenotypes and endotypes to improve diagnosis, prognosis and treatment. Earlier classifications based on reaction to environmental allergens, age, sex and lung function have evolved, and today, the use of precision medicine guided by biomarkers offers new perspectives on asthma management. Identifying biomarkers that may reveal the underlying pathophysiology of the disease will help to select the patients who will benefit most from specific treatments. This review explores the classification of asthma phenotypes and focuses on the most recent advances in using biomarkers to guide treatment.
Asthma is a chronic disease of the lower airways characterized by wheezing and airflow obstruction (Schoettler and Strek, 2020). It is estimated that 300 million people worldwide have asthma, placing considerable burdens on healthcare systems and economy (Loftus and Wise, 2015). Presently, the management of asthma revolves around symptom control, exacerbation prevention, and averting long-term complications. For mild to moderate asthma, standard treatment mainly consists of inhaled corticosteroids (ICS), long-acting beta-agonists (LABAs) and leukotriene antagonists, as recommended by the Global Initiative for Asthma (GINA) guidelines (Asthma, 2022).
According to GINA guidelines 3.7% of asthma patients have severe asthma, and ICS and LABA therapy has been proven insufficient (Asthma, 2022). In these cases, biologic treatment with monoclonal antibodies targeting specific cytokine pathway may be considered for selected phenotypes (Castillo et al., 2017), or additional treatment may encompass long-acting muscarinic-antagonists (LAMAs) and in some cases, azithromycin, an antibiotic known for its potential anti-inflammatory properties and impact on airway infections (Asthma, 2022). It is essential to recognize that not all asthma phenotypes respond favourably to the currently available treatment strategies, including biologic treatments, LAMA and azithromycin. Therefore, focus has shifted towards personalized medicine, highlighting the significance of biomarkers in directing the allocation of more costly treatment alternatives to patients that will benefit most from them.
This review will explore the phenotyping of asthma and focus on the biomarkers that may help guide treatment for patients with severe, uncontrolled asthma, Table 1.
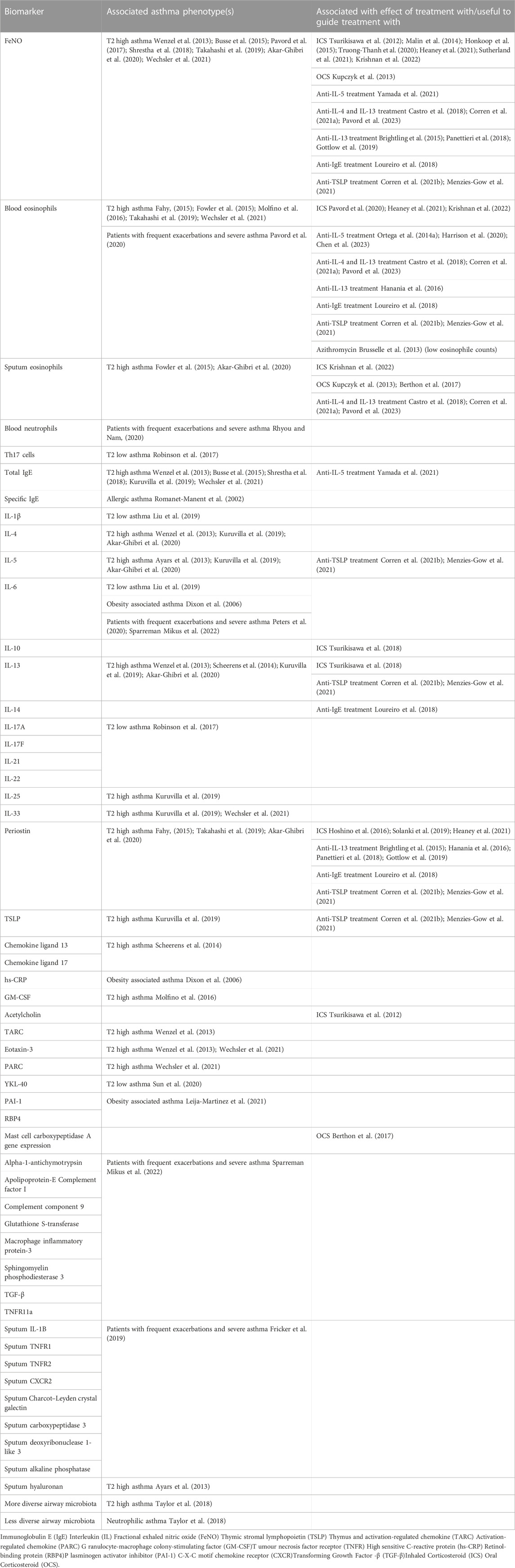
Table 1. Overview of biomarkers in different asthma phenotypes and association to treatment.
Asthma has been divided into allergic and non-allergic phenotypes. Allergic or atopic asthma is characterized by an earlier onset, and the reactions towards environmental allergens contribute to the development of symptoms and airway inflammation (Schatz and Rosenwasser, 2014; Akar-Ghibri et al., 2020). It can be diagnosed by relevant response to exposure to various allergens combined with antigen-specific tests with increased immunoglobulin E (IgE) (Romanet-Manent et al., 2002). Allergic asthma is more frequently associated with atopic dermatitis or eczema, conjunctivitis and possibly rhinitis (Romanet-Manent et al., 2002; Schatz and Rosenwasser, 2014; Akar-Ghibri et al., 2020), and it is associated with increased T2 inflammation and higher levels of cytokines such as interleukin (IL)-4, IL-5 and IL-13. T2 inflammation is also associated with increased levels of blood and sputum eosinophils, fractional exhaled nitric oxide (FeNO) and the lesser known periostin (Akar-Ghibri et al., 2020). Non-allergic or type 2 low asthma is a heterogenous phenotype, without clear cut definition, less well-characterised biomarkers and fewer, less effective treatment options.
Stratification of asthma into phenotypes can be based on clinical features, genetics, proteomics and metabolomics, as well as by biomarkers. The area is complex and the feasibility of obtaining sample in a clinical everyday setting varies, however proteomics (Riccio et al., 2020; Suzuki et al., 2021) and metabolomics (Maniscalco et al., 2018; Kachroo et al., 2021) definitely play a huge role in future asthma phenotyping, and a study even points to a role of lipidomic profiling (Brandsma et al., 2023).
Microbiota composition may also vary among patients with different asthma phenotypes. One study examined 167 participants with various (eosinophilic, neutrophilic, paucigranulocytic, or mixed) asthma phenotypes and found that airway microbiology was less diverse and more dissimilar in participants with neutrophilic asthma than in those who had eosinophilic asthma (Taylor et al., 2018).
Surprisingly, the pathophysiological asthma phenotypes may not be lifelong, or even long term. In a cohort study of 169 patients, asthma phenotype clusters were defined by physiological variables (i.e., lung function, reversibility and age of onset of the disease) or by biomarkers (i.e., FeNO levels and differential counts in induced sputum). Patients were followed up after 1 year, and at this time, the cluster allocation of a large proportion of the patients had changed (in 24% of patients stratified by physiological variables and 42% of patients stratified by FeNO levels and differential counts in induced sputum). The variability of the phenotypes was not influenced by change in oral or inhaled corticosteroid dose, nor by the number of exacerbations (Kupczyk et al., 2014).
T2 high asthma is characterized by reduced lung function, poor asthma control, increased IgE levels, increased responsiveness to ICS treatment and persistent eosinophilic inflammation mediated by cytokines such as IL-4, IL-5 and IL-13. The inflammation is aggravated by activation of thymic stromal lymphopoietin (TSLP), IL-25 and IL-33 as a reaction to microbes and allergens. This activates T cells, B cells and innate lymphoid cells, which in turn produce the cytokines involved in T2 high asthma. (Kuruvilla et al., 2019).
Patients with T2 high asthma are frequently atopic, more likely to be young at diagnosis and less likely to have a high body mass index (BMI). They frequently exhibited high bronchodilator reversibility (≥20%) in a retrospective analysis of 698 patients with poorly controlled asthma. (Busse et al., 2015; Shrestha et al., 2018).
FeNO is an easily measured indicator of T2 airway inflammation because it is produced by nitric oxide synthase in the airway epithelium, which is induced by IL-13 (Kuo et al., 2019). The U-BIOPRED study on 610 patients with asthma found that increased levels of FeNO could predict and classify T2 high asthma (Busse et al., 2015; Pavord et al., 2017; Shrestha et al., 2018), and high FeNO levels have been linked to asthma attacks (Couillard et al., 2021), however FeNO did not correlate with sputum eosinophilia in a study on 328 patients with asthma (Hastie et al., 2013).
The T2 high-associated increase in FeNO levels could be decreased by combined inhibition of IL-4 and IL-13 signalling in 104 patients with persistent, moderate-to-severe asthma. The decrease in FeNO correlated well with an improvement in Forced Expired Volume in the first second (FEV1) (Wenzel et al., 2013). Inhibition of the upstream alarmin IL-33 using a monoclonal antibody also reduced FeNO levels in 296 patients with moderate-to-severe asthma (Wechsler et al., 2021).
High IgE levels may also be associated to T2 high asthma (Busse et al., 2015; Shrestha et al., 2018), and like FeNO the T2 high-associated increased total IgE levels decreased during inhibition of alarmin IL-33 (Wechsler et al., 2021), IL-13 (Scheerens et al., 2014) and dual IL-4 and IL-13 signalling (Wenzel et al., 2013).
Blood eosinophilia and sputum eosinophilia are intrinsic to T2 high asthma, but do not correlate in all studies; in a study based on data collected from a clinical database of 163 patients attending the Manchester Severe Asthma Service between 2006 and 2013 found that using a cut-off of 0.45 × 109 cells/L for blood eosinophilia could predict airway eosinophilia in patients with severe asthma (Fowler et al., 2015), and another study found that both blood eosinophil counts and serum periostin levels were good indicators of T2 high asthma and could help to guide treatment with personalized medicine (Fahy, 2015). However, in the study on 328 patients with asthma with no correlation between FeNO and sputum eosinophiles, there was also no correlation between blood eosinophil counts and sputum eosinophil levels (Hastie et al., 2013). Inhibition of IL-13 yielded no reduction in airway eosinophils in 64 patients with uncontrolled asthma (Austin et al., 2020), however inhibition of alarmin IL-33 reduced blood eosinophil counts in 296 patients with moderate-to-severe asthma (Wechsler et al., 2021).
Periostin is an extracellular matrix protein with an upregulated expression in airway epithelial cells and fibroblasts after activation by IL-13 and alarmin IL-33 (Wechsler et al., 2021) in patients with some types of asthma and allergic inflammation, but also in pulmonary fibrosis (Murata et al., 2018; Nukui et al., 2019; Katoh et al., 2020; Matsumoto, 2020). It may be linked to T2 high inflammation and correlate to type 2 asthma markers such as FeNO and blood eosinophils (Takahashi et al., 2019) but not necessarily sputum eosinophils (Cianchetti et al., 2019), and it may be suppressed by ICS (Solanki et al., 2019). In the context of activation in pulmonary fibrosis, periostin expression is also associated to persistent airway obstruction (FEV1/vital capacity [VC] < 88%) (Cianchetti et al., 2019).
Many other potential biomarkers have been investigated in RCTs involving patients with T2 high asthma. Many proteins are activated or inhibited by interleukins associated with type 2 asthma. For example, sputum hyaluronan (a matrix glycosaminoglycan) levels may be decreased by inhibiting IL-5 (Ayars et al., 2013), inhibiting IL-13 signalling decreases the levels of chemokine ligands 13 and 17 by approximately 25% (Scheerens et al., 2014), and inhibiting IL-4 and IL-13 signalling lowers thymus and activation-regulated chemokine (TARC) and eotaxin-3 levels (Wenzel et al., 2013). Inhibiting IL-33 reduced plasma eotaxin-3 as well as serum pulmonary and activation-regulated chemokine (PARC) levels (Wechsler et al., 2021). Higher levels of transforming growth factor (TGF)-beta, and lower levels of granulocyte-macrophage colony-stimulating factor (GM-CSF) and basic fibroblast growth factor (bFGF) was associated to persistent airway obstruction (FEV1/VC < 88%) in asthma (Cianchetti et al., 2019), but it is unknown, if they can predict it. An RCT examined the effect of inhibiting GM-CSF, which benefitted especially patients with blood eosinophils >300/mL or FEV1 reversibility ≥20% (Molfino et al., 2016). All these possible future biomarkers need further studies before clinical use.
Other proteins seem less promising as biomarkers; though OX40/OX40L interaction contributes to the allergic T cell response and helps sustain memory T cells, inhibition of the OX40/OX40L had no effect on airway hyperresponsiveness or blood eosinophil counts (Gauvreau et al., 2014a). Similarly, no association between IL-8 and RANTES levels and persistent airway obstruction was observed (Cianchetti et al., 2019), and hence neither of these are promising biomarkers to pursue.
Aspirin-induced asthma may pose a challenge for only 0.5% of the population, however patients with aspirin-induced asthma were more likely to take sick leave, require emergency treatment for asthma or experience lower respiratory symptoms than patients with aspirin-tolerant asthma in a Swedish questionnaire of 30,000 randomly selected subjects. Obesity is a strong risk factor for aspirin-induced asthma, traditionally making it challenging to treat, (Eriksson et al., 2015), however a recommended treatment is aspirin desensitization, though it may be associated with adverse reactions. A tiny RCT examined treatment with IgE inhibition prior to desensitization with possible effect, however it included only 11 participants (Lang et al., 2018). Hence, IgE signalling may be involved in aspirin-exacerbated respiratory disease and may have a role to play as a biomarker for prophylactic treatment before desensitization therapy.
T2 low asthma is a polymorphic entity characterized by severe, uncontrolled asthma in absence of T2 inflammation. Patients with type 2 low asthma had more asthma primary care attendances, were more likely to have a previous admission to an ICU and to be receiving maintenance oral corticosteroids in a study on 301 patients (McDowell et al., 2022).
There are biomarkers useful for various phenotypes of non-eosinophilic and T2 low asthma; Th17 cells may be responsible for associated with a severe asthma phenotype, which is characterized by neutrophilic inflammation and interleukins such as IL-17A, IL-17F, IL-21 and IL-22 (Robinson et al., 2017). Neutrophilic inflammation may also be associated with YKL-40 in serum and in lung tissue, as it is secreted by neutrophils, and correlates with increased severity of asthma (Sun et al., 2020), and with cytokines such as IL-1β and IL-6 (Liu et al., 2019).
An analysis based on the AMAZES RCT with 142 patients, showed that in the sputum of patients with neutrophilic asthma tumour necrosis factor receptor (TNFR)1 and TNFR2 were significantly increased with a dose-response relation to more severe neutrophilic asthma and correlated with poorer lung function, poorer asthma control, and increasing age (Niessen et al., 2021).
Asthma symptoms such as wheezing and shortness of breath are more prevalent among people with elevated BMI in a study involving 85,437 Danes using Mendelian randomization (Colak et al., 2016) and a cross-sectional survey of 15,454 Europeans (Jarvis et al., 2002). The degree of obesity has been shown to be negatively correlated with lung function (Huang et al., 2012), and a small RCT with 90 patients showed that abdominal adiposity was associated with poorer asthma control, even after controlling for BMI (Lv et al., 2014). Therefore, asthma control and asthmatic symptoms may be associated with both obesity and distribution of adiposity.
Obesity has been shown to be associated with elevated levels of pro-inflammatory cytokines; IL-6 and highly sensitive assays for serum C-reactive protein (hs-CRP) from <2 to >7 mg/mL (Dixon et al., 2006). A study on asthma in adolescents investigated retinol-binding protein (RBP4) and plasminogen activator inhibitor (PAI-1) and found that RBP4 was useful in predicting non-allergic asthma in adolescents with obesity (Leija-Martinez et al., 2021). Therefore, RBP4 may be useful in identifying obesity-related asthma, differentiating it from other forms of asthma. However, further research is needed.
T2 high symptoms and biomarkers have also been investigated in obese patients with suspected T2 high asthma. Obesity was not associated with hayfever or nasal allergies, or with levels of IgE to house dust mites, grass, or cats, or with total IgE levels in the cross-sectional survey of 15,454 Europeans (Jarvis et al., 2002). Similarly, sinonasal disease was not associated with obesity in an RCT of 236 patients with asthma (Kanagalingam et al.).
A simple history-based model extended with spirometry could identify patients who developed asthma exacerbations in a primary care-based cohort analysis of 611 patients. The additional value of FeNO was modest; however, the patients in this study were not phenotyped, which may have masked a potential predictive role of FeNO among patients with T2 high disease (Loymans et al., 2016). Another primary care based RCT, also with patients who were not phenotyped, studied the risk of exacerbations among 304 patients followed for 12 months. This study highlighted some parameters that may be used to quantify future risk: female gender (OR, 2.34), a severe exacerbation in the previous year (OR, 3.17), an increase of half a point on the baseline Asthma Control Questionnaire (ACQ) (OR, 1.87), and an additional litre in FEV1 (OR, 0.63); however, there was no association with FeNO levels (Boer et al., 2019).
Initial studies on asthma showed that the risk of a severe asthma event increased in patients who were undergoing treatment with short-acting beta-agonists (SABAs) alone. However, in an RCT with 675 patients who were followed for 52 weeks, the proportion of patients undergoing treatment with SABAs alone who had a severe exacerbation increased progressively with increasing blood eosinophil count (Pavord et al., 2020). Among patients receiving moderate dose ICS, exacerbations were associated with lower eosinophil counts in blood and sputum and with higher neutrophil counts in sputum (Rhyou and Nam, 2020). Hence, blood and sputum eosinophil counts may be good biomarkers for ICS treatment suitability and for quantifying the risk of exacerbations without ICS treatment, whereas sputum neutrophils may be a marker for a high risk of exacerbations despite ICS treatment.
One study investigated potential sputum biomarkers in a cohort of 142 patients from the AMAZES RCT with asthmatic symptoms despite ICS and LABA treatment. It defined sputum Charcot–Leyden crystal galectin, carboxypeptidase 3, deoxyribonuclease 1-like 3, alkaline phosphatase, C-X-C motif chemokine receptor (CXCR)2, and IL-1B as possible predictors of an exacerbation. (Fricker et al., 2019). Although CXCR2 may predict exacerbations among symptomatic patients despite ICS and LABA treatment, an antagonist of CXCR2 (AZD5069) was not a promising target for therapy in a phase III RCT; among 640 patients of whom 478 received AZD5069, there was no effect on the primary endpoint of frequency of severe exacerbations (O'Byrne et al., 2016).
Another RCT, involving 147 patients, investigated the effect of inhaled interferon (IFN)-beta as a treatment for asthma exacerbations following cold symptoms to assess the risk of exacerbations after a viral infection. The study found that inhaled IFN-beta had no effect on ACQ, but there was an effect on secondary endpoints including peak expiratory flow recovery, the need for additional treatment, and boosted innate immunity as assessed by blood and sputum biomarkers (Djukanovic et al., 2014). A study of 406 asthmatic patients found that IL-6 levels were correlated with frequent exacerbations, whereas blood eosinophil counts were not (Peters et al., 2020).
A biomarker study on 142 patients with mild-moderate and severe asthma, showed that elevated levels of alpha-1-antichymotrypsin, apolipoprotein-E, complement component 9, complement factor I, macrophage inflammatory protein-3, IL-6, sphingomyelin phosphodiesterase 3, TNF receptor superfamily member 11a, TGF-β and glutathione S-transferase was associated to more severe asthma. Treatment with oral corticosteroids decreased the expression of most, but not all of these biomarkers (Sparreman Mikus et al., 2022).
Another method for identifying severe asthma phenotypes involves studying the response to different treatments and then retrospectively determining the characteristics of patients’ asthma. One recent study used responsiveness to anti IL-5 medication as an indicator of different phenotypes of severe eosinophilic asthma by monitoring changes in FEV1 (Yamada et al., 2021). This study identified five phenotypes based on differences in the FEV1 response to medication and the Asthma Control Test (ACT) response to medication. Further, there were differences in the quantities of type 2 inflammation markers, age of onset, smoking exposure and BMI. The most responsive cluster had a moderate increase in IgE and FeNO levels relative to blood eosinophils and had less exposure to smoking. The moderately responsive clusters had a greater degree of T2 inflammation, compared with the non-responsive clusters.
The identification of different asthma phenotypes or endotypes can contribute to relevant treatment of patients as they provide an option for precision medicine targeted towards specific cellular signalling pathways based on specific biomarkers. Such medicine includes ICS, antibiotics, as well as biological treatment using monoclonal antibodies targeted against cellular signalling pathways based involved in the pathophysiology of asthma, for example, cytokines involved in Th2 inflammation in patients with asthma.
The effect of ICS may be predicted using patient clinical characteristics and biomarkers. Low and normal BMI predicted a therapeutic effect of ICS in a post hoc analysis of 894 patients with moderate asthma in pooled data from four double-blind, placebo controlled RCTs. Patients were treated with beclomethasone; however, the effect of beclomethasone decreased with increasing BMI, and was only significant among patients with low or normal BMI (Peters-Golden et al., 2006).
Sputum and blood eosinophiles as well as FeNO predicted response to ICS treatment in an RCT on 237 patients with uncontrolled mild-moderate persistent asthma, (Krishnan et al., 2022). In the BASALT RCT FeNO based adjustment of ICS treatment yielded no significant differences in time to treatment failure. This RCT from 2012 examined 342 patients allocated to three strategies for optimising low-dose ICS therapy: physician assessment-based adjustment, FeNO based adjustment, and symptom-based adjustment for 9 months follow-up with adjustments every 6 weeks for FeNO and physician assessment-based treatment. (Calhoun et al., 2012). One weakness of the BASALT RCT was that the patients were not included by or divided into groups based on phenotypes, which may have masked the benefits of using FeNO as a biomarker for ICS treatment. In a retrospective cohort study of 153 non-smoking, steroid-naïve patients initial FeNO level of ≥25 ppb was associated to an improvement in ACQ during treatment with 500 µg beclomethasone for 6 weeks (Malin et al., 2014). Another cohort study has document that FeNO often decreases with ICS treatment; in a cohort study of 102 Tamilian patients, FeNO decreased from 91–103 ppb to 75–90 ppb over 8 weeks of treatment with ICS (Neelamegan et al., 2016). Hence, despite it frequent use in clinical practise, the role of FeNO as a biomarker is not clear-cut.
In a cohort study of 40 patients with mild-to-moderate asthma, serum periostin decreased from 90 to 59 ng/mL during 4 weeks of ICS treatment, which correlated with an increase in peak expiratory flow rate (68 L/min) and in Asthma QOL (Solanki et al., 2019). Similarly, 42 healthy control subjects and 20 previously ICS naïve patients with asthma who were treated with ICS exhibited decreases in serum periostin, correlating with increased FEV1%, decreased sputum eosinophils and decreased bronchial wall area (Hoshino et al., 2016). Hence, periostin may have a potential as a biomarker for ICS treatment efficacy, at least in some asthma phenotypes. However, these are preliminary data.
In a very small study of 23 patients with steroid resistant asthma, IL-17A and IFN-γ were elevated in comparison to patients with steroid sensitive asthma (Chambers et al., 2015). However, whether these interleukins would be suitable biomarkers remains unclear.
In conclusion, ICS treatment may be particularly beneficial for patients with asthma who have low or normal BMI, elevated sputum eosinophils and/or elevated periostin, and possibly elevated FeNO levels.
Corticosteroid dose may be reduced in accordance with different strategies for monitoring asthma control and treatment efficacy; a lower daily ICS dose (375 ± 203 vs. 424 ± 221 mcg) was achieved at 9 months follow-up among patients whose treatment was guided by Global Initiative for Asthma (GINA) guidelines and FeNO levels, compared with patients whose treatment was guided by GINA alone in an RCT of 176 symptomatic patients with asthma (Truong-Thanh et al., 2020). Similarly, a strategy involving treatment guided by ACQ and FeNO yielded improved asthma control and a lower accumulated dose of asthma medication but not increased quality of life, compared with treatment guided by ACQ alone in a nonblind cluster-randomized trial of 611 patients in primary care (Honkoop et al., 2015). Finally, in a Japanese cohort study of 90 patients with moderate or severe asthma, a successful reduction in ICS dose of 50% was achieved guided by FeNO levels (Tsurikisawa et al., 2012). However, one weakness common to these three studies is that the patients were not phenotyped before study entry. Different asthma phenotypes may generate different results, and different monitoring algorithms may be more relevant for particular groups of patients.
In the LASST RCT, a large proportion of the 447 patients had T2 high disease. The patients were treated with moderate doses of ICS, subjected to a step-down algorithm, and followed for 56 weeks. During the trial, FeNO was measured at 6-week intervals, as well as other biomarkers, including levels of multiallergen IgE. None of these biomarkers, including FeNO, predicted loss of asthma control during the ICS step-down process (Bose et al., 2020).
To investigate patients with T2 low asthma, an RCT examined 180 adults with suspected asthma and FeNO ≤27 ppb. In this study, a daily dose of 400 µg budesonide had no effect on symptom control or on FEV1 (Sutherland et al., 2021). Hence, in patients with asthma symptoms and low FeNO levels, ICS may have limited benefit and dose may be decreased with little risk of lowering symptom control or quality of life.
Using a more extensive algorithm that included blood eosinophil counts, serum periostin and FeNO levels also led to a greater decrease in corticosteroid dose than treatment guided by asthma symptoms, lung function and recent exacerbation history. This was achieved without a drop in asthma control or quality of life in a single-blind, parallel group RCT of 301 patients with severe asthma, who were treated based on the algorithm for 48 weeks. In this study, an inclusion criterion was FeNO <45 ppb (Heaney et al., 2021). Therefore surprisingly, a T2 high-based algorithm was effective in predicting safe ICS reduction in patients with T2 low asthma. However, in a post hoc analysis of this trial the decrease in corticosteroid dose was only seen in women (Eastwood et al., 2023).
Blood eosinophil counts ≥0.3 × 109/L were able to predict an effect of ICS in an open-label RCT of 675 patients with mild asthma. Additionally, in this trial, 200 µg of budesonide twice a day was not more effective than SABA alone in preventing exacerbations among patients with blood eosinophil counts <0.15 × 109/L during a 52-week follow-up period (Pavord et al., 2020).
In a Japanese cohort study, low serum IL-33 levels, low peak expiratory flow variability over 1 week, childhood onset of asthma (at age <10 years), and high serum IL-10 levels were associated with a safe reduction in ICS dose. In this cohort study, 223 patients underwent a 50% reduction in ICS dose over 36 months and were monitored for asthma control (Tsurikisawa et al., 2018). In another Japanese cohort of 90 patients with a similar setup, the predictors of a safe 50% reduction in ICS dose were serum acetylcholine levels, FeNO levels, length of time with no clinical symptoms before dose reduction, as well as higher FEV1% (Tsurikisawa et al., 2012). Hence, many of these parameters are potential clinical markers and biomarkers for ICS treatment suitability and/or safe ICS dose reduction. However, appropriate trials are needed before they can be implemented clinically.
Finally clinical parameters such as poor adherence, chronic upper airway complications and, to a lesser degree, sleep disorders and psychiatric comorbidities, such as depression, anxiety and somatoform disorders have been associated with failed ICS dose reduction in a cohort of 222 well-controlled asthma patients receiving ICS or ICS/LABA (Saito et al., 2017).
In conclusion, ICS dose may be reduced safely in some patients with low FeNO levels, blood eosinophil counts <0.15 × 109/L, low IL-33 levels, high IL-10 levels, high serum acetylcholine, low peak expiratory flow variability, and/or a long period of time with no clinical symptoms.
An RCT investigated the effect of treatment with 50 mg prednisolone for 10 days in patients with stable asthma. Patients with higher levels of sputum and blood eosinophils, higher levels of mast cell carboxypeptidase A gene expression, or poorer lung function were more likely to have a beneficial response to treatment with oral corticosteroids (Berthon et al., 2017).
Another RCT examined treatment with 0.5 mg/kg prednisolone for 2 weeks in 84 patients with severe asthma and 62 patients with mild-to-moderate asthma. The patients who experienced beneficial effects from treatment with oral corticosteroids had higher FeNO levels, higher levels of sputum eosinophils, lower FEV1% and lower quality of life (Kupczyk et al., 2013).
Hence, patients with T2 high asthma or with poor lung function may experience greater benefits from short-term, oral corticosteroid treatment than patients with T2 low asthma.
Montelukast is an inhibitor of [3H]-leukotriene D4-receptor specific binding (Schoors et al., 1995). In a post hoc analysis with pooled data from four RCTs including 3,073 patients with moderate asthma montelukast was as effective for patients with obesity as it was for patients with normal BMI. In contrast, the effectiveness of beclomethasone decreased with increasing BMI (Peters-Golden et al., 2006). Hence, montelukast might be a more attractive treatment option for patients with asthma and obesity. Additionally, montelukast might benefit patients with asthma and chronic rhinosinusitis with nasal polyps in combination with nasal corticosteroid treatment and surgery (Nonaka et al., 2010), however there is no data on the predictive value of nasal involvement in treatment of asthma with montelukast.
Roflumilast is an oral, once-daily phosphodiesterase 4 inhibitor that was developed to treat chronic obstructive pulmonary disease (COPD) and asthma. It decreases the levels of tumour necrosis factor (TNF)-alpha (Timmer et al., 2002).
A meta-analysis of evidence from eight placebo-controlled, double-blind phase I–III studies with a total of 197 patients examined the effect of roflumilast, compared to placebo. In all studies, the patients had asthma and the required pre-bronchodilator FEV1% was at least 50%; in five of the eight studies, and in the remaining the required pre-bronchodilator FEV1% was ≥70%. The meta-analysis found that roflumilast attenuated early and late allergen-induced bronchoconstriction and reduced FeNO levels, sputum eosinophil and neutrophil counts, and serum TNF-alpha and urinary leukotriene E4 levels (Bardin et al., 2015). An effect of Roflumilast on FEV1 was seen in a large noninferiority RCT of 499 patients with persistent asthma, in which roflumilast improved FEV1% by 12%. This was similar to the effect of ICS, which increased FEV1 by 14%. However, in the trial, the patients had an FEV1% of 50%–85%, indicating a potentially chronic or remodelling component to their obstructive disease (B et al., 2006). A small RCT examined combined treatment with roflumilast and montelukast and found a possible additive effect in FEV1% improvement, patient-reported outcomes, and a further reduction in urinary leukotriene E4 levels (Bateman et al., 2016).
Hence, roflumilast may have a role among asthmatics with chronically decreased FEV1.
Anti-IL-5 treatment by specific blocking antibodies is available as benralizumab, mepolizumab and reslizumab. This treatment leads to depletion of eosinophils and reduction of eosinophilic inflammation (Brusselle and Koppelman, 2022).
Mepolizumab reduces exacerbation rates and the need for oral corticosteroids, and it improves asthma control, quality of life and lung function in patients with severe asthma and elevated blood eosinophils (≥300 cells/µL) (Ortega H. G. et al., 2014; Harrison et al., 2020). It also reduces blood eosinophil counts (Ortega H. G. et al., 2014). The DREAM RCT showed that the effects of mepolizumab were enhanced in patients with elevated blood eosinophils, and in those with higher airway reversibility (Ortega H. et al., 2014), and post hoc analyses of data from the DREAM and MENSA RCTs showed that the exacerbation rate reduction with mepolizumab increased progressively from 52% in patients with blood eosinophil count ≥150 cells/µL to 70% in patients with blood eosinophil count ≥500 cells/µL (Ortega et al., 2016). Other key predictors for treatment benefit for severe exacerbations included exacerbation history, baseline ACQ5 score and age, and those for symptom control included blood eosinophil count and presence of chronic rhinosinusitis with nasal polyps, which also benefitted from the treatment (Chen et al., 2023; Chupp et al., 2023; Liu et al., 2023). In the MAPLE trial on 27 patients treated with mepolizumab, addition of oral corticosteroids had no significant effect on symptoms or quality of life, but they did still improve small-airway obstruction and reduce T2 biomarkers (Yang et al., 2022). Surprisingly, among patients with high airway reversibility, a higher BMI also correlated with increased benefits of mepolizumab treatment (Ortega H. et al., 2014).
Similarly, trials on reslizumab showed reduced exacerbation rates in patients with high eosinophilia and poorly controlled, moderate-to-severe asthma (Castro et al., 2015). In addition, chronic rhinosinusitis with nasal polyps was also associated with a high responsive to anti-IL-5 treatment with reslizumab (Weinstein et al., 2019).
Finally, studies that used benralizumab to treat uncontrolled eosinophilic asthma showed reduced exacerbation rates and increased FEV1 (FitzGerald et al., 2016; Park et al., 2016). Sera from patients in phase I and IIa studies were analysed before and after treatment with benralizumab, and these analyses showed that benralizumab reduced blood eosinophil counts and serum eosinophil-derived neurotoxin, as well as eosinophil cationic protein relative to baseline. No changes were observed in TNF or IFN-γ levels, whereas IL-5, eotaxin/CCL11, and eotaxin-2/CCL24 levels increased (Pham et al., 2016). Likewise, benralizumab, exhibits a notable positive effect on chronic rhinosinusitis with nasal polyps (Tversky et al., 2021; Bachert et al., 2022).
Hence, blocking the IL-5 pathway may be a good treatment option for patients with asthma and elevated blood eosinophils when ICS does not control the disease. Other biomarkers may also be used, but blood eosinophils are easy to measure in clinical practice.
IL-13 is a central mediator of allergic asthma. IL-13 is released along with IL-4 by Th2 cells in response to allergens and leads to IgE isotype switching, airway hyperresponsiveness, recruitment of eosinophils, macrophage activation, increased permeability of the airway epithelium and increased mucus production (Ingram and Kraft, 2012). IL-4 is a part of the same pathway and increases airway inflammation via isotype switching of B-cells and allergen sensitization (Busse, 2019).
Dupilumab is a monoclonal antibody that binds to the IL-4 receptor, blocking IL-4 and IL-13 signalling. Dupilumab lowered total IgE and FeNO, but not blood eosinophile levels in 104 patients with persistent, moderate-to-severe T2 high asthma with blood eosinophils ≥300 cells/µL or sputum eosinophils ≥3%. The decrease in FeNO levels induced correlated to improvement in FEV1. (Wenzel et al., 2013). Dupilumab also significantly reduced severe exacerbations and improved FEV1 and asthma control in the QUEST trial on patients with type 2 high asthma with elevated FeNO, blood eosinophils ≥300 cells/µL or sputum eosinophils ≥3% (Castro et al., 2018; Corren et al., 2021a; Pavord et al., 2023). The effects of dupilumab were enhanced in patients with concomitant chronic rhinosinusitis (Busse et al., 2020; Maspero et al., 2020) and among patients with persisting airway obstruction (Hanania et al., 2023). Hence, the phenotype for which dupilumab is a suitable treatment option has been examined thoroughly. After 52-week of treatment, dupilumab decreased FeNO levels, blood eosinophils, total IgE and TARC levels in an RCT on 1,902 patients (Busse et al., 2020; Maspero et al., 2020).
Lebrikizumab is an anti-IL-13 monoclonal antibody, which has been examined in two RCTs. The LAVOLTA I and II trials each continued for a total of 52 weeks and included 1,081 and 1,067 patients, respectively. Similar to dupilumab, lebrikizumab reduced exacerbation rates and improved FEV1 in patients with uncontrolled asthma. In particular, patients with high concentrations of type 2 biomarkers, such as serum periostin ≥50 ng/mL or blood eosinophils ≥300 cells/µL, benefitted from treatment with lebrikizumab (Hanania et al., 2016), just as with dupilumab.
Tralokinumab is another anti-IL-13 monoclonal antibody that was used to treat patients with severe, uncontrolled asthma in two phase III RCTs, STRATOS 1 and 2. Tralokinumab reduced asthma exacerbations in participants with severe asthma and FeNO ≥37 ppb in STRATOS 1, but not STRATOS 2. FeNO and periostin were the only biomarkers that could predict the effect of tralokinumab treatment (Brightling et al., 2015; Panettieri et al., 2018; Gottlow et al., 2019).
In conclusion, inhibition of IL-4 and IL-13, and to a lesser degree inhibition of IL-13 alone, may benefit patients with T2 high asthma, such as those with elevated FeNO levels, elevated blood eosinophils (≥300 cells/µL) or sputum eosinophils (≥3%), and/or elevated periostin. It may also benefit patients with concomitant chronic rhinosinusitis.
Omalizumab binds IgE in the blood and interstitial fluid as well as membrane bound IgE on the surface of B lymphocytes. Omalizumab decreased asthma symptoms in patients with severe, uncontrolled asthma (n = 850) over 48 weeks (Hanania et al., 2011). In another study omalizumab might have benefitted patients with type 2 high asthma; allergic asthma and non-allergic asthma with high levels of FeNO, IL-14, eosinophils or periostin (Loureiro et al., 2018). Additionally, omalizumab has been proven beneficial for patients with chronic rhinosinusitis with nasal polyps (Damask et al., 2022; Gevaert et al., 2022), though neither comorbid allergic rhinoconjunctivitis, chronic rhinosinusitis, recurrent acute sinusitis nor nasal polyps was associated with the treatment response of omalizumab on asthma (Chen et al., 2021).
Quilizumab is a humanized IgG1 monoclonal antibody targeting IgE, leading to depletion of IgE-switched B-cells and memory B cells (Harris et al., 2016). It reduced serum IgE levels and attenuated the early and late asthmatic reaction following allergen challenge in 36 patients with mild asthma (Gauvreau et al., 2014b). Quilizumab reduced total-serum and allergen-specific IgE levels by 30%–40%, but had no impact on asthma exacerbations, lung function, or symptoms in an RCT on 578 patients with allergic asthma that could not be controlled by high-dose ICS (Harris et al., 2016).
In conclusion, anti-IgE treatment may have a role in particular subgroups of patients with type 2 high asthma or allergies, but no certain clinical markers or biomarkers that defines these subgroups has been identified.
TSLP is a member of the IL-2 cytokine family and is released from airway epithelia into the bronchoalveolar fluid as part of an allergic inflammatory response and may play a role in asthma pathogenesis that is primarily T2 driven (Li et al., 2018; Peebles and Aronica, 2019). Tezepelumab is an anti-TSLP human monoclonal antibody that reduced exacerbation rates, increased lung function, and improved asthma control and quality of life in RCTs (Corren et al., 2021b; Menzies-Gow et al., 2021; Corren et al., 2023).
Experience from the NAVIGATOR trial showed that Tezepelumab is more efficient among patients with allergies (Corren et al., 2023). The effects of tezepelumab were also greater in patients with T2 high asthma with higher levels of blood eosinophils, TSLP, FeNO, IL-5, IL-13 and serum periostin, and treatment with tezepelumab decreased the levelse of blood eosinophils, FeNO, IgE, IL-5, IL-13, periostin, TARC, and TSLP over a 52-week treatment period (Corren et al., 2021b; Menzies-Gow et al., 2021).
Histamine is released by mast cells and plays a role in regulating inflammatory processes in response to environmental allergens. These effects are mediated by T helper lymphocytes and cytokines such as IL-4, IL-10 and IL-13, which promote T2 high inflammation. Four histamine receptors are expressed in pulmonary tissue (Yamauchi et al., 2019); histamine receptor 1 (H1R) promotes cellular migration, vasodilatation and bronchoconstriction and plays a role in hypersensitivity reactions and allergic asthma. Activation of histamine receptor 4 (H4R) leads to increased expression of pro-inflammatory cytokines and migration of eosinophils (Thangam et al., 2018).
An oral H4R antagonist (JNJ-39758979) has been examined in a phase IIa RCT. The primary endpoint of improved FEV1% was not met. The study included 115 patients, who were followed during the 12-week trial. The study also found no clinically relevant changes in FeNO levels or blood or sputum eosinophil counts (Kollmeier et al., 2018).
Azithromycin is a macrolide antibiotic that may be used to control asthma. In a planned post hoc analysis of an RCT, low-dose azithromycin was given to patients with severe asthma and blood eosinophils ≤200/µL. Azithromycin protected against severe exacerbations and lower respiratory tract infections requiring treatment with antibiotics (OR, 0.44). This effect was not seen in patients with eosinophilic asthma (OR, 1.03) (Brusselle et al., 2013). Similarly, azithromycin treatment was able to reduce sputum TNFR2 and TNF levels relative to placebo, but only in patients with non-eosinophilic asthma (Niessen et al., 2021). Hence, treatment with azithromycin may be particularly suitable for patients with type 2 low asthma. On the topic of chronic rhinosinusitis with nasal polyps, Azithromycin may (de Oliveira et al., 2020) or may not (Videler et al., 2011) be beneficial, however the data is insufficient to draw a conclusion, and there is no data on the predictive value of nasal involvement in treatment of asthma with azithromycin.
CRP is a marker of inflammation and infection that is synthesized in the liver (Sigari and Ghasri, 2013). It is regulated by IL-6, which is secreted locally in response to infection and tissue injury (Tanaka et al., 2014). A prospective case–control study of 100 patients with asthma and 50 healthy control subjects investigated the correlation between hs-CRP and spirometry, as well as for clinical indications of asthma control. The study found no correlation between hs-CRP and FEV1 or other indicators of asthma control such as ACT scores. hs-CRP was elevated in all patients with asthma who participated in the study, including those with controlled asthma (Sigari and Ghasri, 2013). In contrast, one study of 30 patients with asthma and 30 healthy control subjects reported that hs-CRP was related to severity of asthma and ACT scores, highlighting hs-CRP as a possible marker for the severity and control of asthma (Kilic et al., 2012). Another study of 120 patients and 115 control subjects measured hs-CRP and ACT scores, and found higher hs-CRP measurements in patients with asthma than in healthy control subjects, which increased with disease severity. (Monadi et al., 2016). Therefore, hs-CRP measurements may be useful in predicting asthma control and treatment response.
FEV1 reversibility predicted a response to treatment with LAMA in an RCT of 237 patients with mild persistent asthma (Krishnan et al., 2022). LAMA treatment decreased airway wall thickness and improved airflow obstruction in an RCT that included 53 patients with symptomatic asthma and FEV1% 60%–90% who had previously been treated with ICS/LABA. Addition of LAMA did not affect FeNO levels (Hoshi et al., 2016). Hence, LAMA treatment may be suitable for the treatment of asthma in some patients, but further studies should investigate which phenotypes may benefit most from LAMA treatment.
RCTs have suggested that a combination of weight loss and exercise may be effective in treating obesity-associated asthma. Weight loss and exercise improved asthma control and quality of life and decreased the use of reliever medication (Stenius-Aarniala et al., 2000; Scott et al., 2013; Dias-Junior et al., 2014; Ma et al., 2015; Scott et al., 2015; Freitas et al., 2017; Ozbey et al., 2020; Turk et al., 2020). A weight reduction of as little as 5%–10% may improve asthma control (Scott et al., 2013). However, these studies all had short-term (<12 months) follow-up periods (Stenius-Aarniala et al., 2000; Scott et al., 2013; Dias-Junior et al., 2014; Ma et al., 2015; Scott et al., 2015; Freitas et al., 2017; Ozbey et al., 2020; Turk et al., 2020). An RCT of 51 patients with a mixed intervention of weight loss and exercise and a 3 months follow-up period found effects on FEV1, FVC, and levels of FeNO, IL-4, IL-6, IL-10, leptin, adiponectin, TNF-alpha, and CCL2 (Freitas et al., 2017), some of which may serve as biomarkers for treatment with weight loss and exercise.
The effects of anorectic medications, such as sibutramine (10 mg per day in patients with no cardiovascular risk factors) and orlistat (maximum dose of 120 mg per day), on asthma control in patients with obesity have also been investigated (Dias-Junior et al., 2014). Preliminary results show some promise; a study of 33 patients that investigated the effects of a calorie restricted diet and anorectics, with a 6 months follow-up period, showed that these interventions had an effect on asthma control, but no effects on sensitivity to methacholine challenge, FeNO levels, sputum counts, total IgE, or leptin, TGF-beta or eotaxin levels (Dias-Junior et al., 2014). A lot more research will be anticipated in this area with the arrival of Glucagon Like Peptide (GLP)-1 analogues.
An RCT of 34 patients with severe obesity-associated asthma who underwent a 3-month high-intensity pulmonary rehabilitation programme found sustained improvements in asthma control 9 months after the intervention (Turk et al., 2020).
Hence, pulmonary rehabilitation may be very beneficial in patients with asthma, particularly obesity-associated asthma.
An RCT that included outpatients with asthma and gastro-oesophageal reflux found that asthma symptoms were relieved or improved in 18 of 51 patients who had 40 mg of once-daily omeprazole for 8 weeks. Patients who responded well to treatment with proton pump inhibitors were more likely to have higher BMI or to have more severe reflux (Kiljander et al., 2001).
A small RCT with 36 patients looked at the effect of 2 months treatment with ataria multiflora Boiss (Z. multiflora) and saw a reduction in symptoms and an improvement in pulmonary function as well as a reduction in eosinophils and hs-CRP (Alavinezhad et al., 2022).
Serum procalcitonin-guided antimicrobial therapy allows antibiotic exposure to be reduced in patients with severe acute asthma exacerbations, with no obvious adverse effects. This was confirmed by two RCTs of 169 and 293 patients requiring hospitalization for severe acute exacerbations of asthma. Serum procalcitonin-guided antimicrobial therapy was compared to standard antimicrobial therapy, and at 12-month follow-up, patients treated using the procalcitonin-guided antimicrobial therapy were substantially less likely to require antibiotic therapy. This was achieved without inferior outcomes in terms of clinical recovery, length of hospital stay, clinical, laboratory and spirometry measures (Tang et al., 2013; Long et al., 2014).
Although the phenotyping/endotyping of asthma and identification of relevant biomarkers provides opportunities to target treatments towards the underlying causes of the disease, there are also challenges and issues associated with the use of precision medicine via biomarkers. Some of these issues partly explain why biomarker measurements are not yet routinely used in clinical practice.
First, identifying patient phenotypes is time consuming and requires extra resources. Furthermore, reimbursement may not be as readily available for phenotyping as it is for other standard diagnostic tests. Second, some of the currently available biomarkers are measured from sputum samples, which may cause discomfort for patients, and requires specialist equipment and training, and the identification of phenotypes involves extra laboratory work. Third, there is a substantial gap in the available, RCT tested biomarkers used in everyday clinical life to assess relevant treatment options and treatment optimisation for patients with severe or difficult to treat asthma. This gap can only be closed by substantial research within the field, both in the areas of primary research and subsequent clinical testing in RCTs.
In some cases, asthma can remit to a less symptomatic and less severe disease level. In these cases it is important to focus on a therapeutical step down strategy. Focus on limiting oral corticosteroid treatment is already in practice, however step down of other side-effect prone therapeutics should also be prioritised. Even treatment with biologics may be reduced without recurrence of a severe asthma phenotype after a period with well-controlled disease. At present, we have very little biomarkers predictive of remission. Some biomarkers may aide in determining a relevant ICS dose, and procalcitonin can predict when antibiotic treatment can be stopped against an infectious asthma exacerbation. This is valuable, as ICS is a cornerstone in asthma treatment and overuse of antibiotics poses a huge challenge worldwide. However, there is a substantial gap in biomarkers predictive of disease remission and safe step-down of therapeutic treatment.
Asthma phenotypes may vary over time, and ideally, annual phenotyping may be required to update relevant treatment indication. Moreover, many asthma phenotypes, especially T2 low phenotypes, still lack relevant treatment options and not all treatments are endorsed by payers (e.g., treatment with anorectics and instructor guided exercise for obesity-associated asthma). Finally, current guidelines are not yet updated to endorse the use of biomarkers and precision medicine to treat asthma that is not severe.
Using biomarkers, it has become possible to identify subgroups of patients with severe asthma based on different phenotypes and endotypes. This process is ongoing and new findings are needed and constantly emerging, altering the way asthma is classified. Discovery of new biomarkers, improvement in the understanding of biomarkers associated with different types of asthma will and already is creating opportunities to offer targeted biologic treatments to patients with severe, uncontrolled asthma.
Some of these biomarkers may be used to fine-tune treatments and reduce corticosteroid use or dosage. Improvements in these guided treatment methods based on personalized medicine may result in simpler, cheaper treatment programmes that are more widely endorsed by clinicians, benefitting more patients with asthma.
BB: Conceptualization, Writing–original draft. J-UJ: Writing–review and editing. Writing–original draft. AM: Writing–review and editing. AC: Writing–review and editing. PS: Conceptualization, Writing–original draft and editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The research salary of PS was sponsored by Herlev and Gentofte Hospital, University of Copenhagen. AGM was supported by the National Institute for Health and Care Research Manchester Biomedical Research Centre (NIHR Manchester BRC, NIHR203308) and by an NIHR Clinical Lectureship in Respiratory Medicine. This work was supported by the COP:TRIN network www.coptrin.dk.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Akar-Ghibril, N., Casale, T., Custovic, A., and Phipatanakul, W. (2020). Allergic endotypes and phenotypes of asthma. J. Allergy Clin. Immunol. Pract. 8 (2), 429–440. doi:10.1016/j.jaip.2019.11.008
Alavinezhad, A., Ghorani, V., Rajabi, O., and Boskabady, M. H. (2022). Zataria multiflora extract influenced asthmatic patients by improving respiratory symptoms, pulmonary function tests and lung inflammation. J. Ethnopharmacol. 285, 114888. doi:10.1016/j.jep.2021.114888
Asthma, G. I. f. (2022). Global strategy for asthma management and prevention. Available from: www.ginasthma.org.
Austin, C. D., Gonzalez Edick, M., Ferrando, R. E., Solon, M., Baca, M., Mesh, K., et al. (2020). A randomized, placebo-controlled trial evaluating effects of lebrikizumab on airway eosinophilic inflammation and remodelling in uncontrolled asthma (CLAVIER). Clin. Exp. Allergy 50 (12), 1342–1351. doi:10.1111/cea.13731
Ayars, A. G., Altman, L. C., Potter-Perigo, S., Radford, K., Wight, T. N., and Nair, P. (2013). Sputum hyaluronan and versican in severe eosinophilic asthma. Int. Arch. Allergy Immunol. 161 (1), 65–73. doi:10.1159/000343031
Bachert, C., Han, J. K., Desrosiers, M. Y., Gevaert, P., Heffler, E., Hopkins, C., et al. (2022). Efficacy and safety of benralizumab in chronic rhinosinusitis with nasal polyps: a randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 149 (4), 1309–1317 e12. doi:10.1016/j.jaci.2021.08.030
Bardin, P., Kanniess, F., Gauvreau, G., Bredenbröker, D., and Rabe, K. F. (2015). Roflumilast for asthma: efficacy findings in mechanism of action studies. Pulm. Pharmacol. Ther. 35, S4–S10. doi:10.1016/j.pupt.2015.08.006
Bateman, E. D., Goehring, U. M., Richard, F., and Watz, H. (2016). Roflumilast combined with montelukast versus montelukast alone as add-on treatment in patients with moderate-to-severe asthma. J. Allergy Clin. Immunol. 138 (1), 142–149. doi:10.1016/j.jaci.2015.11.035
Berthon, B. S., Gibson, P. G., Wood, L. G., MacDonald-Wicks, L. K., and Baines, K. J. (2017). A sputum gene expression signature predicts oral corticosteroid response in asthma. Eur. Respir. J. 49 (6), 1700180. doi:10.1183/13993003.00180-2017
Boer, S., Sont, J. K., Loijmans, R. J. B., Snoeck-Stroband, J. B., Ter Riet, G., Schermer, T. R. J., et al. (2019). Development and validation of personalized prediction to estimate future risk of severe exacerbations and uncontrolled asthma in patients with asthma, using clinical parameters and early treatment response. J. Allergy Clin. Immunol. Pract. 7 (1), 175–182. doi:10.1016/j.jaip.2018.06.007
Bose, S., Bime, C., Henderson, R. J., Blake, K. V., Castro, M., DiMango, E., et al. (2020). Biomarkers of type 2 airway inflammation as predictors of loss of asthma control during step-down therapy for well-controlled disease: the long-acting beta-agonist step-down study (LASST). J. Allergy Clin. Immunol. Pract. 8 (10), 3474–3481. doi:10.1016/j.jaip.2020.06.067
Bousquet, J., Aubier, M., Sastre, J., Izquierdo, J. L., Adler, L. M., Hofbauer, P., et al. (2006). Comparison of roflumilast, an oral anti-inflammatory, with beclomethasone dipropionate in the treatment of persistent asthma. Allergy 61 (1), 72–78. doi:10.1111/j.1398-9995.2005.00931.x
Brandsma, J., Schofield, J. P. R., Yang, X., Strazzeri, F., Barber, C., Goss, V. M., et al. (2023). Stratification of asthma by lipidomic profiling of induced sputum supernatant. J. Allergy Clin. Immunol. 152 (1), 117–125. doi:10.1016/j.jaci.2023.02.032
Brightling, C. E., Chanez, P., Leigh, R., O'Byrne, P. M., Korn, S., She, D., et al. (2015). Efficacy and safety of tralokinumab in patients with severe uncontrolled asthma: a randomised, double-blind, placebo-controlled, phase 2b trial. Lancet Respir. Med. 3 (9), 692–701. doi:10.1016/S2213-2600(15)00197-6
Brusselle, G. G., and Koppelman, G. H. (2022). Biologic therapies for severe asthma. N. Engl. J. Med. 386 (2), 157–171. doi:10.1056/NEJMra2032506
Brusselle, G. G., Vanderstichele, C., Jordens, P., Deman, R., Slabbynck, H., Ringoet, V., et al. (2013). Azithromycin for prevention of exacerbations in severe asthma (AZISAST): a multicentre randomised double-blind placebo-controlled trial. Thorax 68 (4), 322–329. doi:10.1136/thoraxjnl-2012-202698
Busse, W. W., Holgate, S. T., Wenzel, S. W., Klekotka, P., Chon, Y., Feng, J., et al. (2015). Biomarker profiles in asthma with high vs low airway reversibility and poor disease control. Chest 148 (6), 1489–1496. doi:10.1378/chest.14-2457
Busse, W. W. (2019). Biological treatments for severe asthma: a major advance in asthma care. Allergol. Int. 68 (2), 158–166. doi:10.1016/j.alit.2019.01.004
Busse, W. W., Maspero, J. F., Lu, Y., Corren, J., Hanania, N. A., Chipps, B. E., et al. (2020). Efficacy of dupilumab on clinical outcomes in patients with asthma and perennial allergic rhinitis. Ann. Allergy Asthma Immunol. 125 (5), 565–576. doi:10.1016/j.anai.2020.05.026
Calhoun, W. J., Ameredes, B. T., King, T. S., Icitovic, N., Bleecker, E. R., Castro, M., et al. (2012). Comparison of physician-biomarker-and symptom-based strategies for adjustment of inhaled corticosteroid therapy in adults with asthma: the BASALT randomized controlled trial. JAMA 308 (10), 987–997. doi:10.1001/2012.jama.10893
Castillo, J. R., Peters, S. P., and Busse, W. W. (2017). Asthma exacerbations: pathogenesis, prevention, and treatment. J. Allergy Clin. Immunol. Pract. 5 (4), 918–927. doi:10.1016/j.jaip.2017.05.001
Castro, M., Corren, J., Pavord, I. D., Maspero, J., Wenzel, S., Rabe, K. F., et al. (2018). Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N. Engl. J. Med. 378 (26), 2486–2496. doi:10.1056/NEJMoa1804092
Castro, M., Zangrilli, J., Wechsler, M. E., Bateman, E. D., Brusselle, G. G., Bardin, P., et al. (2015). Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet Respir. Med. 3 (5), 355–366. doi:10.1016/S2213-2600(15)00042-9
Chambers, E. S., Nanzer, A. M., Pfeffer, P. E., Richards, D. F., Timms, P. M., Martineau, A. R., et al. (2015). Distinct endotypes of steroid-resistant asthma characterized by IL-17A(high) and IFN-γ(high) immunophenotypes: potential benefits of calcitriol. J. Allergy Clin. Immunol. 136 (3), 628–637. doi:10.1016/j.jaci.2015.01.026
Chen, M., Choo, E., Yoo, B., Raut, P., Haselkorn, T., Pazwash, H., et al. (2021). No difference in omalizumab efficacy in patients with asthma by number of asthma-related and allergic comorbidities. Ann. Allergy Asthma Immunol. 126 (6), 666–673. doi:10.1016/j.anai.2021.01.015
Chen, W., Reddel, H. K., FitzGerald, J. M., Beasley, R., Janson, C., and Sadatsafavi, M. (2023). Can we predict who will benefit most from biologics in severe asthma? A post-hoc analysis of two phase 3 trials. Respir. Res. 24 (1), 120. doi:10.1186/s12931-023-02409-2
Chupp, G., Alobid, I., Lugogo, N. L., Kariyawasam, H. H., Bourdin, A., Chaker, A. M., et al. (2023). Mepolizumab reduces systemic corticosteroid use in chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. Pract. doi:10.1016/j.jaip.2023.08.015
Cianchetti, S., Cardini, C., Puxeddu, I., Latorre, M., Bartoli, M. L., Bradicich, M., et al. (2019). Distinct profile of inflammatory and remodelling biomarkers in sputum of severe asthmatic patients with or without persistent airway obstruction. World Allergy Organ J. 12 (11), 100078. doi:10.1016/j.waojou.2019.100078
Colak, Y., Afzal, S., Lange, P., and Nordestgaard, B. G. (2016). Obese individuals experience wheezing without asthma but not asthma without wheezing: a Mendelian randomisation study of 85,437 adults from the Copenhagen General Population Study. Thorax 71 (3), 247–254. doi:10.1136/thoraxjnl-2015-207379
Corren, J., Ambrose, C. S., Griffiths, J. M., Hellqvist, Å., Lindsley, A. W., Llanos, J. P., et al. (2023). Efficacy of tezepelumab in patients with evidence of severe allergic asthma: results from the phase 3 NAVIGATOR study. Clin. Exp. Allergy 53 (4), 417–428. doi:10.1111/cea.14256
Corren, J., Katelaris, C. H., Castro, M., Maspero, J. F., Ford, L. B., Halpin, D. M. G., et al. (2021a). Effect of exacerbation history on clinical response to dupilumab in moderate-to-severe uncontrolled asthma. Eur. Respir. J. 58 (4), 2004498. doi:10.1183/13993003.04498-2020
Corren, J., Pham, T.-H., Garcia Gil, E., Sałapa, K., Parnes, J. R., Colice, G., et al. (2021b). Baseline type 2 biomarker levels and response to tezepelumab in severe asthma. Allergy 77 (6), 1786–1796. doi:10.1111/all.15197
Couillard, S., Shrimanker, R., Chaudhuri, R., Mansur, A. H., McGarvey, L. P., Heaney, L. G., et al. (2021). Fractional exhaled nitric oxide nonsuppression identifies corticosteroid-resistant type 2 signaling in severe asthma. Am. J. Respir. Crit. Care Med. 204, 731–734. doi:10.1164/rccm.202104-1040LE
Damask, C., Chen, M., Holweg, C. T. J., Yoo, B., Millette, L. A., and Franzese, C. (2022). Defining the efficacy of omalizumab in nasal polyposis: a polyp 1 and polyp 2 subgroup analysis. Am. J. Rhinol. Allergy 36 (1), 135–141. doi:10.1177/19458924211030486
de Oliveira, I. S., Guimaraes, A. F., Arantes Pêgas, G. F., Machado, C. J., Cassali, G. D., Barbosa Nunes, F., et al. (2020). Azithromycin for chronic eosinophilic rhinosinusitis with nasal polyp: a placebo-controlled trial. Rhinology 58 (6), 610–617. doi:10.4193/Rhin20.071
Dias-Junior, S. A., Reis, M., de Carvalho-Pinto, R. M., Stelmach, R., Halpern, A., and Cukier, A. (2014). Effects of weight loss on asthma control in obese patients with severe asthma. Eur. Respir. J. 43 (5), 1368–1377. doi:10.1183/09031936.00053413
Dixon, A. E., Shade, D. M., Cohen, R. I., Skloot, G. S., Holbrook, J. T., Smith, L. J., et al. (2006). Effect of obesity on clinical presentation and response to treatment in asthma. J. Asthma 43 (7), 553–558. doi:10.1080/02770900600859123
Djukanovic, R., Harrison, T., Johnston, S. L., Gabbay, F., Wark, P., Thomson, N. C., et al. (2014). The effect of inhaled IFN-beta on worsening of asthma symptoms caused by viral infections. A randomized trial. Am. J. Respir. Crit. Care Med. 190 (2), 145–154. doi:10.1164/rccm.201312-2235OC
Eastwood, M. C., Busby, J., Jackson, D. J., Pavord, I. D., Hanratty, C. E., Djukanovic, R., et al. (2023). A randomized trial of a composite T2-biomarker strategy adjusting corticosteroid treatment in severe asthma: a post hoc analysis by sex. J. Allergy Clin. Immunol. Pract. 11 (4), 1233–1242 e5. doi:10.1016/j.jaip.2022.12.019
Eriksson, J., Ekerljung, L., Bossios, A., Bjerg, A., Wennergren, G., Rönmark, E., et al. (2015). Aspirin-intolerant asthma in the population: prevalence and important determinants. Clin. Exp. Allergy 45 (1), 211–219. doi:10.1111/cea.12359
Fahy, J. V. (2015). Type 2 inflammation in asthma--present in most, absent in many. Nat. Rev. Immunol. 15 (1), 57–65. doi:10.1038/nri3786
FitzGerald, J. M., Bleecker, E. R., Nair, P., Korn, S., Ohta, K., Lommatzsch, M., et al. (2016). Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet 388 (10056), 2128–2141. doi:10.1016/S0140-6736(16)31322-8
Fowler, S. J., Tavernier, G., and Niven, R. (2015). High blood eosinophil counts predict sputum eosinophilia in patients with severe asthma. J. Allergy Clin. Immunol. 135 (3), 822–824. doi:10.1016/j.jaci.2014.09.034
Freitas, P. D., Ferreira, P. G., Silva, A. G., Stelmach, R., Carvalho-Pinto, R. M., Fernandes, F. L. A., et al. (2017). The role of exercise in a weight-loss program on clinical control in obese adults with asthma. A randomized controlled trial. Am. J. Respir. Crit. Care Med. 195 (1), 32–42. doi:10.1164/rccm.201603-0446OC
Fricker, M., Gibson, P. G., Powell, H., Simpson, J. L., Yang, I. A., Upham, J. W., et al. (2019). A sputum 6-gene signature predicts future exacerbations of poorly controlled asthma. J. Allergy Clin. Immunol. 144 (1), 51–60. doi:10.1016/j.jaci.2018.12.1020
Gauvreau, G. M., Boulet, L. P., Cockcroft, D. W., FitzGerald, J. M., Mayers, I., Carlsten, C., et al. (2014a). OX40L blockade and allergen-induced airway responses in subjects with mild asthma. Clin. Exp. Allergy 44 (1), 29–37. doi:10.1111/cea.12235
Gauvreau, G. M., Harris, J. M., Boulet, L. P., Scheerens, H., Fitzgerald, J. M., Putnam, W. S., et al. (2014b). Targeting membrane-expressed IgE B cell receptor with an antibody to the M1 prime epitope reduces IgE production. Sci. Transl. Med. 6 (243), 243ra85. doi:10.1126/scitranslmed.3008961
Gevaert, P., Saenz, R., Corren, J., Han, J. K., Mullol, J., Lee, S. E., et al. (2022). Long-term efficacy and safety of omalizumab for nasal polyposis in an open-label extension study. J. Allergy Clin. Immunol. 149 (3), 957–965 e3. doi:10.1016/j.jaci.2021.07.045
Gottlow, M., Svensson, D. J., Lipkovich, I., Huhn, M., Bowen, K., Wessman, P., et al. (2019). Application of structured statistical analyses to identify a biomarker predictive of enhanced tralokinumab efficacy in phase III clinical trials for severe, uncontrolled asthma. BMC Pulm. Med. 19 (1), 129. doi:10.1186/s12890-019-0889-4
Hanania, N. A., Alpan, O., Hamilos, D. L., Condemi, J. J., Reyes-Rivera, I., Zhu, J., et al. (2011). Omalizumab in severe allergic asthma inadequately controlled with standard therapy: a randomized trial. Ann. Intern Med. 154 (9), 573–582. doi:10.7326/0003-4819-154-9-201105030-00002
Hanania, N. A., Castro, M., Bateman, E., Pavord, I. D., Papi, A., FitzGerald, J. M., et al. (2023). Efficacy of dupilumab in patients with moderate-to-severe asthma and persistent airflow obstruction. Ann. Allergy Asthma Immunol. 130 (2), 206–214 e2. doi:10.1016/j.anai.2022.10.018
Hanania, N. A., Korenblat, P., Chapman, K. R., Bateman, E. D., Kopecky, P., Paggiaro, P., et al. (2016). Efficacy and safety of lebrikizumab in patients with uncontrolled asthma (LAVOLTA I and LAVOLTA II): replicate, phase 3, randomised, double-blind, placebo-controlled trials. Lancet Respir. Med. 4 (10), 781–796. doi:10.1016/S2213-2600(16)30265-X
Harris, J. M., Maciuca, R., Bradley, M. S., Cabanski, C. R., Scheerens, H., Lim, J., et al. (2016). A randomized trial of the efficacy and safety of quilizumab in adults with inadequately controlled allergic asthma. Respir. Res. 17, 29. doi:10.1186/s12931-016-0347-2
Harrison, T., Canonica, G. W., Chupp, G., Lee, J., Schleich, F., Welte, T., et al. (2020). Real-world mepolizumab in the prospective severe asthma REALITI-A study: initial analysis. Eur. Respir. J. 56 (4), 2000151. doi:10.1183/13993003.00151-2020
Hastie, A. T., Moore, W. C., Li, H., Rector, B. M., Ortega, V. E., Pascual, R. M., et al. (2013). Biomarker surrogates do not accurately predict sputum eosinophil and neutrophil percentages in asthmatic subjects. J. Allergy Clin. Immunol. 132 (1), 72–80. doi:10.1016/j.jaci.2013.03.044
Heaney, L. G., Busby, J., Hanratty, C. E., Djukanovic, R., Woodcock, A., Walker, S. M., et al. (2021). Composite type-2 biomarker strategy versus a symptom-risk-based algorithm to adjust corticosteroid dose in patients with severe asthma: a multicentre, single-blind, parallel group, randomised controlled trial. Lancet Respir. Med. 9 (1), 57–68. doi:10.1016/S2213-2600(20)30397-0
Honkoop, P. J., Loijmans, R. J. B., Termeer, E. H., Snoeck-Stroband, J. B., van den Hout, W. B., Bakker, M. J., et al. (2015). Symptom- and fraction of exhaled nitric oxide-driven strategies for asthma control: a cluster-randomized trial in primary care. J. Allergy Clin. Immunol. 135 (3), 682–688.e11. doi:10.1016/j.jaci.2014.07.016
Hoshino, M., Ohtawa, J., and Akitsu, K. (2016). Effect of treatment with inhaled corticosteroid on serum periostin levels in asthma. Respirology 21 (2), 297–303. doi:10.1111/resp.12687
Hoshino, M., Ohtawa, J., and Akitsu, K. (2016). Effects of the addition of tiotropium on airway dimensions in symptomatic asthma. Allergy Asthma Proc. 37 (6), 147–153. doi:10.2500/aap.2016.37.3991
Huang, F., del-Río-Navarro, B. E., Alcántara, S. T., Ontiveros, J. A. P., Cienfuegos, D. R. P., Bello González, S. A., et al. (2012). Plasminogen activator inhibitor-1, fibrinogen, and lung function in adolescents with asthma and obesity. Endocr. Res. 37 (3), 135–144. doi:10.3109/07435800.2012.654555
Ingram, J. L., and Kraft, M. (2012). IL-13 in asthma and allergic disease: asthma phenotypes and targeted therapies. J. Allergy Clin. Immunol. 130 (4), 829–842. quiz 843-4. doi:10.1016/j.jaci.2012.06.034
Jarvis, D., Chinn, S., Potts, J., and Burney, P.European Community Respiratory Health Survey (2002). Association of body mass index with respiratory symptoms and atopy: results from the European Community Respiratory Health Survey. Clin. Exp. Allergy 32 (6), 831–837. doi:10.1046/j.1365-2222.2002.01380.x
Kachroo, P., Sordillo, J. E., Lutz, S. M., Weiss, S. T., Kelly, R. S., McGeachie, M. J., et al. (2021). Pharmaco-metabolomics of inhaled corticosteroid response in individuals with asthma. J. Pers. Med. 11 (11), 1148. doi:10.3390/jpm11111148
Kanagalingam, S., Shehab, S. S., Kaminsky, D. A., Wise, R. A., Lang, J. E., and Dixon, A. E. (2018). Effect of obesity on sinonasal disease in asthma. J. Asthma 55 (5), 525–531. doi:10.1080/02770903.2017.1341522
Katoh, S., Matsumoto, N., Tanaka, H., Yasokawa, N., Kittaka, M., Kurose, K., et al. (2020). Elevated levels of periostin and TGF-β1 in the bronchoalveolar lavage fluid of patients with idiopathic eosinophilic pneumonia. Asian Pac J. Allergy Immunol. 38 (3), 208–213. doi:10.12932/AP-111018-0414
Kilic, H., Karalezli, A., Hasanoglu, H. C., Erel, O., and Ates, C. (2012). The relationship between hs-CRP and asthma control test in asthmatic patients. Allergol. Immunopathol. Madr. 40 (6), 362–367. doi:10.1016/j.aller.2011.10.002
Kiljander, T., Salomaa, E. R., Hietanen, E., Helenius, H., Liippo, K., and Terho, E. O. (2001). Asthma and gastro-oesophageal reflux: can the response to anti-reflux therapy be predicted? Respir. Med. 95 (5), 387–392. doi:10.1053/rmed.2001.1055
Kollmeier, A. P., Greenspan, A., Xu, X. L., Silkoff, P. E., Barnathan, E. S., Loza, M. J., et al. (2018). Phase 2a, randomized, double-blind, placebo-controlled, multicentre, parallel-group study of an H4 R-antagonist (JNJ-39758979) in adults with uncontrolled asthma. Clin. Exp. Allergy 48 (8), 957–969. doi:10.1111/cea.13154
Krishnan, J. A., Lazarus, S. C., Blake, K. V., Sorkness, C. A., Covar, R., Dyer, A. M., et al. (2022). Biomarkers to predict response to inhaled corticosteroids and long-acting muscarinic antagonists in adolescents and adults with mild persistent asthma. Ann. Am. Thorac. Soc. 19 (3), 372–380. doi:10.1513/AnnalsATS.202105-613OC
Kuo, C. R., Spears, M., Haughney, J., Smith, A., Miller, J., Bradshaw, T., et al. (2019). Scottish consensus statement on the role of FeNO in adult asthma. Respir. Med. 155, 54–57. doi:10.1016/j.rmed.2019.07.010
Kupczyk, M., Dahlén, B., Sterk, P. J., Nizankowska-Mogilnicka, E., Papi, A., Bel, E. H., et al. (2014). Stability of phenotypes defined by physiological variables and biomarkers in adults with asthma. Allergy 69 (9), 1198–1204. doi:10.1111/all.12445
Kupczyk, M., Haque, S., Middelveld, R. J. M., Dahlén, B., and Dahlén, S. E.BIOAIR Investigators (2013). Phenotypic predictors of response to oral glucocorticosteroids in severe asthma. Respir. Med. 107 (10), 1521–1530. doi:10.1016/j.rmed.2013.07.014
Kuruvilla, M. E., Lee, F. E., and Lee, G. B. (2019). Understanding asthma phenotypes, endotypes, and mechanisms of disease. Clin. Rev. Allergy Immunol. 56 (2), 219–233. doi:10.1007/s12016-018-8712-1
Lang, D. M., Aronica, M. A., Maierson, E. S., Wang, X. F., Vasas, D. C., and Hazen, S. L. (2018). Omalizumab can inhibit respiratory reaction during aspirin desensitization. Ann. Allergy Asthma Immunol. 121 (1), 98–104. doi:10.1016/j.anai.2018.05.007
Leija-Martinez, J. J., Patricio-Román, K. L., Del-Río-Navarro, B. E., Villalpando-Carrión, S., Reyes-Garay, J. A., Vélez-Reséndiz, J. M., et al. (2021). Retinol-binding protein 4 and plasminogen activator inhibitor-1 as potential prognostic biomarkers of non-allergic asthma caused by obesity in adolescents. Allergol. Immunopathol. Madr. 49 (3), 21–29. doi:10.15586/aei.v49i3.73
Li, Y., Wang, W., Lv, Z., Li, Y., Chen, Y., Huang, K., et al. (2018). Elevated expression of IL-33 and TSLP in the airways of human asthmatics in vivo: a potential biomarker of severe refractory disease. J. Immunol. 200 (7), 2253–2262. doi:10.4049/jimmunol.1701455
Liu, L., Zhang, X., Liu, Y., Zhang, L., Zheng, J., Wang, J., et al. (2019). Chitinase-like protein YKL-40 correlates with inflammatory phenotypes, anti-asthma responsiveness and future exacerbations. Respir. Res. 20 (1), 95. doi:10.1186/s12931-019-1051-9
Liu, M. C., Bagnasco, D., Matucci, A., Pilette, C., Price, R. G., Maxwell, A. C., et al. (2023). Mepolizumab in patients with severe asthma and comorbidities: 1-year REALITI-A analysis. J. Allergy Clin. Immunol. Pract. doi:10.1016/j.jaip.2023.07.024
Loftus, P. A., and Wise, S. K. (2015). Epidemiology and economic burden of asthma. Int. Forum Allergy Rhinol. 5 (1), S7–S10. doi:10.1002/alr.21547
Long, W., Li, L. J., Huang, G. Z., Zhang, X. M., Zhang, Y. C., Tang, J. G., et al. (2014). Procalcitonin guidance for reduction of antibiotic use in patients hospitalized with severe acute exacerbations of asthma: a randomized controlled study with 12-month follow-up. Crit. Care 18 (5), 471. doi:10.1186/s13054-014-0471-7
Loureiro, C. C., Amaral, L., Ferreira, J. A., Lima, R., Pardal, C., Fernandes, I., et al. (2018). Omalizumab for severe asthma: beyond allergic asthma. Biomed. Res. Int. 2018, 3254094. doi:10.1155/2018/3254094
Loymans, R. J., Honkoop, P. J., Termeer, E. H., Snoeck-Stroband, J. B., Assendelft, W. J. J., Schermer, T. R. J., et al. (2016). Identifying patients at risk for severe exacerbations of asthma: development and external validation of a multivariable prediction model. Thorax 71 (9), 838–846. doi:10.1136/thoraxjnl-2015-208138
Lv, N., Xiao, L., Camargo, C. A., Wilson, S. R., Buist, A. S., Strub, P., et al. (2014). Abdominal and general adiposity and level of asthma control in adults with uncontrolled asthma. Ann. Am. Thorac. Soc. 11 (8), 1218–1224. doi:10.1513/AnnalsATS.201405-214OC
Ma, J., Strub, P., Xiao, L., Lavori, P. W., Camargo, C. A., Wilson, S. R., et al. (2015). Behavioral weight loss and physical activity intervention in obese adults with asthma. A randomized trial. Ann. Am. Thorac. Soc. 12 (1), 1–11. doi:10.1513/AnnalsATS.201406-271OC
Malinovschi, A., Van Muylem, A., Michiels, S., and Michils, A. (2014). FeNO as a predictor of asthma control improvement after starting inhaled steroid treatment. Nitric Oxide 40, 110–116. doi:10.1016/j.niox.2014.06.009
Maniscalco, M., Paris, D., Melck, D. J., Molino, A., Carone, M., Ruggeri, P., et al. (2018). Differential diagnosis between newly diagnosed asthma and COPD using exhaled breath condensate metabolomics: a pilot study. Eur. Respir. J. 51 (3), 1701825. doi:10.1183/13993003.01825-2017
Maspero, J. F., Katelaris, C. H., Busse, W. W., Castro, M., Corren, J., Chipps, B. E., et al. (2020). Dupilumab efficacy in uncontrolled, moderate-to-severe asthma with self-reported chronic rhinosinusitis. J. Allergy Clin. Immunol. Pract. 8 (2), 527–539. doi:10.1016/j.jaip.2019.07.016
Matsumoto, H. (2020). Role of serum periostin in the management of asthma and its comorbidities. Respir. Investig. 58 (3), 144–154. doi:10.1016/j.resinv.2020.02.003
McDowell, P. J., Busby, J., Hanratty, C. E., Djukanovic, R., Woodcock, A., Walker, S., et al. (2022). Exacerbation profile and risk factors in a type-2-low enriched severe asthma cohort: a clinical trial to assess asthma exacerbation phenotypes. Am. J. Respir. Crit. Care Med. 206 (5), 545–553. doi:10.1164/rccm.202201-0129OC
Menzies-Gow, A., Corren, J., Bourdin, A., Chupp, G., Israel, E., Wechsler, M. E., et al. (2021). Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N. Engl. J. Med. 384 (19), 1800–1809. doi:10.1056/NEJMoa2034975
Molfino, N. A., Kuna, P., Leff, J. A., Oh, C. K., Singh, D., Chernow, M., et al. (2016). Phase 2, randomised placebo-controlled trial to evaluate the efficacy and safety of an anti-GM-CSF antibody (KB003) in patients with inadequately controlled asthma. BMJ Open 6 (1), e007709. doi:10.1136/bmjopen-2015-007709
Monadi, M., Firouzjahi, A., Hosseini, A., Javadian, Y., Sharbatdaran, M., and Heidari, B. (2016). Serum C-reactive protein in asthma and its ability in predicting asthma control, a case-control study. Casp. J. Intern Med. 7 (1), 37–42.
Murata, K., Koga, Y., Kasahara, N., Hachisu, Y., Nunomura, S., Nakajima, N., et al. (2018). Accumulation of periostin in acute exacerbation of familial idiopathic pulmonary fibrosis. J. Thorac. Dis. 10 (7), E587–E591. doi:10.21037/jtd.2018.06.96
Neelamegan, R., Saka, V., Tamilarasu, K., Rajaram, M., Selvarajan, S., and Chandrasekaran, A. (2016). Clinical utility of fractional exhaled nitric oxide (FeNO) as a biomarker to predict severity of disease and response to inhaled corticosteroid (ICS) in asthma patients. J. Clin. Diagn Res. 10 (12), FC01–FC06. doi:10.7860/JCDR/2016/20656.8950
Niessen, N. M., Gibson, P. G., Baines, K. J., Barker, D., Yang, I. A., Upham, J. W., et al. (2021). Sputum TNF markers are increased in neutrophilic and severe asthma and are reduced by azithromycin treatment. Allergy 76 (7), 2090–2101. doi:10.1111/all.14768
Nonaka, M., Sakanushi, A., Kusama, K., Ogihara, N., and Yagi, T. (2010). One-year evaluation of combined treatment with an intranasal corticosteroid and montelukast for chronic rhinosinusitis associated with asthma. J. Nippon. Med. Sch. 77 (1), 21–28. doi:10.1272/jnms.77.21
Nukui, Y., Miyazaki, Y., Masuo, M., Okamoto, T., Furusawa, H., Tateishi, T., et al. (2019). Periostin as a predictor of prognosis in chronic bird-related hypersensitivity pneumonitis. Allergol. Int. 68 (3), 363–369. doi:10.1016/j.alit.2019.02.007
O'Byrne, P. M., Metev, H., Puu, M., Richter, K., Keen, C., Uddin, M., et al. (2016). Efficacy and safety of a CXCR2 antagonist, AZD5069, in patients with uncontrolled persistent asthma: a randomised, double-blind, placebo-controlled trial. Lancet Respir. Med. 4 (10), 797–806. doi:10.1016/S2213-2600(16)30227-2
Ortega, H., Li, H., Suruki, R., Albers, F., Gordon, D., and Yancey, S. (2014b). Cluster analysis and characterization of response to mepolizumab. A step closer to personalized medicine for patients with severe asthma. Ann. Am. Thorac. Soc. 11 (7), 1011–1017. doi:10.1513/AnnalsATS.201312-454OC
Ortega, H. G., Liu, M. C., Pavord, I. D., Brusselle, G. G., FitzGerald, J. M., Chetta, A., et al. (2014a). Mepolizumab treatment in patients with severe eosinophilic asthma. N. Engl. J. Med. 371 (13), 1198–1207. doi:10.1056/NEJMoa1403290
Ortega, H. G., Yancey, S. W., Mayer, B., Gunsoy, N. B., Keene, O. N., Bleecker, E. R., et al. (2016). Severe eosinophilic asthma treated with mepolizumab stratified by baseline eosinophil thresholds: a secondary analysis of the DREAM and MENSA studies. Lancet Respir. Med. 4 (7), 549–556. doi:10.1016/S2213-2600(16)30031-5
Ozbey, U., Balaban, S., Sözener, Z. Ç., Uçar, A., Mungan, D., and Mısırlıgil, Z. (2020). The effects of diet-induced weight loss on asthma control and quality of life in obese adults with asthma: a randomized controlled trial. J. Asthma 57 (6), 618–626. doi:10.1080/02770903.2019.1590594
Panettieri, R. A., Sjöbring, U., Péterffy, A., Wessman, P., Bowen, K., Piper, E., et al. (2018). Tralokinumab for severe, uncontrolled asthma (STRATOS 1 and STRATOS 2): two randomised, double-blind, placebo-controlled, phase 3 clinical trials. Lancet Respir. Med. 6 (7), 511–525. doi:10.1016/S2213-2600(18)30184-X
Park, H. S., Kim, M. K., Imai, N., Nakanishi, T., Adachi, M., Ohta, K., et al. (2016). A phase 2a study of benralizumab for patients with eosinophilic asthma in South Korea and Japan. Int. Arch. Allergy Immunol. 169 (3), 135–145. doi:10.1159/000444799
Pavord, I. D., Afzalnia, S., Menzies-Gow, A., and Heaney, L. G. (2017). The current and future role of biomarkers in type 2 cytokine-mediated asthma management. Clin. Exp. Allergy 47 (2), 148–160. doi:10.1111/cea.12881
Pavord, I. D., Deniz, Y., Corren, J., Casale, T. B., FitzGerald, J. M., Izuhara, K., et al. (2023). Baseline FeNO independently predicts the dupilumab response in patients with moderate-to-severe asthma. J. Allergy Clin. Immunol. Pract. 11 (4), 1213–1220 e2. doi:10.1016/j.jaip.2022.11.043
Pavord, I. D., Holliday, M., Reddel, H. K., Braithwaite, I., Ebmeier, S., Hancox, R. J., et al. (2020). Predictive value of blood eosinophils and exhaled nitric oxide in adults with mild asthma: a prespecified subgroup analysis of an open-label, parallel-group, randomised controlled trial. Lancet Respir. Med. 8 (7), 671–680. doi:10.1016/S2213-2600(20)30053-9
Peebles, R. S., and Aronica, M. A. (2019). Proinflammatory pathways in the pathogenesis of asthma. Clin. Chest Med. 40 (1), 29–50. doi:10.1016/j.ccm.2018.10.014
Peters, M. C., Mauger, D., Ross, K. R., Phillips, B., Gaston, B., Cardet, J. C., et al. (2020). Evidence for exacerbation-prone asthma and predictive biomarkers of exacerbation frequency. Am. J. Respir. Crit. Care Med. 202 (7), 973–982. doi:10.1164/rccm.201909-1813OC
Peters-Golden, M., Swern, A., Bird, S. S., Hustad, C. M., Grant, E., and Edelman, J. M. (2006). Influence of body mass index on the response to asthma controller agents. Eur. Respir. J. 27 (3), 495–503. doi:10.1183/09031936.06.00077205
Pham, T. H., Damera, G., Newbold, P., and Ranade, K. (2016). Reductions in eosinophil biomarkers by benralizumab in patients with asthma. Respir. Med. 111, 21–29. doi:10.1016/j.rmed.2016.01.003
Rhyou, H. I., and Nam, Y. H. (2020). Predictive factors of response to inhaled corticosteroids in newly diagnosed asthma: a real-world observational study. Ann. Allergy Asthma Immunol. 125 (2), 177–181. doi:10.1016/j.anai.2020.04.025
Riccio, A. M., Mauri, P., De Ferrari, L., Rossi, R., Di Silvestre, D., Bartezaghi, M., et al. (2020). Plasma Galectin-3 and urine proteomics predict FEV(1) improvement in omalizumab-treated patients with severe allergic asthma: results from the PROXIMA sub-study. World Allergy Organ J. 13 (1), 100095. doi:10.1016/j.waojou.2019.100095
Robinson, D., Humbert, M., Buhl, R., Cruz, A. A., Inoue, H., Korom, S., et al. (2017). Revisiting Type 2-high and Type 2-low airway inflammation in asthma: current knowledge and therapeutic implications. Clin. Exp. Allergy 47 (2), 161–175. doi:10.1111/cea.12880
Romanet-Manent, S., Charpin, D., Magnan, A., Lanteaume, A., and Vervloet, D.EGEA Cooperative Group (2002). Allergic vs nonallergic asthma: what makes the difference? Allergy 57 (7), 607–613. doi:10.1034/j.1398-9995.2002.23504.x
Saito, N., Kamata, A., Itoga, M., Tamaki, M., Kayaba, H., and Ritz, T. (2017). Assessment of biological, psychological and adherence factors in the prediction of step-down treatment for patients with well-controlled asthma. Clin. Exp. Allergy 47 (4), 467–478. doi:10.1111/cea.12888
Schatz, M., and Rosenwasser, L. (2014). The allergic asthma phenotype. J. Allergy Clin. Immunol. Pract. 2 (6), 645–648. doi:10.1016/j.jaip.2014.09.004
Scheerens, H., Arron, J. R., Zheng, Y., Putnam, W. S., Erickson, R. W., Choy, D. F., et al. (2014). The effects of lebrikizumab in patients with mild asthma following whole lung allergen challenge. Clin. Exp. Allergy 44 (1), 38–46. doi:10.1111/cea.12220
Schoettler, N., and Strek, M. E. (2020). Recent advances in severe asthma: from phenotypes to personalized medicine. Chest 157 (3), 516–528. doi:10.1016/j.chest.2019.10.009
Schoors, D. F., De Smet, M., Reiss, T., Margolskee, D., Cheng, H., Larson, P., et al. (1995). Single dose pharmacokinetics, safety and tolerability of MK-0476, a new leukotriene D4-receptor antagonist, in healthy volunteers. Br. J. Clin. Pharmacol. 40 (3), 277–280. doi:10.1111/j.1365-2125.1995.tb05785.x
Scott, H. A., Gibson, P. G., Garg, M. L., Pretto, J. J., Morgan, P. J., Callister, R., et al. (2013). Dietary restriction and exercise improve airway inflammation and clinical outcomes in overweight and obese asthma: a randomized trial. Clin. Exp. Allergy 43 (1), 36–49. doi:10.1111/cea.12004
Scott, H. A., Gibson, P. G., Garg, M. L., Pretto, J. J., Morgan, P. J., Callister, R., et al. (2015). Determinants of weight loss success utilizing a meal replacement plan and/or exercise, in overweight and obese adults with asthma. Respirology 20 (2), 243–250. doi:10.1111/resp.12423
Shrestha, S. K., Drews, A., Sharma, L., Pant, S., and Neopane, A. (2018). Relationship between total serum immunoglobulin E levels, fractional exhaled breath nitric oxide levels and absolute blood eosinophil counts in atopic and non-atopic asthma: a controlled comparative study. J. Breath. Res. 12 (2), 026009. doi:10.1088/1752-7163/aa95da
Sigari, N., and Ghasri, H. (2013). Correlation between hs-CRP and asthma control indices. Tanaffos 12 (3), 44–48.
Solanki, B., Prakash, A., Rehan, H. S., and Gupta, L. K. (2019). Effect of inhaled corticosteroids on serum periostin levels in adult patients with mild-moderate asthma. Allergy Asthma Proc. 40 (1), 32–34. doi:10.2500/aap.2019.40.4179
Sparreman Mikus, M., Kolmert, J., Andersson, L. I., Östling, J., Knowles, R. G., Gómez, C., et al. (2022). Plasma proteins elevated in severe asthma despite oral steroid use and unrelated to Type-2 inflammation. Eur. Respir. J. 59 (2), 2100142. doi:10.1183/13993003.00142-2021
Stenius-Aarniala, B., Poussa, T., Kvarnström, J., Grönlund, E. L., Ylikahri, M., and Mustajoki, P. (2000). Immediate and long term effects of weight reduction in obese people with asthma: randomised controlled study. BMJ 320 (7238), 827–832. doi:10.1136/bmj.320.7238.827
Sun, Y., Shi, Z., Liu, B., Li, X., Li, G., Yang, F., et al. (2020). YKL-40 mediates airway remodeling in asthma via activating FAK and MAPK signaling pathway. Cell Cycle 19 (11), 1378–1390. doi:10.1080/15384101.2020.1750811
Sutherland, L., Shaw, K., Parrish, C., Singleton, N., McKeever, T. M., Stewart, I., et al. (2021). A low exhaled nitric oxide level excludes a short-term benefit from inhaled corticosteroids in suspected asthma: a randomized placebo-controlled trial. Respirology 26 (7), 666–672. doi:10.1111/resp.14055
Suzuki, M., Cole, J. J., Konno, S., Makita, H., Kimura, H., Nishimura, M., et al. (2021). Large-scale plasma proteomics can reveal distinct endotypes in chronic obstructive pulmonary disease and severe asthma. Clin. Transl. Allergy 11 (10), e12091. doi:10.1002/clt2.12091
Takahashi, K., Meguro, K., Kawashima, H., Kashiwakuma, D., Kagami, S. I., Ohta, S., et al. (2019). Serum periostin levels serve as a biomarker for both eosinophilic airway inflammation and fixed airflow limitation in well-controlled asthmatics. J. Asthma 56 (3), 236–243. doi:10.1080/02770903.2018.1455855
Tanaka, T., Narazaki, M., and Kishimoto, T. (2014). IL-6 in inflammation, immunity, and disease. Cold Spring Harb. Perspect. Biol. 6 (10), a016295. doi:10.1101/cshperspect.a016295
Tang, J., Long, W., Yan, L., Zhang, Y., Xie, J., Lu, G., et al. (2013). Procalcitonin guided antibiotic therapy of acute exacerbations of asthma: a randomized controlled trial. BMC Infect. Dis. 13, 596. doi:10.1186/1471-2334-13-596
Taylor, S. L., Leong, L. E. X., Choo, J. M., Wesselingh, S., Yang, I. A., Upham, J. W., et al. (2018). Inflammatory phenotypes in patients with severe asthma are associated with distinct airway microbiology. J. Allergy Clin. Immunol. 141 (1), 94–103. doi:10.1016/j.jaci.2017.03.044
Thangam, E. B., Jemima, E. A., Singh, H., Baig, M. S., Khan, M., Mathias, C. B., et al. (2018). The role of histamine and histamine receptors in mast cell-mediated allergy and inflammation: the hunt for new therapeutic targets. Front. Immunol. 9, 1873. doi:10.3389/fimmu.2018.01873
Timmer, W., Leclerc, V., Birraux, G., Neuhäuser, M., Hatzelmann, A., Bethke, T., et al. (2002). The new phosphodiesterase 4 inhibitor roflumilast is efficacious in exercise-induced asthma and leads to suppression of LPS-stimulated TNF-alpha ex vivo. J. Clin. Pharmacol. 42 (3), 297–303. doi:10.1177/00912700222011328
Truong-Thanh, T., Vo-Thi-Kim, A., Vu-Minh, T., Truong-Viet, D., Tran-Van, H., and Duong-Quy, S. (2020). The beneficial role of FeNO in association with GINA guidelines for titration of inhaled corticosteroids in adult asthma: a randomized study. Adv. Med. Sci. 65 (2), 244–251. doi:10.1016/j.advms.2020.03.001
Tsurikisawa, N., Oshikata, C., Sato, T., Kimura, G., Mizuki, M., Tsuburai, T., et al. (2018). Low variability in peak expiratory flow predicts successful inhaled corticosteroid step-down in adults with asthma. J. Allergy Clin. Immunol. Pract. 6 (3), 972–979. doi:10.1016/j.jaip.2017.10.036
Tsurikisawa, N., Oshikata, C., Tsuburai, T., Mitsui, C., Tanimoto, H., Takahashi, K., et al. (2012). Markers for step-down of inhaled corticosteroid therapy in adult asthmatics. Allergol. Int. 61 (3), 419–429. doi:10.2332/allergolint.11-OA-0402
Turk, Y., Theel, W., van Huisstede, A., van de Geijn, G. J. M., Birnie, E., Hiemstra, P. S., et al. (2020). Short-term and long-term effect of a high-intensity pulmonary rehabilitation programme in obese patients with asthma: a randomised controlled trial. Eur. Respir. J. 56 (1), 1901820. doi:10.1183/13993003.01820-2019
Tversky, J., Lane, A. P., and Azar, A. (2021). Benralizumab effect on severe chronic rhinosinusitis with nasal polyps (CRSwNP): a randomized double-blind placebo-controlled trial. Clin. Exp. Allergy 51 (6), 836–844. doi:10.1111/cea.13852
Videler, W. J., Badia, L., Harvey, R. J., Gane, S., Georgalas, C., van der Meulen, F. W., et al. (2011). Lack of efficacy of long-term, low-dose azithromycin in chronic rhinosinusitis: a randomized controlled trial. Allergy 66 (11), 1457–1468. doi:10.1111/j.1398-9995.2011.02693.x
Wechsler, M. E., Ruddy, M. K., Pavord, I. D., Israel, E., Rabe, K. F., Ford, L. B., et al. (2021). Efficacy and safety of itepekimab in patients with moderate-to-severe asthma. N. Engl. J. Med. 385 (18), 1656–1668. doi:10.1056/NEJMoa2024257
Weinstein, S. F., Katial, R. K., Bardin, P., Korn, S., McDonald, M., Garin, M., et al. (2019). Effects of reslizumab on asthma outcomes in a subgroup of eosinophilic asthma patients with self-reported chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. Pract. 7 (2), 589–596. doi:10.1016/j.jaip.2018.08.021
Wenzel, S., Ford, L., Pearlman, D., Spector, S., Sher, L., Skobieranda, F., et al. (2013). Dupilumab in persistent asthma with elevated eosinophil levels. N. Engl. J. Med. 368 (26), 2455–2466. doi:10.1056/NEJMoa1304048
Yamada, H., Nakajima, M., Matsuyama, M., Morishima, Y., Arai, N., Hida, N., et al. (2021). Identification of distinct phenotypes related to benralizumab responsiveness in patients with severe eosinophilic asthma. PLoS One 16 (3), e0248305. doi:10.1371/journal.pone.0248305
Yamauchi, K., and Ogasawara, M. (2019). The role of histamine in the pathophysiology of asthma and the clinical efficacy of antihistamines in asthma therapy. Int. J. Mol. Sci. 20 (7), 1733. doi:10.3390/ijms20071733
Yang, F., Busby, J., Heaney, L. G., Pavord, I. D., Brightling, C. E., Borg, K., et al. (2022). Corticosteroid responsiveness following mepolizumab in severe eosinophilic asthma-A randomized, placebo-controlled crossover trial (MAPLE). J. Allergy Clin. Immunol. Pract. 10 (11), 2925–2934 e12. doi:10.1016/j.jaip.2022.06.050
Keywords: asthma, biomarker, phenotype, personalized medicine, asthma treatment
Citation: Bonnesen B, Jensen J-US, Mathioudakis AG, Corlateanu A and Sivapalan P (2023) Promising treatment biomarkers in asthma. Front. Drug Saf. Regul. 3:1291471. doi: 10.3389/fdsfr.2023.1291471
Received: 09 September 2023; Accepted: 25 October 2023;
Published: 07 November 2023.
Edited by:
Josuel Ora, Policlinico Tor Vergata, ItalyReviewed by:
Konstantinos Bartziokas, Independent Researcher, Trikala, GreeceCopyright © 2023 Bonnesen, Jensen, Mathioudakis, Corlateanu and Sivapalan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pradeesh Sivapalan, UHJhZGVlc2guc0BkYWRsbmV0LmRr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.